
Abstract
Introduction:
Our study aimed to compare the sociodemographic, diagnostic, clinical, and self-report scale data of adults diagnosed with ADHD in childhood/adolescence versus adulthood and to identify risk factors associated with delayed/missed diagnosis for ADHD.
Method:
Sociodemographic, clinical, and diagnostic data of 214 adults with ADHD, followed at the Adult Neurodevelopmental Disorders Clinic, Selçuk University, between January 2022 and January 2024, were analyzed. The diagnostic evaluations were made using the Structured Clinical Interview for DSM-5 Clinician Version. Clinical data included age, gender, years of education, alcohol/substance use, diagnosis age, and current medication use for ADHD. Data collected from self-report scales included both ADHD-related measurements and comorbidity-related measurements.
Results:
The findings revealed that only 34.4% (n = 74) of sample received a formal ADHD diagnosis during childhood/adolescence. Adults diagnosed with ADHD in adulthood were older and had higher education levels, more severe ADHD symptoms, and increased maladaptive daydreaming (MD) scores, compared to those diagnosed in childhood or adolescence. Logistic regression analysis indicated that the severity of MD was associated with being in the group diagnosed with ADHD in adulthood while controlling for other significant parameters from bivariate analyses, such as age, years of education, and current medication use for ADHD. Finally, analyses conducted separately in both groups showed that: (1) increased MD severity was a predictor of higher ADHD symptoms in those diagnosed in adulthood, but not in those diagnosed in childhood/adolescence, and (2) MD severity had a stronger correlation with ADHD symptoms, the number of comorbid psychiatric disorders, and symptoms of excessive mind wandering, depression, and anxiety in those diagnosed in adulthood compared to those diagnosed in childhood/adolescence.
Conclusion:
MD may delay ADHD diagnosis until adulthood by masking and compensating ADHD symptoms and delay in referral to mental health professionals, and it might also be a predictive symptom for recognizing ADHD in adults who have never been diagnosed; however, longitudinal studies are needed to confirm this.
Introduction
ADHD is the most common childhood-onset neurodevelopmental disorder, characterized by attention problems, overactivity, impulsiveness, and executive dysfunctions, with high heritability (Demontis et al., 2023; Faraone et al., 2021). ADHD diagnosis persists throughout adulthood in at least half of children with ADHD. Adults with ADHD have a cumulative burden associated with a higher risk of psychiatric disorders (e.g., depression, anxiety disorders, substance use disorder, and personality disorders), physical illnesses (e.g., obesity, cardiovascular diseases, asthma, and autoimmune diseases), and social difficulties (e.g., school disengagement, sexually transmitted infections, accidents, and injuries) compared to those without ADHD (Kooij et al., 2019). ADHD in childhood, youth, and adulthood causes a significant financial burden to countries due to direct costs, well-being losses, and productivity losses (Chhibber et al., 2021). Growing evidence has shown that early and effective treatment of ADHD improves ADHD-related negative outcomes in adults with the condition; however, this necessitates early and accurate diagnosis (Faraone et al., 2024; Kooij et al., 2019).
Although ADHD is not a new diagnosis, it was recognized relatively later than many other psychiatric conditions from a historical perspective (Rivas-Vazquez et al., 2023). Concerns with early and accurate diagnosis continue, especially in the adult population, which may be due to: (1) the changing presentation of ADHD symptoms as individuals transition into adulthood, (2) gender differences, with females more likely to exhibit inattentive symptoms and less hyperactivity, impulsivity, and behavioral symptoms, leading to fewer referrals to professionals, as well as having more coping strategies and psychiatric comorbidities compared to males, (3) coping strategies, comorbid conditions, high intelligence, and social problems in adults with ADHD that may mask the symptoms, (4) lack of knowledge and experience among practitioners regarding ADHD in adulthood, and (5) despite the changes in DSM-5 that have facilitated the diagnosis of ADHD in adults, experts argue that DSM symptoms do not reflect ADHD in adults. Additionally, there may still be a lack of assessment tools specifically designed for this population (Asherson et al., 2016; Barkley, 2024; Kooij et al., 2019; Vingilis et al., 2015).
Notably, while the severity of hyperactivity and impulsivity tends to decrease with age, attention problems persist to impair functionality. These attention problems may include certain patterns of mind wandering, a term used for all spontaneous thoughts that negatively affect attention to some extent, independent of external stimuli (Chaieb et al., 2022). Additionally, excessive mind wandering refers to continuous mental overactivity characterized by multiple, rapid, unrelated, and fleeting thoughts (Mowlem et al., 2019). The European Network Adult ADHD stated their recent consensus report that excessive mind wandering is one of the distinctive symptoms of adults with ADHD (Kooij et al., 2019). However, there is no assessment of this in DSM-5. Moreover, a recent study emphasized that certain thought process (mentation patterns), including excessive mind wandering, may mediate the relationship between ADHD symptoms and comorbidities in adults with ADHD (Kandeğer et al., 2024). Thus, thought process patterns may increase comorbidities, potentially masking the diagnosis of ADHD.
Another mentation pattern with interesting findings reported in relation to ADHD is Maladaptive Daydreaming (MD), which is defined as compulsive fantasizing characterized by shifting attention from external stimuli to inner imaginative scenarios. These fantasies generally function as emotional compensation and an escape from negative feelings. MD can exhibit a behavioral addiction pattern, with people frequently choosing to imagine their fantasies during the day when they feel overwhelmed by negative thoughts and emotions (Pietkiewicz et al., 2018). This pattern leads to impaired social, occupational, and academic functionality by consuming a significant amount of daily time and widening the gap between fantasies and reality, which has been described as “parallel lives” in certain cases (Somer, Somer, & Jopp, 2016).
MD has been associated with dissociative symptoms due to their shared phenomenological characteristics, such as high absorption, fantasy proneness, and even double consciousness. There has been speculation that childhood trauma could be a causal factor for both dissociative symptoms and MD. However, Somer et al. (2017), in the first comorbidity report of MD according to DSM-5, found that the most common diagnosis was ADHD, particularly the predominantly inattentive type. In a recent study involving 83 adults with ADHD, Theodor-Katz et al. found that only 20.5% of participants had MD, suggesting that MD is a distinct construct from ADHD. Consequently, the researchers recommend that future studies differentiate between attention problems, MD, and mind wandering symptoms to better understand these conditions (Theodor-Katz et al., 2022).
Valuable efforts have been made to understand what is the delaying factors of ADHD diagnosis. A recent study comparing adults diagnosed with ADHD in childhood/adolescence versus adulthood found that the clinical characteristics of both groups were largely similar (Hutt Vater et al., 2024). However, there are no studies evaluating specific findings in adults with ADHD, such as excessive mind wandering, and confounding mentation patterns such as MD and dissociation. Our aim in this study is to investigate the potential factors associated with the delay in ADHD diagnosis from childhood to adulthood. Specifically, this study will evaluate ADHD symptoms, sociodemographic and clinical factors, as well as comorbid symptoms that often accompany ADHD. Groups are divided into those diagnosed in childhood or adolescence and those diagnosed in adulthood.
Materials and Methods
Study Center
Our study is a cross-sectional study conducted between January 2022 and January 2024, focusing on adults diagnosed with ADHD who were referred to the Adult Neurodevelopmental Disorders Clinic in the Department of Psychiatry at Selçuk University. This is the only specialized outpatient clinic dealing neurodevelopmental disorder in adults in the city of Konya, which has a population of approximately two million and is located in the Central Anatolia in Türkiye.
Participants and Procedure
Sociodemographic and clinical data of the participants were collected, diagnostic confirmation and evaluation of comorbid psychiatric diagnoses were conducted using the SCID-5-CV form, and functionality was assessed with the Global Assessment of Functioning. However, since this diagnostic process required considerable time, it was completed over two separate sessions. Additionally, an online link designed for this study via Google documents to collect self-report data stated below, has been sent to participants.
During this period, 256 individuals diagnosed with ADHD were included in the study; however, participants with incomplete forms, those diagnosed with intellectual disabilities or neurocognitive disorders, and those with psychotic or bipolar disorders who were not in remission were excluded from the sample. Data collection was completed for 214 participants. The study protocol was approved by the Local Ethics Committee of Selçuk University (Decision Number: 2022/113).
Measurements Tools
ADHD-related Measurements
The Adult ADHD Self-Report Scale (ASRS) is an 18-item self-report scale designed to assess adult ADHD symptoms based on DSM-IV-TR criteria (American Psychiatric Publishing, 2000; Kessler et al., 2005). Attention deficit symptoms are questioned with the first nine items, and hyperactivity and impulsivity symptoms are questioned with the last nine items. Higher scores on the ASRS indicate more severe ADHD symptoms. The validity and reliability of the Turkish version have been confirmed by two studies involving both clinical and non-clinical samples (Dogan et al., 2009; Evren et al., 2016)
The Wender Utah Rating Scale (WURS), developed by Ward et al. (1993), assesses childhood ADHD symptoms to aid in diagnosing ADHD in adults. Initially, it was a 61-item, 5-point Likert-type self-assessment scale. Subsequent analysis refined it to 25 items that best differentiate adults with ADHD from healthy controls. The WURS adapted into Turkish by Öncü et al (2005).
The Mind Excessively Wandering Scale (MEWS), developed by Mowlem et al. (2019), assesses excessive mind wandering, a characteristic feature of adults with ADHD according to the European consensus (Kooij et al., 2019). The MEWS is a 12-item Likert-type scale where higher scores indicate higher levels of excessive mind wandering. An adaptation study in adults with ADHD found that the Turkish version of the MEWS is a valid and reliable measurement tool (Aksoy et al., 2022).
Comorbidity-related Measurements
The Hospital Anxiety Depression Scale (HADS), a 4-point Likert-type scale consisting of 14 questions, was developed by Zigmond and Snaith (1983) to measure the severity of depression and anxiety in a hospital setting. Seven of the questions assess anxiety severity, while the remaining seven evaluate depression severity. A Turkish validity and reliability study was conducted by Aydemir (1997).
The Childhood Trauma Questionnaire (CTQ), developed by Bernstein et al. (1994), is a self-report tool that retrospectively and quantitatively evaluates experiences of abuse and neglect before age 20. It consists of 28 questions across five sub-dimensions: emotional abuse, physical abuse, physical neglect, emotional neglect, and sexual abuse. The Turkish version, validated by Sar et al. (2012), demonstrated strong internal consistency.
The Dissociative Experiences Scale (DES) is a self-report questionnaire with 28 items designed to measure dissociative experiences, ranging from minor experiences like absorption to severe symptoms such as depersonalization-derealization and dissociative amnesia (Holmes et al., 2005; Putnam, 1997). The Turkish version has demonstrated excellent reliability and validity (Yargic et al., 1995).
The Maladaptive Daydreaming Scale (MDS) is a 16-item self-assessment questionnaire developed by Somer in 2016 to identify MD behaviors and symptom levels in both adolescents and adults (Somer, Lehrfeld, et al., 2016). The Turkish validity and reliability study was conducted by Metin et al. (2022).
Analyses
The data entry and analysis process were conducted using the Statistical Package for the Social Sciences 22 package program. Cronbach alpha values were calculated to evaluate the reliability of the measurement tools. Skewness and kurtosis values between −2 and + 2 were used to determine the normal distribution (George, 2011). After completing the descriptive analyses, the sample was divided into two groups based on whether ADHD was first diagnosed in childhood/adolescence (diagnosed at < age 18 years) or adulthood (diagnosed at ≥ age 18 years). Numerical variables between the two groups were compared according to distribution characteristics the independent t-test or Mann Whitney U test, while categorical variables were compared using the chi-square test. Effect sizes were estimated using Cohen’s d for parametric and non-parametric comparisons, and Cramer’s V for categorical variables. Effect sizes were considered as ≥0.8 large, 0.5 to 0.79 intermediate, 0.2 to 0.49 small, and <0.2 no effect (Cohen, 2013; Husted et al., 2000).
Pearson correlation analysis was used to correlate numerical data. A backward (likelihood ratio) logistic regression model was used to determine the best predictors for being first diagnosed with ADHD in adulthood, with related factors identified from bivariate analyses assigned as independent variables. Finally, two linear regression analyses were conducted to test the prediction of MDS scores on ASRS scores for each group separately. In these models, partial regression plots were generated to illustrate the relationship between the ASRS scores and MDS scores, excluding the effects of confounding factors. Multicollinearity was checked using “Variance Inflation Factor (VIF)” and “tolerance” values. Risk values were determined with a 95% confidence interval, and statistical significance was set at p < .05.
Results
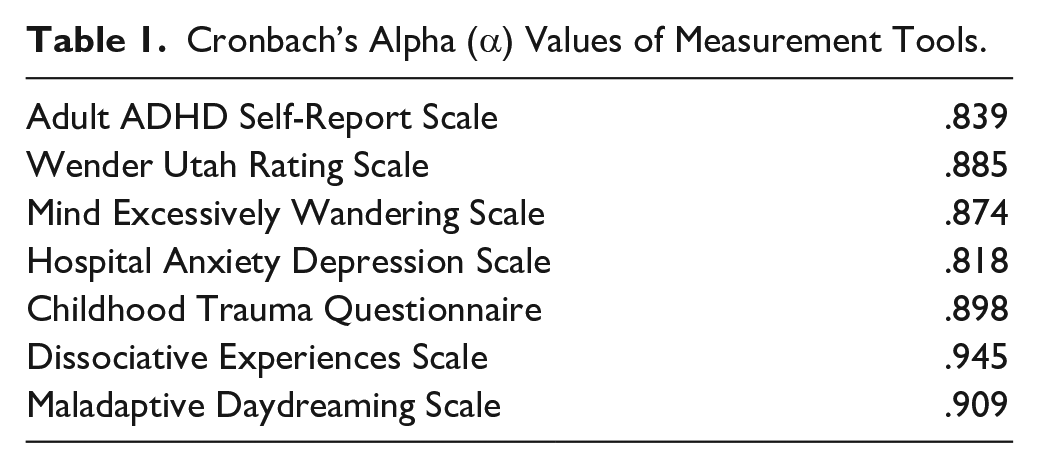
All measurement tools demonstrated good to excellent reliability, with Cronbach’s alpha values ranging from .818 to .945 in this study, as presented in Table 1.
Cronbach’s Alpha (α) Values of Measurement Tools.
The mean age of the 214 adults with ADHD who completed the study protocol was 23.24 ± 5.3 years (18–49, min–max), and 53.3% (n = 114) were female. The findings revealed that only 33.6% (n = 72) of participants reported having received a formal ADHD diagnosis during childhood or adolescence. According to the SCID-5-CV examination, 71.5% (n = 153) of the sample had at least one psychiatric comorbidity, with the mean number of comorbid psychiatric diagnoses being 1.45 ± 1.6.
When comparing individuals first diagnosed with ADHD in childhood/adolescence (diagnosed at < age 18 years) versus adulthood (diagnosed at ≥ age 18 years), several differences emerged, as presented in Table 2. Those diagnosed in adulthood were characterized by older age (t = 5.90, p < .001) and higher education levels (t = 4.72, p < .001), both with intermediate effect sizes (0.71 and 0.68, respectively). They also exhibited greater ADHD symptoms in both inattention (ASRS subscale A; t = 2.69, p = .008) and hyperactivity/impulsivity (ASRS subscale B; t = 2.50, p = .014), elevated MD scores (t = 2.34, p = .020), and a lower rate of current medication use for ADHD (χ² = 49.832, p < .001). Small effect sizes were reported for these differences (0.39, 0.39, 0.34, and 0.21, respectively) compared to those diagnosed in childhood/adolescence. However, there were no differences between the two groups in terms of gender, ADHD subtype, psychiatric comorbidity rate, global assessment of functioning scores, or self-reported symptom severity of depression, anxiety, childhood trauma, dissociative experiences, excessive mind wandering, and retrospectively reported childhood ADHD symptoms (assessed via the WURS).
Comparison of Demographic, Clinical, Diagnostic, and Self-report Measurements Data Between Groups.
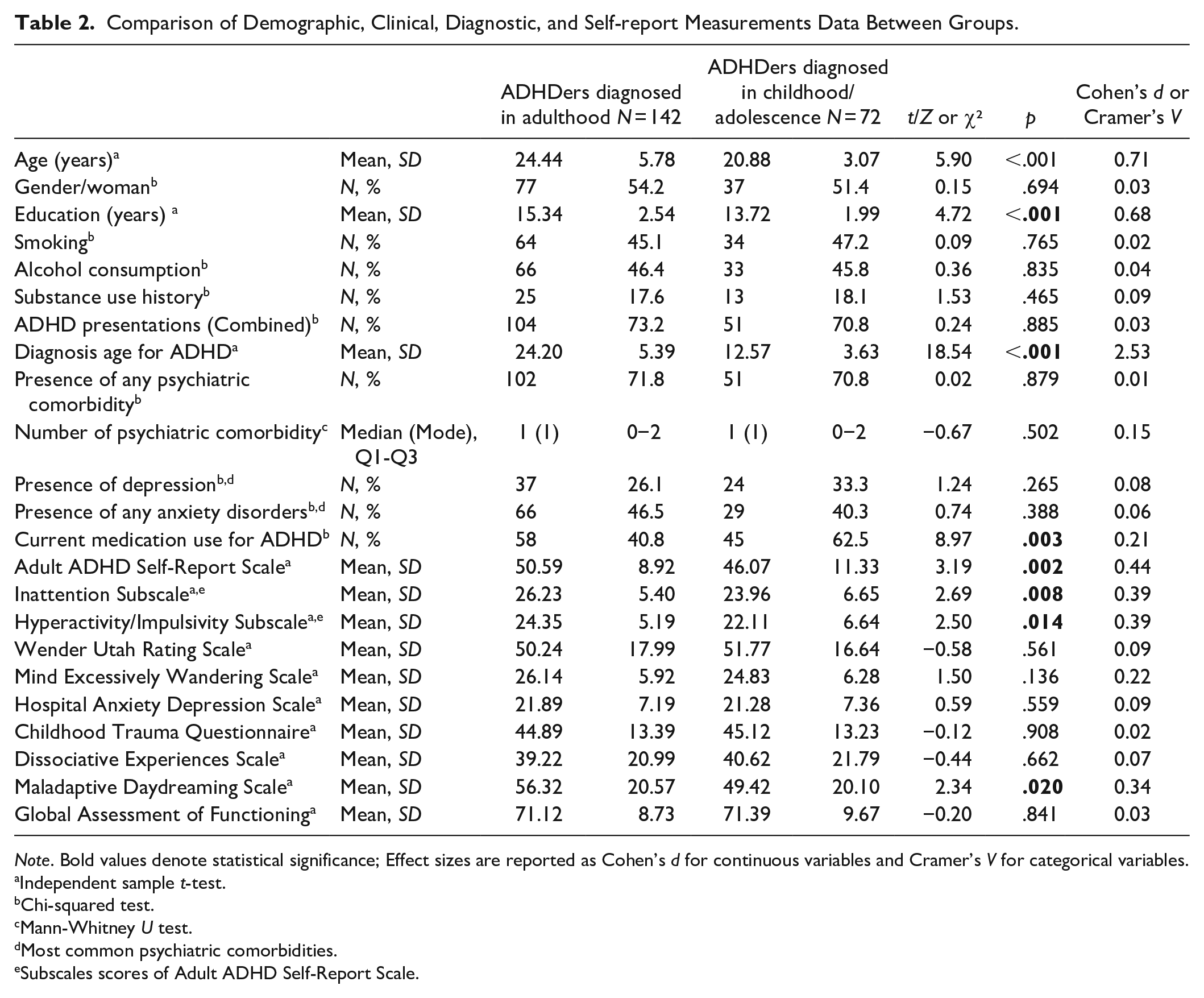
Note. Bold values denote statistical significance; Effect sizes are reported as Cohen’s d for continuous variables and Cramer’s V for categorical variables.
Independent sample t-test.
Chi-squared test.
Mann-Whitney U test.
Most common psychiatric comorbidities.
Subscales scores of Adult ADHD Self-Report Scale.
The backward (likelihood ratio) logistic regression model was used to identify the best predictors of first being diagnosed with ADHD in adulthood. The significant parameters from bivariate analyses included as independent variables in the model were age, gender (male/female), years of education, current medication use for ADHD (yes/no), inattention and hyperactivity/impulsivity subscores of the ASRS, and MDS scores.
The findings of the final step of a 4-step backward model, as presented in Table 3, indicated that older age at present (Odds = 1.172; p = .005; 95% confidence interval [1.050, 1.308]), higher years of education (Odds = 1.207; p = .005; 95% confidence interval [1.023, 1.425]), presence of current medication use for ADHD (Odds = 0.398; p = .005; 95% confidence interval [0.208, 0.762]), and increased severity of MD (Odds = 1.012; p = .022; 95% confidence interval [1.002, 1.022]) were associated with delayed diagnosis of ADHD until adulthood. The model showed a preferable significance value of .146 for the goodness-of-fit test in the Hosmer-Lemeshow test and explained between 19.9% (Cox and Snell R2) and 27.5% (Nagelkerke R2) of the variance in being first diagnosed with ADHD in adulthood, correctly classifying 75.5% of cases overall.
Logistic Regression Analysis for Predictors of First Being Diagnosed With ADHD in Adulthood.
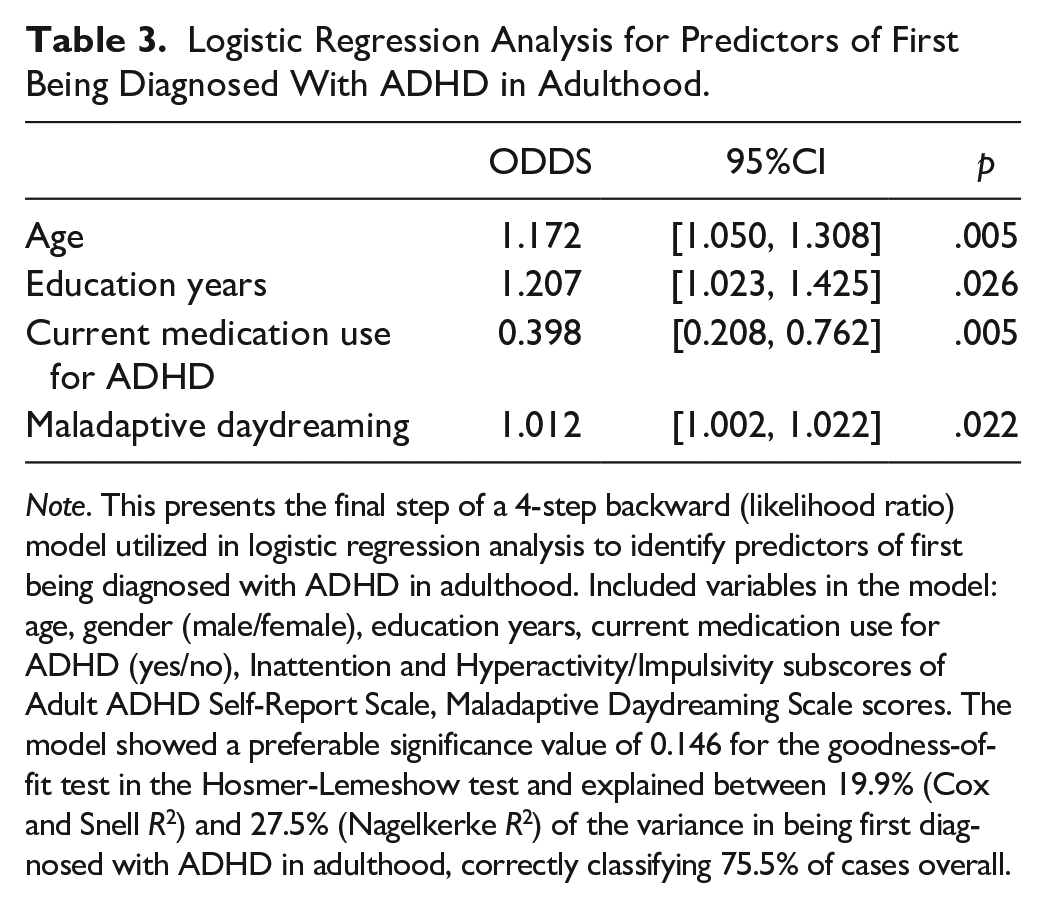
Note. This presents the final step of a 4-step backward (likelihood ratio) model utilized in logistic regression analysis to identify predictors of first being diagnosed with ADHD in adulthood. Included variables in the model: age, gender (male/female), education years, current medication use for ADHD (yes/no), Inattention and Hyperactivity/Impulsivity subscores of Adult ADHD Self-Report Scale, Maladaptive Daydreaming Scale scores. The model showed a preferable significance value of 0.146 for the goodness-of-fit test in the Hosmer-Lemeshow test and explained between 19.9% (Cox and Snell R2) and 27.5% (Nagelkerke R2) of the variance in being first diagnosed with ADHD in adulthood, correctly classifying 75.5% of cases overall.
To test whether MD scores were a potential predictor of ADHD symptoms, two separate linear regression analyses were conducted for both groups, controlling for age, gender, years of education, presence of comorbid psychiatric disorder, current medication use for ADHD and anxiety/depression scores. Both models yielded significant F values with p < .05. The findings indicated that increased MD scores predicted more severe ADHD symptoms in those diagnosed in adulthood (t = 4.04, p < .001, 95% confidence interval [0.048, 0.140]), but not in those diagnosed in childhood/adolescence (t = 1.33, p = .188). Partial regression plots, as shown in Figure 1, were used to illustrate the relationship between MD severity and ADHD symptoms, excluding the effects of covariates, in both groups. In addition, multicollinearity was evaluated in linear regression analysis, and the fact that “VIF” values (1.07–1.09, min–max) are <5 and “tolerance” values (0.51–0.93, min–max) are not >5 and not less than 0.2 indicates that there is no multicollinearity that may adversely affect the power of the regression model (Kim, 2019).
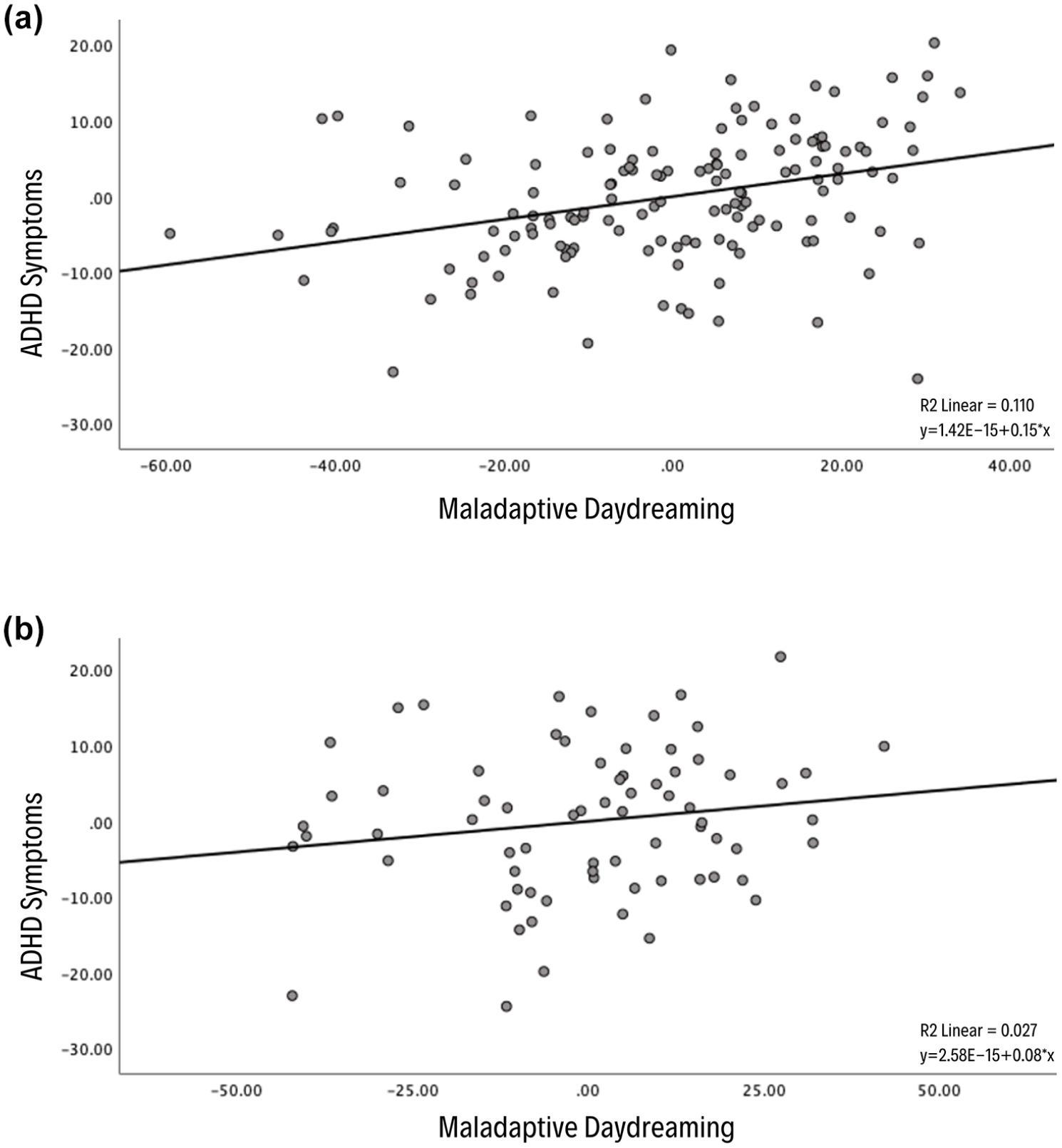
Partial regression plots were used to illustrate the relationship between maladaptive daydreaming severity and ADHD symptoms excluding the effects of covariates such as age, gender, years of education, presence of comorbid psychiatric disorder, current medication use for ADHD and anxiety/depression scores in adults with ADHD diagnosed in both adulthood (a) and childhood/adolescence (b). Accordingly, in adults first diagnosed with ADHD in adulthood, maladaptive daydreaming severity significantly predicted ADHD symptoms (R² = .110, t = 4.04, p < .001), whereas no such prediction was observed in those first diagnosed in childhood/adolescence (R² = .027, t = 1.33, p = .188).
Finally, examining the correlation of MD scores with other clinical measures in both groups revealed that MD severity exhibited stronger positive correlations with current and childhood ADHD symptoms, the number of comorbid psychiatric disorders, and self-reported comorbid symptoms in adults first diagnosed with ADHD in adulthood compared to those first diagnosed in childhood/adolescence. The findings of the correlation analysis are presented in Table 4.
Coefficients of Correlations of Maladaptive Daydreaming With Other Clinical Measures for Each Group.
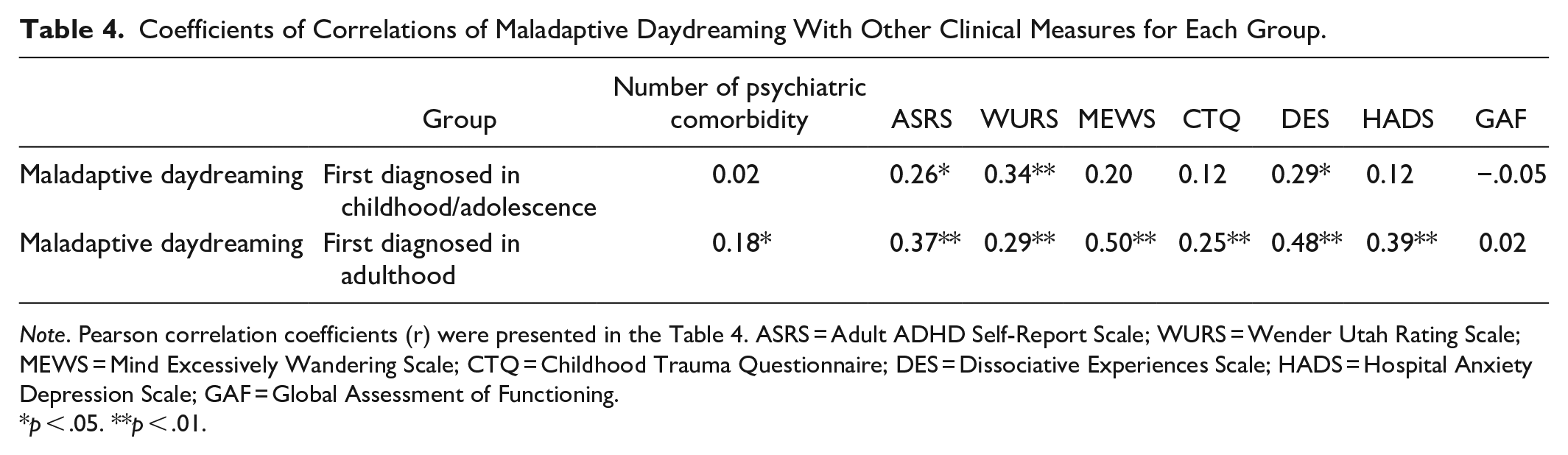
Note. Pearson correlation coefficients (r) were presented in the Table 4. ASRS = Adult ADHD Self-Report Scale; WURS = Wender Utah Rating Scale; MEWS = Mind Excessively Wandering Scale; CTQ = Childhood Trauma Questionnaire; DES = Dissociative Experiences Scale; HADS = Hospital Anxiety Depression Scale; GAF = Global Assessment of Functioning.
p < .05. **p < .01.
Discussion
This study aimed to address the issue of delayed or missed ADHD diagnoses until adulthood. We divided 214 adults with ADHD into two groups based on the age of first diagnosis: childhood/adolescence and adulthood. Bivariate and regression analyses revealed that older age, higher education levels, lower current ADHD medication use, and higher MD severity were associated with being first diagnosed with ADHD in adulthood. MD was positively associated with ADHD symptom severity in those first diagnosed with ADHD in adulthood but not in those diagnosed in childhood/adolescence. Finally, MD showed a stronger positive correlation with number of comorbid psychiatric disorders, ADHD- and comorbidity-related symptoms in those first diagnosed with ADHD in adulthood compared to those diagnosed in childhood/adolescence.
In our study, adults diagnosed with ADHD for the first time were older, had higher education levels, and exhibited higher rates of current ADHD medication use compared to those diagnosed in childhood or adolescence. This difference is most likely attributable to the age of presentation to the clinic. Individuals diagnosed in childhood or adolescence often transition to adult ADHD services in early adulthood, typically through referrals from child and adolescent psychiatrists. In contrast, those without a prior diagnosis may present at any stage of adulthood for a variety of reasons. Moreover, earlier presentations are commonly associated with fewer years of education (e.g., high school graduates or early university students), whereas later presentations are often linked to higher levels of education (e.g., university graduates or those pursuing postgraduate studies).
Unsurprisingly, individuals diagnosed with ADHD in childhood or adolescence reported a higher rate of ADHD medication use and lower symptom severity compared to those diagnosed in adulthood. Notably, when these parameters were included as covariates in further analyses, the relationship between ADHD symptoms and being diagnosed in adulthood did not persist. Nevertheless, we should acknowledge the limitation of including only cross-sectional data on medication use (yes/no) without accounting for the duration of ADHD treatment, which may have influenced our findings.
In the study sample, the proportion of women and men was nearly equal, and this balance persisted when the sample was divided by the timing of ADHD diagnosis (childhood/adolescence vs. adulthood). Although it is commonly believed that females with ADHD are diagnosed later than males, stronger evidence supports this for childhood cases (Kooij et al., 2019). A recent Swedish population study of approximately 85,000 adults with ADHD found that females were diagnosed and treated about 4 years later than males. However, this study considered at least one ADHD diagnosis (F90 according to ICD-10) or a single prescription for ADHD medication as a diagnosis, which may not exclude false positives despite Sweden’s high treatment thresholds (Skoglund et al., 2024). Consensus reports and expert opinions suggest that diagnosing ADHD in adults typically requires a process lasting 2 to 3 hr over multiple visits (Adamou et al., 2024). In our clinic, the diagnostic process involves at least two sessions. As a tertiary university hospital serving a large population, our sample likely includes individuals with more severe and complex symptoms compared to community-based studies. Another clinical study of 150 adults with ADHD found no difference between the sexes in the “duration of untreated illness,” indicating that clinical and community-based studies might show differences in age of diagnosis between males and females (Oliva et al., 2021).
When comparing the severity of ADHD- and comorbidity-related symptoms, no significant differences were found between the two groups, except for current ADHD symptoms, and MD severity. Afterwards, when current ADHD medication use was considered in further analyses, this difference in current ADHD symptoms lost statistical significance. This finding supports the neurodevelopmental nature of ADHD, which typically begins in childhood and persists into adulthood. In one of his final studies, the world-renowned ADHD researcher Joseph Biederman (whom we commemorate with admiration and respect) questioned whether ADHD characteristics differ between adults diagnosed in childhood/adolescence and those diagnosed in adulthood. The authors briefly answered in their paper that “they do not,” as they found similar clinical variables in both groups (Hutt Vater et al., 2024). However, MD severity emerged as an exception, serving as a predictor of both being diagnosed in adulthood and the severity of ADHD within this group.
The correlation between MD and dissociative experiences across the whole sample supports the view of researchers who propose MD as a dissociative pattern, yet distinct enough to warrant its separate diagnosis (Soffer-Dudek & Somer, 2022). However, dissociative experiences did not vary based on the age at which ADHD was diagnosed, while MD was specifically associated with being diagnosed with ADHD in adulthood. Another widely accepted notion is that the predominantly inattentive presentation of ADHD may receive a late diagnosis (Faraone et al., 2024). In the first comorbidity report related to MD, a strikingly high rate of 69% of individuals with MD was found to have predominantly inattentive ADHD (Somer et al., 2017). However, our findings did not reveal any differences in ADHD presentations or ADHD symptom severity based on the age of diagnosis, after controlling for confounding factors. This suggests that the primary factor delaying ADHD diagnosis may not be inattention symptoms but rather MD symptoms, potentially leading to an overdiagnosis of ADHD in this study. Our findings indicate that MD, likely due to its unique characteristics, is associated with late diagnosis of ADHD, independent of ADHD presentations and dissociative experiences.
The first of our two possible explanations for how MD severity may delay ADHD diagnosis until adulthood is that MD is an often-overlooked clinical phenomenon where individuals engage in organized daydreaming for extended periods, leading to a diminished connection with the real world. While this provides relief from negative emotions, it can lead to functional impairment due to the compulsive pattern of such a behavioral addiction (Bigelsen et al., 2016). MD may serve as a compensatory mechanism for ADHD symptoms through features such as temporary emotion regulation, hypoactivity, and sustained focus on a single mental process without interruption. Another supporting explanation is that comorbid diagnoses often mask ADHD symptoms, yet these comorbid diagnoses (e.g., anxiety disorders, depression, and substance use disorders) typically prompt individuals to seek mental health services (Ginsberg et al., 2014). In the case of MD, despite its disruptive impact on functionality, the individual’s immersion in their inner world and lack of externalizing symptoms make it challenging for both individuals and those around them to recognize MD as a disorder, potentially delaying the pursuit of mental health support.
While this study provides valuable insights, it has several limitations. As a cross-sectional study conducted at a single center, the findings may not be broadly generalizable and are subject to retrospective recall bias. The use of self-report scales provides more subjective data compared to objective diagnostic tools. Although current ADHD medication use was included in the analyses, the duration of medication use and the specific pharmacotherapeutic agents used for ADHD throughout the course of the disorder were not accounted for, potentially influencing the difficulties reported by participants. The relatively young age range of our sample, with a mean age of 23 years, limits the generalizability of our findings to older adults with ADHD. Future research should aim to include a broader age range to explore whether the observed patterns persist across different stages of adulthood.
In conclusion, MD is a strong predictor of delayed ADHD diagnosis until adulthood. It may contribute to this delay by both masking and compensating for ADHD symptoms. Additionally, MD was (1) associated with the severity of ADHD symptoms and (2) more strongly correlated with the number of comorbid psychiatric disorders and both ADHD- and comorbidity-related symptoms in adults diagnosed in adulthood compared to those diagnosed in childhood/adolescence. These findings suggest that MD should be considered in structured diagnostic interviews for ADHD in adulthood, as it may strengthen the diagnosis of ADHD. However, these findings need to be supported by longitudinal clinical studies.
Footnotes
Acknowledgements
This study was presented by the first author, Ali Kandeğer, at the European College of Neuropsychopharmacology (ECNP) Congress 2024, where it was honored with one of the “Excellence Awards” for poster presentations.
Author Contributions
AK: Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology, Supervision, Project Administration, and Writing—Original Draft Preparation. HAG: Conceptualization, Formal Analysis, Validation, and Writing—Original Draft Preparation. MSÖ: Data Curation, Formal Analysis, Investigation, Methodology, Resources, and Software. ÖB: Data Curation, Investigation, Resources. HS: Data Curation, Investigation, and Resources. EY: Data Curation, Investigation, Resources. BS: Supervision, and Writing—Review & Editing.
Data Availability Statement
The data available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved by the Local Ethics Committee of Selçuk University (Decision Number: 2022/113).