
Abstract
Objective:
Cognitive Disengagement Syndrome (CDS) is increasingly viewed as a distinct childhood condition. Although it overlaps with ADHD in some features, emerging evidence suggests a unique behavioral and cognitive profile. However, research examining social functioning and emotion recognition in children with pure CDS remains limited.
Methods:
This study compared social competence and facial emotion recognition abilities among children aged 8 to 12 years across three groups: those with elevated CDS symptoms (n = 43), those with ADHD (n = 40), and healthy controls (n = 43). Social functioning and peer relationships were evaluated using parent- and child-report social skills scales and peer interaction questionnaires. Emotion recognition was measured with the Reading the Mind in the Eyes Test (RMET).
Results:
Children with CDS showed significantly lower social skills and RMET scores than both ADHD and control groups (p < .001). Teachers reported fewer school friendships for the CDS group compared to ADHD and controls (p < .001), and CDS children also reported fewer out-of-school friendships than peers in the other groups (p = .035). Both child and teacher reports noted greater peer relationship difficulties in the CDS group compared to the other groups (p < .001). Teachers also observed more solitary behavior and lower group participation among CDS children (p < .001). Within the CDS group, social skills were negatively associated with oppositionality (r = −.347) and positively associated with inattention severity (r = .346). Regression analysis identified social skills scores as independent predictors of peer relationships across the full sample (p < .001).
Conclusion:
These findings suggest that children with elevated CDS symptoms experience greater social difficulties and more pronounced emotion recognition impairments than both ADHD and typically developing peers, reflecting a distinct social-cognitive profile that extends beyond overlapping ADHD symptoms. The results underscore the importance of early recognition and targeted interventions.
Introduction
Cognitive disengagement syndrome (CDS), formerly known as sluggish cognitive tempo, has recently emerged as a distinct clinical construct characterized by symptoms such as excessive daydreaming, mental confusion, and slowed thinking and behavior. While historically conceptualized as a dimension of ADHD, growing empirical evidence supports the classification of CDS as a separate syndrome with unique cognitive and behavioral profiles (Becker et al., 2023). Although CDS has gained increasing empirical attention, it is not currently recognized as a distinct diagnostic category in the DSM-5-TR, but rather remains a research-based construct often observed in children with attentional difficulties that are not fully explained by existing ADHD presentations (Becker, 2025; Kaçmaz et al., 2024).
Recent studies have identified CDS as a prevalent concern in child and adolescent psychiatry, with approximately one-third of referred cases presenting with clinically significant symptoms (Yildirim, 2023). Community-based data also suggest that 15% to 25% of school-aged children exhibit CDS-related behaviors. CDS has been shown to associate more strongly with internalizing symptoms—such as anxiety, depression, somatic complaints, and sleep disturbances—than with hyperactivity or impulsivity, supporting its distinction from traditional ADHD symptomatology (Burns et al., 2023). In addition to emotional difficulties, children with CDS frequently exhibit significant impairments in social functioning, including social withdrawal, peer disengagement, and rejection—often more severe than those observed in ADHD (Cano-Crespo et al., 2024).
To contextualize the current study, it is important to distinguish between emotion regulation and emotion recognition, as these represent different cognitive-emotional domains. Emotion recognition refers to the ability to identify others’ emotional states based on cues, while emotion regulation involves modulating one’s own emotional responses (Sevincok et al., 2021). Although both contribute to social behavior, they are underpinned by distinct mechanisms. Existing evidence suggests that children with CDS may show impairments specifically in emotion recognition, particularly in decoding emotional expressions and mental states (Cano-Crespo et al., 2024; Sevincok et al., 2021). This distinction holds important implications for interventions, as deficits in recognition may require approaches different from those targeting emotional control, which is typically emphasized in ADHD treatments.
Complicating the understanding of CDS-specific features, many existing studies include overlapping ADHD comorbidity, making it difficult to isolate the pure CDS profile. Up to half of children with elevated CDS symptoms also meet criteria for ADHD (Inci Izmir et al., 2024; Sevincok et al., 2021), reinforcing the need for research that directly compares children with pure CDS, pure ADHD, and typically developing peers. Despite growing recognition of these issues, only a limited number of studies have examined differences between these groups in social competence and emotion recognition using validated tools such as the Reading the Mind in the Eyes Test (RMET; Burns et al., 2024). Given the central role of emotion recognition and peer relationships in psychosocial development, the present study aims (Becker et al., 2023) to compare school-aged children with pure CDS, pure ADHD, and healthy controls in terms of social competence and emotion recognition abilities, and (Kaçmaz et al., 2024) to examine how these domains predict peer relationships.
Materials and Methods
Sample
This study was performed with the Institutional Review Board protocol approval date 09.02.2023 and number 2023/02-05 between February 2023 and February 2024. The study included 126 children aged 8 to 12 years, divided into three groups: 43 with Cognitive Disengagement Syndrome (CDS), 40 with ADHD, and 43 healthy controls. Clinical participants were recruited from a child psychiatry outpatient clinic, including newly diagnosed or follow-up cases. All participants were enrolled in this study after obtainment of written informed consent. Inclusion criteria included a confirmed elevated CDS symptoms or diagnosis of ADHD, age between 8 and 12 years, literacy in both the child and at least one parent, a full-scale IQ score of 80 or above, and absence of any psychiatric comorbidity other than oppositional defiant disorder (ODD). Exclusion criteria included: chronic medical illness, neurological disorder, intellectual disability, use of psychiatric medication in the past 3 months, history of head trauma, illiteracy, or refusal to participate.
Study Procedure
Children and adolescents with symptoms of inattention, hyperactivity, or impulsivity were assessed through a structured diagnostic process based on DSM-5 criteria. As part of the initial evaluation, parents completed the Child Behavior Checklist (CBCL) and the DSM-IV-Based Disruptive Behavior Disorders Rating Scale, while teachers were asked to fill out the same DSM-based scale along with a Teacher Information Form. Cases scoring 2 or higher on two or more of the CDS-related items (items 13, 17, 80, and 102) on the CBCL were flagged for possible CDS and further assessed using the Barkley Child Attention Scale, completed by both parents and teachers. Cognitive capacity was assessed using the Wechsler Intelligence Scale for Children-Revised (WISC-R). To rule out other psychiatric conditions, the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL, Turkish version) and the DSM-IV-Based Rating Scale were administered to all participants, including the control group. All cognitive assessments using the WISC-R were administered by licensed clinical psychologists. Psychiatric evaluations, including the administration of the K-SADS-PL, were conducted by a child and adolescent psychiatry resident. Children were assigned to diagnostic groups following a two-stage screening process: first, a parent-rated BCAS was used to identify elevated CDS symptoms (cut-off score ≥23), and then, a structured K-SADS-PL interview was conducted to confirm or exclude ADHD and other psychiatric diagnoses. In cases of diagnostic complexity or uncertainty, final group assignment was made in consultation with senior psychiatrists. Children with comorbid CDS and ADHD were excluded. Due to the nature of the clinical setting and prospective recruitment strategy, detailed records of total screened participants and the number of comorbid exclusions were not systematically retained. A large-scale study comparing children with autism, ADHD, and general school populations found that across all groups, those with CDS experienced significantly greater peer rejection and were more frequently withdrawn and shy, despite no differences in prosocial behavior (McFayden et al., 2022). Moreover, a 2024 study of children aged 3 to 7 years showed that higher CDS scores were significantly associated with worse parent-rated social communication and greater social withdrawal across groups including neurotypical, ADHD, autistic, and co-occurring autism + ADHD samples (Mayes et al., 2023).
Parents of all participants completed additional questionnaires including a sociodemographic and clinical data form, the Social Skills Rating System (parent form). Teachers were also asked to complete the Peer Relationships Clinical Data Form, Barkley Child Attention Scale, and the DSM-IV-Based Disruptive Behavior Disorders Rating Scale. Children in both clinical and control groups were given the Social Skills Rating Scale (child form), the Children’s Depression Inventory (CDI), and the Peer Relationships Clinical Data Form. Finally, all participants underwent administration of the Reading the Mind in the Eyes Test.
Measures
Sociodemographic Data Form
This researcher-designed form collected basic demographic and clinical information, including the child’s birth date, school status, medical and psychiatric history, family income, and parental education and mental health background. It also assessed peer relationships and social participation from the perspectives of the child, parents, and teachers—such as number of friends, activity involvement, peer acceptance, and parental restrictions on social interactions.
Schedule For Affective Disorders and Schizophrenia for School Aged Children—Present and Lifetime Version (K-SADS-PL-Turkish Version)
A semi-structured interview developed by Kaufman et al. to assess current and lifetime psychopathologies in children and adolescents aged 6 to 18, based on DSM-III-R (APA, 1987) and DSM-IV (APA, 1994) diagnostic criteria (Kaufman et al., 1997). K-SADS-PL has since been updated to align with DSM-5. Turkish validity reliability study was performed by Gökler. The interview consists of three main sections: evaluation of sociodemographic and functional domains, screening for specific psychiatric disorders, and assessment of overall clinical functioning (Gökler 2004).
Wechsler Intelligence Scale for Children—Revised (WISC-R)
The WISC-R is a standardized intelligence test designed to assess verbal and non-verbal cognitive abilities in children aged 6 to 16. Originally developed in 1949 and revised in 1974, it has been adapted for use in Turkey with established validity and reliability. The test consists of two main components, Verbal and Performance, each comprising six core subtests and one supplementary subtest (Savaşır & Şahin, 1995; Wechsler, 1974).
DSM-IV-Based Disruptive Behavior Disorders Rating Scale
Developed by Atilla Turgay, this scale transforms DSM-IV diagnostic criteria into questionnaire form and is completed by parents and teachers of children suspected of having ADHD. It consists of 41 items grouped into five symptom domains: inattention (9 items), hyperactivity (6 items), impulsivity (3 items), oppositional defiant disorder (8 items), and conduct problems (15 items). Each item is rated on a 4-point Likert scale (0 = not at all and 3 = very much), reflecting symptom severity. Diagnostic thresholds require elevated ratings (2 or 3) in a minimum number of items per category, with symptoms persisting for at least 6 months (Turgay, 1995). The scale has been validated and standardized for use in Turkey (Ercan, 2001).
Child Behavior Checklist (CBCL)
The CBCL is a parent-report questionnaire developed in 1983 to evaluate emotional and behavioral functioning in children and adolescents aged 6 to 18 years. Although it is not used for diagnostic purposes, it helps identify areas of strength and behavioral problems based on parental observations. The scale includes two main sections: social competence and problem behaviors. The social competence section assesses participation in activities, peer relationships, family and school functioning, and generates a total competence score. The problem behavior section includes 113 items rated on a 3-point scale (0 = not true and 2 = very true/often true), reflecting behavioral and emotional difficulties observed over the past 6 months (Achenbach, 1991). The scale has been validated for use in Turkey (Erol, 1995).
Barkley Child Attention Scale (BCAS)
Developed by Russell Barkley, this 12-item questionnaire is designed to assess symptoms associated with CDS. It uses a 4-point Likert scale (1 = never/rarely to 4 = very often). Ratings of 3 or 4 on individual items are considered indicative of clinically relevant symptoms. The scale also evaluates functional impairment across four domains: school, home life, peer relationships, and leisure activities. A CDS diagnosis is considered when at least three clinically significant symptoms are present in two or more of these domains. Factor analysis of the original version identified two subscales: sluggishness (seven items) and daydreaming/confusion (five items). The scale has shown high internal consistency (α = .934) and test-retest reliability (r = .84). In Turkish validation studies, the Cronbach’s alpha was found to be .86, and the clinical cut-off score was established at 23 (Fırat et al., 2018).
Social Skills Evaluation Scale (SSES)
The Social Skills Evaluation Scale, developed and validated by Akçamete and Avcıoğlu (2007), is designed for use with children aged 7 to 12. The scale consists of 62 items grouped into 12 subcategories and is rated by parents using a 5-point Likert scale ranging from “always” to “never.” Higher scores reflect more advanced social skills. It assesses a broad range of social behaviors by evaluating how frequently the child displays specific social skills in daily life. The scale has demonstrated excellent internal consistency, with a Cronbach’s alpha of .98, and its content validity was established through expert review. The instrument has been validated for use in Turkish populations (Akçamete & Avcıoğlu, 2005).
Social Skills Scale
Developed by Kocayörük, this 20-item Likert-type scale is designed to assess the development of key social skills in school-aged children. It evaluates abilities such as maintaining eye contact, active listening, initiating and sustaining conversation, greeting, asking for help or permission, giving compliments, joining group activities, apologizing, persuading, sharing responsibilities, and self-rewarding behaviors. Each item is rated on a 4-point scale (1 = never to 4 = always), with total scores ranging from 20 to 80. Higher scores indicate stronger social skill performance (Yaya, 2000).
Reading the Mind in the Eyes Test (RMET)—Child Version
Originally developed by Baron-Cohen in 1997 and revised in 2001, the RMET assesses emotion recognition and theory of mind abilities by asking participants to infer mental states from photographs of eye regions. The child version includes 28 items, each presenting a pair of eyes surrounded by four possible emotional or cognitive state descriptors. Participants select the option that best matches what the individual in the photo is feeling or thinking. Higher scores reflect more advanced theory of mind skills (Baron-Cohen et al., 2001). The Turkish adaptation and validation for children and adolescents was conducted by Girli (2014).
Children’s Depression Inventory (CDI)
Developed by Kovacs in 1980, the CDI is a self-report measure designed to assess the severity of depressive symptoms in children and adolescents aged 6 to 17 years. Modeled after the Beck Depression Inventory, the CDI consists of 27 items that evaluate symptoms experienced over the past 2 weeks. Each item offers three response options scored from 0 to 2, with total scores ranging from 0 to 54. Higher scores indicate greater symptom severity, and a cut-off score of 19 is used to identify clinically significant depressive symptoms. The scale has been validated for use in Turkish populations (Oy, 1990).
Statistical Analysis
All the data were analysed with SPSS (Statistical Package for the Social Sciences) software for Windows (v21.0; IBM, Armonk, NY, USA). Individual and aggregate data were summarized using descriptive statistics including mean, standard deviations, medians (min-max), frequency distributions, and percentages. Normality of data distribution was verified by Kolmogorov-Smirnov test. Comparison of the variables with normal distribution was made with Student t test. The variables which were not normally distributed, the Mann Whitney and Kruskal Wallis tests were conducted to compare between groups. Evaluation of categorical variables was performed by Chi-Square test. p-Values of <.05 were considered statistically significant.
Results
The study sample consisted of children residing in an urban region of Türkiye, and detailed demographic characteristics of the participants are provided in Table 1. There were no statistically significant differences among the CDS (mean age = 10.12 ± 1.60), ADHD (mean age = 9.55 ± 1.26), and control groups (mean age = 9.63 ± 1.44) in terms of age (p = .186) or gender distribution (p = .234), as these variables were intentionally balanced during participant recruitment to minimize potential confounding effects. In terms of depressive symptoms, the CDS group showed the highest scores on the Children’s Depression Inventory (11.28), followed by the ADHD (9.40) and control groups (6.88; p < .001). Finally, the highest scores on the Barkley Child Attention Scale were found in the CDS group (30.35), significantly exceeding both the ADHD (15.90) and control (13.23) groups (p < .001).
The Demographic Characteristics of the Study Sample.
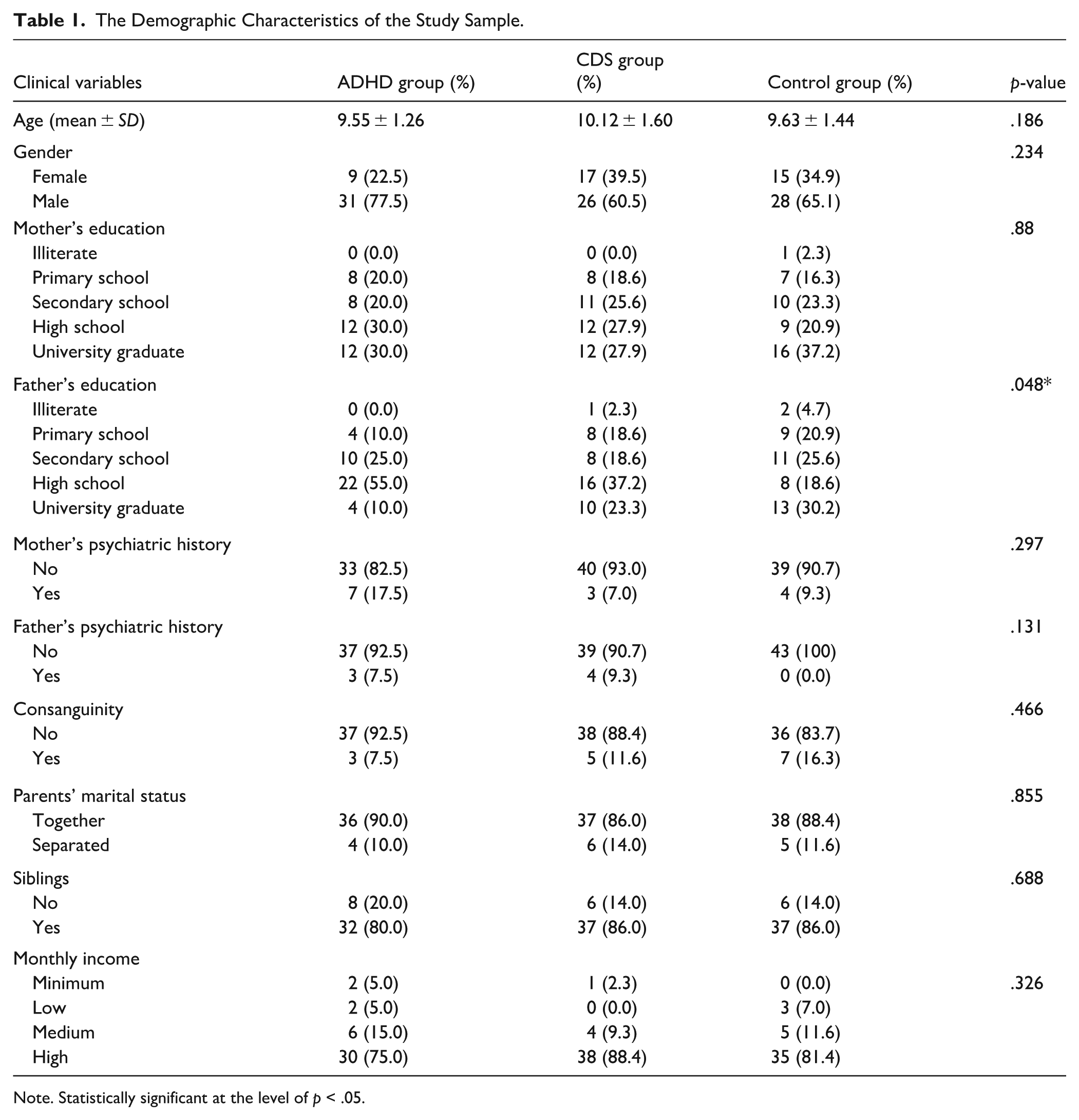
Note. Statistically significant at the level of p < .05.
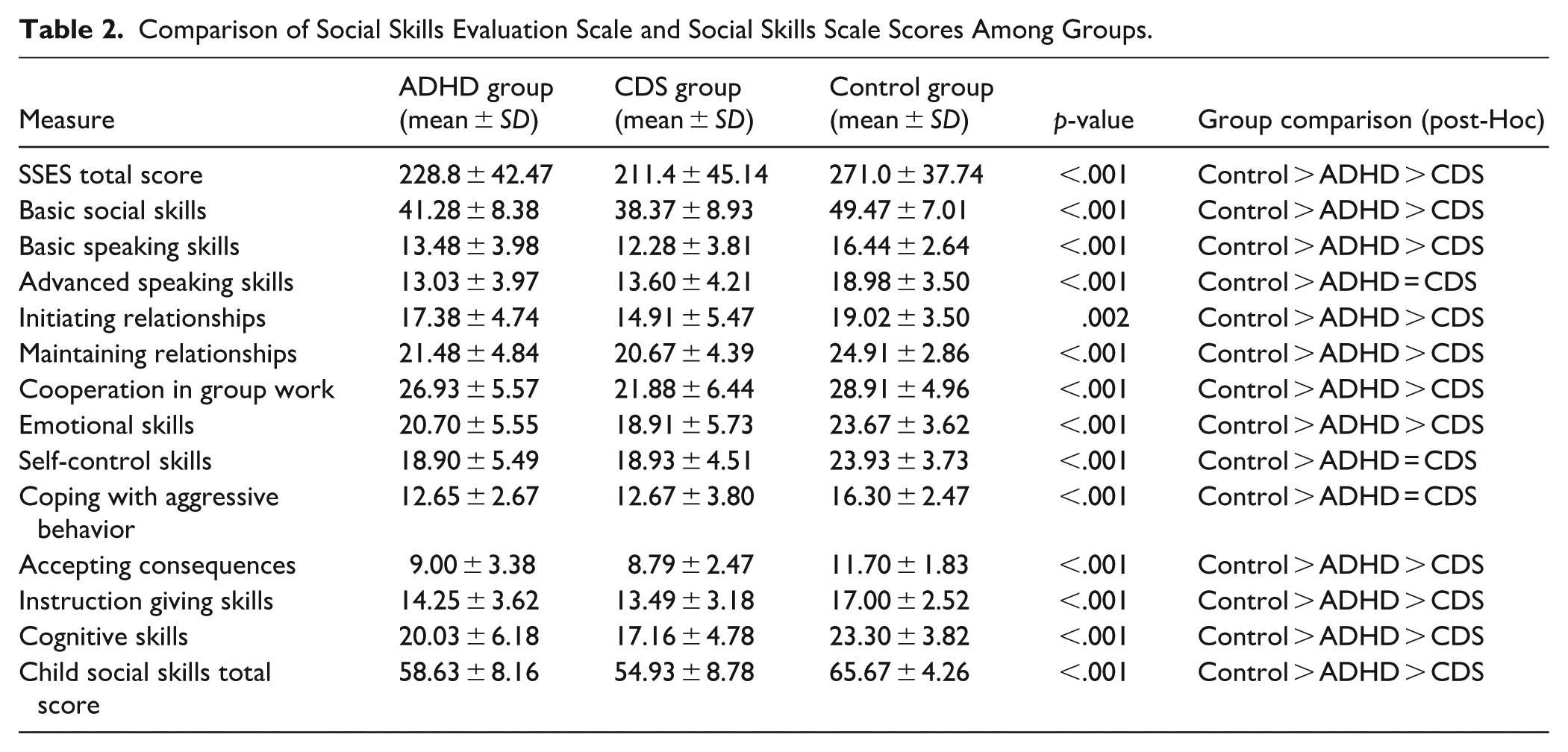
Based on the results from the Social Skills Assessment Scale and the Social Skills Scale, children in the CDS group demonstrated significantly lower total social skills scores compared to both the ADHD and control groups (p < .001). Subscale analyses revealed that the CDS group scored significantly lower in basic social skills, basic and advanced communication, relationship initiation and maintenance, group collaboration, emotional skills, acceptance of outcomes, instruction-following, and cognitive skills compared to the other groups (all p < .001). For self-control and coping with aggressive behaviors, the control group had significantly higher scores than both clinical groups (p < .001). Additionally, the total score on the Social Skills Scale was also significantly lower in the CDS group compared to ADHD and control groups (p < .001; Table 2).
Comparison of Social Skills Evaluation Scale and Social Skills Scale Scores Among Groups.
Moreover, the RMET revealed significant differences among the three groups. The CDS group scored significantly lower (14.56 ± 3.93) than both the ADHD group (16.15 ± 3.12) and the control group (19.91 ± 1.96; p < .001).
In our study, teacher evaluations indicated that children in the CDS group had significantly fewer friendships at school compared to those in the ADHD and control groups (p < .001). Regarding friendships outside of school, child reports revealed that having six or more friends was significantly less common among children in the CDS group than in the other groups (p = .035). Peer relationship assessments showed that both children and teachers reported significantly more difficulties in initiating and maintaining peer relationships in the CDS group compared to the ADHD and control groups (p < .001 for both). Additionally, family and child reports indicated that children in the ADHD group were more frequently subject to parental restrictions on socializing compared to their peers (p = .009 and .013, respectively). Teacher observations further highlighted that children in the CDS group were significantly more likely to avoid participating in group activities (p = .002), spend recess alone (p < .001), and be less accepted by their peers (p < .001; Table 3).
Group Differences In In-school and Out-of-school Friendships and Peer Relationships Based on Parent, Child, and Teacher Reports.
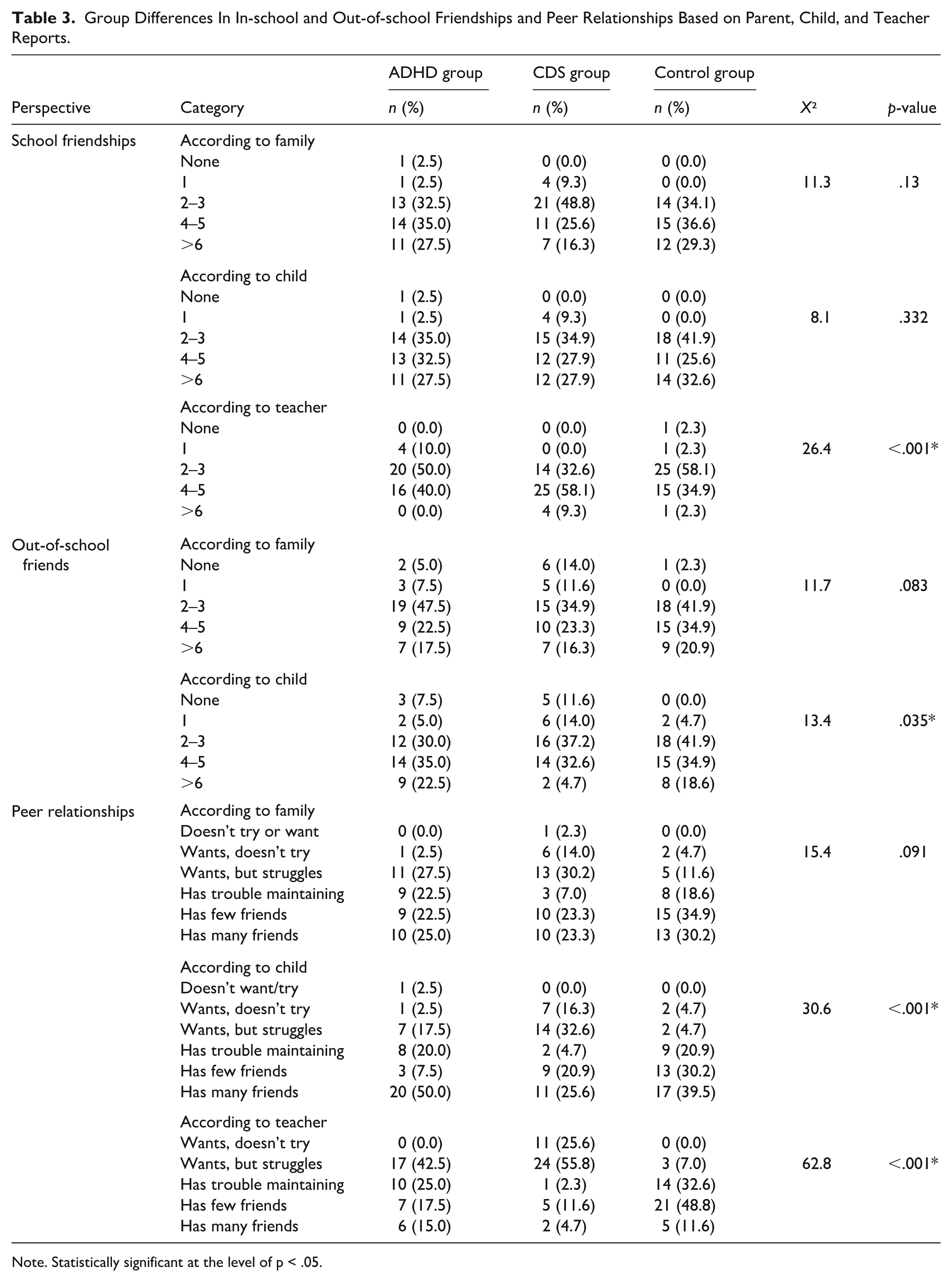
Note. Statistically significant at the level of p < .05.
In the CDS group, a statistically significant negative correlation was found between the Turgay—ODD subscale total score and the Social Skills Evaluation Scale (SSES) total score (r = -0.347, p = .023), while a significant positive correlation was observed between the Turgay inattention subscale total score and the Barkley total score (r = .346, p = .023). Additionally, a logistic regression analysis for teacher-rated peer relationships showed that the model including SSES total score, Child Social Skills total score, and RMET total score was statistically significant (p < .001, R2 = .218). Univariate analysis revealed that the SSES total score significantly predicted peer relationships (OR = 2.83, 95% CI [0.002, 0.011], p = .005), as did the Child Social Skills total score (OR = 2.91, 95% CI [0.012, 0.064], p = .004), identifying them as independent predictors of teacher-rated peer relationships.
Discussion
Researchers have outlined key mechanisms, highlighting behavioral inhibition and poor social self-regulation as potential contributors to the social disengagement observed in the CDS population. Becker et al. (2019) in a study of 158 children aged 7 to 12 years referred for ADHD evaluations, found that higher levels of CDS symptoms, measured via both parent and teacher ratings, were significantly associated with poorer social functioning outcomes, even after controlling for ADHD-IN, ADHD-HI, ODD, and internalizing symptoms. Specifically, teacher-rated CDS symptoms were strongly associated with greater asociality (β = significant, p < .001), increased peer ignoring (β = significant, p = .01), and greater peer exclusion (p = .02), while parent-rated CDS symptoms predicted lower parent-rated social engagement (p = .02). Similarly, McFayden et al. (2022) significantly related CDS symptoms to parent-rated social impairment in youth diagnosed with ADHD, Autism Spectrum Disorders (ASD), or their combination, regardless of diagnostic category. They reported that CDS contributed to social deficits above and beyond the impairments associated with ADHD or ASD alone. Moreover, Becker et al. conducted a multimethod evaluation and reported that children exhibiting CDS symptoms spent significantly more time alone during recess (mean = 5.06% vs. 1.23%; p < .001) and demonstrated significantly fewer positive peer behaviors (mean = 66.45% vs. 79.95%; p < .001) compared to their ADHD peers. Teachers also rated children with CDS as more asocial (mean = 1.62 vs. 1.38; p < .01), more frequently ignored (mean = 1.90 vs. 1.50; p < .01), and excluded by peers (mean = 1.58 vs. 1.32; p < .001). Furthermore, teacher ratings revealed significantly higher levels of conflicted shyness (mean = 2.27 vs. 1.93; p < .01) and social disinterest (mean = 2.74 vs. 2.21; p < .001). Self-reported loneliness was also significantly greater in the CDS group (mean = 4.87 vs. 3.49; p < .01) than ADHD peers (Becker et al., 2025). Our current findings are consistent with and further extend the published data. In our study, children in the CDS group demonstrated significantly lower total scores on both the Social Skills Evaluation Scale and the Social Skills Scale compared to the ADHD and control groups (p < .001), with specific deficits across multiple domains including communication, emotional regulation, group collaboration, and instruction-following. Beyond overall social skill impairments, our results revealed that CDS children had markedly fewer friendships at school based on teacher evaluations (p < .001) and were significantly less likely to report having friends outside of school (p = .035). Both child and teacher assessments indicated more pronounced difficulties in initiating and maintaining peer relationships (p < .001), while teacher observations highlighted elevated avoidance of group activities (p = .002), solitary behavior during recess (p < .001), and reduced peer acceptance (p < .001). These findings mirror and reinforce prior studies. Particularly, Becker (2025) observed that children with elevated CDS symptoms, as rated by both parents and teachers, exhibited greater asociality, peer ignoring, and exclusion, even after accounting for comorbid ADHD and ODD symptoms. Similarly, their multimethod study showed that CDS children spent significantly more time alone during recess, had fewer prosocial interactions, and were more frequently described by teachers as socially disinterested and withdrawn (Becker et al.,2025). Supportively, our logistic regression results also support the predictive value of CDS-associated deficits on peer functioning, with both SSES and child-rated social skills emerging as significant independent predictors of teacher-rated peer relationships (OR = 2.83, p = .005; OR = 2.91, p = .004).
In general, CDS symptoms appear to be associated with social withdrawal, isolation, and low initiative in forming social relationships. This highlights the importance of better understanding the relationship between CDS and social functioning, as well as the need to structure psychosocial intervention strategies when CDS symptoms are present. These findings emphasize that interventions focusing on social skills should be considered as an essential component of treatment. Although children with ADHD scored higher than those with CDS, their scores were still lower than those of the control group. This suggests that, while children with ADHD may exhibit more outward-oriented behavior compared to those with CDS, their lower scores compared to controls may reflect qualitative deficits in the content and effectiveness of their social skills. Children with CDS scored significantly lower on the self-reported social skills scale compared to both the ADHD and control groups (CDS < ADHD < Control). A similar pattern was also observed in the parent-reported Social Skills Evaluation Scale (SSES) total scores, suggesting that children with CDS not only struggle more with social skills but are also aware of these difficulties. This awareness may indicate a level of insight into their social challenges. Furthermore, such self-awareness may be associated with higher rates of internalizing disorders, such as depression and anxiety. The finding that children with ADHD also scored lower than the control group on the self-reported social skills scale suggests that they too experience social difficulties and possess some level of awareness regarding these challenges. The consistency observed in both the CDS and ADHD groups—across parent- and self-reported measures—enhances the reliability of the study’s findings. Moreover, this insight into their own social limitations highlights the potential value of incorporating self-awareness components into social skills training programs designed for these populations.
Studies directly examining emotional face recognition in children with pure CDS using the Reading the Mind in the Eyes Test (RMET) are notably limited. The closest comparable data come from a study by Sevinçok et al., which documented RMET performance in children with ADHD and measured CDS symptom severity using the BCAS. The sample included 50 children with ADHD and 40 typically developing controls, aged 8 to 14 years. The ADHD group scored significantly lower on the RMET than the control group (p = .001). Importantly, within the ADHD sample, higher CDS symptom severity was significantly associated with poorer RMET performance. In addition, CDS severity was significantly correlated with ADHD-inattention symptoms (r = .34, p = .013), internalizing behaviors (r = .37, p = .007), and performance on another ToM task (UOT; r = .38, p = .006). A regression analysis further revealed a significant negative association between CDS severity and second-order ToM scores (β = .261, Exp(B) = 1.933, p = .045), suggesting that greater CDS symptoms predict lower capacity for complex mental state attribution (Sevincok et al., 2021). Although studies directly examining RMET performance in pure CDS populations are limited, existing research on RMET outcomes in clinically diagnosed ADHD samples—particularly those assessing CDS symptom severity dimensionally—provides a relevant and appropriate framework for interpreting our findings. For instance, Aydın et al. reported that adults with predominantly inattentive ADHD performed significantly worse on RMET compared to neurotypical controls, despite showing no deficits in cognitive flexibility. This suggests a specific impairment in social-cognitive processing among individuals with CDS-like profiles (Aydın et al., 2022). Similarly, Çıray et al. (2022) found that adolescents with ADHD exhibited significantly reduced RMET scores, with particular difficulties in decoding mental states. Özyurt et al. extended these findings by showing that children with comorbid ADHD and disruptive mood dysregulation disorder (DMDD)—a subgroup likely to share affective and attentional dysregulation with CDS—also had significantly lower RMET scores than both ADHD-only and control groups (Özyurt et al., 2024). Moreover, Yilmaz Kafalı et al. (2021) demonstrated that even within the ADHD population, RMET deficits were predictive of increased social vulnerability: each one-point decrease in RMET score was associated with a 53% higher risk of peer victimization and a 21.6% increase in bullying perpetration. In accordance with these data in present study, children in the CDS group had significantly lower RMET scores compared to both ADHD and control groups (p < .001). This difference is notable in that it persists even in comparison to the ADHD group, which itself is known to exhibit social cognition deficits.
In conclusion, this study directly compared children with pure CDS and pure ADHD in terms of social functioning and affective theory of mind abilities. Our findings provide compelling evidence that children with CDS experience more pervasive and severe social impairments than their ADHD and typically developing peers. These impairments encompass reduced peer engagement, fewer friendships, increased social withdrawal, and difficulties in initiating and maintaining relationships. Moreover, CDS was associated with significantly lower performance on the Reading the Mind in the Eyes Test (RMET), indicating specific deficits in the recognition of subtle emotional cues and mental state attribution. These findings suggest that CDS is linked to a distinct disruption in social cognitive functioning that cannot be fully explained by overlapping ADHD symptoms. The consistent and pronounced nature of these deficits highlights the clinical relevance of CDS as a separate construct and underscores the urgent need for early identification and targeted interventions aimed at improving social understanding and peer relationships in this population.
The lower emotion recognition abilities observed in children with CDS compared to those with ADHD and the control group may be partially explained by deficits in working memory and selective attention. Activation of the prefrontal cortex is known to play a key role in recognizing emotional facial expressions, and structural and functional impairments in the prefrontal cortex—commonly reported in the etiology of ADHD—may account for the difficulties ADHD children face in this domain. Furthermore, ADHD-related symptoms such as distractibility, impulsivity, and oppositional behavior may also contribute to challenges in emotion recognition. It is therefore suggested that targeted support in emotion recognition, a subdomain of social cognition, could positively influence the social skills of both groups.
Limitations
This study has several limitations. First, the cross-sectional design limits our ability to infer causality or assess developmental trajectories of social functioning and emotion recognition in children with CDS and ADHD. Longitudinal studies are needed to better understand how these impairments evolve over time. Second, much of the data was based on caregiver and teacher reports, which may be subject to bias or limited by the informants’ perspective. Although we included multi-informant sources and standardized measures, future studies should incorporate more objective methods, such as direct behavioral observations or neuropsychological assessments.
Another limitation of the study is that we did not systematically record the total number of children assessed or excluded due to comorbid CDS and ADHD. Therefore, while rigorous criteria were applied to ensure diagnostic separation, we are unable to report precise figures on diagnostic overlap or recruitment yield. Future studies should prospectively track this information to enhance methodological transparency.
Finally, given the number of variables and statistical tests conducted in the present study, there is an increased risk of Type I error. Although findings were interpreted with caution, future studies with larger samples and adjusted significance thresholds (e.g., Bonferroni correction) are warranted to validate these results.
Footnotes
Ethical Considerations
Institutional Review Board protocol approval number: 2023/02-05. Institutional Review Board protocol approval date: 09.02.2023.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.