
Abstract
Black cisgender women in the Southern United States experience disproportionate human immunodeficiency virus (HIV) rates. Pre-exposure prophylaxis (PrEP) is an effective HIV prevention tool but is underutilized in this population. We assessed PrEP cascade outcomes and correlates among Black women in the Southern United States. Between March and June 2022, we administered a cross-sectional online survey to Black cisgender women residing in the Southern United States who reported unprotected sex in the past 6 months and were negative for HIV by self-report. Participants provided information on sociodemographic characteristics, HIV knowledge, PrEP awareness and use, psychosocial factors, and health care access. We used descriptive statistics and multivariate logistic regression models to describe the sample and assess the correlates of PrEP outcomes, respectively. Participants included 491 Black women, with a mean age of 40.1 years (SD: 17.5); 53% had a college degree or lower, and 79% were single. PrEP awareness was 39.5%, willingness 25.7%, and current use only 5.5%. The factors associated with PrEP awareness included younger age (aOR = 1.02, 95% CI: 1.01–1.03), higher education (aOR = 1.68, 95% CI: 1.09–2.60), medical trust (aOR = 1.09, 95% CI: 1.03–1.15), binge drinking (aOR = 1.77, 95% CI: 1.06–2.94), and HIV testing in the past year (aOR = 1.55, 95% CI: 0.98–2.45). The PrEP willingness predictors included HIV testing in the past year (aOR = 1.80, 95% CI: 1.11–2.90) and HIV worry (aOR = 1.84, 95% CI: 1.09–3.09). HIV testing emerged as a key facilitator for both PrEP awareness and willingness, suggesting that testing encounters represent critical opportunities for PrEP integration. PrEP strategies should address both individual-level factors and structural barriers, particularly medical trust within health care systems.
Introduction
Human immunodeficiency virus (HIV) infections continue to be a significant public health issue in the United States, with approximately 1.2 million people currently living with the virus. 1 An estimated 32,000 new cases of HIV were recorded in 2021, reflecting a decrease from previous years. 2 However, disparities persist, particularly within geographical regions and within Black communities. The Southern United States faces a disproportionate burden of HIV. Despite comprising only 38% of the national population, the US South accounts for 52% of all new HIV infections in the nation, with the rates continuing to rise even as other regions see declines. 3 This geographic disparity is compounded by profound racial inequities, with Black Americans disproportionally affected when compared with other races. 4 Black Americans account for 40% of new HIV infections despite representing only 12% of the US population. 2 Among US women, 60% of new HIV infections are in Black cisgender women (subsequently referred to as “women”), who comprise just 13% of the female population. 5 These intersecting geographical patterns, racial, and gender disparities call for targeted HIV prevention strategies that address the unique context of Black women in the Southern United States.
Pre-exposure prophylaxis (PrEP) is a highly effective HIV prevention strategy for people who are vulnerable to HIV infection. 6 The US Food and Drug Administration (FDA) has approved two daily oral pills—emtricitabine/tenofovir disoproxil fumarate (F/TDF) and emtricitabine/tenofovir alafenamide (F/TAF) 7 —and two long-acting injectable medications—cabotegravir (CAB-LA) 8 and lenacapavir 9 —as PrEP medications, with F/TDFCAB-LA and lenacapavir available for use among women.7,8 PrEP 9 when delivered at a scale to populations vulnerable to HIV infections, has the potential to significantly reduce HIV acquisition and contribute to ending the HIV epidemic.10–12 The PrEP cascade is critical to the successful implementation of PrEP interventions.13,14 This framework outlines the key stages necessary for maximizing the impact of PrEP, including awareness, access, initiation, and adherence. 13 Understanding the barriers at each step of the PrEP cascade can inform strategies to mitigate these challenges and promote successful PrEP utilization. 13
Despite PrEP’s demonstrated effectiveness, utilization remains notably low among women nationally, with even lower rates documented in the South.15,16 Previous studies have identified several barriers to PrEP uptake and adherence among Black women, including limited awareness or knowledge of PrEP as a preventive option for women.17–23 One critical barrier is the lack of PrEP marketing materials targeted toward women, with most campaigns focusing on men who have sex with men (MSM). 20 This absence of representation in promotional materials leaves many women unaware of PrEP’s potential benefits for them, contributing to a gap in PrEP utilization among women.21,23–26 Another barrier is a low perception of vulnerability to HIV infection among women.23,27,28 When considering the benefits and drawbacks of using PrEP, some women may not perceive their vulnerability to HIV as significant enough to justify the potential side effects or other concerns associated with PrEP use.21–23,26,28
However, a critical gap exists in understanding how these factors operate specifically among Black cisgender women in the Southern United States, a population at the intersection of multiple vulnerabilities. The Southern United States faces unique challenges in PrEP implementation. PrEP usage in this region is lower than in other parts of the country. 23 Barriers in the South include limited access to health care services, a higher proportion of uninsured individuals, a shortage of primary care physicians and PrEP providers, and heightened levels of HIV-related stigma.29–31 Additional barriers include concerns about trust within patient–provider relationships and understanding the short- and long-term side effects of PrEP.15,28,32 While much of the existing research has focused on PrEP cascade barriers among MSM (including Southern MSM populations) and some studies have examined barriers among women nationally, limited data characterize the specific cascade outcomes and associated factors for Black cisgender women residing in the South.17,19,20 This knowledge gap is particularly significant given that this population faces both structural barriers unique to the Southern region and gender- and race-specific barriers documented in other contexts. Without data specific to this population and setting, interventions might not be tailored to the factors influencing PrEP uptake among those who need it the most. Given the low PrEP utilization rates among Black cisgender women and the high incidence of HIV in the Southern United States, applying the PrEP cascade framework may identify specific factors influencing PrEP awareness, willingness, and uptake that are specific to this population.
In the current study, we assessed PrEP cascade outcomes among Black cisgender women residing in the Southern United States. We applied the PrEP cascade framework proposed by Nunn et al. (2017) 13 to examine PrEP awareness, willingness, and use in this population. By identifying the factors associated with these cascade steps, this study provides crucial insights for developing targeted interventions aimed at increasing PrEP uptake among Black cisgender women in the Southern United States. Such efforts are essential for reducing HIV incidence in this disproportionately affected population.
Methods
Study design and participants
A cross-sectional online survey was administered between March and June 2022. To ensure eligibility, all participants completed a screening questionnaire before study participation. Participants were eligible if they identified as a Black woman, reported a negative HIV status, lived in the Southern United States (Alabama, Arkansas, Delaware, the District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia), were proficient in English, had at least one incidence of unprotected sex within the last 6 months in line with CDC’s PrEP eligibility guidelines, 33 and provided informed consent.
Participants were recruited through Qualtrics’ online panels. These panels comprise individuals living across the United States who were willing to participate in research studies. The research team worked with the Qualtrics program coordinator to distribute an anonymous survey. The survey included questions about demographic factors, HIV knowledge and risk perception, health care access, lifestyle factors such as alcohol usage and smoking habits, past health care experiences, and PrEP awareness and likelihood of usage. The majority of questions had binary or Likert-scale response options. The survey took approximately 25 min to complete once participants provided informed consent. Participants were compensated approximately $30 for completing the survey. Participants could decline participation due to safety or privacy concerns, and an emergency button was included on each survey page that redirected the responder to a Google search engine if clicked. The survey did not allow participants to visit previous pages. The survey was pilot tested with 15% of the total respondents before deployment. Following the pilot, the Qualtrics program coordinator implemented a speed check that automatically terminated participants who were not responding thoughtfully, with a cutoff time of 7 min. In addition, browser cookies were used to prevent multiple submissions from the same user. To ensure anonymity, IP addresses were not tracked.
All research procedures were approved by the Old Dominion University Institutional Review Board (#1866874-2). All participants provided written informed electronic consent for the study procedures before accessing the survey.
Measures
PrEP cascade outcomes
For this study, the PrEP cascade outcomes included awareness, willingness, and uptake of PrEP. We created a mutually exclusive PrEP stage variable based on participants’ responses to questions about PrEP awareness, willingness, and uptake. For this study, we only measured oral PrEP. At the time of survey development, oral PrEP was the most widely available and accessible form of PrEP; thus, our survey items focused primarily on oral PrEP. Although long-acting injectable PrEP (cabotegravir) had been approved, its availability and public awareness were limited. We only asked about participants’ willingness to use long-acting injectable PrEP should it become available. Oral PrEP awareness was measured through the question, “Truvada is a pill that HIV-negative people can take to prevent HIV infection. This is called PrEP or Pre-Exposure Prophylaxis. How familiar are you with PrEP or Truvada?” The response options included “not at all familiar,” “somewhat familiar,” and “very familiar.” Responses were dichotomized to “yes” and “no.” “Somewhat familiar” and “very familiar” responses were coded as “yes” for PrEP awareness. In contrast, “not at all familiar” responses were coded as “no.” PrEP willingness was measured with the question, “how likely would you be to use PrEP?” The answer choices included “extremely unlikely,” “somewhat unlikely,” “somewhat likely,” “likely,” and “extremely likely.” Responses were dichotomized to “yes” and “no” in accordance to the previous literature—“Extremely unlikely,” “somewhat unlikely,” and “somewhat likely” were all coded as “no,” and “likely” and “extremely likely” were coded as “yes.” PrEP uptake was measured with the question, “are you currently taking PrEP or Truvada?” The response options included “yes” and “no.” These PrEP cascade outcome measures were adapted from a previous study. 34
Independent variables
The demographic variables included age (in years), education level, income, relationship status, and nativity. Income was dichotomized based on the Federal Poverty Level guidelines, with participants categorized as either below the poverty threshold (annual income <$12,000) or at/above the poverty threshold (annual income ≥$12,000).
Other covariates
The distance to clinic was determined by asking respondents, “How far away is your current medical provider from where you live?” A binary variable was created to separate responses into ≥5 miles and <5 miles.
Medical trust was measured using a 6-item scale that was modified from the original 12-item group-based medical mistrust scale. 35 We selected six items that were relevant to our target population, and the revised scale had a good reliability (Cronbach’s α = 0.73). Statements included “I feel comfortable being open with my medical provider about my sexual history.” Responses were collected using a Likert scale, where 1 represented strong disagreement and 5 represented strong agreement, with a higher overall score indicating greater trust. One question, “I feel that my medical provider looks down on me because of my race,” was reverse-coded to follow the higher score indicates greater trust.
PrEP stigma was measured using 15 items selected from the 22-item PrEP stigma scale previously validated in the United States by Kelin and Washington. 36 We selected these 15 items based on their relevance to our target population (revised scale, Cronbach’s α = 0.93). The sample items included the following: “People will think I am HIV-positive if I take PrEP.” Response options followed a Likert scale format, ranging from 1 indicating “strongly disagree” to 5 indicating “strongly agree.” Scores were summed, with higher scores indicating greater stigma.
Binge drinking was measured using a single item: “Over the past month, when you drank alcohol, what was the largest number of drinks you drank on any one occasion?” Consistent with the definition of binge drinking for women used by the US Substance Abuse and Mental Health Services Administration, participants who reported four or more drinks on any drinking occasion in the past month were coded positive for binge drinking. 37 We assessed binge drinking for it has been shown to influence HIV prevention and PrEP use, increase sexual risk behaviors, and lower engagement in the PrEP care continuum. 38
HIV knowledge was assessed using shortened10-item HIV knowledge scale developed by Oglesby and Alegmagno, which has been validated in both general and key populations, including Black women. 39 Survey respondents answered 10 questions about HIV. The response options for all questions were “yes,” “no,” or “don’t know.” Sample statements included “A woman can get HIV if she has anal sex with a man.” The number of correct responses was calculated for each respondent, with higher scores indicating higher HIV knowledge.
Perceived HIV risk was determined through the survey question, “how likely is it that you will become HIV-positive in your lifetime?” The response options included “very unlikely,” “unlikely,” “somewhat unlikely,” “likely,” and “very likely.” A binary variable was created with “very unlikely,” “unlikely,” and “somewhat unlikely” being coded as “no” and “likely” and “very likely” being coded as “yes.”
HIV worry was determined through the question, “how often do you worry that you might get HIV?” The response options included “never,” “sometimes,” “often,” and “always.” We created a binary variable with “never” coded as “no” and “sometimes,” “often,” and “always” coded as “yes.”
HIV testing in the past year was assessed by asking participants how often they get tested for HIV. Participants who responded being tested in 1 year or less were coded as “yes” for testing in the past year. Participants who responded that they had been tested more than a year or had never been tested were categorized as “no” for not testing in the past year.
Social support was assessed using three sets of questions regarding the availability of supportive individuals in participants’ lives. The questions included the following: (1) “How many people are so close to you that you can count on them if you have great personal problems?” (2) “How much interest and concern do people show in what you do?” (3) “How easy is it to get practical help from neighbors if you need it?” Responses were dichotomized to create a binary social support variable, with participants reporting no support coded as “no” for social support, while those reporting at least one close confidant, degree of interest/concern, and “easy” and “very easy” support from neighbors were coded as “yes” for social support.
Statistical analysis
We used descriptive statistics to characterize the sample. Mean and standard deviations were used to describe continuous variables, while frequencies and percentages were used for categorical variables. We conducted bivariate analysis to determine the associations between demographic factors, HIV risk factors, health care experiences, and PrEP cascade outcomes. To identify the factors associated with PrEP cascade outcomes, we performed multivariate logistic regression analysis on outcomes with adequate sample sizes for reliable modeling. Regression models were conducted for PrEP awareness and willingness. However, PrEP uptake was excluded from the multivariate analysis due to the small number of participants reporting current PrEP use (n = 27) compared with nonusers (n = 464), which limited model reliability. Theoretically relevant variables (education level and relationship status) 20 and covariates that were significant at p < 0.05 in bivariate analysis were added to the multivariate logistic regression on PrEP cascade outcomes. We assessed statistical significance using 95% confidence intervals and p < 0.05. Statistical analyses were performed using STATA version 18.
Results
Sample characteristics
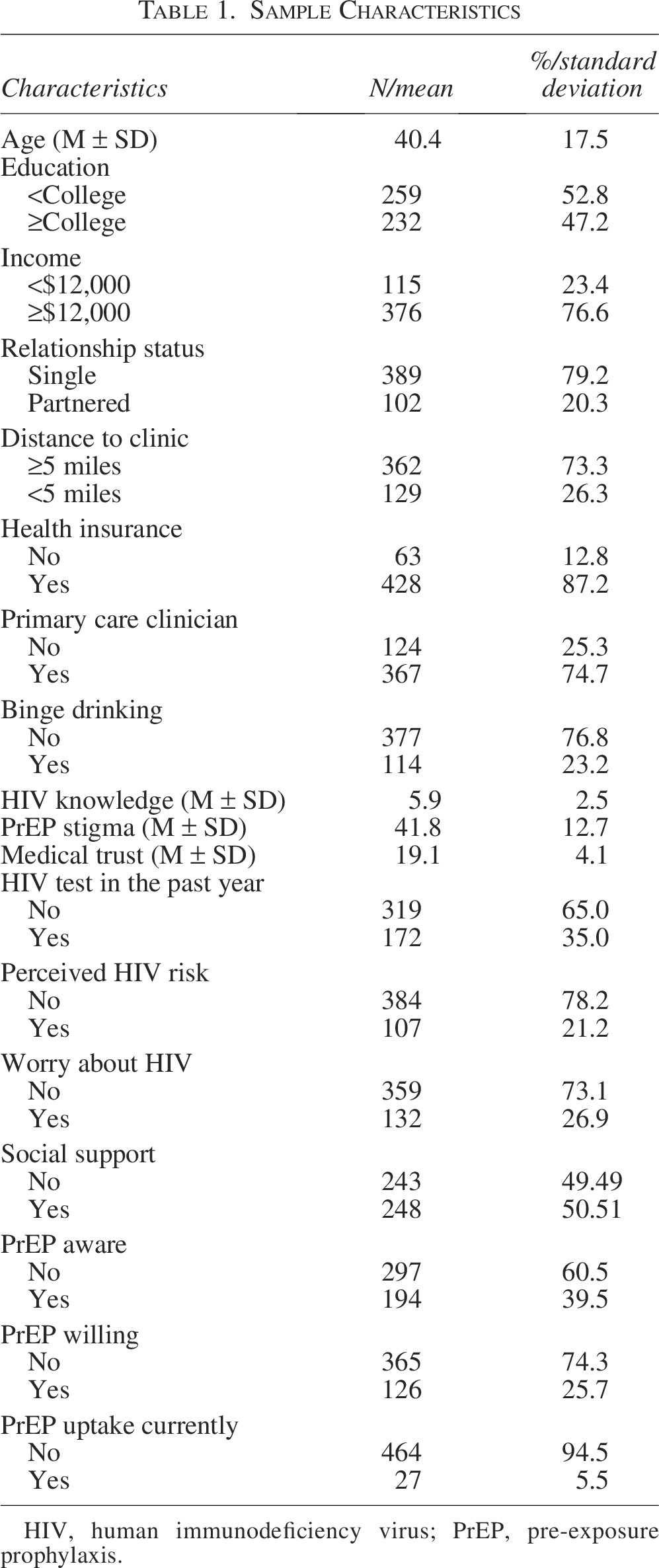
Table 1 shows the sample characteristics. Among the 491 women who responded to the survey, the mean age was 40.4 years (SD: ±17.5), and the education level was split: 52.8% had less than a college degree, and 47.2% had completed college or higher. Most participants (76.6%) reported an annual income of $12,000 or more, and the majority (79.2%) were single. In terms of health care access, most participants (73.3%) lived 5 or more miles from their current provider and had health insurance (87.2%). In addition, many participants (74.7%) had a primary care clinician. The mean HIV knowledge score was 5.9 (SD: ±2.5, range: 0–10), and the mean PrEP stigma score was 41.8 (SD: ±12.7, range: 15–75), indicating moderate stigma levels. Medical trust was measured at a mean of 19.1 (SD: ±4.1, range: 6–30). Within the past year, 35.0% of the participants reported receiving an HIV test. Although 54% of participants either perceived themselves at risk of HIV or expressed worry about HIV, and 45% were eligible for PrEP, only 39.5% were aware of PrEP, 25.7% expressed willingness to use it, and the current PrEP uptake remained low at 5.5% (Fig. 1).
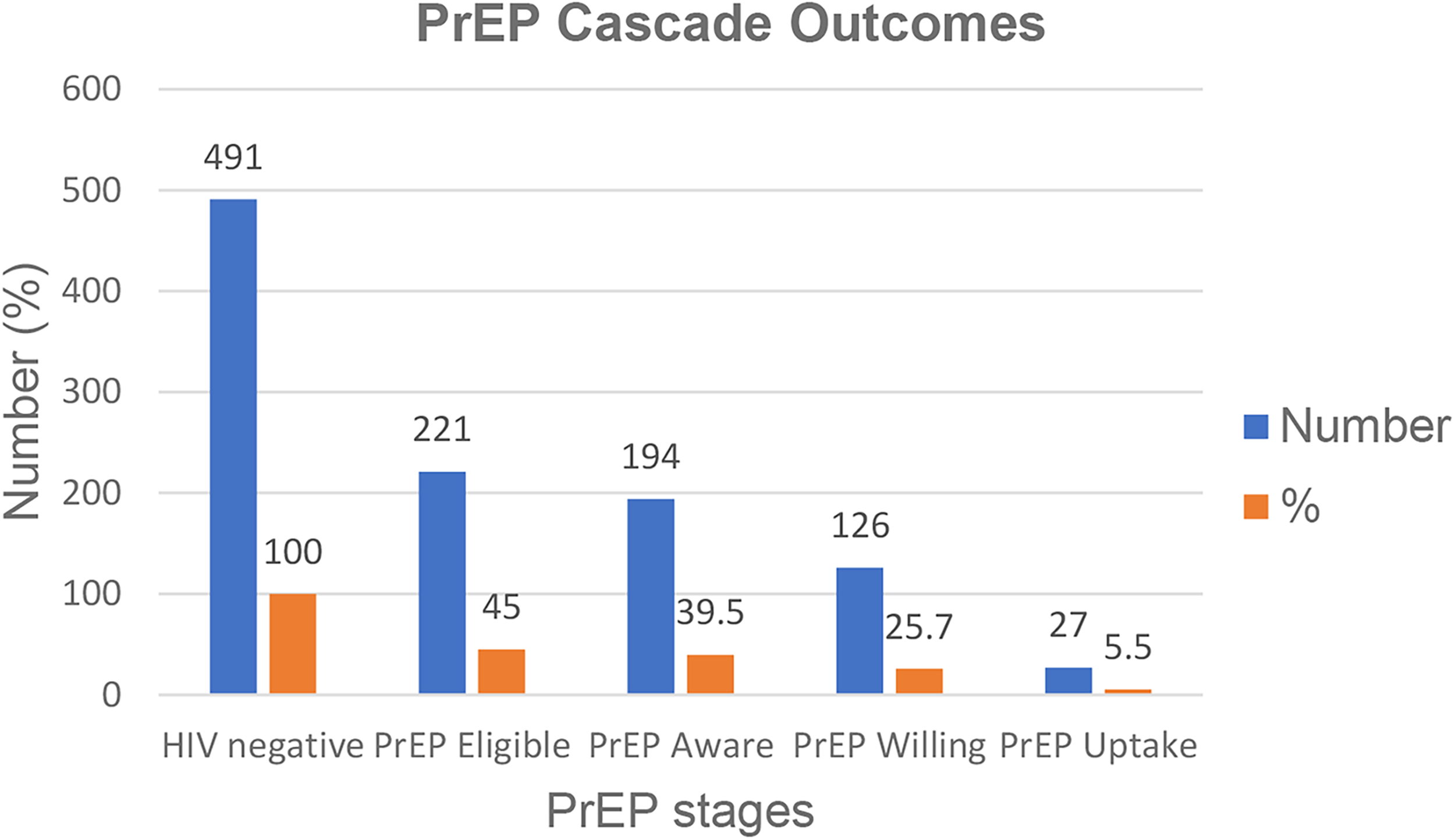
Outcomes based on PrEP cascade stages. PrEP, pre-exposure prophylaxis.
S
HIV, human immunodeficiency virus; PrEP, pre-exposure prophylaxis.
Factors associated with PrEP awareness, willingness, and uptake among Black women in the South
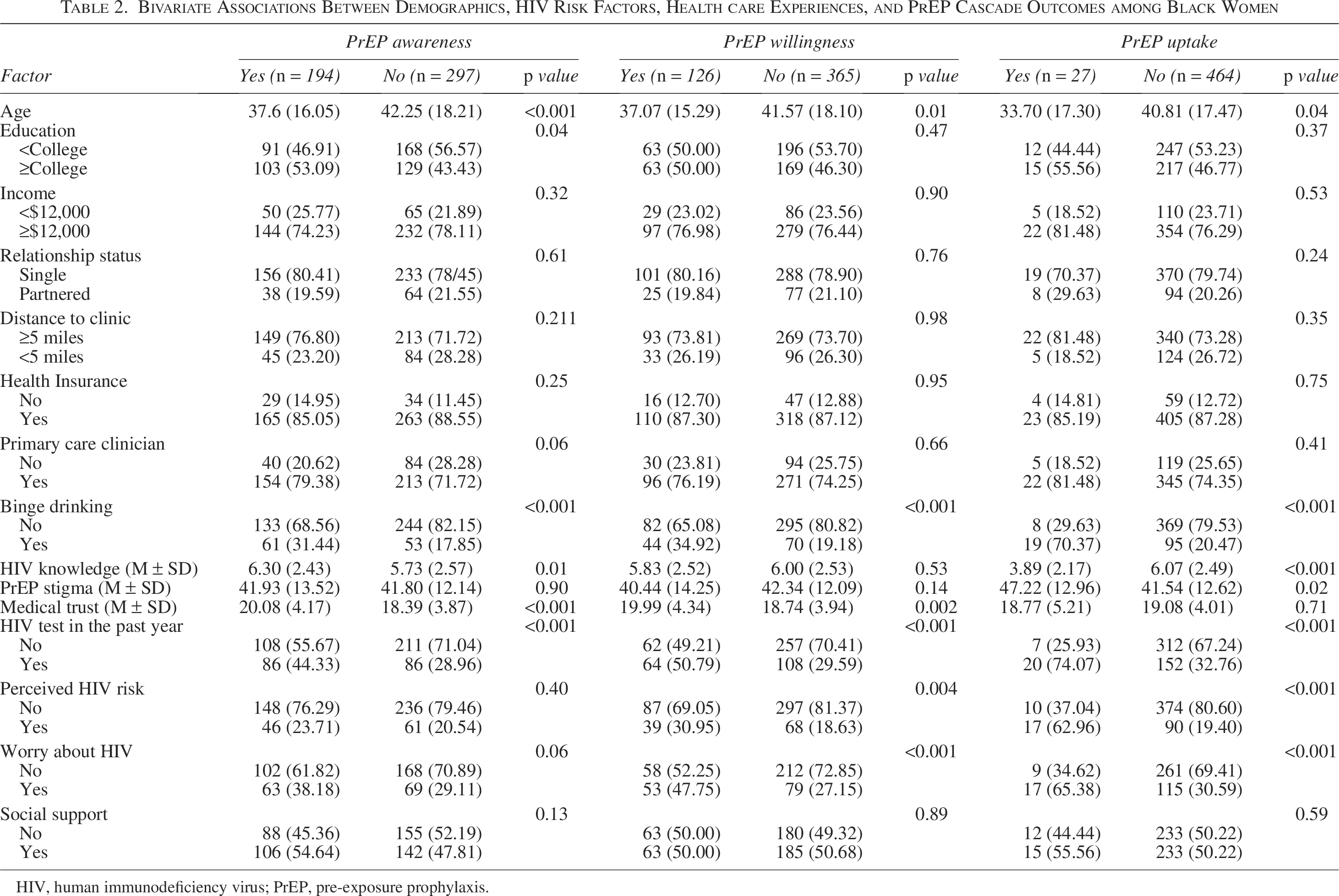
In bivariate analyses (Table 2), several factors were significantly associated with PrEP awareness, willingness, and uptake among Black women in the study. Younger participants were more likely to be aware of PrEP (mean age: 37.6 vs. 42.2 years, p < 0.001), willing to use it (mean age: 37.1 vs. 41.6 years, p = 0.01), and report uptake (mean age: 33.70 vs. 40.8 years, p = 0.04). Higher education attainment was linked to PrEP awareness (53.1 vs. 43.4, p = 0.04) but showed no significant association with willingness or uptake. Binge drinking was associated with higher PrEP awareness (31.4 vs. 17.8, p < 0.001), PrEP willingness (34.9 vs. 19.2, p < 0.001), and PrEP uptake (70.4 vs. 20.5, p < 0.001). Higher HIV knowledge was positively associated with awareness (mean: 6.3 vs. 5.7, p = 0.01), but not with PrEP uptake (mean: 3.9 vs. 6.1, p < 0.001). Participants with greater PrEP stigma demonstrated higher uptake (47.2 vs. 41.5, p = 0.02), while medical trust was linked to increased awareness (mean: 20.1 vs. 18.4, p < 0.001) and willingness (mean: 20.0 vs. 18.7, p = 0.002). Having an HIV test in the past year was significantly associated with greater awareness (44.3 vs. 28.9, p < 0.001), willingness (50.8 vs. 29.6, p < 0.001), and uptake (74.1 vs. 32.8, p < 0.001). Perceived HIV risk was associated with PrEP willingness (30.9 vs. 18.6, p = 0.004) and PrEP uptake (63.0 vs. 19.4, p < 0.001), but not with awareness. Also, worry about HIV was associated with PrEP willingness (47.6 vs. 27.1, p < 0.001) and uptake (65.4 vs. 30.6, p < 0.001).
B
HIV, human immunodeficiency virus;
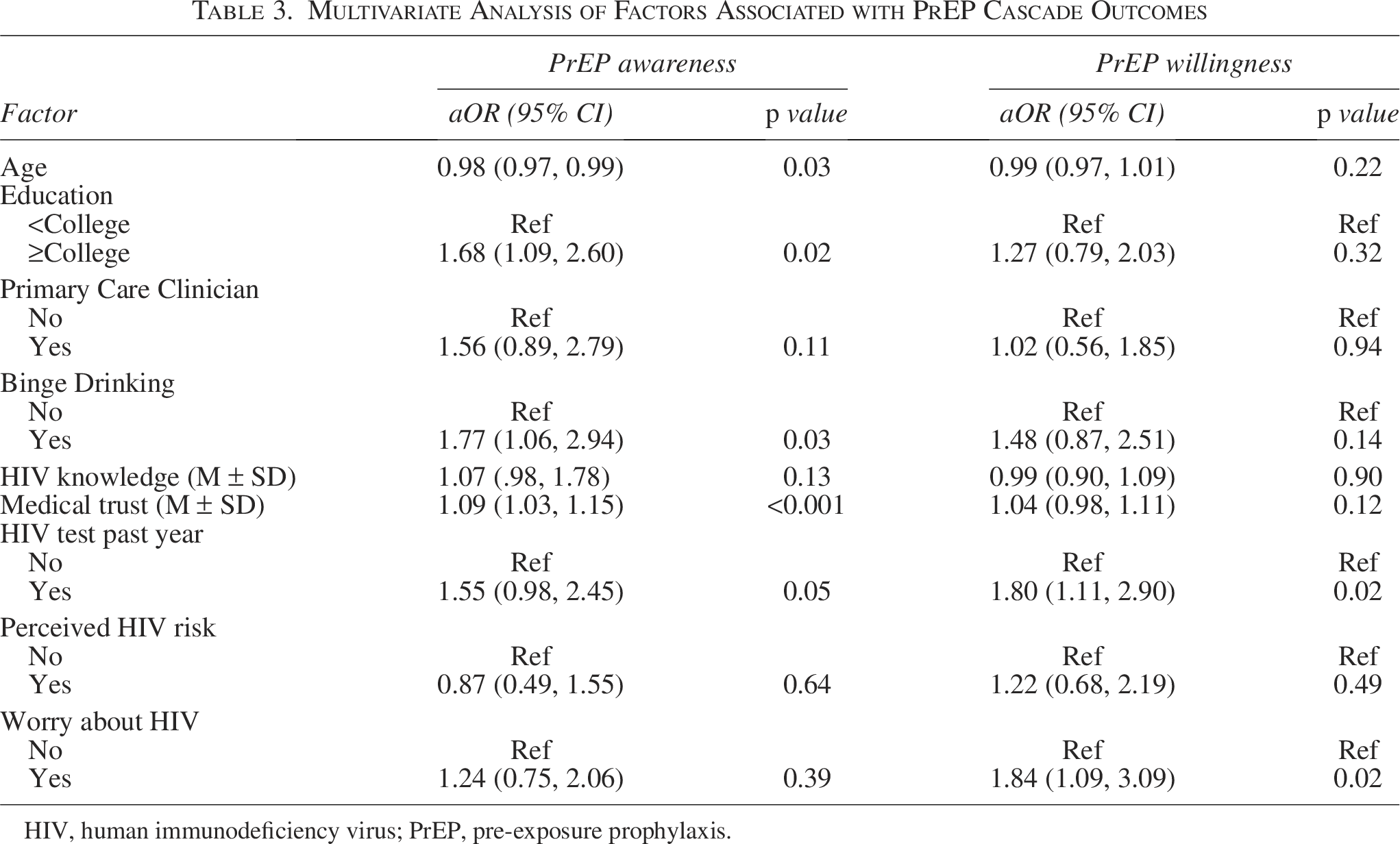
In the adjusted regression model (Table 3), several key factors remained significantly associated with PrEP cascade outcomes (PrEP awareness and willingness). Younger age was associated with higher PrEP awareness (aOR = 0.98, 95% CI: 0.97–0.99, p = 0.03), and having a college education or higher showed 68% higher odds of PrEP awareness than those with less than a college education (aOR = 1.68, 95% CI: 1.09–2.60, p = 0.02). Behavioral factors such as binge drinking showed that participants who reported binge drinking had 77% higher odds of PrEP awareness (aOR = 1.77, 95% CI: 1.06–2.94, p = 0.03), and medical trust was significantly associated with PrEP awareness (aOR = 1.09, 95% CI: 1.03–1.15, p < 0.001). Also, health engagement, as measured by HIV testing in the past year, was significantly associated with PrEP awareness, with those tested showing 55% higher odds of awareness (aOR = 1.55, 95% CI: 1.00–2.43, p = 0.05).
M
HIV, human immunodeficiency virus;
The pattern of associations differed between PrEP willingness and awareness. Only two factors were statistically significant predictors of PrEP willingness in the adjusted model. HIV testing in the past year showed the strongest association with PrEP willingness, with participants who had been tested demonstrating 80% higher odds of PrEP willingness (aOR = 1.80, 95% CI: 1.11–2.90, p = 0.02). Worry about HIV was also significantly associated with PrEP willingness, with those expressing worry showing 84% higher odds of willingness (aOR = 1.84, 95% CI: 1.09–3.09; p = 0.02). Notably, several factors that were significant predictors of PrEP awareness showed no significant association with willingness, including age, college education, binge drinking, and medical trust (aOR = 1.04, 95% CI: 0.98–1.11, p = 0.12). Please note that we did not perform adjusted analyses for PrEP uptake due to the small sample size (current PrEP users = 27 vs. non-PrEP users = 464), which could yield unreliable estimates.
Discussion
We assessed PrEP cascade outcomes (awareness, willingness, and uptake) and identified the factors associated with each outcome. In the adjusted logistic regression model, PrEP awareness was significantly predicted by younger age, college education or higher, binge drinking, greater medical trust, and HIV testing in the past year. In contrast, PrEP willingness was associated with only two factors: HIV testing in the past year and worrying about HIV. PrEP uptake was very low (5%), which prevented regression analysis due to an insufficient sample size. However, bivariate analyses identified correlates, including younger age, binge drinking, HIV knowledge, PrEP stigma, recent HIV testing, perceived HIV risk, and HIV-related worry. Across all cascade stages, recent HIV testing emerged as the most consistent predictor, suggesting that health care engagement is crucial throughout the PrEP cascade.
The finding of recent HIV testing as a consistent predictor across the PrEP cascade suggests that regular health care engagement serves as a critical gateway for PrEP knowledge and consideration. This pattern indicates that women who are already engaged with HIV prevention services are more likely to learn about PrEP and express willingness to use it. This finding aligns with previous research demonstrating the importance of health care engagement in PrEP adoption, particularly studies showing that HIV testing serves as an entry point for PrEP discussions.40–43 However, our results extend beyond the existing literature by revealing distinct predictor patterns across cascade stages, specifically among Black women in the South.
The finding that demographic factors such as younger age and higher education primarily influence awareness, rather than willingness, suggests that once women become aware of PrEP, their decision-making process shifts toward more HIV-specific concerns and personal risk assessment. While prior studies have identified education and age as general predictors of PrEP awareness across diverse populations,43,44 our findings suggest that these demographic factors may be less influential in determining actual willingness to use PrEP in this specific population. The role of medical trust in awareness aligns with the broader literature on health care disparities affecting Black communities,15,45 although its absence as a willingness predictor suggests that trust may be more critical for initial information seeking than for personal decision-making about PrEP use. In addition, women with greater trust in health care systems may be more likely to engage in health information seeking (thus learning more about PrEP); however, trust alone does not overcome the practical barriers to access or the concerns about stigma and side effects that influence willingness and uptake decisions.15,28,31 The finding regarding the low perception of vulnerability among women represents a critical individual-level barrier, as some women may not perceive their HIV risk as significant enough to justify the potential concerns associated with PrEP use.44,46,47 This aligns with our finding that worry about HIV was a significant predictor of PrEP willingness and highly correlated with PrEP uptake in this sample, confirming that risk perception plays an important role in PrEP decision-making.
The Southern United States faces unique implementation challenges that lead to lower PrEP use compared with other regions. These barriers include limited access to health care services,29,31 higher proportions of uninsured individuals,48,49 shortages of primary care physicians and PrEP providers,29,50 and high levels of HIV-related stigma.51,52 Our findings contribute to this literature by providing data on the PrEP cascade, specifically among Black cisgender women in the South, a population that has remained unreached for HIV PrEP. 46 The differences we identified between the factors associated with PrEP awareness and those predicting willingness and uptake are particularly important, as they suggest that awareness alone may be inadequate to facilitate PrEP use without addressing deeper structural and social barriers. Recent interventions on cisgender women support this finding.53,54 A pilot randomized controlled trial by Dale et al. (2024) testing motivational interviewing to increase PrEP uptake among Black women demonstrated that even when women are aware of PrEP, targeted behavioral interventions are needed to facilitate uptake. 53 Also, Clement et al. (2024) identified multiple implementation strategies from the provider, clinic, and community levels necessary to support PrEP access among Black cisgender women in New Orleans. 54 These studies reinforce that awareness campaigns alone are insufficient and should be paired with interventions that directly address medical mistrust, provider communication barriers, and structural barriers to care.
We noted one unexpected finding from our analysis that calls for future investigation. The positive association between binge drinking and higher PrEP awareness, willingness, and uptake was particularly surprising and may indicate that individuals engaging in such behaviors are more likely to be exposed to HIV prevention messaging or targeted interventions. This finding may reflect a subgroup of individuals with increased health care engagement despite engaging in risk behaviors. This finding therefore supports the need for nonjudgmental, supportive messaging that connects harm-reduction strategies with access to preventive care. In addition, while 54% of participants either perceived themselves at risk of HIV or expressed worry about HIV, and 45% were eligible for PrEP, only 39.5% were aware of PrEP, 25.7% expressed willingness to use it, and the current uptake remained low at 5.5%. This substantial gap between risk perception and prevention behaviors suggests that factors beyond risk awareness significantly influence PrEP uptake, such as stigma, cultural attitudes toward preventive medication, and trust in health care institutions
Several limitations should be acknowledged when interpreting these findings. First, the cross-sectional design limits our ability to establish causal relationships between the identified factors and PrEP outcomes. Second, self-reported data on HIV risk factors and behaviors may be subject to social desirability or recall bias. Third, our survey used oral PrEP (emtricitabine and tenofovir disoproxil fumarate), which may have limited our ability to capture PrEP awareness given that the FDA approval of injectable cabotegravir (CAB-LA) occurred in December 2021, 8 shortly before our data collection period. However, this limitation also highlights an important consideration for future PrEP studies in the US South. Long-acting injectable options may address barriers unique to the South, including a lack of health insurance coverage, geographical distance to PrEP-providing facilities, restrictive Medicaid policies, and historical and ongoing medical mistrust. Future research should assess awareness of and preferences for long-acting injectable PrEP among Black women in the South, and implementation strategies. Fourth, while we assessed a range of individual and behavioral factors, we did not assess structural barriers that affect PrEP engagement, such as limited access to culturally competent care, discrimination, and racism within health care settings. We also did not assess insurance coverage gaps and multiple forms of stigma surrounding both HIV and PrEP use that may affect Black women.
Fifth, our focus on Black women in the Southern United States may limit generalizability to other geographic regions or demographic groups. In addition, our analysis did not include geographic-level variables, such as HIV incidence, prevalence, or urban versus rural residence. Future research should explore how these contextual factors influence PrEP awareness and uptake among Black women. Finally, a relatively small sample size for PrEP uptake analysis may have limited the statistical power to detect significant associations, and we cannot rule out unmeasured confounders that might explain the observed relationships.
Despite these limitations, this study’s strengths include a large and experientially diverse sample of Black women from the Southern United States, a population disproportionately impacted by HIV yet often underrepresented in PrEP research. Second, we used the PrEP cascade framework to characterize PrEP use in this population, something that has not been done for Black women in the US South. Third, these findings have direct important implications for PrEP implementation strategies for Black women in the US South. First, the central role of HIV testing suggests that expanding routine HIV testing services and integrating PrEP education into testing encounters could significantly improve the cascade outcomes. Community-based testing sites may be particularly strategic given their accessibility and reduced stigma when compared with traditional clinical settings. Second, health care providers should prioritize PrEP discussions during HIV testing visits, as these represent optimal opportunities for both awareness-building and willingness assessment. Third, the finding that different factors influence awareness and willingness suggests that interventions should be tailored to cascade stages, with broader demographic and trust-building approaches for awareness campaigns and more personalized risk assessment strategies for willingness support. Future research studies should examine the effectiveness of HIV testing-integrated PrEP interventions among Black women. In addition, future qualitative studies could explore how factors such as medical trust and HIV-related worry influence decision-making at different stages of the PrEP cascade. Lastly, longitudinal studies should track individuals through the PrEP cascade to establish causal relationships and identify optimal points for intervention.
In conclusion, PrEP is a highly effective HIV prevention tool, but its full potential remains unrealized because awareness does not always translate to willingness or uptake. Our findings demonstrate that individual, social, and structural factors influence each stage of the PrEP cascade among Black women in the US South. To improve PrEP outcomes, programs and interventions must focus not only on raising awareness but also on ensuring access while addressing the unique barriers at every stage of the cascade. Public health initiatives should actively promote PrEP as a vital prevention option for high-risk populations by integrating it into HIV testing encounters.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number K01MH136935. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health.