
Abstract
New HIV treatment modalities, including long-acting injectable antiretroviral therapy (LAI-ART), increase the range of options available to people with HIV (PWH). As new treatments become available, it is important to understand how PWH perceive these new options and the role of providers in informing patients about them. We explored the perspectives of gay, bisexual, and other men who have sex with men with HIV (MWH) on new HIV treatment modalities and provider communication about these modalities. Semi-structured interviews were conducted with a total of 18 MWH from the US (n = 9) and Australia (n = 9), who were recruited in partnership with two community organizations. Participants identified as gay, cisgender men aged 29–66 years (Median = 54). All reported taking oral ART and having an undetectable viral load. Two main themes were identified: (1) Long-acting injectables are not as simple as daily pills, and (2) Providers should inform patients about new HIV treatments. Most MWH perceived LAI-ART to be more complex compared with their current oral treatment regimen because of frequent clinic visits to receive injections, discomfort with needles, and concerns about missed doses and side effects. MWH believed providers should inform all patients about new treatments and were less likely to do so if they did not have a relationship with their patients, were not satisfied with patients’ current treatment, or were limited on time. Standardizing patient education about new treatments and broadening information channels may enhance informed decision-making among PWH, including those most likely to benefit from new modalities.
Introduction
As of 2022, an estimated 1.2 million people were living with HIV in the US (0.4% of the general population), with gay, bisexual, and other men who have sex with men accounting for about two-thirds. 1 Likewise, in Australia, men who have sex with men account for about 71% of the 30,010 people with HIV (PWH; 0.14% of the general population). 2 Since the late 1990s, the availability and use of effective antiretroviral therapy (ART) have improved the health and quality of life of PWH and prevented HIV transmission. 3 In recent years, HIV treatment options have become increasingly diverse in both their formulations and delivery methods, raising questions about consumer preferences and how individuals stay informed about these evolving options.
Early ART regimens, although effective in reducing AIDS-related deaths, involved complex dosing schedules, adverse effects, and a high pill burden.4,5 Recent pharmacological improvements in ART have aimed to simplify treatment, including the development of potent, tolerable, and safe regimens with more convenient dosing (e.g., from three times a day to twice or once a day).4,5 Long-acting injectable options have been developed to eliminate pill burden, enhance adherence, and alleviate concerns about treatment fatigue. 6 The injectable combination of cabotegravir and rilpivirine (Cabenuva) was approved by regulatory agencies in Australia and the US in 2021 for monthly or bimonthly use by PWH who are virally suppressed on a stable regimen.7,8 Despite this approval, cost remained a barrier in both countries—access to subsidized Cabenuva was limited in Australia until 2022, 9 while insurance coverage concerns persist in the US.10,11 Similarly, a twice-yearly injectable treatment for multi-drug resistant HIV, lenacapavir (Sunlenca), although approved for use in both countries,12,13 is not yet publicly funded in Australia, restricting affordability. 14
As a relatively new form of treatment, research on long-acting injectable ART (LAI-ART) has focused on exploring the perceptions of PWH and their willingness to use it.15–21 Studies have identified eliminating pill burden, improving adherence, reducing social stigma, and increasing privacy and safety as key motivators for using LAI-ART.23,15,16,24,15,16,22 However, among PWH, including gay, bisexual, and other men who have sex with men, the use of needles, potential side effects, and the frequency of clinic visits have been identified as substantial barriers to LAI-ART uptake. 15 Together, these findings suggest that PWH’s understanding, perceptions, and choices regarding LAI-ART involve not only biomedical factors but also broader social and contextual factors. 24
Knowledge plays a key role in shaping interest in or willingness to engage with new HIV treatment options. In a sample of Black sexual minority men in the US South, 96% were aware of LAI-ART, but knowledge levels varied by information source, highlighting the need for high-quality sources and targeted education. 15 In the US, PWH often learn about LAI-ART through commercial advertising and the internet;15,25 whereas in countries like Australia, where direct-to-consumer pharmaceutical marketing is restricted, awareness typically arises through research participation, medical providers, or community campaigns.26–28 Across contexts, health care providers remain key sources of information 29 and collaborators in treatment decision-making. 30
This qualitative study explores the perspectives of sexual minority men with HIV (MWH) in Australia and the US on new treatment forms, including LAI-ART, and health provider communications about these treatments. While both countries have HIV epidemics that are concentrated among gay, bisexual, and other men who have sex with men,1,2 the differences in the two countries’ health care systems provided a valuable basis for comparing how MWH in different settings perceive developments in long-acting HIV treatment and their expectations of clinicians.
Methods
Participants
We recruited a total of 20 MWH in partnership with community-based organizations in Australia and the US between February and June of 2023. Australian participants (n = 10) were recruited by the National Association of People with HIV Australia (NAPWHA), and US participants (n = 10) were recruited by Prevention Access Campaign (PAC). Participants were eligible if they were (a) 18 years or older, (b) able to read and answer interview questions in English, (c) living in Australia or the US, (d) a cisgender or transgender man, (e) sexually active with men in the past 12 months, and (f) living with HIV.
Data collection
We used a purposeful sampling strategy to select prospective participants who could serve as key informants to enhance our understanding of the topic under study. 31 Our partners at the two community organizations contacted prospective participants via email. The emails included a flyer inviting MWH to take part in an interview study about new HIV prevention and treatment options with a link to an online screening survey.
Semi-structured interview guides were collaboratively developed by study team members (M.H., C.T., L.B., T.R.B., B.R.B., and S.K.C.) based on a review of relevant literature and the team’s expertise in HIV prevention and treatment. The current analysis focuses on MWH’s experiences related to their current ART regimen and perceptions of LAI-ART, including patient-provider communication about treatment options. The interview guide also covered patient-provider communication about Undetectable = Untransmittable (U = U) and HIV risk, intersections of HIV service delivery with stigma and equity, and provider training needs. One-hour in-depth interviews were conducted via phone or videoconference by SKC, a White, heterosexual cisgender woman from the US who was the principal investigator of the study. Verbal consent was recorded at the beginning of the interview, and after the interview, participants were asked to complete a brief background questionnaire sent via email. The questionnaire included items related to sociodemographic characteristics, health care, current treatment, viral load status, and recent sexual behavior and injection drug use history.
Participants received a $75 Amazon e-gift card in the currency of their country of residence (AUD or USD) as compensation for their time. The institutional review boards of the University of New South Wales (HC220734) and George Washington University (NCR224429) approved all study procedures.
Data analysis
Interviews were audio-recorded and transcribed. The coding team comprised two US-based research assistants, including D.A.K., a White gay cisgender man. In consultation with S.K.C., D.A.K., and another research assistantread all transcripts and developed an analytical framework guided by the Framework Method. 32 This thematic analysis approach involves a seven-step procedure of transcription, data familiarization, coding, developing an analytical framework, framework application, data charting, and data interpretation. 34 The analytical framework was refined through an iterative process involving D.A.K. and another research assistant independently coding a transcript using NVivo (Version 14; 35), comparing coding, discussing discrepancies, and revising existing codes. Once the analytic framework had been finalized and intercoder reliability established, the remaining transcripts were coded by a single research assistant.
K.C.O., a Black cisgender Nigerian-born US woman, organized the data from each transcript into a matrix using a spreadsheet, categorizing key themes to guide interpretation and identify representative quotations. Other study team members included cisgender men and women of diverse sexual orientations, racial and ethnic backgrounds, and HIV statuses.
Two of the 20 participants, one from Australia and one from the US, did not discuss the topics of new HIV treatment options or patient-provider communication about new options during their interviews and were excluded from the analysis.
Results
Participant characteristics
Of the 18 men in the analytic sample, a total of 15 men (8 from Australia and 7 from the US) returned their background questionnaires reporting sociodemographic and other characteristics (Table 1). The 15 men were aged 29 to 66 years (Mdn [IQR] = 54 [27] years). Over half of the Australian participants were born overseas, and 4 were from a culturally and linguistically diverse background. 33 Most of the US participants identified as non-Hispanic Black/African American. All participants identified as gay, cisgender men, were engaged in HIV care, were receiving HIV treatment, and reported an undetectable viral load. All participants were taking HIV medication as a daily pill, with only one reporting prior use of an injectable—a twice-daily regimen for individuals with resistant HIV.
Sample Characteristics
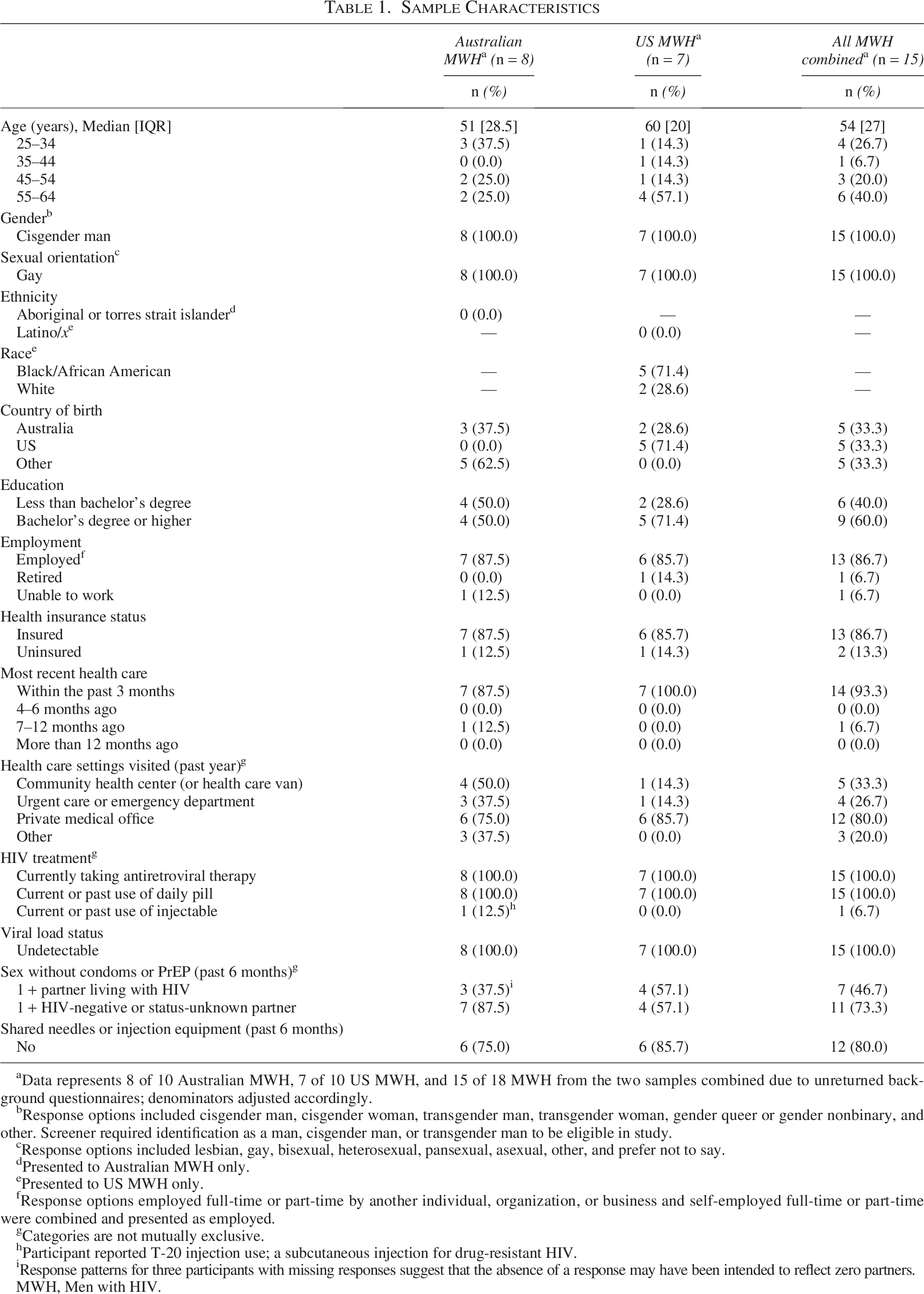
Data represents 8 of 10 Australian MWH, 7 of 10 US MWH, and 15 of 18 MWH from the two samples combined due to unreturned background questionnaires; denominators adjusted accordingly.
Response options included cisgender man, cisgender woman, transgender man, transgender woman, gender queer or gender nonbinary, and other. Screener required identification as a man, cisgender man, or transgender man to be eligible in study.
Response options included lesbian, gay, bisexual, heterosexual, pansexual, asexual, other, and prefer not to say.
Presented to Australian MWH only.
Presented to US MWH only.
Response options employed full-time or part-time by another individual, organization, or business and self-employed full-time or part-time were combined and presented as employed.
Categories are not mutually exclusive.
Participant reported T-20 injection use; a subcutaneous injection for drug-resistant HIV.
Response patterns for three participants with missing responses suggest that the absence of a response may have been intended to reflect zero partners.
MWH, Men with HIV.
Qualitative themes
Two main themes were identified: (1) Long-acting injectables are not as simple as daily pills, and (2) Providers should inform patients about new HIV treatments.
LAI-ART are not as simple as daily pills
Both Australian and US participants generally expressed satisfaction with their current oral regimens, with one Australian participant describing: “It’s simple; I mean it’s one tablet a day.” Given these sentiments, participants from both countries described the perceived inconvenience associated with the use of and adherence to LAI-ART as reasons for a lack of interest in the new treatment option, including required visits to clinics, the mode of administration (injections), and potential side effects.
One participant relayed that both his primary care provider and a specialist had advised him against switching to LAI-ART because of the schedule demands:
I think because of my work schedule. It’d be more convenient to … keep receiving the medication at home, rather than having to schedule an appointment for getting a shot. Being able to get there during the hours that they’re open. [MWH 18, US]
In addition to the restricted hours during which injections might be available, MWH perceived the required frequency of health visits to pose a threat to adherence, particularly given their busy schedules:
I travel a fair bit for work, and so it could be hard to make sure that I’m getting that injection… exactly on schedule. And I think in a way, probably more anxiety about being separated from treatment through, you know, through that process [LAI-ART], rather than, you know, with pills, you can always take an extra bottle of pills. [MWH 13, US]
Given that LAI-ART requires clinic-based administration, most participants perceived the reliance on clinic access as a barrier compared with oral pills. For MWH, this perceived loss of control contributed to feelings of unease, especially in the event of a worldwide crisis such as another global pandemic, as one participant described:
I want to try the shot. But then again, I’m like, what if the world freezes, and I’m not able to get my shot or something, or whatever. Versus, even though I still might not be able to get my pills, maybe I have enough pills leftover or something? I don’t know. It’s just something to think about. [MWH 17, US]
Participants also noted that the frequency of LAI-ART administration was inconvenient because of its incongruence with their current non-HIV medication regimens. For those taking oral medications for other health reasons, oral ART could be better integrated into daily dosing, whereas switching to LAI-ART would introduce a new requirement outside of their daily routines, which some regarded as increasing the mental load—adding another thing that they needed to remember.
While some participants perceived the frequency of LAI-ART administration as inconvenient, others were more concerned with the mode of administration, citing fear of or discomfort with needles. One participant expressed this succinctly:
I don’t like needles. I am needle-phobic. I don’t like having to have my bloodwork done. I don’t. None of that is fun for me. I said [to my provider], “Give me the tablet. I’ m swallowing a pill.” [MWH 11, US]
In contrast, prior experience with needles could be associated with more positive attitudes to LAI-ART. One participant did not see the frequency or mode of administration as a barrier to LAI-ART because he was already taking non-HIV medications in a monthly injectable form:
I am on injectables for other conditions, but not for HIV, so that doesn’t overly worry me. If I moved from a daily tablet to a monthly injection. I am already doing monthly injections… for migraines. So, going on to a monthly injection [for HIV], I am not averse to it. [MWH 1, AUS]
Given the novelty of LAI-ART, some participants had questions about what happened when doses were missed, how missed doses would be managed, and the potential effects of the treatment on the body. To assuage these concerns, one participant said that he would prefer to know about others’ experiences with LAI-ART before trying it:
… I like to wait and watch and see what… people are getting and seeing what their immune system is also doing. Is there a massive swing for a couple of months? Is there you know a big side effect that no one realized? I like to watch. Do they get a boil on the bum at the injection site? These are the things that I want to know before I would try it. [MWH 1, AUS]
Overall, most participants perceived LAI-ART to be less convenient than oral ART. However, a few US participants described LAI-ART as potentially beneficial for PWH who experienced pill fatigue or found the daily pills to be an unwelcoming reminder of their diagnosis. One US participant familiar with LAI-ART described who they believed to be best suited for this treatment:
I think it’s good for some. The part about the injectable is that you can’t miss a shot. Period… I just think this is something that you really have to stay on top of. So, it’s good for some, especially those that want to do that [use LAI-ART]… It stops people from having to remember to take a pill. [MWH 15, US]
Providers should inform patients about new HIV treatments
In the second main theme, both Australian and US participants described how they expected health providers to volunteer information about new HIV treatments to them and other PWH without being prompted by patients. This reflected the patients’ perception of health providers as subject matter experts in HIV care:
I mean it [information about new HIV treatment] has to be coming from the doctors and you know really giving that consumer-centered rights, like what their [patient] options are and you know what works for their [patient] lifestyle, what works for their [patient] circumstances… it has to come from them [providers] because they’re the experts in their field. [MWH 5, AUS]
However, participants believed that providers’ ability and willingness to communicate about new HIV treatment options would be affected by various factors, including patient-provider rapport, provider satisfaction with patients’ current treatment regimens, and time constraints on clinical appointments.
Participants who had an ongoing relationship with their providers trusted their providers to initiate conversations about new HIV treatment options with them. For one MWH with comorbidities, his HIV provider had suggested a change to his regimen:
Once she actually phoned me and said, “I think it’s time we did a change. No reason. We are just trying to get you off this and on to something that’s a little bit healthier for you.” So, [when] she is reluctant to do things because of other [medical] conditions, I know that… she is also proactive, so I have 100% trust [in her]. [MWH 1, AUS]
Another participant shared that although his provider had not initiated a conversation about LAI-ART, in the past, the provider had facilitated a change in the patient’s oral medications:
I was taking something else before, and he said this [oral ART] is better because… this is a better treatment because the other one can upset the kidneys… he keeps track of that pretty closely because I’ve got other issues. [MWH 8, AUS]
Some participants reported that although their providers were aware of new treatments like LAI-ART, as suggested by pamphlets and flyers they had seen in offices and waiting areas, the providers discussed them only when deemed relevant to patient needs. A few participants described this approach as “if it ain’t broke, don’t fix it,” which left patients to advocate for themselves if they wanted to learn about or consider new treatment options. One participant expressed that this attitude may create inequities for those who may be less able to self-advocate due to other structural barriers:
I know that the approach right now is that doctors wouldn’t change a treatment… if it’s just working. I’m not sure if it’s the lack of resources, but maybe it’s that “don’t change anything because it’s working”… which is why I had to really advocate for myself. And not a lot of people have that luxury of advocating for them[selves]… especially… someone who’s a migrant, someone who’s not Medicare eligible… maybe [they] would have a sense of gratitude like… let’s just stick to the treatment because it’s free anyway. [MWH 5, AUS]
Another factor voiced by participants was the limited time with providers. Many felt that appointment times were insufficient to address multiple health concerns, often leading providers to deprioritize discussions about new HIV treatments. One Australian participant, who regularly visited his general practitioner, explained that his comorbidities consumed most of the visits, leaving little opportunity to discuss new treatment options even in extended appointments:
… I have, you know, a few different things going on with me, and routinely I have long appointments, and we usually run out of time for those long appointments. So, we just don’t get around to talking about HIV meds. [MWH 7, AUS]
One US participant noted that having some knowledge about new treatment options would save time during provider visits:
I believe they [providers] are charged to give patients their options. I believe it should always be a collaboration between a doctor or provider and a patient… The doctors I’ve had over the years, I think they appreciate that… because it saves them a lot of time when you’re a little bit knowledgeable. And if they have to tweak it [your knowledge]… it still saves time when you’re knowledgeable, as opposed to just the doctor doing all the work… I think you [patient] should be proactive about your health. Period. [MWH 19, US]
Discussion
This qualitative study examined perceptions of new HIV treatments among MWH in Australia and the United States, and how they communicate about them with their providers. Overall, MWH were satisfied with their current oral regimen, and switching to LAI-ART did not appeal to them. Specifically, participants perceived that visiting clinics to receive LAI-ART would be inconvenient, had fears or concerns regarding needles, and expressed concerns about side effects and missed doses as challenges to switching to the injectable treatment. Participants valued the ability to easily access their oral medications and perceived the clinic-administered LAI-ART as limiting their autonomy and flexibility in treatment access. These findings are consistent with existing literature on barriers to LAI-ART among PWH.34–38 Although none of our participants saw LAI-ART as an appealing option for themselves, a few US participants identified potential benefits of LAI-ART (e.g., alleviating pill burden) that may appeal to other PWH.
In terms of educating PWH about LAI-ART, participants emphasized their health care providers’ role as the primary, trusted source of information about new HIV treatment and the importance of patient-provider communication about this topic. Providers have long been recognized as key sources of medical knowledge, whether serving in the role of counselor or collaborator on a decision.29,30 However, systemic factors (e.g., limited visit times) and interpersonal factors (e.g., patient–provider relationship) shaped participant perceptions of the likelihood of providers discussing new HIV treatments. These factors have been identified in other studies: For example, a study on PWH in a rural Australian setting found that patients who felt their appointments were rushed or lacked thoroughness also considered their general practitioners to be dismissive of their complex health needs, leading to patients feeling less confident about the provider. 39 While the systemic and interpersonal factors identified by participants may depend on the type of provider or health care setting, they nonetheless illustrate the necessity of health provider communication across health systems.
Interestingly, although all participants were asked the same set of questions, most US participants focused on perceptions of LAI-ART, while Australian participants emphasized patient–provider communication. This may reflect differences in awareness of and access to LAI-ART, as well as treatment priorities, even though LAI-ART was approved and available in both countries at the time of the study. These findings suggest that sociocultural factors (e.g., country of residence) and structural factors (e.g., treatment availability) may shape which issues are most salient for and prioritized by MWH.
Our study highlights PWH’s views that providers should initiate conversations about new treatment despite participants’ satisfaction with their current oral regimen and lack of interest in switching to LAI-ART at the time. These findings suggest that patient–provider communications about new treatments remain important, independent of anticipated patient interest or immediate clinical change. Additionally, given system limits on providers’ time with patients, our findings underscore the need for expanding information dissemination about new HIV treatment through multiple channels. With only two countries—the US and New Zealand—permitting direct-to-consumer advertising for prescription drugs, 40 health providers in other countries may face a greater responsibility to proactively address gaps in patient knowledge about new treatments. 41 To further improve knowledge accessibility and availability, particularly for those with less frequent provider visits, public health education, community leaders, trusted peers, and community organizations (e.g., NAPWHA, PAC) can also serve as critical sources of information and support, whether provided in person, online, or via other modalities.42–44 Additionally, leveraging other health professionals, such as pharmacists, may present benefits by increasing opportunities for patient education through more frequent points of contact. 45
Our study should be interpreted in the context of several considerations and limitations. First, we recruited MWH via community organizations, which restricted our sample pool to only those engaged with these organizations. Additionally, our sample was largely composed of men who were middle-aged, gay, and cisgender, all of whom reported taking oral ART and having an undetectable viral load. Due to the qualitative, exploratory nature of the study and our use of a purposeful sampling strategy, findings are not intended to generalize to a broader population. 31 Thus, our participants’ comfort with their current ART regimen and reliable access to care may explain their limited interest in LAI-ART, whereas MWH who are newly diagnosed may be more receptive to alternate ART modalities. Likewise, LAI-ART may appeal to younger individuals with adherence challenges; for example, a study on long-acting ART strategies found that while long-acting oral ART was the preferred method among US youth, long-acting intramuscular injection was perceived as the most efficacious in achieving and sustaining viral suppression. 46
Second, although LAI-ART was approved in both countries, its delayed listing on Australia’s Pharmaceutical Benefits Scheme (which makes it affordable through public subsidy) may have limited exposure to this treatment at the time of data collection. Combined with restrictions on direct-to-consumer advertising, this may have reduced the depth of Australian MWH’s conversations about new HIV treatment modalities. Lastly, the first author, K.C.O., who primarily conducted the analysis, is an HIV-negative US-based researcher with limited pre-existing knowledge of the Australian health care system and the experiences of Australian MWH; however, collaboration with Australian coauthors with decades of advocacy and research experience helped contextualize findings and mitigate this limitation.
In summary, our findings show that compared with oral regimens, LAI-ART was regarded as less convenient by the MWH in our study, highlighting potential challenges to greater use of this new form of HIV treatment. Additionally, many expected to—but did not consistently—learn about new treatments from their providers. These findings are important to situate perceptions of LAI-ART in a fuller context, considering the complexities of individuals’ lives.
With LAI-ART now available in both countries, future research and educational initiatives could focus on promoting awareness and understanding of the full array of treatment options for PWH, particularly PWH who have experienced challenges with oral treatment regimens (e.g., suboptimal adherence, difficulty swallowing pills). Existing evidence suggests that factors such as age, education, mental health considerations, and access to care may be associated with LAI-ART preferences.47,48 Other treatment formulations, such as injectables that require less frequent health center visits or can be self-administered, may offer appealing alternatives in the future for those who find currently available regimens overly burdensome. With respect to improving patient-provider communication, dyadic studies could further illuminate the patient–provider relationship, offering insights to strengthen these interactions and improve communication about new treatment options. In addition, the recent approval of cabotegravir and lenacapavir for PrEP,49,50 presents an opportunity to assess how injectable modalities enhance quality of life for both MWH and HIV-negative gay, bisexual, and other men who have sex with men, and how status-neutral approaches directed to both simultaneously can guide the dissemination of treatment and prevention information.51
Authors’ Contributions
Conceptualization: M.H., C.T., L.B., T.R.B., B.R.B., and S.K.C. Data collection and analysis: K.C.O., M.H., D.A.K., C.T., A.K.J.S., B.R.B., and S.K.C. Article preparation, review, and revision: K.C.O., M.H., D.A.K., C.T., E.C., A.K.J.S., L.B., T.R.B., B.R.B., and S.K.C.
Footnotes
Acknowledgments
The authors thank all the individuals who participated in this study, generously donating their time and sharing their experiences and perspectives. The authors thank Justino J. Flores for coding the transcripts and codeveloping the analytical framework. They also wish to thank their community partners, the National Association of People with HIV Australia (NAPWHA) and Prevention Access Campaign (PAC), who assisted with recruitment and other aspects of the project.
Author Disclosure Statement
C.T. has received speaker fees from Gilead Sciences. B.R.B. and S.K.C. have received honoraria, support for travel expenses, and/or unrestricted research grants directly or indirectly from Gilead Sciences and ViiV Health care. The authors have no other relevant financial or nonfinancial interests to disclose.
Funding Information
This project was supported by funding from a University Facilitating Fund Award and Nick-of-Time Impact Microgrant from the George Washington University to SKC. SKC’s effort and travel were supported by a 2023 Fulbright Future Scholarship from the Australian-American Fulbright Commission as part of the Fulbright US Scholar Program. The Centre for Social Research in Health and The Kirby Institute receive funding from the Australian Government Department of Health, Disability and Ageing. The content of the article, including the views and information presented, is solely the responsibility of the authors and does not represent the George Washington University, Fulbright Program, Institute of International Education (IIE), or Australian or US governments.