
Abstract
Doxycycline postexposure prophylaxis (DoxyPEP) is an emerging strategy to prevent bacterial sexually transmitted infections (STIs) among men who have sex with men (MSM) and transgender women (TGW). We evaluated early DoxyPEP implementation in a university-affiliated infectious diseases clinic providing HIV and pre-exposure prophylaxis (PrEP) care in Durham, North Carolina. This retrospective study included two overlapping cohorts: (1) patients prescribed DoxyPEP through December 31, 2024, to characterize early prescribing and follow-up with contextual clinic comparison; and (2) MSM and TGW diagnosed with a bacterial STI between July 1, 2023, and December 31, 2024, in whom factors associated with DoxyPEP receipt were evaluated using mixed-effects logistic regression. Among 219 patients prescribed DoxyPEP, 41% had a bacterial STI in the preceding year, more frequently among people with HIV (PWH) than PrEP users (51% vs. 30%, p = 0.002). Although PWH comprised 90% of the clinic population, they accounted for 53% of DoxyPEP recipients, signaling disproportionate adoption by HIV status. Among 276 MSM/TGW patients with a bacterial STI during the study period, 26% were prescribed DoxyPEP during a median follow-up of 11 months (interquartile range: 6–14). PrEP use (adjusted odds ratio [aOR]: 11.1, 95% confidence interval [CI]: 2.97–41.2) and encounters after Centers for Disease Control and Prevention guideline release (aOR: 2.46, 95% CI: 1.03–5.83) were associated with DoxyPEP receipt. Recurrent bacterial STI incidence prior to DoxyPEP initiation was 51 per 100 person years. Despite increasing uptake over time, missed opportunities for DoxyPEP prescribing were observed following STI diagnoses, particularly among PWH. Targeted strategies are needed to support integration of DoxyPEP into routine HIV care.
Introduction
Bacterial sexually transmitted infections (STIs) remain a persistent public health challenge in the United States, particularly among people with HIV (PWH) and individuals using HIV pre-exposure prophylaxis (PrEP). Doxycycline postexposure prophylaxis (DoxyPEP), in which a single 200 mg dose of doxycycline is taken within 72 h of condomless sex, has been shown to reduce incident STIs by approximately 60% among men who have sex with men (MSM) and transgender women (TGW) with recent STI diagnoses.1–4 In June 2024, the Centers for Disease Control and Prevention (CDC) issued guidance recommending DoxyPEP for MSM and TGW with a bacterial STI in the prior 12 months and supporting its consideration for others with ongoing STI risk behaviors.
Following the publication of randomized trial data and subsequent CDC guidance, emerging studies of early DoxyPEP adoption in the United States have largely focused on sexual health and PrEP-oriented clinical settings, where uptake has been relatively robust.5–7 However, existing clinical data suggest lower uptake among PWH.8–11 Additionally, national cross-sectional data suggest that there are geographic disparities in DoxyPEP uptake among MSM, with low awareness and use outside early-adopting regions.12,13 Clinically-grounded data on DoxyPEP implementation and uptake in the southern United States, where bacterial STI and HIV incidences are among the highest, remain limited.5–7,9,10,14 In this study, we characterize adoption of DoxyPEP at a university-based HIV and PrEP clinic in the southern United States during an early implementation period spanning evolving clinical evidence and the release of national guidelines. We describe prescribing and follow-up patterns, patient characteristics, and patterns of uptake and nonprescribing following bacterial STI diagnoses in routine clinical care.
Methods
Study design and clinical setting
We conducted a retrospective observational study to characterize early implementation of DoxyPEP in infectious disease (ID) clinics within the Duke University Health System in Durham, North Carolina. HIV and PrEP care are provided across several ID clinic locations within the health system, with care primarily delivered through a hospital-based clinic, annually serving approximately 2000 PWH and 300–350 individuals receiving PrEP. This retrospective study comprised two overlapping but analytically distinct cohorts drawn from the same clinical practice: (1) a DoxyPEP cohort designed to describe early prescribing practices and implementation patterns; and (2) an STI cohort designed to evaluate DoxyPEP adoption following bacterial STI diagnoses and to identify encounters without documented DoxyPEP discussion or prescription among eligible patients. During the study period, there were no formal clinic-wide protocols, electronic health record (EHR) order sets, or systematic prompts for DoxyPEP prescribing. Provider awareness was primarily driven by emerging literature and conference presentations and an Infectious Diseases Grand Rounds presentation on emerging DoxyPEP evidence in late June 2024, coinciding with the release of official CDC guidelines. 15
DoxyPEP cohort
The DoxyPEP cohort included all patients aged ≥18 years who received a prescription for doxycycline intended for postexposure prophylaxis from an ID clinician between May 2022 and December 31, 2024. May 2022 was selected as the start date to capture any early DoxyPEP prescribing following dissemination of preliminary trial results in mid-2022, although the first DoxyPEP prescription from our clinic was not issued until October 2022. Prescriptions were identified using the SlicerDicer query tool within the Epic EHR system (Epic Systems Corporation, Verona, WI) and filtered using discrete dosing variables consistent with DoxyPEP (single 200 mg dose) and keywords such as “sex,” “STI,” “STD,” or “intercourse” in the instructions. All identified prescriptions were manually reviewed and confirmed to represent DoxyPEP by a practicing ID physician.
For patients in the DoxyPEP cohort, we abstracted demographic characteristics, clinical encounter data, and STI laboratory results from the Duke Enterprise Data Unified Content Explorer (DEDUCE) data warehouse. 16 Because EHR-derived gender identity, sexual orientation, and sexual partner data were frequently missing, an ID clinician manually reviewed provider notes, sexual history documentation, and gender identity descriptors for individuals prescribed DoxyPEP. Due to ICD code nonspecificity for PrEP-related care, manual chart review was also conducted to confirm and distinguish between active PrEP use and confirmed HIV infection. Prescription-level characteristics included number of DoxyPEP doses dispensed, number of authorized refills, timing of prescription relative to clinical encounter, and cumulative doses prescribed over follow-up. Follow-up STI testing within 90 and 180 days of initial prescription was also assessed.
To contextualize characteristics of individuals prescribed DoxyPEP, we compared the DoxyPEP cohort to the overall HIV/PrEP clinic population. These individuals were identified by having at least one qualifying HIV or PrEP-related clinic encounter between July 1, 2023, and December 31, 2024, based on ICD-10 diagnosis codes for HIV and HIV prevention. The time frame for this comparison window differs from the full inclusion period for DoxyPEP prescribing to reflect a period of contemporaneous clinical practice following dissemination of DoxyPEP trial evidence, during which DoxyPEP prescribing began to increase meaningfully. Comparisons to the overall HIV/PrEP clinic population were performed solely for contextual framing, not intended to estimate predictors of DoxyPEP receipt.
STI cohort
The STI cohort included MSM or TGW diagnosed with a bacterial STI while receiving HIV or PrEP care between July 1, 2023, and December 31, 2024. This population reflects the inclusion criteria of the DoxyPEP clinical trials and the drafted and official DoxyPEP guidelines by the CDC. 15 The study period was selected to capture early clinical adoption of DoxyPEP following publication of trial results in May 2023 and included time preceding release of official CDC guidance. STI diagnoses were defined as (1) a positive N. gonorrhoeae or C. trachomatis nucleic acid amplification test at any anatomical site (pharyngeal, urine, rectal, and vaginal), or (2) a newly positive Treponema pallidum antibody test or a fourfold increase in rapid plasma reagin (RPR) titer from the most recent available test. The first qualifying STI diagnosis(es) during the study period was designated as the index STI diagnosis. Patients were excluded if they (1) were not identified as MSM or TGW, based on chart review validation; (2) had no clinical encounters on or after the index STI diagnosis date, precluding opportunity for DoxyPEP prescribing; (3) were already prescribed DoxyPEP at the time of the index STI; and (4) had an index syphilis diagnosis determined by chart review to represent a previously treated infection without subsequent STIs during follow-up. Patient demographics, clinical encounter data, and STI laboratory results were abstracted from the DEDUCE data warehouse. Manual chart review was conducted by an ID clinician to validate sexual orientation, gender identity, HIV status, and PrEP use.
Among individuals in the STI cohort, we enumerated all possible opportunities for DoxyPEP prescribing, which was defined as any clinical encounter, including telemedicine encounters, that occurred after the index STI and before the end of the study period. Encounters occurring after a patient had initiated DoxyPEP were excluded from the risk set. An encounter was classified as resulting in DoxyPEP if a prescription was issued on the encounter date or within 7 days thereafter. The cumulative STI count in the prior 24 months was computed on each encounter date using all Duke laboratory data up to the date. Chart review was performed for encounters without a DoxyPEP prescription to document potential reasons for nonprescription (e.g., described abstinence, patient preference, or undocumented).
Statistical analysis
Descriptive statistics were used to summarize prescribing trends, patient characteristics, and prescription patterns in the DoxyPEP cohort, including contextual comparisons with the overall clinic population. Differences in categorical variables between PWH and PrEP users prescribed DoxyPEP were assessed using chi-square or Fisher’s exact tests, as appropriate, and continuous variables were assessed using Wilcoxon rank-sum tests.
For the STI cohort, we compared patient characteristics of individuals prescribed DoxyPEP during the observation period to those who were not prescribed, using chi-square or Fisher’s exact tests, as appropriate. We additionally evaluated patient-level and encounter-level factors associated with receipt of DoxyPEP within 7 days of a clinical encounter using a mixed-effects logistic regression model. A random intercept for a patient accounted for multiple encounters per individual. Pre-specified patient-level covariates included race (Black and White vs. all other races), ethnicity (Hispanic vs. non-Hispanic), HIV status (HIV vs. PrEP), insurance status (Medicare/Medicaid vs. uninsured/self-pay vs. Private/Commercial), care engagement at the time of the index STI diagnosis (initiating vs. established); and encounter-level covariates included encounter timing relative to CDC guideline release (pre-June 2024 vs. post-June 2024) and cumulative number of STI diagnoses in the preceding 24 months.
A Kaplan–Meier curve was generated to illustrate time from the index STI until DoxyPEP initiation, with a log-rank test performed to compare time to DoxyPEP initiation by HIV status. Patients were censored at their last observed ID clinical encounter, reflecting the end of clinical exposure to a DoxyPEP prescribing opportunity.
Among patients in the STI cohort, recurrent STI incidence was calculated using person-time beginning 30 days after the index STI diagnosis to avoid immortal time bias and continuing until DoxyPEP initiation or the end of the study period, whichever occurred first. Recurrent infections were summed across follow-up, and incidence rates were expressed per 100 person-years with exact Poisson 95% confidence intervals.
The Duke University Health System Institutional Review Board reviewed this study and waived the need for informed consent due to the use of existing clinical data. Analyses were performed using R (Version 4.4.3), with statistical significance defined as p < 0.05.
Results
DoxyPEP prescribing over time
The first prescription of DoxyPEP was issued to patients in Duke Infectious Diseases clinics in October 2022, and 219 patients received a prescription by the end of the study period. Prescribing remained infrequent until October 2023, temporally coinciding with the release of CDC’s draft DoxyPEP guidelines (Fig. 1). Thereafter, monthly prescribing increased steadily through 2024, driven primarily by patients who did not have a bacterial STI diagnosis in the previous 12 months.
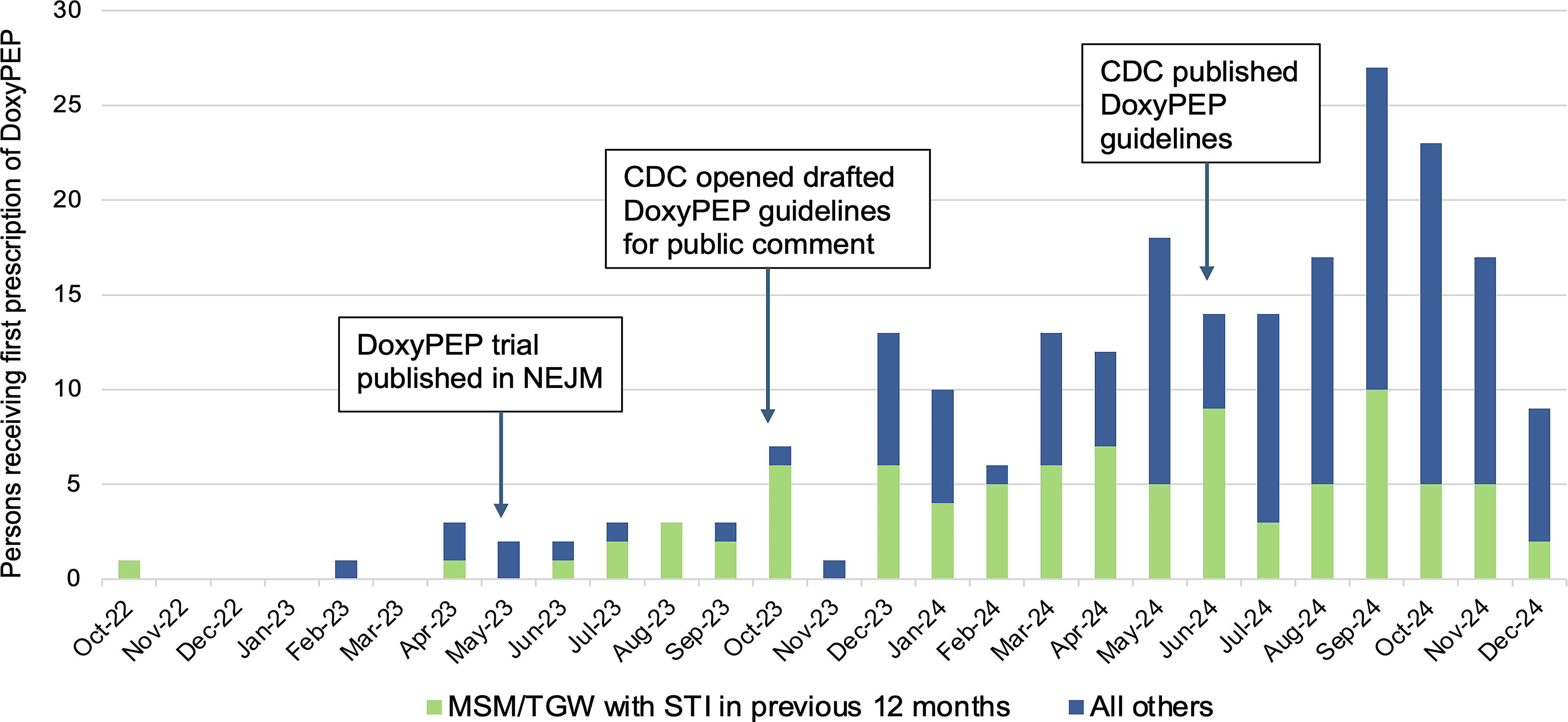
Monthly number of patients receiving a first DoxyPEP prescription, stratified by STI diagnosis in the preceding 12 months. DoxyPEP, doxycycline postexposure prophylaxis; STI, sexually transmitted infection; NEJM, New England Journal of Medicine; CDC, Centers for Disease Control and Prevention.
Characteristics of individuals prescribed DoxyPEP
The characteristics of the 219 patients who were prescribed DoxyPEP are summarized in Table 1. Fifty-three percent of patients prescribed DoxyPEP were living with HIV. Chart-reviewed assessment of sexual orientation and gender identity demonstrated that nearly all patients (97%) prescribed DoxyPEP were MSM, with the remainder including one transgender woman, two individuals assigned female at birth who identified as transgender men or nonbinary, and four heterosexual cisgender men. Forty-one percent of patients receiving DoxyPEP had a bacterial STI diagnosed in the 12 months prior to their first DoxyPEP prescription. Among those with a recent STI, 51% had rectal gonorrhea or chlamydia and 36% had syphilis. In the 24 months before DoxyPEP initiation, PWH had a higher number of STI diagnoses than individuals on PrEP (median 1 [IQR: 0–2] vs. 0 [IQR: 0–1], p = 0.01).
Characteristics of Patients Prescribed Doxycycline Postexposure Prophylaxis Compared with the Overall HIV/Pre-Exposure Prophylaxis Clinic Population
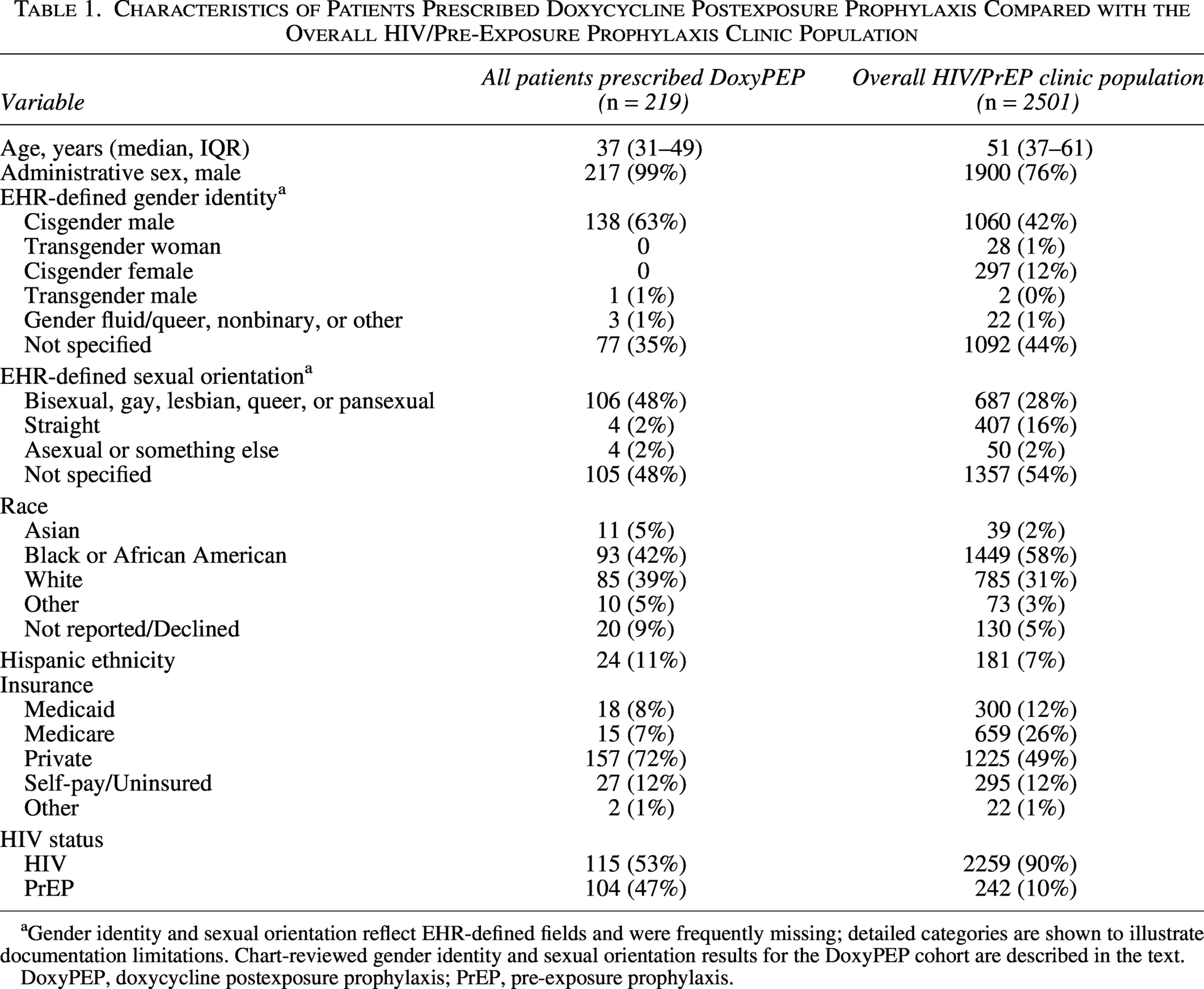
Gender identity and sexual orientation reflect EHR-defined fields and were frequently missing; detailed categories are shown to illustrate documentation limitations. Chart-reviewed gender identity and sexual orientation results for the DoxyPEP cohort are described in the text.
DoxyPEP, doxycycline postexposure prophylaxis; PrEP, pre-exposure prophylaxis.
Contextual comparison with the overall clinic population
For contextual framing, characteristics of patients prescribed DoxyPEP were compared with the overall HIV/PrEP clinic population during the implementation period (Table 1). The overall clinic population (n = 2501) was 76% male by administrative sex, 58% Black, 7% Hispanic, and had a median age of 51 years. About half of the clinic population had missing sexual orientation and gender identity data in the EHR. Compared with the overall clinic population, individuals who received DoxyPEP were younger, more likely to be male, less likely to be Black, and less likely to have Medicare insurance. Notably, although PWH represented 90% of the overall clinic population, they comprised only 53% of individuals prescribed DoxyPEP.
Initial DoxyPEP prescription characteristics
DoxyPEP prescription characteristics are shown in Table 2. Most patients (65%) received an initial prescription for 15 doses with no refills. Eighty-five percent of initial prescriptions were issued on the same day as an HIV or PrEP clinical encounter, and an additional 6% received a prescription within 7 days of such an encounter. Approximately one-third of PrEP users prescribed DoxyPEP received their initial prescription at the time of establishing care in the clinic.
Characteristics of Doxycycline Postexposure Prophylaxis Prescriptions
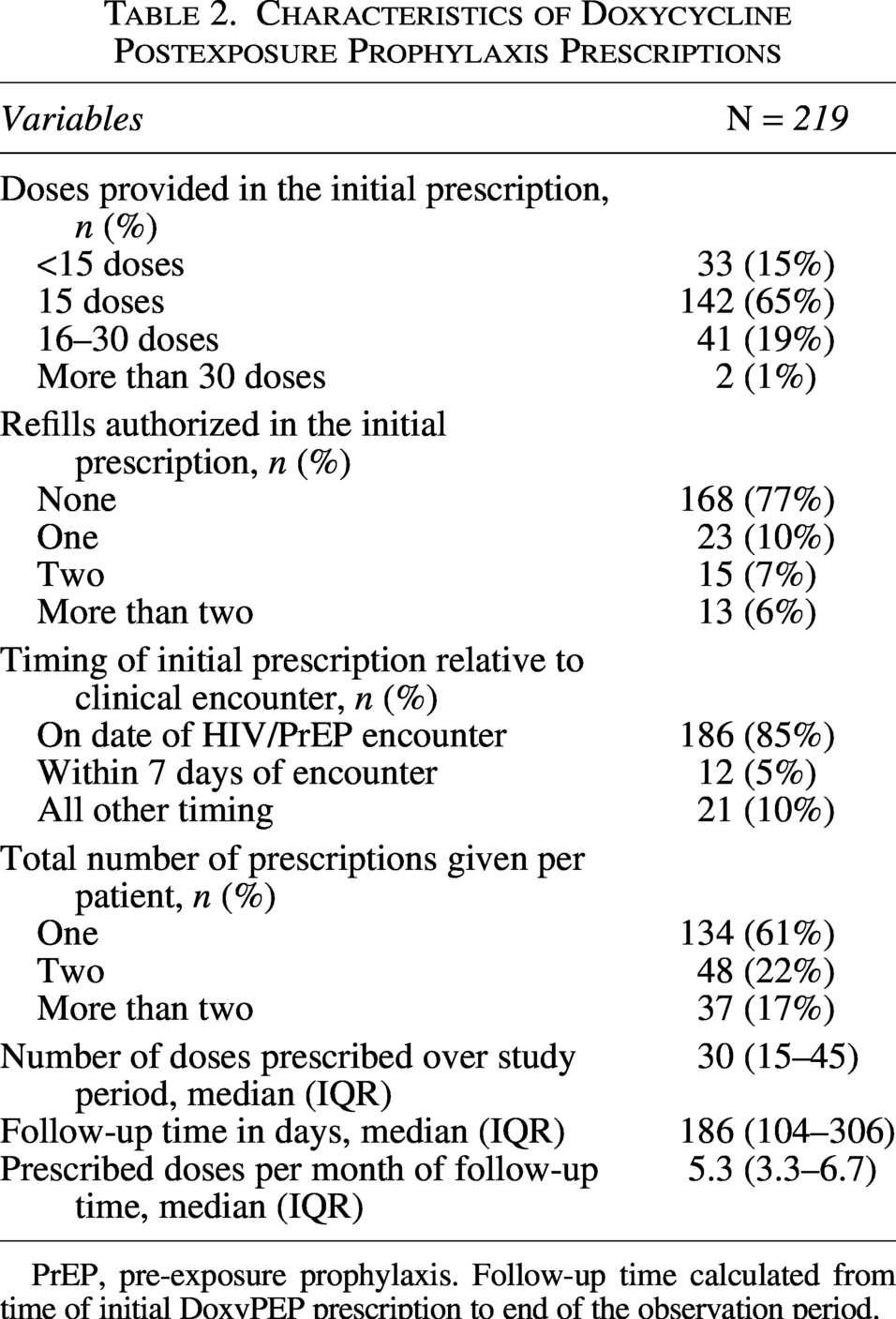
PrEP, pre-exposure prophylaxis. Follow-up time calculated from time of initial DoxyPEP prescription to end of the observation period.
Follow-up after DoxyPEP initiation
Among those initiated on DoxyPEP, 61% received only a single prescription during the study period, 22% received two prescriptions, and 17% were issued more than two prescriptions. The median cumulative number of doses prescribed before the end of the observation period was 30 per person (IQR: 15–45), corresponding to a median of 5.3 doses prescribed per month (IQR: 3.3–6.7).
Among the 173 patients with at least 90 days of observed follow-up after DoxyPEP initiation, 25% had STI testing performed within 90 days. Among 114 patients with at least 180 days of follow-up, 62% received STI testing. STI testing within 180 days was more common among patients taking PrEP compared with PWH (78% vs. 51%, p = 0.006).
Characteristics of the STI cohort
During the study period, 276 MSM/TGW were diagnosed with a bacterial STI, representing approximately 11% of the clinic population (10% among PWH and 21% among PrEP users). These patients had a median age of 34 years; nearly all were MSM, and 66% identified as Black (Table 3). Index STI diagnoses included gonorrhea (40%), chlamydia (38%), and syphilis (34%). Forty-five percent of individuals had more than one bacterial STI in the 24 months prior to inclusion in the cohort.
Patient Characteristics of Sexually Transmitted Infection Cohort by Doxycycline Postexposure Prophylaxis Prescription Status
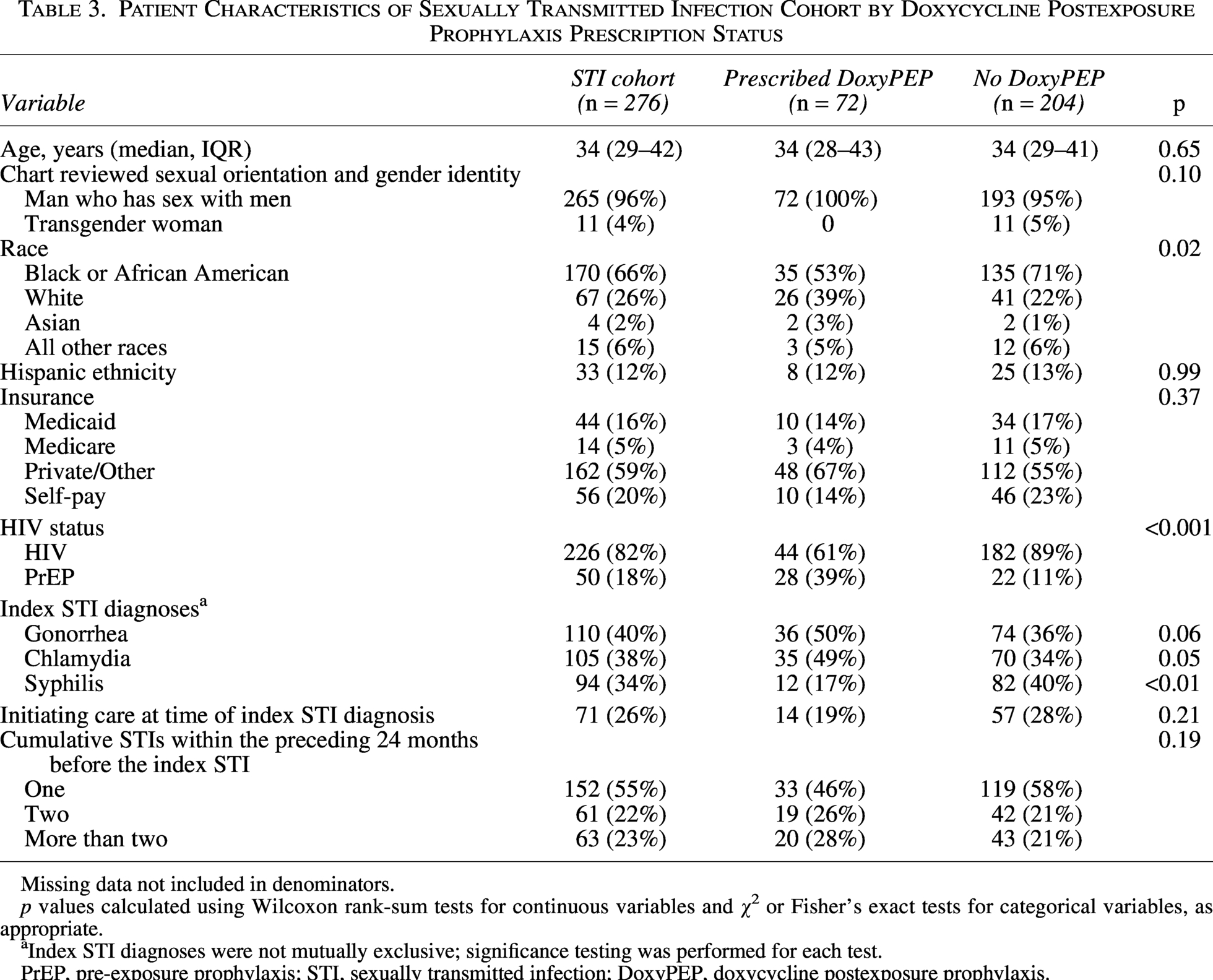
Missing data not included in denominators.
p values calculated using Wilcoxon rank-sum tests for continuous variables and χ² or Fisher’s exact tests for categorical variables, as appropriate.
Index STI diagnoses were not mutually exclusive; significance testing was performed for each test.
PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection; DoxyPEP, doxycycline postexposure prophylaxis.
Likelihood of receiving DoxyPEP among the STI cohort
Among the STI cohort, 72 (26%) were prescribed DoxyPEP during follow-up. When comparing patient characteristics, patients who ultimately were prescribed DoxyPEP were less likely to have HIV, to be of Black race, and to have syphilis as their index STI during the study period.
In an encounter-level mixed-effects logistic regression with a random intercept for patient, PrEP users had 11-fold higher adjusted odds of receiving DoxyPEP compared with PWH (aOR: 11.07, 95% CI: 2.97–41.23; Fig. 2). Encounters occurring after the CDC guideline release were also associated with increased odds of DoxyPEP prescription (aOR: 2.46, 95% CI: 1.03–5.83). Higher cumulative STI burden at each encounter trended toward increased odds of DoxyPEP receipt, though the association was not statistically significant (aOR: 1.29 per additional STI, 95% CI: 0.98–1.69). Other variables, including age, race, ethnicity, care engagement status, and insurance status, were not associated with DoxyPEP receipt when adjusting for other variables, though confidence intervals were wide.
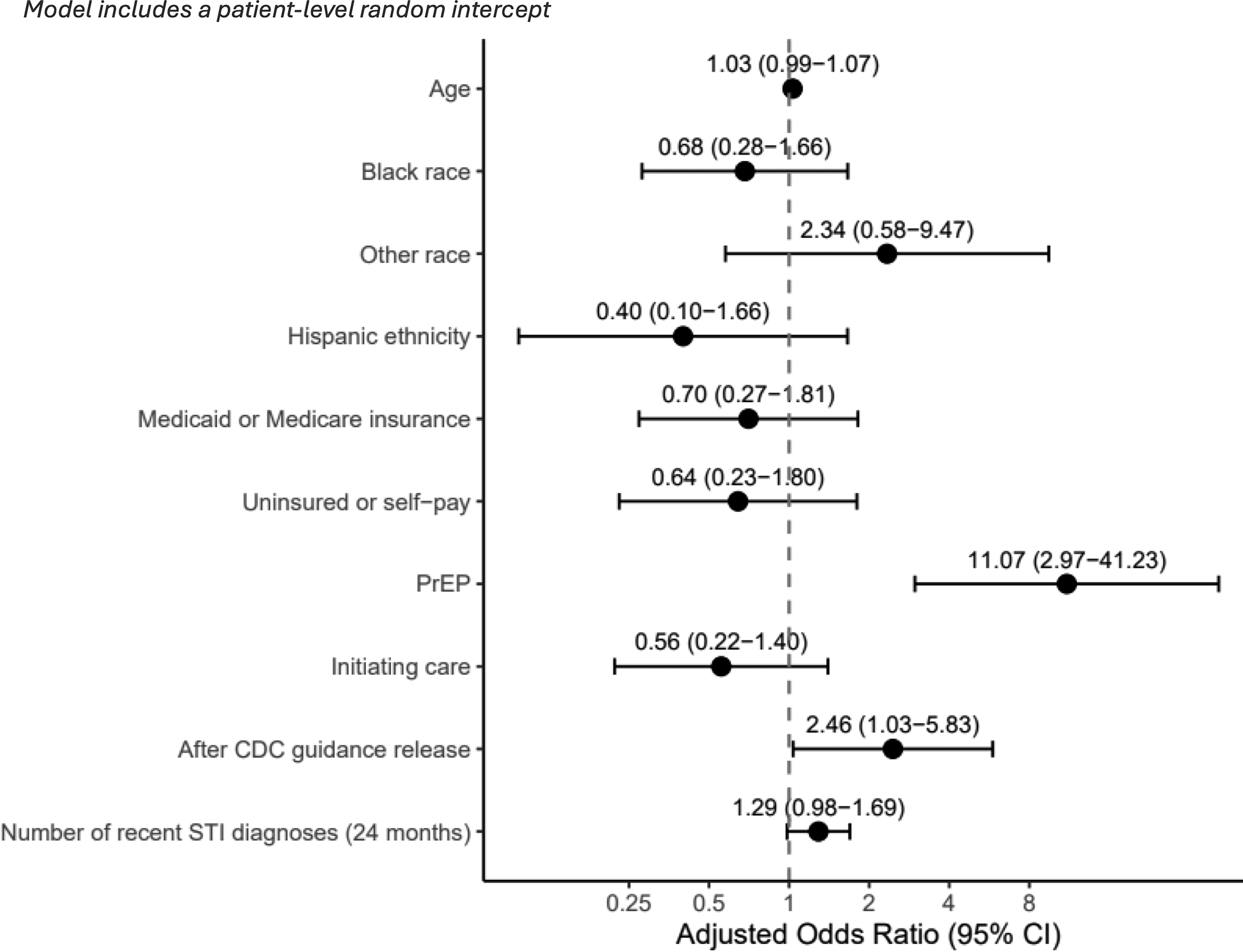
Mixed-effects logistic regression model of factors associated with receipt of DoxyPEP. DoxyPEP, doxycycline postexposure prophylaxis.
Time to DoxyPEP initiation and encounters without DoxyPEP prescription
After an index STI, patients had a median of two clinical encounters and were followed for a median of 189 days (IQR: 20–340) until DoxyPEP initiation or censoring at the last clinical encounter. Among those who ultimately received DoxyPEP, the median time from index STI to prescription was 144 days (IQR: 15–252). Kaplan–Meier analysis demonstrated delayed initiation of DoxyPEP following index STI diagnosis, with substantial differences by HIV status (Fig. 3). One hundred eighty days after the index STI, the estimated cumulative probability of DoxyPEP initiation was 43% (95% CI: 27–57%) for individuals on PrEP versus 13% (95% CI: 7–18%) for PWH (log-rank p < 0.001).
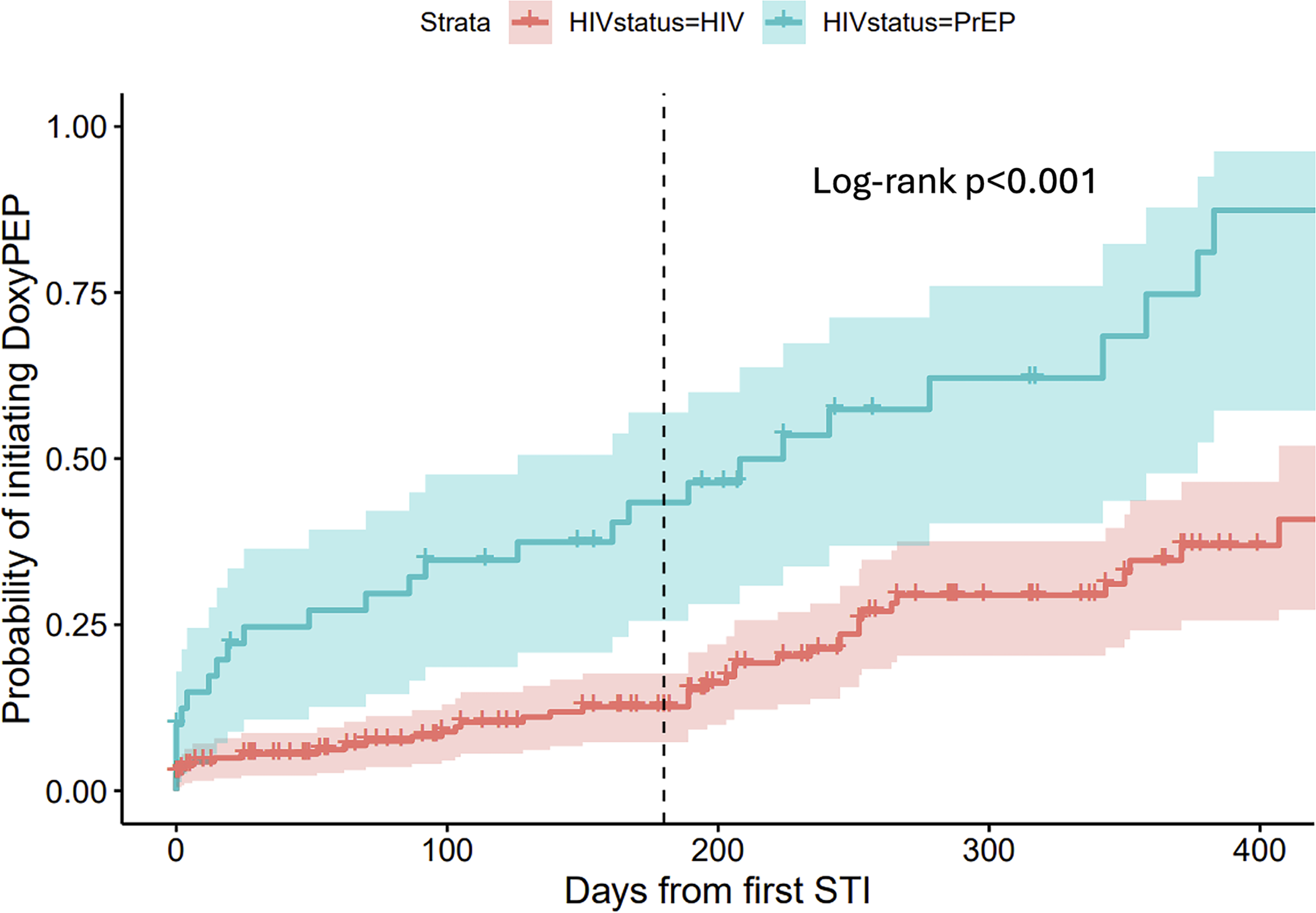
Kaplan–Meier curve showing time from index STI diagnosis to DoxyPEP prescription. DoxyPEP, doxycycline postexposure prophylaxis; STI, sexually transmitted infection.
Only 12% (n = 34) were prescribed DoxyPEP immediately after the index STI diagnosis or before their next clinic visit. Twenty-eight percent (n = 78) did not return for follow-up during the study period. Among 164 patients with at least one follow-up encounter after the index STI, 20 received DoxyPEP at that visit, leaving 144 patients with at least one encounter without documented DoxyPEP prescription after an index STI. Of these, 126 (88%) were PWH.
Reasons for nonprescribing
Among patients with one or more encounters without a DoxyPEP prescription after an index STI, documented reasons for not prescribing were uncommon. Three patients had a documented doxycycline allergy, two had DoxyPEP prescribed by another healthcare provider, and two had DoxyPEP prescribed by an ID provider identified through chart review but not captured in prescription-derived definitions. Current abstinence was documented in 30 encounters (12%), though 74% of encounters contained no documentation of current sexual behavior. Four individuals had documentation of explicitly declining DoxyPEP after discussion with a provider. There were 227 encounters among 126 patients in which there was no documented reason for not prescribing DoxyPEP.
Recurrent STIs after an index STI
Following an index STI, 56 (20%) individuals were diagnosed with a subsequent bacterial STI over a median follow-up of 242 days (IQR: 159–401) until DoxyPEP initiation or study end. This corresponded to an incidence rate of 51 recurrent infections per 100 person-years (95% CI: 41–62). Recurrent STI incidence rates were similar for PWH (50 per 100 person-years, 95% CI: 39–62) and PrEP users (58 per 100 person-years, 95% CI: 34–94).
Discussion
In this single-center study from the southern United States, we describe early real-world implementation of DoxyPEP in an HIV and PrEP clinical setting. Although DoxyPEP prescribing increased after publication of the official CDC guidelines, overall uptake remained modest during this early implementation period. Only one-quarter of patients with a bacterial STI were prescribed DoxyPEP, and fewer than half of those prescribed had a recent bacterial STI, highlighting both underutilization among individuals meeting trial-based eligibility criteria and early adoption among similar populations without recent STIs, especially among those on PrEP.2–4
Beyond overall uptake, substantial heterogeneity was observed in how DoxyPEP was prescribed and monitored in routine clinical practice. Most patients received limited initial quantities and no refills, and it remains unclear whether this reflected individualized risk assessment or variability in provider implementation. While the CDC does not provide guidance on the number of doses to prescribe, a post hoc analyses of the DoxyPEP trial suggest that dispensing 15 doses per 3-month period would provide incomplete coverage of DoxyPEP-eligible exposure events for approximately half of participants. 17 Despite the variability in dispensing amounts, estimated utilization of five doses per month was consistent with prior studies.5,7,10 In contrast, follow-up patterns differed substantially from those evaluated in clinical trials and recommended by the CDC. Only one-quarter of patients underwent STI testing within 90 days, and fewer than two-thirds received testing within 180 days after DoxyPEP initiation. This divergence between evidence-based guidance and real-world clinical practice may influence both effectiveness and antimicrobial resistance monitoring considerations as DoxyPEP is scaled.
A central finding of this study is the high frequency of clinical encounters following an index STI in which DoxyPEP was not prescribed, occurring during a period of early implementation that followed the release of high-impact clinical trial data and spanned 1 year prior to and 6 months after publication of the official CDC guidelines. Only 12% of MSM or TGW patients were rapidly initiated on DoxyPEP after a bacterial STI diagnosis, and many experienced multiple clinical encounters before receiving DoxyPEP, if at all. The interval between the index STI diagnosis and DoxyPEP initiation represents a period of ongoing STI acquisition risk, reflected in the high rate of recurrent STIs observed during this time. In this context, these encounters are critical opportunities for DoxyPEP prescribing, particularly as clinical guidance became more established. Notably, encounters occurring after CDC guideline release were associated with higher odds of DoxyPEP receipt, suggesting that timely uptake of this prevention strategy among eligible patients may continue to improve with provider awareness and integration into routine care.
Encounters without DoxyPEP prescribing after an index STI were most common among PWH. Despite DoxyPEP being a status-neutral intervention supported by similar evidence of effectiveness across both groups, PrEP patients were significantly more likely to receive DoxyPEP following a bacterial STI diagnosis, even after accounting for encounter frequency. Clear clinical contraindications were infrequent, and very few patients declined DoxyPEP when it was discussed, consistent with prior studies demonstrating high patient acceptability of DoxyPEP.9,12,18,19 Several structural and contextual factors may contribute to the lower uptake of DoxyPEP among PWH observed here. One important limitation is that we were unable to fully adjust for provider-level variation in prescribing. More than 30 clinicians cared for patients in the STI cohort, but one high-volume clinician disproportionately provided PrEP care, limiting our ability to disentangle differences in DoxyPEP prescribing by HIV status from provider-level practice patterns. Therefore, the association of HIV status and DoxyPEP receipt likely reflects the combined influence of patient group and provider context in this clinical setting. The findings of relatively low uptake of DoxyPEP among PWH align with other published evidence to date and indicate that implementation efforts should prioritize integration of DoxyPEP into routine HIV care.8,11,20 Given the epidemiological and biological synergy between bacterial STIs and HIV, improving STI prevention among those living with HIV is crucial for broader HIV control efforts.21–23
Additionally, several local contextual factors likely influenced DoxyPEP uptake observed in this study. During the study period, a single division-wide CME presentation on DoxyPEP evidence and CDC guidelines was delivered in June 2024, coinciding with the release of official guidance, and may have contributed to increased clinician adoption thereafter. However, no standardized clinic protocols or coordinated local public health initiatives supported DoxyPEP prescribing during this time. HIV care in this clinical setting is decentralized across a large and diverse group of clinicians, and adoption of DoxyPEP, therefore, likely depended on individual clinician familiarity, clinical focus, and completing priorities during patient encounters. These contextual factors may have contributed to the differential uptake observed between HIV and PrEP patients, where clinical workflows and prevention focus differ. Since completion of this analysis, a standardized DoxyPEP order has been added to clinicians’ preference panels to facilitate prescribing. However, limited structured documentation of sexual orientation and sexual practices within the EHR continues to pose challenges for implementing automated clinical decision support to prompt DoxyPEP prescribing at the time of STI diagnosis.
This study has additional limitations inherent to retrospective analyses using EHR data, including potential misclassification of prescriptions and patient characteristics. Validation of HIV status by chart review was performed for the DoxyPEP cohort and the STI cohort but was not conducted for the overall HIV/PrEP clinic cohort, making some degree of misclassification likely in this reference group. Additionally, thorough documentation of patients’ sexual behaviors was frequently incomplete in the EHR, even with manual abstraction, limiting our ability to determine whether all encounters truly represented appropriate opportunities for DoxyPEP discussion or prescribing.
In summary, understanding how DoxyPEP is operationalized in real-world clinical environments is critical to maximazing its public health impact. Early DoxyPEP implementation in this clinic setting was characterized by increasing but uneven uptake, with several opportunities for DoxyPEP prescribing. Differences in uptake of DoxyPEP by HIV serostatus were particularly notable. Targeted implementation strategies that support providers, standardize prescribing practices, and center equity across HIV status and clinical care engagement will be essential as DoxyPEP is scaled further.
Authors’ Contributions
E.D.N.: Conceptualization, data curation, formal analysis, and writing—original draft. C.M.B., M.M., and J.F.: Conceptualization and writing—reviewing and editing. A.K.: Methodology, supervision, and writing—reviewing and editing. N.L.O.: Conceptualization, supervision, and writing—reviewing and editing.
Ethical Considerations
This study was reviewed and approved by the Duke University Institutional Review Board (approval # Pro00117019).
Footnotes
Author Disclosure Statement
N.L.O. has received consulting fees from ViiV Healthcare and Gilead Sciences. M.M. has research funding from Gilead Sciences, unrelated to the current study. The funder had no role in the design, conduct, or reporting of this work. E.D.N., C.M.B., A.K., and J.F. have no disclosures to report.
Funding Information
E.D.N. was supported by the National Institutes of Health under an institutional training grant (T32AI007392). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.