
Abstract
Over 7000 youth ages 13–24 are diagnosed annually with HIV-1 in the United States despite the 2018 approval of oral pre-exposure prophylaxis (PrEP) for adolescents, highlighting the need for more research on provider prescribing practices in pediatric populations. Prior research chiefly focuses on patient barriers to accessing PrEP, and thus, our study explored provider barriers. From August to December of 2023, we conducted a survey of medical providers in pediatrics, family medicine (FM), and internal medicine (IM)/pediatrics. A 5-point Likert scale (0–4) assessed comfort in providing adolescent sexual health care and potential barriers to PrEP prescription, including discussions around sexual activity, gender identity, sexual orientation, sexually transmitted infections, and PrEP. In total, 158 responses were received. FM providers were more familiar with PrEP (3.4 to 1.5, 76.4% difference) and with prescribing PrEP (3.4–0.7, 131.2%) than pediatric providers. Logistic regression analysis found that FM providers were 32 times more likely to prescribe PrEP than pediatric providers. Pediatric providers were 3.4 times more likely than FM providers to identify barriers to PrEP prescription, notably “lack of time to counsel on risk reduction”, “lack of capacity for follow-up”, “lack of knowledge,” and “lack of comfort” and non-prescribers were 2.7 times more likely than prior prescribers to identify barriers, notably “lack of knowledge” and “lack of comfort”. This study highlights the crucial need for educational interventions for pediatric providers around PrEP provision, but also adolescent sexual health care more widely.
Introduction
Combination antiretroviral therapy revolutionized HIV treatment and clinical outcomes, 1 but until the past decade, HIV prevention methods were primarily focused on the recommendations of condom use, abstinence, and routine HIV screening. In 2012, the U.S. Food and Drug Administration (FDA) approved the use of combination tenofovir disoproxil fumarate and emtricitabine (TDF/FTC) as HIV pre-exposure prophylaxis (PrEP) for prevention with 99% effectiveness when taken as prescribed.2,3 Currently, there are four forms of PrEP, two oral medications (TDF/FTC and TAF/FTC) and two long-acting injectable options (intramuscular cabotegravir and subcutaneous lenacapavir), all estimated to be roughly 99% effective when taken as prescribed.4–6 However, it was only in 2018 that the FDA amended its recommended indication for PrEP to include adolescents (anyone with a minimum weight of 35 kg), and in 2021 was expanded to all sexually active persons who inconsistently use condoms or have recently been diagnosed with a sexually transmitted infection (STI). 7
Despite these updated recommendations, there remains a significant gap between the Center for Disease Control and Prevention’s (CDC) official recommendations for PrEP prescription and actual uptake among adolescents.8–10 Every year, youth aged 13–24 account for roughly 20% of new HIV infections in the United States and more than half of adolescents are unaware that they are living with HIV, despite only 13% of all adults not knowing their status.11,12 Youth aged 13–24 have similar rates of HIV viral suppression and linkage to care when compared with adults; however, larger gaps exist in HIV prevention. Only 23% of young adults for whom PrEP is indicated have been prescribed the therapy. 12 As such, increased focus and attention need to be given to HIV diagnosis and biomedical prevention in youth populations.
Despite this need, awareness and uptake of PrEP among young people are significantly lower when compared with adults.13–15 Age consistently correlates with knowledge of/or prior PrEP usage across studies, and youth generally demonstrate a lack of knowledge about and access to PrEP despite the incidence and prevalence rates of HIV in this demographic.13–15 HIV prevention is particularly crucial in young adult populations, as they are often at increased risk for failure to achieve viral suppression and linkage to health care services when compared with adults with HIV.12,16 Further, racial, gender, and sexual minorities are not only less likely to know about and have access to PrEP, but are often at higher risk of poorer clinical outcomes when diagnosed with HIV.17,18 African American adolescents and young adults have been shown to have the lowest rate of viral suppression and the highest rates of viral rebound. 17 Transgender patients are also at increased risk of HIV acquisition, having reportedly higher rates of HIV risk factors, including unprotected sex or commercial sex work. 19 As such, further research to expand PrEP prescription and uptake is crucial for our young adult population, but especially for communities that have historically lower PrEP prescription rates and higher barriers to health care.
To date, most research on PrEP has focused either exclusively on the patient perspective or has consisted of small focus groups of pediatric and adolescent providers.20,21 Studies of adolescent medical providers have determined that they are unfamiliar with the established CDC clinical guidelines for PrEP, are worried about parental involvement and patient confidentiality laws, and are concerned about monitoring for side-effects and adherence.22–24 However, these studies have either been limited by survey or focus group sample size. 20 Very few studies have looked at a wide continuum of providers able to prescribe PrEP to pediatric patients, such as family medicine providers, medicine/pediatrics trained physicians, and advanced practice providers (e.g., physician assistants [PAs] and/or advanced practice nurses [APNs]). In 2017, data indicated that primary care providers were much less likely to be aware of, feel comfortable talking about, and have prescribed PrEP than HIV-specific providers, however, only adult providers were represented, indicating a need for specific focus on providers who serve adolescent populations. 22
Our primary study objective was to utilize a provider survey adapted from Petroll et al. to determine adolescent provider characteristics that are associated with an increased likelihood of prescribing HIV PrEP. 22 Secondarily, we sought to determine the comfort and familiarity of medical providers in speaking with adolescents about sexual health care, sexual orientation, and gender identity, and provider-perceived comfort and identified barriers to PrEP prescription.
Methods
From August to December of 2023, we conducted an anonymous cross-sectional, online survey of adolescent providers, including physicians (MD/DO), APNs, and PAs within the disciplines of pediatrics, family medicine, and IM/pediatrics. Respondents were recruited via IRB-approved solicitation emails to provider listservs within two Chicagoland academic hospital systems, and to private provider groups within Chicago, Northwest Indiana, Florida, and West Virginia. Participant eligibility criteria included: (1) identification as a provider in an ambulatory/outpatient setting, and (2) specialty of general Pediatrics, Family Medicine, or IM/Pediatrics. Exclusion criteria included specialists within the fields of Infectious Diseases or Adolescent Medicine.
The 30-item measure (Appendix A) assessed respondent characteristics, including professional background, practice type, and years in practice. Comfort and familiarity in adolescent sexual health care were assessed, including questions about sexual activity, gender identity, sexual orientation, and STIs. 5-point Likert scales (0 = very uncomfortable; 2 = neutral, 4 = very comfortable) measured respondents’ level of comfort in each activity. Provider comfort and familiarity with PrEP were assessed with the same Likert scale and included questions on comfort and familiarity with PrEP overall, the different forms of PrEP administration, on-demand PrEP, and for specific adolescent populations, including gender and sexual minorities.
Respondents were presented with a list of potential barriers to prescribing PrEP and offered an open response box to describe their own perceived barriers. Finally, respondents were asked if they had prescribed PrEP in the past year, and if so, to estimate how many prescriptions they provided.
Statistical analysis
For all respondents, descriptive analyses with unweighted frequencies and weighted proportions of item measure responses were compared according to provider characteristics. For each characteristic, Likert scale responses were averaged. The association between provider characteristics and the likelihood of a provider having prescribed PrEP in the past was described via multivariable logistic regression. Only pediatrics and family medicine providers were included within this analysis due to the small number of IM/pediatric respondents. Multiple logistic models were built; to assess the statistical significance of including additional parameters in our models, we conducted likelihood-ratio (LR) tests comparing a full unrestricted model (with every item measure) with restricted models including sequentially fewer parameters. Using LR tests, we iteratively compared progressively simpler models until the simplest restricted model with an adequate fit to the data was selected. Additionally, we generated correlation matrices of responses to all non-provider-characteristic item measures to assess for meaningful correlation coefficients between Likert-scaled integer responses (0–4). The Pearson correlation coefficient assumed a linear relationship between the variables. Analyses were conducted using StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC.
Results
Provider characteristics
A total of 158 providers responded to the survey, 94 (59.5%) of whom were in General Pediatrics and 60 (38.0%) in FM. Of those responding, 88 (55.7%) providers identified as attending physicians, 31 (19.6%) as APNs, 28 (17.7%) as pediatric residents, 9 (5.7%) as PAs, and 2 (1.3%) as pediatric fellows (Table 1). Of all providers surveyed, 117 (74.1%) worked only in outpatient settings, while 38 (24.1%) worked in both inpatient and outpatient settings. Most respondents, 67 (42.4%), worked in private practice, 51 (32.3%) in federally qualified health centers, and 24 (15.2%) in academic medicine. Nine (5.7%) respondents identified as working in other settings, including telehealth or rural community clinics. There was a wide range of experience, with 43 (27.2%) of respondents having 0–4 years of experience, 37 (23.4%) with 5–9 years of experience, and 53 (33.5%) with more than 10 years’ experience.
Characteristics of Provider Respondents (N = 158)
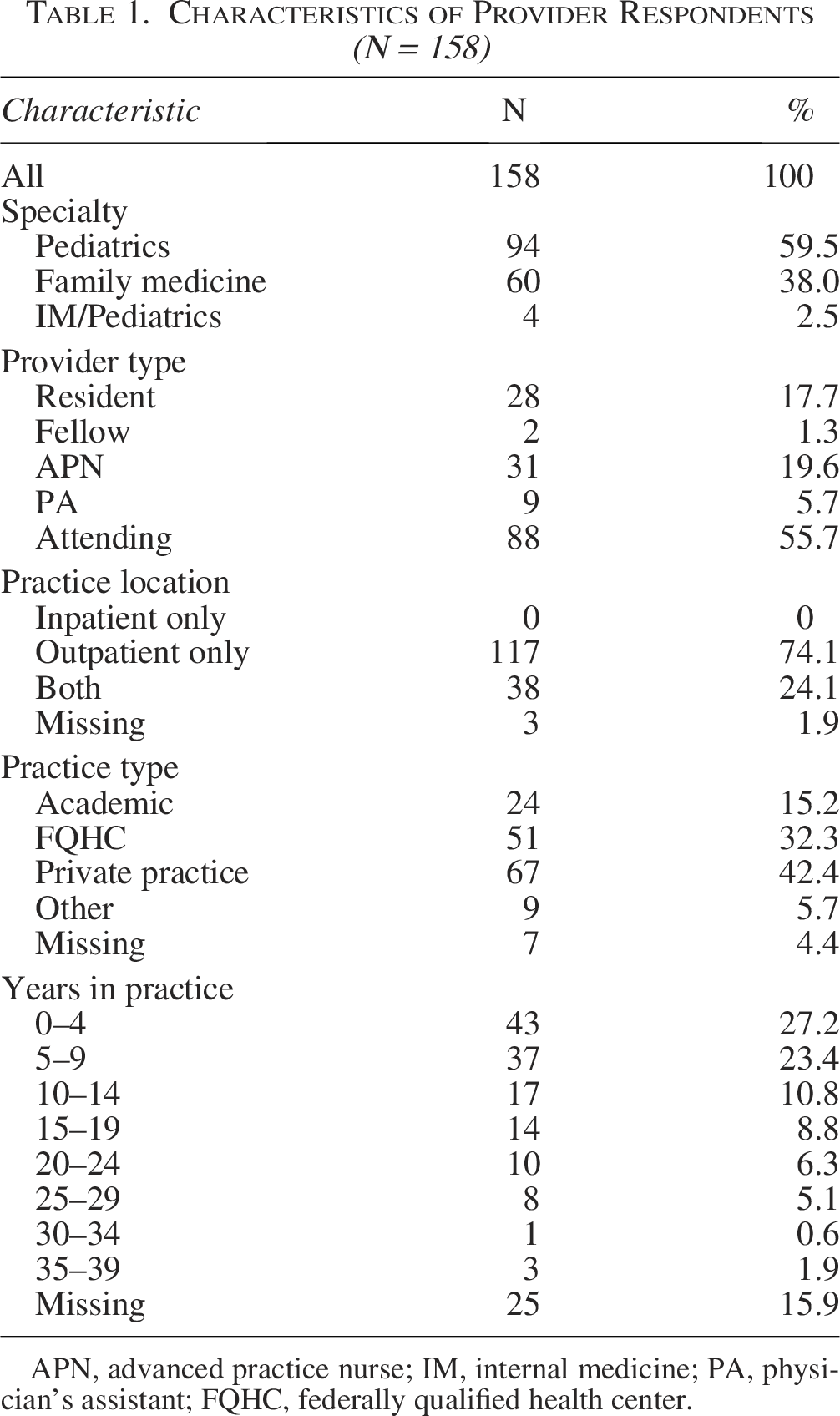
APN, advanced practice nurse; IM, internal medicine; PA, physician’s assistant; FQHC, federally qualified health center.
Comfort and familiarity with sexual health care
Pediatric and FM providers were compared in their level of comfort and familiarity with different aspects of sexual health care using 17 different Likert-scaled questions inspired by the Petroll et al. (2017) study. 22 Family medicine providers were identified as being more comfortable across all aspects of sexual health care that were asked about, as compared with pediatric providers (Table 2). Differences in comfort and familiarity were notably different with PrEP overall (3.42 to 1.53, 76.4% difference), prescribing PrEP (3.37 to 0.70, 131.2%), with PrEP for cisgender men who have sex with men (0.97 to 3.22, 107.40%), with PrEP for transgender and gender diverse persons (0.85 to 2.88, 108.85%), PrEP for cisgender women (0.81 to 2.88, 112.20%), and with prescribing on-demand PrEP (2.42 to 0.60, 120.5%). Additionally, family medicine providers were more comfortable discussing sexual orientation (3.45 to 3.01, 13.62%), gender identity (3.32 to 2.72, 19.87%), providing treatment for STIs (3.72 to 3.19, 15.34%), and diagnosing HIV (2.17 to 1.53, 34.59%).
Comparing Comfort and Familiarity in Different Aspects of Sexual Health Care Between Pediatrics and Family Medicine (N = 154)
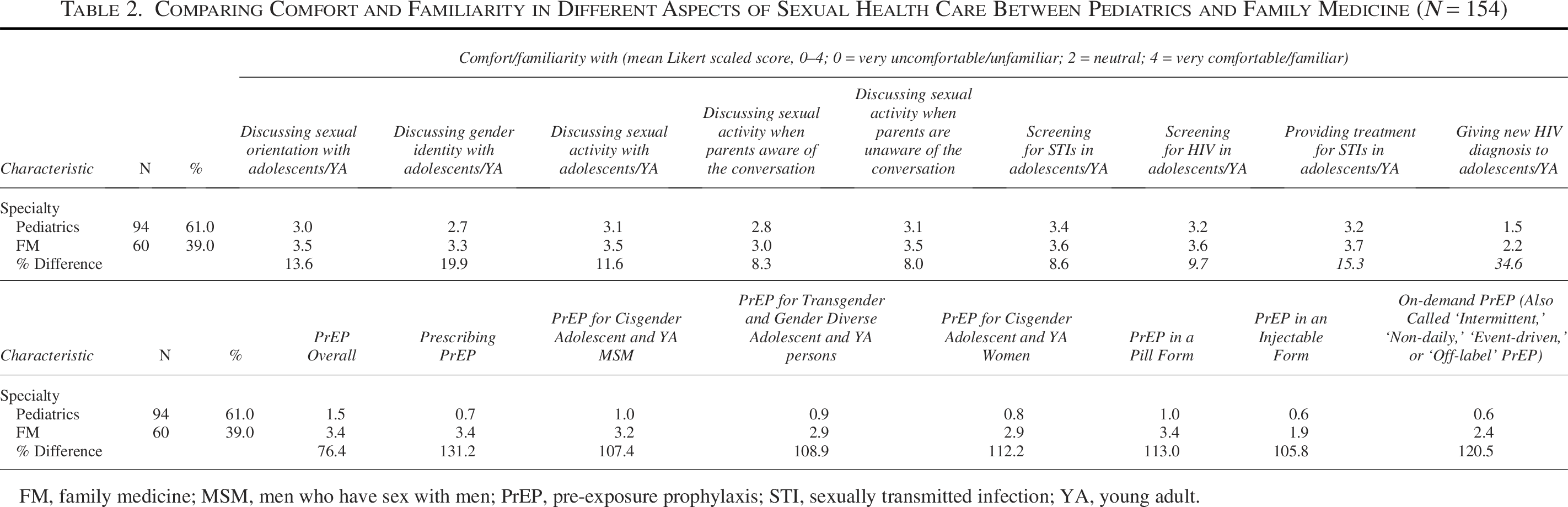
FM, family medicine; MSM, men who have sex with men; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection; YA, young adult.
Likelihood of having been prescribed PrEP
Multivariable logistic regression was utilized to assess whether specialty type, provider type, practice type, and/or a provider’s comfort in talking about sexual orientation and/or gender identity significantly predicted their likelihood of having prescribed PrEP (Table 3). Of the covariates, only specialty and provider type were significantly predictive, where it was found that family medicine providers were 32 times more likely to prescribe PrEP than pediatric providers. Additionally, attending physicians were nearly 10 times more likely than residents/fellows and nearly four times more likely than APNs/PAs to prescribe PrEP.
Multivariable Associations Between Provider Characteristics and Likelihood of Having Prescribed PrEP
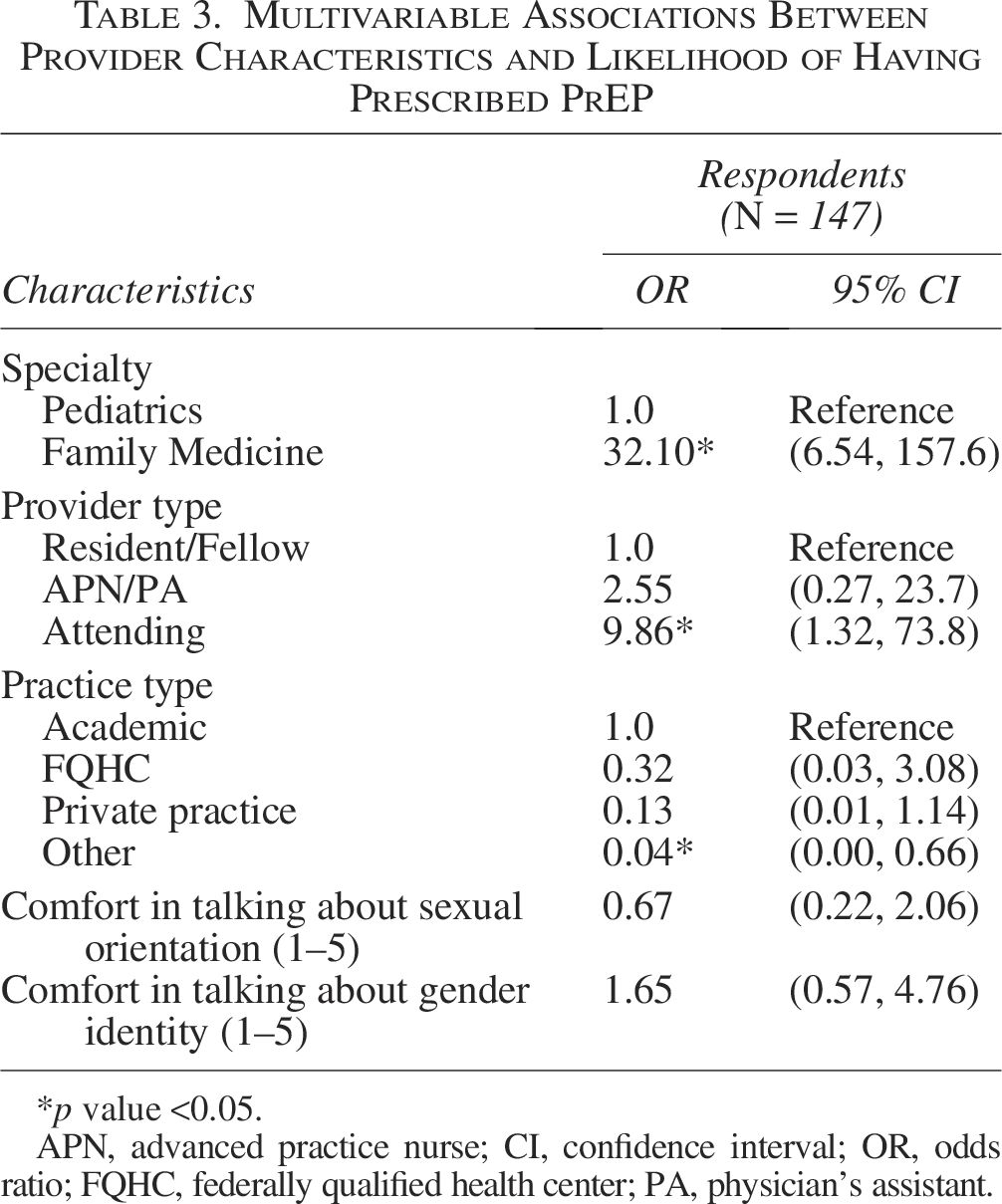
p value <0.05.
APN, advanced practice nurse; CI, confidence interval; OR, odds ratio; FQHC, federally qualified health center; PA, physician’s assistant.
Comparing family medicine to pediatric providers
Pediatric providers were 3.43 times more likely to identify barriers to PrEP prescription than family medicine practitioners (95% CI: 1.75–6.89, p = 0.0003). About 71% of pediatricians identified at least one barrier to PrEP prescription compared with 42% of family medicine providers. When looking at individual barriers identified, statistically significant differences between family medicine and pediatric providers were found with “lack of time to counsel on risk reduction” (p = 0.048), “lack of capacity for follow-up” (p = 0.018), “lack of knowledge with PrEP” (p < 0.0001) and “lack of comfort with PrEP” as barriers to prescription (p < 0.0001). Notably, of pediatric providers, 67.0% identified a lack of knowledge with PrEP as a barrier, and 60.6% identified a lack of comfort as a barrier, compared with 11.7% and 8.3% of family medicine providers, respectively (Fig. 1).
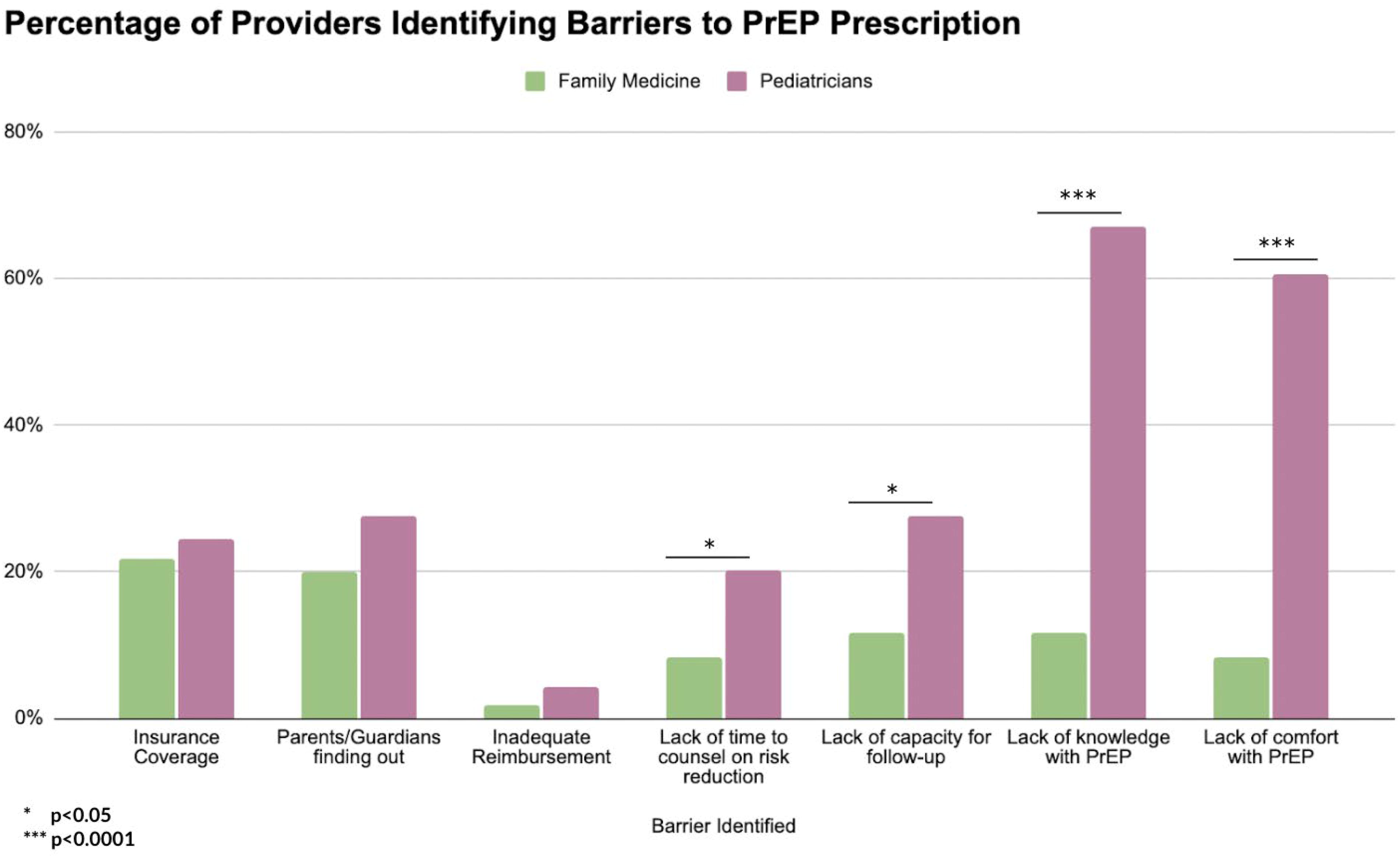
Differences in Pediatric and Family Medicine Providers Identified Barriers to PrEP Prescription. PrEP, pre-exposure prophylaxis.
Comparing prior PrEP prescribers to non-prescribers
Providers who had never prescribed PrEP in the past were 2.68 times more likely than prior PrEP prescribers to identify barriers to PrEP prescription (95% CI: 1.39–5.25, p = 0.003). Approximately 45% of PrEP prescribers identified at least one barrier to PrEP prescription compared with 69% of non-prescribers (p = 0.004). When looking at individual barriers identified, statistically significant differences between PrEP prescribers and non-prescribers were found only with “lack of knowledge with PrEP” (p < 0.0001) and “lack of comfort with PrEP” (p < 0.0001) as barriers to prescription. Notably, 66.0% of non-prescribers identified a lack of knowledge with PrEP and 60.6% identified a lack of comfort as barriers, compared with 15.6% and 10.9% of PrEP Prescribers, respectively (Fig. 2).
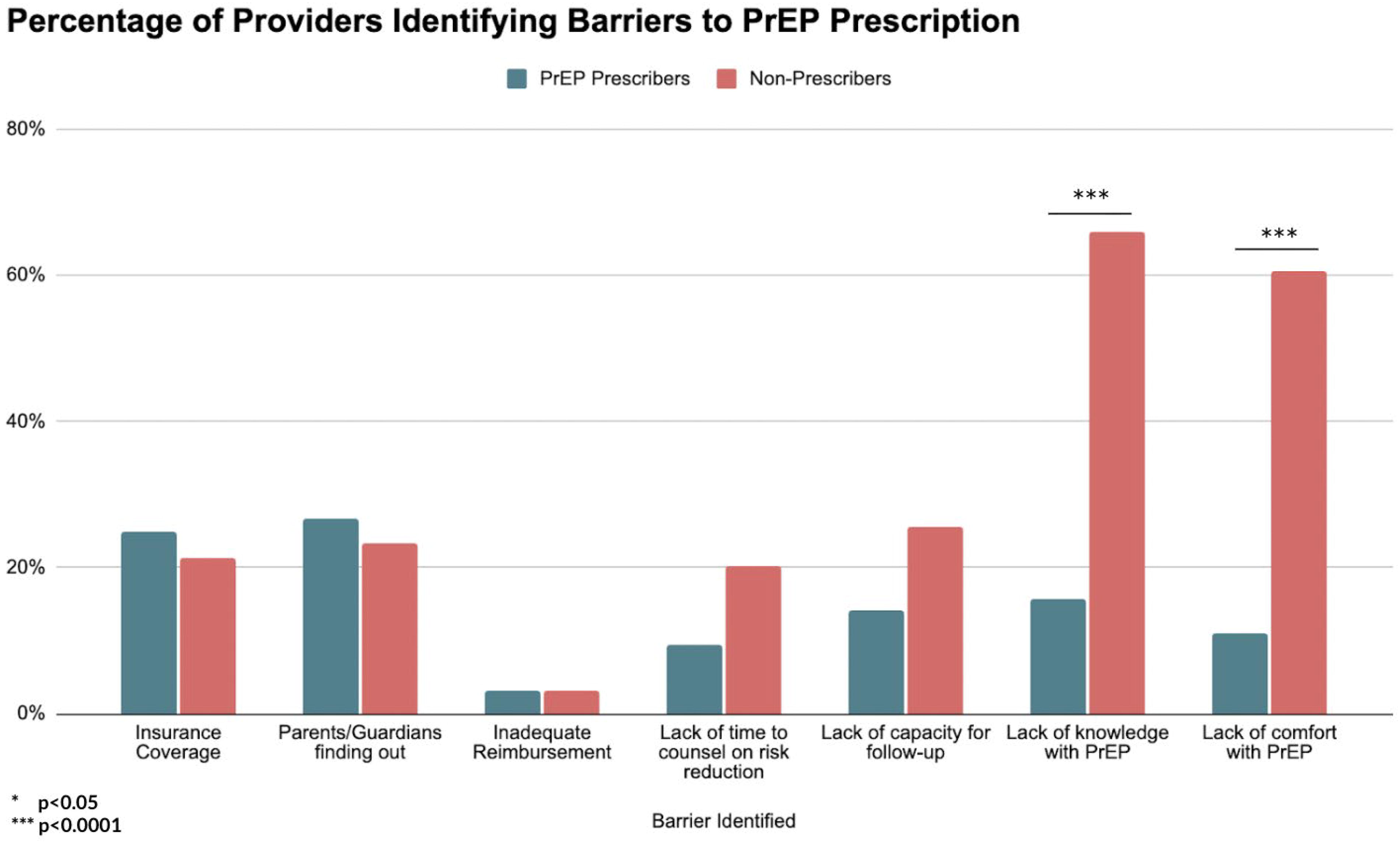
Differences in Prior PrEP Prescribers and Non-Prescribers Identified Barriers to PrEP Prescription. PrEP, pre-exposure prophylaxis.
Discussion
Our study highlights a significant gap between family medicine and pediatric providers in discussing and providing sexual health care to adolescents. Family medicine providers were universally more comfortable discussing different aspects of sexual health care, including prescribing PrEP to adolescents, being 32 times more likely to have prescribed PrEP than pediatric providers. Perhaps even more stark is the comparison of Likert-scaled comfort and familiarity in different aspects of sexual health care, comparing pediatric and family medicine providers. Notably, pediatric providers reported lower comfort with all aspects of adolescent sexual health care (discussing gender/sexuality, treating STIs, etc.). The inference is that pediatric providers, because they do not routinely see adult patients and therefore, may have a patient population with less sexually active patients. However, the 2023 Youth Risk Behavior Surveillance System estimated that 32% of high school students have had sex, and only around half of those teenagers had used a condom during their last sexual encounter. 25 As such, there is a clear role for pediatric providers to play in discussing sexual health care with their patients, a role explicitly outlined by the American Academy of Pediatrics (AAP). 26 It is thus vital to improve the pediatric provider’s role in promoting safe adolescent sexual health.
Our study’s distinct gap between family medicine and pediatric providers’ Likert-scale ratings of comfort with adolescent sexual health care can partially be explained by a profound lack of standardization in pediatric residency training on topics of adolescent medicine. 27 Further, we showed that there is a lack of knowledge and comfort around PrEP for HIV prevention in pediatric providers, a finding that is fairly well-known and appreciated in the literature. 28 However, prior research methodologies have either only included small focus groups, been limited in survey scope, or been focused on patient-specific barriers to care.10,20,29 Our study is the first to show this finding on a large scale and from the provider perspective. Targeted educational interventions are needed to increase PrEP knowledge and comfort for pediatric providers. Research on the role of adolescent medicine rotations has shown that pediatric residents do increase their self-perceived skill level, especially regarding sexual health care; however, considerable variation exists in the timeline of adolescent medicine blocks, faculty and institutional infrastructure, and the range of services available for trainees to learn.27,30 Further, the AAP has identified that, despite their explicit guidelines and recommendations regarding sexual and reproductive health care for adolescents, there is substantial room for improvement across training programs and clinical offices. 31 Finally, few educational interventions have been created and implemented to address the well-identified lack of pediatric provider comfort and knowledge of PrEP, and, when done so, those interventions almost exclusively target adult providers or target providers outside of the United States.32,33 It is our hope that the results of this study will motivate future research endeavors to create targeted graduate and continuing medical education initiatives to improve pediatric provider knowledge of PrEP using both formal didactic instruction and simulation exercises, as done in prior successful studies. 32
Nearly half of the providers who had previously prescribed PrEP were still able to identify at least one barrier to its prescription. For these clinicians, one of the most identified barriers to PrEP was insurance coverage (25.0%). This is particularly noteworthy given that, under the Affordable Care Act, individuals with household incomes below 150% of the federal poverty level are eligible to receive PrEP at no cost, and many states offer PrEP Drug Assistance Programs to further support access. Despite these resources, insurance coverage continues to be significantly associated with PrEP utilization, and literature has noted that even small increases in out-of-pocket PrEP cost can lead to drastic increases in patient abandonment rates.34,35 Prior research has underscored the need to expand insurance access and leverage community-based organizations to broaden PrEP availability. 36 However, these solutions often depend on patient initiative or large-scale systemic and policy reform. In this context, it becomes increasingly critical for pediatric practices to establish strong partnerships with local organizations and proactively offer support to uninsured patients, particularly amid the ongoing threat to erode insurance coverage at the national level.
Further, 26.6% of PrEP prescribers identified concerns about parental or guardian discovery of a PrEP prescription as a perceived barrier. Although this proportion did not significantly differ from non-prescribers, it reflects a persistent tension between adolescent confidentiality and parental involvement. The literature highlights that legal protections for adolescent confidentiality in the context of HIV prevention remain fragmented across states, with only 33 jurisdictions allowing minors to consent to PrEP and only 18 of those specifying confidentiality protections. 37 Structural factors, such as insurance billing practices, also pose risks to confidentiality. Under the Affordable Care Act, explanation of benefits (EOBs) are typically sent to the primary policyholder, often a parent or guardian, deterring adolescents from seeking care and disproportionately impacting adolescents from low-income families.36,38 Strengthening confidentiality protections at the state and federal level, alongside clearer clinical guidelines and increased partnerships with community-based organizations that do not have to provide EOBs, may reduce this barrier. Innovative delivery models for PrEP, such as Illinois’ Pharmacy Act, which allows pharmacists to prescribe PrEP, and school-based health centers, represent promising avenues to improve equitable access to PrEP without compromising confidentiality. 39 Lastly, more formal training around adolescent confidentiality laws is needed within medical school and residency curriculum to ensure pediatric providers, like their family medicine counterparts, can feel confident and comfortable prescribing PrEP. 40
While providing valuable insight into the key differences between FM and pediatric providers with respect to PrEP prescription in adolescent populations, there are several limitations to our study. A 30-item measure, while based on prior published research, is a survey of limited depth. 22 We attempted to balance survey comprehensiveness with length to optimize response rates, but this survey did not ask questions regarding specific types of STIs or other aspects of sexual health care, such as pregnancy and contraception. Moreover, we were unable to assess response rates due to the nature of survey distribution being through listservs. We did not assess other basic provider demographics, such as urban versus rural location of practice, which may have influenced results, as most HIV transmission through sexual contact occurs in urban settings. 12 Respondents were also not queried about the ages of patients they see. Most studies of HIV for adolescent and young adults include patients between the ages of 13–24, despite roughly 80% of new HIV diagnoses in this category occurring among patients at least 20 years of age. 11 As such, further research might benefit from elucidating the specific needs of adolescents (age 13–17) versus young adults (age 18–24), especially as young adults are much more likely than adolescents to experience a gap in health care access. 41 Though we attempted to mitigate biases via the dissemination of an anonymous survey to various groups of providers across the United States, our research is limited by biases inherent in surveys, such as the possibility of social desirability bias, selection bias, and recall bias. Finally, though our findings suggest a lack of knowledge and comfort with PrEP are key barriers to increasing prescription rates, we did not elucidate the specifics behind what information providers would like to know to feel knowledgeable and comfortable with PrEP.
Building on the findings of this study, future research should aim to further elucidate specific gaps in provider knowledge related to PrEP and adolescent sexual health care, potentially through the utilization of provider interviews and/or focus groups. Insights gleaned from this qualitative data, in combination with the current study findings, could inform the development of future educational and systemic interventions to enhance provider competence and confidence in discussing and prescribing PrEP. Given the ongoing scarcity of research focused on PrEP access and utilization among adolescents, continued investigation in this area is essential. Improving provider knowledge and reducing barriers to PrEP is a critical step toward expanding access to this vital preventive therapy for youth populations.
Authors’ Contributions
A.R.: Methodology, formal analysis, investigation, resources, writing—original draft, writing—review and editing, visualization. J.R.: Conceptualization, methodology, resources, writing—review and editing, supervision. J.M.: Conceptualization, methodology, software, validation, formal analysis, investigation, resources, writing—original draft, writing—review and editing, visualization, supervision.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This article was supported by the National Research Service Award under grant award 5TL1TR002388 (for J.M., MD, MS; PI: David Meltzer, MD, PhD). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of National Center for Advancing Translational Science/National Institutes of Health.
Appendix A
Sexual Health Care in Pediatrics – Survey Instrument
(Select one)
Pediatrics Internal Medicine/Pediatrics Family Medicine Pediatric Hospitalist Medicine Medical Student
(Select one)
Attending Fellow Resident Physician’s Assistant Advanced Practice Nurse
(Select one)
Pediatrics Internal Medicine/Pediatrics Family Medicine
(Select one)
Outpatient Pediatrics Inpatient Pediatrics Both
(Select one)
Private Practice Academic Pediatrics Federally Qualified Health Center (FQHC) Other: ___________________________
(5-point Likert Scale: Very Uncomfortable | Somewhat Uncomfortable | Neutral | Somewhat Comfortable | Very Comfortable)
Discussing sexual orientation with adolescent/young adult patients Discussing gender identity with adolescent/young adult patients Discussing sexual activities with adolescent/young adult patients Discussing sexual activities with adolescent/young adult patients Discussing sexual activities with adolescent/young adult patients Screening for STIs (not including HIV) in adolescent/young adult patients Screening for HIV in adolescent/young adult patients Providing treatment for STIs in adolescent/young adult patients Giving a new diagnosis of HIV to an adolescent/young adult patient
(5-point Likert Scale: Very Unfamiliar | Somewhat Unfamiliar | Neutral | Somewhat Familiar | Very Familiar)
PrEP overall Prescribing PrEP PrEP for cisgender adolescent and adult men who have sex with men (MSM) PrEP for transgender and gender diverse adolescent and adult persons PrEP for cisgender adolescent and adult women PrEP in a pill form PrEP in an injectable form On-demand PrEP (also called “intermittent,” “non-daily,” “event-driven,” or “off-label” PrEP)
Yes No
(Select one)
0 1–10 11–20 21–50 51–100 100+
(Select all that apply)
Cisgender adolescent and adult MSM Transgender and gender diverse adolescents and adults Cisgender adolescent and adult women
Yes No
Yes No
Concerns about insurance coverage Concern about parents/guardians finding out Inadequate reimbursement Lack of time needed to counsel on risk-reduction Lack of capacity for follow-up monitoring Lack of knowledge about PrEP Lack of comfort/familiarity in prescribing PrEP Other: ____________________________