
Abstract
Background:
Attention deficit hyperactivity disorder (ADHD) has been associated with comorbid conditions, especially psychiatric comorbidities. On the other hand, getting an ADHD diagnosis has been linked to children’s relative age. The aim of this study was to describe diagnostic patterns of ADHD patients of all ages, and to compare comorbidity and birth month between ADHD patients and matched controls.
Methods:
This nationwide study cohort included incident ADHD patients with records of ADHD medication and/or ADHD diagnosis in Finland during 2015 to 2020, and with no such records during 2010 to 2014. Four controls were matched with each patient based on age, gender, and place of residence.
Results:
Altogether 66,146 incident ADHD patients and 256,270 matched controls were identified, and their average follow-up time was 3.5 years. Mean age at the first ADHD diagnosis was 15.9 years for males and 22.3 for females. Prior to being diagnosed with ADHD, patients visited health care remarkably more often than controls. Comorbid diagnoses were the most prevalent at index date, and compared to controls, the prevalence of these comorbidities within 3 years preceding the index date increased more in ADHD patients. The odds of ADHD increased with later birth months across all age-gender groups, except among girls under 6 years of age. The association was more pronounced among males.
Conclusion:
ADHD is associated with a significant comorbidity burden across all age groups, even before ADHD diagnosis. Individuals who are younger in relative age are more likely to be diagnosed with ADHD.
Introduction
Inattention, hyperactivity, and impulsivity are the core symptoms of attention deficit hyperactivity disorder (ADHD). In addition, emotional dysregulation and executive function deficits support ADHD diagnosis (Adler et al., 2013; Faraone et al., 2021; Kooij et al., 2019; van Stralen, 2016). The two most used international diagnostic criteria for ADHD are the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013) and the International Statistical Classification of Diseases and Related Health Problems (10th [ICD-10] and 11th [ICD-11] revisions; World Health Organization, 2019, 2025). In both criteria, a confirmed diagnosis requires a persistent pattern of developmentally inappropriate symptoms that cause at least moderate functional impairment, are present in several different settings, and cannot be better explained by another condition.
ADHD was first described as a childhood disorder but is now well recognised to be frequently persistent also in adults (Barkley et al., 2002; Faraone et al., 2006; Kooij et al., 2019). Although approximately two-thirds of children with ADHD continue having clinically significant symptoms and functional impairment in their adulthood, symptoms and diagnosis may pass unnoticed in adults (Biederman et al., 2000; Faraone et al., 2006). The presentation of symptoms may vary between individuals and change from childhood to adulthood, being less external in adults (Adler et al., 2013; Larsson et al., 2006; Polanczyk et al., 2007).
ADHD is often associated with adverse health outcomes, such as comorbidities, risk-taking behaviour, distress, and higher risk of different types of addictions that impact everyday functioning (Bernardi et al., 2012; Faraone et al., 2021). ADHD commonly occurs alongside other psychiatric disorders (Hartman et al., 2023). It is estimated that roughly 66% to 80% of children and adolescents with ADHD also exhibit one or more psychiatric comorbidity (Kessler et al., 2014; Reale et al., 2017). When additional psychiatric disorders are present ADHD symptoms tend to be more severe and overall outcomes are often poorer (Faraone et al., 2024; Njardvik et al., 2025). ADHD is also associated with higher use of health care services (Polyzoi et al., 2018).
In childhood, the most common psychiatric comorbidities of ADHD include oppositional defiant disorder, conduct disorder, behaviour disorders, anxiety disorders, autism spectrum disorders, tic disorders, learning disorders, and sleep disorders (Gnanavel et al., 2019; Hartman et al., 2023; Kessler et al., 2014; Njardvik et al., 2025; Reale et al., 2017). The most common co-occurring psychiatric conditions among adults are depression, bipolar disorder, anxiety disorders, and substance use disorder (Bernardi et al., 2012; Chen et al., 2018; Hartman et al., 2023). A recent nationwide cohort study from Taiwan reported primarily learning disabilities and tics as psychiatric comorbidities of ADHD for children (0–12 years), oppositional defiant and conduct disorders for adolescents (13–18 years), and anxiety, depression, bipolar disorder, and substance misuse for adults (≥18 years; Kao et al., 2025). Additionally, children and adolescents with ADHD have been shown to experience more pain, such as stomach pain and headache (Kerekes et al., 2021) and to exhibit higher prevalence of chronic pain syndrome than peers (Mundal et al., 2024). Comorbidities with overlapping symptoms and between-subject variation in clinical manifestation highlight the importance of careful clinical assessment and differentiation diagnosis. Of somatic diseases, associations between ADHD and obesity (Cortese, Moreira-Maia, et al., 2016), type 2 diabetes mellitus and hypertension (Chen et al., 2018), asthma (Cortese et al., 2018), and sleep disorders (Marten et al., 2023) have been published.
Relative age effect refers to phenomenon whereby young-in-class children are more likely to be rated with ADHD symptoms by both parents and teachers than their older-in-class peers (Deng et al., 2024; Frisira et al., 2025; Karlstad et al., 2017; Vuori et al., 2020). In relation to variability in symptom recognition, the increased risk of ADHD diagnosis and the higher use of ADHD medication have been linked to children’s relative age (Karlstad et al., 2017; Layton et al., 2018; Morrow et al., 2012; Vuori et al., 2020). In Finland, where children born in December are the youngest in the class, the use of ADHD medication has been observed to be more common among both genders born in May–August or September–December than among those born in January–April (Vuori et al., 2020).
The aim of the present study was to thoroughly describe diagnostic patterns of ADHD patients of all ages in a nationwide Finnish cohort, and to widely but accurately analyse their comorbidities before and after ADHD recognition. The aim was also to compare this disease burden with matched controls without ADHD. To increase knowledge about the relative age effect in ADHD diagnosis, this study also examined this issue using a controlled design.
Methods
This was a cohort study utilising secondary data from national administrative databases in Finland. Nationwide Care Registers for Health Care maintained by the Finnish Institute for Health and Welfare as well as nationwide prescription registers and reimbursement register maintained by the Social Insurance Institution of Finland were used to identify people with ADHD. A more detailed description of the identification of the ADHD patients can be found in a previous publication (Westman et al., 2025a). In addition to the above-mentioned registers, information about gender, date of birth, and place of residence were captured from the Digital and Population Data Services Agency. Dates of death were obtained from Statistics Finland. Personal-level data were linked across data sources by the authorities using unique personal identity numbers.
The study cohort included incident ADHD patients of any age who fulfilled any of the ADHD identification criteria – prescription or drug purchase of ADHD medication, higher than regular reimbursement specifically for ADHD medication, or ICD-10 F90* diagnosis for ADHD – for the first time during 2015 to 2020, and none of the criteria during the history period 2010 to 2014. An individual index date was defined as the first date when any of the identification criteria was met. The date of the first ADHD diagnosis was identified for individuals with at least one ADHD diagnosis (ICD-10 F90*) record during the study period.
Four controls without any of the ADHD criteria were identified for each incident ADHD patient, when possible, by Digital and Population Data Services Agency. Controls were matched with ADHD patients based on the year of birth (+/− 1 year), gender, and place of residence in the beginning of 2015 (or at the time of birth if later than Jan 01, 2015). For each control, the corresponding comparison time point was assigned based on the matched ADHD patient’s index and diagnosis date. All individuals were followed until emigration, death, or Dec 31, 2021, whichever occurred first. For some ADHD patients, no controls or only a limited number of controls could be identified. In analyses comparing the ADHD population with the control population, only ADHD patients with at least one control were considered.
For patients with an ADHD diagnosis record, diagnostic patterns were evaluated by examining the age distribution at the first ADHD diagnosis (ICD-10 F90*) and the distribution of the first ADHD diagnoses. Health care visits and contacts during the 24 months before the first ADHD diagnosis were observed monthly and compared with the respective records of controls.
Comorbidities were classified using ICD-10 at three-digit precision. Comorbidities of special interest included 12 conditions most commonly associated with ADHD or most relevant for differential diagnosis (considering the control setting): anxiety disorders (F40–F41, F93); unipolar depression and undefined mood disorders (F32–F39); learning disabilities or motor coordination disorder, including developmental disorders of speech, language, scholastic skills, or motor coordination (F80–F83); conduct disorders, including oppositional defiant disorder (F91–F92); pervasive developmental disorders, including autism spectrum disorders (F84); stress and adjustment disorders (F43); substance use disorders (F10–F19); bipolar disorder (F30–F31); non-affective psychotic disorders (F20–F29); tic disorders (F95); obsessive-compulsive disorder (F42); mental retardation (F70–F79).
Prevalence of the 12 pre-specified comorbidities was assessed at half-year intervals from 3 years before to 3 years after the individual index date for ADHD patients and controls. Each half-year interval represented the proportion of people who had a health care contact within +/− 3 months, among those who survived the corresponding 6-month time window. A comparative interrupted time-series analysis was conducted to compare the trends in the prevalence of the pre-specified comorbidities among ADHD patients and controls before and after the index date (that is, interruption; Fry & Hatfield, 2021). Ordinary least square regression models were estimated including the following independent variables: half-year time point, an indicator for whether the time point was before or after the index date, indicator for the cohort (ADHD patient or control), and interactions between each variable. The model included seven time points before (and including) the index date, and five time points after. The 6-month time point was excluded to allow the change to occur. Baseline refers to the first time point.
Prevalences of the 12 pre-specified comorbidities were also summarised for different age groups within time windows of −3 to 0 years, 0 to 1 year, and 1 to 3 years from the index date, separately for ADHD patients and controls. The first two intervals represent the proportions of individuals in the entire population who had a health care contact for a specified comorbidity during the respective time windows. Because follow-up after index date did not exceed 1 year for all individuals, proportions at 1 to 3 years after the index date were derived using Kaplan-Meier estimation.
In addition, the 15 most common ICD-10 codes (also at the three-digit level) were identified for ADHD patients (excluding Z* codes). The prevalence of each comorbidity during the 3 years preceding the index date was assessed and compared between ADHD patients and controls using standardized mean difference (SMD). An absolute value of SMD ≥ 0.10 was considered as an indication of a meaningful difference (Austin, 2009).
Time of birth was analysed both as a continuous and a categorical variable. The distribution of birth month categories (January–April, May–August, and September–December) was described for ADHD patients. The association between birth month and incident ADHD was assessed using conditional logistic regression, with ADHD status coded as a binary outcome variable (1 = ADHD, 0 = control). First, to evaluate a linear trend in the odds of ADHD across the calendar year, birth month was treated as a continuous variable. The respective p-values for the trend were reported. Second, to evaluate the potential end-of-year effects, birth month was treated as a categorical variable, and the likelihood of ADHD between those born in May–August or September–December and those born in January–April was compared. The association was quantified as odds ratios (OR) with 95% confidence intervals (CI).
Analyses were performed using R version 4.2.2. Throughout the study, all visits and contacts in both primary and secondary health care, as well as the diagnoses linked to them, were considered, and ICD-10 codes for both primary and secondary diagnoses were included in the diagnostic analyses. Multiple diagnoses were allowed for 1 day. Analyses were conducted across the following age groups: young children (<6 years), children (6–12 years), adolescents (13–17 years), and adults (≥18 years). Age grouping was based on age at the index date or at the first ADHD diagnosis, depending on the analysis, and matched controls were grouped accordingly. Birth month analyses were additionally stratified by gender. In the statistical models, p < .05 was considered statistically significant. Results with frequencies of less than five individuals were never reported to protect the privacy of singular individuals.
Study permit was granted by Finnish Social and Health Data Permit Authority Findata with diary number THL/3461/14.02.00/2022. Study protocol was subjected to ethical consideration during the Findata permit process. No separate ethical committee process was required according to local legislation. Along with the data handling, the authorities pseudonymised the data sets to ensure privacy of individuals. Data were stored and analysed in a validated secure data environment provided by Statistics Finland.
Results
Altogether, 66,146 incident ADHD patients and 256,270 controls were identified. For 56,268 (85.1%) of the ADHD patients, an ADHD diagnosis (ICD-10 F90*) record was found during the study period. Furthermore, 64,752 patients had at least one matched control in the full dataset, and 55,059 of them had ADHD diagnosis. Average time from index date to end of follow-up was 3.5 years for both the ADHD patients and the controls.
Mean age at the first ADHD diagnosis was 15.9 years (median 11) for males and 22.3 (median 20) for females. Age groups at the first ADHD diagnosis are presented in Table 1. Among males, 57.9% were diagnosed under the age of 13 years and 29.4% during adulthood, whereas the corresponding proportions for females were 26.3% and 56.3%, respectively. The distributions of the first ADHD diagnoses (ICD-10 F90*) by age group are presented in Table 2. The most common initial F90* diagnosis was disturbance of activity and attention (F90.0) set for 60.0% to 92.0% of the incident patients with an ADHD diagnosis. One third (33.4%) of young children got the diagnosis hyperkinetic disorder, unspecified (F90.9) first. Prior to the F90* diagnosis, 1.6% of young children, 4.0% of older children, 7.1% of adolescents, and 2.7% of adults with any ADHD diagnosis had received a diagnosis of attention deficit disorder, ICD-10 F98.8 (other specified behavioural and emotional disorders with onset usually occurring in childhood and adolescence).
Age Group at the First ADHD Diagnosis (ICD-10 F90*), Overall and by Gender, N (%).

Distributions of the First ADHD Diagnoses (ICD-10 F90*) by Age Group, N (%).
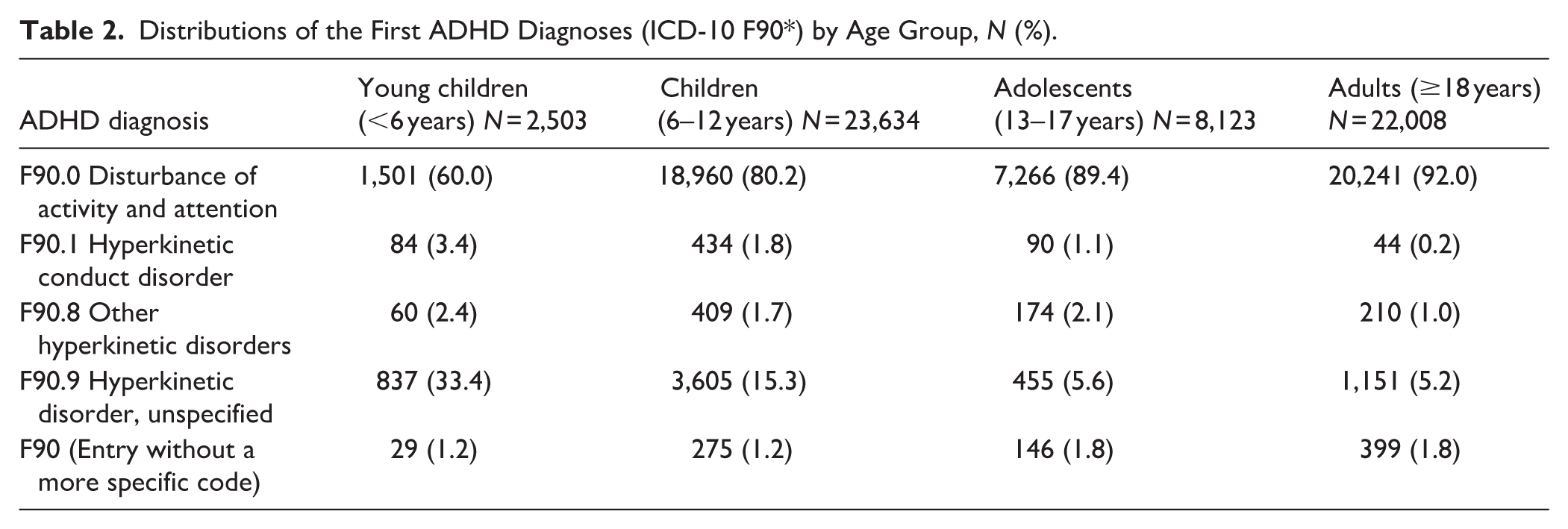
Figure 1 shows monthly health care contacts of diagnosed ADHD patients and their controls 24 months prior to the first ADHD diagnosis. In all age groups, ADHD patients visited health care more often than the controls (Figure 1a), and especially the number of contacts per person was higher in the ADHD patients compared to the controls (Figure 1b). There was an increase in the use of health care services in the ADHD population during the months prior to the ADHD diagnosis. Within the 24 months preceding the ADHD diagnosis, the ADHD population had a higher number of distinct diagnoses (at three-digit ICD-10 level) compared to their controls: an average of 5.6 diagnoses per person compared to 3.3 among the controls.
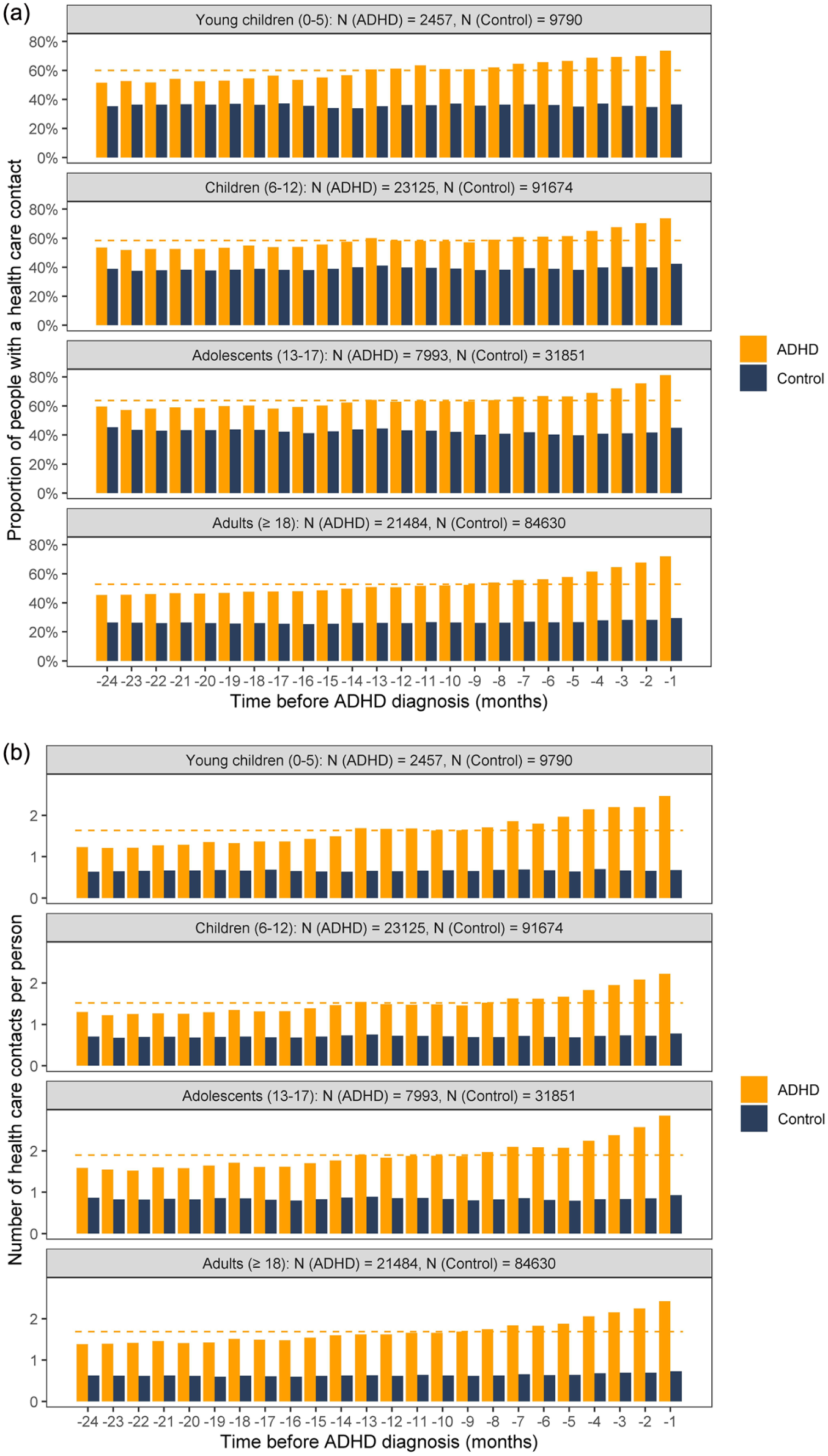
Monthly health care visits and contacts preceding the first ADHD diagnosis for ADHD patients and respectively for matched controls: (a) Proportion of individuals with at least one contact; (b) number of contacts. Dashed line represents the ADHD population average across the considered period.
Proportion of individuals with 12 pre-specified comorbid diagnoses from 3 years before to 3 years after the index date are presented in Figure 2. Among ADHD patients, the prevalence of these comorbid diagnoses was the highest at the time of the index date and decreased or remained similar after that. During the 3 years before the index date, ADHD patients experienced greater increases in the prevalence of each of the 12 pre-specified comorbidities compared to matched controls (Table S1). The greatest absolute increases among ADHD patients were observed for anxiety disorders (half-year change in prevalence 3.2%), unipolar depression and mood disorders (2.7%), learning disabilities or motor coordination disorder (3.0%), and conduct disorders (1.3%). The declines in the prevalence during the period 1 to 3 years after the index date relative to the period −3 to 0 years were the greatest for these same comorbidities. The age group specific prevalences for the pre-specified comorbid diagnoses at −3 to 0 years, 0 to 1 year, and 1 to 3 years from the index date are presented in Tables S2 to S4.
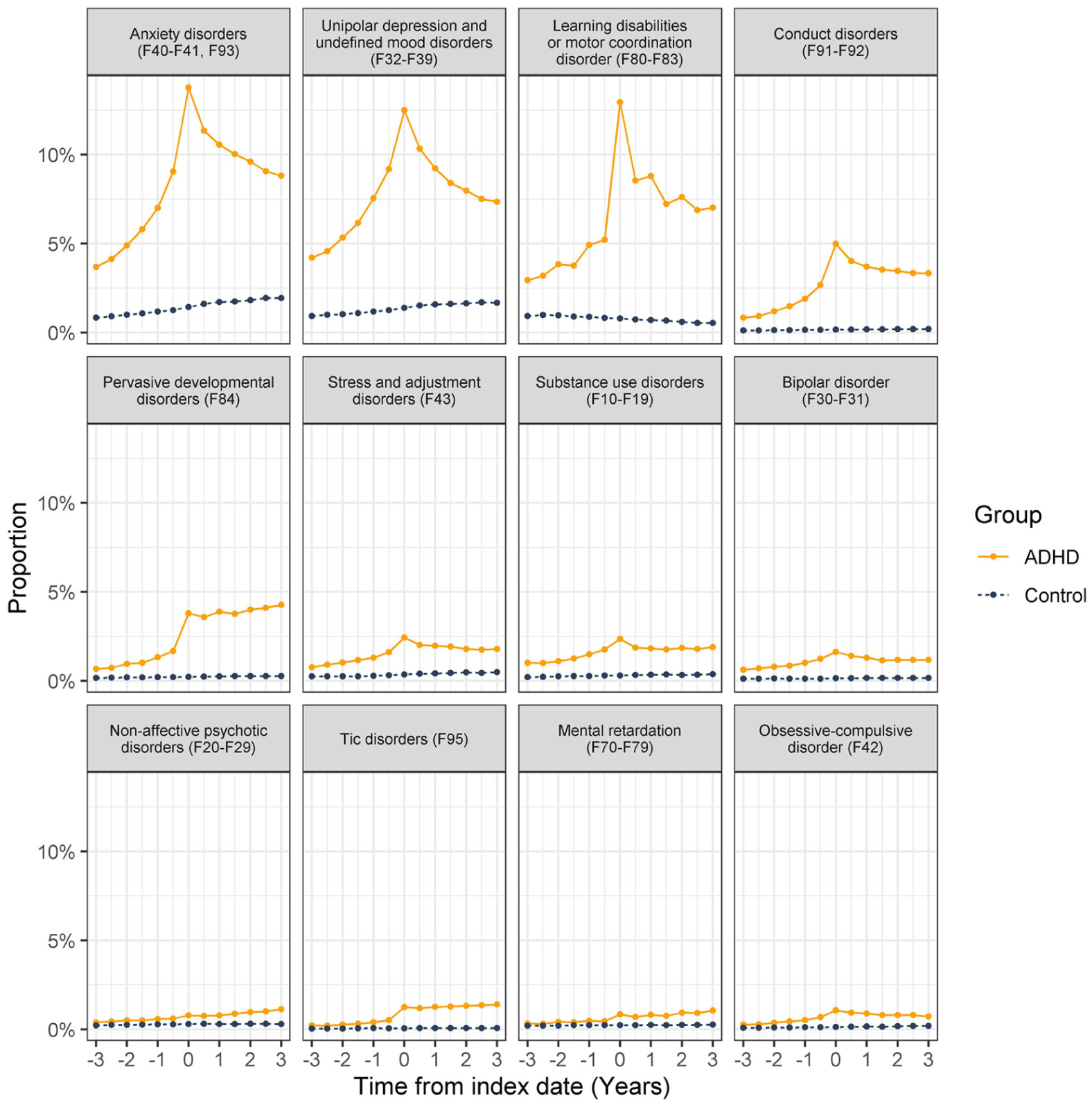
Proportion of ADHD patients and matched controls with pre-specified comorbid diagnoses from 3 years before to 3 years after the individual index date.
Table 3 presents the 15 most common comorbidities observed among ADHD patients during the 3 years preceding the index date, shown for both ADHD patients and their controls. The most common comorbidity, along with four other frequently observed ones, was related to odontology. The top diagnosis was dental caries, which was more common (SMD ≥ 0.10) among ADHD patients compared to their controls in all age groups. In addition, acute upper respiratory infections and asthma were more commonly diagnosed in ADHD patients than in their matched controls, and in the youngest age groups, otitis media and conjunctivitis were also more frequent. Depressive episodes and other anxiety disorders were five times more common in adult ADHD patients than in adult controls, but their occurrence also decreased more in ADHD patients during the follow-up. Abdominal and pelvic pain, and dorsalgia were twice as common in adult ADHD patients as in adult controls.
Proportion (%) of ADHD Patients and Matched Controls With the 15 Most Common Comorbidities (ICD-10, 3-Digit Level) Identified Among ADHD Patients Within 3 Years Prior to the Index Date, Stratified by Age at Index Date, With Group Comparisons Using Standardized Mean Difference (SMD). A Value of SMD ≥ 0.10 Was Considered as an Indication of a Meaningful Difference.
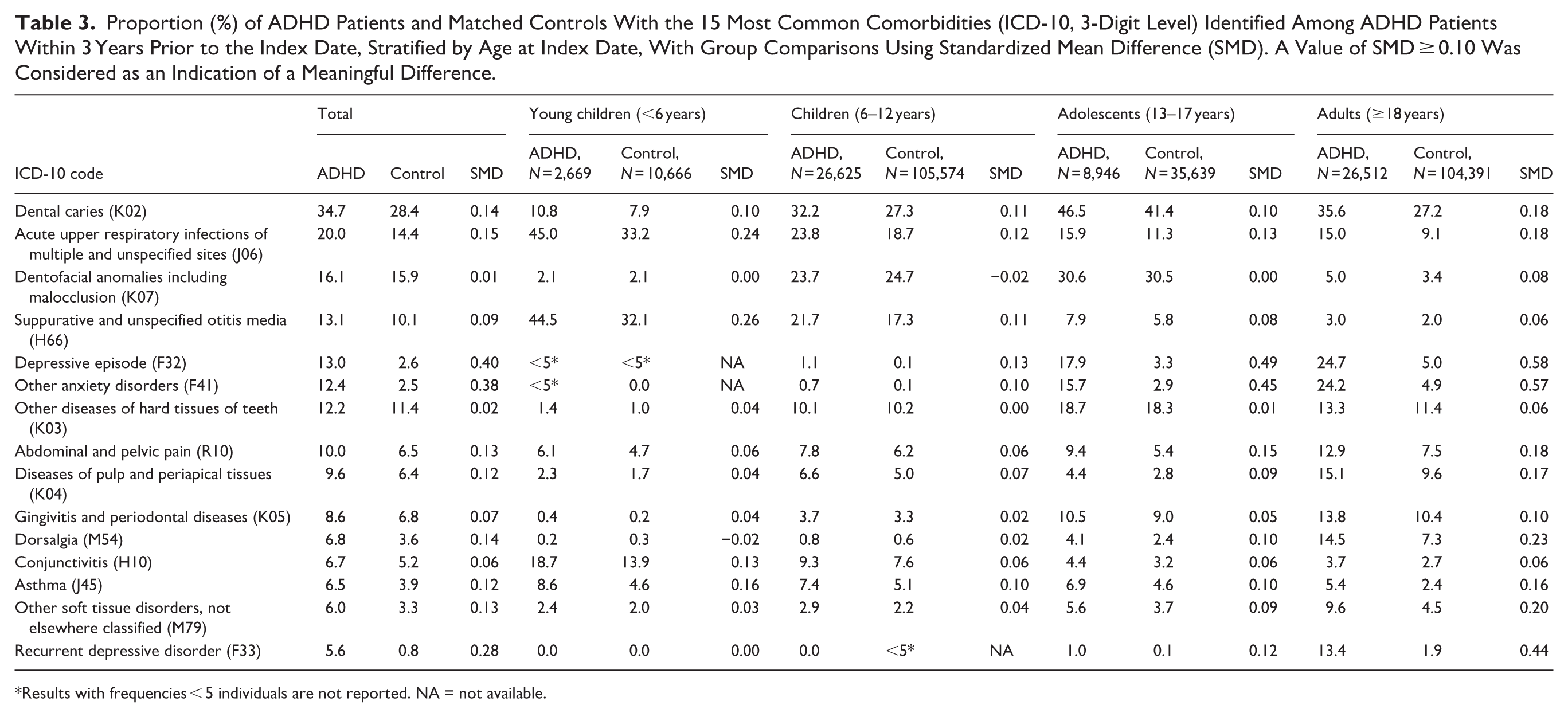
Results with frequencies < 5 individuals are not reported. NA = not available.
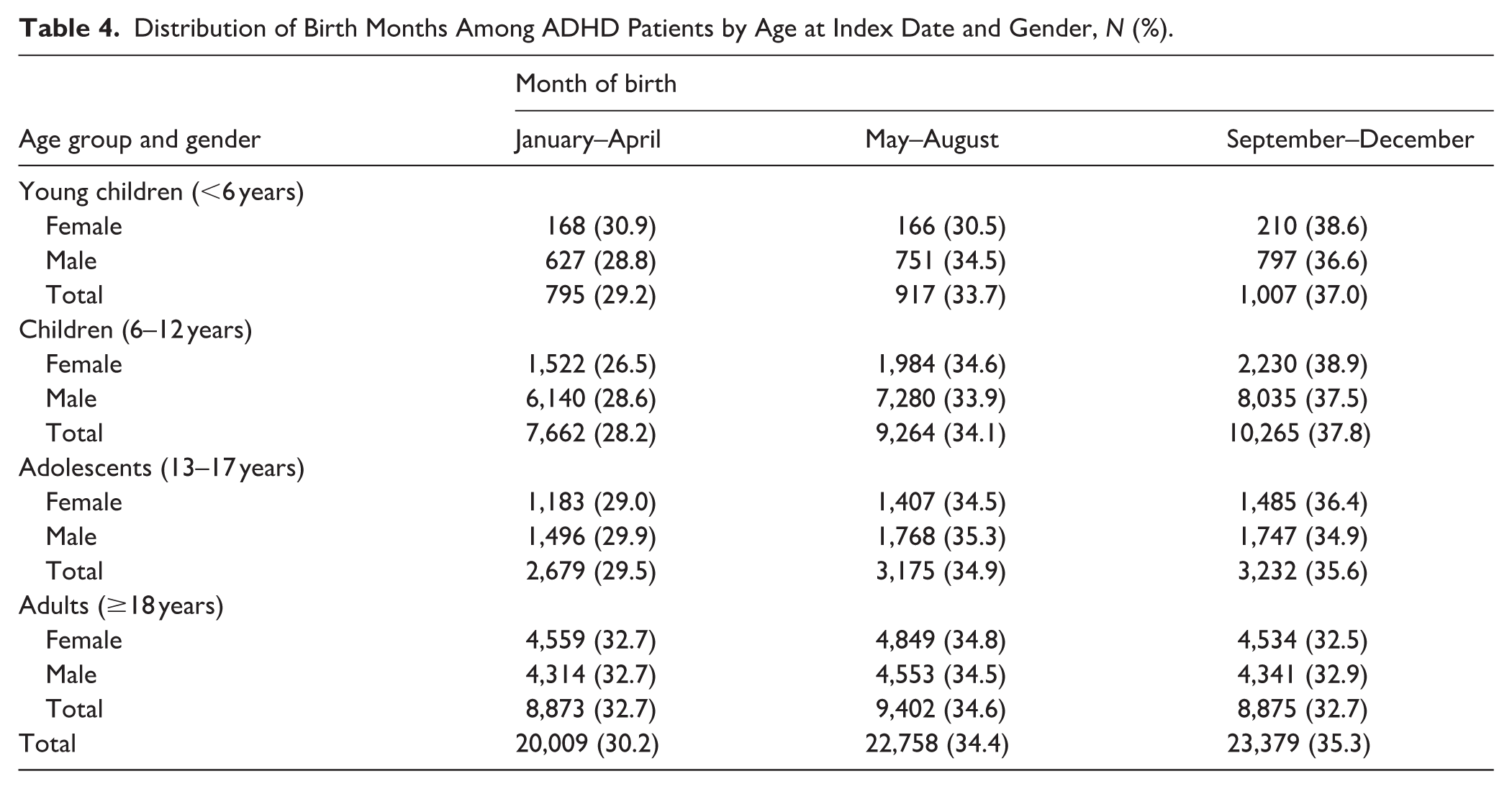
A larger proportion of individuals with ADHD were born in the later months of the calendar year, particularly in the younger age groups (Table 4). Analysis of the ratio of ADHD patients to controls by birth month showed a linear increase in the odds of ADHD across the calendar year in all age groups and both genders (Figure 3). This trend was statistically significant in all other age groups except for young children (<6 years old). The end-of-year effect was detected in all age-gender groups except in girls under 6 years: birth in September–December was associated with statistically significantly increased odds of ADHD compared to birth in January–April (ORs 1.2–1.8, Table 5). In addition, among males under 18 years, those born in May–August had statistically significantly higher odds of ADHD compared to those born in January–April (ORs 1.2–1.4).
Distribution of Birth Months Among ADHD Patients by Age at Index Date and Gender, N (%).
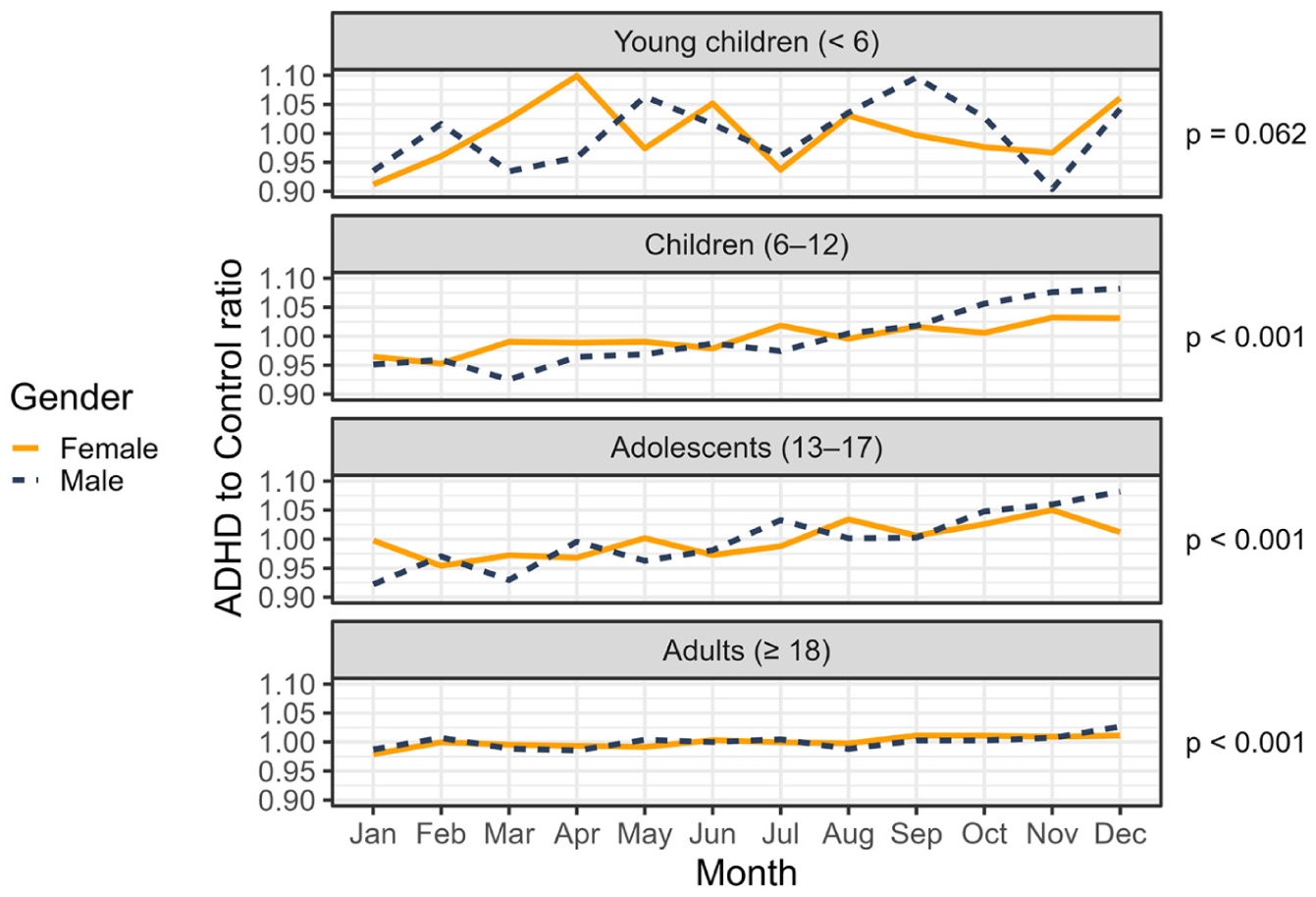
Ratio of individuals with ADHD to their matched controls across birth months, stratified by age at index date and gender, with p-values for increasing trend for each age group.
Conditional Logistic Regression Results for the Likelihood of ADHD by Birth Month Category (Reference: January–April), Stratified by Age Group and Gender.
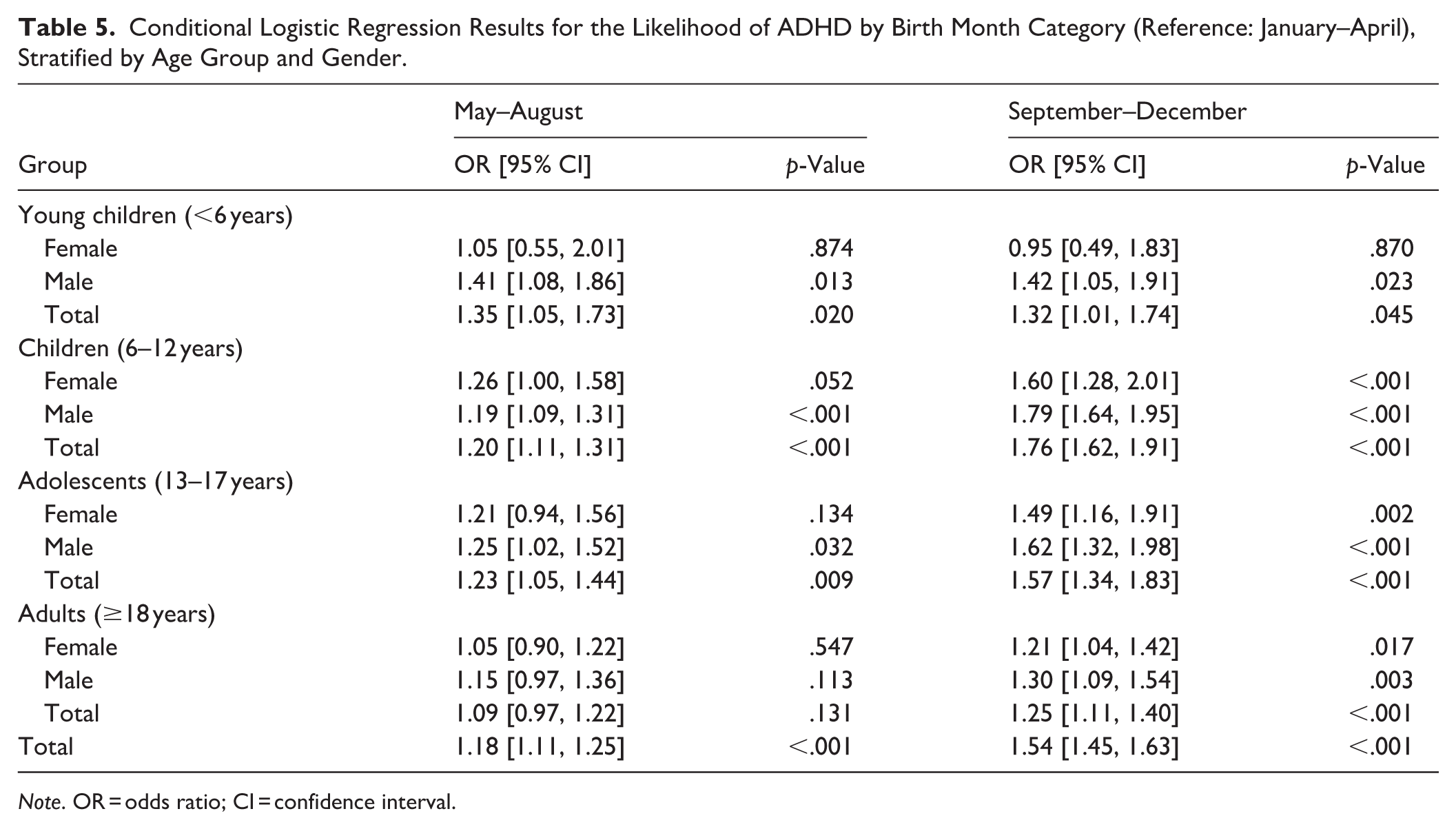
Note. OR = odds ratio; CI = confidence interval.
Discussion
This nationwide cohort study presents ADHD patients’ diagnosis trajectories and compares their comorbidities with a matched control population. The results indicate that females got their ADHD diagnosis at a clearly later age compared to males, and that relative age affected the odds of ADHD especially among males. The health care burden among individuals diagnosed with ADHD was higher than that of controls across all measures – number of contacts, number of people with contacts, and number of diagnoses per person – during the 24 months prior to ADHD diagnosis. A steady increase in health care service use was observed in the ADHD population, especially during the 6 months preceding ADHD diagnosis. This period overlaps with the examination period needed to set the diagnosis. In addition, in the ADHD population, the prevalence of comorbidities peaked at the time of ADHD recognition.
In Finland, linking register data from several national-level registers is possible with a unique identifier for each of about 5.5 million citizens. In our study cohort, we had about 66,000 people with incident ADHD, of which 64% were males. The most often used first ADHD diagnosis code was ICD-10 F90.0, and 95% of these patients maintained this ADHD code without receiving any other ADHD diagnosis. More than half of the males with ADHD were 6 to 12 years old at the time of diagnosis, while more than half of the females were diagnosed at the age of 18 or older. Particularly in girls, the recognition of ADHD may be more difficult due to the presence of symptoms related to other conditions such as anxiety (Auro et al., 2024; Skoglund et al., 2024). It is important to delve into this topic in the future, as anxiety among young females has generally increased remarkably in the recent years (Kiviruusu et al., 2024; Ranta et al., 2024).
Previously, anxiety and depression have been linked with ADHD in adulthood (Ahnemark et al., 2018; Giacobini et al., 2023). They were the most common disorders of the pre-specified comorbidities of interest also in the present study. In our analyses, they were the most prevalent at the time of ADHD diagnosis in the total ADHD population. Depression and anxiety were also present on the list of the 15 most common comorbidities, and they were five times as common in adolescent and adult ADHD patients than in their respective controls.
Beside anxiety and depression, the third most common pre-specified category of comorbidities of special interest was related to learning disabilities highlighted naturally in school-age children. About 20% of the 6 to 12-year-old ADHD patients suffered from these, which is remarkably more than their respective controls. The result is in line with the practice that language and motor difficulties are often identified at the same time with ADHD. At that point, with a comprehensive assessment, the records in the patient registry are the most accurate. Later, learning difficulties may become under-recorded, if they do not affect performance, as visits tend to focus on ADHD. Initiation of ADHD medication may improve a child’s ability to function in school. Occurrence of tic disorders and obsessive-compulsive behaviour did not increase remarkably after ADHD diagnosis.
There is growing epidemiological evidence that ADHD would be linked to inflammatory conditions (Westman et al., 2025b), such as asthma (Cortese et al., 2018), allergic rhinitis, atopic dermatitis, and eczema (Chuang et al., 2022; van der Schans et al., 2017). A cohort study assessing the association between infections from birth to late adolescence, showed that children with infections requiring hospital admission or prescriptions for anti-infective medications had increased risk of later mental disorders and approximately doubled risk of ADHD (Köhler-Forsberg et al., 2019). Also, stimulant medication use has been found to be associated with increased risk of upper respiratory tract infections (Dereschuk et al., 2025). Inflammatory diseases (acute respiratory infections, otitis media, conjunctivitis, and asthma) were among the most common comorbidities also in the present ADHD population, and they were more common in all underaged ADHD patient groups compared to their respective controls. As our study period overlapped with the beginning of the pandemic, we analysed also the prevalence of severe COVID-19 cases requiring emergency care, and found no difference between ADHD patients and controls (data not presented).
Previously, more frequent and multisite pain (headache, stomach pain, musculoskeletal pain) have been reported in children and adolescents with ADHD compared with peers (Mundal et al., 2024). In the present data, abdominal, pelvic, and dorsal pain were prevalent especially in ADHD patients, and they were twice as common in them than in their respective controls. Eating disorders (ICD-10 F50) did not belong to the 15 most common comorbidities but were about twice as common in adolescent ADHD patients than in their respective controls (data not presented). In analyses with all comorbidity data, the biggest differences in prevalences between ADHD patients and their controls were seen in different mental and behavioural disorders (ICD-10 F; more common in ADHD patients) and in pregnancy, childbirth, and the puerperium (ICD-10 O; more common in controls; data not presented).
In Finland, all children start a compulsory, structured 1-year pre-primary education in August the year they turn 6 years old. Respectively, they start school 1 year later, in August the year they turn 7 years old. This applies to the entire country, and individual exceptions are rare. The curriculums for early childhood education and school are nationwide and guide education in the same way across the entire country. ADHD medication use has been shown to be more common among Finnish children and adolescents born in May–August or September–December compared to those born in January–April (Vuori et al., 2020) in a study where ADHD definition was based on reimbursed prescriptions only. It has been suggested that higher use of ADHD medication among those born in the summer or later during the year might be due to unrealistic school expectations related to relative age. In our study, the definition of ADHD included both prescriptions and purchases of ADHD medication, as well as ADHD diagnoses. According to the guidelines, diagnosis before school age and prescribing ADHD medication for patients younger than 6 years of age require extra-careful caution (ADHD: Current Care Guidelines, 2025). Reliable diagnosis is rarely possible before the age of five, and ADHD medications are indicated from the age of 6 years onwards in Finland.
Earlier publications about relative age and school enrolment, and their relationship with ADHD have typically included school-age children and reported differences between the youngest and the oldest in their grade only (Evans et al., 2010; Karlstad et al., 2017; Layton et al., 2018; Morrow et al., 2012). In the present study, an important finding is not only that the children born at the beginning of the year have a lower risk of ADHD, but the risk increases linearly throughout the calendar year. The same phenomenon has been seen in a Swedish setting (Halldner et al., 2014). We observed less prominent but statistically significant linear increase across the calendar year also in adults, although they are not continuously compared with their peers, as children are. This may be at least partly explained by the accumulation of entries in school and healthcare records related to attention difficulties, learning issues, and behavioural problems already in their childhood, even though the formal diagnosis is made only in adulthood. A child’s birthdate has been shown to strongly influence teachers’ assessments of whether the child exhibits ADHD symptoms, suggesting that many diagnoses may be driven by teachers’ perceptions of poor behaviour among the youngest children in a classroom (Elder, 2010). These types of perceptions may have long-lasting consequences. As ADHD diagnosis relies on a relative comparison of children within the same school year, even small age differences can result in significant variation in skills and capabilities. Our results suggest that such an opinion might already occur among daycare staff, which may possibly influence parents to report the matter to health care. Interestingly, almost no relative age effect is seen in Denmark, where the school starting age is more flexible (Kuntsi et al., 2022; Pottegård et al., 2014).
ADHD interferes with multiple areas of life, including academic performance, work, social relationships, and daily routines (Bernardi et al., 2012; Faraone et al., 2021). In the present cohort with ADHD patients of all ages, more than half of the females received their ADHD diagnosis as adults, whereas males were commonly diagnosed during childhood. A previous register study showed that females received their diagnosis approximately 4 years later than males and were more likely to have psychiatric comorbidities both before and after their ADHD diagnosis (Skoglund et al., 2024). This later recognition of ADHD in women may be related to suggestion that the presentation of ADHD symptoms would differ between genders, girls being less hyperactive or impulsive but rather inattentive and emotionally sensitive (Cortese, Faraone, et al., 2016; Faheem et al., 2022; Gershon, 2002; Mowlem et al., 2019). Overlapping symptom profiles with other psychiatric conditions may lead to under-recognition of ADHD symptoms and make differential diagnosis challenging. Furthermore, it has been suggested that the diagnostic criteria of ADHD have been set according to the presentation of symptoms in boys (Gaub & Carlson, 1997; Mowlem et al., 2019; Nussbaum, 2012). The diagnostic assessment has also been criticised to be subjective, despite the use of interviews, screening tools and rating scales (Faraone et al., 2021).
In conclusion, based on health care contacts, ADHD is associated with a significant burden across all age groups even before the 6-month pre-diagnostic assessment period. In young children, it is important to consider that factors such as recurrent infections may signal the presence of underlying ADHD. In adolescents and adults, it is particularly important to pay attention to factors that may manifest as anxiety or depressive symptoms, and to assess the potential contribution of ADHD to these presentations. Furthermore, our study provides novelty value in insights regarding the impact of birth month on ADHD diagnosis. Birth month is associated with ADHD diagnosis already before preschool when relative age-related demands should not yet occur.
Limitations
Information from private health care, which in great part organises occupational health care in Finland, has been missing from nationwide register data until 2020. Due to this, we may have missed diagnoses of adult patients. However, in the cohort identification, we considered ADHD medication as inclusion criteria too, so all patients with ADHD medication are reliably included in our study population.
ADHD diagnosis was defined as ICD-10 F90* and thus we did not consider ICD-10 F98.8 Other specified behavioural and emotional disorders with onset usually occurring in childhood and adolescence as ADHD in the cohort identification. However, ADHD medication was considered in the inclusion criteria. There were only 680 patients (1%) in our cohort with ADHD medication and the code F98.8 without any F90 code.
Future Directions
In the future, our aim is to investigate mortality and causes of death among ADHD patients compared to their matched controls.
Supplemental Material
sj-docx-1-jad-10.1177_10870547261451069 – Supplemental material for ADHD Diagnosis Patterns: Comorbidities and the Impact of Relative Age on Diagnosis Likelihood
Supplemental material, sj-docx-1-jad-10.1177_10870547261451069 for ADHD Diagnosis Patterns: Comorbidities and the Impact of Relative Age on Diagnosis Likelihood by Elisa Westman, Tuire Prami, Alvar Kallio, Ilona Iso-Mustajärvi, Essi J. Peltonen, Joel Jukka, Paavo Raittinen, Maarit J. Korhonen, Anita Puustjärvi and Sami Leppämäki in Journal of Attention Disorders
Footnotes
Acknowledgements
We thank MSc Pharm Hilkka Ylinärä from Oriola for her kind and valuable help in applying the study permits. PhL Jussi Harmanen is acknowledged for conducting analysis quality check. We also wish to thank PhD Teri Kanerva from Takeda Oy for constructive commenting of the manuscript.
ORCID iDs
Author Contributions
The authors contributed the work as follows: Conceptualisation: EW, JJ, AP, SL; Data curation: AK, PR; Formal Analysis: AK, EJP, PR; Funding acquisition: EW, JJ; Investigation: EW, TP, II, JJ, MJK, AP, SL; Methodology: TP, EJP, PR, MJK; Project administration: EW, II; Resources: EW, II; Software: AK, PR; Supervision: MJK, AP, SL; Validation: PR, MJK; Visualisation: AK, EJP; Writing – original draft: EW, TP, AK, PR; Writing – review & editing: II, EJP, JJ, MJK, AP, SL. All authors have contributed to the manuscript substantially and fully meet the criteria 1 to 4 of the International Committee of Medical Journal Editors (ICMJE) for authorship. They have agreed to the final submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Takeda Oy.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EW and JJ are employees of Takeda Oy but have no Takeda stock or stock options. TP, AK, II, EJP, PR, and MJK are employees of Oriola, and Oriola received research funding for this study by Takeda Oy. AP has received consultation fees from Takeda and Biocodex and SL from Takeda, Lundbeck and Janssen.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.