
Abstract
Homicide defendants asserting the insanity defense make a volatile combination. Numerous studies review inmates with murder convictions, yet the literature is not rich regarding defendants found not guilty by reason of insanity (NGRI) for murder. This study analyzes 27 years of insanity acquittals in Missouri, finding significant differences between those defendants found NGRI for murder and those found NGRI for other crimes. The get-tough-on-crime initiatives found in the criminal justice system may have led to longer hospital stays post-1996 for NGRI murder acquittees, yet hospitalization lengths increased for all NGRI acquittees, a potential unintended consequence. Policy implications and future research directions are discussed.
Introduction
The crime of murder typically arouses harsh sentiments regarding assuring appropriate and just punishment, or assuring that punishment fits the crime. This attitude is consistent even though the number of incarcerated individuals has slightly declined (Glaze, 2010), as has the number of homicides. Starting in 1972, those convicted of homicide in the United States numbered 18,670, peaking in the 1980s to the mid-1990s, with a high of 24,703 in 1991, gradually decreasing to a total in 2009 of 15,241 (Sourcebook of Criminal Justice Statistics, 2009). Consistent with national figures, those convicted of first and second degree murder in Missouri accounted for 8.5% of the total institutional population on June 30, 2004 (Missouri Department of Corrections, 2005), and 8.3% on June 30, 2010 (Missouri Department of Corrections, 2010).
When those accused of murder raise mental health concerns to request lesser sentences, or have a past history of untreated mental illness, it leads to additional controversy and often public outrage. As examples, Mary Winkler, convicted of murdering her husband in Tennessee in 2006, received a sentence to a mental health facility and released after 60 days to public outrage (Bailey, 2007). Cho Seung-Hui murdered 33 people at Virginia Tech in April, 2007 and then killed himself. Subsequent information revealed that he had been deemed dangerous to himself or others as a result of a mental illness but was not committed to a mental health facility (“Officials Knew Troubled State of Killer in 2005,” 2007).
Even greater public outrage ensues when adding the defense of not guilty by reason of insanity (NGRI) as a possibility for a murder suspect. High-profile cases in which defendants attempted this plea, such as John Hinckley, John du Pont, David Berkowitz, Jeffrey Dahmer, Lee Boyd Malvo, and John Salvi III, result in great media focus on mentally disordered offenders. Yet of that list, only John Hinckley was found NGRI, and his case still evokes public outcry when he requests weekend passes from St. Elizabeth’s Psychiatric Hospital in Washington, D.C., where he remains committed. Silver et al. (1994) found public perception to be that 37% of felony indictments yield insanity pleas, with acquittals successfully obtained in 44% of cases. However, contrary to that public opinion, studies have countered that perception, instead finding that the insanity defense is not used on a frequent basis (Perlin, 1994, 2000). The insanity defense is only used in approximately 1% of all felony charges and then is successful in only one fourth of that 1% (Steadman et al., 1993). The majority of offenders successfully pleading insanity become the responsibility of state departments of mental health, not prisons, and public opinion is often that this population has successfully escaped punishment (Brakel, 1988; Steadman, Monahan, Hartstone, Davis, & Robbins, 1982). It is difficult to imagine a population such as those charged with murder and being acquitted as NGRI acting as a greater lightning rod for controversy. Therefore, it is this population at the intersection of the criminal justice and mental health systems that is the focus of the current study.
Literature Review
Whether to have an insanity defense as a plea option in criminal cases is left to each state. The federal government and most states have elected to offer an option to defendants which hold them not responsible for their criminal conduct as they are incapable of forming the necessary criminal intent (Brakel, 1988; Linhorst & Dirks-Linhorst, 1997; Rottman & Strickland, 2006). Once found not responsible, variation exists among the states as to how those NGRI acquittees will be committed to state public mental hospitals (Brakel, 1988; Rottman & Strickland, 2006). Even though a small percentage of offenders use the insanity defense, those NGRI acquittees have a profound effect on the mission and goals of these public mental health facilities, resulting in increased attention to security and public safety (Dirks-Linhorst & Linhorst, 2006; Linhorst & Dirks-Linhorst, 1997). Effects include a long-term commitment by state departments of mental health for facility operation costs, staffing, and public safety considerations. As a result, such public facilities must carefully consider public safety considerations when such an offender is ready for release to the community, and then request the release from a court of competent jurisdiction. This also represents a time commitment, since in excess of 44% of all inpatient long-term care psychiatric beds in the Missouri Department of Mental Health (DMH) are occupied by NGRI acquittees, and in fiscal year 2008, they accounted for 39.4% of the DMH’s inpatient budget, and approximately 19.6% of DMH’s total psychiatric services budget (S. Reeves, personal communication, November 5, 2010). The concept of public safety increases in importance when dealing with offenders found NGRI on a charge of murder, as the public wants to be assured that such acquittees are not released too quickly.
This public concern is replicated in correctional systems. Such systems have dealt with an increasing call for consistent sentencing guidelines to reduce judicial discretion in sentencing. They have also dealt with potential public outrage over the granting of parole, should such a disposition even be an option for the local parole authority due to mandatory minimums (Gross, 2008). Yet some research has found that discretionary release decisions may result in more time spent in prison than for those defendants whose release is mandated (Ireland & Prause, 2005).
In Missouri, defendants found NGRI are indefinitely committed to one of four public psychiatric hospitals, with a level of security matching the seriousness of the committing offense (Dirks-Linhorst & Linhorst, 1994; Section 552.030, Revised Statutes of Missouri [RSMO] Supp. 2009). Many NGRI acquittees are hospitalized for extended periods of time. According to unpublished data, Missouri insanity acquittees under DMH supervision on July 1, 2009 who had remained hospitalized since the time of their NGRI acquittal were hospitalized a mean of 147.7 months (SD = 111.6, Mdn = 130.8) and ranged from less than 1 year to 36 years of continuous hospitalization. Even some NGRI acquittees who had received releases to reside in the community were hospitalized for extensive periods of time prior their first release. Missouri insanity acquittees under supervision on July 1, 2009 who had received conditional releases to reside in the community and who had committed the highest level of felony as a committing offense were hospitalized a mean of 85.2 months (SD = 73.2, Mdn = 67.2), whereas those with lesser offenses were hospitalized a mean of 58.8 months (SD = 62.4, Mdn = 36.0), with hospitalizations ranging from less than 1 year to 32 years. Even with this indefinite commitment, the public maintains a skeptical attitude concerning whether justice has been served in NGRI acquittal cases.
Public opinion can often be reflected in policy and program changes. Beginning in the late 1970s, the American criminal justice system experienced an increase in a get-tough-on-crime approach, fueled in part by public opinion (Stack, Cao, & Adamzyck, 2007). Recent research provides a label for this public perception, calling ours a “law and order culture” (Stack et al., 2007, p. 294). This is further evidenced by the adoption of three strikes legislation, which prescribes stiff penalties for those offenders found guilty of three separate felony offenses, and mandatory minimum sentences in each state (Gross, 2008; Jones & Newburn, 2006). Federal legislation, specifically the Violent Crime Control and Law Enforcement Act of 1994, mirrored such increased punishment requirements (Jones & Newburn, 2006). Goals for such an approach included deterrence messages for those who may commit future crimes, and incapacitation to stop specific criminal offending (Kovandzic, Sloan, & Vieraitis, 2004).
States also have enacted legislation that reflects the tough on crime attitude, including mentally ill offenders. Approximately 12 states have used a plea option known as Guilty But Mentally Ill (GBMI). This finding results in a conviction, but with the expectation that psychiatric treatment be provided in the assigned correctional setting (Melville & Naimark, 2002), although no guaranteed right to treatment exists for this option (Callahan, McGreevy, Cirincione, & Steadman, 1992). When offered, this disposition was intended to offset the public’s concern regarding the insanity defense by acknowledging the potential effects of mental illness on criminal behavior but committing the defendant to corrections and not a state psychiatric hospital. Yet it does not appear to have done so (Palmer & Hazelrigg, 2000). Commitment, in fact, does not have to be to an institution, but instead could be probation (Palmer & Hazelrigg, 2000). Compared with those defendants found guilty, those found GBMI receive longer sentences (Palmer & Hazelrigg, 2000). Contrary to the original intent, research suggests that states enacting GBMI have not seen corresponding reductions in insanity plea numbers (Callahan et al., 1992; Linhorst & Dirks-Linhorst, 1999; Palmer & Hazelrigg, 2000), although those that have also saw a decrease in NGRI acquittals that truly met statutory criteria (Bumby, 1993).
As another example of tough on crime legislative initiatives, in 1996 the Missouri legislature tightened various aspects of Missouri’s NGRI system. Specifically, Missouri statute was changed to require that any release applications for NGRI violent dangerous acquittees be filed in the committing court rather than the probate court of the county in which the DMH facility was located (Section 552.040.10, RSMO Supp. 2009). Second, victims were added to the required notification list for NGRI release applications (Section 552.040.10(2), RSMO Supp. 2009). A third 1996 change added increased testimony requirements for dangerous offenses and several felonies to the list of dangerous offenses (Section 556.061(8), RSMO Supp. 2009). The extra testimony requires that to be eligible for release, the individual “is not likely in the reasonable future to commit another violent crime against another person because of such person’s mental illness,” and that the individual understands “the nature of the violent crime committed against another person,” knows that it was criminal, and can now conform his or her conduct to the law’s requirements (Section 552.040.20, 1 and 2, RSMO Supp. 2009). The length of time allowed for prosecutors’ to object to any release was increased from 15 to 30 days (Section 552.040.5, RSMO Supp. 2009). Prosecutors from committing courts must also receive a written statement of the reasons that a particular placement is appropriate for an NGRI acquittee (Section 630.620.3, RSMO Supp. 2009), and they must receive notice if the individual is to be transferred from one facility to another (Section 632.370.1, RSMO Supp. 2009). The legislation also barred NGRI acquittees from returning to their home state as long as the NGRI commitment endured (Section 630.805.1, RSMO Supp. 2009). All provisions enacted in 1996 remain statutorily required at the current time. A return of release decisions to the committing court, victim notification and more stringent release requirement would, conceivably, allow the original judge, prosecuting attorney, and victims to advocate more effectively against the proposed release of NGRI acquittees into the community. The absconding and subsequent rearrest of an NGRI murder acquittee led, in part, to these legislative changes as well as additional levels of security within the institutions, enhanced risk assessment tools, and a review of treatment modalities.
Given this public and political response to crime, the question arises as to whether the mental health system reflects the same public safety concerns and responses for NGRI acquittees who, but for a successful insanity defense, would have been convicted and sentenced to a correctional setting. Indeed, long lengths of hospitalization for NGRI acquittees can raise issues regarding whether the primary goal of hospitalization is for treatment purposes, or actually reflects punishment (Silver, 1995; Skipworth, 2005). Past research has shown few differences between defendants charged with murder who successfully attempted the insanity defense and those unsuccessful who were ultimately sentenced to a correctional setting. Differences that do exist include that those unsuccessful were more likely to be tried before a jury and have higher IQ scores, while those found NGRI were more likely to have incompetent to stand trial findings before the court (Boehnert, 1989). The research is virtually silent as to differences between NGRI murder acquittees and all other NGRI acquittees.
The Current Study
The current study uses data of 1,130 Missouri NGRI acquittees. Missouri has a relatively high prevalence of NGRI acquittals. The last national study of NGRI acquittals rates found that Missouri ranked sixth among reporting states for frequency of successful insanity pleas to reported crimes (Pasewark & McGinley, 1985). There have been no definitive studies as to why Missouri had such a high ranking to date. Since virtually all such acquittals in Missouri do not occur as a result of jury trials, one can speculate that perhaps agreement among the courtroom work group members resulted in such acquittal rates. This may be based in part on judges and prosecutors’ comfort with the statutory requirement of indefinite commitment and Missouri’s community case monitoring system, which requires monthly contact with the released acquittees. As the restriction of release requirements occurred in 1996, the number of such acquittals has decreased, perhaps in part due to defense attorneys becoming less likely to recommend it as a plea option due to increased length of stay.
The current study focused on three research questions. The first two research questions help set the context for interpreting the third and final research questions.
Research Question 1: What characteristics distinguish NGRI acquittees acquitted of murder and those acquitted of lesser charges?
Research Question 2: What is the relationship between crime severity and commitment to DMH? Specifically, are those individuals who commit murder less likely to be granted conditional releases and unconditional releases, and do those individuals who commit murder reside in a hospital setting for longer periods of time and have longer periods of oversight than those who are acquitted of lesser offenses?
Research Question 3: Did the lengths of hospitalization change for murder and other offenses after passage of the 1996 Missouri statute previously discussed?
Answers to these questions provide additional clarification as to the role of crime severity in release decisions and, more generally, whether the mental health system’s approach to violent offenders followed the get-tough-on-crime prevailing policy. If treatment is the primary goal of NGRI acquittal and hospitalization, lengthened hospitalization of NGRI murder acquittees may not be anticipated. If punishment is a primary consideration, then increased lengths of inpatient hospitalization and a decreased likelihood of successful release may be anticipated. Although there may be additional explanations for longer inpatient hospitalizations, such as new treatment modalities or improved risk assessment instruments, it is likely such innovations resulted from the public demanding additional safety measures.
Method
Sample
A secondary analysis was conducted using a data set of NGRI acquittees made available by DMH. This is the primary data set used by forensic services to record NGRI acquittees information. It is updated as NGRI acquittees enter or leave the system, when they move from hospitalization to supervised community release or when they are rehospitalized. The 1,130 NGRI acquittees constitute all defendants acquitted between fiscal years 1980 and 2007 (July 1, 1979 and June 30, 2007) that were contained in the data set. This data set may omit some NGRI acquittees who were acquitted in the beginning of the fiscal year 1980 but who left the system by unconditional release before 1986 or died before 1995. Given indefinite commitment to hospitalization or community supervision, this number is believed to be small. Criminal offenses for which the 1,130 NGRI acquittees were acquitted included 13.3% for murder, 50.1% for other violent offenses, and 36.6% for nonviolent offenses. Additional descriptive information is included in the Results section.
Variables
Program status
The study included four categories of program statuses. Those hospitalized on June 30, 2007, on supervised release on June 30, 2007, unconditionally released by the criminal courts during the 28-year study period, and other releases from the DMH system during the study period. The other category included death, absconding, transferred to prison, deported, NGRI overturned by the criminal courts, release on a Writ of Habeas Corpus, and reclassified as sexually violent predators.
Demographic variables
Demographic variables included age, gender, race, and marital status. Age was calculated at time of NGRI acquittal. Race was recoded into two groups, White and minority because the number of Hispanic and Native American NGRI acquittees (N = 21. 1.9%) was too small to constitute a separate category. The low population of other races is consistent with census data (1.6% in 1990, and 4.1% in 2000) and Missouri Department of Corrections inmate data (2.4% in 2010; Missouri Department of Corrections, 2010) for the period of the study. Marital status was coded to reflect never married or ever married, with the latter including currently married, widowed, divorced, and separated.
Clinical variables
Clinical variables included psychiatric diagnoses, hospitalization history, and prescription of psychiatric medication. Psychiatric diagnoses were recoded into six discrete categories based on DSM-IV-TR diagnostic numbers (American Psychiatric Association, 1994) for NGRI acquittees who were under DMH supervision on June 30, 2007 and the DSM version that was applicable to the other NGRI acquittees when they left the NGRI system. The categories included psychotic disorders (schizophrenia, schizoaffective disorder, and other psychotic disorders), mood disorders (bipolar disorder, major depression, and other mood disorders), substance abuse (substance dependence and abuse), other Axis I disorders (dementia, sexual disorders, and others); intellectual disability (mental retardation and borderline intellectual functioning), and personality disorders (antisocial personality disorders, personality disorders not otherwise specified, and borderline personality). As most NGRI acquittees had more than one diagnosis, the categories were coded as the presence or absence of each diagnostic category. Hospitalization history was measured in the data set as an ordinal variable with five groups of number of hospitalizations (1 = 0-1 hospitalization, 2 = 2-4 hospitalizations, 3 = 5-9 hospitalizations, 4 = 10-19 hospitalizations, and 5 = 20 or more hospitalizations). Whether clients were taking psychiatric medication was identified, for NGRI acquittees who were under DMH supervision on June 30, 2007, and at the time of exit from the NGRI system for all others.
Crime variables
Crime variables included date of NGRI acquittal, NGRI committing offense, prior criminal history, and county of committing court. Specific crimes were recoded into three categories: murder, other violent offenses, and nonviolent offenses. When defendants were acquitted for one than one offense, the most serious offense was selected for recoding into these categories. The category of murder included first and second degree murder and voluntary manslaughter as defined by Missouri statute. To arrive at appropriate categories of other violent and nonviolent offenses, all Missouri criminal statutes were reviewed, in conjunction with Part I and Part II Index Offense categories set forth in the Uniform Crime Reports. These sources were combined into the three categories. Part I offenses were included in the other violent offenses category, when they matched with Missouri’s definition of dangerous felony in Chapter 556.061(8) (RSMO Supp., 2009). Similarly, Part II offenses were included in the nonviolent offense category. The violent crime category included first degree assault, domestic assault, kidnapping, felonious restraint, elder abuse, vulnerable person abuse, stalking, forcible rape, statutory rape, sexual assault, forcible sodomy, robbery, arson, armed criminal action, resisting arrest, incest, and sexual abuse. The nonviolent crime category included invasion of privacy, child molestation, child endangerment, deviate sexual misconduct, prostitution, causing catastrophe, property damage, trespass, burglary, stealing, receiving stolen property, forgery, bad checks, counterfeiting, harassment, enticement of a child, drugs, bribery theft, identity theft, gambling, possession of firearm, concealed weapon charges, child pornography, obscene material, peace disturbance, hindering prosecution, and other miscellaneous offenses. Prior criminal history was indicated in the database as whether the defendant had a felony conviction prior to the NGRI acquittal. The 115 Missouri counties were recoded into three categories: urban, suburban/small city, and rural. Using Missouri county 2007 population estimates from the U.S. Census Bureau, urban consisted of the state’s two major metropolitan inner cores, suburban included five counties that were either contiguous with the urban center or contained small cities, and rural included the remaining counties (U.S. Census Bureau, 2007). Of the 5,878,415 Missourians in 2007, 17.3% resided in urban areas, 36.1% in suburban areas, and 46.6% in rural areas.
Release variables
The data set included the date of release into the community following the first conditional release after NGRI acquittal and the date of unconditional release, if conditional or unconditional releases were obtained. From these dates, months of first hospitalization were determined by the length of time of NGRI acquittal to first conditional release, months of total commitment to DMH prior to unconditional release determined by length of time from NGRI acquittal to unconditional release. The pre-post statutory change variable used 1996 as the key year.
Data Analysis
To address the first research question, chi-square and ANOVAs were used in bivariate analyses to identify characteristics to distinguish NGRI acquittees acquitted of murder, other violent offenses, and nonviolent offenses. In addition, a multiple logistic regression analysis was used to identify factors associated with acquittal for murder compared with all other crimes when controlling for the effects of demographic, psychiatric, and crime variables. Four analyses were conducted to address the second research question, the relationship between crime severity and conditional release and length of commitment to DMH. First, chi-square was used to analyze differences in rates of conditional and unconditional releases across the three crime categories. Second, ANOVAs were used to analyze differences in mean length of time to July 1, 2007 for those NGRI acquittees who had never been released, time to conditional release, and time to unconditional release across the three crime categories. Third, two multiple logistic regression analyses was used to identify factors associated with conditional and unconditional releases when controlling for the effects of demographic, psychiatric, and crime variables. Fourth, three multiple linear regression analyses were used identify factors effecting the length of hospitalization to July 1, 2007 for those NGRI acquittees who had never been released, the length of hospitalization prior to conditional release, and the length of commitment until unconditional release when controlling for the effects of demographic, psychiatric, and crime variables. The third research question used t tests to determine if lengths of hospitalization were different before and after the 1996 Missouri statute for the separate categories of murder, other violent offenses, and nonviolent offenses.
Missing Data
Three variables contained missing data. Missing data is problematic because it can distort the relationship between variables (Roth, Switzer, & Switzer, 1999). The number of missing values ranged from 5 (0.4%) for felony conviction prior to NGRI acquittal, to 145 (12.8%) for number of psychiatric hospitalizations, to 236 (20.9%) for taking psychiatric medication. The dependent variables contained no missing data. Acceptable levels of missingness are about 10% to 40% (Fox-Wasylyshyn & El-Masri, 2005). Data for the three variables were not missing at random (Saunders et al., 2006). A multiple imputation approach was used to replace missing data. Multiple imputation is a preferred method for addressing missing data and appropriate for studies of murder (Riedel & Regoeczi, 2004). Using the Predictive Analytics SoftWare (PASW) 18 multiple imputation module, five data sets were imputed for each of the multivariate analyses. In each case, all variables included in the logistic regression and linear regression analyses were used to predict missing values, and imputed dichotomous data were rounded (Allison, 2002). Data were pooled using the PASW 18 algorithm for missing data at the univariate combination level. The algorithm uses variations in each of the imputed data sets to arrive at a final pooled statistic and accompanying standard error, effective degrees of freedom, and p value. For the estimated parameter, the algorithm is simply the average of the parameter from each of the five data sets. PASW 18 does not pool together the χ2 or Naglekerke R2. The mean for each of these statistics was calculated from the five imputed data sets.
Results
Characteristics Distinguishing Murder
Several factors distinguished receiving an NGRI acquittal for murder compared with those acquitted for other violent crimes and nonviolent crimes in the bivariate analyses. Among demographic variables, NGRI murder acquittees tended to be older, female, racial minorities, and to have married. Three of six diagnostic categories were associated with NGRI acquittal for murder. NGRI murder acquittees were less likely to have other Axis I disorders, personality disorders, or intellectual disabilities. NGRI murder acquittees also had fewer prior psychiatric hospitalizations. Four clinical variables were not associated with NGRI acquittal for murder. These included being diagnosed with a psychotic disorder, a mood disorder, or a substance abuse disorder, and taking psychiatric medication. Finally, both crime variables were associated with NGRI acquittal for murder. NGRI murder acquittees were more likely to have been acquitted in an urban county and less likely to have a felony conviction prior to the NGRI acquittal. See Table 1 for additional information.
Characteristics of NGRI Acquittees Acquitted for Murder and Lesser Charges
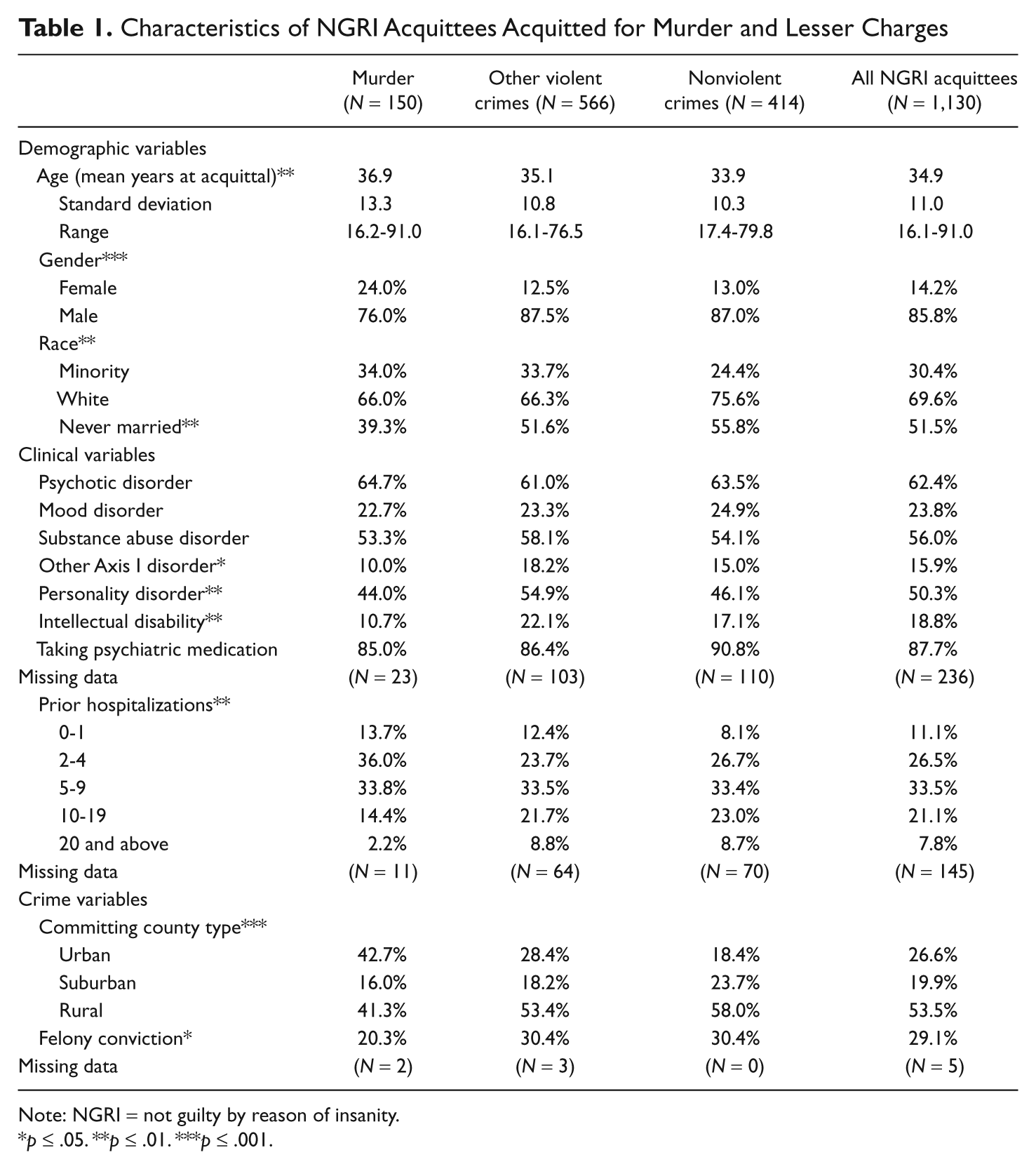
Note: NGRI = not guilty by reason of insanity.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Factors associated with an NGRI acquittal for murder compared with all other crimes were also identified through a logistic regression analysis. When controlling for the effects of the other variables, five factors were associated with a murder acquittal. Being female and being acquitted in an urban county compared with a rural county increased the odds of a murder acquittal, whereas being never married, being diagnosed with an other Axis I disorder, and having greater numbers of psychiatric hospitalizations decreased with odds of acquittal for murder. Additional information is included in Table 2.
Multiple Logistic Regression of Factors Associated With NGRI Acquittal for Murder
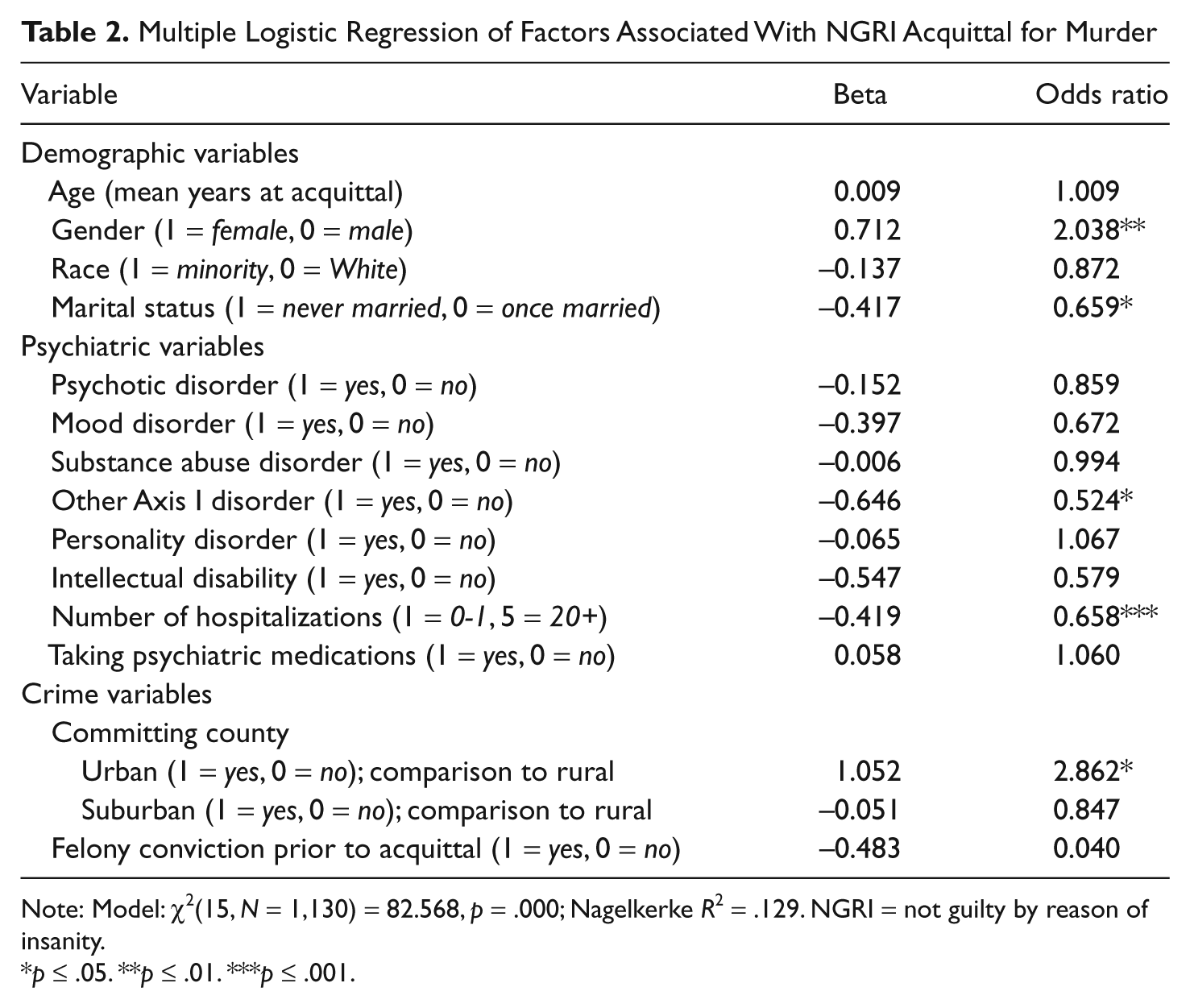
Note: Model: χ2(15, N = 1,130) = 82.568, p = .000; Nagelkerke R2 = .129. NGRI = not guilty by reason of insanity.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Crime Severity and Commitment
NGRI murder acquittees were less likely to obtain conditional releases than NGRIs acquitted for other violent crimes and nonviolence crimes (68%, 73.5%, and 89.5%, respectively, p = .000). Likewise, NGRI murder acquittees were less likely to obtain unconditional releases (15.3%, 21.6%, and 31.4%, respectively, p = .001). These findings held even when controlling for demographic, psychiatric, and other crime variables in logistic regression analyses. Compared with NGRI murder acquittees, the odds of conditional release increased 1.7 times for those acquitted for other violent crimes and increased 5.4 times for those acquitted of nonviolent offenses. Similarly, compared with NGRI murder acquittees, the odds of unconditional release increased 2.3 times for those acquitted of other violent crimes and increased 4.0 times for those acquitted of nonviolence offenses. See Table 3 for additional information.
Multiple Logistic Regression of Factors Associated With Conditional Release and Unconditional Release
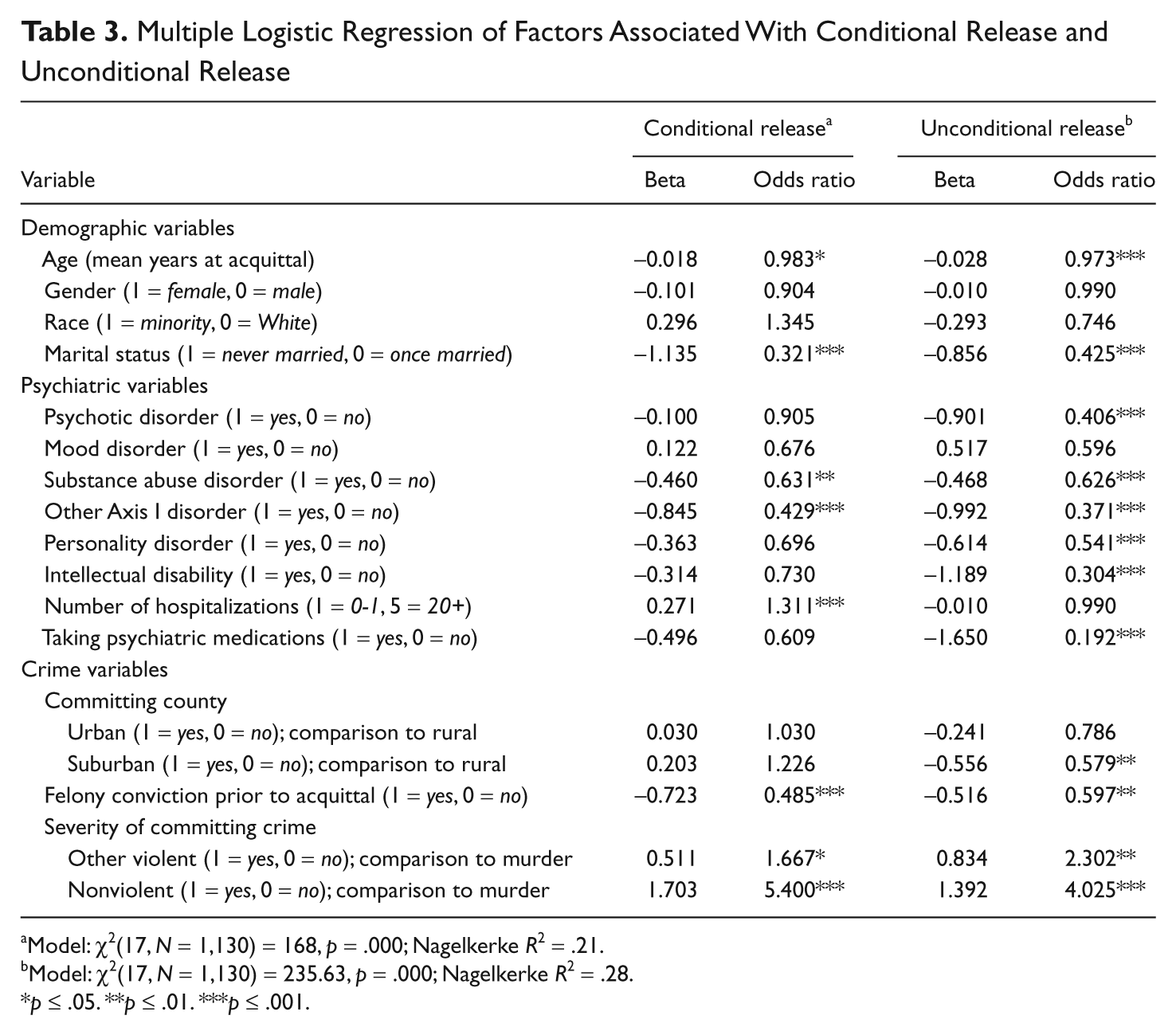
Model: χ2(17, N = 1,130) = 168, p = .000; Nagelkerke R2 = .21.
Model: χ2(17, N = 1,130) = 235.63, p = .000; Nagelkerke R2 = .28.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
The effect of crime severity on length of commitment, rather than the release decision, was less clear. Among NGRI acquittees who had been conditionally released, NGRI murder acquittees were hospitalized substantially longer than those acquitted of other violent offenses or of nonviolent offenses (72.9 months, 49.0 months, and 35.1 months, respectively). Among NGRI acquittees who had been hospitalized continuously since their acquittal without conditional or unconditional release, the length of hospitalization did not vary across the three crime categories. Similarly, months of total commitment to DMH prior to unconditional release did not vary across the three crime categories. See Table 4 for additional information. Similar findings resulted when controlling for other factors in multiple linear regression analyses in which the three time periods served as dependent variables. For NGRI acquittees who had been granted conditional releases, acquittal for other violent crimes reduced the mean number of months of hospitalization prior to first conditional release by 27.8 months compared with murder acquittees and was reduced by 39.2 months for those acquitted of nonviolent offenses compared with murder acquittees. Among NGRI acquittees who had been hospitalized continuously since their acquittal without conditional or unconditional release, those acquitted for nonviolent crimes were hospitalized 31.5 months longer than those acquitted of murder, the opposite of what would be expected. Among NGRI acquittees granted unconditional release, crime severity did not affect the length of time to unconditional release. See Table 5 for additional information.
Mean Months of Commitment by Severity of Committing Crime
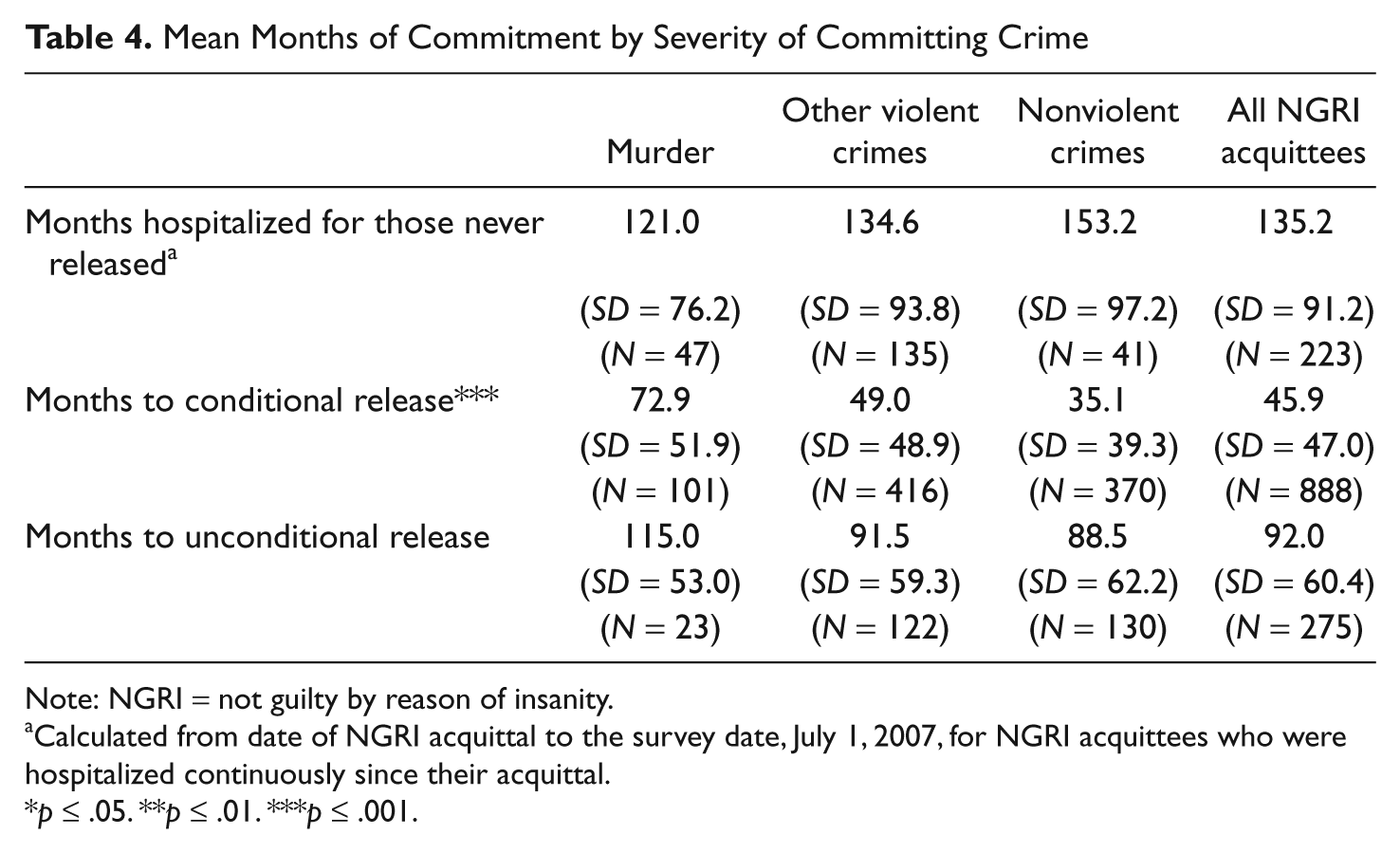
Note: NGRI = not guilty by reason of insanity.
Calculated from date of NGRI acquittal to the survey date, July 1, 2007, for NGRI acquittees who were hospitalized continuously since their acquittal.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Multiple Linear Regression of Months Continuously Hospitalized for NGRI Acquittees Never Released, Months Continuously Hospitalized Until First Conditional Release, and Months Under DMH Supervision Until Unconditional Release
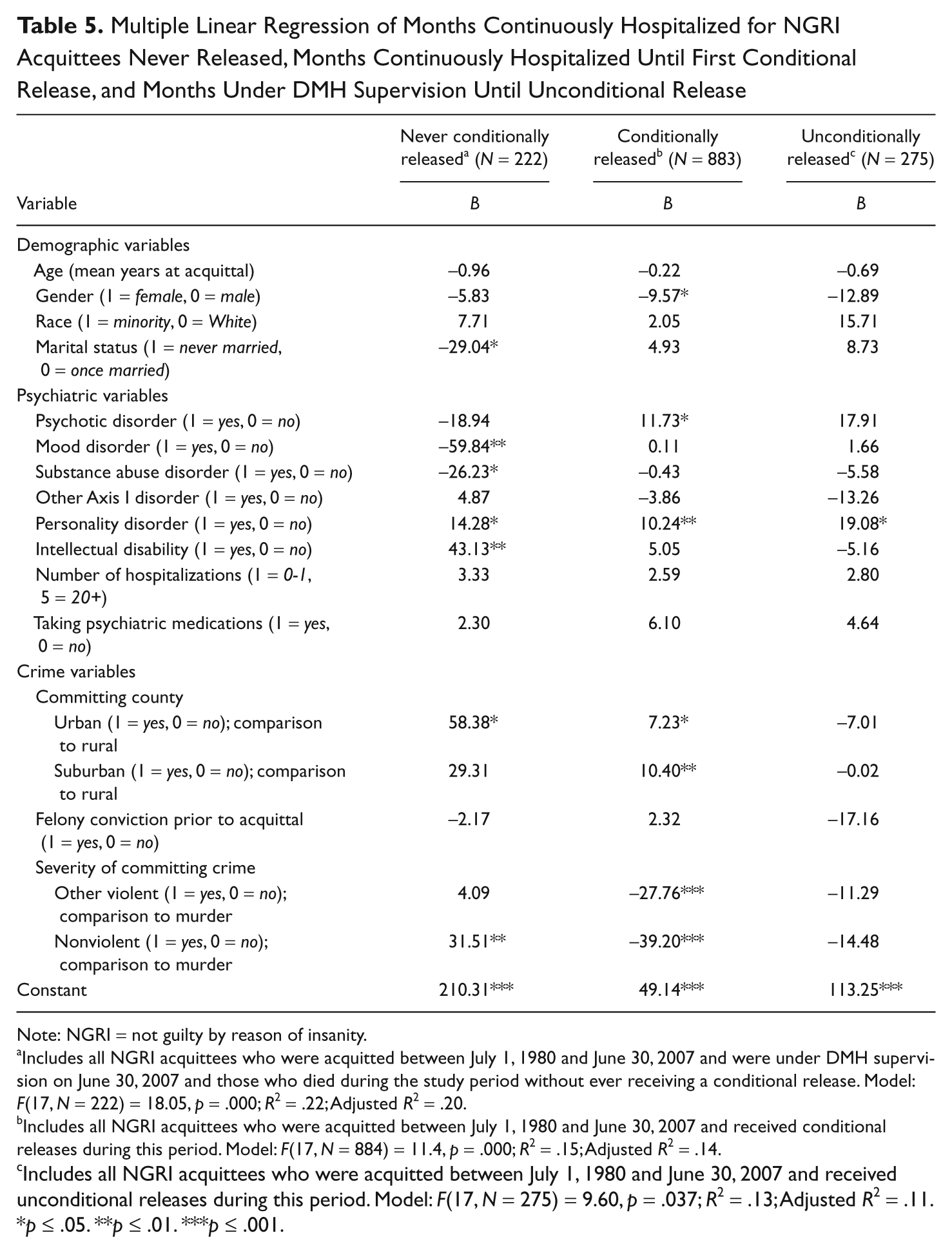
Note: NGRI = not guilty by reason of insanity.
Includes all NGRI acquittees who were acquitted between July 1, 1980 and June 30, 2007 and were under DMH supervision on June 30, 2007 and those who died during the study period without ever receiving a conditional release. Model: F(17, N = 222) = 18.05, p = .000; R2 = .22; Adjusted R2 = .20.
Includes all NGRI acquittees who were acquitted between July 1, 1980 and June 30, 2007 and received conditional releases during this period. Model: F(17, N = 884) = 11.4, p = .000; R2 = .15; Adjusted R2 = .14.
Includes all NGRI acquittees who were acquitted between July 1, 1980 and June 30, 2007 and received unconditional releases during this period. Model: F(17, N = 275) = 9.60, p = .037; R2 = .13; Adjusted R2 = .11.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Effect of 1996 Statutory Change
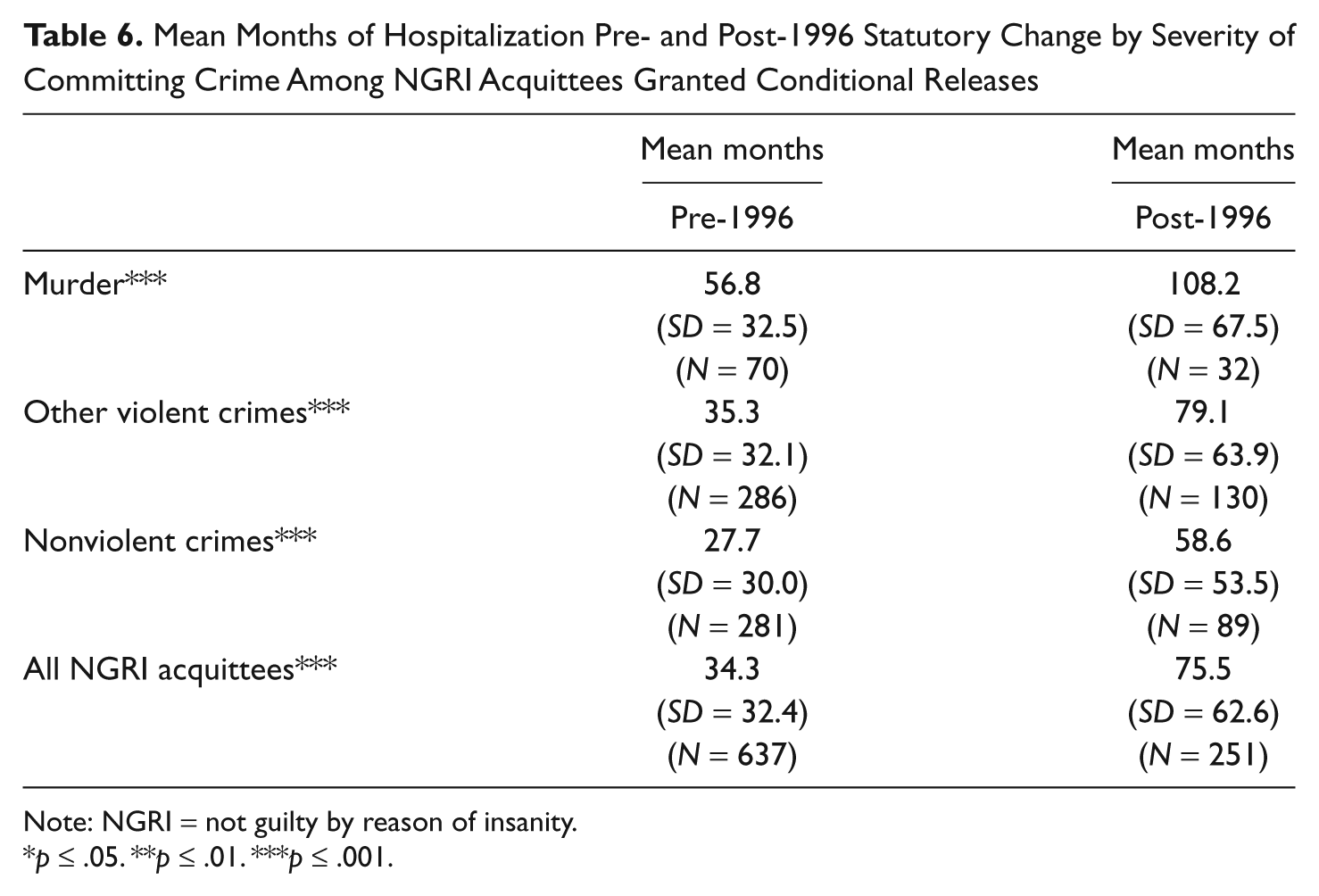
To determine whether the mental health system mirrored the criminal justice system’s tough on crime stance, lengths of first hospitalization were measured to determine if NGRI murder acquittees remained on an inpatient status longer before or after the 1996 law change for those NGRI clients who were granted a conditional release. NGRI murder acquittees were hospitalized, on average, much longer after the law change, increasing from a mean of 56.8 months to a mean of 108.2 months. However, lengths of hospitalization increased similarly for the other two crime categories as well. Table 6 has complete hospitalization information.
Mean Months of Hospitalization Pre- and Post-1996 Statutory Change by Severity of Committing Crime Among NGRI Acquittees Granted Conditional Releases
Note: NGRI = not guilty by reason of insanity.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Discussion
A total of 13% of the entire NGRI acquittee study population had murder as the committing offense. This percentage is consistent with Cirincione, Steadman, and McGreevy’s (1995) research finding murder as the charge in an average of 14% of NGRI cases across seven states. Not unexpectedly, there were differences when comparing NGRI murder acquittees with those acquitted of all other offenses. They were older, and typically married at some point in their life, although for NGRI murder acquittees they are overwhelmingly more likely to be widowed as their potential victim may have been their blood relative or spouse (Nestor & Haycock, 1997). This may be consistent with those convicted of murder and sentenced to corrections, as more than 50% have a nonstranger victim (Fox & Zawitz, 2007). However, homicide offenders in corrections had the mean age of offending at 26.4 (Fox & Zawitz, 2007), so the NGRI population at 36.9 years of age is a decade older.
NGRI murder acquittees were proportionally more likely to be female. However, when reviewing committing offenses in the correctional population, females committed murder at a rate of 1.3 per 100,000 people compared with 11.5 per 100,000 for males (Greenfeld & Snell, 1999), a trend consistent from 1976 through 2005 (Fox & Zawitz, 2007). NGRI female murder acquittees do not reflect that rate. Compared with offenses for all female offenders in correctional settings, generally the number of murders committed has decreased, accounting for 11.8% of all sentenced prisoners under state jurisdiction at year end 2008 (West, Sabol, & Greenman, 2010), and for 7.5% of females within Missouri’s Department of Corrections (DOC) institutions on July 1, 2006 (Missouri Department of Corrections, 2007). Yet murder accounts for 22% of female NGRI acquittees in Missouri. This is consistent with past research including female NGRI acquittees (Breheney, Groscup, & Galietta, 2007; Hodgins, Hebert, & Baraldi, 1986). In 1993, Perlin and Dorfman (1993) contended that legal decision making can be, among other attributes, sexist when deciding mental health related cases. The current result may support that contention. If the public and the judiciary believe the insanity defense is a lesser disposition, then the idea that women are more favorably treated in sentencing (Young & Reviere, 2006) may be reflected in the disparity of correctional female murder statistics compared with NGRI female murder acquittees. If so, almost 20 years later, Perlin and Dorfman’s challenge to recognize such decision-making flaws may have failed. In addition, theories as to exactly why women commit murder have been the subject of much research, albeit with a multitude of results or perspectives (Grana, 2002; Isser & Schwartz, 2008), though very little of the research has included NGRI female murder acquittees. Potential system and/or gender bias should continue to be a research focus.
Clinically, there was no difference between the NGRI murder acquittees and other NGRI acquittees when comparing psychotic disorders or mood disorders (such as schizophrenia, bipolar, or major depression), substance abuse disorders, or other Axis I diagnoses (such as dementia or sexual disorders). This may reflect that the seriousness of the mental illness was in fact considered in assessing whether all acquittees met the statutory test for an NGRI acquittal, not solely a consideration for murder acquittees. NGRI murder acquittees had fewer prior psychiatric hospitalizations when compared with all other acquittees. It is uncertain how, or why, the number of prior psychiatric hospitalizations affect such NGRI acquittals. Again, as the vast majority of insanity acquittals do not occur in jury trial settings, the importance of such factors, or the lack of such importance, to courtroom work group members is unclear. One potential explanation may be that such successful murder acquittees have failed to seek mental health treatment prior to the committing offense, thereby being unknown to the mental health treatment system. Without treatment, the symptoms may have exacerbated, resulting in a more serious offense. This explanation, of course, is speculative. Although few reasons immediately present, this area should be recognized for future research.
An analysis of crime variables in the bivariate analysis found that those acquitted of murder were less likely to have a prior felony conviction. This may indicate that an individual who has been found guilty prior to the current crime may have a higher burden to show that he or she did not know right from wrong based on past interactions with the criminal justice system. Just as the public has, at least, expressed limited support for considering criminal history as part of the sentencing in the criminal justice system (Roberts, 1996), judges, prosecutors, and juries may use such information in NGRI defense decision making. It should be noted that this finding did not hold when controlling for other factors in the multivariate analysis.
NGRI murder acquittees were also less likely to have obtained a conditional release, so it may be that their symptoms take longer to either resolve or control; that the seriousness of the offense results in a more cautious or tempered approach when considering release decisions, with NGRI murder acquittees being required to demonstrate longer periods of psychiatric stability and nondangerous behavior; or that an immediate admission to maximum security, not required for most other crime categories, may result in an increased length of stay. This finding appears consistent with previous research concluding that crime seriousness did affect length of stay to conditional release (Silver, 1995). They were also less likely to obtain an unconditional release, which is consistent with prior research on Missouri’s NGRI population (Linhorst, 1999). However, an interesting finding emerged that nonviolent acquittees who had never obtained any release, compared with murder acquittees, were hospitalized longer. Mental illness severity is a possible explanation for this finding.
Race was not a significant factor between the two NGRI acquittee study populations when controlling for other variables in the multivariate analysis. This was true even though urban locations were a significantly higher NGRI murder acquittal referral source. African Americans represented approximately 50% of the population in the St. Louis City as recently as 2009, (McKinnon, 2001; U.S. Census Bureau, 2009), and 28% of Kansas City’s population (City-Data.com, 2009). This result may also be inconsistent with trends in homicide perpetrators in the correctional system, which has seen African Americans overrepresented in that crime category for at least 30 years (Fox & Zawitz, 2007), homicide numbers in large cities decline (Duhart, 2000; Fox & Zawitz, 2006), and higher rates of murder charges among African American defendants when compared with Whites (Krivo & Peterson, 2000; Phillips, 1997). A possible explanation for this inconsistency may be that proportionally a smaller number of African American defendants are successful in claiming the insanity defense, but that data are beyond the scope of the current study.
After reviewing the differences between NGRI murder acquittees, and all other acquittees, the issue of whether those differences were reflected in increased length of stay for the murder acquittees. As get-tough-on-crime initiatives single out more serious offenders, with arguably increased criminogenic factors, one may speculate that lengths of stay for NGRI murder acquittees would have increased. Even with the differences as outlined within the NGRI acquittees, the results suggest a much broader potential impact from the get-tough-on-crime era.
The mean time for NGRI murder acquittees to obtain a conditional release did increase when comparing the pre- and post-1996 statutory change, but more importantly, it increased for all three crime categories. It may not be the law change itself that can be linked to increased length of stays, but the increasingly conservative get-tough-on-crime attitudes that led to the creation of laws of that nature, and the corresponding public attitudes that account for increased lengths of stay for all NGRI acquittees. Even though increased lengths of stay could be attributed to increased security levels, new treatment modalities, or enhanced risk assessment instruments, the rationale for initiating many such programs is often public demand for accountability and increased safety, similar to the impetus for tough on crime initiatives. It appears that although the get-tough-on-crime approach may not have had the intended punitive effect on correctional sentencing practices (Jacobson, 2006; Stolzenberg & D’Alessio, 1997), albeit the possibility of a potential modest deterrent effect for homicide rates (Chen, 2008; Kovandzic et al., 2004), it has affected, perhaps as an unintended consequence, those defendants that mount a successful affirmative defense of insanity and are indefinitely committed to one of Missouri’s public psychiatric hospitals, as well as affecting all such acquittees, not simply those acquitted for murder.
A potential future research direction may be to apply restorative justice principles to victims of NGRI murder acquittees, as it is used in death penalty cases (Eschholz, Reed, Beck, & Leonard, 2003). It may provide an improved opportunity for understanding on the part of the victim’s family, and the NGRI acquittee’s family as well, and may improve release transitions. However, public support will most likely be limited for such an approach for offenses at the level of murder (Roberts & Stalans, 2004), if it is perceived that it will help defendants escape responsibility or accountability.
Another future research direction should focus on whether states begin to refine insanity statutes that require lengthy or indefinite hospital commitments postacquittal given decreasing state operating budgets, in the same pattern as those states who may reconsider three strikes legislation due to skyrocketing operating costs, as have Mississippi and Louisiana (Chen, 2008; Jacobson, 2006; Kovandzic et al., 2004). This is an important line of research as a critical component of such commitments is the release process. Although states do vary in the statutory release mechanism for NGRI acquittees, a review of all states’ NGRI acquittee release processes finds them grouped in three broad categories. First, some use civil commitment criteria for release; next, some states allow release from indefinite commitment only by judicial review and order; and finally, some states require that the NGRI commitment last only so long as the length of sentence the acquittee would have received had they been incarcerated (Linhorst & Dirks-Linhorst, 1999). Briefly, civil commitment criteria mandates that ongoing hospitalization is conditioned on, typically, imminent harm to self or others. This litmus test is traditionally not interested in crime severity or past psychiatric history, but instead periodically reviews the acquittee’s current mental status and propensity for harm. Whenever the imminent harm test is not met, release occurs. Indefinite commitment is viewed as more restrictive than tests using civil commitment criteria, and studies have found longer hospitalization times as a result (Linhorst, 1997).
As governmental budgets continue to decrease, states that use the first two release methodologies may want to consider that measures to tighten the release for NGRI murder acquittees may actually result in longer hospitalization length for all such acquittees. This is a possible unintended consequence, but one with monetary ramifications. They may wish to compare the NGRI murder acquittees to their correctional counterparts to determine that the application of sentencing guidelines utilizing correctional sentence lengths may in fact offset public safety, while not affecting the lengths of stay of all other NGRI acquittees. Further analysis could determine the cost benefit of such policy changes.
As murder tends to be the crime associated in the public’s mind with the insanity defense, it is an important area of study to confirm or offset the public’s perceptions or fear. An analogy may be made to another plea that intersects the criminal justice and mental health systems, the intended consequences or outcomes of the GBMI option, often seen as a response to public outrage or concern. Yet research indicates that a GBMI plea does not routinely solve the public’s dilemma with defendants who also have mental illness. Tightening NGRI acquittee release criteria may, like the GBMI resolution, fail to address the initial problem, as there may not, in fact, have been a quantified one. The unintended consequences may lead to additional criminalization of the mentally ill as “. . .very little is known about the bond that the systems of criminal justice and mental health share, particularly when producing outcomes predicated on the joint effects of law and medicine” (Arrigo, 1996, pp. 572-573). The goal of NGRI acquittee research should be to provide policy makers with information, under the assumption that better policy decisions can be made when information is available.
Fear of these defendants, whether sentenced to corrections, or indefinitely committed to a psychiatric hospital, may still drive policy decisions and practices. Just as the NGRI population intersects the criminal justice and mental health system, fear is an attitude that also intersects the two systems. NGRI murder acquittees have differences not only when compared with all other acquittees but also when compared with their correctional system counterparts. The get-tough-on-crime approach has affected, whether intended or not, all those acquitted and sent to mental health systems. Public attention to the actual outcomes of such reforms is vital. Whether risk concerns, cost realities, or public attitudes will or should moderate the get-tough-on-crime approach in the future remains unknown.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.