
Abstract
Objective:
Research suggests there is a higher prevalence of anxiety in individuals with ADHD compared to those without ADHD. However, estimated prevalence rates vary greatly due to differences in methodologies used across studies. This study is the first meta-analysis investigating differences in anxiety measure scores between adults with and without ADHD, and possible moderators of this effect.
Method:
Our analysis included 58 studies that compared anxiety scores in adults with/without ADHD (N = 18,821; k = 112).
Results:
The average effect size (Hedges’s g) of anxiety scores in those with ADHD relative to controls was 0.77 (SE = 0.066); a medium effect. The only significant moderator was the type of comparison group used, with comparisons to non-clinical control groups (g = 0.954, SE = 0.08) yielding significantly larger effects than comparisons to clinical control groups (g = 0.437, SE = 0.09). None of the other moderator variables examined (Method of characterising ADHD, Anxiety Measure Type, Anxiety Measure Focus, Age or Gender) moderated the effect. There was some evidence of publication bias, therefore results should be interpreted with this in mind.
Conclusion:
Overall, this study indicates that ADHD is associated with higher levels of anxiety symptomology. This has important implications in the diagnosis and treatment of individuals presenting with ADHD or anxiety, including the consideration and screening of each of these conditions as potentially co-occurring with the other. Adaptions made to clinical practice in line with this would better support this population, improve symptom management and overall quality of life. Suggestions for future research are discussed.
Keywords
Introduction
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition that impacts individuals’ daily functioning with symptoms of inattentiveness and/or hyperactivity and impulsivity (American Psychological Association [APA], 2013). Individuals with ADHD can experience forgetfulness, difficulties with planning and organisation, restlessness and mood instability (Ambrosini et al., 2013). ADHD can affect an individual’s relationships, education and work (Michielsen et al., 2018) as well as general adaptive functioning and quality of life (Meaux et al., 2009).
ADHD has historically been viewed as a childhood disorder that improves with age; however, recent research has shown that ADHD continues into adulthood (Johnson et al., 2021; Michielsen et al., 2018), impacting around 2% to 5% of adults worldwide (Ayano et al., 2023). Despite its prevalence adult ADHD is poorly understood. However, meta-analyses have shown that the prevalence rate of ADHD is higher within adult populations that have concurrent mental health diagnoses, although there is substantial variation in this prevalence estimate varying from 6.9% to 38.75% depending on the ADHD assessment used and sampling method (Gerhand & Saville, 2022). Notably, Adamis et al. (2022) is the only meta-analysis to report a pooled prevalence rate, estimating that 26.7% of psychiatric outpatients have ADHD. This highlights the high co-occurrence of mental health difficulties in ADHD, yet there remains a lack of evidence on whether the severity of mental health symptoms differ in this population compared to those without ADHD, and whether this is true of specific mental health diagnoses, for example, anxiety.
ADHD and Co-occurring Conditions
ADHD has been found to co-occur with several mental health conditions, neurodevelopmental conditions, and substance misuse, within both cross-sectional (e.g. Halmøy et al., 2009) and longitudinal studies (e.g. Biederman et al., 2006). Indeed, 75% of adults with ADHD are thought to have at least one other psychiatric diagnosis (Kooij et al., 2010).
Systematic reviews have found the most common co-occurring conditions in adults with ADHD are substance use disorder (2.3%–82.9%), mood disorders (4.45%–80.8%), anxiety disorders (3.9%–84%) and personality disorders (0.31%–65.95%) (Choi et al., 2022; Katzman et al., 2017). Choi et al. (2022) concluded that prevalence rates of these conditions are higher in samples with ADHD compared to samples without ADHD, irrespective of the presence of any other prior mental health diagnoses. However, this research (Choi et al., 2022) did not include any statistical analysis to quantify group differences or explore possible moderators. The wide range of prevalence estimates of co-occurring mental health conditions in ADHD is likely due to methodological differences across studies, such as whether the sample was from the general public or a clinical population, and how ADHD and comorbid mental health conditions were each diagnosed (Choi et al., 2022; Katzman et al., 2017). Prevalence estimates are less varied when study methods are controlled (Polanczyk, et al., 2014).
The rate and severity of current and lifetime mental health conditions can vary based on whether someone was diagnosed with ADHD in childhood or adulthood (Able et al., 2007; Halmøy et al., 2009; Quintero et al., 2019). ADHD has been seen to affect the clinical course of mental health conditions (Biederman et al., 2006), including increased rates of episodes (Rydén et al., 2009) and functional impairment (Asherson et al., 2012). Co-occurring conditions have also been seen to increase with age, particularly with life transitions such as when individuals leave their family home (Barkley et al., 2002). Moreover, ADHD populations have been found to have lower quality of life, often in relation to severity of ADHD symptomology, social functioning and emotional control (Agarwal et al., 2012). Increased ADHD symptomology also increases the likelihood of self-harm and suicidal behaviours (Austgulen et al., 2023), potentially in relation to impulsivity being a core symptom in ADHD (APA, 2013). The presence of co-occurring mental health disorders such as affective disorders, anxiety disorders and substance misuse, have been found to mediate the relationship between ADHD and suicidality (Balazs & Kereszteny, 2017) likely in relation to difficulty coping with the impact of these on quality of life (Furczyk & Thome, 2014). Given the significant role of anxiety disorders in mediating the relationship between ADHD and quality of life, as well as their high co-occurrence, further exploration of this comorbidity is essential to understanding its impact.
ADHD and Anxiety
ADHD and anxiety disorders frequently co-occur (Biederman et al., 2006; Katzman et al., 2017; Kessler et al., 2006; Lynch & Davison, 2022; O’Rourke et al., 2020), particularly social anxiety, specific phobias and post-traumatic stress disorder (Kessler et al., 2006), with individuals meeting diagnostic criteria for both conditions, even when potential overlapping symptoms like physical restlessness are excluded (Milberger et al., 1995). The prevalence of co-occurring anxiety disorders has been found to range from 4.3% to 47.1% in individuals with ADHD sampled from the general population and 3.9% to 84% when the ADHD sample is taken from a psychiatric population (Choi et al., 2022). Hartman et al. (2023) found similar variability in prevalence rates (2.2%–44.3%) in their systematic review comparing anxiety in ADHD adults and controls which resulted in a pooled odds ratio of 5.0, yet it is unclear the extent to which the symptomology and severity of anxiety is the same or different between these groups.
Research examining the impact of this co-occurrence has found that anxiety can change the presentation, course and prognosis of ADHD across the lifespan (D’Agati et al., 2019; Schatz & Rostain, 2006). Anxiety has been found to worsen cognitive deficits seen in ADHD, particularly working memory (Roth et al., 2004). Furthermore, anxiety sometimes interferes with impulsivity and inhibitory control deficits in ADHD (Schatz & Rostain, 2006). There are mixed findings as to whether this improves performance or not (Brown, 2000; Oosterlaan & Sergeant, 1998), but anxiety has been found to negatively impact the self-esteem of individuals with ADHD (Brown, 2000). Research has also indicated challenges in treatment for individuals with co-occurring ADHD and anxiety (D’Agati et al., 2019; Koyuncu et al., 2022). For example, responses to methylphenidate treatment for ADHD are varied in individuals with co-occurring anxiety (Koyuncu et al., 2022) and these individuals may benefit less from cognitive behavioural treatment alone, needing supplementary medication (D’Agati et al., 2019). It is therefore important for assessments to carefully consider the developmental course of the conditions to reduce the likelihood of misdiagnosis and ensure effective treatment (D’Agati et al., 2019).
Several theories aim to explain the increased prevalence of anxiety disorders in ADHD (D’Agati et al., 2019; Jarrett & Ollendick, 2008; Schatz & Rostain, 2006). Research has highlighted a potential genetic underpinning to comorbidities, utilising latent class analysis to analyse patterns to indicate subgroups (Neuman et al., 2001) or highlighting a potential underlying risk factor due to high rates of familial association (Braaten et al., 2003). However, this means it can be hard to differentiate nature and nurture in the interplay of ADHD and anxiety. The Cognitive Processing Model (Schachar et al., 1995) proposes that symptoms of ADHD lead to difficulties conforming with norms and meeting demands thus resulting in anxiety. The Executive Inhibition (Barkley, 1997) and Motivational models (Quay, 1998) similarly consider the impact of socially inappropriate behaviour, but add the potential of executive functioning difficulties resulting in undefined anxiety.
Other models have considered the impact of poor regulation (Brown, 2000) and coordination (Posner & Peterson, 1990) in attentional systems in ADHD leading to increased focus on threatening stimuli and decreased regulation of emotion, that is, anxiety. Levy (2004) created a hybrid theory to address the contradiction that individuals with ADHD can be both impulsive and daring, yet experience high anxiety (Schatz & Rostain, 2006). This integrates prior theories and considers both cortical and subcortical malfunction in ADHD leading to difficulties in regulating attention and focus on anxiety provoking stimuli and poor regulation of anxiety states (Levy, 2004). These theories offer insights into the link between ADHD and anxiety, suggesting how genetic, neurobiological and environmental factors may each contribute to anxiety in individuals with ADHD.
Rationale for the Present Study
As discussed, there is high variability in the estimated prevalence of co-occurring ADHD and anxiety which could be due to sampling and diagnostic differences across previous studies (Davies et al., 2022). Behavioural studies converge on the idea that individuals with ADHD experience a greater level of anxiety than controls (Agarwal et al., 2012; Nelson & Liebel, 2018). However, overlapping symptoms and subjective experiences of these conditions can make their differentiation difficult in self-identification (Koyuncu et al., 2022). Previous research has shown a discrepancy between ADHD participants who self-reported anxiety compared to those who met the clinical criteria for a lifetime anxiety disorder (Halmøy et al., 2009). Therefore, to further understand the relationship between ADHD and anxiety this study only includes scores on questionnaire measures of anxiety, and not self-reported anxiety, as these are generally deemed more objective than relying on participant report of a diagnosis (Hamilton et al., 2017).
Meta-analytic data is needed to quantify the levels of anxiety in individuals with ADHD compared to non-ADHD control groups beyond binary classifications of anxiety being present or not. This will enable the estimation of differences in anxiety symptomology between adults with and without an ADHD diagnosis and aid better understanding of how these conditions co-occur (Gorlin et al., 2016).
Much of the previous research on ADHD has focused on children (Ginapp et al., 2022), but there is a growing interest and focus on ADHD in adulthood (Ramos-Quiroga et al., 2013). This study focuses on the relationship between ADHD and anxiety in adulthood for three main reasons. Firstly, the presence of co-occurring conditions has been seen to affect the diagnosis and treatment of ADHD in adulthood due to a lack of appropriate resources (Ramos-Quiroga et al., 2013). Secondly, co-occurring anxiety has been seen to increase with age alongside changes in overt symptom presentation (Koyuncu et al., 2022). Finally, research with children can often rely on parental ratings of child anxiety which can be inaccurate (Schatz & Rostain, 2006).
Improving understanding of the relationship between ADHD and anxiety could support healthcare professionals in their understanding of ADHD presentations (Ginapp et al., 2022). Understanding disorder-related outcomes would have implications for recognition, assessment and treatment (Jarrett & Ollendick, 2008), which can be important in suicide prevention (Balazs & Kereszteny, 2017) and improving quality of life for adults with ADHD. This in turn may reduce the impact of these conditions (Davies et al., 2022), and potentially change psychiatric trajectories (Katzman et al., 2017).
Moderators
As methodological differences are common in studies on this topic, several moderators were considered. Firstly, prevalence rates of both ADHD and co-occurring anxiety seem to be affected by variability in diagnostic tools and methodologies (Choi et al., 2022) and inconsistencies in how ADHD is defined (Koyuncu et al., 2022). Therefore, we examined the impact of how ADHD was diagnosed and differentiated from non-ADHD groups as a moderator, for example, self-report compared to clinical diagnosis.
We also considered the nature of the control group, that is, whether controls were recruited from the general or clinical population.
Furthermore, due to heterogeneity in how anxiety is measured within studies, it was important to examine whether this moderated effects, including comparisons between the type of anxiety measured (e.g. general and specific anxieties), and whether measured focused on state or trait anxiety. Variability in anxiety measurement can influence research findings, potentially affecting the strength or direction of relationships between anxiety and other variables (Davies et al., 2022).
There is ongoing debate regarding whether there is a gender difference in the prevalence of ADHD with ADHD traditionally being associated with boys (Adamis et al., 2022). However, there is some evidence that females are more impaired on ADHD scales (Robison et al., 2008) and have more co-occurring psychiatric diagnoses (Ginapp et al., 2022). Indeed, prevalence rates of ADHD are likely similar among genders and females are potentially underdiagnosed, particularly in childhood, due to differences in symptom presentation, particularly a higher level of emotional symptoms (Adamis et al., 2022; Robison et al., 2008). Research has also consistently found higher prevalence rates of anxiety in females than males (Bandelow & Michaelis, 2015). Therefore, gender was considered as a moderator in this analysis.
Age related changes in the association between ADHD symptomology and anxiety have been reported (D’Agati et al., 2019), thus age was also considered as a moderator. Finally, the publication status of the research was included as a moderator to examine the risk of publication bias.
Research Questions
This study addresses two main research questions. Firstly, is there a difference in anxiety measure scores between adults with and without ADHD? Secondly, is this difference moderated by participant or methodological variables? Within this, we specifically considered the effects of (a) method of categorising ADHD; (b) control group type; (c) anxiety measure type; (d) anxiety measure focus; (e) gender; (f) age; and (g) publication status.
Method
Database Search and Inclusion Criteria
The systematic review and meta-analysis were conducted in line with Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). Searches were conducted in PsychINFO, MEDLINE, ERIC, Scopus and ProQuest databases for publications and dissertations. Searches included terms related to ADHD (“Attention Deficit Disorder”, “Attention Deficit Hyperactivity Disorder”, “ADHD”, “Hyperkinetic Syndrome”, “Minimal Brain Dysfunction) and for Anxiety (“Anxiety”, “Phobia”, “Sociophobia”, “Panic”, “Agoraphobia”, “Claustrophobia”, “GAD”, “Hypochondria”) within the title or abstract (see Appendix A for the full search strings used). The operationalisation of anxiety, and subsequent search terms were decided based on the categories of anxiety disorder featured within the DSM V (APA, 2013). A request for unpublished data was also distributed by the research team to their personal networks, as well as to COGDEVSOC and EUNETHYDIS listservs for distribution to their mailing lists (see Appendix B for the call for data).
The study inclusion criteria were that the study needed to be (a) written in English or have a suitable translation available, (b) contain new data, and (c) be completed/published from 1994 to June 2024. The start date was selected based on the publication of the fourth volume of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; APA, 1994), which demonstrated a shift in the definition and understanding of ADHD and the inclusion of the three subtypes seen today (Epstein & Loren, 2013). The end date was the date the literature search was completed.
Furthermore, studies needed to (d) include participants aged 18 and over and (e) utilise a between-group design with one group categorised as having ADHD through either clinical diagnosis, self-report of prior diagnosis, or questionnaire with cut-off, and another control group without ADHD. Finally, (f) the study needed to include at least one measure of anxiety.
Data Screening and Extraction
Results from the database searches were uploaded to Rayyan software, and duplicates were removed. A two-stage screening process was undertaken as shown in Figure 1. In stage one, joint title and abstract screening was undertaken by the first author (89% articles) and two second coders (11% articles each). Half of all papers screened were double screened, that is, reviewed for a second time by one of the other coders resulting in a 97% inter-rater agreement. Any papers with disagreements in ratings were discussed with reference to the inclusion criteria and resolved.
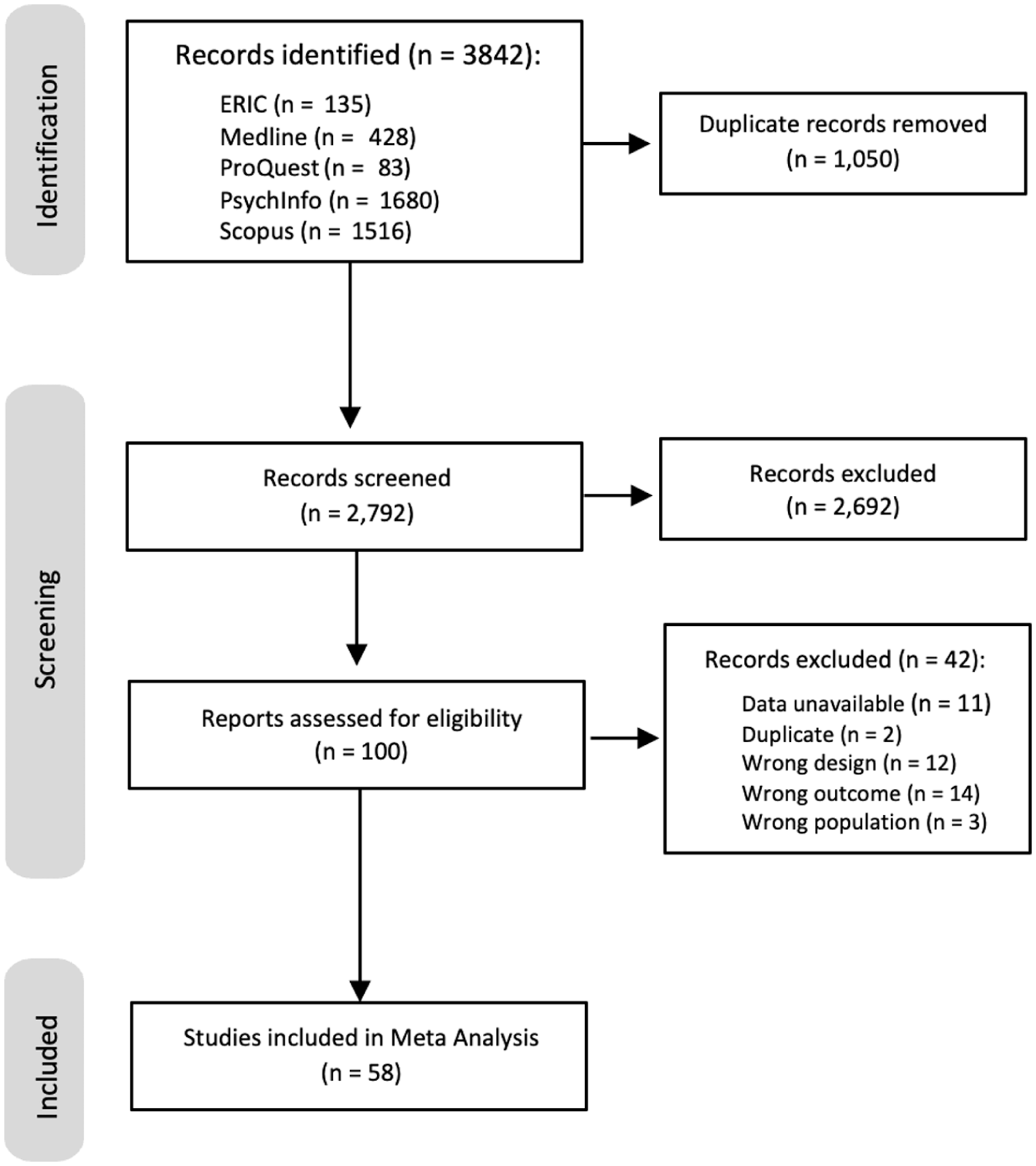
PRISMA diagram outlining search strategy and reasons for excluded studies.
100 articles progressed to stage two for full text screening. This was completed by the first author, with 15% of these screened a second time by a second coder (research student), giving 86.7% inter-rater agreement.
The first author independently collected and collated data from the included studies, including the mean and standard deviation on the anxiety measure for the ADHD group and any non-ADHD groups. Authors were contacted if the paper did not provide sufficient data to calculate effect sizes. Of these, 11 did not respond so were excluded from the meta-analysis, resulting in 58 studies included.
Each measure of ADHD was reviewed ensuring that the directionality of each measure was the same with a higher score meaning higher anxiety.
Moderator Variables
The operational definitions for moderator variables are presented below.
Method of Categorising ADHD
ADHD categorisation was coded categorically as a binary variable. Studies were categorised as “clinical” if ADHD group was determined using a researcher interview, with or without a questionnaire (Royal College of Psychiatrists, 2017), or participants had a confirmed diagnosis from a clinic. Alternately, the “self-report” category was used for studies who grouped participants based on participant-report of ADHD or questionnaire only.
Control Group Type
For this meta-analysis we compared ADHD groups with a control group who did not have ADHD. Differences in the type of control group were examined as a moderator.
The type of control group was a binary variable, coded categorically for each study. The label “non-clinical control” was used if the group was from the public, “clinical control” was used for participants recruited from psychiatric or hospital settings or where participants were determined to have a specific clinical diagnosis (e.g. bipolar disorder/ social anxiety disorder).
Anxiety Measure Type
For each study, two specific characteristics of the anxiety measure were considered. Firstly, the type of anxiety measured was coded categorically as either “general” if the measure assessed broad anxiety symptoms (e.g. Beck Anxiety inventory; Beck et al., 1988), or “specific” if the measure focused on a particular type of anxiety only, for example, Liebowitz Social Anxiety Scale; LSAS (Liebowitz, 1987).
Anxiety Measure Focus
Secondly, the form of anxiety was considered. The anxiety measure used was coded categorically as either “state” for anxiety measures that focused on how a person was feeling at that specific moment, or “trait” for measures assessing more stable individual tendencies (Leal et al., 2017). Within this research, we also included the category of “prolonged-state” (Hood et al., 2015) where the measure considers symptoms of anxiety over an extended period, that is, 2 weeks to 1 month.
Gender
The gender ratio of participants in the ADHD group was coded continuously as the percentage of females in the ADHD group compared to the total number of participants in the group.
Age
The age of ADHD group participants was coded continuously based on mean age in years. As this research was interested in whether the age of the ADHD participants impacted on relations with anxiety symptoms, due to evidence indicating changes in symptomology with age (D’Agati et al., 2019), the age of the control group was not used as a moderator.
Type of Publication
For each study, the publication status was coded categorically as “peer reviewed publication” if the data was obtained from an article within a journal or “dissertation” if the data was from unpublished university theses and dissertations.
Analytical Approach
All analysis was completed in RStudio (Version 2024.12.1+563; see Appendix B for output). The Rcode for this analysis will be openly available on our OSF page upon publication (https://osf.io/rh6du/). The mean and standard deviation of the anxiety measure for each ADHD and non-ADHD group were used to calculate the Cohen’s d effect sizes (Borenstein et al., 2009). The Cohen’s d effect sizes were then converted to Hedges’ g values by multiplying them by a correction factor based on the pooled sample size (Turner & Bernard, 2006). The standardised mean difference statistic of Hedges’ g was used to estimate the mean difference between ADHD group and non-ADHD group scores as this corrects for small sample bias (Hedges, 1981). Hedges’ g values are generally interpreted the same as the guidelines for Cohen’s d (Brydges, 2019). They are interpreted as 0.2 being a small effect, 0.5 a medium, and 0.8 a large effect (Cohen, 1988, 1992).
Meta-analyses and metaregressions were completed using the robumeta package (Fisher & Tipton, 2015) in RStudio adapted from code used in Hawes et al. (2022). Specifically, robust variance estimation (RVE) was used due to some studies contributing multiple effect sizes to the meta-analysis as they included more than one anxiety measure comparison between the ADHD and control groups. RVE is particularly useful for handling cases where multiple effect sizes are extracted from a single study, as it accounts for within-study correlations and prevents overweighting of studies contributing multiple outcomes (Fisher & Tipton, 2015; Tipton, 2015; Tipton & Pustejovsky, 2015). Instead of aggregating effect sizes or selecting only one per study, RVE allows for all reported effects to be included while adjusting for their interdependence through correlated effects modelling (Fisher & Tipton, 2015; Tipton, 2015; Tipton & Pustejovsky, 2015). The Spearman’s Rho correlation coefficient (ρ) represents the assumed dependence between effect sizes within a study. Based on prior recommendations (Tipton, 2015), we initially set this value at 0.8 but conducted sensitivity analyses to examine the robustness of our results under different correlation assumptions. Specifically, we varied ρ from 0.1 to 1.0 (Tanner-Smith & Tipton, 2014), assessing whether changes in the assumed within-study dependence led to substantial shifts in the estimated effect sizes. This approach ensures that the summary effects are not unduly influenced by the choice of correlation coefficient and helps verify the stability of our findings.
Between-study heterogeneity was assessed using T2 to estimate the degree of variability in effect sizes across studies that cannot be attributed to random sampling error. T2 indicates the variance of the true effect sizes, a higher T2 value indicates greater heterogeneity, suggesting that true effect sizes vary meaningfully across studies rather than simply due to chance (Deeks et al., 2008; Engels et al., 2000). The square root of this number, Tau (T), estimates the standard deviation of the true effects (Deeks et al., 2008).
To further assess variability, we calculated I2, which quantifies the proportion of total observed variation that stems from actual differences between studies rather than random error (von Hippel, 2015). I2 is independent of the number of studies in the meta-analysis a stable (Higgins & Thompson, 2002). Interpretation guidelines suggest that values below 25% indicate low heterogeneity, while values of 50% and 75% suggest moderate and high heterogeneity, respectively (Higgins et al., 2003). Lower I2 values are preferable, as they indicate that the observed variation is primarily due to chance rather than systematic study differences.
Forest plots were generated for the main effect of ADHD on anxiety symptomology. These show mean effect sizes for each study. The effects in these are underweighted and differ to the main analyses effects as dependencies are not considered as they only include the mean effect size per study and not individual effect sizes.
Moderator Analysis
Separate regressions were used to investigate the effect of moderators. This was done as there was not a complete data set for all moderators. Therefore, if all moderators were entered into one model, the model would exclude an effect size for which any one moderator was missing, therefore many effect sizes would be excluded and the power of the analysis substantially reduced. Individual regressions for each moderator allowed for the case-by-case exclusions of effect sizes based on missing data for the moderator in question only. For categorical variables, an omnibus Wald (HTZ) test was used to test the difference between categories of the moderator (Wald, 1943).
Publication Bias
Several steps were taken to ensure against potential publication bias in line with those utilised by prior meta-analyses (Gunnerud et al., 2020; Hawes et al., 2022). The outcome of these is presented in the results section.
First, published and unpublished studies were compared with moderator analysis. Secondly, funnel plot asymmetry was assessed, following the recommendations of Rodgers and Pustejovsky (2021). Funnel plots visually represent effect sizes (x-axis) in relation to their standard errors (y-axis). Studies with larger standard errors appear toward the bottom of the plot, and the average effect size is shown by a central vertical line. An asymmetrical funnel plot, with a greater number of studies appearing on the right side of the vertical line, may indicate bias (Sterne et al., 2011).
This study utilised two approaches: effect-size-level funnel plots to identify selective outcome reporting (disaggregated effect sizes) and study-level funnel plots to detect selective publication (aggregated effect sizes). An asymmetrical plot with disaggregated effect sizes would indicate selective reporting bias, whereas asymmetrical funnel plots with aggregated effect sizes can suggest publication bias (Sterne et al., 2011). Asymmetry was tested for statistically using Robust Egger’s Regression (Egger et al., 1997), specifically utilising the Precision Effect Estimate with Standard Error (PEESE) and the Precision-Effect Test (PET) to analyse disaggregated dependent effects (Rodgers & Pustejovsky, 2021).
The third step taken for publication bias was to use the two-step trim-and-fill method aimed at identifying sources of potential bias and adjusting results for it to indicate the impact of these on effect sizes (Duval & Tweedie, 2000; Mavridis & Salanti, 2014).
Results
Study Characteristics
The meta-analysis on the impact of ADHD on anxiety symptoms included 112 anxiety measurements (effect sizes) from 58 studies from 19 countries. Characteristics of each of the studies are presented in Table 1. In total, 18,821 participants (ADHD N = 5,595; Control N = 13,226) were included in the meta-analysis. The average age for ADHD participants across all studies was 29.11 years (SD = 6.49), and 29.82 years (SD = 7.13) for controls. There was a slightly higher average percentage of females across the control groups (57%) than ADHD groups (46.19%). Across studies, the mean number of anxiety measures reported (effect sizes) per study was 1.93 (min = 1, max = 6).
Characteristics of Studies Included in the Meta-Analysis.
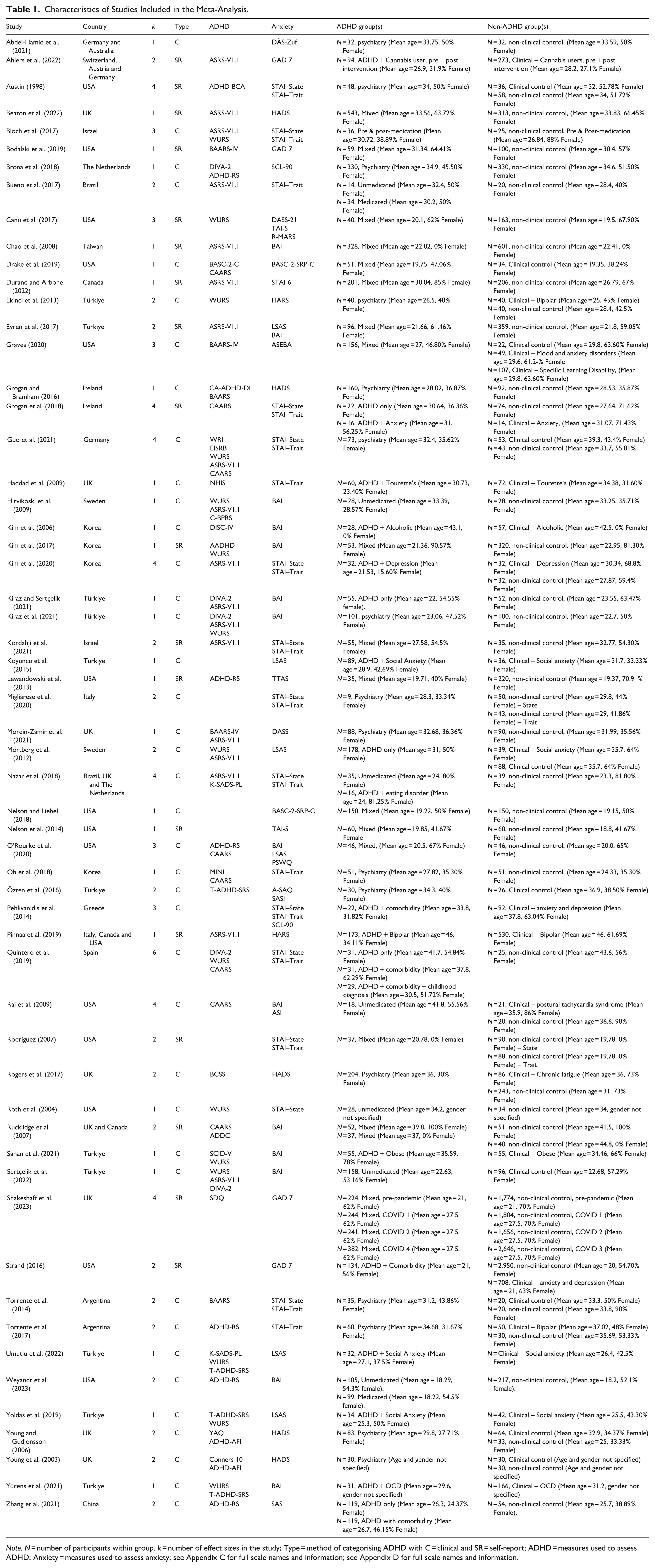
Note. N = number of participants within group. k = number of effect sizes in the study; Type = method of categorising ADHD with C = clinical and SR = self-report; ADHD = measures used to assess ADHD; Anxiety = measures used to assess anxiety; see Appendix C for full scale names and information; see Appendix D for full scale names and information.
Overall Effect of ADHD on Anxiety
The overall effect of ADHD on anxiety was g = 0.77, SE = 0.066, 95% CI [0.638, 0.901], p < .001. This indicates a medium effect of ADHD on severity of anxiety symptomology (Cohen, 1988, 1992). Between-study variability, T2, was estimated to be 0.22, indicating a low to moderate level of variability. Approximately 90.35% of the variance (I2 = 90.47) related to true variance rather than random error, this indicates substantial heterogeneity (Higgins et al., 2003). Varying the assumed correlation between the within-study effect sizes from 0.1 to 1, had no impact on the overall effect, standard error, and estimates of heterogeneity.
A visual summary of the average effect size (Hedges g) and confidence intervals for each study can be seen in the forest plot (Figure 2). As noted below, this is based on the average effect from each study, yet shows some studies have very wide confidence intervals, potentially suggesting high variability.
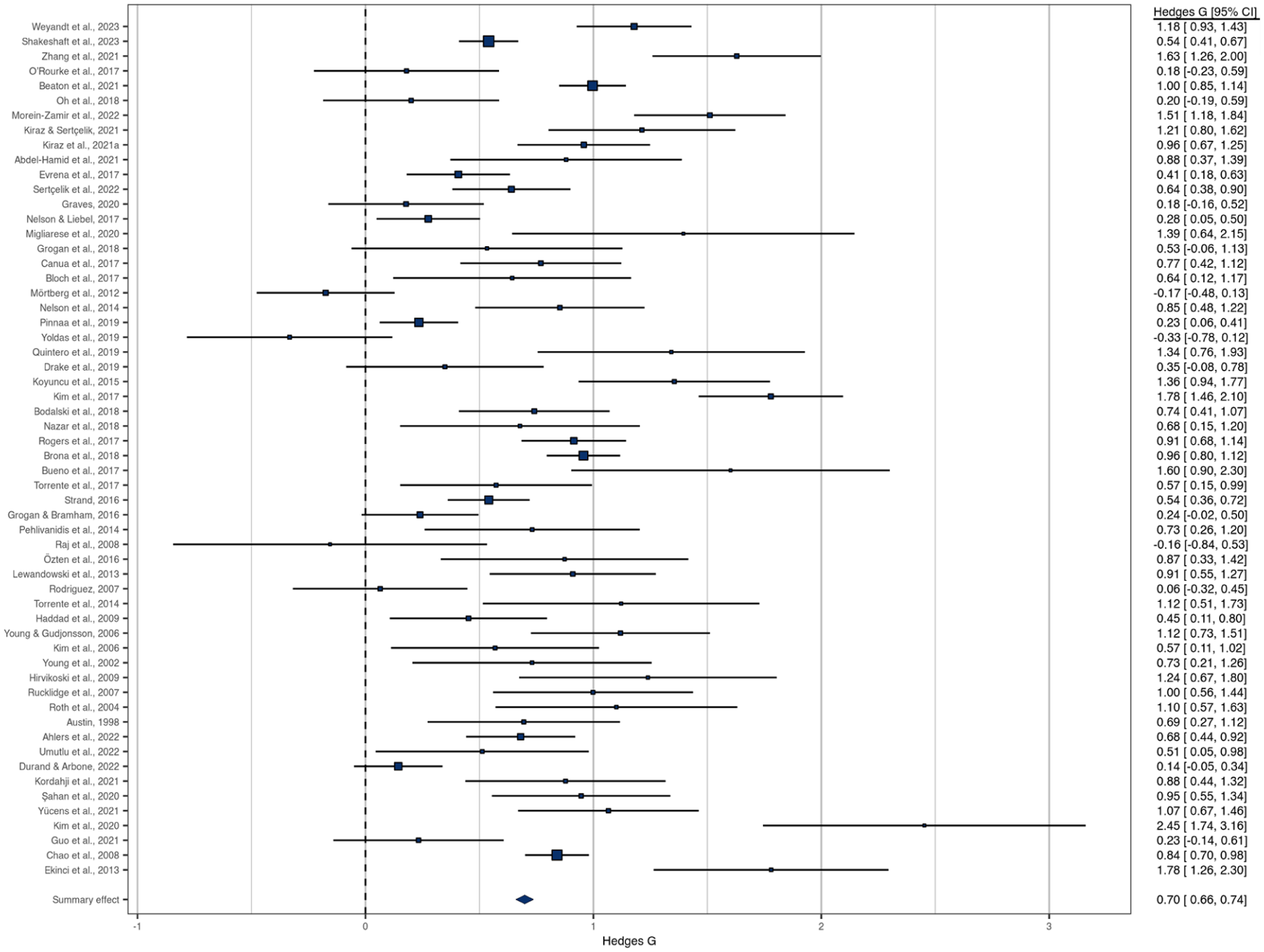
Forest plot of effect sizes of differences in anxiety scores between those with and without ADHD scores.
Moderator Effects
The results of the moderator analyses are reported in Table 2. Of the five categorical variables examined, only Control Group Type (Clinical vs. Non-clinical) emerged as a statistically significant moderator. A much larger effect was seen when the study utilised a non-clinical control group (mean effect (g) = 0.954) compared to a clinical control group (mean effect (g) = 0.437) (β = −0.517; p < .001). Neither of the continuous variables, age or gender, were significant.
Results of Moderator Analyses for the Effect of ADHD on Anxiety.
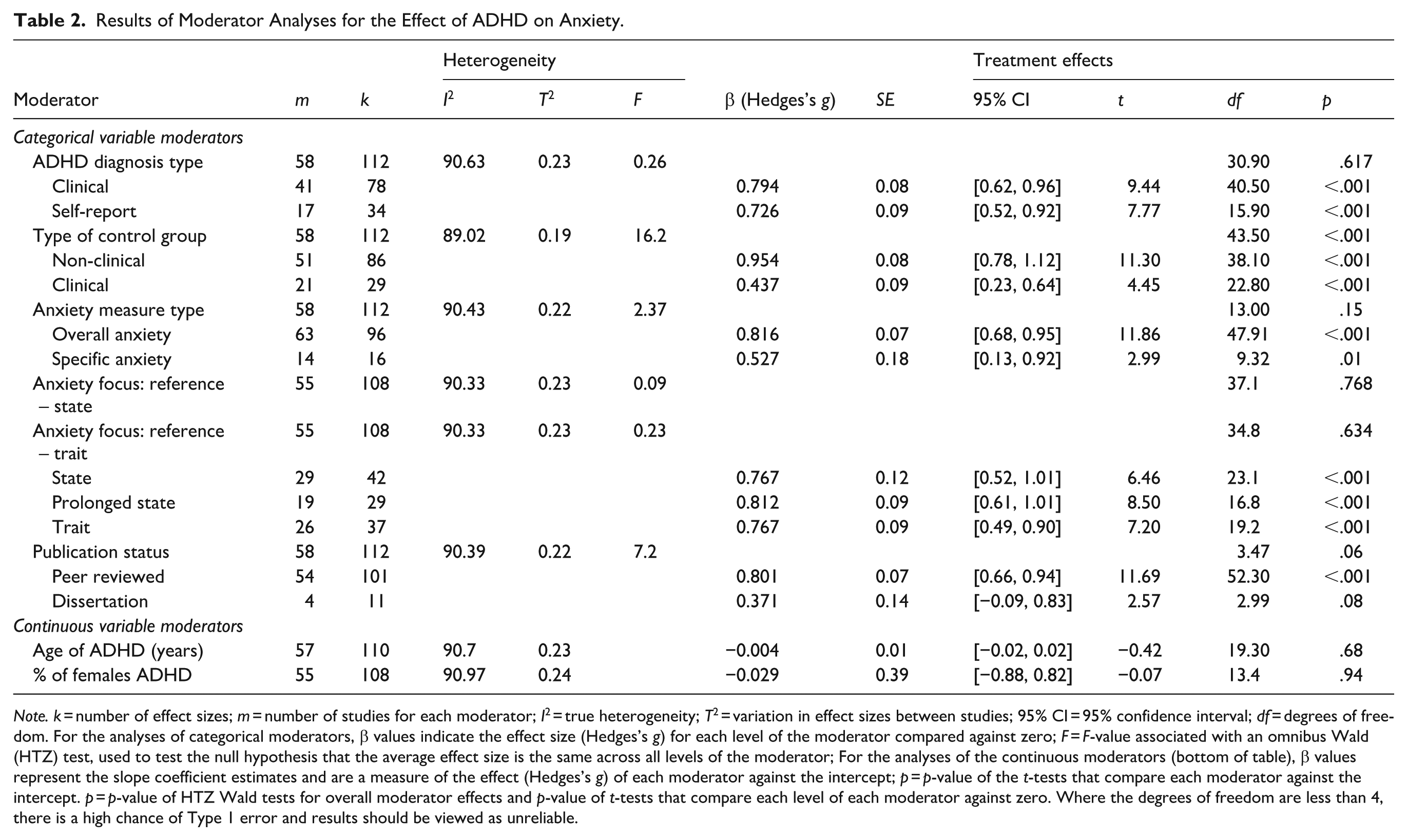
Note. k = number of effect sizes; m = number of studies for each moderator; I2 = true heterogeneity; T2 = variation in effect sizes between studies; 95% CI = 95% confidence interval; df = degrees of freedom. For the analyses of categorical moderators, β values indicate the effect size (Hedges’s g) for each level of the moderator compared against zero; F = F-value associated with an omnibus Wald (HTZ) test, used to test the null hypothesis that the average effect size is the same across all levels of the moderator; For the analyses of the continuous moderators (bottom of table), β values represent the slope coefficient estimates and are a measure of the effect (Hedges’s g) of each moderator against the intercept; p = p-value of the t-tests that compare each moderator against the intercept. p = p-value of HTZ Wald tests for overall moderator effects and p-value of t-tests that compare each level of each moderator against zero. Where the degrees of freedom are less than 4, there is a high chance of Type 1 error and results should be viewed as unreliable.
Publication Bias
The effect of ADHD on anxiety severity was different for published studies (mean effect (g) = 0.801) compared to unpublished studies (mean effect (g) = 0.371), but this was not significant (β = −0.429; p = .06) (see Table 2). A Wald test similarly showed no significant effect of publication type as a moderator, F (3.47) = 7.2, p = .06, I2 = 90.39, T2 = 0.22.
Funnel plots were generated to further assess publication bias. Visual inspection of the plot of aggregated effect sizes (Figure 3a) indicates right sided asymmetry, but the Precision Effect Estimate with Standard Error (PEESE) test was not statistically significant (p = .055). A funnel plot of disaggregated effect sizes was generated to consider selective outcome reporting. Visual inspection of this plot (Figure 3b) also showed some right sided asymmetry, and the Precision-Effect Test (PET) test was statistically significant (p = .05). The trim and fill method found no indications of missing studies and minimal publication bias.
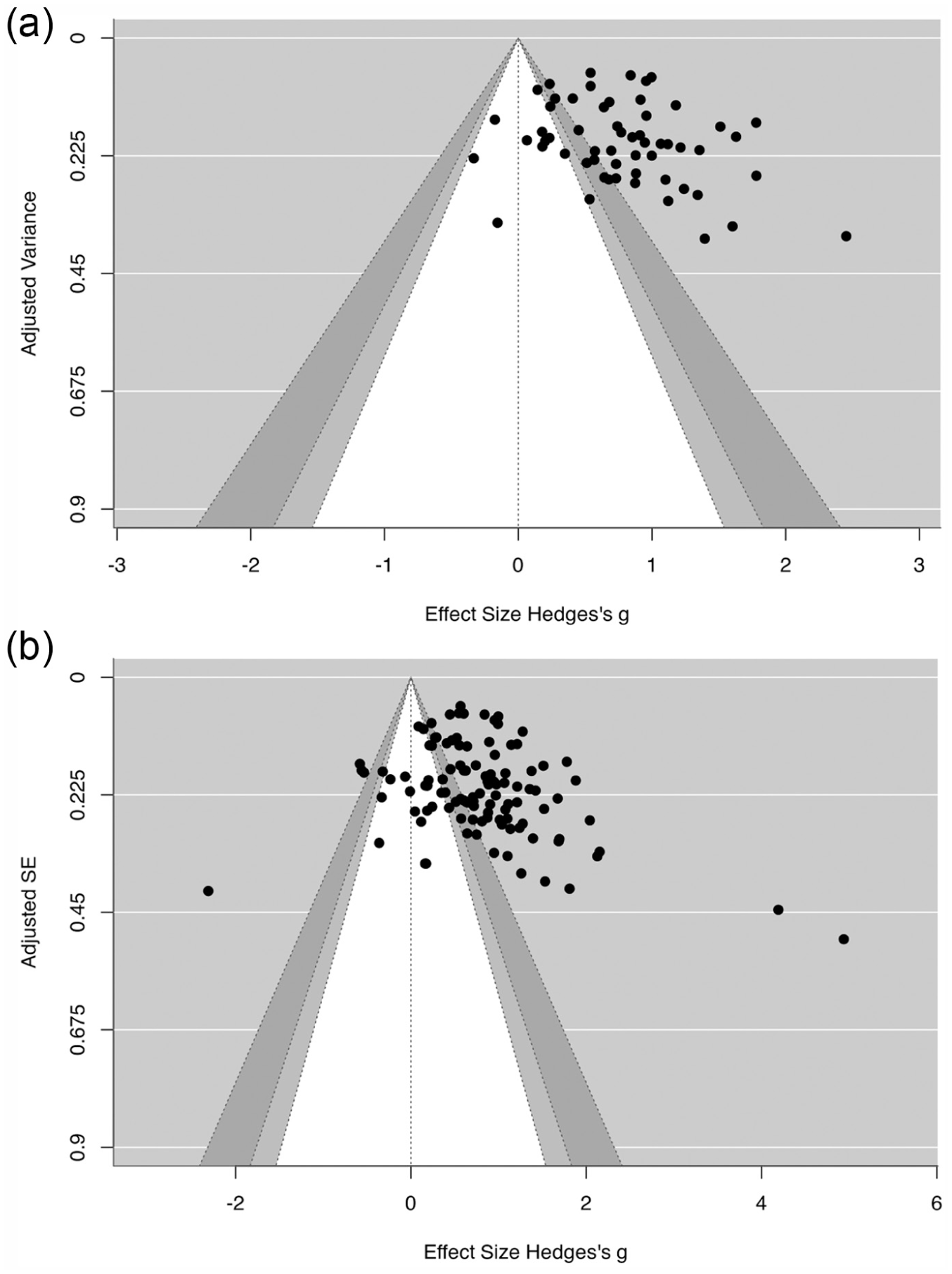
(a) Study level funnel plot of aggregated effect sizes for ADHD on anxiety and (b) effect size level funnel plot of disaggregated effect sizes for ADHD on anxiety.
Discussion
This study addressed the question of whether there is a difference in scores on anxiety measure between individuals with and without ADHD. Prior systematic reviews indicate an increased prevalence of anxiety in individuals with ADHD (Choi et al., 2022; Hartman et al., 2023) however, this is the first meta-analysis quantifying the differences in symptoms and severity of anxiety between adults with and without ADHD, rather than focusing on categorical diagnostic status alone.
The results from this meta-analysis indicate that across studies anxiety scores are higher in adults with ADHD, compared to those without ADHD and that this is a moderate sized effect (g = 0.77). These findings add to the overall understanding of the relationship between ADHD and anxiety and are important to consider in relation to prior research that has indicated that this co-occurrence can change the presentation and prognosis of each condition (D’Agati et al., 2019).
The meta-analysis indicated some heterogeneity between studies (T2 = 0.22) with a substantial percentage of this related to true difference rather than random error (I2 = 90.47) (Higgins et al., 2003). Heterogeneity is important within meta-analyses as it can indicate that studies are highly different and not measuring the same effect. Combining these studies could be unsuitable (Engels et al., 2000) and present challenges in drawing a robust overall conclusion. Although I2 is independent to the number of studies included in a meta-analysis (Higgins & Thompson, 2002), research has indicated that the I2 statistic increases with larger samples (Rücker et al., 2008). This indicates a limitation in using the I2 statistic, especially using it to indicate clinical heterogeneity in studies (Borenstein et al., 2017; Rücker et al., 2008). The T2 value may be more representative of variation between studies as this is insensitive to sample size or number of studies (Rücker et al., 2008). There was a low T2 in this study, indicating low to moderate heterogeneity. Furthermore, as studies included were expected to be diverse yet clinically relevant to the research question, the heterogeneity reinforced the need for the moderator analysis.
Moderators in the Relationship Between ADHD and Anxiety Symptomology
Interestingly, of the moderators considered, only the type of control group emerged as having a statistically significant effect. When a non-clinical population was used as the comparison group, a large mean effect (g = 0.954) was seen (Cohen, 1988, 1992). This is in line with findings that in the general population there is a higher prevalence of anxiety disorders in individuals with ADHD (Choi et al., 2022; Kessler et al., 2006) and provides further evidence for the suggestion that individuals with ADHD experience greater levels of anxiety (Agarwal et al., 2012; Nelson & Liebel, 2018).
When adults with ADHD were compared to a clinical population without ADHD a small to medium mean effect (g = 0.437) was seen (Cohen, 1988, 1992). This indicates that although the prevalence rate of anxiety is higher in individuals from psychiatric populations with ADHD than without (Choi et al., 2022) there is less difference in the severity of anxiety symptomology. This result may relate to findings that anxiety and mood disorders are the dominant conditions that individuals seek mental health treatment for (Gorlin et al., 2016; Wang et al., 2005), for example in some of these studies the comparisons made are very conservative comparing adults with ADHD to adults with a clinical diagnosis of anxiety or depression.
There are some potential limitations of the binary method used in this study to categorise control groups. This approach was selected due to several studies having unspecified mixed clinical control groups. Future research could consider how the specific nature of a clinical control group moderates the effect of ADHD on anxiety symptoms. Particularly as negative effects were seen when individuals with ADHD were compared to individuals from specific sub-groups, for example those with Postural orthostatic tachycardia syndrome (POTS; Raj et al., 2009).
Furthermore, studies that included a clinical control group with anxiety were included in this study. This was due to the overarching interest in considering whether the presence of ADHD impacted on anxiety symptom severity when compared to any non-ADHD population. A further level to the control group moderator was considered to differentiate clinical control groups which included those with anxiety, however, this was not possible as there were too few studies to split the effect sizes and the analysis would have been under powered. It would be useful for future meta-analyses to compare scores on anxiety measures for individuals with anxiety with and without co-occurring ADHD.
Although this study found that the type of anxiety measure used (general vs. specific) did not moderate the effect of ADHD on anxiety scores, the “specific” category encompassed various forms of anxiety, such as test anxiety and separation anxiety. Given the diverse nature of anxiety disorders, future research should investigate whether differences in anxiety scores between individuals with and without ADHD vary depending on what specific type of anxiety is assessed. For example, despite previous research indicating a higher prevalence of social anxiety in individuals with ADHD (Gorlin et al., 2016; Kessler et al., 2006), two studies in this meta-analysis reported a negative effect of ADHD on LSAS (Liebowitz, 1987) scores when comparing individuals with social anxiety to those with ADHD (Mörtberg et al., 2012) or both ADHD and social anxiety (Yoldas et al., 2019).
Despite prior research highlighting the impact of heterogeneity in ADHD diagnosis and definition on the co-occurrence between ADHD and anxiety diagnoses (Choi et al., 2022; Koyuncu et al., 2022), no moderation effect was found for the method used to categorise the ADHD group. Little difference was seen in the effect sizes when a study used a clinical procedure including an interview (g = 0.794), or an ADHD questionnaire or self-report alone (g = 0.726). The criteria for inclusion in each category was agreed by the primary research team, yet this relied on how the authors of studies described the method used to determine ADHD. A lack of detail regarding the ADHD classification criteria used in some papers may impact on the validity of the categories used in this analysis. It will be important for authors of future research to ensure they include clear descriptions of how ADHD status is determined to facilitate the inclusion of this as a potential moderating factor in meta-analyses on ADHD. Future research may also wish to include correlational analysis comparing the severity of ADHD and anxiety measures.
Neither age or gender of the ADHD group were found to influence the effect of ADHD on anxiety symptomology. However, some studies did not specify age or gender or only did so for the whole sample. As this study focused on adults, the mean age of participants within studies ranged from 18.2 to 46 years. It would be beneficial for future research to include under 18s and adults later in life to better understand the relationship between co-occurring ADHD and anxiety across the full life span. There were more males in the ADHD groups which is in line with findings that females are often under-diagnosed with ADHD (Adamis et al., 2022; Robison et al., 2008). Despite research indicating a higher prevalence of ADHD in Transgender and Gender Diverse (TGD) individuals (Goetz & Adams, 2024), only one study found within this review reported the number of TGD participants (Bodalski et al., 2019). Future research is needed to further understand the symptomology and severity of co-occurring ADHD and anxiety across gender identities, particularly given the risk of higher minority stress in TGD individuals (Ignatova et al., 2025).
This review included studies from around the world (Table 1), with the highest proportion originating from Europe (N = 21, 36.21%). The individual countries with the largest contribution were the United States of America (N = 16, 27.59%) and Türkiye (N = 11, 18.96%). A small proportion of studies were from Asia (N = 6, 10.34%), and South America (N = 4, 6.90%) but no studies were found from Africa. Although there has been an increase in global awareness and interest in ADHD, geographical differences have been found in the focus and publication of ADHD research (Hodgkins et al., 2012). As cultural differences have been seen in the expression and recognition of both ADHD and anxiety (Hofmann & Hinton, 2014; Wilcox et al., 2007), it would be beneficial for future research to explore whether this influences the relationship between ADHD and co-occurring anxiety.
Considerations
The findings of this meta-analysis should be interpreted in the context of some limitations that may have influenced the effects. First, only one author extracted data from the studies for analysis. However, steps were taken to ensure data accuracy, including reviewing extracted data prior to creation of effect sizes, then inspecting any outliers. Furthermore, criteria for allocation to moderator categories was agreed within the research team. Although there is evidence indicating that independent data extraction can result in more errors (Buscemi et al., 2006), errors and disagreements have similarly been seen when multiple reviewers are utilised, yet little impact has been found on overall conclusions (Jones et al., 2005).
Although no significant moderation effect was found for publication type suggesting lower risk of publication bias, as the degrees of freedom were less than four, this increases the likelihood of a type 1 error (Tanner-Smith et al., 2016). The lack of significance may be due to the small number of studies within the dissertation group. Overall, there does appear to be some publication bias within these findings, so results should be interpreted with this in mind. To aid with this, future researchers should endeavour to adhere to open research practices and to publish/make available all findings on anxiety and ADHD, even if not significant, that is, null findings.
Implications
Anxiety is a common sometimes debilitating condition (Davies et al., 2022) and has been seen to worsen ADHD symptomology (Reimherr et al., 2017) and have a significant impact on the quality of life of individuals with ADHD (Agarwal et al., 2012). Despite this, there is a lack of awareness regarding the association and interaction between these co-occurring conditions (D’Agati et al., 2019). The findings of this study provide further insight into anxiety symptomology for individuals with ADHD and how this can differ in severity to individuals without ADHD. This information is important for healthcare professionals who are involved in the assessment or treatment of individuals with ADHD and/or anxiety, as this deeper understanding will allow for appropriate adjustments to practice and guidelines. This may include further assessment questions to differentiate symptomology, or screening for anxiety in individuals with ADHD and providing resources and signposting for symptom management so that co-occurring anxiety is not overlooked. Given that ADHD is often underdiagnosed in individuals with other co-occurring mental health difficulties (Gorlin et al., 2016), these findings also reinforce the suggestion to test adult patients presenting with more severe anxiety symptomology for ADHD (Pehlivanidis et al., 2014). Importantly, it will be important for clinicians to distinguish symptoms carefully to prevent misdiagnosis (Koyuncu et al., 2022). Such adjustments could lead to substantial improvements in the quality of life of individuals with ADHD and reduce the likelihood of further psychiatric difficulties developing (Brown, 2000; Katzman et al., 2017).
The findings of this study also have implications for individuals with ADHD and their support network. For example, psychoeducation on anxiety symptomology in ADHD could lead to better understanding and reduced stigma from self or others. These preventative measures may also support children with ADHD who may be at risk of elevated anxiety. However, further research is needed to understand if there is a difference across the lifespan. Furthermore, additional meta-analysis research into the impact of anxiety on ADHD symptomology would be beneficial due to potential implications for the effective treatment of ADHD (Gorlin et al., 2016) given recent debate as to whether anxiety exacerbates ADHD symptomology or is a protective factor (Jarrett & Ollendick, 2008; Reimherr et al., 2017).
Conclusion
This study aimed to comprehensively and systematically review the literature to better understand the relationship between ADHD and anxiety. Analysis found that individuals with ADHD score higher on measures of anxiety than individuals without ADHD. This adds to prior research indicating an increased prevalence of anxiety disorders in individuals with ADHD, indicating that anxiety symptoms are elevated in those with ADHD irrespective of anxiety diagnostic status. This effect is moderated by the type of comparison group used, with the difference being larger when individuals with ADHD are compared to a non-clinical population than to a clinical population. No moderation effect was found from the age or gender ratio of the ADHD group, the method of classifying ADHD or the type or focus of the anxiety measure used. These findings have important implications for the diagnosis and treatment of individuals with ADHD and co-occurring anxiety to ensure effective support for this population to improve symptom management and overall quality of life. Future research is needed to better understand factors influencing the relationship between ADHD and anxiety to help towards comprehending the aetiology and chronicity of this co-occurrence.
Footnotes
Appendix A: Search Strings
Appendix B: Analytical Approach
Outputs from Rstudio demonstrating each stage of analysis (Figures B1–B13).
Appendix C: Study ADHD Measures
Information regarding all the measures used to determine ADHD within studies included in the meta-analysis (Table C1).
Appendix D: Study Anxiety Measures
Information regarding all the measures used to measure anxiety within studies included in the meta-analysis (Table D1).
Acknowledgements
We thank and acknowledge Faye Darmanin and Matthew Poole for their assistance in the data search and extraction process.
Ethical Considerations
This review article does not contain any studies with human or animal participants. Therefore, no ethical review was required.
Consent to Participate
As this review article did not contain participants, no informed consent was required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was undertaken as part of Jessica’s doctoral training, which was funded by NHS England. The authors have no other funding sources to acknowledge.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.