
Abstract
Objective:
The purpose of this study was to examine the acceptability, feasibility, and replicability of a manualized group cognitive-behavioral intervention designed to enhance executive self-management in college students with ADHD. Whereas the first trial of this intervention was conducted in a private university in a small city in the Netherlands, the current open trial was administered at an urban, public college in the northeast United States. A simultaneous goal of the study was to train PhD-level psychologists to administer the intervention.
Methods:
Forty-one students meeting rigorously assessed DSM-5 criteria for ADHD were enrolled in one of six 12-week treatment groups that addressed time-management, organization, and planning, and also targeted procrastination, distractibility, and negative automatic thoughts. Strategies were also included to improve attention to and retention of reading materials and guidance in organizing and writing essays. Each group was co-led by an experienced therapist and one of three clinical psychologists undergoing training. Pre- and post-treatment measures included number and severity of inattentive and hyperactive-impulsive symptoms as assessed on a structured diagnostic interview (AISRS) and via a self-report (CAARS) questionnaire, as well as measures of executive skills (BRIEF-A, LASSI-III). At the end of treatment, students rated the helpfulness of each of the program’s components and strategies, and provided a personal narrative of the most important effects of the program on their daily functioning and personal well-being.
Results:
Thirty-six of the 41 enrollees fully or partially completed the treatment and provided post-treatment data for the analyses. Repeated measures ANOVA yielded significant main effects for decreases in clinician-rated and self-rated number and severity of inattentive symptoms. Change in executive self-management was associated with change in ADHD Inattention severity after controlling for pre-treatment inattention. Significant improvement was also observed on the BRIEF-A Metacognitive Index and LASSI-III composite score. Overall, 67% of students rated the group program as “very helpful” and 30% as “moderately helpful.”
Conclusions:
The results of this study demonstrate the feasibility and acceptability of the intervention. Pre- to post-treatment reductions in clinician- and self-rated ADHD symptoms and executive self-management skills were observed, although, of course, conclusions regarding efficacy/effectiveness cannot be drawn from uncontrolled trials. This replication of the group CBT intervention in a public, urban setting, with training of interventionists, supports the feasibility of the treatment, and warrants a large-scale randomized controlled trial against an active control group to evaluate efficacy, with potential for dissemination across college campuses generally (ClinicalTrials.gov ID NCT05588505).
Introduction
ADHD has a pronounced negative impact on the academic performance and emotional well-being of college students (Ramsay & Rostain, 2015; Thomas et al., 2013). The most recent National College Health Assessment Survey, of 103,639 undergraduates found that 13.8% self-reported ever having been diagnosed by a professional as having ADHD (American College Health Association, 2024). College students with ADHD withdraw from more courses (C. Advokat et al., 2011), have lower GPAs (C. Advokat et al., 2011; C. D. Advokat et al., 2008; Blase et al., 2009 ; DuPaul et al., 2021), are more likely to be placed on academic probation (Heiligenstein et al., 1999), and are less likely to graduate (Barkley et al., 2006; Gormley et al., 2016). A longitudinal study of 45,000 first-year college students, including 2,000 students with ADHD, found that a previous ADHD diagnosis predicted lower first-year grades; an effect mediated by “academic adjustment,” which included time-management, study skills, and adjusting to college academic demands (Carroll et al., 2025).
Although stimulant medication is effective in reducing ADHD symptoms in children and adults (Barkley, 2014a), research in college students is limited. Cross-sectional studies show no association between stimulant use and improved symptoms or impairment (Blase et al., 2009; Rabiner et al., 2007). Lisdexamfetamine reduced ADHD symptoms and executive dysfunction in a small randomized, placebo-controlled study (DuPaul et al., 2011); however, sizable differences in both domains persisted in those with ADHD compared to controls. Low adherence (Nguyen et al., 2025) and high rates of stimulant diversion and misuse on college campuses (Molina et al., 2020) further limit the utility of pharmacological treatment. These limitations underscore the need for effective non-pharmacological interventions targeting ADHD symptoms and ADHD-related executive dysfunction.
Executive Dysfunction in ADHD
Executive dysfunction is a critical contributor to academic difficulties in ADHD (DuPaul et al., 2021). Multiple studies have shown differences between children and adults with and without ADHD with respect to executive functioning (Willcutt et al., 2005), which includes the component processes of working memory, tracking and shifting tasks, self-monitoring, self-inhibition, organization, planning, problem-solving, effort allocation, temporal discounting, and emotional self-regulation (Barkley, 2012). In adult ADHD, these manifest as poor organization, planning, and task initiation and completion. College demands – for independent self-care, regular attendance, and long-term academic planning – magnify these challenges. Students with ADHD often must manage increased demands without the prior supports of parents and teachers. The college environment also presents more distractions – including socializing, substance use, and digital media. Individuals with ADHD tend to prioritize immediate rewards over delayed academic benefits (Jackson & MacKillop, 2016; Scheres et al., 2013), a tendency associated with weaker study strategies (Scheres & Solanto, 2021). Consequently, college represents a crucial period for intervention targeting executive skill development.
Psychosocial Treatment of Executive Dysfunction in Adults With ADHD
Cognitive-behavioral interventions for adults with ADHD have demonstrated significant benefits in both individual (Safren et al., 2010) and group formats (Solanto et al., 2010), and in adults receiving (Safren et al., 2010) and not receiving (Solanto et al., 2010) concurrent medication. These programs address poor time-management and planning, as manifested in procrastination, missed deadlines, inadequate or inaccurate work, inefficiency, and failure to plan. Meta-analyses confirm that CBT reduces symptoms of ADHD (Liu et al., 2023; Young et al., 2020), augments the effects of stimulant medication (Li & Zhang, 2024), and reduces comorbid internalizing symptoms (López-Pinar et al., 2020). A recent umbrella meta-analysis documented that CBT was the most effective non-pharmacological treatment for ADHD in adults, based on both self-rated and clinician-rated core ACHD symptoms (Gosling et al., 2025).
Status of CBT Intervention for ADHD on College Campuses
Recent efforts have adapted CBT for the college context. A 12-session, 2-hr group CBT open trial in the Netherlands improved structured clinical interview-based ADHD symptoms and self-reported executive self-management (Solanto & Scheres, 2021). Another open trial of a six-session group intervention also reported promising results (Hartung et al., 2022). Anastopoulos and colleagues conducted a randomized controlled trial (RCT) of their ACCESS program, which included eight group sessions and six sessions of individual mentorship, followed by a one-semester “maintenance” phase of reduced treatment. Results yielded improvements in questionnaire self-reports of ADHD symptoms, executive function, and cognitive mechanisms, with gains maintained through the second semester, although academic outcomes did not improve (Anastopoulos & King, 2015; Anastopoulos et al., 2021; Eddy et al., 2021). The SUCCEEDS program, initiated by Andrea Chronis-Tuscano et al., which integrates motivational interviewing and organizational-skills training, also shows promise (Meinzer et al., 2020).
Availability of CBT Intervention for Adult ADHD
A recent study conducted by the U.S. Centers for Disease Control estimated a prevalence of 6% of ADHD among U.S. adults, of whom one-third were receiving stimulant treatment alone, one-third were receiving both stimulants and “counseling,” and the remaining third were receiving no treatment (Staley et al., 2024). Lack of availability of psychologist-providers of CBT specialized for ADHD has been cited as one reason for under-treatment (Rout et al., 2026). Informal survey reveals a comparable dearth of psychological interventions for ADHD on U.S. college campuses, and a corresponding need to develop a treatment that is both effective and scalable to the college setting.
Contributions of the Current Study
The current study builds on this growing literature. Pre-post treatment change was assessed on a structured diagnostic interview, rather than solely on self-report, thereby reducing expectancy effects. The 12-session structure allowed for more extensive presentation and practice of executive self-management strategies, including application to academic skills such as reading and writing. Dedicated sessions targeted negative automatic beliefs common among students with ADHD. The longer (2-hr) session format supported individualized feedback, group support, and positive modeling. This intensive structure may enhance overall treatment impact.
Growing demand for ADHD services on campuses underscores the need for scalable EF-based interventions. Therefore, the current study aimed to:
Replicate the initial study, conducted with college students at a private university in the Netherlands (Solanto & Scheres, 2021), in an open trial with students at a public, 4-year college in the Northeast United States.
Evaluate the feasibility and acceptability of the treatment, on the basis of attendance at the group sessions, and completion of the home exercise.
Examine pre-post change in core ADHD symptoms and executive skills, as assessed by structured diagnostic interviews and standardized self-report measures.
Obtain the participants’ ratings of the helpfulness of: each session and strategy presented; the group processes, and the overall helpfulness of the program.
Begin to develop a program to train Ph.D.-level clinical psychologists to deliver the intervention.
Method
Eligibility Criteria
Participants were undergraduate students recruited from an urban, public, 4-year college in New York City. Participants were 18- to 30-years-old, achieved a severity score ≥9 on a brief telephone screen for ADHD (ASRS v1.1), and after a comprehensive evaluation, met DSM-5 criteria for ADHD, Predominantly Inattentive or Combined Presentations. Participants were excluded if they had experienced childhood trauma that precluded determination of the presence of ADHD symptoms in childhood. Exclusion criteria included: autism spectrum disorder (ASD); borderline personality disorder, neurological disorder (e.g., seizure disorder) or traumatic brain injury; and suicidal ideation (including passive ideation) within the past year and/or attempted suicide after 12 years of age. Participants with a serious psychiatric condition (e.g., severe anxiety or depression) with treatment priority were excluded. Participants were also excluded if they exhibited overtly hostile or aggressive behavior that was likely to alienate other group members. Participants receiving ADHD medication were required to have been receiving medications for at least 2 months and on a stable dose for at least 1 month (See Figure 1). Participants were informed that if accepted into the study, they would be asked to not make changes in any medication or psychological therapy during the course of the group treatment unless clinically necessary, in which case they were asked to notify the investigators.
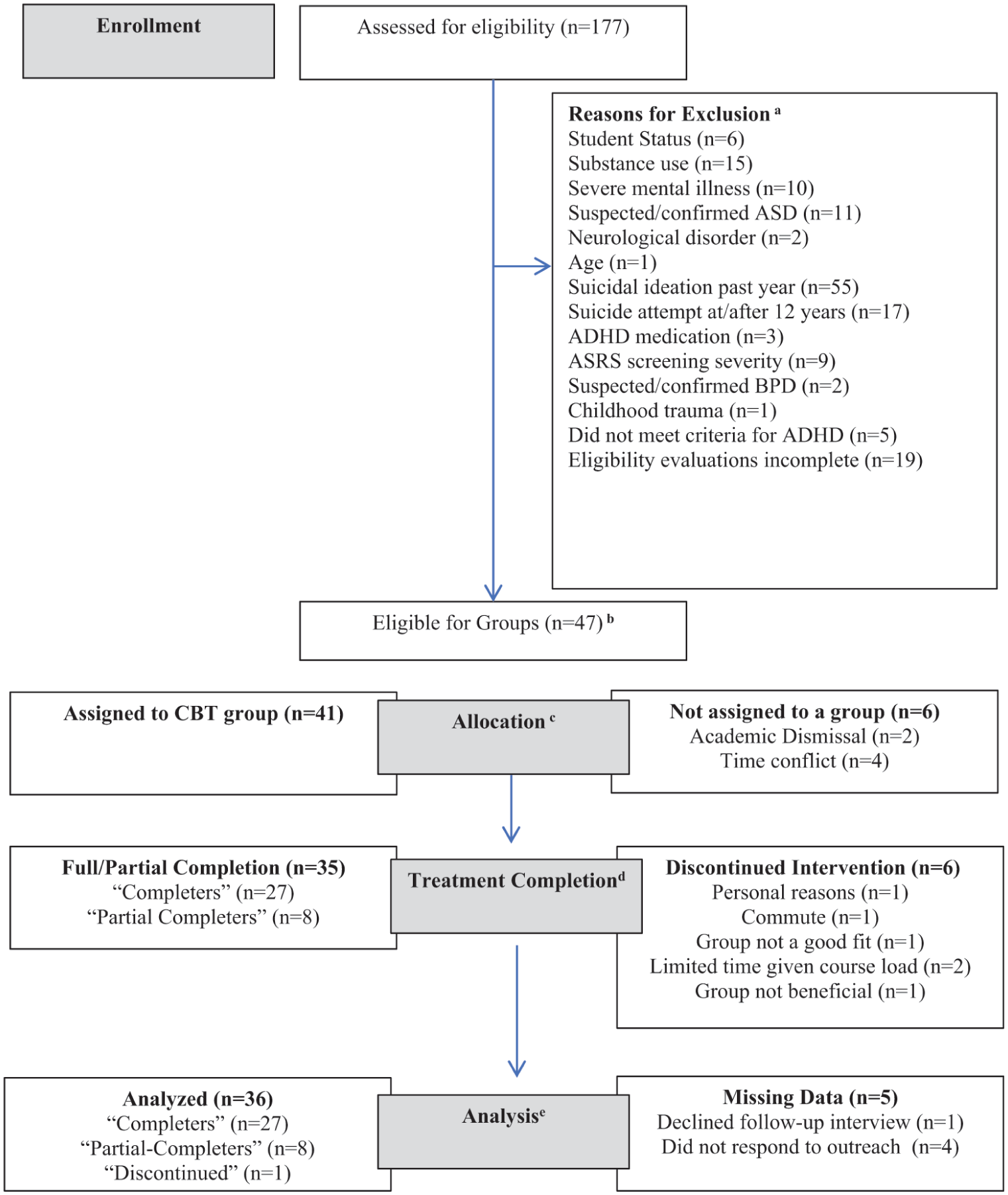
CONSORT flow diagram.
Recruitment
Information about the study was sent to all undergraduate students via email and flyers were posted around campus. Students were referred to the study via: the CCNY Counseling Center, Psychological Center, Student Disability Services, and departmental academic advisors or faculty. Students also learned about the study from friends or other students who had participated.
Phone Screen
After providing informed oral consent to complete telephone screening, students responded to the six screening items of the World Health Organization Adult ADHD Self-Report Scale (ASRS v1.1) (Kessler et al., 2007). Individuals with scores ≥9 were eligible to continue. Students self-reported demographic information and answered preliminary questions regarding eligibility criteria (e.g., ADHD medication use, mental health history, substance use, etc.).
Screening Questionnaires
Individuals who remained eligible after the phone screen completed written informed consent to undergo further evaluation via questionnaires and interviews and, if eligible, to participate in the intervention. The Beck Depression Inventory-2nd edition (BDI-II) (Beck et al., 1996) assessed presence and severity of depression and suicidality. ASD was assessed via the Autism Questionnaire (AQ) (Baron-Cohen et al., 2001). Participants who received a score ≥32 were interviewed by one of the three investigators using the ASD module of the Mini-International Neuropsychiatric Interview – English Version 7.0.2 (MINI) (Sheehan et al., 1998). Participants completed the Alcohol Use Disorders Identification Test (AUDIT, Saunders et al., 1993) and the Drug Use Disorders Identification Test (DUDIT, Berman et al., 2005) to screen for harmful alcohol and other drug use, respectively. The 10-item AUDIT and 11-item DUDIT assess consumption, dependence and impairment consequent to use. Responses are summed, with AUDIT scores ≥8 and DUDIT scores ≥2 for women and ≥6 for men indicating high risk for harmful use. For those students, follow-up was conducted with the Substance Use module of the MINI (Sheehan et al., 1998); those who met DSM-5 criteria for a substance use disorder were excluded.
Individuals who remained eligible completed baseline pre-treatment questionnaires assessing ADHD severity (CAARS), executive skills (BRIEF-A) and knowledge and use of study skills and strategies (LASSI-III).
Diagnostic Assessment of ADHD
Participants who remained eligible through the screening described above completed a formal diagnostic evaluation of ADHD severity with one of the three investigators using two structured diagnostic interviews. The Adult ADHD Investigator Symptom Rating Scale (AISRS) (Spencer et al., 2009) was administered first. Presence of ADHD in childhood by age 12, as required by the DSM-5 (American Psychiatric Association, 2022), was assessed using the childhood module of the Adult ADHD Clinical Diagnostic Scale (ACDS) (Kessler et al., 2010).
For both the AISRS and the ACDS, clinicians rated each item on a 0 (not present) to 3 (severe) scale. Any item rated 2 or 3 was considered to pass threshold and was counted as a symptom. The number of inattentive and hyperactive/impulsive symptoms passing threshold was counted to generate number of symptoms in each domain. Individual item ratings were also summed to obtain severity scores separately for inattention and hyperactive/impulsivity.
In cases in which it was not possible to fully assess childhood symptoms due to the participant’s uncertainty or inability to remember, participant consent was sought to speak to the parent or another adult who knew the student well in childhood. Parents/caregivers were asked to complete the Childhood Symptoms Scale-Other Report Form (Barkley & Murphy, 1998) over the telephone and their reports were integrated with the student report, such that the parent report of the symptom superseded the student’s self-report of childhood symptoms.
Diagnostic Assessment of Comorbid Psychopathology
Each eligible participant met individually with one of the investigators to complete the MINI, English Version 7.0.2 (Sheehan et al., 1998) to assess comorbid DSM-5 diagnoses. The SCID-II Borderline Personality Disorder module (First et al., 1997) was also administered to anyone for whom borderline personality disorder was suspected. All individuals were also administered the screening version of the Columbia Suicide Severity Rating Scale, a 6-item measure to aid in determination of risk level of self-harm (Bjureberg et al., 2021).
Outcome Measures
ADHD Symptoms
The AISRS was repeated post-treatment (by the same evaluator who had conducted the pre-treatment interview) to ascertain changes in number and severity of inattentive and hyperactive-impulsive symptoms. In addition, the Conners Adult ADHD Rating Scale – Long Version Self-Report (Conners et al., 1999; Erhardt et al., 1999) was administered pre- and post-treatment to ascertain change in self-report of ADHD and related symptoms.
Executive Self-Management
Two measures were administered before and after treatment to assess changes in students’ executive self-management:
Feasibility and Acceptability
Students’ attendance at each of the Group sessions (including time of arrival) and their completion of the previous week’s Home Exercise (None, Partial, Complete) were documented by group leaders. In addition, students rated the helpfulness of the previous week’s session, which was reviewed by the clinician-investigators at the weekly supervisory meetings. At the end of the treatment program, students rated the helpfulness of each session, the key strategies presented, and the Group process using a 4-point Likert scale (0 = “Not at all Helpful”; 3 = “Very Helpful”).
Intervention
Six group cohorts comprising an average of seven students each (SD = 1) were conducted over four semesters. Each group met for 2 hr, once per week for 12 weeks during the course of an academic semester. Each group cohort was jointly led by the first author (psychologist) and one of the three PhD-level clinical psychologists who were undergoing in vivo training to deliver the intervention. Training was also conducted by the first author via several preliminary background lectures about ADHD in adults, and by review and discussion of the manualized intervention material during a 1-hr meeting with the trainees that preceded each group session. The sessions were also observed via ZOOM by the second senior author (psychiatrist). Each group session was followed by a supervisory meeting between the group leader undergoing training and the three senior clinician- investigators to review and discuss the process and results of the previous evening’s session, and make any needed adjustments to the protocol.
The design of this manualized intervention was guided by several foundational principles and practices. First, a small group format was chosen in order to allow for intensive feedback, guidance, and positive reinforcement from group leaders, while also providing critical opportunities for peer support and positive modeling of successful strategies. Second, the program aimed to impart explicit skills and to promote development of the corresponding habits necessary for successful executive self-management – for example, regular use of a planner. A third component was to impart “rules” (adaptive internal speech) to guide daily scheduling, prioritizing, self-activation, and organization. Some of these were crystallized as “mantras” which were repeated strategically throughout the program in order to facilitate internalization and maintenance as guides to self-management. An example is, “If I’m having trouble getting started, then the first step is too big,” which cues both the stimulus situation (procrastination) and the adaptive response (break the task down into more manageable chunks). Other strategies presented and promoted in the program included positive self-reinforcement contingent upon completion of difficult or aversive tasks, strategies for avoiding or overcoming distractions, and visualization of long-term rewards of present behavior (e.g., studying now to get a good grade in the course later, a good job after college etc.) to counteract temporal discounting. Two sessions were devoted to identifying and challenging automatic negative (irrational) beliefs. Finally, three sessions were devoted to development of academic skills related to reading actively for retention, and organizing, writing, and presenting academic papers.
Session Format
At the start of each session, each student completed the Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001) to assess severity of depression over the past week, including the presence of suicidal ideation. Any student who endorsed suicidal ideation met individually with one of the group leaders at the conclusion of the group for a risk assessment, and resources were provided as needed. At this time students also completed a question inquiring about whether there had been any change in their pharmacological or non-pharmacological treatment since the previous week.
The first hour of each group session was dedicated to a round-table review of the results of the previous week’s home exercise with each participant, during which successive approximations to the desired behavior(s) were identified and positively reinforced, and sources of difficulty were explored and resolved with suggestions for future more adaptive responses. Contributions of other group members were welcomed during this part of the session.
The second hour of the session was devoted to presentation and discussion of the week’s topic and associated strategies, as outlined in the manualized material. The rationale for each strategy was presented via the Socratic Method, following which students practiced the strategy via an in-group exercise. The session closed with a review of the home exercise for the upcoming week with anticipatory trouble-shooting of potential difficulties.
Program Content
The program comprised 12 sessions (See Table 1), covering psychoeducation about ADHD, self-care (e.g., sleep), time-management and other executive self-management skills, and academic skills. Two sessions were devoted to cognitive reframing to identify and challenge negative automatic beliefs and thereby counter anxiety, low mood, perfectionism, and low self-esteem, which may have developed over a lifetime of negative feedback and failure experiences. In keeping with the iterative nature of program development, and as displayed in Table 1, some changes were made in course content and session order on the basis of student feedback.
Session Content.
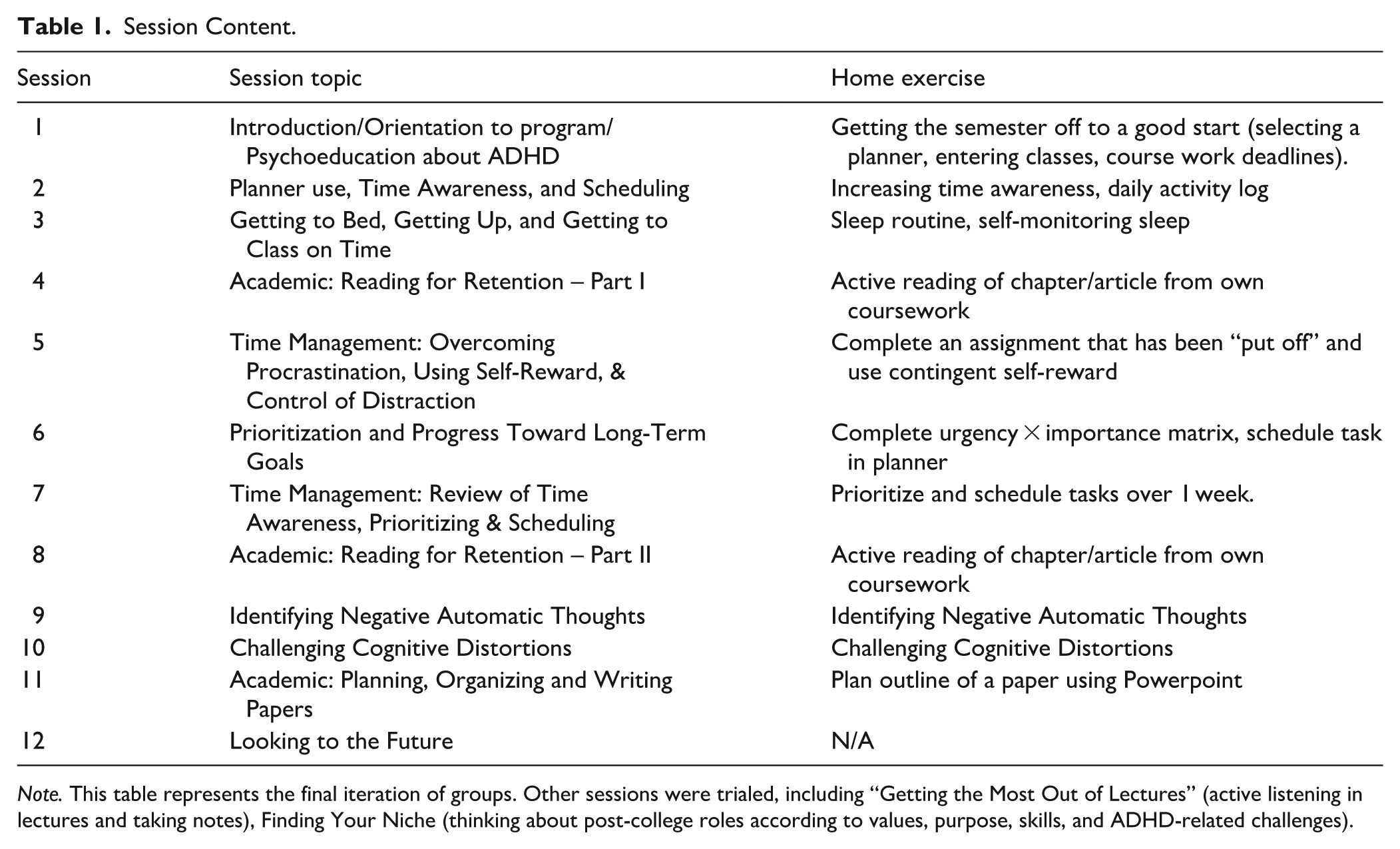
Note. This table represents the final iteration of groups. Other sessions were trialed, including “Getting the Most Out of Lectures” (active listening in lectures and taking notes), Finding Your Niche (thinking about post-college roles according to values, purpose, skills, and ADHD-related challenges).
Compensation and Ethics
Individuals who completed all evaluation procedures received a written report of the results of the evaluation. Participants who completed the post-treatment clinician-administered interview about their ADHD behaviors were compensated with $25 in cash. All study procedures were reviewed and approved by the Institutional Review Boards of the City University of New York (CUNY) University Integrated Institutional Review Board (CUNY-UI IRB) (Protocol #2022-0008), Feinstein Institutes for Medical Research – Northwell Health IRB (Protocol #20-0013), and Cooper Health IRB (Protocol #22-019).
Attrition
Forty-seven students were eligible for enrollment in the study. Six students were not allocated to a group because their schedules conflicted with the time the groups were being offered, or they were academically dismissed in the period between completing the evaluation and the start of the groups. Forty-one students were each allocated to the next available group in the order in which they qualified for the study. Twenty-seven students “completed” the intervention, defined as attending at least 9 of the 12 sessions for at least one hour. A further eight were “partial completers,” in that they attended fewer than nine sessions, and six students formally withdrew. The post-intervention clinical interviews were carried out with 36 of the 41 participants, and are included in the final analyses, consistent with an “intent-to-treat” approach (see Figure 1).
Statistical Analyses
Data were analyzed using SPSS-version 30. Differences in ADHD severity, and EF from pre- to post-intervention were analyzed using repeated measures analysis of variance (ANOVA). A repeated measures multivariate analysis of variance (MANOVA) was carried out with the six LASSI-III subscales as the dependent variables. Follow-up univariate repeated measures analyses of variance were conducted for significant subscales to determine whether change was observed in specific skills. The Holm-Bonferroni method was used to adjust for multiple testing (Holm, 1979). Effect size for all variables was reported as partial eta squared (ηp²), and also as Cohen’s dz (i.e., Cohen’s d for repeated measures) to facilitate comparisons across studies.
Linear regression analyses were carried out to determine whether change in EF was related to post-intervention Inattention or Hyperactivity/Impulsivity symptom count or severity (measured using the AISRS) after accounting for these same measures pre-intervention.
Feasibility and acceptability of the intervention were assessed using frequency of participants who attended at least 9 of the 12 sessions for at least 60 min and who completed home exercises, as well as mean (SD) helpfulness of each session and each strategy. Last, participants’ written narrative responses regarding the single factor (if any) that changed the most following participation in the groups were examined for common themes.
The outcome analyses were conducted in two ways: with the entire sample of 36 with whom post-treatment measures were carried out (consistent with an “intent to treat” model) (see Table 2) and, second, with the sample of 27 who were designated as treatment “completers” (see Table 3).
Pre- and Post-Treatment Measures of ADHD and EF (Entire Sample).
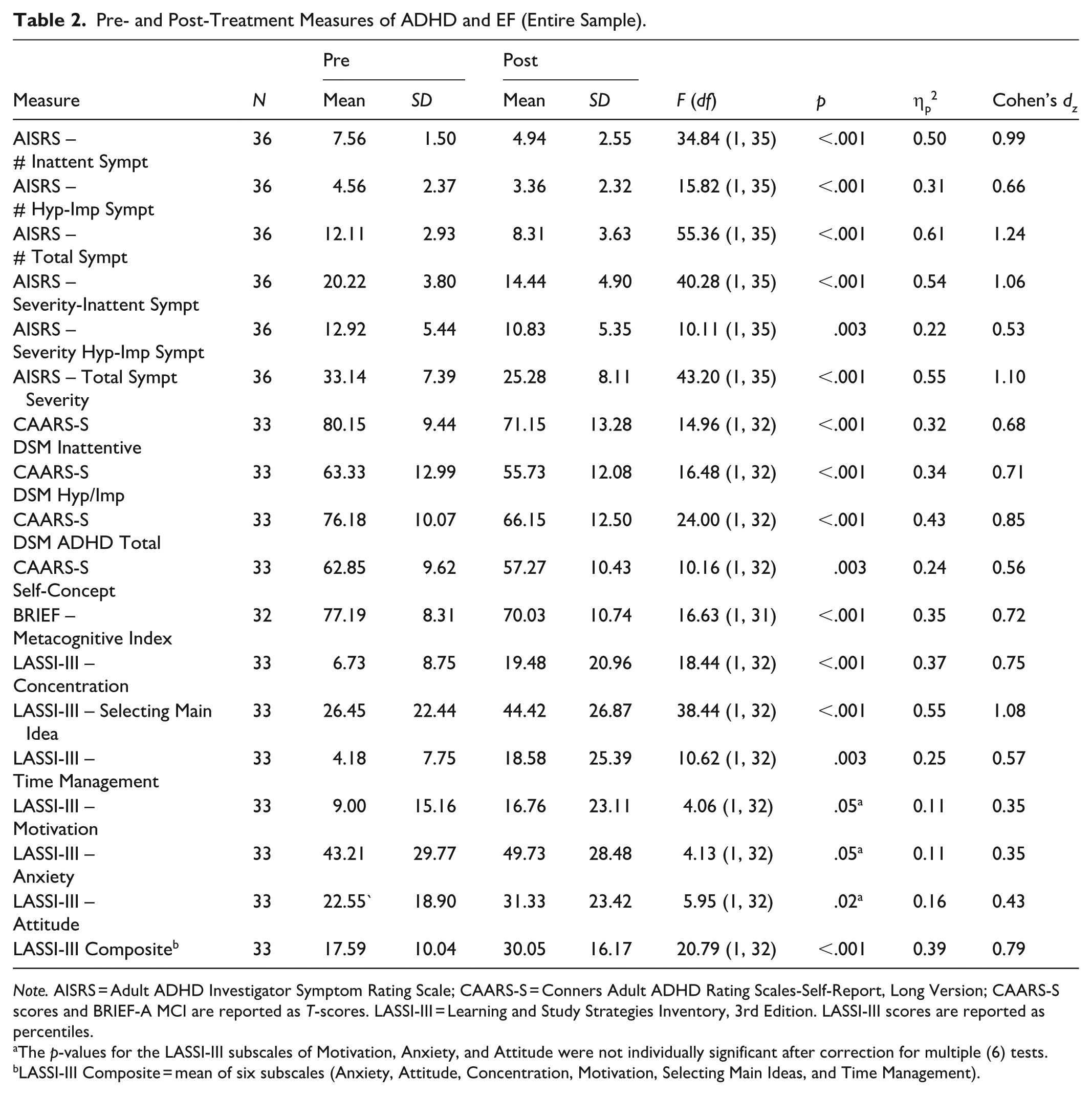
Note. AISRS = Adult ADHD Investigator Symptom Rating Scale; CAARS-S = Conners Adult ADHD Rating Scales-Self-Report, Long Version; CAARS-S scores and BRIEF-A MCI are reported as T-scores. LASSI-III = Learning and Study Strategies Inventory, 3rd Edition. LASSI-III scores are reported as percentiles.
The p-values for the LASSI-III subscales of Motivation, Anxiety, and Attitude were not individually significant after correction for multiple (6) tests.
LASSI-III Composite = mean of six subscales (Anxiety, Attitude, Concentration, Motivation, Selecting Main Ideas, and Time Management).
Response on Pre- and Post-Treatment Measures of ADHD and EF for Treatment “Completers Only.”
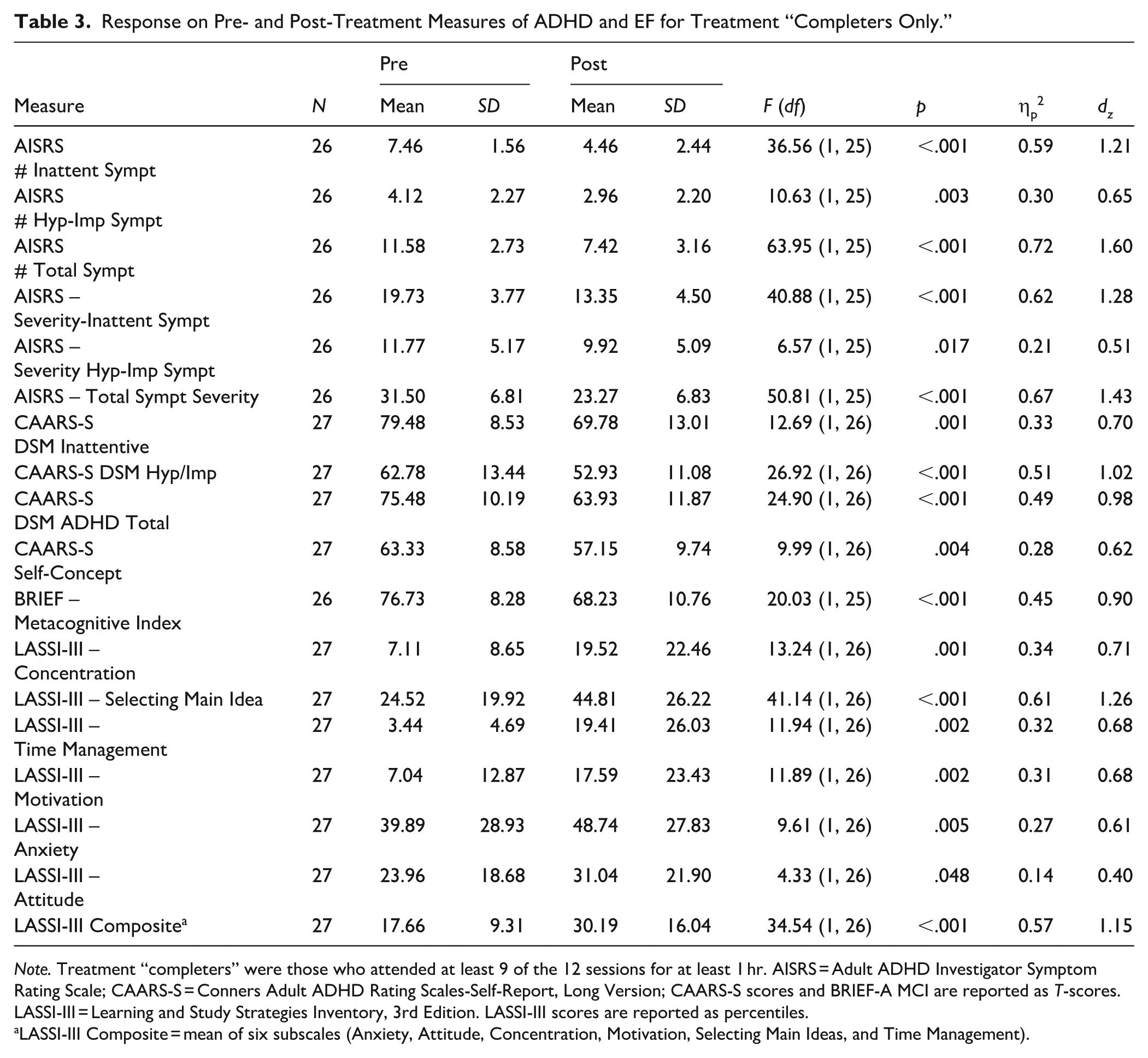
Note. Treatment “completers” were those who attended at least 9 of the 12 sessions for at least 1 hr. AISRS = Adult ADHD Investigator Symptom Rating Scale; CAARS-S = Conners Adult ADHD Rating Scales-Self-Report, Long Version; CAARS-S scores and BRIEF-A MCI are reported as T-scores. LASSI-III = Learning and Study Strategies Inventory, 3rd Edition. LASSI-III scores are reported as percentiles.
LASSI-III Composite = mean of six subscales (Anxiety, Attitude, Concentration, Motivation, Selecting Main Ideas, and Time Management).
Results
Sample Characteristics
Forty-one (M = 21.82 years, SD = 2.75) participants met all inclusion and exclusion criteria for the study and were assigned in order of enrollment to the next available treatment group. These students were recruited via referrals from the Student Counseling Center (n = 7, 17%), other faculty or advisors (n = 3, 7%), or other students (n = 4, 10%). Two-thirds of students (n = 27, 66%) self-referred after receiving advertisements sent to their student email accounts.
Demographic characteristics are summarized in Table 4. Participants were ethnically (n = 12, 29.3% Latine) and racially diverse: n = 2, 4.9% American Indian/Native Alaskan; n = 11, 26.8% Asian; n = 13, 31.7% Black/African American; n = 8, 19.5% White; n = 7, 17.1%. “Other” racial identification included 3 who self-reported that they identified according to their Latine ethnicity, and 4 who identified as Middle Eastern/North African (MENA) or MENA/American. More than half of the participants identified as female (n = 29, 70.7%). Over three quarters of students lived off-campus with one or more family members (n = 32, 78%), two (4.9%) lived with a partner or spouse, and 7 (17.1%) lived with roommates.
Key Demographic Characteristics at Baseline Assessment (N = 41).
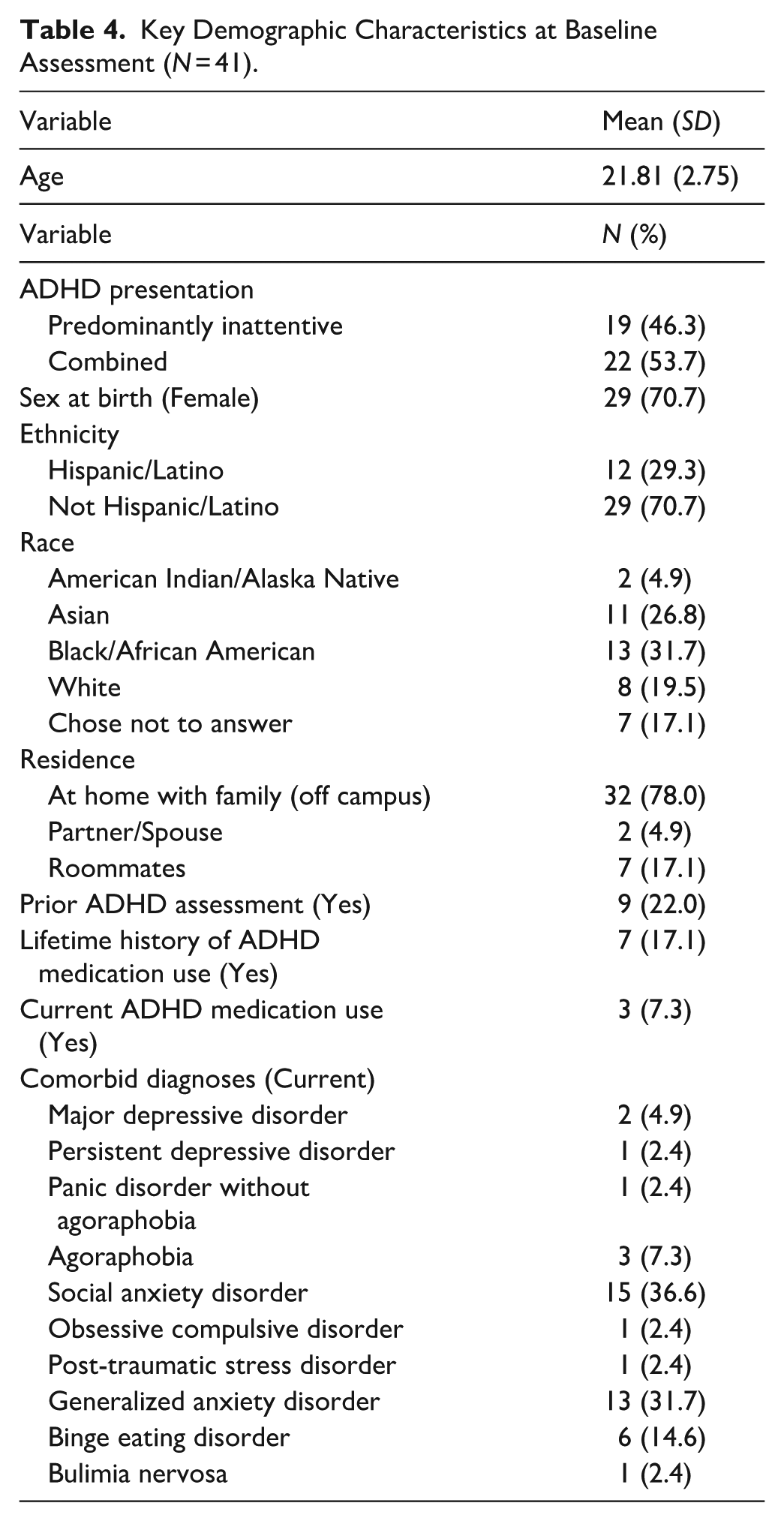
Most students had never undergone an ADHD assessment prior to their evaluation to determine eligibility for the study (n = 32, 78%). Four participants had previously been evaluated as adults (≥17 years; n = 4, 10%) and 5 (12%) during childhood. Following a comprehensive evaluation for this study, n = 19 (46%) students met DSM-5 criteria for ADHD Predominantly Inattentive Presentation and n = 22 (54%) for Combined Presentation. Many students (n = 25, 61%) also met DSM-5 diagnostic criteria for at least one current, comorbid disorder (range = 0–4. The most common of which were Social Anxiety Disorder (n = 15, 37%), Generalized Anxiety Disorder (n = 13, 32%), and Binge Eating Disorder (n = 6, 15%).
Consistent with the low rates of assessment for ADHD, only 7 (17%) had a lifetime history of ever having taken medication for ADHD, and even fewer were currently taking medication (n = 3, 7.3%). Most had a history of having received psychotherapy (n = 26, 63%), but this was not necessarily related to their ADHD behaviors. Among the 41 participants, one person reported having discontinued individual counseling at approximately week 2 of the intervention, and one person began individual psychotherapy for academic-related stress between session 8 and 9 of the program. There were no reports of changes made to medication regimens.
Pre-to-Post Treatment Changes
Pre- and post-treatment results for all variables are shown for the entire sample in Table 2 and for treatment completers in Table 3. Effect sizes are expressed both as Partial eta squared (ηp2 ) and Cohen’s dz (for repeated measures).
ADHD Symptom Count and Severity
Analyses revealed significant reductions in both number and total severity of DSM-5 Inattentive, Hyperactive/Impulsive, and Total symptoms. All showed robust effect sizes and retained significance after Holm-Bonferroni correction for multiple testing. Improvement was greater for inattentive than hyperactive-impulsive symptoms. On the clinician-rated AISRS, the number of inattentive symptoms decreased from M = 7.56 (SD = 1.50) to M = 4.94 (SD = 2.55), F(1, 35) = 34.84. p < .001, ηp2 = .65, as did severity of inattention from M = 20.22 (SD = 3.80) to M = 14.44 (SD = 4.90), F(1, 35) = 40.28. p < .001, ηp2 = .54. Although there were also significant decreases in number and severity of hyperactive/impulsive symptoms from pre- to post-intervention, effect sizes were about half (for severity) to two-thirds (for symptom frequency) of those observed for inattention. Overall, 12 of 36 students who completed the post-treatment interview no longer met DSM-5 adult criteria for ADHD, based on their having fewer than five ADHD symptoms in both domains (American Psychiatric Association, 2022).
Executive Self-Management
Significant improvement was observed in executive self-management skills. The BRIEF-A MCI decreased from pre- (M = 77.19, SD = 8.31) to post-intervention (M = 70.03, SD = 10.74), F(1, 31) = 16.63, p < .001, ηp2 = .35. Students also reported improvement in their knowledge and use of skills and strategies specific to the college context: the LASSI-III Composite percentile score increased (i.e., improved) from M = 18.69 (SD = 9.50) to M = 30.05 (SD = 16.17) following participation in the groups, F(1, 32) = 20.79, p < .001, ηp2 = .39.
A repeated measures MANOVA of the six LASSI-III subscales comprising the Composite was significant, Pillai’s Trace F(6, 27) = 7.34, p = .0001, ηp2 = .62. After correcting for multiple testing using the Holm-Bonferroni procedure (Holm, 1979), follow-up univariate tests yielded significant improvement in Selecting Main Ideas (Percentile increase 26.45 to 44.42, F(1, 32) = 38.44; p < .001, ηp2 = .55), Concentration (6.73 to 19.48, F(1, 32) = 18.44, p < .001, ηp2 = .37), and Time Management (4.18 to 18.58, F(1, 32) = 10.62, p = .003, ηp2 = .25). The LASSI-III subscales of Attitude, Anxiety, and Motivation did not show significant improvement after correction for multiple testing (all ps ≥ .02).
Engagement of the Treatment Target
Linear regression showed that change in executive self-management, whether measured by BRIEF-A or LASSI-III, was significantly related to post-intervention Inattention symptom count and severity after accounting for pre-intervention Inattention (Table 5). Furthermore, effect sizes were moderate (LASSI-III Composite βs = −.36 to −.38) to large (BRIEF-A MCI βs = .61–.67). Change in executive self-management was not related to post-intervention Hyperactivity/Impulsivity, all ps ≥ .55.
Regression Analyses Showing Change in ADHD Symptomatology as a Function of Change in EF From Pre- to Post-Intervention.
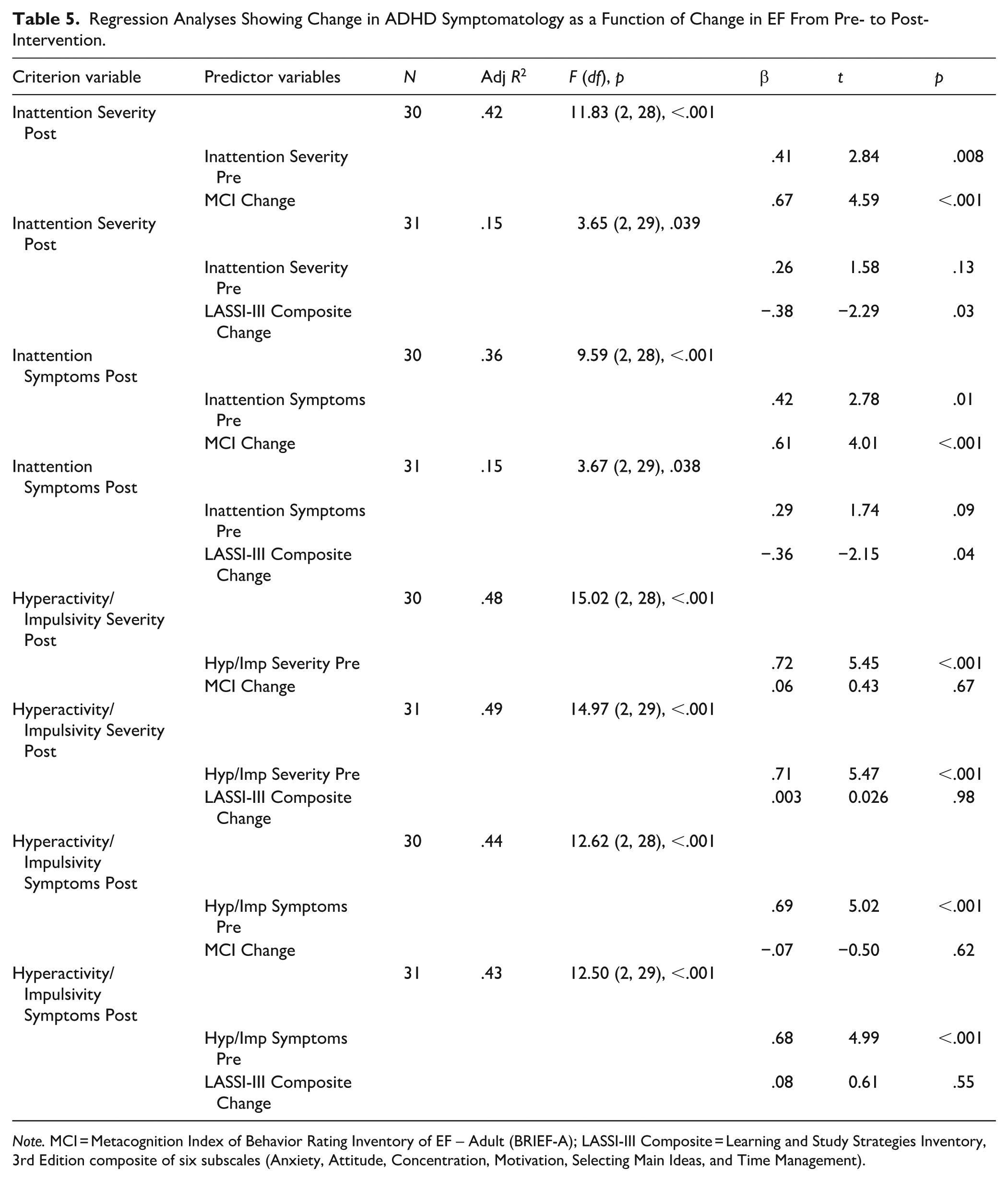
Note. MCI = Metacognition Index of Behavior Rating Inventory of EF – Adult (BRIEF-A); LASSI-III Composite = Learning and Study Strategies Inventory, 3rd Edition composite of six subscales (Anxiety, Attitude, Concentration, Motivation, Selecting Main Ideas, and Time Management).
Feasibility and Acceptability
Twenty-seven (66%) of students attended ≥9 sessions for at least 60 min, which was the criterion for treatment “completion” used in prior studies (Scheres & Solanto, 2021; Solanto et al., 2010). Across all participants, the mean (SD) number of sessions attended was 8.44 (3.14), with the range being 1 to 12. Students’ home exercise completion was variable. On average, approximately two-thirds of participants partially or fully completed the home exercises. The session on Challenging Cognitive Distortions was the only one on which more than half of participants (58.3%) did not attempt the home exercise, which may reflect the challenges involved in re-framing their automatic negative belief(s). Nonetheless, this was one of the most highly rated sessions.
Ratings of Sessions
All the sessions focused on executive self-management, with the exception of the Review of Time-Management, were rated between “moderately” and “very” helpful (≥2.00; Table 6). Among the academic sessions, the first Reading session was generally well-received, with 51% rating it as moderately or very helpful, but the corresponding score for the second Reading session was only 33%. A higher rating was given to the session on Lectures (54%), suggesting it may be more advantageous to include this module to replace the second session on Reading in future iterations of this program. The session on Organizing, Outlining, and Writing Papers was generally well-received, with 76% rating it as “moderately” or “very” helpful. This session was rated somewhat more highly than “Finding Your Niche.” It may be more important to include the former than the latter in future iterations.
Participant Ratings of Group Process and Overall Program Helpfulness.
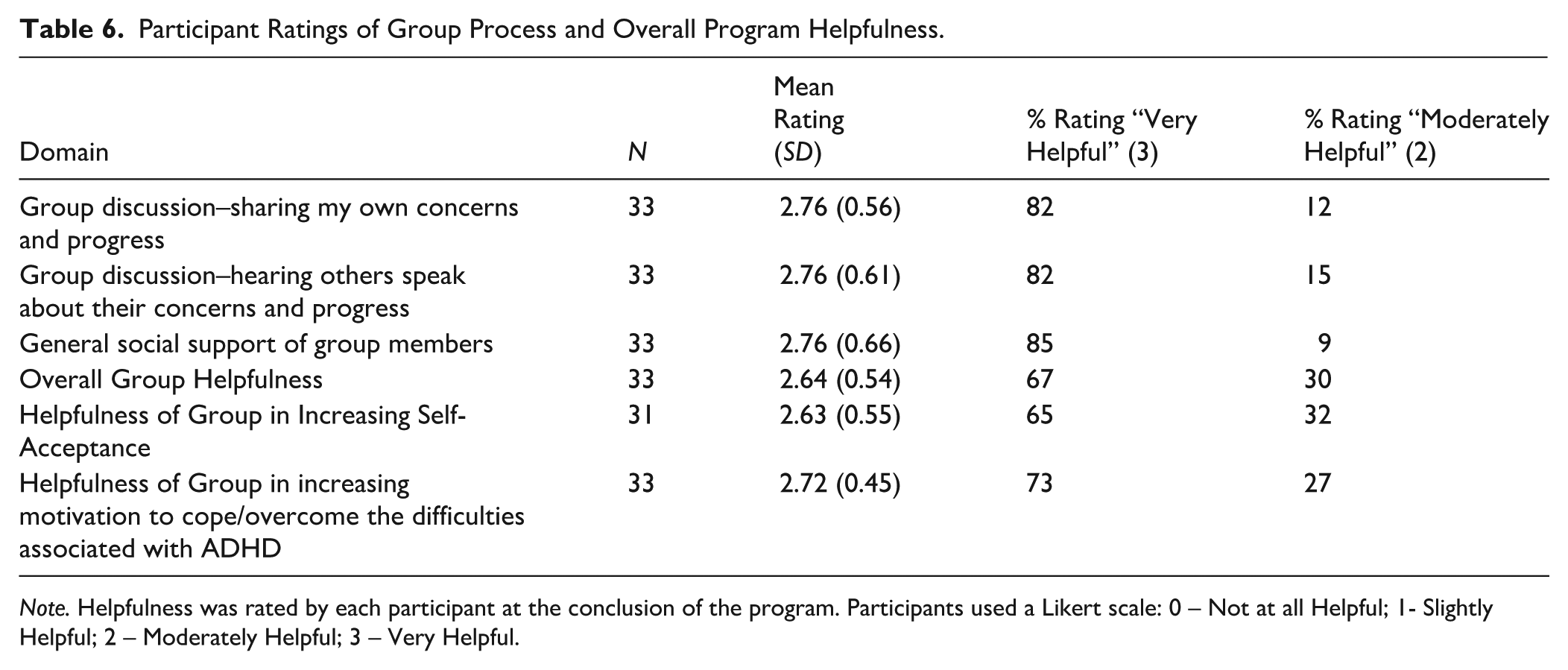
Note. Helpfulness was rated by each participant at the conclusion of the program. Participants used a Likert scale: 0 – Not at all Helpful; 1- Slightly Helpful; 2 – Moderately Helpful; 3 – Very Helpful.
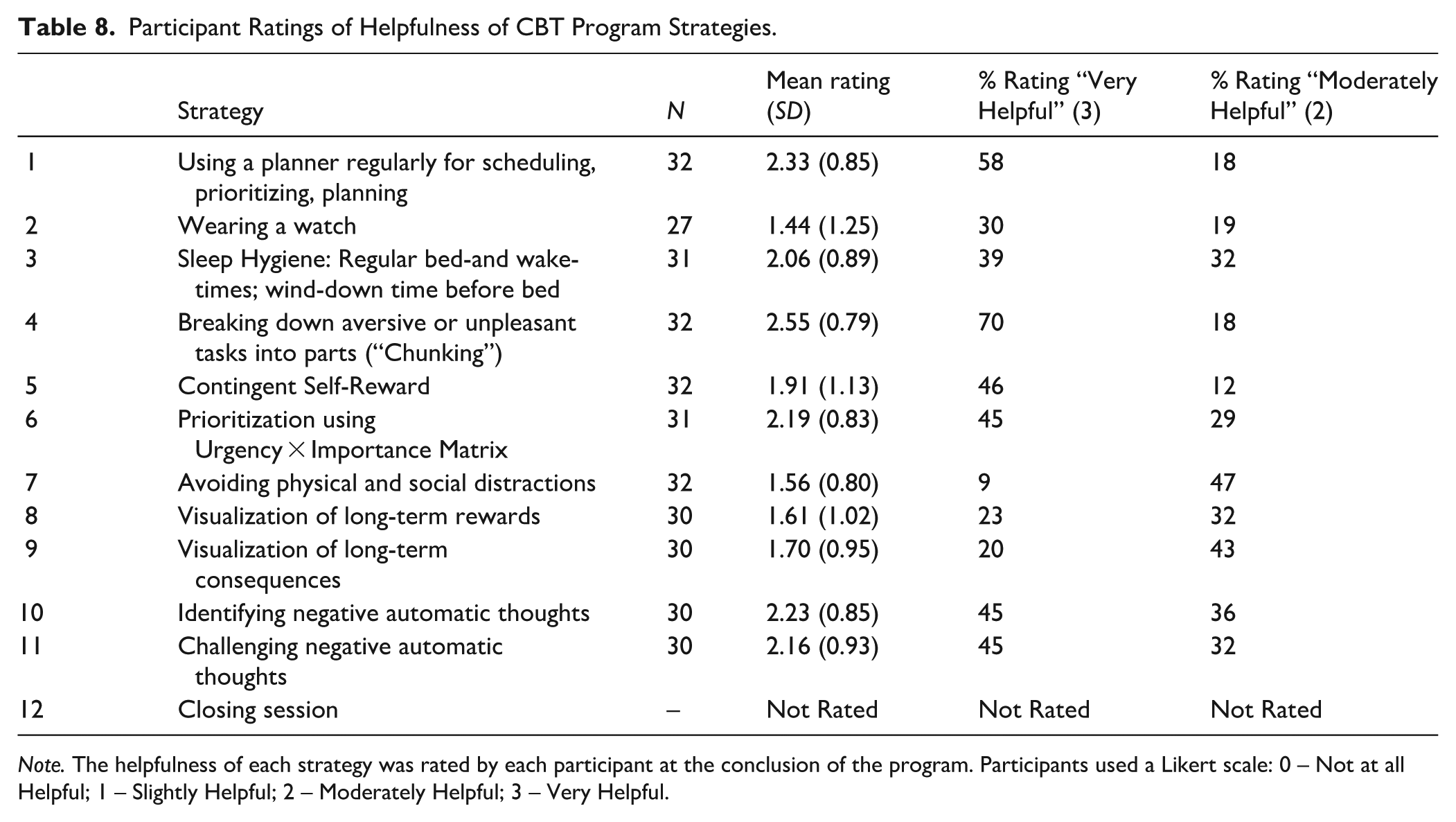
Rating of Strategies
Six of the strategies received mean ratings in the “moderately” to “very helpful” range: breaking down aversive or unpleasant tasks into manageable chunks, regular planner use, identifying and challenging negative automatic thoughts, prioritizing tasks using the Importance × Urgency matrix, and winding down before bed (Table 7).
Participant Ratings of Helpfulness of CBT Program Sessions.
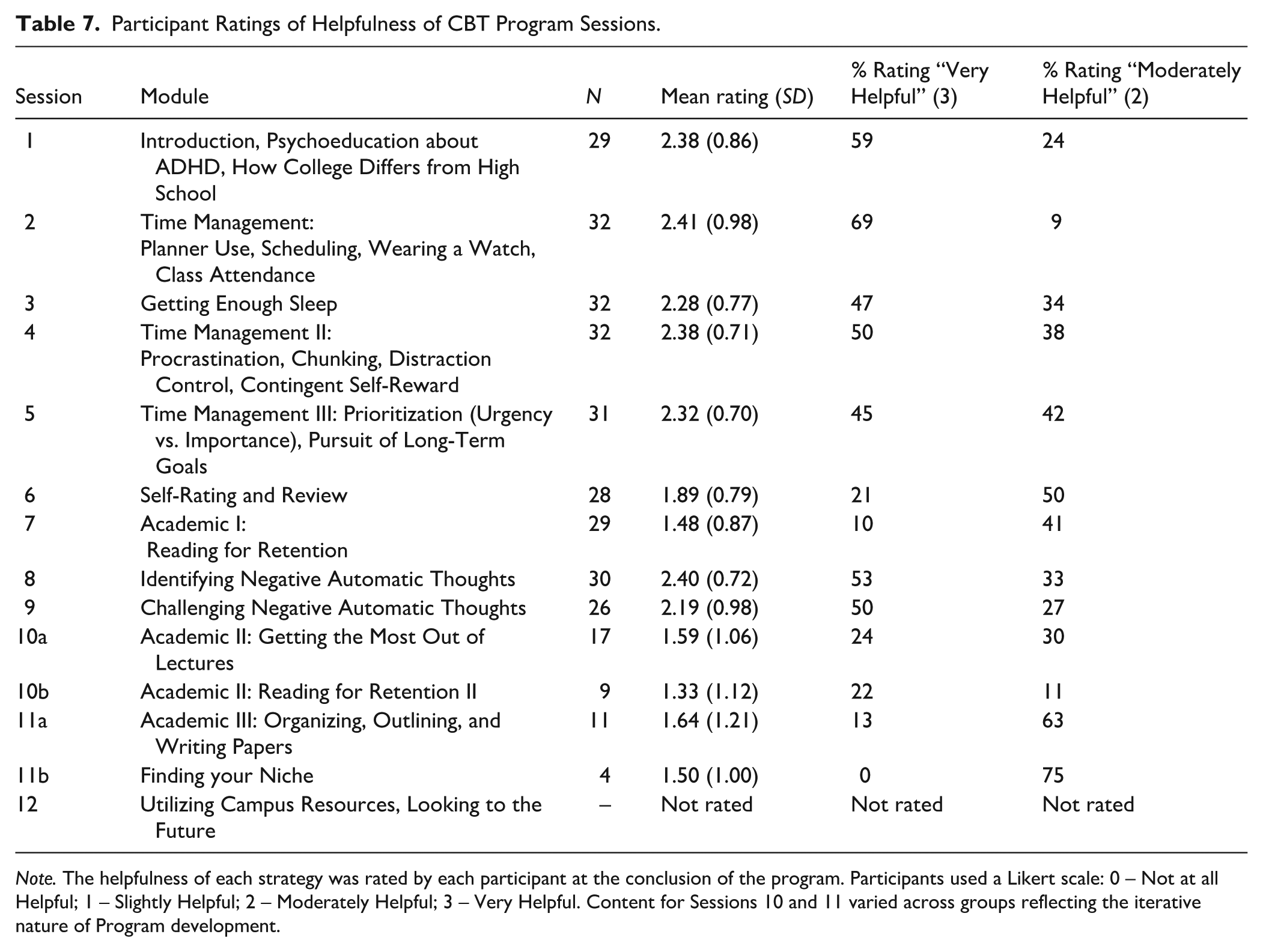
Note. The helpfulness of each strategy was rated by each participant at the conclusion of the program. Participants used a Likert scale: 0 – Not at all Helpful; 1 – Slightly Helpful; 2 – Moderately Helpful; 3 – Very Helpful. Content for Sessions 10 and 11 varied across groups reflecting the iterative nature of Program development.
Overall Helpfulness of the Group
Participants found the group program to be “Moderately” to “Very Helpful” (M = 2.64, SD = 0.54). The group process seemed to be essential to the program’s success: overwhelmingly, students appreciated sharing their own progress and concerns with the group, hearing others speak about their progress and concerns, and the general support of their peers. As reflected in students’ perception of greater empowerment, they evaluated the group as “moderately to “very helpful” in increasing their motivation to cope and overcome their ADHD-related difficulties (Table 8).
Participant Ratings of Helpfulness of CBT Program Strategies.
Note. The helpfulness of each strategy was rated by each participant at the conclusion of the program. Participants used a Likert scale: 0 – Not at all Helpful; 1 – Slightly Helpful; 2 – Moderately Helpful; 3 – Very Helpful.
Asked whether they thought the program should be extended, approximately half (53.1%) indicated that the program was sufficient in duration. The remaining respondents (46.9%) felt that the program could beneficially be extended by, variously, from 1 to as many as 12 more sessions, affording addition of topics such as interpersonal functioning, intimate partner relationships, money management, and physical activity and nutrition to also be covered.
Self-Report Narratives and Self-Concept
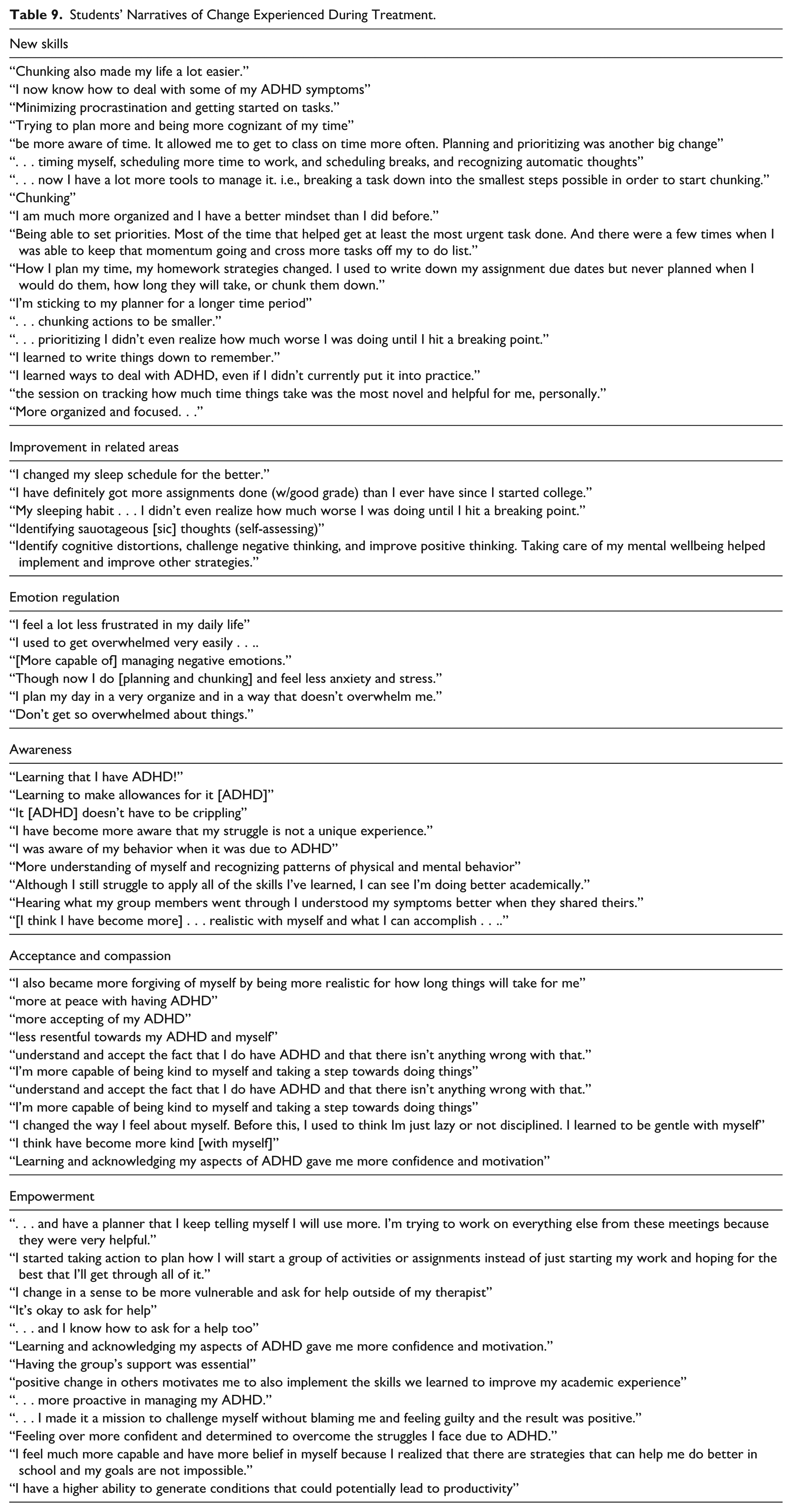
Participants reflected on “the single way (if any) that (they) changed the most as a result of participating in the group program.” Several themes emerged from these narratives. Students reported that they had learned new skills (“Chunking made my life a lot easier”); and gains had transferred beyond ADHD or executive function to associated areas of functional impairment (e.g., “I changed my sleep schedule for the better”) and emotion regulation capacity (e.g., “I feel a lot less frustrated in my daily life”). Students reported being more aware of ADHD, how the disorder is manifested in their behavior, and recognition that it “doesn’t have to be crippling” (e.g., “Hearing what my group members went through I understood my symptoms better.”). Of critical importance, students expressed growing acceptance of their diagnosis and self-compassion (e.g., “I also became more forgiving of myself by being more realistic for how long things will take for me”). They also seemed empowered as a result of the knowledge and skills they had attained, and through the role-modeling and support of their group members (e.g., “I made it a mission to challenge myself without blaming me and feeling guilty and the result was positive”; “positive change in others motivates me to also implement the skills we learned to improve my academic experience”). This was reflected in students’ ratings of how helpful the group was in increasing their self-acceptance (M = 2.63, SD = 0.55, “Moderately” to “Very Helpful”) and their Self-Concept, which improved from pre-treatment (CAARS Self-Concept Mean T Score = 62.85, SD = 9.62) to post-treatment (M = 57.27, SD = 10.43), F(1, 32) = 10.16, p = .003, ηp2 = 0.24 (Table 9).
Students’ Narratives of Change Experienced During Treatment.
Results for Treatment Completers
It was anticipated that students who “completed” the program (i.e., attended ≥9 sessions) would experience better results with respect to reduction of ADHD symptoms, and improvement in executive self-management skills (Table 3). Comparison with analyses comprising all participants (Table 2) did reveal that completers exhibited larger effect sizes for: number and severity of Inattentive symptoms (AISRS); self-ratings of DSM Hyperactive-Impulsive symptoms (CAARS); as well as the Meta-Cognitive Index (BRIEF-A), and LASSI-III scales of Anxiety, Motivation, and Selecting the Main Idea.
Discussion
In this study, Group CBT for college students with ADHD was associated with significant pre- to post-treatment improvement on ADHD symptoms and executive self-management skills of participants, and was feasible to implement in the college setting. Of note, there was near-universal approval by study participants of the value of the intervention, with quantitative and qualitative measures showing improvement on the key measures. The finding that the subgroup of those who “completed” the treatment exhibited notably better results across measures than those who did not, also supports the merits of the program.
ADHD Symptoms
Significant reductions in clinician-rated (AISRS) and self-reported (CAARS) symptoms of inattention and hyperactivity/impulsivity were observed. The large effect sizes for reduction in total ADHD symptom number (ηp² = 0.61; Cohen’s dz = 1.24) and severity (ηp² = 0.55; Cohen’s dz = 1.24), indicate there was clinically meaningful improvement. The reduction of inattentive symptoms from 7.56 to 4.94 was comparable to the Netherlands study (6.78–4.22) (Solanto & Scheres, 2021) and 33% of the participants no longer met criteria for ADHD at the conclusion.
Executive Self-Management Skills
The improvement in LASSI-III composite percentile scores from 18.69 to 30.05 is further evidence of the study’s impact on skills and strategies pertinent to college success. The subscales showing greatest improvement were “Selecting Main Ideas” (from reading), Concentration, and Time Management, all of which were targets of the intervention. Furthermore, regression analyses verified that changes in executive self-management skills were associated with ADHD symptomatology.
The BRIEF-A Metacognition Index (MCI) scores improved post-intervention, indicating reduced executive impairment in everyday life. The pre-post change in T scores was almost 0.75 standard deviations (0.77–0.70), although the final score remained in the clinically elevated range. The MCI domain comprises initiation, planning/organization, working memory, problem-solving monitoring, and material organization – all processes targeted by the intervention.
Feasibility
Direct observation of trainee performance during the sessions, as well as post-session discussions indicated that trainees adhered to the content and tone of the protocol as specified in the manual, and developed good rapport with the students. The program completion rate (66%), while lower than that seen in the Netherlands study (Solanto & Scheres, 2021), indicates the intervention was generally acceptable. On average, two-thirds attempted or completed the home exercises. Slightly more than half found the program duration was of sufficient length and the remainder thought it should be extended to cover other topics of concern including interpersonal functioning, intimate partner relationships, money management, and physical activity.
Student Narratives
Review of qualitative data obtained from students’ narratives revealed themes of gaining (1) self-acceptance and compassion about having ADHD, (2) awareness of what it means to live with ADHD, (3) better emotional self-regulation, and (4) empowerment and self-confidence about their ability to overcome the challenges of the diagnosis. Virtually all commented on the value of the group format of the intervention insofar as it provided a safe space for sharing their individual struggles with ADHD and for receiving encouragement from others to make changes in coping with the demands of college. Many participants identified key skills they acquired during the intervention which matched the quantitative findings. Chunking and planner use were the top two most helpful strategies identified by our study sample, consistent with the findings of Dutch college study (Solanto & Scheres, 2021) as well as the adult study (Solanto et al., 2010).
Interpretation
The present findings indicate that the intervention effectively targeted both ADHD symptoms and executive deficits. This was accomplished through explicit executive self-management training, intensive practice, and the integration of peer support and adaptive self-talk strategies. Improvements in executive self-management were found to contribute to reductions in ADHD symptoms, consistent with theoretical models that conceptualize ADHD as primarily a disorder of executive function (Barkley, 2014b), as well as studies that show that executive dysfunction is highly correlated with academic impairment in students with ADHD (Willcutt et al., 2012). Finally, the cultural diversity of the study sample (many of whom were from minoritized and historically marginalized communities) makes the favorable outcomes especially salient for institutions of higher education hoping to improve retention and graduation rates in these populations. Having the “double whammy” of a delayed diagnosis of ADHD along with the stigma it holds for individuals from these groups underscores the value of this intervention.
Comparison With Previous Literature
These results are consistent with prior cognitive-behavioral therapy (CBT) trials for adults (Safren et al., 2010; Solanto et al., 2010) and college students with ADHD (Anastopoulos et al., 2021; Solanto & Scheres, 2021). Notably, this study offers three novel contributions. First, change in executive self-management was associated with change in ADHD symptoms. These regression analyses provide a signal that changes in the treatment target (executive self-management) are related to ADHD symptomatology. Second, success in training clinical psychologists with no prior experience administering this group intervention suggests its potential scalability to address gaps in real-world implementation within academic settings.
Third, in contrast to Anastopoulos et al. (2021) ACCESS program, which was developed in two rural campus settings in the southeastern region of the US, and the study by Solanto and Scheres (2021), which was conducted at a private university in the Netherlands, our study sample reflects the urban community of New York City. The sample for this study was more racially and ethnically diverse than those in these prior studies. In addition, most students were living at home, often at a significant distance from the campus, and many were simultaneously working part-time while attending college in order to support themselves or contribute to the support of their families. These factors may have limited the time and effort the students were able to devote to practicing the strategies and completing the Home Exercise, and may account for the lower attendance and completion rate for the program in this study (66%), compared to the Netherlands study (84%). Another difference between this and prior research is that two-thirds of the ACCESS study sample had received a diagnosis of ADHD prior to entering their program, whereas less than a quarter of our sample had been evaluated previously. Nearly half the participants in ACCESS were concurrently taking medication for ADHD, whereas only 7% of our sample was doing so.
Clinical and Practical Implications
The intervention appears feasible and effective for integration into college mental health services. The intervention was also successful for students who, for the most part, had limited or no access to ADHD services up to this point in their education. This skills-based group set within the institutional context may increase accessibility to ADHD intervention, perhaps especially important for students from low resource and disinvested communities.
Strengths and Limitations
Strengths of this study include comprehensive diagnostic evaluations, rigorous eligibility screening, and implementation in a real-world setting with iterative refinement. Large effect sizes across ADHD and executive skills further underscore the potential benefits of the intervention. However, several limitations warrant consideration. The open trial design lacked a control group, and the sample was restricted to a single urban public college, limiting generalizability. Strict co-morbidity exclusion criteria may reduce applicability to more representative populations, and reliance on self-report on measures of executive skills introduces potential bias. In addition, the relatively low completion rate warrants further consideration of strategies to improve successful participation. Finally, although we assessed lifetime psychotherapy and any change in psychotherapy during the course of CBT treatment, we did not additionally quantify the number of students or the type of other psychotherapy students might have been receiving concurrently. Thus, we cannot make any statements about the potential effects of concurrent individual therapeutic support on the benefit received from Group CBT, which will need to be evaluated in future research.
Future Directions
Future research should prioritize randomized controlled trials to confirm efficacy and verify mediation effects. Long-term follow-up is needed to assess maintenance of executive skills and ADHD symptom gains. Investigating academic outcomes such as GPA and retention will clarify functional benefits. Attrition-focused research should evaluate engagement strategies – including hybrid delivery, incentives, and flexible scheduling – to reduce dropout rates. Finally, assessment of the training program and its potential for dissemination across campuses will necessitate standardized ratings of trainee performance, and examination of the efficacy of the intervention when delivered independently by the trained clinicians in a subsequent trial. Pending confirmation of efficacy, the in vivo approach utilized in this study may serve as a model for training clinical psychology graduate students, as well as medical residents and fellows, in the delivery of this CBT intervention for ADHD in college students and adults generally.
Conclusion
In summary, this open trial provides preliminary evidence that a 12-week CBT group intervention can significantly reduce ADHD symptoms and improve executive self-management among college students. The intervention’s emphasis on explicit executive skills training, intensive practice, and peer support appears to address core challenges faced by this population, and large effect sizes suggest the potential for meaningful clinical impact. Importantly, the successful implementation of clinician-led groups under PI supervision highlights the feasibility of integrating this model into campus mental health services, offering a scalable approach to meet growing demand. While limitations such as the absence of a control group and restricted generalizability warrant caution, these findings underscore the promise of structured, skills-based interventions for ADHD in academic settings.
Footnotes
ORCID iDs
Ethical Considerations
Research was approved by the City University of New York (CUNY) University Integrated Institutional Review Board (CUNY-UI IRB) (Protocol #2022-0008), Feinstein Institutes for Medical Research – Northwell Health IRB (Protocol #20-0013), and Cooper Health IRB (Protocol #22-019).
Consent to Participate
All participants provided written informed consent to take part in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this paper was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number R34MH122219 (MPIs: Solanto, M. and Rostain, A. L.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available from authors on reasonable request.*