
Abstract
Objectives:
Children with ADHD obtain lower scores than their peers on standardized language measures but less is known about their conversational language skills. We tested the ability of children with and without ADHD to monitor and repair their language during a conversation (social discourse) with a young adult.
Methods:
Forty-nine 9- to 14-year-old children previously diagnosed with ADHD (17 in partial remission) and an age and sex-matched sample of typically developing (TD) children engaged in a conversation with a young adult. Their conversations were recorded, transcribed, and coded for structural and pragmatic language use. Language error and correction rates were compared across the two groups, for the whole sample and for those meeting full criteria for ADHD.
Results:
The ADHD group made significantly more structural language errors, specifically morphosyntactic mistakes and word repetitions. In their pragmatic language use, children with ADHD were more likely to make unrelated utterances and were less successful in repairing dysfluent responses. The adult conversational partners made more attempts to keep TD participants engaged in conversation and rated them as more likable.
Conclusions:
Subtle differences were identified in the structural and pragmatic language use of children with and without ADHD during social discourse. Conversation partners were more engaged in their interactions with TD children and appeared to experience these interactions more positively. The language skills of children with ADHD, including their conversation skills, should be monitored and considered as targets for intervention.
Introduction
ADHD is a common neurodevelopmental disorder characterized by elevated levels of inattention, hyperactivity, and impulsivity that negatively impact daily functioning (American Psychiatric Association, 2022). In addition to these core symptoms, children with ADHD evidence poorer spoken language skills than typically developing (TD) children. The risk of oral language impairments in children with ADHD is approximately three times that of their non-affected peers (Sciberras et al., 2014). Children with ADHD are also at increased risk for disorders that impact social communication (e.g., autism and social pragmatic communication disorder; Carruthers et al., 2022; Green et al., 2014; Redmond, 2020; Sciberras et al., 2014; Tannock, 2018). Empirical studies have shown that children with ADHD obtain lower scores on standardized language measures (e.g., Green et al., 2014; Korrel et al., 2017), evidence poorer narrative (storytelling) skills (e.g., Carruthers et al., 2022; Jepsen et al., 2022), and weaknesses in their use of language in social interactions (e.g., Carruthers et al., 2022; Green et al., 2014) compared with their typically developing (TD) peers. However, little attention has been paid to the language use of children with ADHD in a social context (i.e., real-time interactions). The range of elements included in studies of their discourse is narrow and research to date has not addressed their ability to monitor and repair their language. In the current study we address these limitations through the in-depth analysis of the conversation skills of children with and without ADHD. This includes attention to grammar and semantic errors, dysfluencies, coherence and clarity of utterances, off-topic utterances, and the children’s ability to detect and correct communication breakdowns.
Comparing the performance of children with and without ADHD on standardized language measures, Korrel et al. (2017) identified large group differences in receptive and expressive structural language (the building blocks of language) 1 as well as pragmatic language (social use of language), 2 favoring TD children. Both Carruthers et al. (2022) and Green et al. (2014) reported children with ADHD receive lower ratings than their TD peers on several subscales of the Children’s Communication Checklist (CCC, most commonly on the coherence, inappropriate initiation, stereotyped language, use of context, and nonverbal communication subscales). These results were mirrored in the meta-analysis by Kessler and Ikuta (2023). Carruthers et al. (2022) also note children with ADHD experience more difficulty understanding irony, sarcasm, faux pas, and presupposition. A recent scoping review by Parks et al. (2023) compared the language skills of children and adolescents with ADHD and those with developmental language disorders (DLD) 3 on standardized language measures. They report children with ADHD experience fewer language difficulties than those with DLD. Specifically, better morphosyntax/grammar, core language, and receptive and expressive abilities, but similar performance on tasks measuring semantics, pragmatic, and figurative language. In general, children with ADHD obtain lower scores than their TD peers on standardized measures of structural and pragmatic language. They demonstrate better structural language skills than children with DLD but comparable pragmatic language skills. The results from standardized language measures, while valuable, do not provide information on how children with ADHD use language during discourse, including in a conversational context.
Reviews of the narrative discourse skills of children with and without ADHD indicate the stories of those with ADHD are less coherent and informative, less syntactically complex, and include more ambiguous references and disruptive errors (Carruthers et al., 2022; Green et al., 2014; Jepsen et al., 2022). Carruthers et al. (2022) and Green et al. (2014) also reviewed studies comparing language use during social discourse (conversation). Green et al. (2014) reported that children with ADHD exhibit poorer topic maintenance and listener adaptation, disorganized speech, and trouble with conversational turn-taking compared with TD children. In their review, Carruthers et al. (2022) reported children with ADHD struggled with conversational reciprocity, perspective-taking appropriate emotional expression, and included more off-topic remarks, compared with their TD peers. The available studies identify several differences in the discourse skills of children with and without ADHD. However, the small number of language elements included in each study limits cross study comparisons and the building of a comprehensive profile of language use during social discourse for children with ADHD.
Successful social discourse requires flexibility in the use of grammar, understanding and production of semantic relationships, and presupposition skills including recognition of shared information and interpretation of contextual cues (R. Landa, 2000). It also requires intact monitoring skills to facilitate topic management (topic initiation, maintenance, and termination) and conversational repair after a communication failure, all while maintaining speech coherence. These monitoring and repair abilities apply at the word, sentence (e.g., grammar or sematic mistakes and dysfluency in speech), turn, and communication cycle (e.g., misunderstanding and failure in reciprocity) levels (R. Landa, 2000; Levelt, 1983; Schegloff et al., 1977). To date a limited number of studies have specifically addressed the conversation skills of children with ADHD and vary in their focus, methodology and coding practices. Most available studies were published more than 10 years ago.
Amongst observational studies focusing on structural language, a number have assessed the presence of speech dysfluencies in the discourse (narrative or social) of children with ADHD. These dysfluencies are sometimes referred to as linguistic “mazes” and are defined as “a series of words (or initial parts of words), or unattached, fragments which do not constitute a communication unit, and are not necessary to the communication unit” (Loban, 1976, p. 22). Such dysfluencies may be affected by internal processes of self-monitoring (Levelt, 1983; Schegloff et al., 1977). Commonly identified dysfluencies include word or sound repetitions, pauses, filled pauses (e.g., “um”), and self-disruptions mid-sentence, for example, stopping or starting a word or sentence, before correcting or starting over (DeJoy & Gregory, 1985; Fiestas et al., 2005).
Redmond (2004) compared the presence of common dysfluencies in the conversations of children with and without ADHD. Those with ADHD produced significantly more dysfluencies than their TD peers; rates of different dysfluency types were not reported or compared. In a study of speech and vocalization patterns, Breznitz (2003) reported boys with ADHD paused more frequently when responding to interview questions than control group participants. In a recent study Boo et al. (2022) investigated filled pauses in conversation during a virtual task and found that TD children produced more filled pauses than ADHD children. In narrative speech (storytelling) studies, Kuijper et al. (2017) reported the responses of children with ADHD included more repetitions than their TD peers, while the speech of the latter included more pauses. In another study, Lee et al. (2017) reported the speech of children with ADHD included a higher overall rate of dysfluencies than control participants. Conversely, Zentall (1988) reported the total repetitions and revisions (self-interruptions) of TD children were higher than those of children with ADHD.
A less studied element of the discourse of children with ADHD is the integrity of their use of semantics (i.e., accurate use of target words) and morphosyntax (grammar). Very little attention has been paid to these aspects of language in the free speech of children with ADHD, with most studies relying on standardized tests (see Korrel et al., 2017). Kuijper et al. (2017) did assess for morphosyntactic mistakes in children’s narratives and reported children with ADHD made more grammatical errors than their TD peers. No studies were found that compared semantic mistakes between children with and without ADHD during social discourse.
Topic maintenance and speech coherence are important aspects of pragmatic language required for successful discourse. There is some evidence that children with ADHD make more off topic utterances than their peers. Employing a simulated “chat room,” in which children typed their responses, Mikami et al. (2007) found children with ADHD made more off-topic comments than their TD peers. Zentall et al. (1983) recorded children’s verbalizations during a listening task, reporting children with ADHD produced more off-task responses than TD children. Freer et al. (2011) and Lorch et al. (2010) investigated children’s speech coherence through storytelling tasks. They reported children with ADHD produced less coherent stories than their TD peers.
Successful social discourse also requires that participants monitor one another’s verbal and nonverbal behavior, adapting their responses to maintain the communication cycle. To date, only one study has investigated participant responses (separately) in conversations between children with and without ADHD and an adult conversation partner. Stroes et al. (2003) found the adult took more verbal initiative (e.g., asked questions and praised/encouraged the child) with TD children than those with ADHD. They also reported the TD children displayed more verbal reciprocity. Consistent with these findings, greater overall verbal reciprocity is noted in the interactions of pairs of TD children than in mixed dyads, that is, TD and ADHD children together (Clark et al., 1988; Hubbard & Newcomb, 1991).
The identified language difficulties of children with ADHD have implications for their current and future functioning. Language skills correlate with academic achievement in both TD children (Duff et al., 2015; Ouellette & Beers, 2010) and those with ADHD (Carrasco et al., 2022; Cohen et al., 2000; Gremillion & Martel, 2012; Jepsen et al., 2024; Sciberras et al., 2014). Structural and pragmatic language skills have been linked to children’s social functioning in the general population (Cochet & Byrne, 2016; Hebert-Myers et al., 2006) and in children with ADHD (Çiray et al., 2022; Hubbard & Newcomb, 1991; Jepsen et al., 2024; Leonard et al., 2011). This association may explain some of the reported social difficulties of children with ADHD, including increased peer rejection and reduced number of friends (Ros & Graziano, 2018; Spender et al., 2023).
Several hypotheses have been proposed to account for the nature and frequency of language difficulties observed in children with ADHD: (1) That the symptoms of ADHD disrupt early language acquisition, interfere with effective communication that is, some ADHD symptoms overlap with SPCD, and reduce opportunities to practice language skills (Camarata & Gibson, 1999; Hawkins et al., 2016). (2) That ADHD and language difficulties share a common etiology. Children with ADHD are at increased risk for language impairment (Scriberras et al., 2014), Autism (Antshel et al., 2016), and SPCD (Redmond, 2020) suggesting overlapping causes; and (3) That the executive function deficits, seen in many children with ADHD, underlie, or contribute to, reduced language proficiency. Working memory is involved in language processing and production through temporary storage and manipulation of linguistic information, during comprehension, sentence formulation, and integration of information (Baddeley, 2003, 2012). Inhibitory control facilitates accurate grammatical and lexical selection, word retrieval, and suppression of irrelevant information (Gandolfi & Viterbori, 2020; Ibbotson & Kearvell-White, 2015; Kaushanskaya et al., 2017; Mirman & Britt, 2014). Cognitive flexibility may also contribute to understanding ambiguous communication and considering other’s perspectives (Blain-Brière et al., 2014). The contribution of these factors to the language difficulties of children with ADHD requires additional research.
The available research suggests the language skills of children with ADHD are less well developed than their TD peers, but generally better than those of children with DLD. However, it is not currently possible to build a comprehensive profile of the social discourse skills of children with ADHD from the existing literature. The current study addresses the need for additional research on the conversational skills of children with ADHD. Here we compare the occurrence, monitoring, and repair of structural (i.e., mistakes and dysfluencies) and pragmatic language (i.e., utterance coherence, clarity, and relevance to conversation topic) during social discourse in children with, or demonstrating symptoms of, ADHD and a matched TD group. Both groups engaged in a conversation with a young adult conversation partner, blind to their group membership. These conversations were recorded, transcribed, and subsequently coded for a broad range of structural and pragmatic language elements in the children’s speech. The conversation partner’s efforts to engage the child (e.g., turns that include questions, praise, and elaborations on a certain topic) were coded together with the child’s response to such efforts. Speech quantity (words and turns) was recorded for the children and their conversation partner. We also examine the conversation partner’s perceived interaction experience through their ratings of child likeability and conversation effortfulness, factors that may contribute to the child’s peer status and friendships in their daily lives.
Based on the existing literature, children with ADHD are hypothesized to make more structural language errors, to produce less coherent speech and make more off topic utterances, that is, poorer monitoring and repair. Conversation partners are expected to make more effort to engage TD children (see Stroes et al., 2003), while children in the ADHD group are expected to show less reciprocity to such efforts, given their anticipated poorer attention and pragmatic skills. While excessive talking is a symptom of ADHD, the available literature does not support greater speech quantity in children with ADHD (Boo et al., 2022; Kuijper et al., 2017; Redmond, 2004) while information on the speech quantity of conversation partners of children with ADHD is not available. As a result, no predictions are made regarding speech quantity for the children or their conversation partners. Given the known social difficulties of children with ADHD we hypothesize their conversation partners will perceive them as less likeable and more effortful to interact with than TD children.
Method
Participants
Data from 9- to 14-year-old children, 49 previously diagnosed with ADHD (boys n = 41), and 49 typically developing (TD) children matched for age (+3 months) and assigned sex, are included in the study (see Table 1 for demographic information). Children in the ADHD group were initially diagnosed between the ages of 5 years 6 months and 10 years 11 months through multi-method multi-informant assessments in a university research clinic (see Supplemental Methods for details). They were invited back 4 years (+ 4 months) later to participate in the current study, 4 aged 9 to 14 years. All children in the ADHD group continued to demonstrate symptoms of ADHD, with 32 (65.3%) meeting full criteria for the disorder. The TD children were recruited through letters of invitation distributed by local schools at the time of the current study. The parents and teachers of all children were asked to participate by completing behavioral questionnaires and interviews about the children’s current behavioral and social functioning.
Demographic Characteristics of the ADHD and Typically Developing (TD) Groups.

Symptom severity derived from the Disruptive Behavior Disorders Rating Scale (DBD, Molina et al., 1998).
n = 48. Data missing for one pair.
Socio-economic status (SES) based on Elley and Irving’s (1985) occupational codes. 1 = professional/technical; 2 = trades; and 3 = semiskilled/unskilled/unemployed.
Inclusion criteria for the ADHD group were a previous diagnosis of ADHD and no current or previous evidence of neurological disorder, including head injury, or psychosis and a Full Scale IQ of at least 70. At the time of the current study, 33 children were prescribed methylphenidate for symptom management. Medication use was suspended for at least 24 hr before participating in the current study. Inclusion criteria for the TD group participants were the same except for the presence of a current or previous diagnosis of ADHD, oppositional defiant disorder (ODD), or conduct disorder (CD), or other significant behavioral difficulties as reported by parents during an initial screening interview. None of the children, in either group, participated in a formal language assessment as part of the current study, the presence of language difficulties was not an exclusion criteria (see Supplemental Table S1 for available information on the children’s language skills).
Three post-graduate psychology students (two male and one female) served as conversation partners for the children during the study.
Procedure
Ethical approval for the study was obtained from the Otago University Ethics Committee. Parents, teachers, and children provided written consent to take part.
All the children participated in an abbreviated diagnostic assessment. Parents and teachers were asked to complete the Disruptive Behavior Disorders Rating Scale (DBD; Molina et al., 1998) to assess for symptoms of DSM-IV ADHD and the Child Behavior Checklist (CBCL; Achenbach, 1991a) or Teacher Report Form (TRF; Achenbach, 1991b) to screen for behavioral and emotional difficulties. Parents (face-to-face) and teachers (telephone) completed semi-structured interviews (developed for the study) about the children’s current social, academic, and behavioral functioning and the children were interviewed about their friends, hobbies, and school performance. The children also completed a cognitive assessment including the Wechsler Intelligence Scale for Children third edition (WISC-III, Wechsler, 1991). Data from the interviews, the DBD, and observations of the child during the cognitive assessment, were used to determine if those in the ADHD group continued to meet the DSM-IV criteria for a diagnosis of ADHD. Those displaying fewer than six symptoms in at least one setting (home or school) or whose symptoms were present in only one setting were recorded as having ADHD in partial remission. Symptoms were not summed across informants. Observed symptoms during the cognitive assessment were counted toward the presence of symptoms across settings. All children in the ADHD group continued to display some symptoms of ADHD.
The children engaged in a 15-min conversation with a young adult conversation partner of the same sex while playing a game of Tumbling Tower (Jenga). This game begins with a tower of wooden blocks, arranged in layers of three blocks whose direction alternates between levels. Players take turns moving one block at a time from the body of the structure and placing it on top of the tower. As the game progresses, the tower becomes less stable. The winner is the last player who successfully plays a turn without collapsing the tower. The game is typically played with two to six players competing against one another.
The conversation partners were asked to maintain the conversation and encourage the child to speak. They were given a set of four possible conversation topics (movies, music, sports, and hobbies) to initiate conversation, together with advice that the conversation need not be restricted to these topics. They were also asked to negotiate up to two game rule changes with the children to encourage conversation. 5 Following each conversation, the adult was asked to rate how likeable they found the child and how effortful they found the conversation using 5-point Likert scales. The conversations were recorded and later transcribed verbatim. The transcripts, but not the original recordings, were available for the current study.
The conversation partners participated in a 1-hr training session to familiarize them with the task protocol, the game, setting, and recording equipment and to practice playing the game. They were informed they would be playing a game and conversing with children aged 9 to 15 years and that the task was designed to measure the children’s conversational skills. They were not informed of the research questions or hypotheses and were blind to the children’s group membership/diagnostic status. The female conversation partner interacted with all female children. The same male conversation partner interacted with 74 (90%) of the participating boys. A second male participated in eight conversations (10%) when the primary male conversation partner was unavailable. Same sex conversation partners were used as research shows most children’s peer relationships tend to be of the same sex (Serbin et al., 1994 cited in Underwood, 2004).
The transcribed conversations were coded by two trained raters blind to the children’s age, sex, and group membership. One rater coded all 98 transcripts, the second rater 25 (25.5%) transcripts selected at random, to assess inter-rater reliability. Only the last 10 min of each transcribed conversation were coded. During the first 5-min, the children were receiving instructions for the game and were becoming familiar with the setting and the adult conversation partner.
Coding Scheme
A coding scheme and detailed coding manual were developed for the current study. This included structural and pragmatic language codes developed with reference to the existing literature on language use in children with ADHD (e.g., Bangert & Finestack, 2020; Kuijper et al., 2017; Redmond, 2004; Stroes et al., 2003) and monitoring and repair in discourse generally (e.g., Levelt, 1983; Schegloff et al., 1977).
Structural language variables included word and sentence level elements, that is, semantic and morphosyntactic errors, repair of these errors 6 by the child and adult language partner, and speech dysfluencies at the single word level (self-interruptions, pauses, repetitions, and filled pauses). 7 Pragmatic language variables operated at the turn and communication cycle level. These included: minimal turns (in which children used a minimal number of words when they had an opportunity to expand on a topic), off topic utterances, dysfluent turns (turns containing at least one speech dysfluency) which are measured on the turn level, repair of dysfluencies (coherence and clarity of turns containing dysfluencies), and the adult’s efforts to engage the child and the child’s subsequent responses. The coding scheme and coding manual are presented in the Supplemental Methods.
Coder Training and Transcript Coding
The two coders participated in four training sessions. These sessions included (1) a review of the coding manual and guidelines and their application to a transcript; (2) practice coding of a transcript using the guidelines; (3) independent coding of two transcripts followed by a discussion of any disagreements; and (4) independent coding of a further two transcripts followed by checking of agreement and consistency. The practice transcripts were additional to the 98 included in the study.
Following training the two raters coded the transcripts in five sets of approximately 20. For each set, the primary rater coded all transcripts and the reliability coder 5 selected at random from the set. Coding of each set of transcripts occurred over the same time-period. After each set of transcripts was coded the raters met to review reliability and check for coder drift. Coder reliability was calculated with Krippendorff’s alpha for the frequency of the conversation variables (see Supplemental Table S2). Reliability was satisfactory with coefficients ranging from .75 (minimal utterances) to .99 (filled pauses). Interclass correlation coefficients were calculated to assess reliability of ratings of coherence and clarity in turns with dysfluencies. These coefficients were .67 and .69, respectively.
Data Preparation
For the structural language variables all counts were converted to rates per 100 words (i.e., number of occurrences per 100 words). For pragmatic language variables a similar procedure was followed, in this case occurrences per 100 turns. The data were converted to rates to control for individual differences in the quantity of speech generated across participants. This approach is common in the analysis of language variables (Arslan et al., 2023; Fiestas et al., 2005; Balčiūnienė & Kornev, 2024; Leadholm & Miller, 1992; Loban, 1976; Redmond, 2004; Zwitserlood et al., 2015). The distributions for all variables were checked for skewness, kurtosis, and presence of extreme outliers. Data was transformed with a log transformation as necessary. Where data transformation did not improve the distributions, the untransformed rates were used in the analyses. Figures presenting the untransformed distributions for the key child language variables are presented in the Supplemental materials (See Figures 1–4).
Data Analytic Plan
For speech quantity, the word and turn (utterances) counts were compared across groups separately for the children and the adult conversation partners using two-tailed paired t-tests.
For the structural language variables, the groups were compared on the log transformed rates of grammar mistakes, self-interruptions, repetitions, and filled pauses. As the ADHD and control groups were matched for age and sex, paired t-tests were used to compare groups. These were one-tailed where the direction of difference was predicted, otherwise tests were two tailed. For correction of mistakes, only data from those subjects who made mistakes was included. Chi square was used to compare the proportions of children and adults who corrected all, some, or none of their mistakes across the two groups. 8 The number of semantic mistakes and pauses was low for both groups and no formal analysis was undertaken for these variables.
For the pragmatic language variables, paired t-tests were performed on the untransformed proportion of dysfluent and minimal turns. For identified dysfluent turns, the proportion of coherent and/or clear turns was compared using a one-tailed independent t-test. Paired t-tests were performed on the log transformed proportion of adult turns involving effort, and on the raw proportions of reciprocated (by child) efforts. As few children engaged in unrelated turns Chi square was used to compare the proportion showing none or at least one unrelated turn across the groups. The adult’s ratings of child likeability and the effortfulness of conversing with the child were compared using paired t-tests.
We also undertook a series of exploratory analyses. The above analyses were repeated with the 32 participants who continued to meet full criteria for ADHD and their matched controls. The association between children’s ADHD symptom severity (sum of item scores) and the conversation variables were assessed with Pearson correlations. Finally, we correlated the adult’s ratings (child likability and effortfulness of the conversation) with the children’s conversation variables.
Prior to any group comparisons, participants Full Scale IQ scores were correlated with the conversation variables as the mean IQ of the ADHD group was significantly lower than that of the TD group (t(48) = 6.13, p < .001). These correlations were small and non-significant (see Supplemental Table S3). There is debate in the literature whether IQ should be controlled in studies of children with ADHD, essentially concerns that removing variance due to IQ is unjustified (Dennis et al, 2009) and may be removing variance due to ADHD itself (Frazier et al., 2004; Miller & Chapman, 2001; Willcutt et al., 2005). None-the-less, we repeated the paired t-test analyses using mixed model multilevel methods to control for Full Scale IQ. In the text we present the results without controlling for IQ.
Given the number of group comparisons undertaken, the Hochberg step-up procedure was applied within families of variables to control for multiple comparisons. This procedure maximizes power while protecting against type 1 errors (Blakesley et al., 2009; Chen et al., 2017). We used the same approach for the families of correlations. Throughout we indicate when controlling for multiple comparisons alters the significance of the findings.
As participant numbers were fixed by the number of children who participated in the follow-up study, and the lack of relevant comparison studies, we did not undertake a power analysis ahead of the study. We did undertake a post hoc sensitivity analysis with the entire sample and for the subsample of children who continued to meet criteria for ADHD and their matched controls.
Results
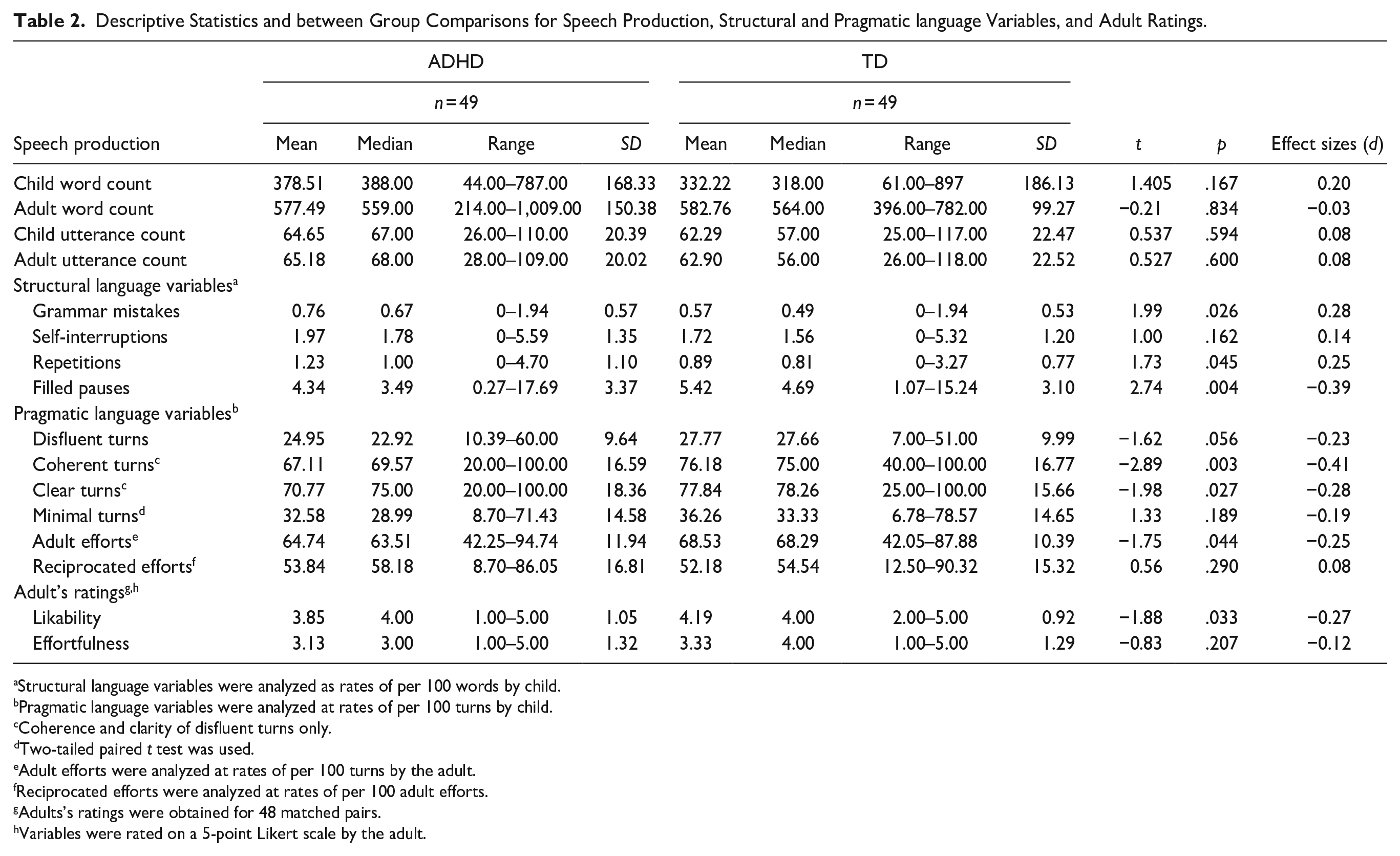
Descriptive statistics (mean, SD, median, and range) and statistical analyses results and effect sizes for the speech quantity and structural and pragmatic language variables are presented in Table 2. Supplemental Table S4 presents the number and percentage of children making each type of speech error.
Descriptive Statistics and between Group Comparisons for Speech Production, Structural and Pragmatic language Variables, and Adult Ratings.
Structural language variables were analyzed as rates of per 100 words by child.
Pragmatic language variables were analyzed at rates of per 100 turns by child.
Coherence and clarity of disfluent turns only.
Two-tailed paired t test was used.
Adult efforts were analyzed at rates of per 100 turns by the adult.
Reciprocated efforts were analyzed at rates of per 100 adult efforts.
Adults’s ratings were obtained for 48 matched pairs.
Variables were rated on a 5-point Likert scale by the adult.
Speech Quantity
The mean word (t(48) = 1.40, p = .167, d = 0.20) and turn (t(48) = 0.54, p = .594, d = 0.08) counts for children in the ADHD and TD groups were not significantly different. The conversation partner word (t(48) = −0.21, p = .834, d = −0.03) and turn counts (t(48) = 0.53, p = .600, d = 0.08) group comparisons were also nonsignificant.
Structural Language
The rate of grammar mistakes (t(48) = 1.98, p = .026, d = 0.28) and repetitions (t(48) = 1.73, p = .045, d = 0.25) was significantly higher in the ADHD group than the TD group. Typically developing children were more likely to use fillers, that is, filled pauses, than children with ADHD (t(48) = −2.741, p = .004, d = −0.39). The rates of self-interruptions were not significantly different across groups (t(48) = 0.996, p = .162, d = 0.14). Chi square analysis showed the proportion of children correcting none, some, or all, of their mistakes (grammar and semantic combined) was not significantly different across the two groups (χ2 (2, N = 81) = 0.288, p = .866). The correction of the child’s mistakes by the adult were analyzed in the same manner with similar results (χ2 (2, N = 81) = 0.340, p = .844). After Hochberg adjustment, the difference in the rate of filled pauses remained significant, while the difference in the rate of grammar mistakes fell just short significance, that is, p = .026, with adjusted = .025.
Pragmatic Language
The rate of dysfluent turns was higher in the TD group than the ADHD group but the difference was not significant (t(48) = −1.62, p = .056, d = −0.23). The rate of dysfluent turns rated as coherent (intact sentence structure; t(96) = −2.89, p = .003, d = −0.41) and/or clear (understandable message) was significantly higher in the TD group than the ADHD group (t(96) = −1.98, p = .027, d = −0.28). The difference in the rate of minimal turns was not significantly different across groups (t(48) = −1.33, p = .189, d = −0.19). Chi square was used to compare the presence of unrelated (off topic) turns. The conversations of children in the ADHD group were more likely to include at least one unrelated turn (χ2 (1, N = 98) = 5.24, p = .022). Following Hochberg adjustment, the difference in the rate of coherent (dysfluent) turns and the presence of unrelated turns remained significant, while the rate of clear (dysfluent) turns was no longer significant, adjusted α = .016.
Adult’s Responses
The proportion of the adult turns coded as efforts to maintain the interaction was significantly higher for the TD group (t(48) = −1.75, p = .044, d = −0.25). The proportion of these efforts that were utilized by the children did not differ across groups (t(48) = 0.56, p = .290, d = 0.08). After adjustment the difference in the adult effort to maintain the interaction remained significant.
The adults rated the TD group children as more likeable than those in the ADHD group (t(47) = −1.88, p = .033, d = −0.27). Their ratings of how effortful they found the conversation didn’t differ across groups (t(47) = −0.83, p = .207, d = −0.12). The difference in ratings of likeability was no longer significant after adjustment for multiple comparisons.
Controlling for the children’s Full Scale IQ scores had little effect on the results except for grammar mistakes and repair of dysfluent turns (clarity scale) which were no longer significantly different (see Supplemental Table S5).
Sensitivity Analysis
For the full sample (N = 98), the sensitivity analysis indicated sufficient power (1 - β = .80) to detect an effect size of d = 0.286 (two-tailed) and d = 0.253 (one-tailed), with α = .05. For the subsample (N = 64), the analysis showed sufficient power to detect an effect size of d = 0.356 (two-tailed) and d = 0.314 (one-tailed) with α = .05.
Exploratory Analyses
Persistent ADHD Subgroup
The results of the subgroup analyses were similar to those for the whole group comparisons, although the effect sizes were generally larger (see Supplementary Table S6). The exceptions were children’s self-interruptions and the adult ratings of child likeability. In the subgroup analysis the ADHD group made significantly more self-interruptions than the TD children (t(31) = 1.8, p = .041, d = 0.32). The adult’s ratings of child likability were not significantly different with this smaller sample (t(30) = −0.66, p = .258, d = −0.12).
Association Between ADHD Symptoms and Child Conversation Variables
Pearson correlation coefficients were calculated separately for inattention and hyperactivity/impulsivity symptom severity and the structural and pragmatic language variables, for the entire sample. Several significant, but small, correlations were identified. Higher levels of inattention correlated with higher rates of self-interruptions (r(95) = .20, p = .046), repetitions (r(95) = .25, p = .016), and off-topic utterances (r(95) = .25, p = .014). The correlation with self-interruptions was no longer significant after controlling for multiple comparisons. Higher levels of hyperactivity/impulsivity correlated with increased rates of repetitions (r(95) = .25, p = .015) and off-topic utterances (r(95) = .28, p = .005) and with decreased rates of minimal utterances (r(95) = −.27, p = .008), and fillers (r(95) = −.25, p = .015). The correlation coefficients for all language variables are presented in Supplemental Table S7.
Association Between the Adult’s Subjective Perception and Child Conversation Variables
We also correlated the adult’s ratings (child’s likability and effortfulness of conversation) with child language variables across the whole sample. A small but statistically significant correlation was found between ratings of likability and minimal utterances (r(95) = −.21, p = .042). Higher rates of minimal utterances were correlated with lower likability ratings. Effortfulness ratings were significantly correlated with self-interruptions rates (r(95) = −.27, p = .008), and minimal utterances rates (r(95) = .31, p = .002). Higher effortfulness ratings correlated with lower self-interruption rates and higher minimal utterances. These full set of correlations is presented in Supplemental Table S7.
Discussion
The current study compared the language use of children with and without ADHD during social discourse with a young adult conversation partner. We evaluated the children’s structural and pragmatic language skills and their efforts to monitor and repair errors. Subtle differences were observed in the structural and pragmatic language skills of children in the two groups. The children in the ADHD group were also less successful than their TD peers in repairing their language errors. The amount of speech produced by the children and adults did not differ across the groups. The adult conversation partner made more effort to engage the TD group children in conversation and rated them as more likable.
Children with ADHD made more grammatical (morphosyntax) mistakes than their TD peers, consistent with reports of poorer morphosyntactic skills on standardized language measures (Parigger et al., 2010; Vassiliu et al., 2023) and during narrative tasks (Bergman & Hallin, 2021; Kuijper et al., 2017). The conversations of children with ADHD included more repetitions, while those of TD children included more fillers (filled pauses). Although classified as a “dysfluency,” fillers are thought to serve a pragmatic function, indicating that the speaker is thinking, rather than reflecting a dysfluency per se (Beeching et al., 2022; Cossavella & Cevasco, 2021). Boo et al. (2022) recently identified a similar pattern of filler use in children with and without ADHD. In terms of their pragmatic language skills, a larger proportion of the children in the ADHD group made off-topic responses, consistent with findings during experimental task performance (Mikami et al., 2007; Zentall et al., 1983).
Group differences were not found for all the child conversation variables. Rates of self-interruptions and the occurrence of minimal utterances were not significantly different across groups. Given the moderate sample size, it is unlikely this is due to a lack of power. The occurrence of pauses and semantic mistakes were low in both groups, the latter suggesting appropriate word use across groups. The children’s utilization of adult efforts to engage them did not differ across groups, suggesting the children with ADHD are similarly engaged in conversation when their interaction partner makes an active effort to include them. It is important to note that we coded whether children utilized the adults’ efforts, not the quality of their responses. Speech quantity did not differ across the two groups, despite excessive talking being a symptom of ADHD. This finding may reflect the research context, for example, conversing with an unknown adult and/or the training and instructions given to the conversation partner. Other studies report similar findings (Boo et al., 2022; Kuijper et al., 2017; Redmond, 2004).
In assessing the children’s conversational repair skills, we focused on their efforts to correct structural mistakes (grammar and semantic errors combined) and dysfluent turns. The proportion of children correcting all, some, or none of their structural mistakes did not differ across groups. This analysis addressed the likelihood of correction only, not the quality of repairs made. Children in both groups evidenced similar awareness of their structural speech errors, although the rate of mistakes was higher in the ADHD group.
All child participants produced dysfluent utterances. Both the coherence and the clarity of these dysfluent turns reflect the children’s efforts to repair their speech, that is, are the children able to restore coherence and/or clarity of the dysfluent utterance. The proportion of dysfluent turns rated as clear and as coherent were significantly smaller in the ADHD group. This suggests children with ADHD are less able to maintain the accessibility of their intended message, making it more difficult for their conversational partner to understand their communicative intentions. Reduced language coherence has previously been reported in narrative production studies with children with ADHD (Freer et al., 2011; Lorch et al., 2010), suggesting it may be a common problem across speech contexts for children with ADHD.
The differences in the measured structural and pragmatic language skills between children with and without ADHD are subtle, both groups of children were able to maintain an extended conversation with the young adult. However, the adult conversational partner demonstrated less effort to keep the children with ADHD engaged in the conversation, that is, the proportion of turns coded as efforts. This finding is consistent with an earlier report by Stroes et al. (2003) that a young adult displayed more verbal initiatives when interacting with TD children compared to those with ADHD. In the current study this effort was not reflected in the quantity of the young adult’s speech, but rather the quality of their interactions, that is, they used more reformulations and praise and asked more questions when interacting with the TD children.
Conversation partners in the current study also rated the children with ADHD as less likeable than their TD peers, despite being blind to their group membership. The reasons for lower likability scores of children with ADHD are not clear. Lower likability ratings correlated with increased minimal utterances, but these didn’t differ across groups. The current results do suggest that even subtle language difficulties may contribute to the social difficulties of children with ADHD.
Not all children in the ADHD group continued to meet full criteria for ADHD, although none were symptom free. Additional analysis of the data for those continuing to meet criteria for ADHD and their matched pairs indicated similar, but stronger effects. This suggests those meeting full criteria for ADHD may be less skilled in their use of structural and pragmatic language than those with subthreshold levels of the disorder.
Having confirmed differences, albeit small, in the social discourse skills of children with and without ADHD, it is important to consider how these differences might arise. Beginning with the symptoms of ADHD, these may impact current performance through interfering with the child’s ability to attend to and respond appropriately during a conversation. While the correlations between ADHD symptom severity and the conversation variables were in the expected direction, they were small. Under controlled experimental conditions ADHD symptom severity appears to predict limited variance in the children’s conversational skills. It is possible that earlier in childhood ADHD symptoms may disrupt the “transactional process” of language learning (Camarata & Gibson, 1999). Elevated levels of hyperactivity/impulsivity would interrupt the caregiver’s response to the child’s utterances, while inattention would prevent the child noticing the caregivers’ corrective feedback. Caregivers might also interpret inattention as disinterest, reducing their efforts to interact or leading to a more directive instructional style, reducing the range and complexity of the interaction (Camarata & Gibson, 1999). Such disruptions could account for several of the current study’s identified group differences. Small correlations observed between current symptoms and performance do not discount this explanation.
Another possible explanation for the current findings is the possible overlap between ADHD and Social Pragmatic Communication Disorder (SPCD). SPCD is a relatively new diagnostic category under Communication Disorders in the diagnostic and statistical manual of mental disorders (American Psychiatric Association, 2022), characterized by impairments in verbal and nonverbal communication. Redmond (2020) reported that 18 of 32 children diagnosed with ADHD in their study, also met criteria for SPCD (Redmond, 2020). It is not yet clear if ADHD and SPCD are separate co-occurring disorders or if ADHD symptoms negatively impact communication skills, increasing the chances of receiving a diagnosis of SPCD.
Children’s executive function skills, for example, working memory, inhibitory control, and cognitive flexibility have been linked to their language proficiency (Baddeley, 2003, 2012; Blain-Brière et al., 2014; Gandolfi & Viterbori, 2020; Ibbotson & Kearvell-White, 2015; Kaushanskaya et al., 2017; Mirman & Britt, 2014). The subtle differences seen in the social discourse performance of our ADHD and TD groups might reflect differences in their cognitive skills. Although not a specific measure of executive function, the ADHD group did obtain significantly lower WISC-III Full Scale IQ scores than their TD peers. That said, controlling for IQ did not eliminate group differences on the social discourse variables. Nonetheless, research addressing the associations between language proficiency and executive functioning in children with ADHD seems warranted given accumulating evidence for differences in the language skills of children with and without ADHD.
Strengths and Limitations
The current study has several important strengths. These strengths include employing a comprehensive coding scheme to assess structural and pragmatic language, as well as conversational partner responses, during social discourse (conversation). This scheme includes novel elements, expanding beyond existing observational coding systems. The sample size is moderate with individual matching for age and sex across groups. Care was taken to thoroughly review the diagnostic status of ADHD and TD groups. There are also some study limitations. Coding was carried out using transcripts only, meaning we were not able to monitor tone of speech, facial expressions, and body language which are part of communication. It is possible that these characteristics contributed to the lower likeability ratings for the ADHD group children. On the other hand, working from transcripts only reduced the likelihood of the coders identifying child group membership or age. Participants did not complete formal language assessments. This prevents us from comparing their conversational performance with scores on standardized language tasks. It also raises the possibility that observed group differences in discourse skills are linked to language impairments in the ADHD group. As the ADHD group were clinic referred, the proportion of boys in the sample is very high, limiting the generalizability of the findings to girls with ADHD and to community samples. In investigating the children’s monitoring and repair skills we only assessed the likelihood of these actions, not the quality of repairs. This should be considered in future studies. Although the conversation partners were psychology majors, experienced in interacting with a wide range of individuals, they were strangers to the children. This coupled with the research context of the interaction may have influenced the children’s speech patterns, although this was the experience of all participants. Finally, while care was taken to ensure the adult conversation partners remained blind to the children’s group membership, they may have formed their own opinions influencing their interactions with, and ratings of, the children.
Conclusions and Clinical Implications
The results of the current study offer new information on the language profiles of children with ADHD during social discourse. We detected subtle differences in the structural and pragmatic language use of children with ADHD and their TD peers. These differences were present in a distraction free environment in the presence of a young adult intentionally working to maintain the children’s engagement. It remains an open question whether the identified differences would be magnified in everyday life, especially with peers who may be less accommodating. Despite the subtlety of the language use differences between children with and without ADHD they may have negatively impacted the relationship with the conversation partner, that is, less effort was made to engage the children with ADHD, and they were rated as less likeable. Additional research and clinical attention should be directed toward understanding and remediating the communication skills of children with ADHD. The potential impact of ADHD symptoms on the transactional process of language learning (Camarata & Gibson, 1999) argues for early remediation of, even subtle, language impairments. There is also a need for research focusing on the possible role of executive function deficits on language development and use. The presence of language difficulties in adults with ADHD (Engelhardt et al., 2011) highlights the importance of early language evaluation and intervention in this group. We encourage longitudinal cohort studies to include language and cognitive evaluations from an early age.
Supplemental Material
sj-docx-1-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-1-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-10-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-10-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-11-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-11-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-12-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-12-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-2-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-2-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-3-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-3-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-4-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-4-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-5-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-5-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-6-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-6-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-7-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-7-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-8-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-8-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Supplemental Material
sj-docx-9-jad-10.1177_10870547251345177 – Supplemental material for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD
Supplemental material, sj-docx-9-jad-10.1177_10870547251345177 for The Conversations of Children With ADHD: Structural and Pragmatic Language Use in Children With and Without ADHD by Hend Samniya, Shelley Taylor, Miho O. Tatsuki and Gail Tripp in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by internal subsidy from Okinawa Institute of Science and Technology Graduate University (OIST).
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.