
Abstract
Background:
Adolescent-specific ADHD self-report screening measures can greatly increase the likelihood of correct diagnosis and timely treatment of ADHD in adolescents. This study provides preliminary evidence for evaluating the reliability and validity of the Adult ADHD Self-Report Scale-Revised (ASRS-R) in a school-based sample of Chinese adolescents.
Methods:
The ASRS-R and the Strengths and Difficulties Questionnaire (SDQ) were administered to 867 adolescents aged 12 to 16 years (Mage = 13.08 years). Construct validity was assessed using correlation analysis of the ASRS-R with the SDQ. Moreover, confirmatory factor analysis (CFA), internal consistency, retest reliability, and measurement invariance of the scales were examined by gender.
Results:
CFA showed a two-dimensional factor structure of the ASRS-R, and the model fitted the data well (χ2/df = 4.370, RMSEA = 0.062, TLI = 0.932, CFI = 0.940, GFI = 0.927, AGFI = 0.907, and SRMR = 0.038). The ASRS-R scale was invariant across gender and had satisfactory internal consistency (Cronbach’s alpha = .934) and test-retest reliability (intraclass correlation coefficient = .874). The construct validity, as calculated using the SDQ, was also acceptable.
Conclusion:
The ASRS-R can be a psychometrically reliable self-report instrument and provide preliminary support as a simple tool for identifying ADHD symptoms in Chinese adolescents. The findings provide evidence for extending the application of the ASRS, previously limited to adults, to the adolescent populations.
ADHD, a neurodevelopmental disorder that typically emerges in childhood, is characterized by higher than normal levels of inattention, hyperactivity, and impulsivity (American Psychiatric Association, 2013). Recent studies have reported a high prevalence of ADHD, with the incidence rate of 6.4% among adolescents in China and 7.2% incidence rate in adolescents worldwide (Li et al., 2022; Wolraich et al., 2019). ADHD has been recognized as a condition that persists throughout life, with approximately 70% individuals experiencing symptoms during adolescence and 30% to 50% continuing to exhibit symptoms into adulthood (Polanczyk et al., 2007). If left untreated, ADHD leads to multiple negative outcomes, such as academic underachievement, impaired social interaction, difficulty with emotional control, poor physical condition, and an increased risk of suicidal ideation and self-injurious behaviors (American Psychiatric Association, 2013; Austgulen et al., 2023; Galera et al., 2023; Ingeborgrud et al., 2023; Lawrence et al., 2021; Zendarski et al., 2021). Therefore, early identification and treatment are critical to the prognosis of ADHD in adolescents. Monitoring ADHD symptoms in adolescents can be challenging. One of the reasons for this is that the symptoms of hyperactivity/impulsivity tend to decrease with age, while attention deficit behaviors become more pronounced, which complicates the successful diagnosis of ADHD (Wolraich et al., 2005). In girls, attention deficit and internalization problems may be more pronounced than hyperactivity and impulsivity; thus, their symptoms may go unnoticed by teachers and other information providers (Hinshaw et al., 2022). Moreover, clinicians or researchers do not pay much attention to diagnosing girls with attention deficit because they tend to not cause problems as adults. The second reason for the diagnosis of ADHD in adolescents being challenging is the occurrence of multiple mental illnesses (Sultan et al., 2021).
Diagnosing ADHD requires a comprehensive and systematic assessment of an individual’s symptoms, medical history, interpersonal relationships, and family history of psychiatric disorders (Sibley, 2021). Screening for ADHD symptoms is crucial and should be a part of a routine mental health assessment (Brahmbhatt et al., 2016). Self-report scales are a time- and cost-effective method for collecting information about ADHD-related symptoms, diagnosing ADHD in adolescents, and determining its severity. However, use of self-report measures for assessing ADHD symptoms is associated with some challenges. First, self-reports are based on an individual’s subjective perceptions of their behaviors, feelings, and thought patterns and are susceptible to self-manipulation (Lovett & Harrison, 2021). Specifically, self-reporting is problematic in a population exhibiting poor self-awareness and self-monitoring, which are highly representative of ADHD. Adults with ADHD tend to underreport or exaggerate their symptoms when self-reporting (Asherson et al., 2016; Nelson & Lovett, 2019). Second, symptomatic manifestations of ADHD can vary over time and across different contexts, and a single assessment at one point in time may not be sufficient to make a diagnosis (Lewczuk et al., 2024). Lastly, lay people may have difficulty distinguishing ADHD symptoms from other health conditions (e.g., anxiety and depression), which can lead to erroneous self-reporting (Sibley et al., 2018). Therefore, the use of self-reporting measures of ADHD alone (excluding observer-report measures, clinician assessments, etc.) is not a recommended clinical ADHD assessment method. While there are some limitations to using self-reporting measures for ADHD assessment, the availability of such measures can considerably increase the likelihood of correct diagnosis of ADHD in adolescents and adults, thereby interfering with on-time treatment. To ensure usefulness of these self-report scales in clinical practice, they must be psychometrically sound and applicable to equivalent clinical populations.
The 18-item Adult ADHD Self-Report Scale (ASRS) is a self-report measure used for identifying symptoms of ADHD (Kessler et al., 2005). In this method, respondents need to report the frequency with which they have exhibited nine attention deficit behaviors and nine symptoms of hyperactivity in the preceding 6 months. The ASRS was originally developed for assessing ADHD symptoms in adults, but it is now increasingly being used in adolescents as well (Green et al., 2019; Olofsdotter et al., 2023; Somma et al., 2019, 2021; Sonnby et al., 2015). The advantage of using the ASRS with adolescents is that it is publicly available, brief, and has been translated into multiple languages. Several studies have demonstrated stronger validity of the ASRS in adolescent clinical populations compared with interviews conducted by clinicians. Somma et al. (2019) applied the ASRS to the adolescent population in Italian communities and found that it exhibits good psychometric properties, confirming its ability to effectively discriminate between adolescents who have received a MINI ADHD diagnosis and those who have not. Sonnby et al. (2015) tested the ASRS on 134 Swedish adolescent psychiatric outpatients aged 12 to 17 years. The ASRS exhibited good internal consistency (Cronbach’s alpha = .92) and a strong correlation with the Kiddle Schedule of Affective Disorders and Schizophrenia (Ambrosini, 2000) ADHD severity scale administered by clinicians (r = .60). Cross-cultural findings suggest the existence of cultural differences in the perception of ADHD and ADHD-like symptoms (Song et al., 2021). The expectations and standards for attention, hyperactivity, and behavioral control differ across cultures. For example, recognizing ADHD symptoms in Brazil may be challenging due to the high level of tolerance of ADHD-like behaviors in the region (Sugaya et al., 2022). In some cultures, hyperactivity may be viewed as a sign of vibrancy or creativity, whereas in others, the same behavior may be considered problematic. Considering linguistics is also integral to the evaluation of ADHD symptoms. The language of the assessment tool must be appropriate to the level of the individual being evaluated. The ASRS is designed to collect information about ADHD symptoms in the context of adulthood, rather than adolescence. Hence, wording of the questions in the ASRS is less likely to be understood by adolescents; for example, words such as “project” and “work.” Ensuring the accuracy and cultural appropriateness of the phrasing and translation is also crucial to avoid misunderstandings caused by literal translations. For example, the term “social situation” in ASRS is not commonly used for Chinese adolescents; using it directly may cause misunderstandings and reduce the reliability of the results. The psychometric properties of the ASRS have, however, not been reported in a sample of Chinese adolescents.
In this study, we revised the ASRS to make it suitable in the context of Chinese adolescents and validated it. Additionally, we evaluated the reliability, factor structure, preliminary validity, and measurement invariance of the ASRS in a school-based sample of Chinese adolescents by gender.
Methods
Participants and Settings
To improve mental health support for students, anonymous assessments of mental health were conducted in two schools in a city in China, as part of city-wide efforts. Parents were provided a description of the assessment via a letter. All students in grades 7 to 9 were invited to participate. Students with Chinese as the first language were selected to avoid cultural and lexical biases in questionnaire responses. All participants completed the online survey during a regular school day. Written informed consent was obtained from the students and parents before the questionnaire was administered. Middle school students in grades 7 to 9 (aged 12–16 years) were included and administered the ASRS-R and SDQ. Of the 933 students who were eligible and invited to participate, 867 (93.0% of those eligible) provided complete data. The data from these participants were used for further analyses. Four weeks later, 132 adolescents from this group were randomly selected to complete the ASRS-R again, finally obtaining 120 valid questionnaires (90.9%).
Procedure
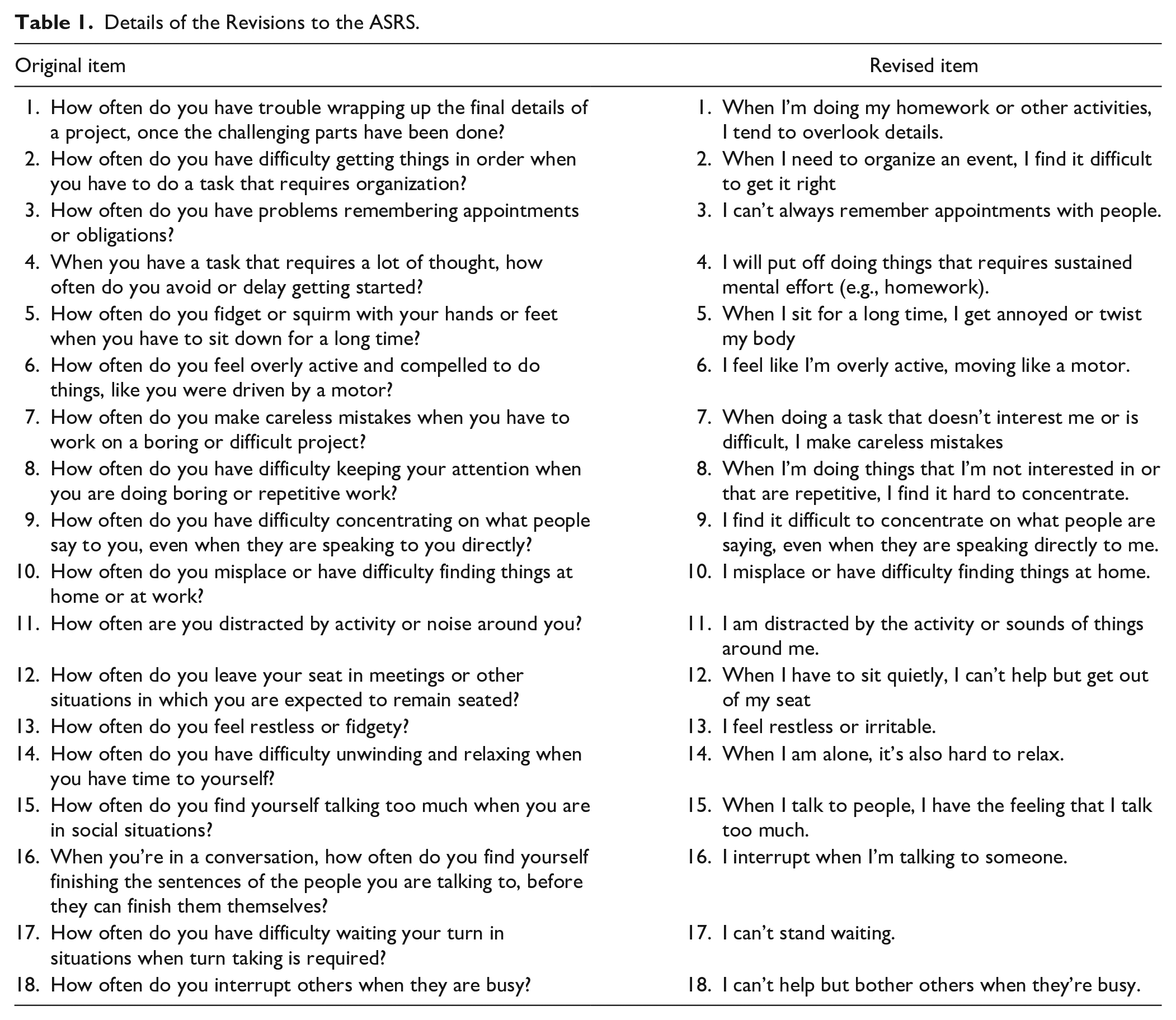
The original English version of the ASRS scale was independently translated into Mandarin by two graduate students who are bilingual, that is, native Chinese speakers as well as fluent in English. Because the ASRS was originally designed for adults, a group of four clinicians and researchers with extensive experience in studying and treating children and adolescents with neurodevelopmental disorders revised the items, ensuring that the content aligns within the context of this population. The main modifications were as follows: (1) because the target audience was teenagers, “project” and “work” were changed to “homework” and “somethings,” respectively. (2) We replaced “you” with “I” and changed the phrasing from questions to declarative sentences, increasing the subjectivity of the questionnaire or assessment tool and allowing the respondents to reflect more directly and naturally on their feelings, experiences, or symptoms. (3) In item 15, “when you are in social situations” was reworded to “when I talk to people.” Details of the revisions are listed in Table 1. The revisions were done by a team of two postgraduate nursing students, one health psychologist, and one expert in clinical neurodevelopmental disorders. The revised measure was named the ASRS-R. Before the questionnaire was administered, the comprehensibility of the adapted items was tested on 10 randomly selected adolescents. All participants reported that they were able to understand the questions.
Details of the Revisions to the ASRS.
Measures
Adult ADHD Self-Report Scale-Revised (ASRS-R)
The Adult ADHD Self-Report Scale-18 item version (ASRS-18; Kessler et al., 2005) comprises 18 items that are explicitly designed to assess ADHD symptoms in adults based on the DSM-IV criteria. The ASRS encompasses two parts: Part A includes 6 items that are considered the best predictors of ADHD, while the remaining 12 items constitute Part B. Consistent with other existing translations of the revised version ASRS-18, the scale was translated into Chinese by using the standard WHO translation and back-translation protocols (Yeh et al., 2008). In the ASRS-18, participants’ behavior over the past 6 months is assessed using a 5-point Likert scale, ranging from 0 (never) to 4 (very often), and the scale is divided into two subscales: inattention (INA) and hyperactivity/impulsivity (HI), each consisting of nine items. In the present study, the value of Cronbach’s alpha was .934.
Strengths and Difficulties Questionnaire (SDQ)
The SDQ comprises 25 items and is used to measure students’ strengths and challenges related to psychosocial adjustment, including psychological symptoms and social behaviors (Goodman, 2001). The version of the SDQ used in this study was the youth self-report. It comprises five dimensions: emotional problems, conduct problems, hyperactivity/inattention, peer interaction problems, and prosocial behaviors. The scores of the first four dimensions constitute the total score of adaptation difficulties. Each item was rated on a 3-point Likert scale, ranging from 0 (strongly disagree) to 2 (strongly agree). In this study, the Cronbach’s alpha value was .717.
Data Analysis
Data analysis was performed using SPSS version 25.0 and AMOS version 28.0. Continuous data are expressed as the mean (SD), and categorical data are expressed as percentages. Statistical significance was set at p < .05. The relationships between the variables are expressed using the Pearson’s correlation coefficient.
In the present study, the absolute and incremental goodness of fit indices used in the CFA were as follows: (1) the chi-square value to degree of freedom ratio (χ2/df) of <5 indicated that the model is acceptable; (2) root mean square error of approximation (RMSEA) with 0.08 as cutoff indicated a poor model fit; (3) comparative fit index (CFI) with ≥0.90 indicated a good fit; (4) Tucker Lewis Index (TLI) with ≥0.90 indicated a good fit; (5) the standardized root mean square residual (SRMR) with <0.08 indicated a good fit; (6) goodness of fit index (GFI) with ≥0.9 indicated a good fit; and (7) adjusted goodness of fit index (AGFI) with ≥0.9 indicated a good fit (Hooper et al., 2008).
Thereafter, construct validity of the ASRS-R was evaluated through Pearson’s bivariate correlations with hyperactivity/inattention, as assessed using SDQ-related dimensions. Associations among the variables were assessed in terms of the significance and effect size. According to the recommended guidelines (Cohen, 1988), values of .1, .3, and .5 were considered to denote small, medium, and large effect sizes, respectively.
The sample was analyzed for measurement invariance (MI) by gender, with configural, metric, and scalar models tested in turn. For configural invariance, factor loadings and intercepts were freely estimated in each group. Factor loadings were assumed to be equal in the measurement of metric invariance, while the intercepts were freely calculated. To assess the scalar invariance, factor loadings and intercepts were set to their fixed values. Differences in model fit indices (i.e., ∆CFI, ∆TLI, ∆RMSEA, and ∆SRMR) were compared for assessing MI. The differences of ∆CFI < 0.01, ∆TLI < 0.01, ∆RMSEA ≤ 0.15, and ∆SRMR < 0.01 were considered to satisfy the criteria for acceptability (Chen, 2007; Cheung & Rensvold, 1999, 2002).
Typically, to ascertain the overall homogeneity of the scale, the corrected coefficients of the correlations between the total ASRS-R score and each item were computed. A scale is considered to have good homogeneity if the corrected correlation coefficient between a single item and total scores is ≥.40 and reaches a significant level (Yang et al., 2021).
To determine the reliability of the ASRS-R, the internal consistency reliability of the scale was evaluated in terms of Cronbach’s alpha. Cronbach’s alpha values of .70 to .79 are considered allowable, those between .80 and .89 are good, and values ≥.90 are excellent (Barker et al., 1994). Retest reliability reflects the stability of the scale determined by calculating the intraclass correlation coefficient (ICC). The ICC ≥ .75 indicates a good level of stability (Cicchetti, 1994).
Results
Characteristics of the Participants
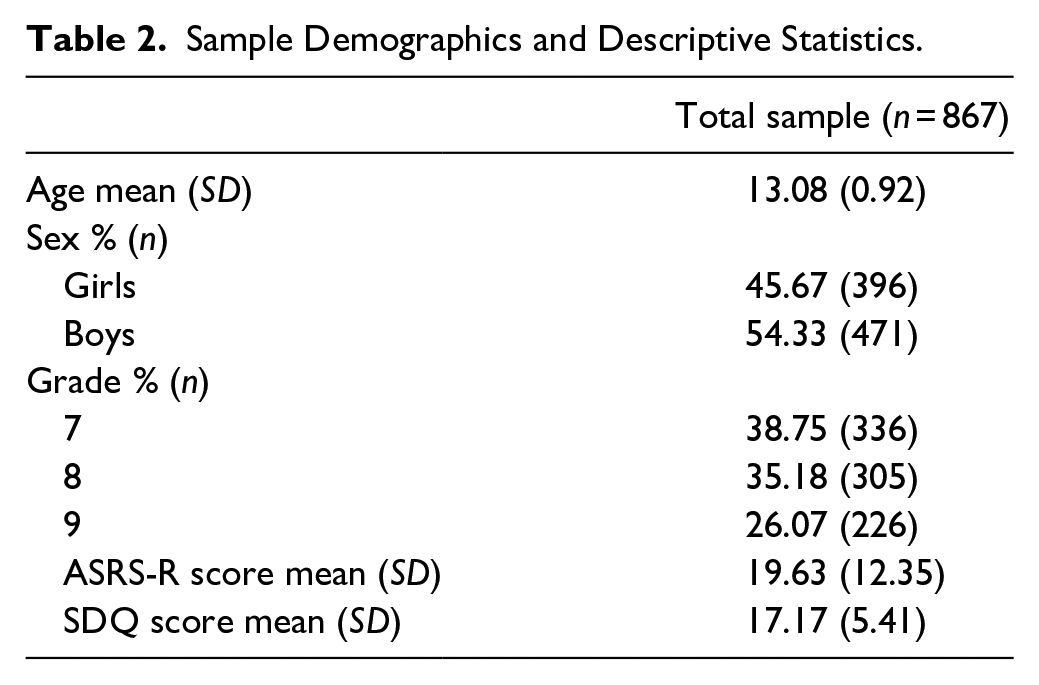
A total of 867 questionnaires were collected. The mean age for all participants was 13.08 years (SD = 0.92; age range = 12–16 years), and 54.33% (n = 471) of the participants were boys. The average scores of ASRS-R and SDQ were 19.63 ± 12.35 and 17.17 ± 5.41, respectively. Table 2 presents the participants’ characteristics in detail.
Sample Demographics and Descriptive Statistics.
Item Analysis
All corrected coefficients of correlation between the total score and each item ranged between .498 and .750. Item total correlations and corrected item total correlations were >.40, which indicated good quality of all items of the ASRS-R. Thus, no item was eliminated at this step.
Confirmatory Factor Analysis
The CFA results indicated excellent fit indices, and the two-factor CFA model fitted the data well (χ2 = 585.593, df = 134, χ2/df = 4.370, RMSEA = 0.062, TLI = 0.932, CFI = 0.940, GFI = 0.927, AGFI = 0.907, and SRMR = 0.038). Regarding the factor loadings in CFA, each factor comprised nine items, similar to the original solution. The range of the standardized factor loadings for each factor was as follows: 0.560 to 0.803 for inattention and 0.532 to 0.776 for hyperactivity/impulsivity. Figure 1 shows the results of CFA.
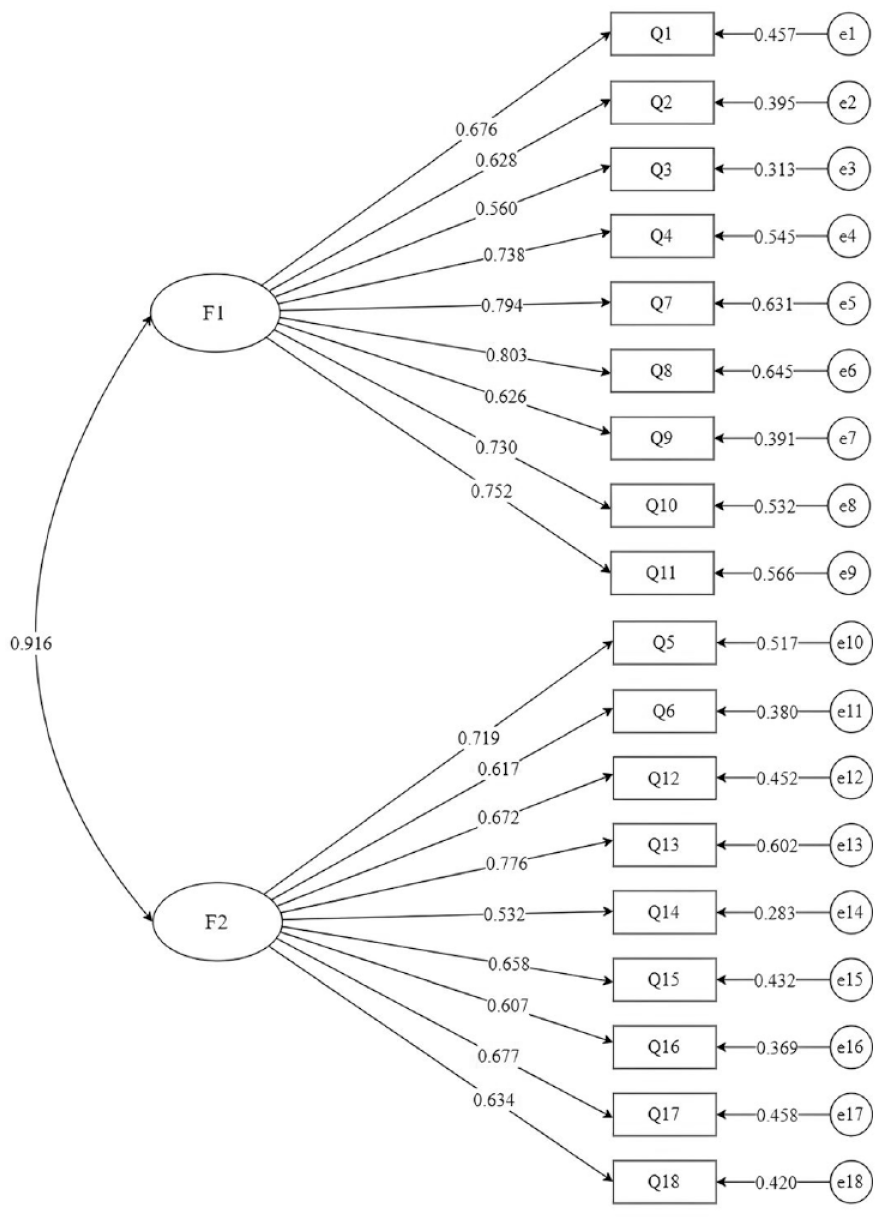
The confirmatory factor model of the ASRS-R. F1 (inattention, nine items) and F2 (hyperactivity/impulsivity, nine items).
Construct Validity
A correlation was noted with a medium-to-large effect size between the ASRS-R factor score, total score, and the SDQ-related dimensions (Table 3). The ASRS-R scores were more significantly associated with the SDQ subscale measuring hyperactivity/inattention (r = .693, p < .001) and emotional problems (r = .652, p < .001) than with the other subscales measuring conduct problems (r = .538, p < .001), peer interaction problems (r = .256, p < .001), and prosocial behaviors (r = −.306, p < .001); this pattern roughly held at factor level.
Correlations Between ASRS-R Factor Score, Total Score, and SDQ-related Dimensions.
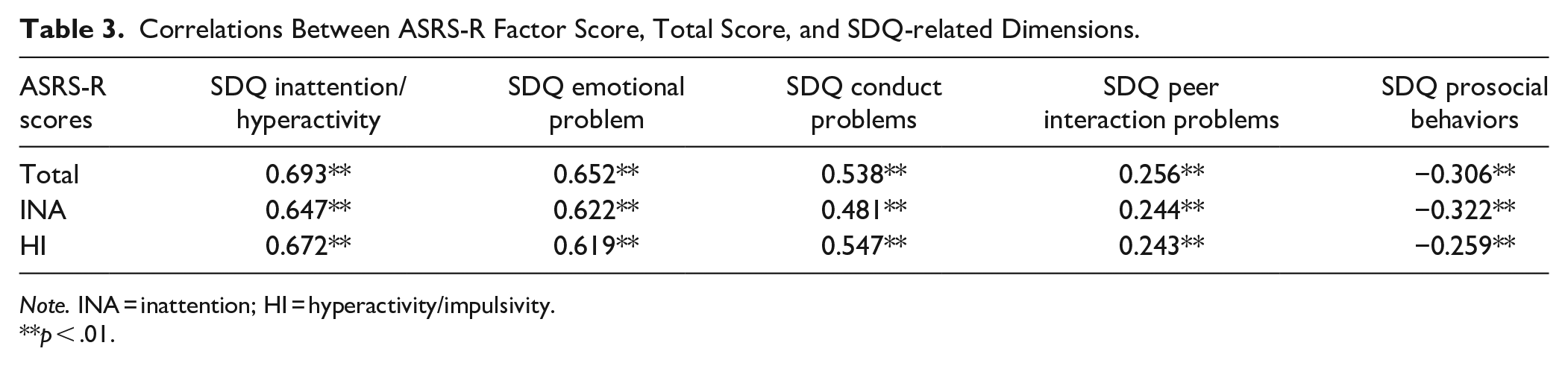
Note. INA = inattention; HI = hyperactivity/impulsivity.
p < .01.
Measurement Invariance
Gender invariants were tested according to the bifactors model, and the results showed that the MI was consistent between the gender groups (Table 4).
Measurement Invariance Across Gender (n = 867).

p < .001.
Fit indices (χ2 = 822.444, df = 266, CFI = 0.926, TLI = 0.915, RMSEA = 0.069, and SRMR = 0.042) for the configural invariance model showed a good fit. Further, the metric invariance model was evaluated, which indicated that the fit of the metric model was similar to that of the configural model (χ2 = 837.751, df = 283, CFI = 0.926, TLI = 0.920, RMSEA = 0.067, and SRMR = 0.044). Next, we evaluated the scalar invariance, and the results of the scalar model also met satisfactory fit indices (χ2 = 928.367, df = 299, CFI = 0.919, TLI = 0.914, RMSEA = 0.070, and SRMR = 0.048). Differences in the fit indices between the configural and metric models were as follows: ∆CFI = 0.000, ∆TLI = −0.005, ∆RMSEA = 0.002, and ∆SRMR = −0.002. Similarly, differences in the fit indices between the metric model and the scalar model were as follows: ∆CFI = 0.007, ∆TLI = 0.001, ∆RMSEA = −0.001, and ∆SRMR = −0.006. The MI values of the ASRS-R were determined in both the male and female groups.
Reliability
The general ASRS-R demonstrated good internal consistency in the sample (Cronbach’s alpha = .934). The inattention and hyperactivity/impulsivity subscales showed good reliability (Cronbach’s alpha values = .897 and .871, respectively). To evaluate test-retest reliability, we invited 120 students to complete the ASRS-R again after a 4-week interval. The ICC was 0.874 (p < .001), indicating satisfactory test-retest reliability.
Discussion
This study examined the psychometric properties of the ASRS-R by examining its reliability, validity, item analysis, and MI in a sample of Chinese adolescents. Consistent with the previously reported results, the ASRS-R demonstrated good psychometric properties in our sample, displaying high reliability and validity (Green et al., 2019; Somma et al., 2021; Sonnby et al., 2015). In addition, significant gender invariant was noted.
The CFA results showed that all fitness indicators of the ASRS-R model were within the acceptable range, suggesting that the factor structure of the ASRS-R in Chinese adolescents is an appropriate bifactor structure similar to the original ASRS, which is consistent with the model reported by Somma et al. (2019) in a community sample of adolescents. For the two dimensions, internal consistency was measured in terms of Cronbach’s alpha value. The reliability estimates for the above dimensions were >.70 on the ASRS-R, which highlighted good internal consistency of the two dimensions. These coefficients were comparable to those in other assessments of ADHD-related symptoms based on parent- and teacher-reports, such as the Chinese version of the Conners Parent Symptom Questionnaire (PSQ) and the Conners Teacher Rating Scale, with Cronbach’s alpha values of .932 and .934, respectively (L. Y. Su, Li, et al., 2001; L. Y. Su, Xie, et al., 2001). However, the coefficients were found to be higher than the Cronbach’s alpha value reported for the Chinese ADHD RS-IV in students aged 6 to 17 years (Y. E. Su et al., 2015) but slightly lower than that reported in children aged 6 to 16 years using the parent-reported SNAP-IV rating scale-parent form (J. B. Zhou et al., 2013). In this study, the ASRS-R also showed high test-retest reliability, demonstrating that the measurement of the ASRS-R was robust and reliable over time.
Further, this study measured gender invariance of the ASRS-R in Chinese adolescents. The CFA showed that the two-factor structure of the ASRS-R was suitable for both boys and girls, demonstrating the stability of the two-dimensional structure of the ASRS-R. In line with the findings of previous studies, the observation of the invariance of the ASRS-R was established for both genders (Green et al., 2019; Morin et al., 2016).
Subsequently, we used the SDQ to evaluate construct validity. In a study, Xiong et al. (2019) found that children with ADHD scored significantly higher than typically developing children on the hyperactivity/inattention subscale of the SDQ. Some studies have also used the SDQ as an indicator of probable ADHD (Man et al., 2023; S. Y. Zhou et al., 2012). Accordingly, we chose the SDQ to test the construct validity. The total and subscale scores of the ASRS-R were found to be more strongly correlated with scores on the hyperactivity/inattention and emotional problem subscales of the SDQ than with scores on the other subscales. This finding is consistent, to some extent, with those reported by Green et al. (2019), who observed weak associations of the ASRS with other emotional and behavioral health subscales but significantly stronger associations with the hyperactive/inattention subscale. These results provide preliminary support for the construct validity of the ASRS-R compared to the SDQ, suggesting that the ASRS-R may be an effective tool for screening potential ADHD in adolescents. To fully assess the validity of the ASRS-R, additional studies using diagnostic gold standards are required.
Of note, the ASRS-R does not identify emotional dysregulation, which is generally considered integral to ADHD symptoms (Shaw et al., 2014). This is supported by the finding that the degree of correlation between the ASRS-R and hyperactivity/attention is similar to that of the correlation with emotional problems, as shown by the results of the construct validity of the ASRS-R and assessed using the SDQ. Emotional dysregulation is one of the most important clinical manifestations of ADHD, and it may not be detected using only the ASRS-R; therefore, other methods of emotional dysregulation assessment should be integrated to more accurately evaluate ADHD symptoms.
The ASRS-R is intended as a screening tool, rather than a confirmatory diagnosis, to identify adolescents who are likely to having ADHD symptoms, enabling more detailed and reliable assessments. In this study, the ASRS-R was used to screen ADHD symptoms only in a sample of adolescents; however, the scale is also essential for the diagnosis and treatment of adolescents with ADHD. Overall, our data extends previous findings, highlighting the significance of the ASRS-R as a potential screening instrument for diagnosing ADHD in adolescents.
Limitations
Some limitations of this study must be acknowledged. First, the study relied on the SDQ to test the construct validity of the instrument. In this study, the ASRS-R and the SDQ were reported by the same person; thus, the validity of the results is likely to be affected by the consistent response style from the same respondent. Moreover, the content from some SDQ items (particularly items measuring inattention/hyperactivity) overlapped with those of the ASRS-R, which may have resulted in a high degree of consistency in the responses; however, this holds less value for determining validity. Future studies could use semi-structured clinical diagnostic interviews to ascertain the construct validity of the ASRS-R. Second, this study relied solely on self-reports and did not incorporate parent or teacher interviews, which may have introduced some bias in the results. Third, this study included students only from two schools, making it unclear whether the results can be extended to other populations and districts. Therefore, replicating studies involving other cultures is necessary to enhance the generalizability and reliability of the current findings. Fourth, the study lacked a diagnostic group, and therefore, the sensitivity and specificity of the ASRS-R could not be assessed. To enhance the accuracy of the results, future studies should add a diagnostic group. Lastly, the study was conducted in a normal population, thus capturing a wide range of responses, which is likely to have affected the psychometric properties. Future studies should consider using data from this study for comparison with clinical samples to verify the reliability of the results.
Conclusion
The findings of this study provide evidence that the ASRS-R is a promising tool for assessing ADHD in Chinese adolescents. These findings are relevant in extending the range of applications of the ASRS-R from ADHD diagnosis at adulthood to adolescence, underscoring its applicability to screen school-going adolescents likely to have ADHD. This will provide opportunities to more effectively identify and manage adolescent ADHD. Childhood ADHD has been well-researched; however, information about this condition in adolescents is unavailable so far. Findings from non-adolescent ADHD samples (i.e., children or adults) cannot be generalized to clinical practice with adolescents mainly because ADHD manifests differently in children, adolescents, and adults (Nichols et al., 2017). The ASRS-R demonstrated good reliability and construct validity in adolescent samples in this study; thus, this self-reporting tool can be used by clinicians and researchers dealing with adolescents to enrich information about ADHD in adolescents. Implementing an easy-to-use self-report ADHD screening measure to identify adolescents in need of a comprehensive assessment of ADHD characteristics may help avoid negative ADHD sequelae (e.g., risk seeking). However, given that multiple factors may contribute to the high rate of false positives in self-report screening measures, clinicians should combine information from multiple sources to assess ADHD, rather than relying solely on self-reporting.
Footnotes
Acknowledgements
The authors thank the support and participant of all the students and providers in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Heilongjiang Province [No. LH2023H021] and the Postgraduate Research & Practice Innovation Program of Harbin Medical University [No. YJSCX2023-297HYD].