
Abstract
Introduction:
Conflicting findings exist regarding the link between attention deficit hyperactivity disorder (ADHD) and cardiovascular diseases. This study aimed to evaluate the frontal QRS-T (fQRS-T) angle and its correlation with symptom severity in children diagnosed with ADHD.
Methods:
The study population consisted of 172 patients diagnosed with ADHD (120 drug naive and 52 drug positive) and 82 healthy controls. ADHD symptoms were assessed using the Atilla Turgay DSM-IV-Based Screening and Assessment Scale for Disruptive Conduct Disorders (T-DSM-IV-Scale). The fQRS-T angle and corrected QT (QTc) interval were obtained from the automated reports of 12-lead electrocardiography device for each patient.
Results:
QTc interval and fQRS-T angle were significantly different among the groups. Post hoc analyses showed that QTc interval and fQRS-T angle of ADHD drug naive and ADHD drug positive patients were significantly higher than the healthy control groups. However, there was no significant difference between drug naive and drug positive patients regarding QTc interval and fQRS-T angle. Both QTc interval and fQRS-T angle showed positive correlations with the severity of ADHD symptoms (r = 0.263, p = .001 and r = 0.175, p = .023 respectively).
Conclusion:
We found that fQRS-T angle was significantly wider in children with ADHD. Therefore, we suggest that fQRS-T angle may help in cardiovascular risk assessment in children with ADHD.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a common psychiatric condition in children and adolescents, characterized by inattention, hyperactivity, and impulsivity (American Psychiatric Association [APA], 2013). Its global prevalence is about 7.6% among children and 5.6% among adolescents (Salari et al., 2023). A multicenter study conducted in Turkey found a prevalence of 12.39% in children aged 6 to 13 years, with 19.48% being without impairment (Ercan et al., 2019). It is more prevalent in males and can present as inattentive, hyperactive/impulsive, or combined types (APA, 2013; Erskine et al., 2013; Faheem et al., 2022). Symptoms often diminish with age but may persist into adulthood (Zalsman et al., 2016). ADHD is associated with other mental health disorders and adverse outcomes like academic underachievement and higher criminal involvement. Early recognition and treatment are important to reduce long-term effects (Cherkasova et al., 2022; Katzman et al., 2017).
Clinical guidelines recommend medication as a key treatment for managing ADHD symptoms, with stimulant (e.g., methylphenidate [MPH], amphetamine [AMP]) and nonstimulant (e.g., atomoxetine [ATX]). Given the chronic nature of ADHD, many patients require long-term pharmacotherapy (Banaschewski et al., 2006; Pliszka & AACAP Work Group on Quality Issues, 2007; Taylor et al., 2004). Although generally safe, these medications may affect cardiac functions by influencing heart rate and blood pressure (BP), because they are sympathomimetic agents (Hennissen et al., 2017). It is recommended to monitoring BP and heart rate regularly in children using MPH and ATX due to their sympathomimetic properties, which may potentially lead to proarrhythmic effects (Lamberti et al., 2015). A meta-analysis reported significant increases in systolic BP (SBP), diastolic BP (DBP), and heart rate with AMP and ATX treatment (Hennissen et al., 2017). In addition, MPH has been reported to prolong corrected QT (QTc) interval, potentially causing life-threatening ventricular arrhythmias (Karpuz et al., 2017a; C. Zhang et al., 2015). A systematic meta-analysis of observational studies did not show association between ADHD medication and risk of cardiovascular disease, but a more recent study suggested that long-term exposure to ADHD medications may be a risk factor for future development of hypertension and arterial disease (L. Zhang et al., 2022, 2024). However, studies have not consistently shown increased risk of cardiovascular events with ADHD medications (Winterstein, 2012). ADHD itself poses an independent risk for cardiovascular diseases (Li et al., 2022), with studies reporting cardiac arrhythmias in medication-free ADHD children (Altay, 2018; Buchhorn & Christian, 2014).
The frontal QRS-T (fQRS-T) angle is a novel marker of myocardial depolarization and repolarization heterogeneity and an increase in this angle shows the electrical instability of the myocardium. It can be calculated as the absolute difference between the frontal plane QRS axis and the T axis on a standard 12-lead electrocardiography (ECG) (Macfarlane, 2012; Tanriverdi et al., 2018). Frontal QRS-T angle has been investigated in many cardiac and non-cardiac diseases and found to be associated with sudden cardiac death, arrhythmias, and poor prognosis (Aro et al., 2012; Colluoglu, et al., 2018; Oehler et al., 2014). Its clinical importance has also been demonstrated in some psychiatric disorders (Tekin et al., 2022; Yılmaz et al., 2024).
Given the potential cardiovascular implications of ADHD and its treatment, understanding risk factors is crucial for preventive strategies. We have thought that fQRS-T angle could be associated with the risk of cardiovascular disease in patients diagnosed with ADHD. To our knowledge, no study has investigated the fQRS-T angle in patients with ADHD. We have hypothesized that ADHD patients may have wider fQRS-T angle than healthy controls. For this reason, we aimed to evaluate the clinical importance of fQRS-T angle in children and adolescents with ADHD. We also will investigate the association of fQRS-T angle with clinical features such as disease severity, medication use, and dosage.
Methods
Study Population
Children and adolescents aged 6 to 18 years who visited the Harran University Faculty of Medicine Child and Adolescent Psychiatry Outpatient Clinic between January 2022 and January 2023, and who were diagnosed with ADHD following psychiatric evaluation were included in the study. During this period, the records of 634 patients diagnosed with ADHD were accessed. Each patient underwent initial evaluation by a senior child and adolescent psychiatry resident and an experienced child and adolescent psychiatrist to assess ADHD and any comorbid psychiatric disorders, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria (APA, 2013). Demographic characteristics, medication histories, and histories of cardiovascular and psychiatric conditions were documented from patient records. ADHD symptoms were evaluated using the Atilla Turgay DSM-IV-Based Screening and Assessment Scale for Disruptive Conduct Disorders (T-DSM-IV-Scale).
The study included two groups: the drug-naive group comprised newly diagnosed patients with ADHD who had not previously received MPH/ATX or other psychiatric medications, and who had a baseline ECG recording. The drug-positive group included patients receiving OROS-MPH monotherapy for at least 1 month, with an ECG record from their latest visit. Exclusion criteria for both groups included other psychiatric or medical disorders, history of cardiovascular abnormalities, prior use of drugs known to affect the cardiovascular system (heart rhythm, blood pressure, and electrocardiogram), smoking, history of substance use, and IQ below 70 (Figure 1). As a control group, 82 healthy children and adolescents without psychiatric or medical conditions or history of drug use, who applied for routine check-up to Harran University Faculty of Medicine Pediatrics Clinic were also included. The study protocol was approved by the Harran University Clinical Research Ethics Committee (approval date XXX, protocol number XXX), and permission from the hospital administration was obtained.

Flow chart of patients with ADHD.
Measures
Sociodemographic Form
Information such as age, gender, weight, height, duration of drug use, and dosage were obtained from the patients’ existing files. Body mass index (BMI) was obtained by dividing body weight by the square of height (kg/m2). Age, gender, weight, and height were also obtained for the healthy control group.
Turgay DSM-IV-Based Child and Adolescent Disruptive Behavioral Disorders Screening and Rating Scale (T-DSM-IV-Scale)
The evaluation tool developed by Atilla Turgay is a scale consisting of 41 items: 9 questions on attention deficit, 6 on hyperactivity, 3 on impulsivity, 8 on oppositional defiant disorder (ODD), and 15 on conduct disorder. It is administered to parents or teachers of children suspected to have ADHD. Each item is rated on a scale of 0 = none, 1 = a little, 2 = a lot, and 3 = very much. The Turkish version of this scale was validated by Ercan et al. (2001). In this study, the T-DSM-IV-Scale filled out by parents was used for evaluation.
Electrocardiography (ECG)
Twelve-lead ECG was performed on all participants in a supine position, using settings of 10 mm/mV amplitude, 25 mm/s speed, and a filter range of 0.16 to 100 Hz. ECG parameters including QRS duration, QT interval, and QT corrected (QTc) interval were automatically calculated from the ECG device report. QRS duration was defined as the time from the beginning of the Q wave to the end of the S wave, while QT interval was measured from the beginning of the Q wave to the end of the T wave. The QTc interval was adjusted for heart rate using Bazett’s (1920) formula. The fQRS-T angle was derived from the automated ECG report, calculated as the absolute difference between the QRS axis and T axis (Colluoglu et al., 2018). If this difference exceeded 180 degrees, the angle was calculated by subtracting it from 360 degrees. An example of an automated ECG report is shown in Figure 2.
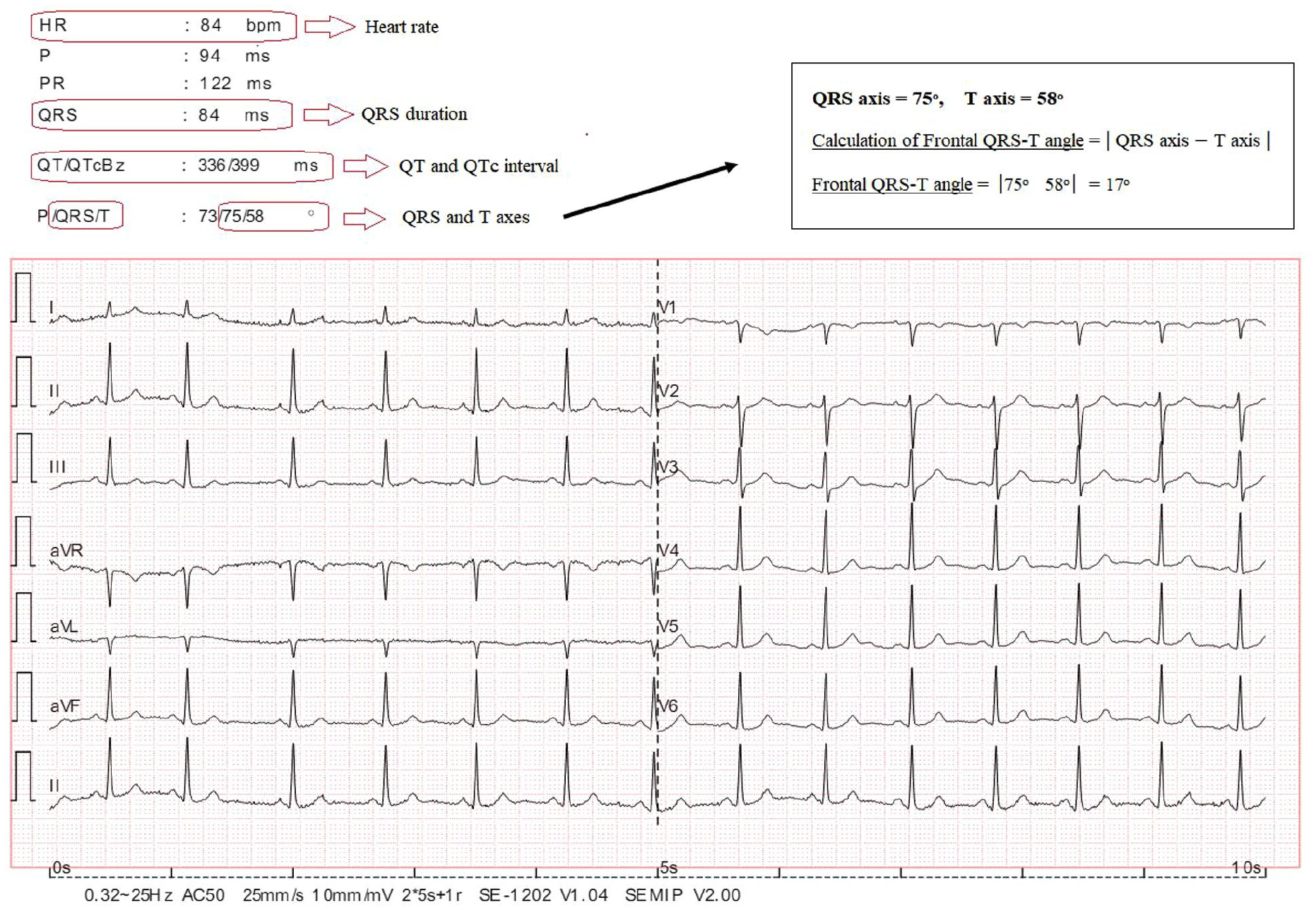
The automatic report of an electrocardiography and calculation of fQRS-T angle from this report.
Statistical Analysis
Statistical analysis was conducted using SPSS version 23.0. The Kolmogorov-Smirnov test was used to assess the distribution of variables. Normally distributed continuous variables were presented as mean ± SD and compared using one-way analysis of variance (ANOVA). Tukey’s post hoc test was employed to identify significant differences among groups. Non-normally distributed continuous variables were reported as median (25th–75th interquartile range, IQR) and compared using the Kruskal-Wallis test. Bonferroni correction was applied for post hoc tests to determine significant differences among groups. Categorical variables were presented as number (percentage) and compared using the chi-square test. Correlation analysis was performed using Pearson or Spearman correlation coefficients as appropriate. A p-value of <.05 was considered statistically significant.
Results
A total of 172 patients diagnosed with ADHD and 82 healthy controls were included in this study. 52 of ADHD patients were under OROS-MPH medication. Comparison of baseline characteristics of the study groups are presented in Table 1. Age (p = 0.181), gender (p = 0.284), body mass index (p = 0.102), SBP (p = 0.108), and DBP (p = 0.466) were similar among the three groups. However, heart rate was significantly different among the groups. It was found that heart rate of ADHD drug naive and ADHD drug positive patients were significantly higher than the healthy control group (Table 1).
Comparison of Baseline Characteristics of the Study Groups.

Note: BMI = Body mass index; SBP = systolic blood pressure; DBP = diastolic blood pressure; SD = standard deviation.
p < .05 versus control group.
Comparison of electrocardiographic parameters of the study groups are listed in Table 2. QRS duration, QTc interval, and fQRS-T angle were significantly different among the groups. Pairwise comparisons with post hoc analyses were performed to determine the difference resulted from which group. We observed that QRS duration and QTc interval of ADHD drug naive and ADHD drug positive patients were significantly higher than the healthy control group. Also, fQRS-T angle was significantly wider in ADHD drug naive and ADHD drug positive patients compared to the healthy control group. However, no significant difference was detected between ADHD drug naive and ADHD drug positive patients in terms of QRS duration, QTc interval, and fQRS-T angle.
Comparison of Electrocardiographic Parameters of the Study Groups.
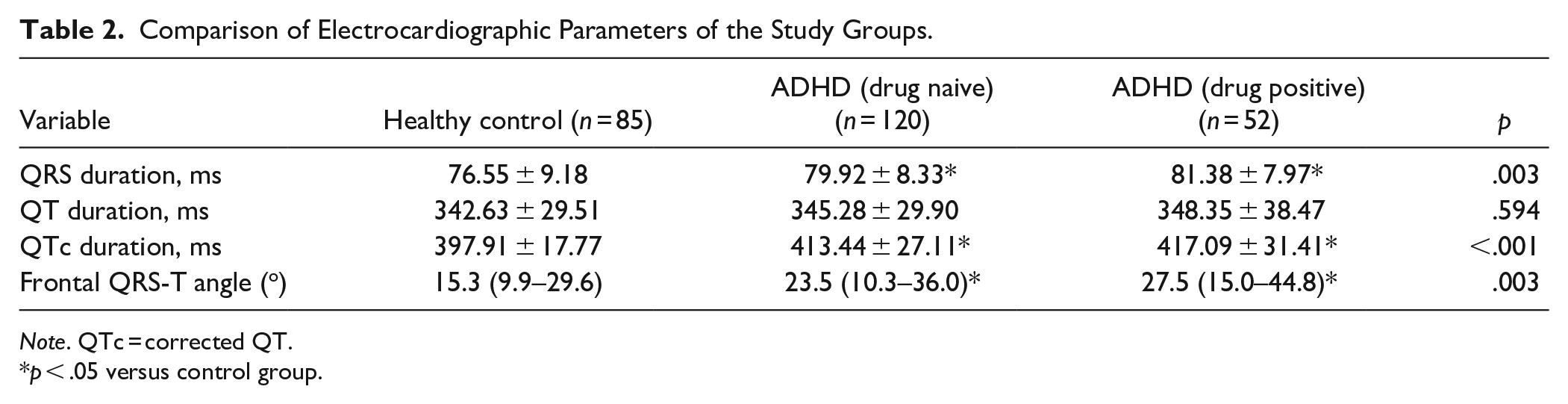
Note. QTc = corrected QT.
p < .05 versus control group.
T-DSM-IV-Scale scores of the drug naive group were significantly higher than the drug positive group. The median duration and dosage of medication in ADHD drug positive patients were 2 months and 27 mg/day, respectively (Table 3).
Comparison of Clinical Features of the Patients With ADHD.

Correlation analysis was performed to determine the correlation of electrocardiographic parameters with clinical parameters. We found that QTc interval and fQRS-T angle was positively correlated with T-DSM-IV-Scale total point (r = 0.263, p = .001 and r = 0.175, p = .023, respectively) (Figure 3). No correlation was found between QTc interval, fQRS-T angle, the mean duration, and dosage of medication (p > .05).
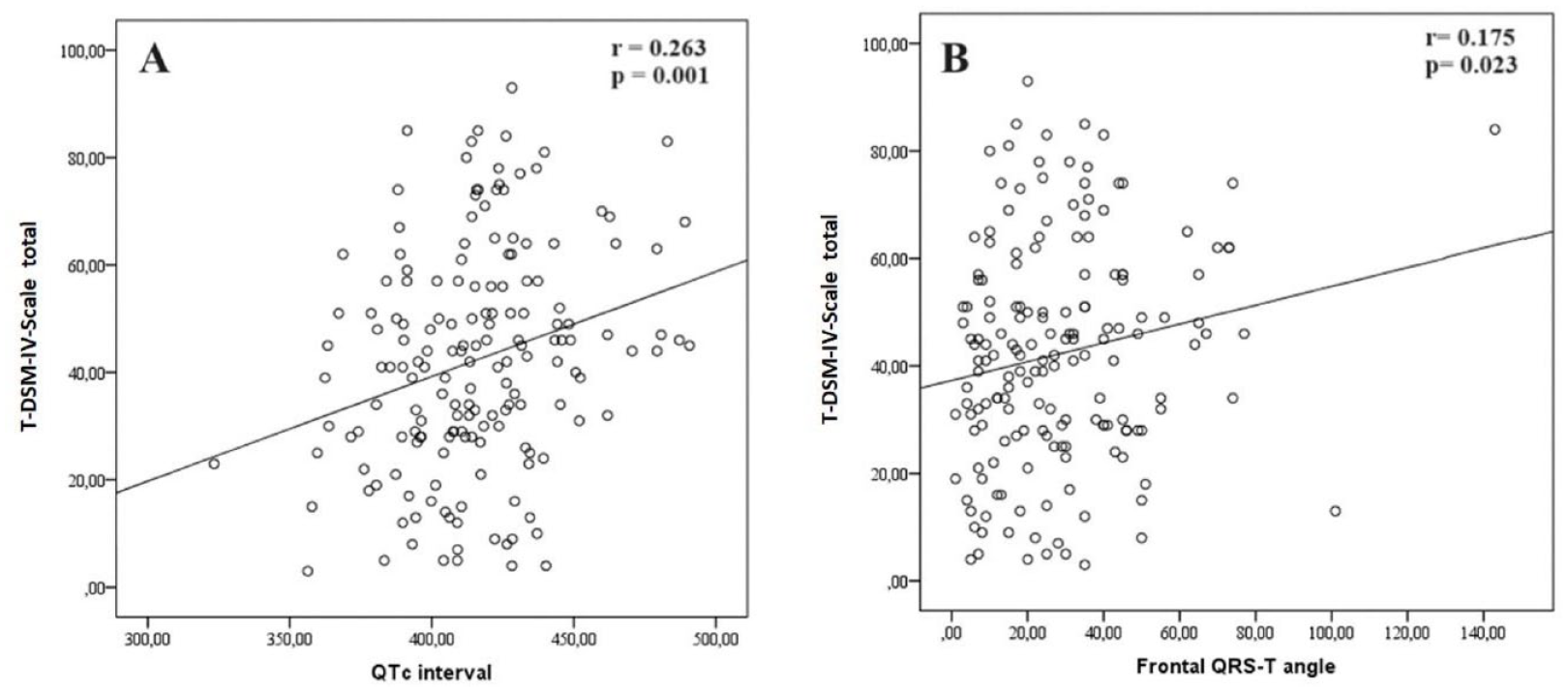
(a) Correlation analysis of QTc interval and (b) fQRS-T angle with T-DSM-IV-Scale total point.
Discussion
The main findings of this study are as follows: (i) Patients diagnosed with ADHD exhibited significantly wider QTc interval and fQRS-T angle values compared to healthy controls. (ii) There was no significant difference in terms of QTc interval and fQRS-T angle between ADHD drug-naive patients and those on medication. (iii) QTc interval and fQRS-T angle were positively correlated with the severity of ADHD symptoms, whereas they were not correlated with the mean duration and dosage of medication. These results highlight the potential cardiac implications in ADHD patients, emphasizing the relevance of QTc interval and fQRS-T angle as markers associated with symptom severity.
Limited studies have investigated ECG abnormalities in children diagnosed with ADHD, with the QT interval being a frequently studied electrocardiographic marker. The QTc interval, reflecting ventricular depolarization and repolarization, is crucial as its prolongation poses a risk for ventricular arrhythmias (Ari et al., 2014). Prasad et al. (2007) observed in their study that a history of stimulant treatment and Caucasian racial origin were linked to significantly longer mean QTc values. Additionally, a recent study by Snircova et al. (2017) reported QTc prolongation following 8 weeks of treatment with ATX and MPH. These findings highlight the importance of monitoring QTc interval in ADHD patients undergoing pharmacological therapies. Isart et al. (2021) reported that although the QTc interval in ADHD patients differed significantly from healthy controls, these differences lacked clinical significance unless considering the addition of QT prolonging drugs. Moreover, their study noted a lower proportion of subjects with QRS values more than 1 standard deviation above the mean (≥94 ms) in the ADHD group compared to controls. Omidi et al. (2021), in a study involving 100 newly diagnosed children aged 6 to 11 years with ADHD, found that after 3 months of MPH treatment, there were significant increases in blood pressure indices, yet no significant changes in the QT interval were observed. Similarly, Lamberti et al. (2015), in their investigation of the acute cardiovascular effects of rapid-release MPH in children and adolescents with ADHD, reported no significant alterations in ECG parameters. In a retrospective study by Türkmenoglu et al. (2020), which examined the medical records of 33 children aged 6 to 15 years receiving MPH treatment for ADHD, no significant differences were observed in QRS, QT, QTc, and QTd intervals before and after treatment. Martinez-Raga et al. (2013) concluded in a comprehensive review that the risk of significant QTc prolongation after stimulant or ATX medications in ADHD treatment is notably low, but caution is warranted in patients with cardiovascular risk factors. Consistent with these findings, Altay (2018) found in a study involving 43 children with ADHD not receiving medication and 36 healthy controls that the QTc interval was statistically longer in ADHD patients compared to controls. Similarly, our study showed that QTc intervals were longer in children diagnosed with ADHD compared to healthy controls, with no significant difference observed between ADHD groups with and without medication. The underlying mechanism for QT interval prolongation in ADHD may be linked to potential abnormalities in cardiac function associated with dopaminergic and noradrenergic genes (Snircova et al., 2017).
Heart rate was reported to be higher in ADHD patients, even in the absence of treatment. Karpuz et al. (2017b) found that average heart rate values were elevated in medication-free ADHD patients compared to controls. Additionally, another study noted significantly reduced heart rate variability (HRV) in untreated children with ADHD, suggesting a potential autonomic disorder (Buchhorn et al., 2012). Decreased HRV is linked to increased cardiac morbidity and mortality in adults, implying a heightened risk of arrhythmias in children with ADHD (Altay, 2018; Buchhorn et al., 2012). In our study, we observed significantly higher average heart rate in both medicated and non-medicated ADHD groups compared to healthy controls, which aligns with findings in the literature. These results underscore the existing literature on the immature physiological development of autonomic function and diminished parasympathetic tone in children diagnosed with ADHD.
Although numerous studies have investigated the QT interval in children diagnosed with ADHD, there is a notable absence of research on the clinical significance of the fQRS-T angle. Studies have demonstrated that the fQRS-T angle is more reliable, reproducible, and less affected by noise compared to QT interval (Raposeiras-Roubín et al., 2014). Therefore, in clinical practice, the fQRS-T angle may serve as a more accurate and accessible electrocardiographic marker than QT interval. Increased fQRS-T angle is associated with impaired myocardial repolarization, which has been linked to ventricular arrhythmias and sudden cardiac death (Aro et al., 2012; Colluoglu et al., 2018). Although limited, there is emerging evidence on the association between the fQRS-T angle and psychiatric disorders. For instance, Tekin et al. (2022) found that schizophrenia patients exhibited a wider fQRS-T angle compared to healthy controls, and this angle was correlated with disease duration and severity of negative symptoms. Similarly, Kapıcı et al. (2023) observed a significantly wider fQRS-T angle in drug-naive first episode psychosis patients compared to healthy controls (Kapıcı et al., 2023). In our study, we found that the fQRS-T angle in children diagnosed with ADHD was significantly wider than in healthy controls. These findings suggest that children with ADHD may be more susceptible to cardiac arrhythmias, and the fQRS-T angle could potentially detect repolarization abnormalities before significant ECG changes or obvious heart disease develop.
In the current study, it was also found that QTc interval and fQRS-T angle was positively correlated with the severity of ADHD symptoms, whereas they were not correlated with the mean duration and dosage of medication in ADHD drug positive patients. There is limited information about the relationship between cardiovascular outcomes and the severity of the disease, duration, and dosage of medication in patients with ADHD in the literature. Only one study has investigated this relationship. Contrary to our findings, Öğütlü et al. (2021) found a statistically significant, negative, moderate correlation between the severity of ADHD symptoms and carotid artery intima-media thickness (cIMT), an indicator of cardiovascular disease. The authors explained this situation as potentially being related to the positive effects of increased physical activity overshadowing the negative effects of increased BMI and maladaptive eating patterns on cardiovascular health in children with ADHD. However, the lack of information on BMI values for the case groups in this study can be considered a limitation. Moreover, the low number of cases in this study can also be considered a limitation that hinders the generalizability of this finding (Öğütlü et al., 2021). The remarkable finding of our study was that increased QTc interval and fQRS-T angle in ECG was associated with higher symptoms scores in children with ADHD. Therefore, it may be considered that higher ADHD symptoms scores are associated with an increased risk of cardiovascular disease in children with ADHD because of their relations with the QTc interval and fQRS-T angle. Meanwhile, the relationship between cardiovascular outcomes and the duration and dosage of medication in patients with ADHD is a controversial topic in the literature. Consistent with our findings, Hammerness et al. (2009), in their study on long-term, high-dose MPH treatment in adolescents, did not observe changes in PR, QRS, and QTc intervals. Also, Hennissen et al. (2017) found no significant effects of various moderators—such as type of medication, dosage, sample size, age, gender, type of ADHD, comorbidity, and dropout rate—on cardiovascular outcomes in children and adolescents with ADHD. Conversely, Donner et al. reported that patients receiving high doses (40 mg/day) of MPH experienced more cardiovascular side effects compared to those receiving lower doses, although vital signs remained stable (Donner et al., 2007). We think that further studies with long follow up duration are needed to better determine the effect of used drugs in ADHD on electrocardiographic parameters and long-term cardiovascular risk.
The limitations of our study include its retrospective nature, the use of data from a single center, and the lack of evaluation of ECG parameters in the same patients before and after treatment. Additionally, the number of ADHD patients receiving medication was relatively low, and the treatment duration was shorter compared to other studies. Last, although we found a significant correlation between fQRS-T angle and ADHD symptom severity, the correlation coefficient was not strong. This may be due to the cross-sectional nature of the study. Therefore, causality may not be inferred between the variables. Future prospective studies are required to better elucidate the association of fQRS-T angle with disease severity. Despite these limitations, our study benefits from the absence of additional psychiatric comorbidities in our ADHD group and a large sample of ADHD patients not receiving medication, which are strengths of our research.
Conclusion
To conclude, fQRS-T angle is wider in children with ADHD than in healthy controls. Therefore, monitoring of fQRS-T angle may help in cardiovascular risk assessment in children with ADHD. To better understand the mechanism underlying the increased fQRS-T angle in ADHD patients, more comprehensive prospective studies are needed in which these patients are followed for the development of cardiovascular disease or arrhythmia.
Footnotes
Acknowledgements
The authors would like to thank all the participants in this study.
CRediT Authorship Contribution Statement
Fethiye Kılıçaslan: Writing – review & editing, Writing – original draft, Methodology, Data curation, Formal analysis.
Aybike Tan: Writing – review & editing, Data curation.
Zulkif Tanriverdi: Writing – review & editing, Writing – original draft, Investigation, Data curation, Conceptualization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved by the Harran University Clinical Research Ethics Committee (approval date 20/02/2023, protocol number 23.03.05), and permission from the hospital administration was obtained.
Availability of Data and Material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.