
Abstract
Objective:
ADHD and borderline personality (BP) disorder are highly comorbid and characterized by emotion dysregulation and peer problems. However, limited research has examined social and emotional predictors of BP features in samples that include youth with ADHD.
Method:
Using a sample of 124 youth with and without ADHD (52% female), ADHD symptoms, peer problems, and emotion dysregulation were assessed in childhood (8–13 years) and in adolescence, along with BP features (13–18 years).
Results:
In addition to the significant effect of ADHD symptoms, teacher-rated child peer victimization and adolescent-reported peer victimization, poorer close friendships, and emotion dysregulation domains significantly predicted adolescent BP features. Greater parent-rated child and adolescent emotion dysregulation domains also significantly predicted adolescent BP features, with ADHD symptoms no longer significant.
Conclusion:
Even for youth with ADHD, peer and emotional vulnerabilities in childhood and adolescence may serve as important markers of risk for adolescent BP features.
There is high comorbidity between ADHD and borderline personality (BP) disorder (Matthies & Philipsen, 2014; Xenaki & Pehlivanidis, 2015), with an estimated 14% of youth with ADHD being diagnosed with BP disorder in adulthood (Matthies & Philipsen, 2014). ADHD is a disorder that first emerges in childhood and is characterized by developmentally atypical difficulties with attention, hyperactivity, and/or impulsivity (American Psychiatric Association [APA], 2013). In contrast, BP disorder is typically not diagnosed until late adolescence or adulthood (APA, 2013), though growing evidence suggests that BP features, including affective instability, identity problems, negative relationships, and self-harm first emerge in childhood (Babinski et al., 2021; Crick et al., 2005; Zanarini et al., 2006). Although research suggests a strong co-occurrence between childhood ADHD symptoms and BP features (Babinski & McQuade, 2019; Babinski et al., 2021; Burke & Stepp, 2012; Haltigan & Vaillancourt, 2016; Stepp et al., 2012; Vaillancourt et al., 2014), the mechanisms linking these symptom domains are not well understood.
ADHD and BP disorder may share an underlying vulnerability for behavioral dysregulation and impulsivity that manifests as symptoms of both disorders (Xenaki & Pehlivanidis, 2015); however, it is also possible that other impairments common to both disorders account for their co-occurrence. Youth with ADHD often display emotion dysregulation (Bunford et al., 2015; Graziano & Garcia, 2016) and peer problems (McQuade, 2020), which have also been identified as predictors of vulnerability for BP features (e.g., Crick et al., 2005; Ibraheim et al., 2017). Yet to date, there has been limited research examining emotion dysregulation and peer problems as vulnerabilities for BP features in samples that include children with ADHD. Given that BP disorder is associated with significant personal, economic, and societal costs (van Asselt et al., 2007), with between 2% and 4% of individuals dying by suicide (Alvarez-Tomas et al., 2019), identifying predictors of the emergence of BP features in adolescence, particularly for at-risk youth, is critically important. Consequently, the present study used a sample of youth with and without ADHD and examined whether emotion dysregulation or peer problems in childhood or adolescence were unique predictors of elevated adolescent BP features when also accounting for the effects of ADHD symptoms.
Emotion dysregulation has been described as a core deficit of both ADHD (Bunford et al., 2015; Graziano & Garcia, 2016) and BP disorder (Carpenter & Trull, 2013; Putnam & Silk, 2005). In BP disorder, emotion dysregulation manifests as high emotional reactivity, heightened and labile negative affect, deficits in adaptive emotion regulation strategies, and reliance on maladaptive emotion regulation strategies (Carpenter & Trull, 2013). High emotional reactivity and lability and impaired emotion regulation strategies also characterize the emotion dysregulation observed in youth with ADHD (Graziano & Garcia, 2016), suggesting that there is overlap in the emotion dysregulation profiles of the two disorders. In adult women, self-reported emotion dysregulation accounted for the effect of retrospectively reported child ADHD symptoms on adult BP disorder (Fossati et al., 2015), which may suggest that emotion dysregulation is a key impairment linking these disorders. However, other work suggests that specific emotion dysregulation deficits may also serve as unique markers of risk for BP features when also accounting for the effects of other forms of psychopathology. Specifically, in an adolescent inpatient sample, adolescents with BP disorder displayed greater concurrent self-reported impulse control difficulties when emotional and had more limited access to emotion regulation strategies as compared to youth with other psychiatric disorders, including ADHD (Ibraheim et al., 2017). However, prior research has been cross-sectional and clinic referred (Fossati et al., 2015; Ibraheim et al., 2017), limiting conclusions about longitudinal processes and if effects are consistent in samples that represent a broader range of impairment levels.
Another shared impairment between ADHD and BP disorder are peer problems (McQuade, 2020; Runions et al., 2021). BP disorder is characterized by unstable relationships and avoidance of abandonment (APA, 2013), which may first emerge in peer relationship challenges. Indeed, research has found that a range of peer problems, including more negative peer relationships, heightened aggression, and peer victimization are observed in youth high in BP features (Runions et al., 2021). In childhood, youth at risk for BP features may be less socially accepted and more disliked by peers (Cicchetti et al., 2014; Rogosch & Cicchetti, 2005). As youth transition into pre-adolescence and adolescence, problems in close friendships including greater exclusivity, more conflict, and less support, also predict BP feature elevations (Crick et al., 2005; Kawabata et al., 2014; Koster et al., 2018). In addition, aggression toward peers and being the target of peer aggression (i.e., peer victimization) have both been identified as markers of risk for BP features concurrently (Babinski & McQuade, 2019; Haltigan & Vaillancourt, 2016) and longitudinally (Crick et al., 2005; Kawabata et al., 2014; Vaillancourt et al., 2014; Winsper et al., 2017; Wolke et al., 2012). These different peer challenges may serve as early indicators of instability in relationships and promote fears of abandonment that are characteristic of BP disorder (APA, 2013). Interestingly, youth with ADHD commonly display peer problems in these same domains (McQuade, 2020), yet little work has jointly considered the effects of ADHD symptoms and peer problems in predicting adolescent BP features. In typically developing samples, peer aggression and victimization were found to uniquely predict later elevations in BP features when also accounting for the effects of ADHD symptoms (Vaillancourt et al., 2014; Winsper et al., 2017). However, only one study has examined the unique effects of peer variables on BP features in a sample that included girls with ADHD, finding that BP features, rather than ADHD symptoms, were significantly associated with concurrent peer aggression (Babinski & McQuade, 2019). Thus it remains unclear, particularly in samples that include youth with ADHD, whether specific peer challenges serve as additional markers of risk for BP features.
Present Study
The present study used a sample of youth with and without ADHD that were assessed both in childhood and adolescence and examined emotion dysregulation and peer problems as longitudinal and concurrent predictors of adolescent BP features when also considering the effects of ADHD symptoms. ADHD symptoms, BP features, and risk factors were examined dimensionally, consistent with a developmental psychopathology perspective, which argues that categorical treatment of symptoms and risk factors creates false distinctions between dimensional constructs (Garber & Bradshaw, 2020). This approach is also consistent with research suggesting that ADHD symptoms and BP features exist along a continuum and that even subthreshold elevations are associated with impairment (Balázs & Keresztény, 2014; Thompson et al., 2019). Inclusion of youth with and without clinical elevations in ADHD symptoms also enabled an examination of associations between risk factors and BP features across a broad range of impairment levels. Although, prior research with this sample has examined concurrent associations between ADHD symptoms, peer problems, and emotion dysregulation in childhood (McQuade & Breaux, 2017; McQuade et al., 2018) and adolescence (McQuade et al., 2021) and the longitudinal effects of childhood parenting on adolescent BP features (McQuade et al., 2022), child or adolescent emotion dysregulation and peer problems have not been examined as predictors of BP features in the present sample. In childhood, teacher and child self-reports of peer problems were assessed, allowing for examination of both adult-observed and child-perceived peer problems; peer problems included aggression, victimization, and peer social acceptance. In childhood, only parent report of children’s emotion dysregulation was available. In adolescence, peer problems were assessed based on adolescent report alone, given that teachers may have less opportunity to observe adolescents socially. In addition to aggression and victimization, adolescent intimacy and trust in close friendships was assessed, given that in adolescence, close relationships become an important way to develop the social skills needed for healthy adult intimate relationships (Grover & Nangle, 2007) and thus may be an important indicator of social vulnerability at this developmental time point. Adolescent emotion dysregulation was assessed based on both parent and adolescent reports, given evidence that adolescents can provide valid information about their emotion dysregulation (Bunford et al., 2020); multiple raters also allowed for an examination of both adult-observed and self-reported subjective emotion dysregulation. Given potential influences of sex on rates of ADHD and BP disorder (APA, 2013), youth sex was also included as a unique predictor in all models. It was hypothesized that there would be both longitudinal and concurrent relationships between youth ADHD symptoms and adolescent BP feature elevations, but that emotion dysregulation and peer problems would also incrementally predict BP elevations.
Method
Participants
Participants were a community sample of youth with and without clinical elevations in ADHD symptoms. To maximize variability in ADHD symptom levels, participants were recruited from fliers posted at healthcare provider’s offices, ADHD specialty clinics, community locations (e.g., public libraries), online, and in newspapers; however, families were not actively referred from healthcare settings. Children were excluded from the original study if they had a diagnosis of autism spectrum disorder or bipolar disorder, had an estimated IQ below 80, were on a medication that could not be withdrawn for the initial child assessment, there was diagnostic uncertainty regarding ADHD status, or the child displayed severe behavior problems during the first study visit that invalidated key measures (McQuade et al., 2017). A sample of 124 youth participated in an initial child study when they were 8 to 12 years-old (M = 10.50, SD = 1.33; McQuade et al., 2017) which included an assessment of peer problems. A subset of 61 youth who participated in the initial child visit also completed a second child study visit 1 year later, when they were 9 to 13 years-old (M = 11.62, SD = 1.29; McQuade & Breaux, 2017) that assessed emotion dysregulation; due to the primary aims of the study, children with clinical elevations in ADHD symptoms were only recontacted if they had at least three symptoms of hyperactivity-impulsivity. Five to 6 years after the initial child study visit, all parents who gave permission to be contacted about future research during the first child visit were re-recruited and invited to complete an online follow-up assessment when youth were 13 and 18 years-old (M = 16.15, SD = 1.40; McQuade et al., 2021), data was provided for 88 adolescents. Figure 1 displays a flow-chart of participation. The full sample assessed at the initial child visit (n = 124) was 52% female and racial distribution was 88% white, 8% other or mixed race, 3% Asian, and 1% Black or African American; 10% identified as Hispanic or Latinx. Parent reporters were 88% mothers, average highest parent education was 16.57 years (SD = 1.05) and the median household income was $90,000 USD. There were no significant demographic differences in youth who did or did not also complete the second child visit or adolescent follow-up.
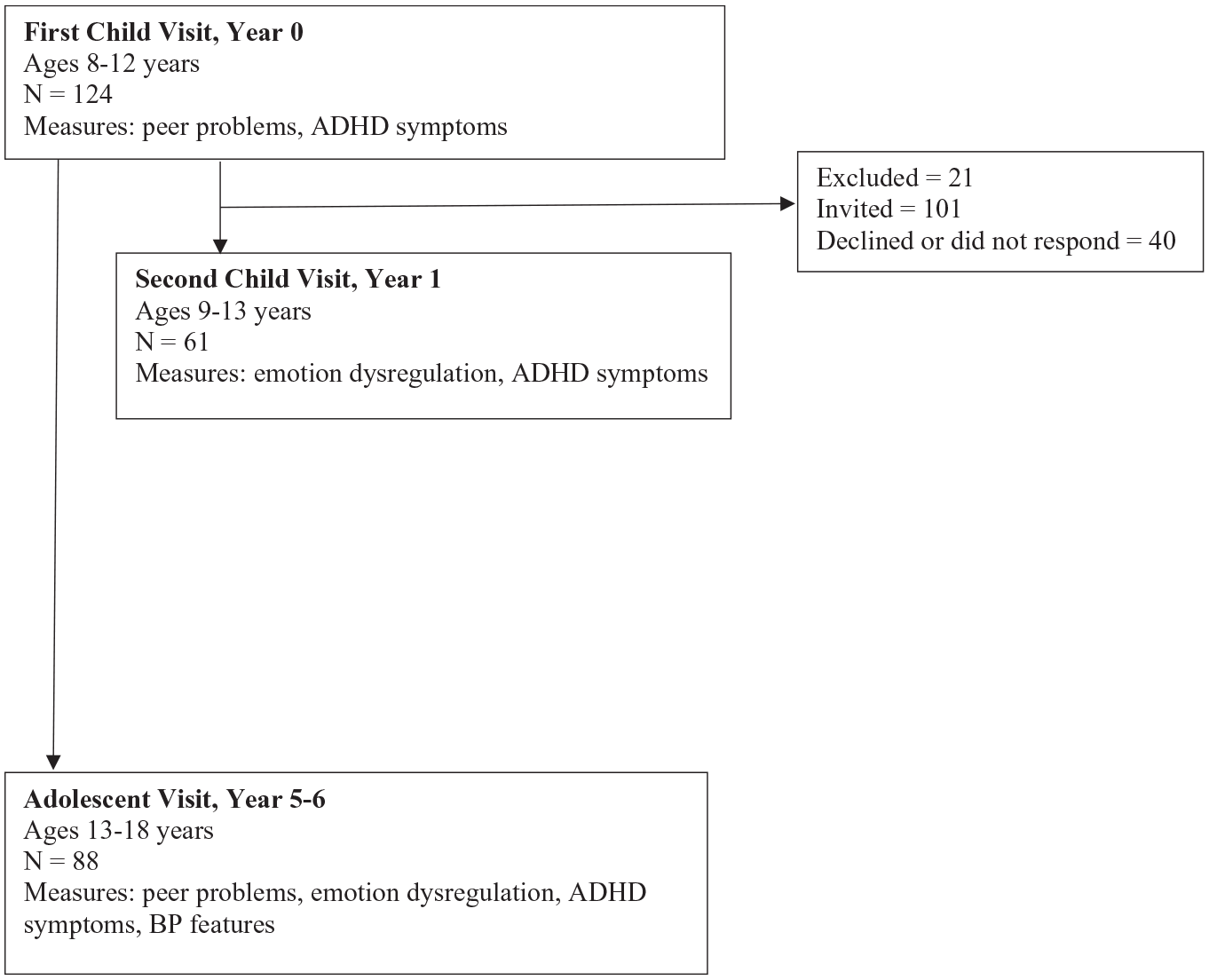
Flow chart of assessment points and participation.
Although symptoms were examined dimensionally, an ADHD diagnostic assessment was completed at the initial child study visit to ensure wide variability in symptom levels within the sample. The assessment included parent report on a semi-structured interview and structured clinical interview and symptom rating scales from a parent and teacher. Based on agreement by a doctorate level psychologist and a clinical psychology graduate student, 40 children (32%; 30% female) met full Diagnostic and Statistical Manual, Fifth Edition (DSM-5; APA, 2013) criteria for ADHD (15 predominantly inattentive, 4 predominantly hyperactive-impulsive, 21 combined presentations), 19 children (15%; 42% female) were classified as displaying subclinical ADHD (i.e., 4 or 5 symptoms of inattention or hyperactivity-impulsivity and meeting DSM-5 cross-domain impairment and age of onset criteria), and 65 children (53%; 69% female) did not meet criteria for ADHD. In adolescence, 65% of adolescents initially identified as having full or subthreshold ADHD in childhood continued to display full or subthreshold ADHD symptoms based on parent report on the Disruptive Behavior Disorder Rating Scale (Pelham et al., 1992). At the first study visit, less parent education and being male were significantly associated with greater ADHD symptoms; no other demographic features related to ADHD symptoms.
The Amherst College Institutional Review Board approved all study procedures at the initial child visit, second child visit, and adolescent follow-up. At each assessment, participating parents provided informed consent for youth under 18 years-old and youth provided assent. Adolescents who were 18 years-old provided consent. During each of the child visits, parents and children completed study measures during laboratory visits and teachers were invited to complete measures online. For the adolescent follow-up, the parent and adolescent each independently completed study measures online. Relevant to this study, at the initial child study visit, measures of childhood ADHD symptoms and peer problems were collected. At the second child study visit, measures of childhood ADHD symptoms and emotion dysregulation were collected. At the adolescent assessment, measures of ADHD symptoms, peer problems, emotion dysregulation, and BP features were collected.
Measures
ADHD symptoms
ADHD symptoms were measured dimensionally at each assessment using the Disruptive Behavior Disorders Rating Scale (DBD; Pelham et al., 1992) which includes the 18 DSM symptoms of ADHD. Adults rated each symptom on a 0 (not at all) to 3 (very much) scale, with items rated as (2) pretty much or (3) very much present counted as endorsed symptoms. At the childhood visits, the parent and teacher each completed the DBD and symptoms endorsed by either rater were counted as present. In adolescence, only parents completed the DBD. Total ADHD symptom counts were computed at each measurement point (αs = .93–.96). 1
Childhood peer aggression
Peer aggression was measured at the initial child visit using teacher and self-report on the Children’s Social Behavior Questionnaire (Crick, 1996). The teacher version included nine items assessing relational (e.g., “spreads rumors or gossips about some peers”) or physical aggression (e.g., “hits or kicks peers”), with items rated on a 1 (never true) to 5 (almost always true) scale. The child version included eight items assessing relational (e.g., “tell lies about a classmate so that the other kids won’t like the classmate anymore”) or overt aggression (e.g., “hit other kids at school”), with items rated on a 1 (never) to 5 (all the time) scale. Items were average to compute teacher- (α = .88) and child-reported aggression (α = .85) scores.
Childhood peer victimization
Peer victimization was measured at the initial child study visit using teacher and self-report on the Children’s Social Experiences Questionnaire (Cullerton-Sen & Crick, 2005). The teacher version included six items describing physical (e.g., “gets hit or kicked by peers”) or relational victimization (e.g., “gets ignored by other children when a peer is mad at them”), with items rated on a 1 (never) to 5 (almost always) scale. The child version included 10 items describing overt (e.g., “get hit by another kid at school”) or relational victimization (e.g., “other kids leave you out on purpose when it is time to play or do an activity”), with items rated on a 1 (never) to 5 (all the time) scale. Teacher- (α = .78) and child-reported victimization (α = .93) were computed by averaging items.
Childhood peer social acceptance
Children’s peer social acceptance was measured at the initial child visit using teacher and self-report on the social acceptance scale from the Self-Perceptions Profile for Children (SPPC; Harter, 2012). Raters read two statements and selected the statement that best described the child (i.e., “Some kids find it hard to make friends” versus “Other kids find it pretty easy to make friends”) and then rated if the statement was sort of true or really true. Items were scored on a 1 to 4 scale, with higher values indicating greater perceived social acceptance; items were averaged to compute subscale scores for the teacher (α = .87) and the child’s rating (α = .83).
Childhood emotion dysregulation
Children’s emotion dysregulation was measured at the second child visit using parent report on the Emotion Regulation Checklist (ERC; Shields & Cicchetti, 1997), which includes two subscales. The negativity/lability subscale (15 items; α = .90) describes labile and intense emotions (e.g., “has wild mood swings,” “can keep his/her excitement under control”); lower scores are more adaptive. The emotion regulation subscale (eight items; α = .72) describes appropriate understanding and responding to emotions (e.g., “is able to say when he/she is feeling sad, angry or mad, fearful or afraid,” “responds positively when another child approaches him/her in a friendly or neutral manner”); higher scores are more adaptive. Parents rated how often their child exhibited behaviors on a 1 (rarely/never) to 4 (almost always) scale, which were averaged to create subscale scores.
Adolescent peer victimization and aggression
Adolescent victimization and aggression was measured at the adolescent follow-up using self-report on the Revised Peer Experiences Questionnaire (Prinstein et al., 2001). Items describe experiences of overt (e.g., “a teen hit, kicked, or pushed me in a mean way”) or relational victimization (e.g., “a teen left me out of what they were doing”) or engagement in overt (e.g., “I hit, kicked, or pushed a teen in a mean way”) or relational aggression (e.g., “I left a teen out of what I was doing”). Adolescents rated the frequency of experiences on a 1 (never) to 5 (a few times a week) scale and victimization (α = .75) and aggression items (α = .83) were separately averaged to create two subscale scores.
Adolescent close friendship
Adolescent close friendships was measured at the adolescent follow-up using self-report on the close friendship subscale from the Self-Perception Profile for Adolescents (Harter, 2012). Six items assessed the presence of close friends whom the adolescent can share personal thoughts and secrets (e.g., “I have a close friend I can share secrets with”). Consistent with prior scoring (Wichstrøm, 1995), respondents were presented with a single description of competency and rated how true the statement was from 1 (describes me/them very poorly) to 4 (describes me/them very well); items were scored such that higher values indicated greater competency and were averaged (α = .77).
Adolescent emotion dysregulation
Adolescent emotion dysregulation was measured at the adolescent follow-up with both self- and parent-report on the Difficulties in Emotion Regulation Scale (DERS; Bunford et al., 2020; Gratz & Roemer, 2004). The adolescent version (Gratz & Roemer, 2004), includes six subscales: non-acceptance of emotions (α = .86), impulse control difficulties when emotional (α = .86), limited access to emotion regulation strategies (α = .90), lack of emotional awareness (α = .87), lack of emotional clarity (α = .77), and difficulty engaging in goal-directed behaviors when emotional (α = .86). The parent version (Bunford et al., 2020) includes parallel items that load onto four subscales 2 : non-acceptance of emotions (α = .88), a combined impulse control difficulties/limited access to emotion regulation strategies (α = .93), a combined lack of emotional awareness/clarity (α = .92), and difficulty engaging in goal directed behavior when emotional (α = .87). Respondents rated items on a 1 (almost never) to 5 (almost always) scale, with items averaged to compute subscale scores.
Adolescent BP features
Adolescent BP features were assessed dimensionally at the adolescent follow-up with both adolescent and parent report on the Borderline Personality Features Scale for Children (Crick et al., 2005). There are 24 items describing BP features of affective instability (e.g., “I go back and forth between different feelings, like being mad or sad or happy”), identity problems (e.g., “I feel that there is something important missing about me, but I don’t know what it is”), negative relationships (e.g., I feel very lonely), and self-harm (e.g., I do things that other people consider wild or out of control). Respondents rated items on a 1 (not at all true) to 5 (always true) scale and, consistent with prior research (Babinski et al., 2021), parent and adolescent ratings were combined by taking the maximum score from the adolescent and parent on an item-by-item basis, with items summed to create a subscale score (α = .91). According to Chang et al. (2011), a score of 66 for adolescent-reported BP features and a score of 72 for parent-reported BP features serve as clinical cut-points in discriminating adolescents with BP disorder. Using these cut-points, 15.3% of adolescents (63% female) had clinical elevations on self-reported BP features and 2.4% had clinical elevations on parent-rated BP features (66% female); however, in all analyses BP features were considered dimensionally as a combined score of parent and adolescent reports.
Data Analytic Plan
Preliminary univariate analyses examined associations between demographic variables and adolescent BP features, bivariate correlations between study variables, and patterns of missingness using one-way ANOVA or chi-square tests. In the primary multivariate analyses, a series of multiple regressions were run examining whether peer problems or emotion dysregulation, assessed in either childhood or adolescence, predicted adolescent BP features when also accounting for the independent effect of ADHD symptoms. Analyses were conducted in Mplus version 8.1 (Muthén & Muthén, 2017) using maximum likelihood with robust standard errors to account for missing data and non-normality of variables. Dimensional BP features was the dependent variable in each regression. For childhood predictors, separate regressions examined child self-reported peer problems (social acceptance, victimization, and aggression), teacher-reported peer problems (social acceptance, victimization, and aggression), and parent-reported emotion dysregulation (negativity/lability and emotion regulation) as independent variables. For adolescent predictors, separate regression examined adolescent self-reported peer problems (close friendships, victimization, and aggression), adolescent self-reported emotion dysregulation (six DERS subscales), and parent rated adolescent emotion dysregulation (four DERS subscales) as independent variables. Each regression also accounted for the effect of youth sex and for age and dimensional ADHD symptoms at the time that other predictors were measured. Significance was interpreted based on unstandardized regression coefficients, with standardized coefficients included to allow comparison of the relative strength of predictors. Follow-up tests of robustness also examined is effects remained significant when a false discovery rate-controlling analysis (Benjamini & Hochberg, 1995) was conducted, with the false discovery rate set to .05.
Results
Preliminary Univariate Analyses
Demographic associations
Preliminary analyses examined associations between adolescent BP features and demographic characteristics. Older age at the initial child assessment (r = −.22, p = .040), second child assessment (r = −.25, p = .094), and adolescent assessment (r = −.23, p = .036) was significantly or marginally significantly associated with lower BP features; no other demographic features were significantly associated with BP features.
Univariate associations
Descriptive statistics and correlations of child predictors and of adolescent predictors are presented in Tables 1 and 2, respectively. Correlations between child and adolescent predictors are reported in the Supplemental Materials. In childhood, greater initial child visit and second child visit ADHD symptoms, greater self-reported aggression and victimization, greater teacher-reported victimization, and greater parent-reported negativity/lability and lower emotion regulation were each significantly correlated with greater adolescent BP features. Additionally, concurrently in adolescence, greater adolescent ADHD symptoms, all measures of peer problems, and all measures of self-reported and parent-rated emotion dysregulation were significantly correlated with greater adolescent BP features.
Descriptive Statistics and Correlations of Childhood Study Variables and Adolescent BP features.
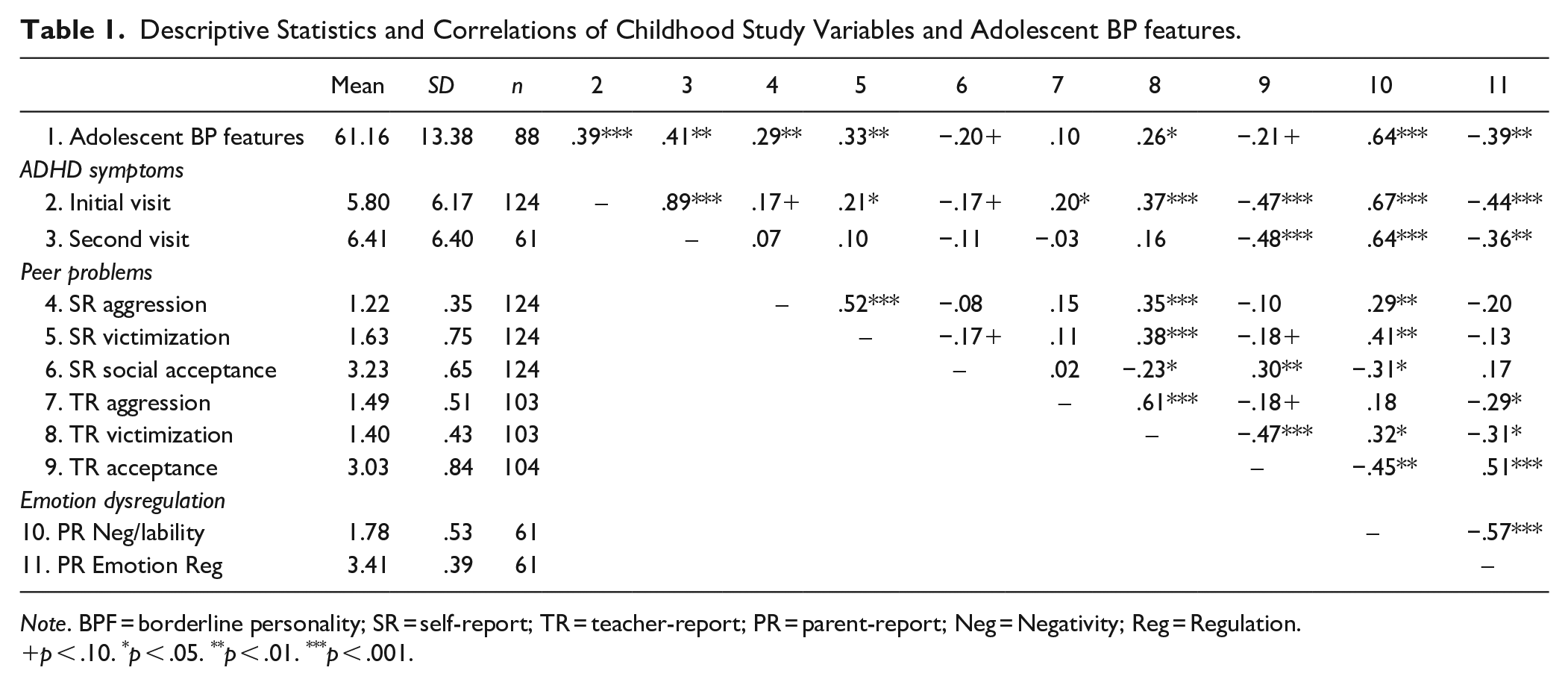
Note. BPF = borderline personality; SR = self-report; TR = teacher-report; PR = parent-report; Neg = Negativity; Reg = Regulation.
p < .10. *p < .05. **p < .01. ***p < .001.
Descriptive Statistics and Correlations of Adolescent Study Variables and Adolescent BP features.
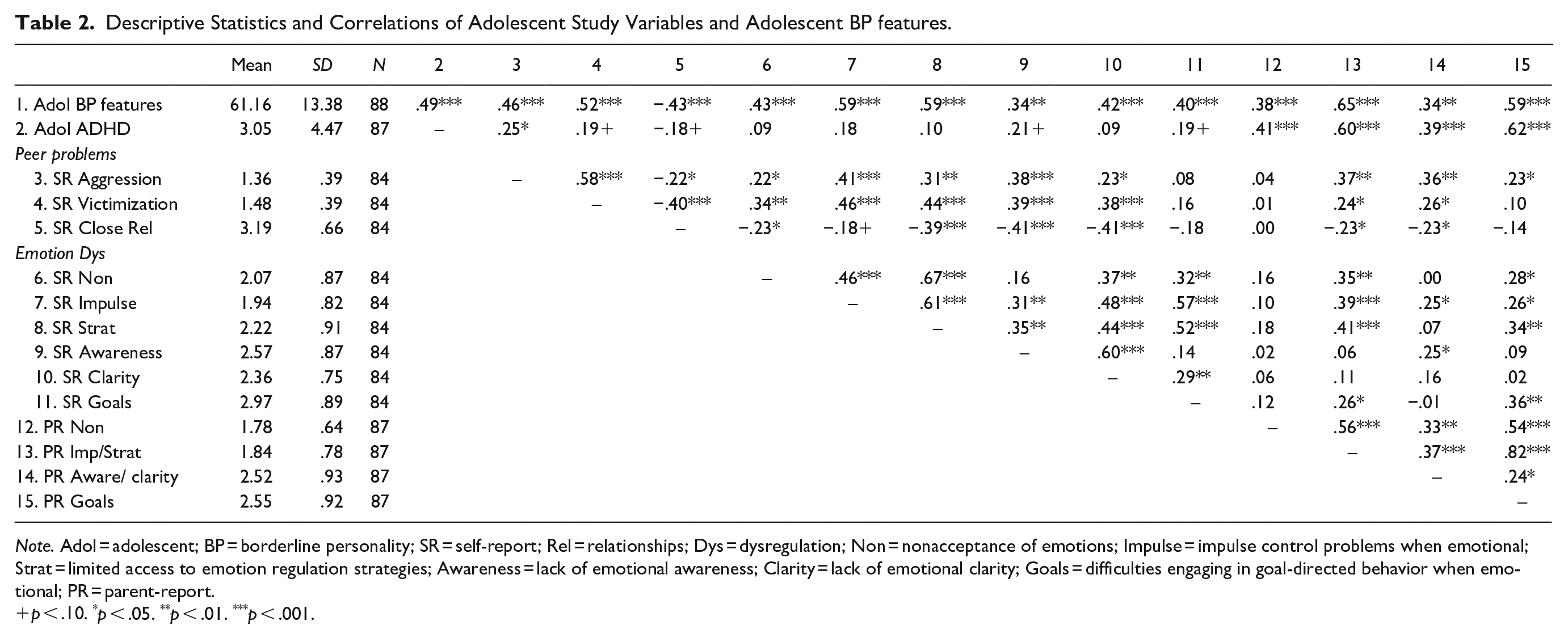
Note. Adol = adolescent; BP = borderline personality; SR = self-report; Rel = relationships; Dys = dysregulation; Non = nonacceptance of emotions; Impulse = impulse control problems when emotional; Strat = limited access to emotion regulation strategies; Awareness = lack of emotional awareness; Clarity = lack of emotional clarity; Goals = difficulties engaging in goal-directed behavior when emotional; PR = parent-report.
p < .10. *p < .05. **p < .01. ***p < .001.
Patterns of missingness
The number of subjects with data available for each variable are reported in Tables 1 and 2. Participants with and without initial teacher data, child emotion dysregulation data, adolescent self-report data, or parent-rated adolescent data did not significantly differ on initial child ADHD symptom levels or any demographic features assessed at the first study visit.
Primary Multivariate Analyses
Childhood longitudinal predictors
As reported in Table 3, when examining child self-reported peer problems as additional predictors, higher ADHD symptoms, but not child-rated peer problems, was a significant predictor. Female sex and younger age were also significant.
Regression Results of Longitudinal Child and Concurrent Adolescent Predictors of Adolescent Borderline Personality Features.
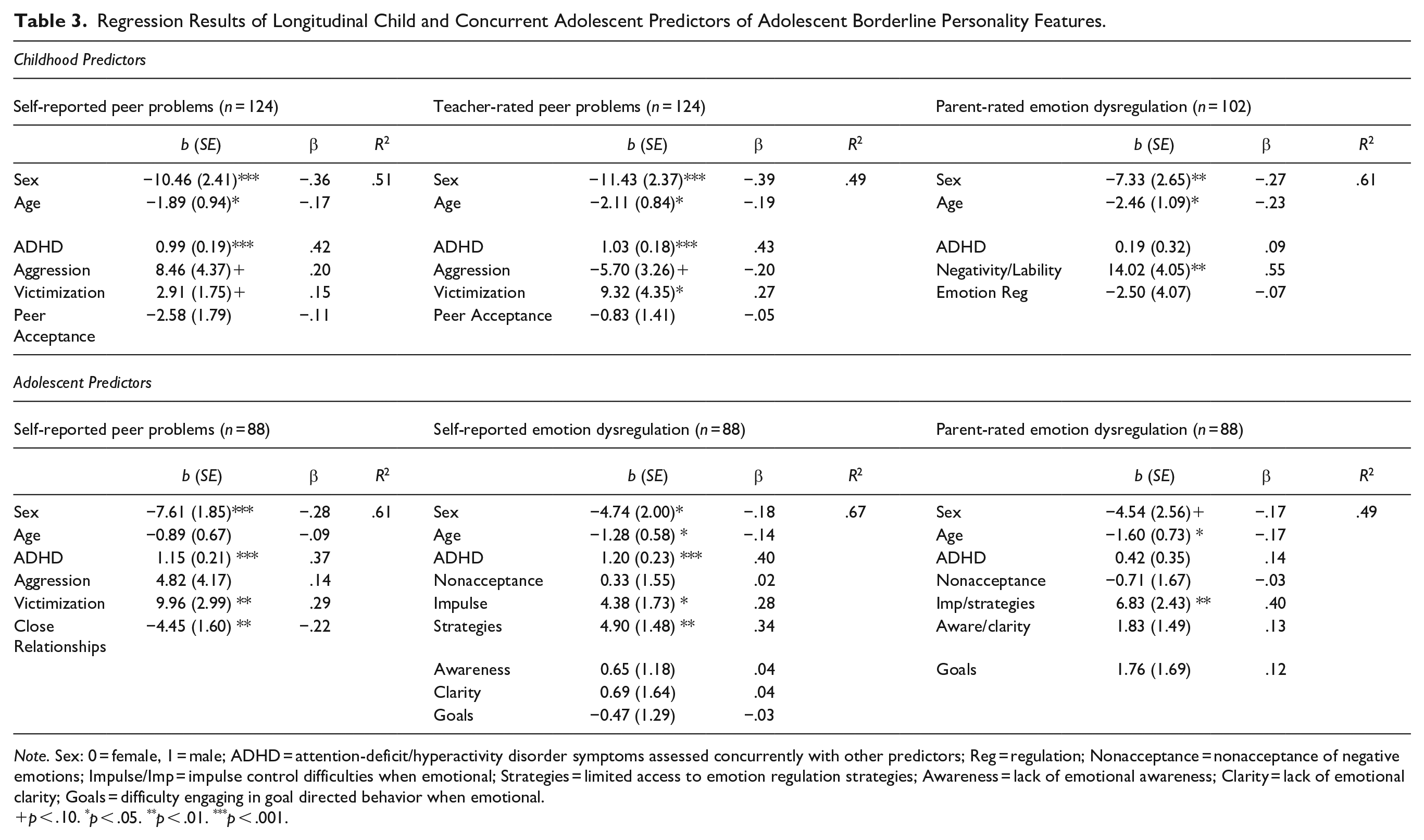
Note. Sex: 0 = female, 1 = male; ADHD = attention-deficit/hyperactivity disorder symptoms assessed concurrently with other predictors; Reg = regulation; Nonacceptance = nonacceptance of negative emotions; Impulse/Imp = impulse control difficulties when emotional; Strategies = limited access to emotion regulation strategies; Awareness = lack of emotional awareness; Clarity = lack of emotional clarity; Goals = difficulty engaging in goal directed behavior when emotional.
p < .10. *p < .05. **p < .01. ***p < .001.
When examining teacher ratings of children’s peer problems as additional predictors, greater ADHD symptoms and greater peer victimization were both unique predictors of BP features, with ADHD symptoms the strongest predictor based on standardized regression coefficients. Teacher-rated aggression and social acceptance were not unique significant predictors. Female sex and younger age covariates were significant (see Table 3).
When examining parent ratings of children’s emotion dysregulation as additional predictors, greater negativity/lability significantly predicted greater adolescent BP features whereas ADHD symptoms and child emotion regulation were not significant. Female sex and younger age also significantly predicted greater BP features (see Table 3).
Adolescent concurrent predictors
As reported in Table 3, when examining adolescent self-reported peer problems as additional predictors, greater adolescent ADHD symptoms, greater self-reported peer victimization, and poorer close friendships each significantly predicted greater adolescent BP features; ADHD symptoms was the strongest predictor based on standardized regression coefficients. Female sex also was a significant predictor whereas adolescent self-reported aggression and age were not significant.
When examining adolescent self-reported emotion dysregulation domains as predictors, greater adolescent ADHD symptoms, greater impulse control problems when emotional, and more limited access to emotion regulation strategies each significantly predicted elevations in BP features; based on standardized regression coefficients, ADHD symptoms was the strongest predictor. The other domains of the adolescent DERS were not significant. Female sex and younger age were significant predictors (see Table 3).
When examining parent report of the adolescent’s emotion dysregulation domains as predictors, the combined DERS subscale of greater impulse control difficulties/limited access to emotion regulation strategies was a significant predictor of greater BP features whereas adolescent ADHD symptoms and the other DERS domains were not significant. Younger adolescent age also was a significant predictor, but youth sex was not (see Table 3).
Follow-Up Tests of Robustness
With the Benjamini- Hochberg procedure (Benjamini & Hochberg, 1995) applied, with a false discovery rate set to 0.05, teacher-rated child peer victimization was no longer a significant predictor of adolescent BP features. In addition, youth age only remained a significant predictor in the model with teacher-rated peer problems as predictors; in all other models age was no longer a significant predictor. All other significant risk factors from the primary multivariate analyses remained significant with the Benjamini-Hochberg procedure applied.
Discussion
Although growing evidence suggests a high co-morbidity between ADHD and BP disorder (Matthies & Philipsen, 2014; Xenaki & Pehlivanidis, 2015), much of what is known about the developmental risk factors for BP disorder comes from typically developing samples in which rates of ADHD and associated impairments are likely to be low. The present study provides an important extension of prior work by examining longitudinal child and concurrent adolescent predictors of BP elevations within a sample that included youth with and without childhood ADHD. Specifically, given that peer problems and emotion dysregulation characterize both adolescent ADHD (Graziano & Garcia, 2016; McQuade, 2020) and BP disorder (Putnam & Silk, 2005; Runions et al., 2021), these vulnerabilities were examined in childhood and adolescence as predictors of adolescent BP features when also considering the independent effect of ADHD symptoms. Unique to this study is the inclusion of multiple-raters, including teacher-ratings of childhood peer problems, which have not been examined as predictors of BP features in ADHD samples. Results suggested that elevated childhood and adolescent ADHD symptoms are associated with vulnerability for adolescent BP features, but that specific peer problems and emotion dysregulation domains, as rated by both adult and self-report, also serve as markers of risk. These findings suggest that in addition to ADHD symptomatology, specific social and emotional vulnerabilities may help identify youth at greatest risk for displaying BP elevations in adolescence.
When examining the unique effects of peer problems on risk for adolescent BP features, ADHD symptoms, assessed in either childhood or concurrently in adolescence, remained a robust predictor of BP elevations. In fact, even when other significant peer factors were identified, ADHD symptoms was the strongest predictor within the model. These results suggest that although peer challenges are common in both ADHD and BP disorder (McQuade, 2020; Runions et al., 2021), peer problems related to poor peer relationships, peer aggression, and peer victimization, do not account for the association between these symptom domains. However, results also indicated that both teacher-reported and adolescent self-reported peer victimization uniquely predicted adolescent BP feature elevations when accounting for the independent effect of ADHD symptoms. The significant effects of peer victimization on BP elevations is consistent with several prior studies using typically developing samples (Kawabata et al., 2014; Winsper et al., 2017; Wolke et al., 2012). Kawabata et al. (2014) propose that physical (e.g., hitting), verbal (e.g., teasing), and relational (e.g., systematic exclusion) forms of victimization may have similar effects as maltreatment by parents (e.g., physical/emotional abuse, neglect), which are theorized to invalidate youth’s emotions, paving the way for instability in identity, relationships, and emotions that are central to BP disorder (e.g., Crowell et al., 2009). In adolescence, trust and intimacy with close friends was also examined as a predictor of BP features and poorer close friendships also independently predicted BP feature elevations. As youth reach adolescence, close friendships typically become more intimate and serve as an important venue for the development of the interpersonal skills needed for healthy adult relationships (Grover & Nangle, 2007). Challenges forming or maintaining healthy close friendships in adolescence may also be an important indicator of the emergence of BP features and may be an early manifestation of relationship instability.
Emotion dysregulation is an additional domain of impairment shared by both ADHD and BP disorder (Graziano & Garcia, 2016; Putnam & Silk, 2005). In the present study, parent-rated negativity and lability in childhood and difficulties with impulse control and accessing emotion regulation strategies when emotional in adolescence uniquely predicted elevations in BP features. In addition, in these analyses, concurrently assessed ADHD symptoms were no longer a significant predictor of adolescent BP features. This may suggest that parent-reported emotion dysregulation serves as a better predictor of BP feature vulnerability than ADHD symptoms. Although the child ERC (Shields & Cicchetti, 1997) and adolescent DERS (Bunford et al., 2020) measures are different, both the ERC negativity/lability subscale and the combined parent DERS impulse control/emotion regulation strategies subscale describe difficulties controlling and recovering from emotions and managing negative emotions (Bunford et al., 2020; Shields & Cicchetti, 1997). These challenges may provide greater specificity into the type of behavioral dysregulation that indicates vulnerability for BP features than overall ADHD symptom levels. There also is some overlap between items on these subscales and ADHD symptoms (e.g., “difficulty controlling his/her behaviors,” Bunford et al., 2020; “Is able to wait for what he/she wants” Shields & Cicchetti, 1997). Thus, it is also possible that parents are referencing the same behaviors when rating both ADHD symptoms and these ERC and DERS subscales, leading to limited unique variance in ADHD symptoms when predicting BP features. It also remains unclear whether emotion dysregulation is a core feature of ADHD (Faraone et al., 2019; Shaw et al., 2014) or is better viewed as transdiagnostic (Beauchaine & Cicchetti, 2019). If emotion dysregulation is indeed a core feature of ADHD, then the present findings may really be identifying multiple aspects of ADHD that are linked to BP features. It will be important for future research to explore whether emotion dysregulation is better viewed as a unique vulnerability for BP features in youth or is better conceptualized as part of an ADHD presentation.
In adolescence, youth also self-reported on their emotion dysregulation using a parallel scale to parent ratings. Interestingly, using adolescent self-report, ADHD symptoms continued to uniquely predict BP features and was the strongest predictor, suggesting that adolescent subjective perception of emotion dysregulation may provide unique predictive information from parent report of ADHD symptoms. However, even with adolescent self-report, the same domains of impulse control challenges when emotional and limited access to emotion regulation strategies emerged as significant predictors of BP feature elevations. These results are also consistent with research using an adolescent inpatient sample, which found that these same self-reported domains of emotion dysregulation uniquely characterized adolescents with a BP diagnosis, relative to adolescents with other psychological disorders, including ADHD (Ibraheim et al., 2017).
When interpreting these results, several limitations must be considered. First, BP features were not measured in childhood and therefore changes in BP features over time could not be assessed. It is possible that BP features first emerged in childhood (e.g., Babinski et al., 2021) and significant childhood predictors may not have preceded the onset of BP features. Relatedly, given the developmental span, different measures were used in childhood and adolescence to assess vulnerabilities, preventing a direct examination of changes in social and emotional problems over time and how those change influenced BP features. To further advance findings, longitudinal research that measures BP features and other vulnerabilities repeatedly across development should be conducted. Second, although inclusion of teacher, parent, and adolescent ratings is a strength, for some variables only one informant was available (e.g., child emotion dysregulation), limiting comparisons across raters. In addition, adult and self-report ratings may be biased and some significant effects may be influenced by shared method variance. Third, the sample was relatively small, with only a subset of participants measured on childhood emotion dysregulation; this may limit the ability to detect smaller magnitude effects, if they existed. In addition, due to the primary aims of the study (McQuade & Breaux, 2017), youth with clinical elevations in ADHD symptoms were not invited to participate in the childhood assessment of emotion dysregulation. Thus, results for childhood emotion dysregulation do not apply to all children with ADHD. Fourth, the sample was primarily white and socioeconomic level was relatively high. Minority status may influence peer treatment (e.g., Xu et al., 2020) and cultural values may influence how youth are socialized to express and manage emotions (e.g., Friedlmeier et al., 2011); thus, results should not be assumed to generalize to all children and additional work in more diverse samples and within specific cultural groups is needed to fully understand vulnerabilities.
Despite these limitations, the study has several strengths, including being the first to examine both social and emotional vulnerabilities as predictors of BP features within a sample that includes youth with ADHD. Inclusion of multiple markers of risk provides greater clarity in the types of impairments that may indicate adolescent BP feature elevations, even for youth with ADHD. In addition, the use of multiple reporters and both child and adolescent time points provides an opportunity to compare results across raters and over time. Self and adult-reports of peer and emotional challenges are likely to provide distinct information about experiences and functioning and there are important developmental differences in these domains between childhood and adolescence. Remarkably, the pattern of results was relatively consistent across raters and time, with peer victimization and emotion dysregulation related emotional control and management of negative emotions emerging as two important markers of risk for BP features.
Results of this study also have important clinical implications. Given the strong effects of ADHD symptoms on later BP features, research should extend on clinical case reports (e.g., Babinski et al., 2018) with randomized controlled trials that investigate whether evidence-based treatments for ADHD mitigate risk for the development of later BP disorder. Integration of modules from dialectical behavior therapy (e.g., interpersonal effectiveness; emotion regulation) have also shown promise in treating adults with ADHD (e.g., Fleming et al., 2015), but their utility for youth with ADHD remains unclear. Addressing peer victimization and close friendship challenges, regardless of ADHD diagnosis, may also be important in reducing risk for BP feature elevations. However, more work is needed to identify highly effective peer treatments, particularly for youth with ADHD (McQuade, 2020). Finally, results suggest that prevention and intervention efforts may want to target emotion dysregulation challenges related to emotional control and management of negative emotions. Emerging work suggests that in both typically developing and ADHD samples, parents can be trained to more effectively support their child’s development of emotion regulation skills (e.g., Breaux & Langberg, 2020; Havighurst et al., 2013), which may have potential downstream effects on risk for BP features. Unfortunately, to date, there is very limited research examining how to best prevent the emergence of BP features, especially for youth with ADHD. The present findings underscore potential vulnerabilities that may need to be targeted in childhood or adolescence in order to prevent BP disorder and the high social and personal burdens that accompany it (van Asselt et al., 2007).
Supplemental Material
sj-docx-1-jad-10.1177_10870547221098174 – Supplemental material for ADHD Symptoms, Peer Problems, and Emotion Dysregulation as Longitudinal and Concurrent Predictors of Adolescent Borderline Personality Features
Supplemental material, sj-docx-1-jad-10.1177_10870547221098174 for ADHD Symptoms, Peer Problems, and Emotion Dysregulation as Longitudinal and Concurrent Predictors of Adolescent Borderline Personality Features by Julia D. McQuade in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by internal start-up funds from Amherst College, awarded to the author.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.