
Abstract
Introduction:
Research findings on specific inflammatory markers (e.g., CRP) in ADHD show considerable heterogeneity. Meanwhile, the potential moderating role of leisure-time physical activity (LTPA) in this relationship is underexplored.
Methods:
Based on data from the National Health and Nutrition Examination Survey (NHANES) conducted between 1999 and 2004, 4,817 adolescents aged 12 to 19 were included. This study used logistic regression analysis and restricted cubic splines (RCS) to explore the association between inflammatory biomarkers and ADHD. Interactive analyses were performed to assess the moderating effect of LTPA on this relationship. Furthermore, subgroup analyses were conducted to validate the robustness of the observed effects.
Results:
After adjusting for all confounding factors, each 1 mg/L increment in C-reactive protein (CRP) was associated with a 9% higher ADHD risk (OR = 1.09, 95% CI [1.01, 1.18]). The chronic low-grade inflammation (CLGI) group exhibited a 57% higher risk of ADHD (OR = 1.57, 95% CI [1.14, 2.15]) compared to the non-GLGI group. The non-linear analysis further revealed that the risk of ADHD reached its peak when CRP was 2.75 mg/L (OR = 1.89, 95% CI [1.39, 2.57]). Compared with the group engaging in less than 60 min of LTPA daily, the association between ADHD and CRP was moderated in the “LTPA ≥60 min/day” group (p for interaction = .04).
Conclusions:
Elevated CRP levels are positively associated with ADHD. More than 60 min/day LTPA may moderate the association between CRP and the risk of ADHD.
Introduction
Attention-Deficit/Hyperactivity Disorder (ADHD) is a prevalent neurodevelopmental disorder affecting approximately 2% to 7% of children and adolescents worldwide (Sayal et al., 2018). It confers substantial risks for academic underachievement, social difficulties, and comorbid mental health conditions, thereby imposing a substantial economic burden on families and society (Sayal et al., 2018). The etiology of ADHD is complex and multifactorial, involving interactions between biological, genetic, and environmental factors (Thapar & Cooper, 2016).
Accumulating evidence suggests that inflammation and immune dysregulation may potentially contribute to the pathophysiology of ADHD (Dunn et al., 2019; Mitchell & Goldstein, 2014). Inflammation is an acute defense mechanism in response to injury, infection, or harmful stimuli. Unresolved acute inflammation may transition into chronic low-grade inflammation (CLGI), which is characterized by systemic immune activation with modestly elevated levels of tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), C-reactive protein (CRP), and other biomarkers—though still lower than levels observed during acute infection or trauma (Osimo et al., 2019; Wärnberg et al., 2010). In pediatric populations, CRP concentrations between 2 and 10 mg/L are indicative of CLGI (Kozlowska et al., 2019). CRP and components of the complete blood count (CBC) were selected as inflammatory markers in this study, primarily due to their distinct biological and methodological advantages. First, synthesized by hepatocytes in response to IL-6 and TNF-α, CRP acts as a downstream mediator of the inflammatory cascade (Coventry et al., 2009; Singh et al., 2025). Its relatively long half-life of approximately 19 hr contributes to its stability and reliability as a biomarker. Meanwhile, these biomarkers are commonly measured, well-standardized, and readily accessible within the NHANES dataset and other similar epidemiological resources. Although more specific inflammatory mediators, such as cytokines (e.g., IL-6, TNF-α), may offer greater mechanistic insight into inflammatory pathways, they are not routinely collected in large-scale surveys like NHANES due to higher associated costs, greater technical complexity, and more stringent sample storage requirements. Accumulating evidence supports an association between ADHD and dysregulated inflammation (Chang et al., 2021; Mitchell & Goldstein, 2014). However, findings on specific inflammatory markers (e.g., CRP, IL-10) in ADHD show considerable heterogeneity and the casual mechanisms remain unclear (Anand et al., 2017; Frank et al., 2019; Misiak et al., 2022; Mitchell & Goldstein, 2014). For instance, while several studies (Chang et al., 2020; Passarelli et al., 2013) report elevated IL-6 and IL-10 levels in ADHD patients compared to controls, others found no significant differences in CRP or IL-10 between ADHD and the general population (Misiak et al., 2022). This heterogeneity in findings may stem from study design, sample characteristics, and detection methodologies, thereby underscoring the need for further validation across diverse populations.
In addition to pharmacological treatment options, the development of accessible non-pharmaceutical adjunctive interventions is important. Leisure-time physical activity (LTPA), a key component of daily physical activity among children and adolescents, has garnered significant attention in research and public health practice (Bull et al., 2020). Various studies have investigated the relationship between physical activity and attention. A meta-analysis demonstrated that physical activity could alleviate symptoms of inattentiveness (Dastamooz et al., 2023). Additionally, a systematic review revealed that long-term exercise interventions are beneficial for both the core symptoms and executive function of children and adolescents with ADHD (Huang et al., 2023).
Although current evidence suggests that physical activity and inflammation are independently associated with ADHD, the potential combined effect of physical activity and inflammatory processes on ADHD among children and adolescents remains poorly elucidated. Leveraging NHANES 1999–2004 data, a multivariate-adjusted model was constructed to investigate (1) the association between inflammatory biomarkers and ADHD and (2) whether LTPA could modulate the association between inflammatory biomarkers and ADHD.
Methods
Database and Study Subjects
The NHANES database is a cross-sectional population survey conducted by the U.S. Centers for Disease Control and Prevention (CDC), utilizing a multi-stage sampling strategy and updated biennially. For this study, data from three cycles of the NHANES database (1999–2000, 2001–2002, and 2003–2004) was utilized. Various data categories were extracted, including demographic characteristics (age, gender, race, family poverty-income ratio, body mass index, educational level), smoking status, asthma, weight measurements, ADHD diagnostic records, peripheral blood inflammation markers, and physical activity metrics.
Measures
Diagnostic Information
Diagnostic information for ADHD was based on self-report/guardian responses to the NHANES database questionnaire: “Has a doctor or health professional ever told (the child) that (he/she) had attention deficit disorder?” The identical ADHD questions were asked of kids who were 16 years old or older, but the terms in parenthesis were changed to (you) and (you), respectively. Response options included “yes,” “no,” “reject,” and “don’t know.” To minimize the potential impact of recall bias, only “yes” and “no” responses were analyzed, whereas “reject” and “don’t know” were categorized as missing data.
Inflammatory Biomarkers
The selection of these inflammatory biomarkers was determined by their availability in the NHANES 1999–2004 cycles for the adolescent cohort. While recent research has highlighted the importance of cytokines (e.g., IL-6, TNF-α) in ADHD, these were not measured in the standardized laboratory protocols for the NHANES cycles. Nevertheless, CRP and CBC-derived indices serve as well-established, standardized markers of systemic inflammation in large-scale epidemiological studies.
Inflammatory biomarkers in peripheral blood were extracted from the Laboratory Tests section of the NHANES database. CRP concentrations were measured by utilizing the Dade Behring Nephelometer II (BNII). Blood cell counts, including White Blood Cells (WBC), Neutrophils (Neu), Lymphocytes (Lym), and Platelets (PLT), were obtained by the Beckman Coulter MAXM instrument at the Mobile Examination Center (MEC). Based on these data, comprehensive inflammatory indices were calculated: NLR (neutrophil-to-lymphocyte ratio), SII (platelet count × neutrophil count/lymphocyte count), and PLR (platelet-to-lymphocyte ratio).
Data points exceeding predefined clinical thresholds (CRP >10 mg/L; WBC >15 × 109 cells/L or WBC <4 × 109 cells/L) are indicative of acute inflammation or underlying disease and were therefore excluded (Kozlowska et al., 2019; Peltola et al., 2006). When CRP concentration was between 2 and 10 mg/L, it was classified as CLGI (Kozlowska et al., 2019).
Daily Duration of Leisure-Time Physical Activity
The “Physical Activity-Individual Activities” questionnaire was utilized to evaluate the intensity, frequency, and duration of leisure-time physical activity over the past 30 days. For each participant, total activity time was calculated based on the duration of moderate-intensity and vigorous-intensity leisure-time physical activities (min/day). Participants with both values missing were excluded from the final analyses. If only one value was missing, the available value was used to represent the participant’s daily activity duration.
Covariates
The covariates included in the analysis were age, gender, ethnicity, Family Poverty Income Ratio (PIR), Body Mass Index (BMI), family size, educational level, smoking status, and asthma. Gender was categorized into male and female. Age was stratified into three intervals (Qu et al., 2024): “12–14, 15–17, and 18–19 years.” Ethnicity was classified into four categories: Hispanic American, non-Hispanic White, non-Hispanic Black, and other races. PIR was divided into four levels (Guo & Le, 2024): “<1, [1, 2], [2, 4], and ≥4.” BMI was categorized into three groups based on standard definitions: normal weight, overweight, and obese. Educational level was divided into three: “High school and above, middle school, and primary school.” Family Size was categorized into three groups: “[1, 3], [4, 6], and ≥7.” The presence of inflammatory conditions such as asthma was determined using the “Medical Conditions Questionnaire.”
Statistical Analysis
All statistical analyses were conducted with appropriate weight adjustments in accordance with the guidelines provided by NHANES for data analysis. Continuous variables were presented as mean ± standard deviation (Mean ± SD), while categorical variables were expressed as counts and percentages (N, %). All missing values of independent and dependent variables were removed, along with outliers of peripheral blood inflammatory markers (CRP >10 mg/L). Missing covariates were subsequently imputed using the random forest method for multiple imputation. T-tests were used to assess differences in continuous variables between the two groups, while chi-square tests were applied for categorical demographic differences. Statistical analyses were performed sequentially according to the following steps.
First, logistic regression analyses were performed to explore the associations between all peripheral inflammatory biomarkers and the risk of ADHD. Based on prior literature (Kozlowska et al., 2019; Schlenz et al., 2014), CRP levels were stratified into two groups: “CRP ≤2 mg/L” was categorized as “Non-CLGI” and “2 < CRP ≤ 10 mg/L” as “CLGI,” with “Non-CLGI” serving as the reference group. Given the absence of a clear classification standard for other inflammatory markers, these markers were divided into quartiles and labeled as “Q1,” “Q2,” “Q3,” and “Q4,” with “Q1” serving as the reference. All results were reported as odds ratios (OR) with 95% confidence intervals (95% CI). Confounding factors were adjusted in multiple models. Model 1 included no covariate adjustments; Model 2 adjusted for age, gender, and ethnicity; Model 3 further adjusted for all covariates, and restricted cubic spline (RCS) was incorporated into Model 3 to explore the potential nonlinear association between peripheral blood inflammatory biomarkers and ADHD.
The second step was to investigate whether the duration of LTPA could modulate the relationship between inflammatory biomarkers and ADHD. In accordance with the WHO guidelines for physical activity in children and adolescents (Bull et al., 2020), LTPA was categorized into two groups: “<60 min/day” and “≥60 min/day.” Logistic regression analyses and RCS were employed to investigate the association between inflammatory biomarkers and ADHD across different LTPA duration groups. Additionally, an interaction term combining inflammatory biomarkers and LTPA was included in the models to evaluate potential interactions between these variables.
In the third step, the subgroup analysis was conducted, incorporating all covariates to investigate whether the association between inflammatory markers and ADHD remained consistent and whether the moderating effect of LTPA persisted across different groups. In this analysis, any variable functioning as a stratification factor was excluded from the list of covariates.
All statistical analyses were conducted using R (version 4.4.1) and SPSS (version 27.0). The significance level was established at p ≤ .05.
Results
4,817 NHANES participants were ultimately included in this study, representing an estimated 23.38 million American adolescents aged 12 to 19 years. The mean age of the participants was 15.37 ± 2.25 years, with 2,528 males and 2,269 females. The detailed data processing is illustrated in Figure 1.
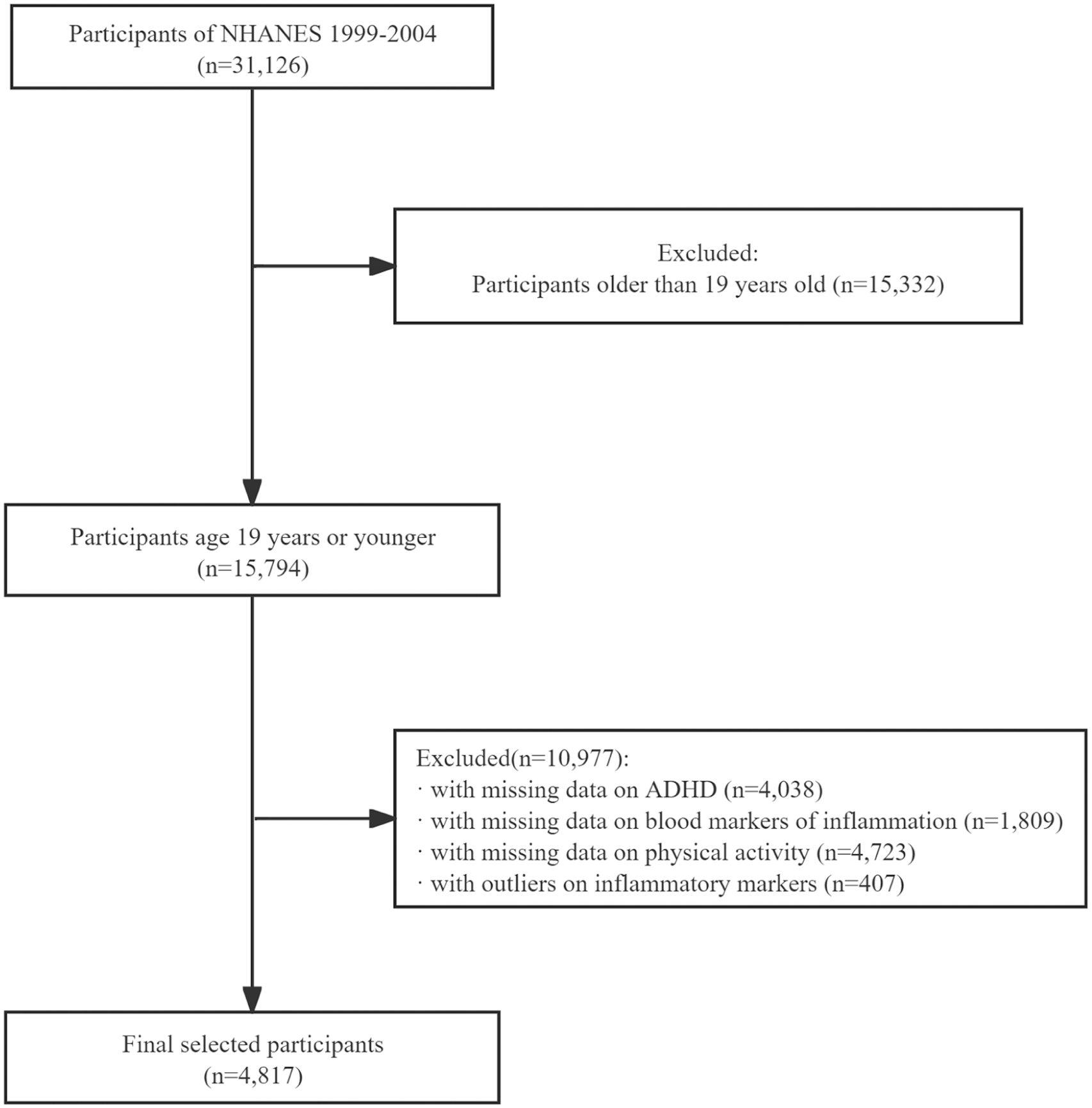
Flow chart for participants recruitment of this study.
Baseline Characteristics of Participants
The prevalence of ADHD was 7.3% (354/4,817). Within the ADHD group, males accounted for 72.3%, significantly higher than females (27.7%). Additionally, the average CRP concentration in the ADHD group was higher than that in the non-ADHD group. A total of 3,004 subjects failed to meet the recommended daily activity level, and 59.0% of individuals with ADHD did not achieve the WHO-recommend daily activity level (Table 1).
Baseline Characteristics of the Study Participants.
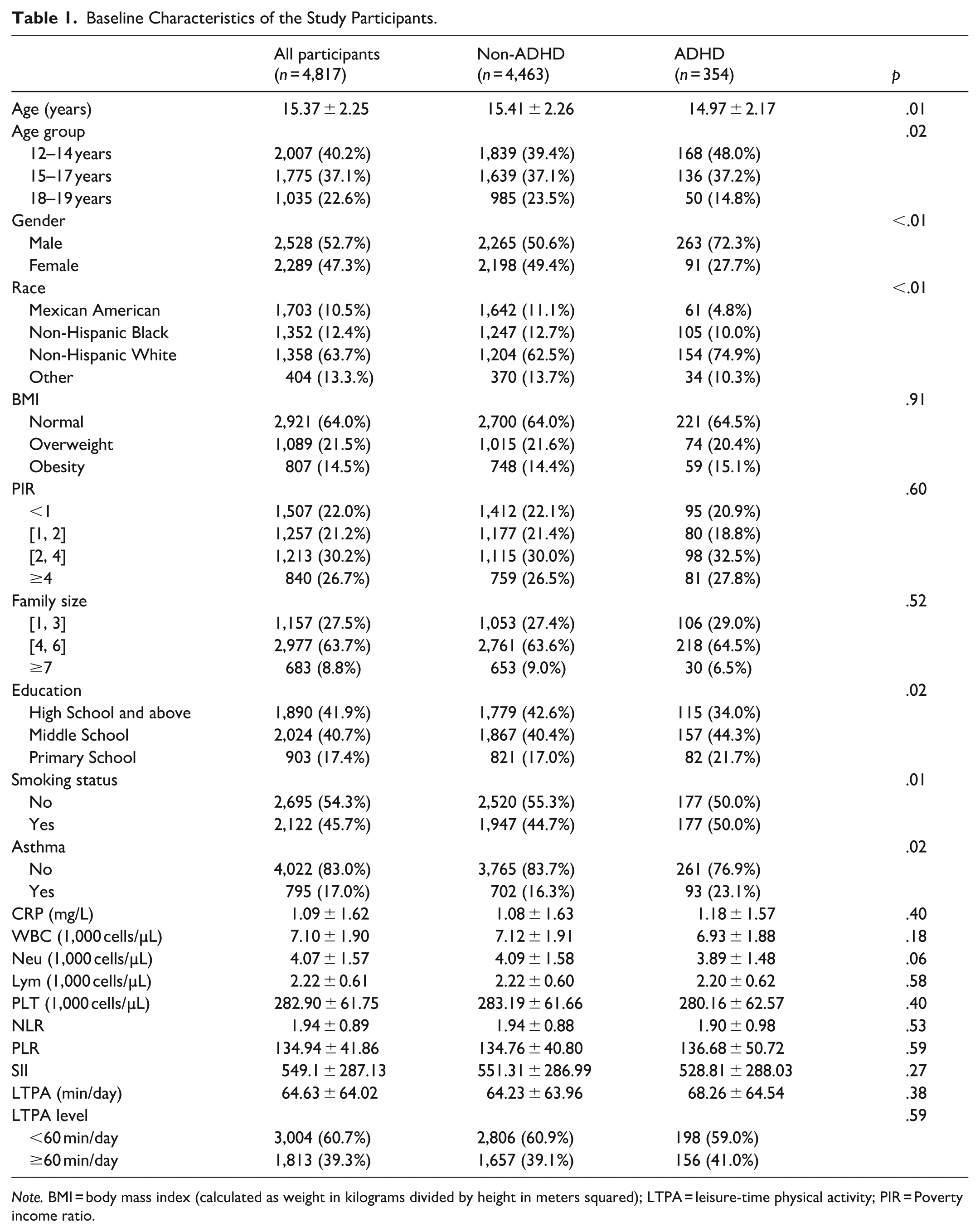
Note. BMI = body mass index (calculated as weight in kilograms divided by height in meters squared); LTPA = leisure-time physical activity; PIR = Poverty income ratio.
The Association Between Inflammatory Biomarkers and ADHD
After adjusting for all confounding factors, the risk of ADHD increased by 9% for each 1 mg/L increment in CRP. Furthermore, the CLGI group exhibited a significantly higher risk of ADHD (OR = 1.57, 95% CI [1.14, 2.15]) compared with the non-CLGI group. However, no significant associations were observed between other inflammatory markers and ADHD in this study (p > .05, see Table 2).
Logistic Regression Analysis of the Association Between Inflammatory Biomarkers and ADHD.
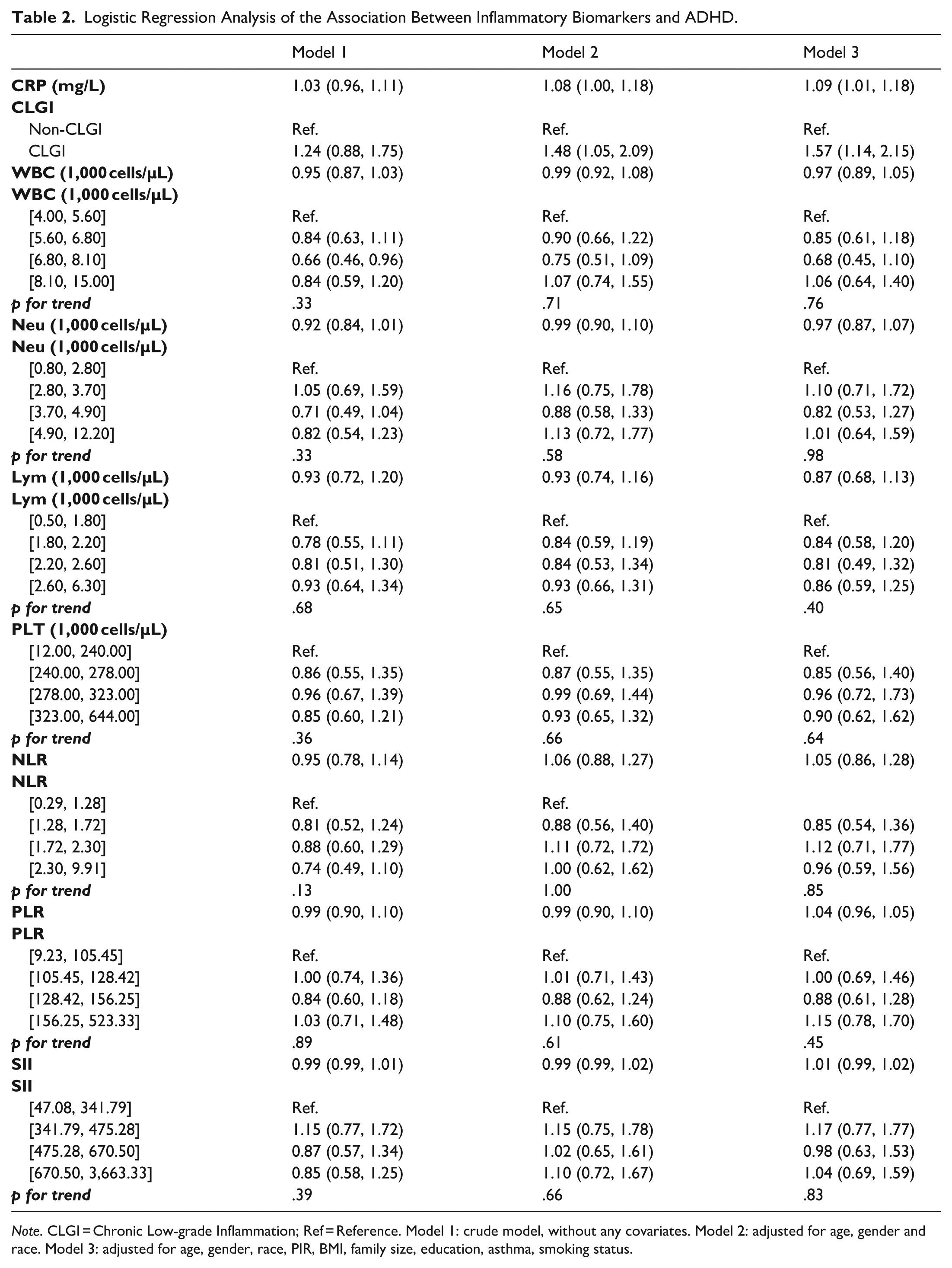
Note. CLGI = Chronic Low-grade Inflammation; Ref = Reference. Model 1: crude model, without any covariates. Model 2: adjusted for age, gender and race. Model 3: adjusted for age, gender, race, PIR, BMI, family size, education, asthma, smoking status.
Moreover, the significant positive association between CRP and ADHD persists consistently across individuals with different BMI categories, asthma status, and other characteristics (details see Table S1).
RCS analysis demonstrated a significant nonlinear relationship between CRP and ADHD (p for nonlinear <.01, Figure 2a)). The risk of ADHD reached its peak when the CRP was at 2.75 mg/L (OR = 1.89, 95% CI [1.39, 2.57]). However, no significant associations were observed between other inflammatory markers and ADHD in this study (p > .05, see Figure 2).
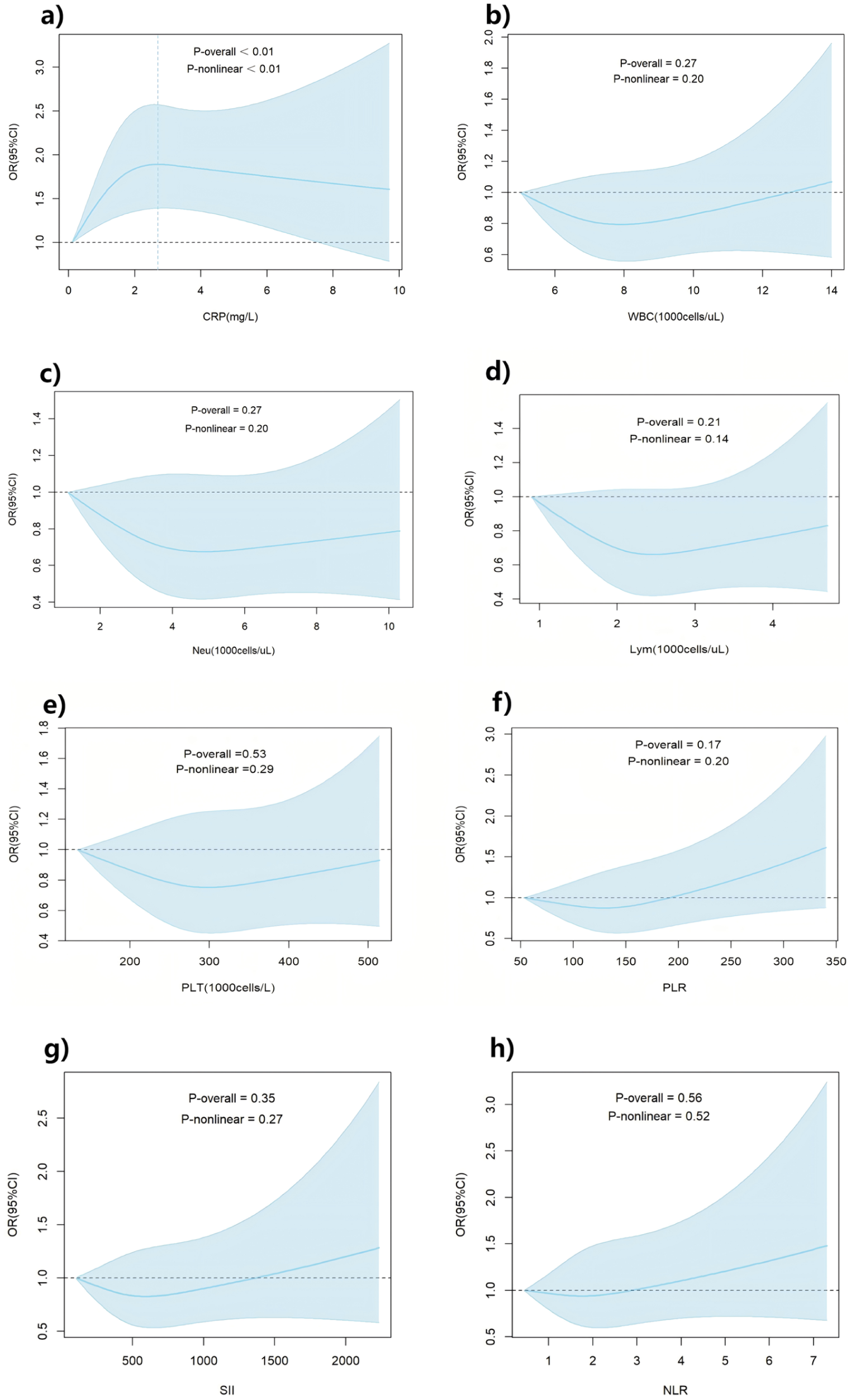
The odds ratio of ADHD with inflammatory biomarkers: (a) The odds ratio of ADHD with CRP. (b) The odds ratio of ADHD with WBC. (c) The odds ratio of ADHD with Neu. (d) The odds ratio of ADHD with Lym. (e) The odds ratio of ADHD with PLT. (f) The odds ratio of ADHD with PLR. (g) The odds ratio of ADHD with SII. (h) Theodds ratio of ADHD with LNR.
The Risk of ADHD Associated With Inflammatory Biomarkers in Different LTPA Groups
After adjusting for all confounding factors, when the LTPA duration was below the recommended level, each 1 mg/L increase in CRP was associated with a 10% increase in the risk of ADHD (p < .05). Furthermore, compared with the non-CLGI group, the CLGI group demonstrated a significantly higher risk of ADHD (OR = 1.64, 95% CI [1.02, 2.63]). However, when the LTPA duration was exceeded the recommendation, the association between each 1 mg/L increase in CRP and ADHD risk was statistically insignificant (p > .05). Simultaneously, no statistically significant difference in the risk of ADHD in the CLGI group was observed compared with the non-CLGI group (OR = 1.42, 95% CI [0.77, 2.64]).
Moreover, there was an interaction between LTPA and CRP in ADHD (p for interaction<.05), indicating that compared with the LTPA <60 min/day group, the association between ADHD and CRP was moderated in the “LTPA ≥60 min/day” group (Table 3).
Logistic Regression Analysis of the Association Between Inflammatory Biomarkers and ADHD in Different LTPA Groups.
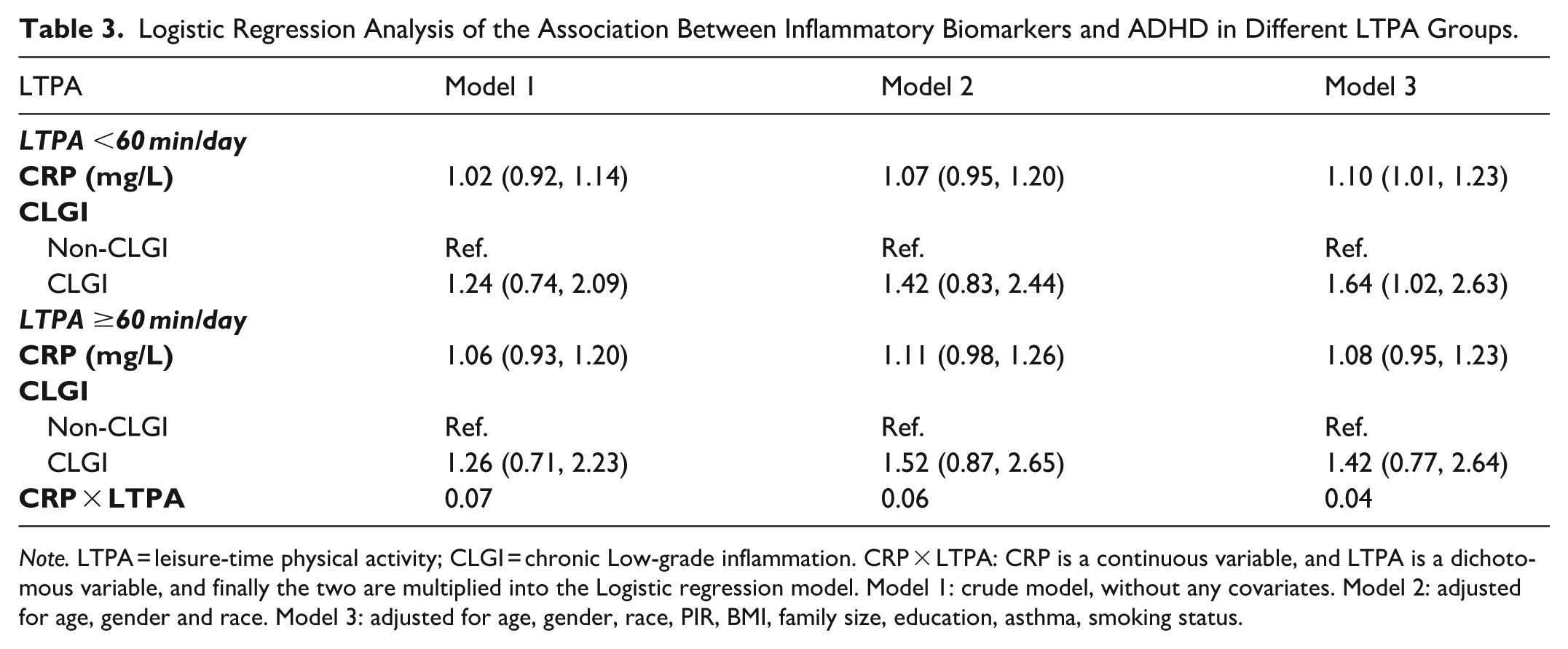
Note. LTPA = leisure-time physical activity; CLGI = chronic Low-grade inflammation. CRP × LTPA: CRP is a continuous variable, and LTPA is a dichotomous variable, and finally the two are multiplied into the Logistic regression model. Model 1: crude model, without any covariates. Model 2: adjusted for age, gender and race. Model 3: adjusted for age, gender, race, PIR, BMI, family size, education, asthma, smoking status.
In the group engaging in less than 60 min of LTPA per day, the risk of ADHD significantly increased with rising CRP concentrations, peaking at 2.84 mg/L (OR = 1.98, 95% CI [1.33, 2.92]). Conversely, within the group participating in 60 min or more of LTPA daily, the association between CRP and ADHD risk was less pronounced. The peak risk occurred at a CRP concentration of 2.49 mg/L (OR = 1.57, 95% CI [0.95, 2.62]), after which the risk gradually declined (Figure 3).
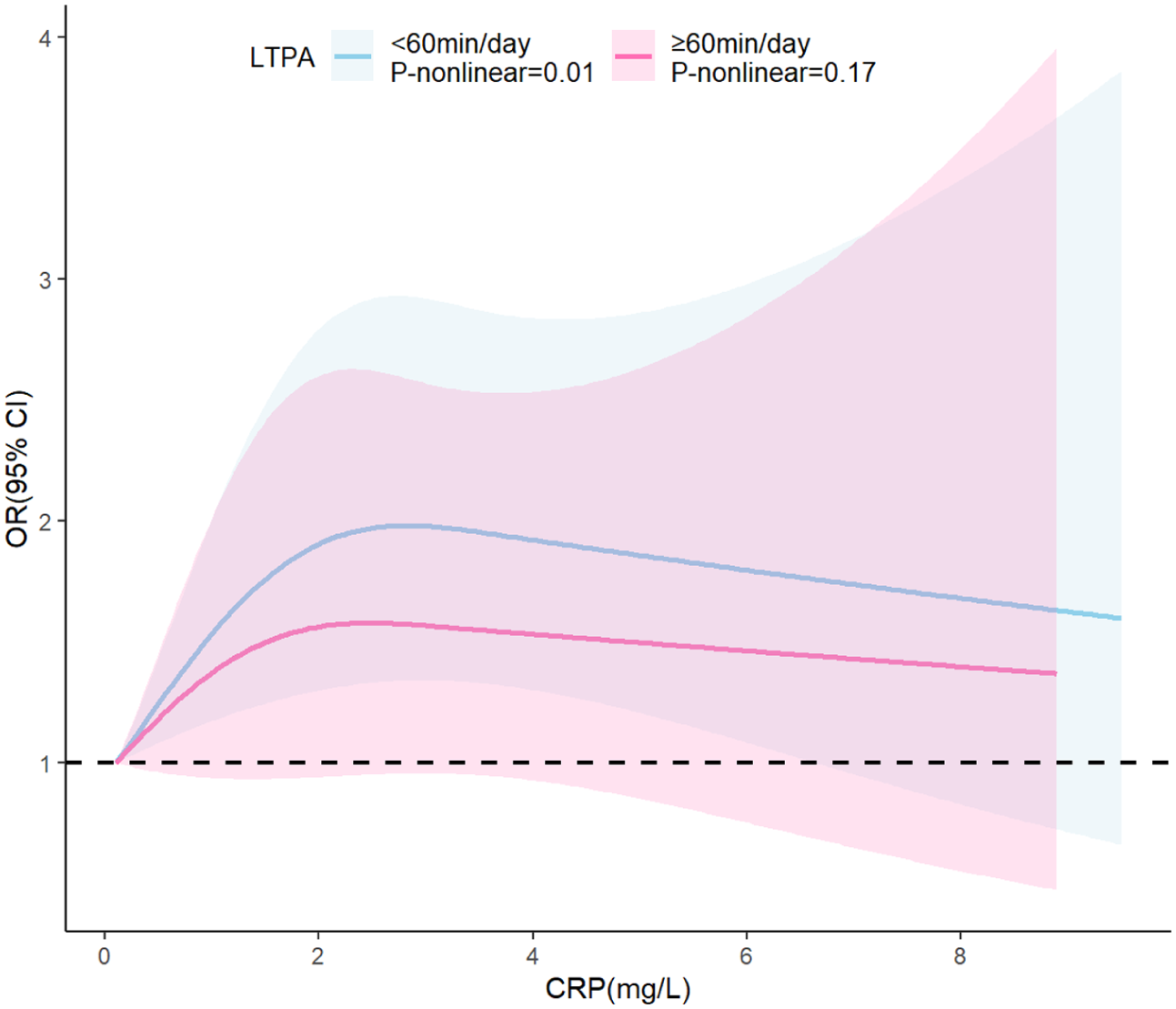
The odds ratio of ADHD with CRP by LTPA type.
Subgroup Analysis of LTPA Interaction Effects
The subgroup analyses revealed a significant moderating effect of LTPA among males, females, Mexican Americans, overweight/obese individuals, households with four to six members, those with middle or high school education level, individuals without asthma, current smokers, participants with both high and low PIR, and adolescents aged 12 to 14 years (p for interaction <.05, see Table 4).
Subgroup Analysis of the Moderating Effect of LTPA.
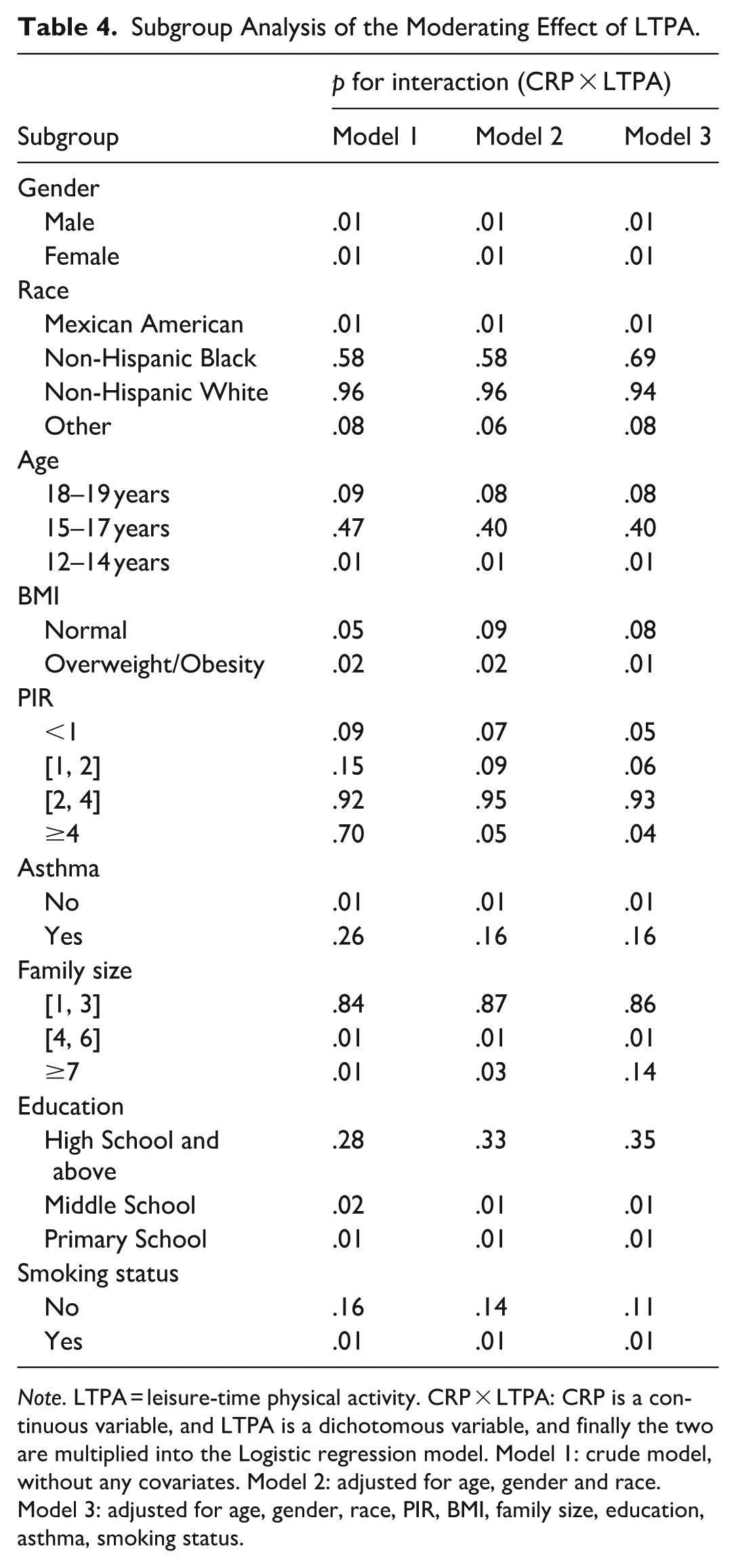
Note. LTPA = leisure-time physical activity. CRP × LTPA: CRP is a continuous variable, and LTPA is a dichotomous variable, and finally the two are multiplied into the Logistic regression model. Model 1: crude model, without any covariates. Model 2: adjusted for age, gender and race. Model 3: adjusted for age, gender, race, PIR, BMI, family size, education, asthma, smoking status.
Discussion
Main Findings
By utilizing 1999–2004 NHANES data, this study discovered that CLGI is a risk factor for ADHD, and CRP could serve as a potential inflammatory biomarker for ADHD. More than 60 min/day LTPA may moderate the association between CRP and the risk of ADHD. These findings provide new insights into the pathophysiology of ADHD and imply that engaging in more physical activities may exert a protective effect.
Association Between Inflammation and ADHD
Accumulating evidence has implicated inflammation in the pathophysiology of ADHD. The underlying mechanisms involve microglial activation-mediated neuroinflammation (Réus et al., 2015), oxidative stress amplification (Hassan et al., 2016), impaired neurotrophic support (Sen et al., 2008), and blood-brain barrier (BBB) dysfunction (Pollak et al., 2018). Consistent with the inflammatory hypothesis, this study identified a significant association between elevated CRP levels and ADHD while no significant associations were observed for the other inflammatory markers. This discrepancy between our findings and some previous study can be explained by several pivotal factors.
First, population heterogeneity may play a critical role. Previous studies reporting elevated CBC-derived markers were primarily based on clinical samples from specialized hospitals, which tend to capture individuals with more pronounced symptoms or acute care-seeking behavior (Akinci & Uzun, 2021; Gędek et al., 2023). This study used a community-representative NHANES sample encompassing a broader spectrum of ADHD severity, including mild or stable cases. In such a diverse population-based survey, the subtle immune signals observed in specific clinical subgroups may be attenuated by the high heterogeneity of the general population. Second, differences in statistical power and potential selection bias should be considered. Prior positive studies utilized relatively small sample sizes (N = 60 –552), which are more susceptible to selection bias and may overestimate effect sizes. However, this study utilized the NHANES database, including 4,817 participants with complete inflammatory markers and covariate information, providing relatively high statistical power. The non-significance of CBC-derived markers in this large model suggests that the robustness as universal biomarkers for ADHD in the general population requires further validation. Notably, our results are not entirely divergent from existing literature; for instance, the lack of significance for Lym, Mon, and MLR in the study by Akinci and Uzun (2021) aligns with our null results. Third, the inherent biological stability of these markers may explain the superior performance of CRP. Peripheral blood cell counts (e.g., WBC, Neu) and related immune indices can reflect immune status but are susceptible to acute physiological fluctuations (e.g., recent infection, stress, diurnal variation) (Haus & Smolensky, 1999; Juul et al., 1984; Li et al., 2020). In contrast, CRP—a stable hepatocyte-derived protein with a half-life of approximately 19 hr—may better reflect the level of CLGI (Kozlowska et al., 2019; Yin et al., 2020). Given that ADHD is a chronic neurodevelopmental disorder, CRP is physiologically more likely to exhibit consistent associations than immune indices prone to acute fluctuations (Kozlowska et al., 2019; Yin et al., 2020). Meanwhile, the direct mechanistic pathway of CRP on brain function provides additional biological plausibility. Unlike many peripheral immune cells that may not cross the BBB under mild inflammatory conditions, CRP may have a more direct pathway to affecting brain function. Evidence indicates that CRP can increase BBB permeability and interact with Fcγ receptors on microglia and brain endothelial cells, potentially triggering neuroinflammatory cascades in regions critical for ADHD, such as the prefrontal cortex and basal ganglia (Kadry et al., 2020; Kuhlmann et al., 2009; Ullah et al., 2021).
Although most inflammatory markers examined in this study were not significantly associated with ADHD, this does not preclude a role for inflammation in the broader pathophysiology of ADHD. Instead, our findings highlight the complexity of identifying robust, inflammatory biomarkers and suggest that CRP—owing to its stability and potential for central nervous system interaction—may be a particularly sensitive peripheral indicator of inflammatory dysregulation in ADHD. Future longitudinal studies incorporating multidimensional biomarker assessments are needed to improve the reliability and validity of inflammatory profiling and to clarify the specific roles of distinct immune pathways across ADHD.
The Overall Effect of LTPA on the Link Between Inflammation and ADHD
Multiple studies have identified physical activity as a protective factor for ADHD (Dastamooz et al., 2023; Huang et al., 2023; Sun et al., 2022), with evidence supporting its dual benefits in mental health promotion and anti-inflammatory processes (Gleeson et al., 2011; Luo et al., 2024). However, prior research has not explicitly investigated whether LTPA could modulate the relationship between inflammatory biomarkers and ADHD risk. Frank et al. (2019) found that physical inactivity may mediate the association between CLGI and exacerbated depressive symptoms. This study reveals a significant interaction between LTPA and CRP on ADHD risk, showing increased disease susceptibility with elevated CRP levels and decreased risk with greater LTPA engagement.
The neuroprotective mechanisms of LTPA in inflammation-related ADHD pathogenesis may involve three critical pathways: First, regular exercise exerts anti-inflammatory effects by reducing pro-inflammatory cytokines (e.g., IL-6, TNF-α, CRP) while simultaneously enhancing anti-inflammatory mediators (e.g., BDNF, IL-10) (Kasapis & Thompson, 2005; Loprinzi & Ramulu, 2013), thereby mitigating neuroinflammation. Second, sustained physical activity attenuates endothelial oxidative stress, strengthens the integrity of BBB, and prevents inflammatory damage to the striatal circuitry, consequently preserving neurotransmitter regulation. Additionally, LTPA promotes neuroplasticity through structural brain modifications, optimized neural connectivity, and enhanced synthesis of neurotransmitters and neurotrophic factors (Huang et al., 2023; Sun et al., 2022). These adaptions collectively—mediated through cytokine regulation (Luo et al., 2024), antioxidant enzyme activation (Kasapis & Thompson, 2005), and neuroendocrine modulation (Gleeson et al., 2011)—effectively reduce neuroinflammation and confer protection against ADHD development.
Subgroup Analysis of LTPA Interaction Effect
The neuroprotective effect of LTPA was robust in the 12 to 14 age group (p = .01), which may be attributed to the heightened vulnerability of developing prefrontal-striatal circuitry to inflammatory insults during early adolescence, compounded by escalating psychosocial stressors (e.g., academic pressures, social anxiety) in this population (Adelantado-Renau et al., 2020; Kasapis & Thompson, 2005; Yim et al., 2010; Zielinski et al., 2010). Mechanistically, LTPA may moderate the association between CRP and ADHD risks through multi-target interventions, including anti-inflammatory cytokine regulation, HPA-axis stabilization, and neurotrophic factor-mediated circuit optimization (Gleeson et al., 2011; Luo et al., 2024).
The interaction between LTPA and CRP in overweight/obese adolescents was significant (p = .01). While obesity and overweight may impair neuroplasticity and promote neuroinflammation (Lee & Yau, 2020), LTPA may mitigate inflammatory responses by enhancing adiponectin and insulin sensitivity, thereby reducing neuroinflammation risk (Kasapis & Thompson, 2005).
The low PIR group has experienced chronic stressors (e.g., housing insecurity), which may trigger inflammation through overactivation of the hypothalamic-pituitary-adrenal (HPA) axis and elevated levels of pro-inflammatory cytokines (Hänsel et al., 2010; Muscatell et al., 2020). In contrast, individuals in the high PIR group exhibit different physiological responses, which may be associated with more adaptive stress regulation mechanisms (Allen et al., 2017; Thacker et al., 2024).
Individuals without asthma may derive greater anti-inflammatory benefits from LTPA, as chronic airway inflammation and exercise limitations associated with asthma may diminish these effects (Leffa et al., 2021). Interestingly, the interaction also remained significant among current smokers. This could be due to their higher baseline CRP levels, offering greater potential for improvement through LTPA, or a “healthy smoker” effect, where physically active smokers may possess better overall health behaviors and resilience against inflammation-related cognitive decline (Ambrose et al., 2020). Taken together, these findings suggest that the moderating role of LTPA in the CRP-ADHD relationship is robust across diverse demographic and behavioral contexts, although the underlying mechanisms may differ by subgroup.
Crucially, LTPA could modulate neuroinflammation through multimodal mechanisms—inflammatory marker suppression (Kasapis & Thompson, 2005), gut microbiota modulation (Quiroga et al., 2020), and psychosocial support enhancement (Kandola et al., 2019)—ultimately reducing ADHD susceptibility across socioeconomic strata.
Strengths and Limitations
This article presents the following strengths: (1) This study utilized logistic regression and RCS to investigate the intricate relationship among LTPA, inflammatory biomarkers, and ADHD. These findings indicated that inflammatory biomarkers were associated with the risk of ADHD, and LTPA could modulate the association between CRP and ADHD risk; (2) In comparison with prior studies, this research leveraged a larger sample size and subgroup analyses to elucidate the regulatory effects of LTPA across diverse populations.
This article also acknowledges certain limitations. First, this study does not allow interpretation for causality because of its cross-sectional nature, so more prospective studies are needed to delve deeper into the relationship between them. Second, several measurement limitations should be acknowledged: (1) The identification of ADHD was based on self-reported information, which might be prone to recall bias; (2) inflammatory markers in peripheral blood were assessed using a single blood sample, which may limit the reliability and representativeness of these measurements; (3) Specific cytokine analyses (e.g., IL-6, TNF-α) could not be conducted as they were not included in the standardized NHANES 1999–2004 laboratory protocols. As these cytokines are considered more direct mediators of the neuroinflammatory pathways discussed in recent literature, the inability to assess them limits our capacity to fully map the intricate inflammatory landscape associated with ADHD. While CRP serves as a robust and well-established marker of CLGI in large-scale epidemiological research, it may not capture the nuanced functional dynamics of specific immune cell signaling. Consequently, future research integrating a broader array of both pro-inflammatory and anti-inflammatory cytokines is essential to further elucidate the granular immune-brain mechanisms underlying ADHD; and (4) the reliance on self-reported physical activity data introduces the potential for recall bias and social desirability bias, highlighting the need for more objective assessment tools. Future studies may benefit from integrating accelerometry with behavioral questionnaires to enhance data accuracy and reliability. Third, although adjustments were made for relevant covariates, residual confounding (e.g., medications, comorbidities) remains a concern. While we observed no statistically significant associations between ADHD and other CBC-derived inflammatory markers (e.g., NLR, PLR), these null findings are important. They suggest that such hematological ratios might be sensitive to specific clinical contexts—such as high symptom severity or specific comorbidities—and may not be robustly associated with ADHD in the broader community-based population. Therefore, future research should replicate these findings in cohorts with more detailed comorbidity information. Additionally, the definition of CLGI was based on general CRP thresholds; future studies should aim to establish pediatric-specific CRP cutoffs through analyses of larger and more diverse pediatric populations.
Conclusions
Elevated CRP levels are positively associated with ADHD. More than 60 min/day LTPA may moderate the association between CRP and the risk of ADHD.
Supplemental Material
sj-docx-1-jad-10.1177_10870547261458103 – Supplemental material for Association of Inflammatory Biomarkers With ADHD and Moderating Effect of Leisure-Time Physical Activity in Adolescents: A Cross-Sectional Study Based on NHANES
Supplemental material, sj-docx-1-jad-10.1177_10870547261458103 for Association of Inflammatory Biomarkers With ADHD and Moderating Effect of Leisure-Time Physical Activity in Adolescents: A Cross-Sectional Study Based on NHANES by Keyu Pan, Shanru Jin, Xiang Gao, Changshuang He, Beibei Shi, Meng Zhang, Yiting Wei and Minghui Quan in Journal of Attention Disorders
Footnotes
Acknowledgements
The study presented in this paper utilized data from the National Health and Nutrition Examination Survey (NHANES). We are grateful to the NHANES program and all participants for their contributions.
List of Abbreviations
Ethical Considerations
The National Health and Nutrition Examination Survey (NHANES) is a publicly available database approved by the National Center for Health Statistics institutional review board. Ethical review and approval were waived for this study since secondary analysis did not require additional institutional review board approval.
Consent to Participate
All participants provided written informed consent when they participated in the national survey in the United States.
Author Contributions
Keyu Pan
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Major Project of the National Social Science Fund of China (Grant No.25&ZD251); the “Dawn” Program of the Shanghai Municipal Education Commission (Grant No. 22SG49); and the Shanghai Oriental Talents Program (Youth, 2023).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.