
Abstract
Objectives:
We sought to examine rates of comorbid ADHD and SUD/AUD using a nationally representative dataset, and to compare this data with established estimates. We hoped to increase available research on ADHD within patients with SUD/AUD.
Methods:
This study is a retrospective secondary analysis of cross-sectional data collected in the National Hospital Ambulatory Medical Care Survey (NHAMCS).
Results:
The data showed less than 1% of comorbid ADHD in either AUD or SUD, and prevalence of 0.6% in patients with both. Our estimated prevalence of ADHD among SUD/AUD patients is more than 30-fold smaller than the 25% consensus.
Conclusion:
The stark difference between our data and prior research indicates a need for further examination of the prevalence of ADHD within acute care. This finding of a large reservoir of ADHD that is unrecognized or undocumented indicates a substantive need for ADHD-focused education with opportunity for improvement in patient treatment.
Introduction
Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder estimated to affect 3% of the adult population, and is common among patients with addictive disorders (Faraone et al., 2015). Alcohol use disorder (AUD) and substance use disorder (SUD) are two addictive processes that have been shown to have a strong association with ADHD, with approximately 25% of patients with SUD or AUD having ADHD, and treatment of AUD or SUD is often unsuccessful if underlying ADHD is not treated (Crunelle et al., 2018). Due to the impact of ADHD on successful treatment of SUD/AUD, it is important that prior diagnoses of ADHD appear in the patient’s medical record.
In recent years, the emergency department (ED) has increasingly become a site of care for both SUD and AUD (Suen et al., 2021). This increase is potentially due to a lack of substance use disorder treatment in primary care offices (Wakeman et al., 2019). ED-initiated treatment for SUD has been shown to be beneficial, and it is important that patients are asked about any existing ADHD diagnoses (D’Onofrio et al., 2015). We sought to examine the national prevalence of comorbid ADHD and SUD/AUD in the ED setting and to compare this with established estimates. We hypothesized that comorbid ADHD may be underrecognized in the emergency department.
Methods
This study is a retrospective analysis of the National Hospital Ambulatory Medical Care Survey (NHAMCS), a national probability sample of ambulatory visits made to acute care hospitals in the U.S. sponsored by the Census Bureau and conducted by the National Center for Health Statistics (NCHS) (McCaig & Burt, 2012). We used the NHAMCS identifications of AUD and SUD abstracted from patient records by trained Census Bureau representatives to identify cases including these diagnoses and significant substance use (Center for Health Statistics, 2014). We then used ICD codes (314 and F90) entered by providers to identify cases of ADHD. Using the provided sampling weights, we estimated the number of ED visits between 2014 and 2019 by patients 18 years or older with SUD or AUD, as well as the frequency of comorbid ADHD. Our study was exempted by the Colorado Multiple Institutional Review Board (COMIRB).
Results
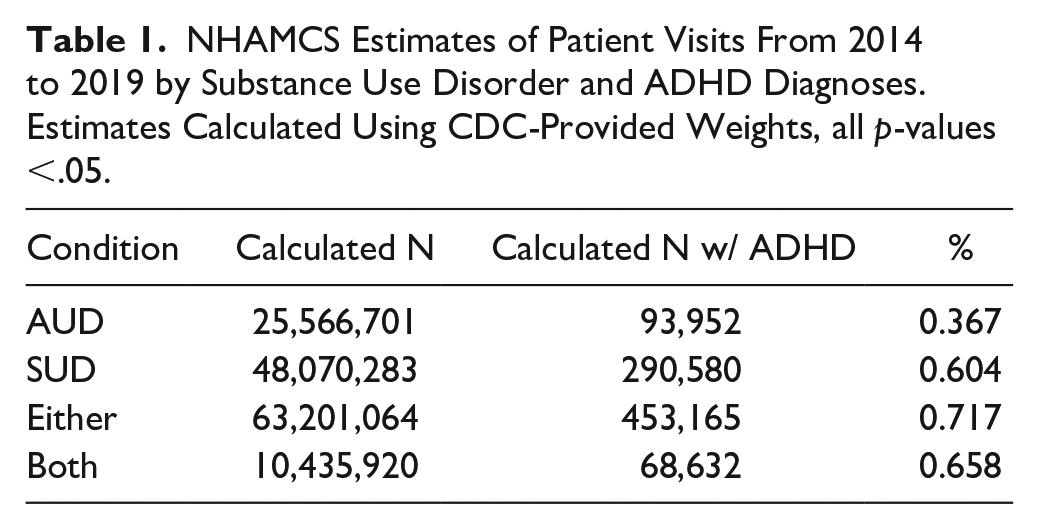
We analyzed a total of 93,382 adult patient records in NHAMCS, representing 649.3 million ED visits (95% CI: 594.0–704.6). Patients with SUD accounted for 48.1 million (95% CI: 39.2–56.9); AUD accounted for 25.6 million, (95% CI: 23.1–28.1); Comorbid SUD and AUD accounted for 10.4 million visits (95% CI: 9.2–11.7). ADHD diagnoses were comorbid in fewer than 1% of SUD/AUD visits (Table 1).
NHAMCS Estimates of Patient Visits From 2014 to 2019 by Substance Use Disorder and ADHD Diagnoses. Estimates Calculated Using CDC-Provided Weights, all p-values <.05.
Discussion
The data showed a rate of less than 1% of comorbid ADHD among patients with either AUD or SUD, and 0.6% in patients with both AUD and SUD, a more than 30-fold decrease from the 25% consensus (Crunelle et al., 2018). This discrepancy may be explained by under-recognition of ADHD and its relationship to addiction, as the difference is specific to ADHD: a similar study found depression rates among NHAMCS SUD/AUD patients were consistent with prior estimates (Suen et al., 2021). Depression is widely acknowledged as a contributing factor for SUD/AUD (Suen et al., 2021); therefore, ED providers are likely primed to recognize symptoms, and may inquire about a patient’s previous diagnoses. ED providers unaware of the link between ADHD and addictive disorders could overlook ADHD symptoms, not ask about previous ADHD diagnosis, or neglect to document an existing diagnosis in the ED visit record. ADHD is difficult to diagnose in the ED, so ED providers should not be expected to accurately identify individuals without prior formal diagnoses (Pittsenbarger et al., 2008). Instead, the discrepancy between estimates and our found rate of ADHD suggests that existing diagnoses are not being documented in the ED record.
It is critically important that ED providers are attentive to prior ADHD diagnoses, as ED providers have significant impacts on a patient’s trajectory within the healthcare system (de Brauwer et al., 2021). In the context of SUD/AUD, they may refer patients to social work, consult addiction services, or request mental health evaluation, all of which can affect patient outcomes (de Brauwer et al., 2021). Additionally, ED-initiated pharmacotherapy could be altered in patients with ADHD; buprenorphine has been associated with increased ADHD symptoms compared to other opioid treatments, and atomoxetine is a low-risk medication that has been shown to reduce ADHD symptoms and drinking in patients with comorbid ADHD and AUD (Perugi et al., 2019). If a treatment plan is made without knowledge of a patient’s ADHD status, clinicians may affect a patient’s likelihood of remission. An increased wariness of ADHD could augment providers’ discernment for the best course of action and improve outcomes.
One limitation to our study is that NHAMCS data lacks detail about why a patient was diagnosed with SUD/AUD, nor does it separate SUD into subcategories such as opioid use disorder or tobacco use disorder. As the utilization of emergency departments for AUD and SUD increases, it is important that underlying conditions are considered. Our finding of a large reservoir of ADHD that may be unrecognized or undocumented by providers indicates a need for provider education with opportunity for large improvement in patient treatment.
Footnotes
Author Contributions
EWH had full access to all the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis. Concept, design, and initial draft: EWH. Critical revision, administrative support, supervision: TC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.