
Abstract
Introduction:
Neurodiversity proponents claim ADHD is a value-neutral, minority neurotype subject to marginalization and discrimination. This paper explores, guided by lived-experiences it’s applicability to ADHD and contrasts it with the medical model and the overmedicalization critique. Here, ADHD is respectively considered as a deficit-to-be-cured or a societal problem compromising identity, fostering stigma and inducing medication use.
Methods:
We conducted a narrative review of in-depth interview studies with ADHD adolescents and adults focused on experiencing: core ADHD characteristics, disablement, diagnosis and medication and evaluated which approach to ADHD matches best the lived experience of ADHD.
Results:
In these lived experiences (1) ADHD characteristics are generally not experienced as universal deficits (2) disability primarily stems from an invalidating mismatch between the ADHD person and their neuronormative environment (3) the ADHD diagnostic label brings both beneficial and disadvantageous consequences and (4) using medication requires balancing its bodily and identity impact, while needing it to navigate unaccommodating environments and meeting self-determined goals.
Discussion:
We conclude that considering ADHD as mere difference instead of as a universal deficit reflects people’s lived experience and eases the self-acceptance of an ADHD diagnosis. Also, conceiving of disability as a person-environment mismatch, rather than as purely individual nor as induced by labeling, provides a helpful framework for the balancing act of medication use. Since ADHD and autistic experiences don’t match entirely, we outline future debates among neurodiversity proponents. Overall, we believe the neurodiversity approach to ADHD is a promising and destigmatizing alternative inspiring new research, clinical and societal pathways.
Introduction
In online and offline discussions, there is an ongoing tendency to view Attention Deficit/Hyperactivity Disorder (ADHD) as an expression of human neurodiversity. ADHD bloggers and content creators, self-advocates, and also some neurodivergent clinicians and academics increasingly claim that ADHD shouldn’t be simply approached as a neurodevelopmental disorder (Carfagnini, 2025; Family First Adolescent Services, 2024; Huijg, 2025). Contrary to mainstream academic and clinical views, they argue that ADHD can and should be seen as a value-neutral neurodivergence: a profile of experiencing and engaging with the world that deviates from dominant cognitive and behavioral norms, but which cannot simply be labeled as a pathology.
Rather than seeing ADHDers 1 as a group of patients needing to be “fixed” by means of medication or psychotherapy, neurodiversity proponents conceive ADHD people as a societal minority group faced with structural injustices, striving for emancipation. In this emancipatory effort, ADHD self-advocates demand that the voices and experiences of people with ADHD are placed center stage (Bertilsdotter Rosqvist et al., 2023; Jackson-Perry et al., 2025).
Our goal for this paper is to explore the applicability, relevance and nuances of a neurodiversity approach to ADHD. More broadly, we aim to contribute to emerging scholarly debate on applying the neurodiversity paradigm beyond autism (for dyslexia see (Rubery, 2022); for dyspraxia see (Elsherif, 2025); for Tourette’s see (G.-J. Vanaken et al., 2025)).
We will proceed in three sections. First, we will introduce the neurodiversity movement and approach, contrasting it with two other dominant approaches in the ADHD field: the medical model and the overmedicalization critique. Here we will argue that in both dominant approaches, first-person perspectives of ADHD are significantly under-represented, compromising the validity of these approaches. In the second section, we will therefore examine key claims of the different approaches to ADHD, based on a narrative selective review of studies documenting first-person perspectives of adolescents and adults with ADHD. While we will point at specificities of ADHD, in the third section, we will ultimately conclude that there are decent empirical arguments in favor of applying a neurodiversity approach to ADHD. Moreover, we believe this approach may be fruitful for both research and clinical work in the ADHD field.
As authors, our collective experience includes conducting research in ADHD and/or autism, either with a background in psychology and philosophy, clinical practice with neurodivergent individuals (mainly ADHD), and personal or familial connections to ADHD. We are Dutch, English and Belgian, and our varied positions—as neurodivergent and neurotypical researchers, as clinicians and academics, and as individuals with close relational ties to neurodivergent experiences—informs our approach to this work.
Neurodiversity, Medical and Overmedicalization Approaches to ADHD
We start this section with an introduction to the neurodiversity movement in general. Thereafter, we provide brief overviews of the key tenets of medical, overmedicalization and neurodiversity approaches to ADHD.
Neurodiversity Movement
The neurodiversity movement can be traced back to the online organizing and self-advocacy of autistic adults in the 1990s. The phrasing “neurological diversity” stems from early conversations taking place via mailing lists hosted by autistic organizers such as Martijn Dekker (Botha et al., 2024). Following this grassroots development, the term “neurodiversity” got picked up early on in both press and academic writing (Blume, 1998; Singer, 2017). Yet, it was only in the past decade that it entered mainstream and academic conversations more systematically (Silberman, 2015).
Currently, the concept of neurodiversity is used as a descriptor of the significant human diversity regarding cognitive, sensorial, behavioral, emotional and communicative ways of experiencing and engaging with the world. The neurodiversity movement, a social movement, strives for acceptance of such diversity and emancipation of neurodivergent minorities against the backdrop of a society organized to meet primarily neurotypical needs (Kapp, 2020). Opposition to biomedical efforts at preventing or curing conditions such as autism has been key in this movement. More specifically, resistance against behavioral interventions such as neuronormative social skills training (Dawson, 2004; Roberts, 2021) and resistance against research in genetics risking the development of prenatal tests for autism, have been at the forefront of neurodivergent organizing (Pring, 2021).
In academia, the neurodiversity paradigm has equipped researchers with a new, critical lens to decenter neurotypical norms, politicize neurodivergent experiences and produce relevant knowledge from the neurodivergent margins (Bertilsdotter Rosqvist et al., 2020; Dwyer, 2022; G. J. Vanaken, 2023; Walker, 2021). Over the course of just a few years, this new paradigm has shown to be productive, both in fundamental and more applied autism research. This led to the introduction of new and relevant concepts such as autistic burnout, masking, inertia and stimming. Autistic researchers revitalized cognitive autism research by proposing new theories that are no longer deficit-based, for example, the double empathy hypothesis and monotropism theories of autism (Milton, 2012; Murray et al., 2005). Similarly, transformations are taking place in clinical autism research and practice. Newly developed, neurodiversity-affirming approaches to diagnostic assessment and psychoeducation promise to foster self-insight self-acceptance and empowerment among autistic people and their relatives (H. M. Brown et al., 2021; Hartman et al., 2023; Pritchard-Rowe & Gibson, 2024). In therapy, existing approaches are being adjusted based on autistic people’s input, and new practices are popping up. This includes, for example post-diagnostic peer support groups (co-)led by autistic people which aim to foster a positive autistic identity buffering against prevalent mental health issues such as loneliness, anxiety and depression (Crane et al., 2021; Davies et al., 2024; Edwards et al., 2025).
Clearly, starting knowledge production from the inside out, based on the experiences and priorities of the community at hand, has proved fruitful in the autism field. In the past years there have been calls to apply neurodiversity approaches not just to autism, but to other conditions traditionally seen as neurodevelopmental “disorders,” including ADHD (Campbell, 2020; Huijg, 2025). More recently, such calls have been responded to with a first set of papers aiming to outline the contours of a neurodiversity-affirming approach to ADHD by ADHD academics (Bertilsdotter Rosqvist et al., 2023, 2025; Jackson-Perry et al., 2025).
To establish its unicity, authors tend to distinguish this neurodiversity approach from a medical (sometimes also referred to as the pathology paradigm), and from an overmedicalization approach to ADHD (sometimes referred to as a “diagnosis critical” or “social constructionist” approach) (e.g., Banaschewski et al., 2024; Dwyer, 2022; Jackson-Perry et al., 2025). We are aware that any such comparison of approaches to ADHD is vulnerable to simplifications and reductions, risking strawman discussions between their proponents. Nevertheless, we believe it is insightful to make such a comparison as it helps to show the limits of the latter two approaches and the potential of exploring a neurodiversity approach to ADHD in more detail. Concretely, we will describe how proponents of each of these approaches conceptualize ADHD, how they conceive of knowledge production and expertise, and which goals they pursue. In Table 1 we provide an overview of assumptions of the three approaches, note that these assumptions not necessarily reflect the nuances within each approach.
Approaches Toward ADHD.
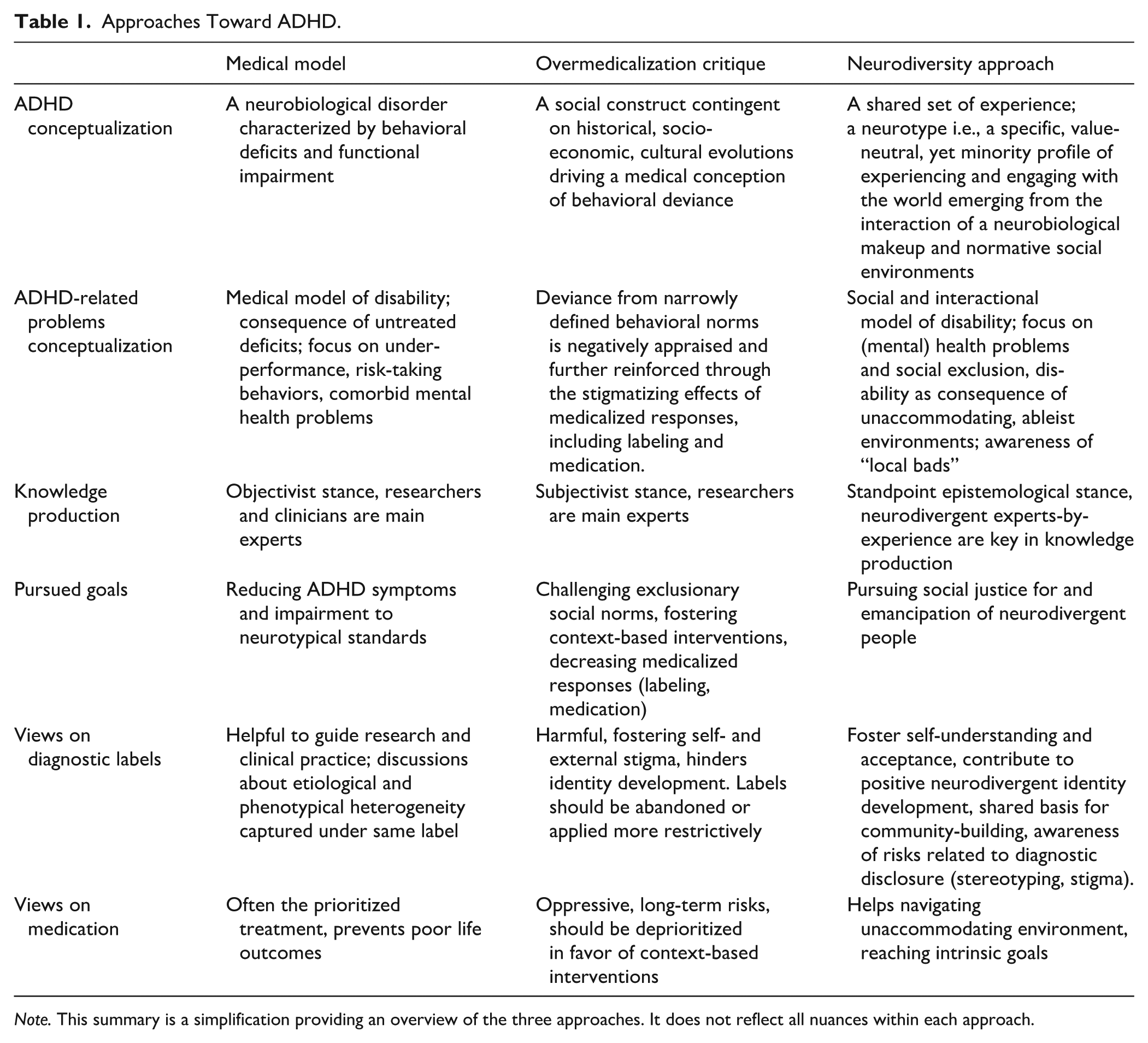
Note. This summary is a simplification providing an overview of the three approaches. It does not reflect all nuances within each approach.
The Medical Model
The vast majority of academic work on ADHD, especially in fundamental biomedical and psychological research and in applied clinical research, has been conducted from (what we refer to as) a medical model approach. In this body of work, explicit acknowledgement of scientific paradigms is scarce, let alone the phrasings “medical model” or “pathology paradigm.” Nevertheless, the conception of ADHD can be deduced. The World Federation of ADHD International Consensus Statement (Faraone et al., 2021), and the Nature Reviews Disease Primers piece on ADHD (Faraone et al., 2024) serve as exemplary writings here.
In a medical model approach, ADHD is assumed to be a neurodevelopmental disorder which unfolds primarily within an individual person. The etiology of ADHD is diverse and multifactorial, but genetic factors are considered to contribute strongly. The underlying mechanisms of ADHD symptoms are assumed to be found in neurobiology and psychological functioning (Faraone et al., 2021). Despite the acknowledgement of the dimensional distribution of ADHD traits and despite the difficulty of finding biological markers, in a medical model approach, ADHD continues to be seen as a categorically different way of developing and functioning which requires clinical attention (Faraone et al., 2024). Although nowadays voices of people with lived experience are more and more heard, this approach is primarily characterized by a positivist research paradigm conceiving of ADHD as a natural entity which can be studied objectively from the outside-in with researchers as the main experts and contributors to knowledge production (Faraone et al., 2024).
Clinically, ADHD is conceived of as an observable set of impairing behaviors often first observed in childhood. These behaviors are understood as manifestations of deficits in sustained attention, lack of impulse control and a surplus of bodily and/or verbal activity (American Psychiatric Association, 2022). Pharmacotherapy, psychotherapy and other clinical interventions mainly aim to reduce core symptoms, comorbid mental health problems and functional impairment, for which there is generally good quality quantitative evidence. More than quality of life, symptom reduction is often considered the primary outcome in research and clinical evaluation. Impairment here is commonly understood as academic or professional underachievement and risk-taking behaviors such as drug abuse, dangerous driving and delinquency.
The Overmedicalization Critique
Over the past decades, even before the rise of the neurodiversity movement, the medical model of ADHD has been criticized by social scientists and social commentators. These critics move away from a positivist toward a social constructionist interpretation of ADHD. Here, ADHD is primarily viewed as a product of medicalization. Medicalization is a sociological concept dating back to the 1970s which refers to the dynamic where medical knowledge, terminology and authority gains ground in domains of life previously outside the scope of medicine. Non-medical, defiant behavior for which non-medical solutions were sought is gradually framed in medical terms. Medical knowledge gets developed and medical treatments are applied to gain control over the behavior in case.
The American sociologist Peter Conrad, one of the founding fathers of the medicalization concept, kickstarted ADHD research from such a social constructionist approach by taking ADHD as a case for his theory (Conrad, 1975). Conrad, and subsequently others, pointed out how the hardly known condition “hyperkinesis” transformed into “ADHD” and came to apply to millions of people over the course of the second half of the 20th century (Bergey, 2024; Conrad & Bergey, 2015, 2014; Conrad & Schneider, 1992). Key mechanisms in the 1960s included the marketing of methylphenidate as targeted treatment for this condition and the formalization of the diagnosis in the Diagnostic and Statistical Manual of Mental Disorders (DSM) (American Psychiatric Association, 2022). In more recent editions of DSM, focus shifted from hyperactivity in childhood to also including inattention issues (without hyperactivity) over the course of a lifetime. This way the diagnostic label became more applicable to girls and adults and drove rising diagnostic rates (Lusardi, 2019).
Strictly speaking, medicalization is a nonjudgemental concept. It purely serves to describe a process without taking a normative stance. It can be considered on par with descriptive concepts such as industrialization or urbanization (Conrad & Bergey, 2015). Yet, in what we call “the overmedicalization critique,” the original concept of medicalization gets combined with normative claims. Medicalization went too far and causes negative effects, the critique says. More specifically, overmedicalization critics point to issues around rising diagnostic prevalence, excessive labeling, and medication use (Banaschewski et al., 2024; Dekkers, 2024; Freedman & Honkasilta, 2017; Honkasilta & Koutsoklenis, 2022; Rafalovich, 2013).
More concretely, critics claim being labeled as disordered fosters external and self-stigma, induces a self-fulfilling prophecy of lowered achievements and negatively impacts identity development (Dekkers, 2024; Honkasilta & Koutsoklenis, 2022). A diagnosis is not seen as a gateway to address issues people with ADHD experience, being labeled actively contributes to such undesirable outcomes. In strong formulations of this overmedicalization critique classificatory diagnostics should be abandoned entirely. Diagnostic labels do not capture a homogenous, natural entities. Nor do they explain sufficiently why someone experiences the life challenges they do. Moreover, these labels in and of themselves would poorly guide clinical care and should be replaced by individualized and contextualized needs-based assessments (Timimi, 2015, 2017; Timimi & Taylor, 2004; Van Os, 2026). Less strong formulations of the overmedicalization critique mainly note that the ADHD label is a product of human deliberation. The diagnostic criteria, diagnostic instruments and clinical judgment aren’t simply delineating a natural entity (Banaschewski et al., 2024; Dekkers, 2024). This can open up the door to concept creep, especially for those on the so-called milder end of the ADHD spectrum (De Vries et al., 2025; Kazda et al., 2021). This latter group of critics still acknowledge the label can be helpful for some people, be it in a more restrictive sense which better balances benefits and harms associated with such labeling (Banaschewski et al., 2024; Dekkers, 2024). Regarding pharmacotherapy, some overmedicalization critics claim that ADHD medication, although backed by a wealth of medical evidence and clinical guidelines, serves as an authoritative form of social control of deviant behavior which unjustly shifts the risk of (long-term) side-effects to people with ADHD (Horwitz, 2010; Rafalovich, 2013). Additionally, impairments associated with ADHD are argued to be primarily contextually contingent and less a direct, unmediated outcome of core ADHD features. It is argued that more attention should be paid to challenging exclusionary societal norms and to contextual interventions that improve the person-environment match, such as parent training (Banaschewski et al., 2024; Dekkers, 2024).
The Neurodiversity Approach
Departing from medical and overmedicalization approaches, neurodiversity proponents introduce a third, distinctive way to view ADHD. 2 Here, the focus is also as in the overmedicalization critique to depathologize ADHD and reconceptualize it as a merely different way of functioning and developing. ADHD features can manifest as difficulties, but equally so as strengths. Think of some ADHDers’ ability to hyperfocus on issues that capture their interest strongly (Jackson-Perry et al., 2025).
In addition, neurodiversity proponents not only seek to depathologise, but also to contextualize and politicize ADHD: the way that ADHD characteristics play out as challenges and strengths, and the extent to which ADHD is related to functional impairment critically depends on social norms, environmental support and power dynamics. Clearly, this approach differs from a mere pathological approach, but it also does not align either with simplistic celebratory takes, framing ADHD as a so-called superpower.
Importantly, a neurodiversity approach to ADHD also differs from the overmedicalization critique as it does not consider ADHD solely as a label or a discursive product, let alone a strictly negative or even oppressive one. Being ADHD, in all its diversity, is first of all a set of minority experiences shared among other ADHD people. Those experiences are partly grounded in biological realities, neurodiversity proponents claim, but emerge in relation to social norms (Bervoets, 2022; Fitzgerald, 2017). Shared experiences are for example, being perceived as “lazy,” overly “intense,” “all over the place” or “restless.” Those are partly manifestations of a given neurological set-up, neurodiversity proponents claim, but only lead to such negative appraisals, exclusionary experiences and overcoming efforts, in societies expecting people to be productive, calm and composed. 2
Neurodiversity proponents claim that the neurodivergent characteristics captured under the ADHD label precede formal recognition and diagnosis. The diagnostic label offers a particular lens to interpret and make sense of these experiences, but the label is not what generates ADHD characteristics in the first place nor does it cast a merely negative shadow over the lives of those who are labeled—as some overmedicalization scholars tend to claim (Honkasilta & Koutsoklenis, 2022; Rafalovich, 2013; Timimi & Taylor, 2004).
Also, and this is a crucial element which sets the approach apart from both medical and overmedicalization approaches, neurodiversity proponents insist on the agency of ADHD people themselves. ADHDers, it is argued, possess a unique, first-person perspective to contribute to knowledge production. It is therefore not merely an ethical issue to include ADHD people in ADHD research and clinics, but also an epistemological matter: more complete and more socially relevant knowledge on ADHD can be produced if first-person perspectives are considered. Emerging community-driven theorizing on concepts such as “hyperfocus” and “interest-based attention” (Bertilsdotter Rosqvist et al., 2023), research priority setting exercises, ADHD-led and participatory research practices exemplify this move (Brown, 2024; Hultman & Hultman, 2024).
As mentioned, this neurodiversity approach has its origins in autistic communities. Instead of opting for a quick copy-and-paste from autism to ADHD, we believe it is worth exploring to what extent the assumptions and claims of this neurodiversity approach line up with the experiences of ADHDers and which amendments might be required. Also, if the neurodiversity approach claims to provide a superior framework to conceive of the ADHD experience, the gaps in medical model and overmedicalization critique should be visible when reviewing the documented lived experience of ADHD. This is what we set out to do in the next section.
The Lived Experience of ADHD
In the following section we provide a narrative overview of first-person experiences of ADHD as documented in qualitative studies with ADHD adolescents and adults. This overview is based on a non-systematic narrative literature review exploring four topics which are key to ADHD lived experience and to our research question. The first two topics are derived from claims of the medical model approach. Are ADHD characteristics indeed experienced as deficits (Not Experiencing ADHD as a Universal Deficit)? Are functional impairments experienced as direct consequences of such deficits (ADHD is Mainly Experienced as a Mismatch With the Environment; This Mismatch Has Far-Reaching Consequences)? Topics three and four are based on assumptions of the overmedicalization critique. Are being diagnosed as ADHD (Ambivalent Experiences of Being Diagnosed With ADHD) and taking ADHD medication (Experiencing Medication) negative, oppressive experiences which should be amended or avoided altogether?
Not Experiencing ADHD as a Universal Deficit
As mentioned, in the medical model approach, ADHD behaviors are considered deficits in attention, activity levels and impulse control. While this approach acknowledges heterogeneity, it tends to portray differences in attention, activity and impulse control as disadvantageous characteristics across the board, as universal deficits. However, qualitative research sheds a different light on the topic. For example, a young adult with ADHD puts it as follows:
I think that deficit might not be the right word because I have an abundance of attention at times, it’s just that I can’t direct it. I don’t get to choose what I pay attention to (Ginapp et al., 2023).
Adolescents and adults rather report fluctuations in their functioning, which are probably better captured by the terms “dysregulation of attention” (Ginapp et al., 2023), “variability in attention” (Bertilsdotter Rosqvist et al., 2023; Fusar-Poli et al., 2024) or “struggling to focus on the ‘right’ thing” (Gerling et al., 2024). In some studies, adults with ADHD describe intermittent abundance of attention (“hyperfocus”), which can be valued at times.
I definitely experience hyperfocus and it’s like my superpower when it’s good . . . I can produce a lot of work in a very short of time and it’s going to be high quality (Ginapp et al., 2023).
Such hyperfocus, often centered around strong interests, can facilitate completing tasks. Yet, such unifocal attention might be difficult to redirect at other activities, compromising eating and sleeping for example. Yet, it also comes with downsides as it complicates directing attention away (Bertilsdotter Rosqvist et al., 2023; Ginapp et al., 2023). This all-consuming attention is not always reported in qualitative studies with adolescents (such as Gerling et al., 2024).
Also, hyperactive and impulsive behavior are not experienced as straightforward deficits, are often not disabling in themselves (see section “ADHD is Mainly Experienced as a Mismatch With the Environment; This Mismatch Has Far-Reaching Consequences”) and are intertwined with intense emotional experiences. For example, an adolescent with ADHD expressed:
I feel everything so strongly, it’s not just anger and sadness but it’s joy and love and all that, too. I think it [ADHD] kind of intensifies everything and that’s a good thing, too (Andersson Frondelius et al., 2019).
Some authors therefore suggest using more neutral terms than hyperactivity or impulsivity, for example an “intensity in relation to oneself or others,” with emotional intensity often also being an important part of their ADHD experience (Andersson Frondelius et al., 2019; Bertilsdotter Rosqvist et al., 2023; Gerling et al., 2024).
ADHD is Mainly Experienced as a Mismatch With the Environment; This Mismatch Has Far-Reaching Consequences
In the medical model approach to ADHD, much attention is paid to functional impairments ADHD people experience, such as sitting still in class all day, having to focus for prolonged periods of time at work or adjusting their speed of talking to social expectations. First-person perspectives corroborate the importance of such impairments, yet people with ADHD tend to report that impairments are often a matter of difficulty in adjusting their behavior to social expectations, rather than experiencing variability in attention or intensity as inherently impairing (Bertilsdotter Rosqvist et al., 2023; Gerling et al., 2024). In the medical approach only minimal attention is given to the impact of difficulty adjusting to these social expectations. An example of an adolescent with ADHD experiencing this difficulty:
I do it all the time [rambling] and I never realize . . . and people . . . you can see people look at you like: stop talking. And then I’m like, oh right, stop (Gerling et al., 2024).
Sometimes, as the medical approach would suggest, this attention variability or intensity is experienced as disabling, and there can be an internal desire for more behavioral control. Peoples’ narratives, however, suggest this experience of ADHD as being disabling in itself is mainly because of internalized expectations of the neurotypical world and because it can make it difficult to reach goals that are important to them or to fit in (Gerling et al., 2024; Schrevel et al., 2016; Van Der Westhuizen & Botha, 2023). For example, an ADHD adolescent expressed the following:
There is nothing powerful enough to tell me to focus and learn . . . so I am just distracted and then. . .that’s just so frustrating, because then, at the end of the day, I will think, ugh, didn’t study again (Gerling et al., 2024).
This pervasive difficulty adjusting to social expectations often sets off a negative interaction cycle with the environment and has far-reaching negative emotional consequences. The medical approach generally does not acknowledge this cycle is set off by a mismatching, unaccommodating and judging environment as much by primarily focusing on individual aspects of disability.
This negative interaction cycle can be as follows. Society, but also people in their direct environment, expect people with ADHD to be able to do presumably simple tasks (e.g., house- or bookkeeping, personal hygiene or homework). Indeed those tasks they can do, but find difficult to start or complete on a regular basis without accommodations or help (Gerling et al., 2024; Schrevel et al., 2016; Smith & McVeigh, 2025; Van Der Westhuizen & Botha, 2023). This creates pressure to adapt and a feeling of failure to the expectations of others, but also internalized expectations that they must be able to do these presumably simple things. People with ADHD express feeling judged by their environment (Gerling et al., 2024; Schrevel et al., 2016), and regularly experience negative reactions of peers, parents, teachers, employers, partners (Smith & McVeigh, 2025; Van Der Westhuizen & Botha, 2023). Often stemming from an individual’s prolonged exposure to this rejection and inability to align with these prevailing environmental or societal expectations (Andersson Frondelius et al., 2019; Fusar-Poli et al., 2024; Gerling et al., 2024; Ginapp et al., 2023), is that minor environmental cues can elicit intense emotional reactions. These negative emotions can manifest as frustration, irritability, depressive or anxious feelings (Gerling et al., 2024) and/or rejection sensitivity dysphoria (Ginapp et al., 2022, 2023; Visser et al., 2024). See below quotes of two adults with ADHD:
Continuously trying so hard, and then you feel disappointed in yourself, because by trying so hard all the time, sooner or later, you get a setback; you can’t do your best all the time. And then people tell you: you are worthless or you are no good (Schrevel et al., 2016). My [childhood] has been quite difficult. You just had a lot of experiences of rejection when you were younger, from friends, teachers, society, on so many levels. I think that, for me, contributed to developing a kind of hypersensitivity to that kind of rejection. To again become that odd boy in the corner of the classroom that nobody really understands (Visser et al., 2024).
Ambivalent Experiences of Being Diagnosed With ADHD
In the overmedicalization critique, the diagnostic label of ADHD is conceived of as a risk as it can induce external and internal stigma and negatively impact identity development (Freedman & Honkasilta, 2017; Honkasilta & Koutsoklenis, 2022; Timimi, 2015). However, the lived experiences of people with ADHD frequently reflect a more nuanced picture and ambivalence toward getting or having an ADHD diagnosis (Long & Coats, 2022; Van Langen et al., 2024; Young et al., 2019), with both positive and negative aspects of being diagnosed with ADHD.
On one hand, a formal diagnosis of ADHD is valued. It fosters recognition and validation of the challenges people encounter in their daily lives and the feelings of non-normality that often accompany them. For example, an adult with ADHD mentions:
But just having that understanding that you do this because you have ADHD, not because you’re a failed human (French & Cassidy, 2026).
Receiving a diagnosis of ADHD can facilitate the process of renegotiating a frequently compromised self-image, thereby contributing to the development of a coherent identity that incorporates ADHD as part of that identity (Andersson Frondelius et al., 2019; Bradley et al., 2025; French & Cassidy, 2026; Fusar-Poli et al., 2024; Visser et al., 2024; Young et al., 2019). A woman with ADHD put this as follows:
As soon as I got the diagnosis, it was just this unbelievable feeling of validation that I’d never had before . . . It was life changing (Bradley et al., 2025).
And in Visser et al.’s (2024) interview study, another woman said:
Since I know I have ADHD, the biggest difference is that I’ve become kinder to myself. And that I think is ultimately the basis on which many practical issues are also going better.
Furthermore, people report that the diagnosis can help with finding support and online social networks of people with shared experiences, fostering relatedness (Eagle & Ringland, 2023; French & Cassidy, 2026; Jones & Hesse, 2018).
There’s such a lovely kinship to be felt with people who also have ADHD, we’re so similar that it’s so nice to be like: this person gets me, and I don’t have to explain it (Smith & McVeigh, 2025).
On the other hand, being diagnosed with ADHD can also create a sense of being a “broken” version of normal, belonging to a group that they themselves looked down on (Andersson Frondelius et al., 2019; Young et al., 2019). This kind of self-stigmatization is expressed by an adolescent with ADHD as follows:
In the beginning it was very hard, in the way that I felt different, I felt very weird almost. It just didn’t feel like me and I felt like a different person. But now I don’t think so. First because it is very common and there are a lot of people who relate (Frick et al., 2025).
But as expected, the ADHD label is also reported to trigger stigmatizing reactions from others, such as this quote from an adolescent with ADHD:
I have friends who previously did not know that I have ADHD, they treated me like a regular person, and when I told them that I had ADHD they immediately started to treat me as if I was a psychopath or something like that (Gerling et al., 2024).
Other expressions of ADHD stigma include lack of understanding, rejection and discrimination but also trivialization (Andersson Frondelius et al., 2019; French & Cassidy, 2026; Gerling et al., 2024; Ginapp et al., 2022; Jones & Hesse, 2018; Visser et al., 2024; Young et al., 2019). A woman with ADHD shared such an experience of trivialization in the following words:
I have often heard “oh yes, you simply want to belong, don’t you” (Visser et al., 2024).
This struggle with this ambivalence is put to words in this quote of a women with ADHD:
For me it also greatly reinforces the feeling of loneliness . . . because you have the feeling that you are different from others, which is actually a very lonely feeling. Finding out there’s a reason for it and . . . there are other people who have this too. But if you are indeed put away by such a comment as being “it doesn’t exist,” then you immediately get that feeling of loneliness again, like you know, you never mind (Visser et al., 2024).
Experiencing Medication
Currently, the most used treatment for ADHD in adolescents and adults is stimulant medication, which has different formulations, but generally does not work for longer than a day. Specific to considering ADHD as neurodivergence is the discussion about medication; between medical and overmedicalization approaches, this is a topic of interest and often heated debate (Saul, 2014; Timimi, 2025; Timimi & Taylor, 2004). In the most extreme applications of this critique medication is purely seen as a negative issue reflecting overuse of medication; an authoritative form of social control of deviant behavior, which unjustly shifts the risk of (long-term) side-effects to people with ADHD (Horwitz, 2010; Rafalovich, 2013). Whilst in the medical approach, medication is generally seen as “curing” ADHD pathology (Faraone et al., 2024). However, in these discussions, peoples lived experiences are often not considered as important source of empirical evidence.
Many people see medication not as an oppressive experience nor as a cure to ADHD, but as necessary in navigating a generally unaccommodating environment and getting them through school or workdays with more focus and ability to manage their behavior to what is expected. Also, it can sometimes be perceived as a “ticket to normality” and to acceptance by the neurotypical majority in our current society (Brinkman et al., 2012; Titheradge et al., 2022). For example, this is put into words by an ADHD young adult:
I need this medication, I want this medication, and I need it to survive in this world, basically, and if I don’t take this medication, this world won’t accept me. (Titheradge et al., 2022).
Additionally, for many, medication is not seen as imposed by others or society but is important to meet intrinsic or extrinsic goals they find important in life, such as social goals, grades or other things (sports, hobbies). For example, an adolescent with ADHD notes:
Medicine helps me to actually pay attention more to other people and listen to what is going on with them because I know I would want somebody to listen to me. My communication skills have gotten sharper (Brinkman et al., 2012).
Similar to the issue of diagnosis, taking medication invokes an ambivalence. Medication is sometimes being perceived as necessary to fit in society, to navigate their daily lives, for acceptance by others and/or to meet important intrinsic goals, but often also having physical and mental adverse effects. These mental adverse effects may be in taking away or suppressing parts of themselves that they value (“not feeling themselves”) or not being valued without taking medication. Further, some people mentioned that medication made them different from others, and taking medication daily was a constant reminder of their differentness (Titheradge et al., 2022). Here some quotes of ADHD adolescents regarding their ambivalent experiences with medication:
In some ways the medicine worked too good but it killed your social life. [. . .] Medicine would make me different. It made me all calm and quiet and stuff and I don’t like that. I like to be wild. [. . .] When your off the medicine, that’s the only time you can really be you (Brinkman et al., 2012).
As medication for ADHD is mostly short acting, every day can be a choice to take medication. At different points in their lives and sometimes even daily people make a tradeoff between benefits of medication in daily life and costs of medication to their bodies, their personality and identity (Bolt & Schermer, 2009; Charach et al., 2014; Titheradge et al., 2022). This is put into words by a young adult with ADHD:
So the medication, it helps, but it’s the side effects of the medication that I didn’t really like. That’s why I was very rebellious against taking medication at some points (Titheradge et al., 2022).
The costs of taking medication can be exacerbated by their environment, seeing medication as “a magic bullet” that is curing ADHD, and valuing them more or only accepting them when they take medication or, the other way around, judging them for taking medication. Especially adolescents may experience external pressure to continue to take medication from clinicians, parents or teachers (Brinkman et al., 2012; Charach et al., 2014; Frick et al., 2025; Gerling et al., 2024; Titheradge et al., 2022), leaving them with very little agency and making them feel that they are only valued when taking medication, feeding into a general negative self-image and questions about their “real” identity. This is put into words by an adolescent with ADHD:
The way I behave and move in everyday life, it changes a lot from when I take the pill and don’t take the tablet, so it makes me think ‘what would it have been like if I didn’t have ADHD?’ (Frick et al., 2025).
Discussion: Applying the Neurodiversity Approach to ADHD
The goal of this paper was to explore the applicability, relevance, specifics and nuances of a neurodiversity approach to ADHD in comparison to currently dominant ones, that is, the medical and the overmedicalization approach, by means of first person’s experiences of ADHD characteristics, the mismatch with the environment, the diagnostic label and medication. In this section we reflect on how these experiences match the core claims of these frameworks.
ADHD as Value-Neutral Neurotype, Mismatching Neuronormative Environments
First-person experiences of ADHD behavior paint a more nuanced and different understanding of ADHD behavior than the universal deficit-focused ADHD symptom descriptions of the medical framework. More specifically, aligning with the neurodiversity approach is the experience of ADHD behavior generally not being experienced as “deficits” in itself, but sometimes being valued in the form of for example, hyperfocus, having an abundance of energy or intensity. ADHD behavior fluctuates and mainly is experienced as disabling in mismatch with the environment. Acknowledged by the overmedicalization critique, is the severe impact of this judging and discriminating environment, which can lead to self-stigma and heightened sensitivity to rejection. However, in the normative turn of the overmedicalization scholarship, this negative environmental impact is assigned to the ADHD label (Kazda et al., 2021), rather than to the mismatch between the ADHD neurotype and neuronormative environments. Further, the emotional intensity is central in many lived experiences; however, some overmedicalization scholars view it as extending the conceptual boundaries of ADHD rather than constituting a core aspect of ADHD (De Vries et al., 2025). In the medical approach this emotional aspect of ADHD is noted as an associated feature of ADHD (American Psychiatric Association, 2022) with an ongoing debate on including this explicitly in the diagnostic criteria (Beheshti et al., 2020; Kooij et al., 2019; Yue et al., 2022). However, this aspect is generally framed in terms of deficit—namely emotional “dysregulation”—rather than emotional intensity, which may also be experienced as meaningful or valuable.
Neuro-Affirming Takes on Diagnosis and Medication
Lived experiences with having or getting an ADHD diagnosis are often ambivalent and may reflect the primarily binary discussion between medical views and overmedicalization criticisms in the media and society. The struggles people are reflecting seem to be internalized beliefs or reactions of their environment of being labeled as someone with a “disorder,” a “deficit” or being someone with a “flaw” in their constitution (the medical approach). On the other hand, the overmedicalization critique also feeds through in internalized beliefs, or reactions of their environment in not believing or trivializing their ADHD diagnosis. These beliefs and reactions make that the diagnosis of ADHD can be difficult for people, it can trigger shame, loneliness, feeling of being “an imposter,” a lower self-concept, and not disclosing their ADHD to their environment or refraining from seeking help (French & Cassidy, 2026; Fusar-Poli et al., 2024; Jones & Hesse, 2018; Visser et al., 2024).
The neurodiversity approach may here give a nuanced view for people, building on elements from both the overmedicalization and medical ones, but adding politicizing and first-person views to the mix (Dwyer, 2022). The neurodiversity approach acknowledges the existence of value-neutral differences between people in how people learn, behave and communicate. Importantly, it considers neurodivergent characteristics as pre-existing to discursive efforts such as diagnostic labeling. This approach helps to validate people’s experiences of difference and (sometimes) suffering. A crucial difference with the medical model approach is that neurodivergent characteristics are not pathologized. Pathologizing such differences may make it difficult for people to accept and embrace such differences as part of their identity, because it implies them being “flawed,” “disordered” or requiring a “cure.” Furthermore, people express that being diagnosed with ADHD helps them to find people alike, fostering an important sense of belonging, relatedness and community with other ADHD people. As opposed to the largely expert-driven social and medical perspectives, the neurodiversity approach explicitly acknowledges the importance and the power of this community for people themselves, to shape research and clinical practice, but also for political and societal change.
People’s experiences with medication also does not entirely support the current dominant approaches. What feeds through in these stories is the balancing act of taking medication (Bolt & Schermer, 2009; Brinkman et al., 2012; Charach et al., 2014; Frick et al., 2025; Titheradge et al., 2022). Sometimes people choose to use medication and suppress their ADHD behavior, which may be due to environmental demands, to feel normal and accepted, but also to reach important goals for them. This often comes with costs, for their bodies, minds or identity as their ADHD behavior is also inevitably part of who they are. The neurodiversity approach may help people in this balancing act. It provides an approach in which ADHD behavior is not seen as something that always needs to be suppressed or cured by medication (as in the medical framework). Nor is ADHD behavior seen as solely to be contextually remediated and primarily a societal problem (as in the overmedicalization critique). The overmedicalization critique, solely focusing on environmental changes, can leave people insufficiently supported in our current generally unaccommodating society. This approach may unduly stigmatize taking medication. In contrast, from a neurodiversity approach perspective, both individual and environmental aspects of addressing disability are considered. People may choose to take medication, temporarily reduce ADHD characteristics, depending on their goals and important outcomes for them, whilst still acknowledging and highlighting the importance of environmental acceptance, adaptations and support. In this view, even though they choose to do reduce their ADHD behavior in some instances for different reasons, in its core ADHD is considered part of their identity.
In sum, lived experiences give indications that the neurodiversity approach to ADHD can be a valid, promising and less stigmatizing alternative to the current approaches to ADHD. Considering ADHD as a difference, and not a universal deficit, nor always a strength or purely social problem, with disability mainly occurring in mismatch with the environment, seems to reflect peoples lived experiences of ADHD. Not only does it validate their experience of already feeling different in our society, but it also empowers them and facilitates bonding with neurodivergent people alike. Moreover, considering ADHD a value-neutral difference rather than a disorder makes it easier to reconcile a part of oneself and one’s identity, and may also ease the balancing act of taking medication.
Cure and Identity: ADHD-Specificities of the Neurodiversity Approach
Although views are beginning to shift, the neurodiversity approach is, to date, mainly based on autistic experiences (Bertilsdotter Rosqvist et al., 2020; Jackson-Perry et al., 2025; Livingstone et al., 2023). By considering ADHD lived experience in more detail, we noticed at least two aspects contrasting current, autistic-centered neurodiversity theorizing: (1) openness to treatment of core ADHD characteristics and (2) moderate uptake of positive ADHD identity and language.
First, we noticed ADHD people were fairly open to consider taking medication to alter or diminish ADHD characteristics. We discussed instances where neuronormative environments executed pressure to do so. However, there also seemed more internal motivation to take medication, be it in certain instances and under certain conditions. At first sight, this might seem irrevocably at odds with the neurodiversity movement’s anti-cure tenet, as developed by autistic people. Relying on a social model of disability, autistic advocates have argued to change the environment (exclusively), not the person. We believe though that this tension here can be overcome. Elsewhere, we already laid out this argument more extensively, be it in relation to Tourettic people’s openness to medication to avoid their most painful tics, or to reduce hindering tics during activities of their choice (Vanaken et al., 2025). A different model of disability proves useful here, that is, Elizabeth Barnes “value-neutral model.” In her book The Minority Body (Barnes, 2016) she argues that, globally, disability is neutral with respect to wellbeing and that this relationship depends on the conditions disability is combined with. Interestingly, her theory of disability creates space for so called “local bads.” Those are disability-related aspects that do cause harm to someone’s wellbeing, be it in specific (local) domains of life. Some ADHD characteristics in some contexts can be theorized as such local bads for which “cure” is welcome. Acknowledging such local bads stays clear however from conceiving of ADHD as a pathological condition altogether and from striving for normalization of all ADHD behavior through medication or therapy. The conclusion of this finding inspired by ADHD experiences is, in our view, that neurodiversity approaches ideally delicately move or stay away from overly strong “anti-cure” positions. Openness to medication, especially when well-informed and self-determined, should not be incompatible with claims for depathologisation of neurodivergence and seeking social change (Vanaken et al., 2025).
As a second novelty, we found an ambivalent appreciation of being diagnosed ADHD which is seemingly at odds with the neuro-affirmative view that a diagnosis is liberating. Of course, such ambivalence also exists among autistic people, but the dynamics driving this ambivalence seem slightly different for ADHD. Some testimonies shared above pointed to feeling “broken” following diagnosis. This can be a consequence of medical model-style of information one received during assessment or through mainstream narratives on ADHD. Yet, other interviewees also pointed to feelings of loneliness after being diagnosed, especially when people challenged the idea that ADHD is a valid diagnosis at all (Clarke, 2011; O’Sullivan (2025); Saul, 2014; Van Os, 2026). Such public debates on the sheer validity of the diagnostic label are, to our knowledge, less prominent regarding autism. When diagnosed ADHD, people thus have to navigate a society where some claim they have a serious neurodevelopmental disorder, while others—provocatively phrased—claim ADHD is but a mere invention favoring the pharmaceutical industry. In this societal context, integrating ADHD in one’s identity as a value-neutral neurotype, is even less evident compared to autism (Silberman, 2015).
This train-of-thought might partly explain why identity-first language is (still) less common among people with ADHD compared to autism (Bottini et al., 2024; Cooper et al., 2026; Pearson et al., 2026). Also, a recent study found indications of different preferences among neurotypes concerning neurodiversity-related terms (e.g., neurodivergent) to describe themselves; ADHD people hardly used those terms whilst autistic and AuDHD people did (Bury et al., 2026). In contrast though, another recent study showed two-thirds of both ADHD and autistic groups did use such words describing themselves (Grant et al., 2025), as those words felt less stigmatizing than specific diagnostic labels. More research is definitely needed on positive identity formation among ADHD people and on community preferences with regards to neurodiversity-related terminology and language (Bury et al., 2026; French et al., 2025; Grant et al., 2025).
Further Steps for Clinical and Research Practice
This paper can give more guidance on the specific interpretation of ADHD as neurodivergence, and can drive clinical, research and policy changes. Slowly, some aspects of the neurodiversity approach are trickling down toward clinical care, mental health policy and research. Driven by the neurodiversity movement, people with ADHD are claiming roles allowing more meaningful involvement in research and development efforts and participatory methodologies are gaining popularity, which we encourage (Flobak et al., 2021; Gerling et al., 2024; Sonuga-Barke et al., 2024). Moreover, research led by ADHD scholars themselves deserves more attention. On top of instances discussed before (e.g., Jackson-Perry et al., 2025), one can look for example at ADHD-led explorations of perceptions of time and reading (Basten, 2023; Tolani & Venkatesan, 2025). Also, additional work on differences among autistic and ADHD people in terms of medication use and identity work might benefit from looking into and extending existing work on AuDHD experiences (Craddock, 2024, 2026).
Next to research guidance, the current paper may also inspire clinical ADHD care. It gives clinicians and ADHD people more background on the specific application of the neurodiversity framework to ADHD and can facilitate dialogue between care users and clinicians. Furthermore, it gives indications of important nuances of the neurodiversity framework to ADHD. Future work could further explore when and how medication can play a role within the framework of neuro-affirming care. It might be interesting to further explore whether the up- and downsides of masking as described in the autism literature, mirrors ADHD experiences with medication. One could also look further into the clinical value of supporting a positive ADHD identity in relation to being diagnosed or taking medication. Looking at the experiences descried above and looking at the autism field, identity-affirming care and support seem an important topic for people, but is to date not discussed in current guidelines and generally not considered in clinical care for ADHD (Van Der Oord et al., in preparation; Visser et al., 2025).
In conclusion, over the past years ADHD people have been adopting a neurodiversity approach to discuss their experiences with one another (Eagle & Ringland, 2023; Grant et al., 2025). Yet, scholarly work on the topic is scarce, especially more empirically driven research on applications of the neurodiversity paradigm in the ADHD field are still in their infancy. With the current article, we hope to have contributed to this body of work. However, we do acknowledge that our argumentation is shaped by our positionality and by the included set of qualitative research papers. Although we did include systematic reviews of such papers (Fusar-Poli et al., 2024; Ginapp et al., 2022), our non-systematic search strategy might have limited the findings. In any case, we do encourage future work on the topic, informed and co-produced by ADHD people, to fully shape, adopt and integrate the neurodiversity approach in ADHD research and clinical care with all its nuances and specifics for ADHD people.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.