
Abstract
Thoracic aortic thrombi are a well-known cause of distal embolic phenomena. There is a paucity of case reports because of the rarity of this condition, and thus clear management guidelines are lacking. The authors present a case of a mobile thoracic aortic thrombus managed by a surgical approach. This report demonstrates how intraoperative transesophageal echocardiography (TEE) proved to be critical in guiding surgical management. The utility of TEE in the diagnosis and management of aortic thrombi is also discussed. In addition, currently reported management strategies for this complex condition are reviewed.
Keywords
Case
A 63-year-old woman with a history of rheumatoid arthritis and hypertension presented to our hospital with shortness of breath and severe abdominal pain. The patient was hemodynamically stable with normal mental status. Her platelet count was 1219 × 103/µL; her hemoglobin and coagulation profile were within normal limits. On a computed tomography scan with intravenous contrast the patient was found to have bilateral pulmonary emboli, as well as significant infarcts in the spleen and kidney. In addition, a large intraluminal thrombus in the thoracic aorta was visualized, with extension into the proximal portion of the left common iliac artery. Lower extremity Doppler exam revealed evidence for deep venous thrombosis. Transesophageal echocardiography (TEE) was subsequently performed. The examination demonstrated a mobile, nonocclusive thrombus within the thoracic aorta, with a stalk of attachment to the thoracic aortic wall appearing to arise just distal to the left subclavian artery. The cause of the thrombosis was thought to be secondary to the patient’s history of rheumatoid arthritis and secondary thrombocytosis. After extensive discussion regarding the medical versus surgical management of this large, mobile aortic thrombus, a thoracotomy and aortic thrombectomy was planned—a surgical approach was favored because of the occurrence of distal emboli from the aortic thrombus. A heparin drip was initiated; anticoagulation was to be continued in the postoperative period because of the evidence for deep venous thrombosis and pulmonary emboli. If the patient experienced significant perioperative bleeding and became a contraindication for anticoagulation, an inferior vena cava filter would be placed intraoperatively.
The next day, the patient presented to our operating room for definitive management of her thoracic aortic thrombus. Anesthesia was induced and a left double-lumen endotracheal tube was placed for lung isolation; anesthesia was maintained with sevoflurane, fentanyl, and vecuronium. A radial arterial catheter and an internal jugular venous catheter were placed. A TEE probe was introduced to confirm the location and extent of the thrombus, as well as to help guide surgical thrombectomy. With the probe in a neutral position, the descending aortic short-axis and long-axis views were obtained. The mobility of the thrombus and the location of the stalk were confirmed (Figures 1 and 2). In addition, precise localization of the stalk of the thrombus was performed, noting that it arose 2 cm distal to the left subclavian artery. Because of the mobility of the thrombus and risk for further embolization, direct surgical palpation of the aorta was avoided. The surgeon was able to palpate the location of the TEE transducer in the esophagus and place his aortic cross-clamp just proximal to the probe—the patient remained hemodynamically stable during cross-clamp placement. The surgeon then performed an aortotomy above the stalk and successfully resected the entire thrombus through the small aortic incision (Figure 3). The aortotomy was then sealed with a small patch graft (Figure 4). Use of intraoperative TEE not only helped guide surgical management but also helped in allowing the patient to have only a small aortotomy, rather than a large aortic incision and potential replacement with a tubular graft. The patient’s remaining clinical course was complicated by another PE, for which an inferior vena cava filter was placed. The patient was eventually discharged from the hospital after return to her baseline state of health; she requires lifelong anticoagulation and hydoxyurea therapy for her thrombocytosis.
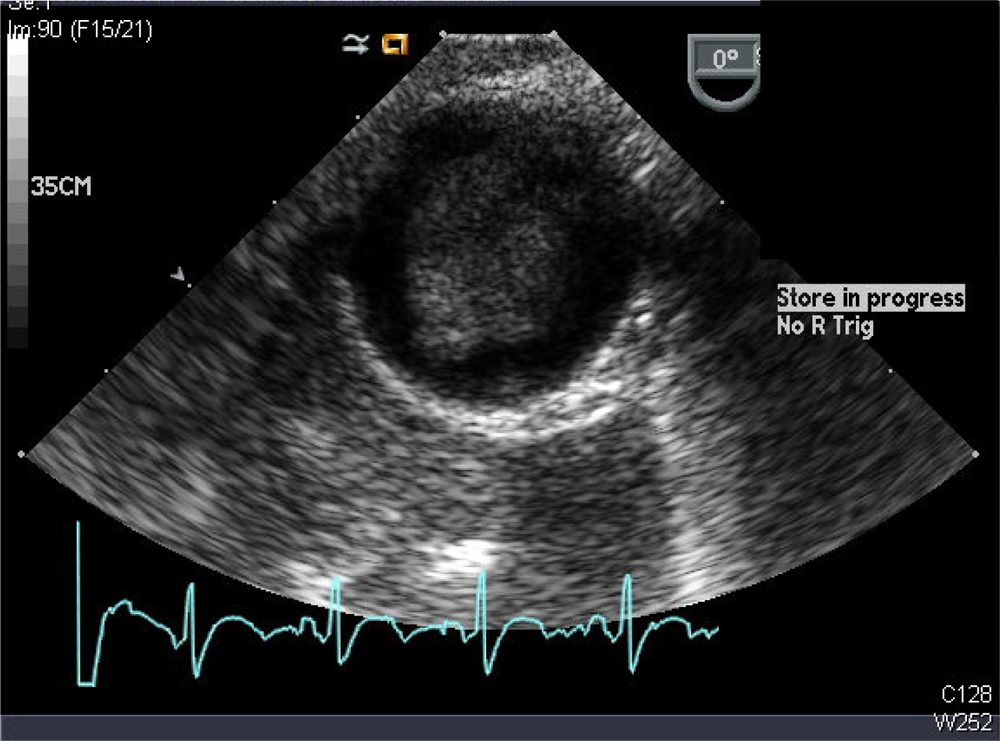
Transesophageal echocardiography descending aorta short-axis view demonstrating a thrombus in the descending thoracic aorta, nearly filling the entire aortic lumen
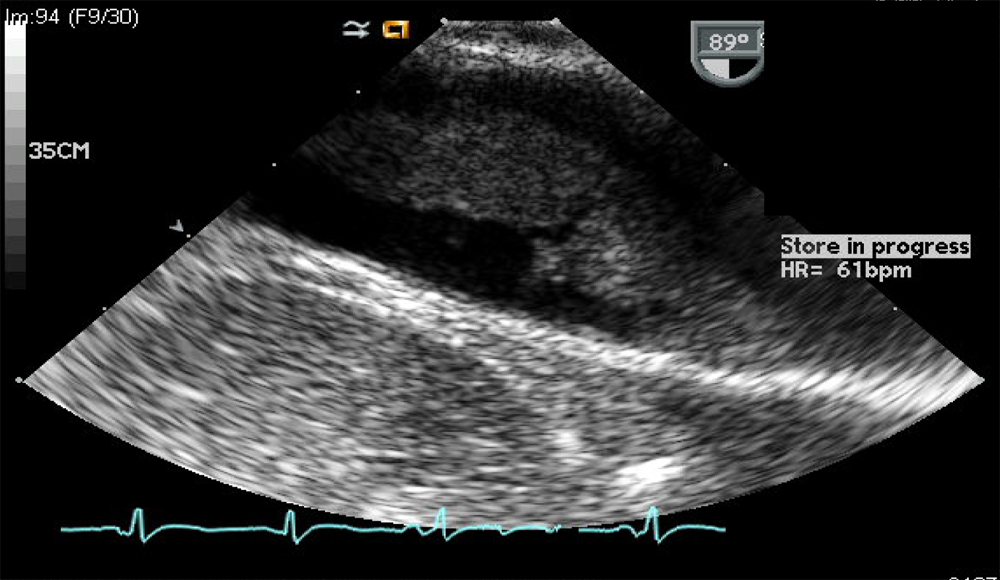
Transesophageal echocardiography descending aorta long-axis view demonstrating a stalk of attachment to the aortic wall. On further examination, this stalk was about 2 cm from the left subclavian artery

The entire thrombus was removed as one piece from the stalk through the aortotomy
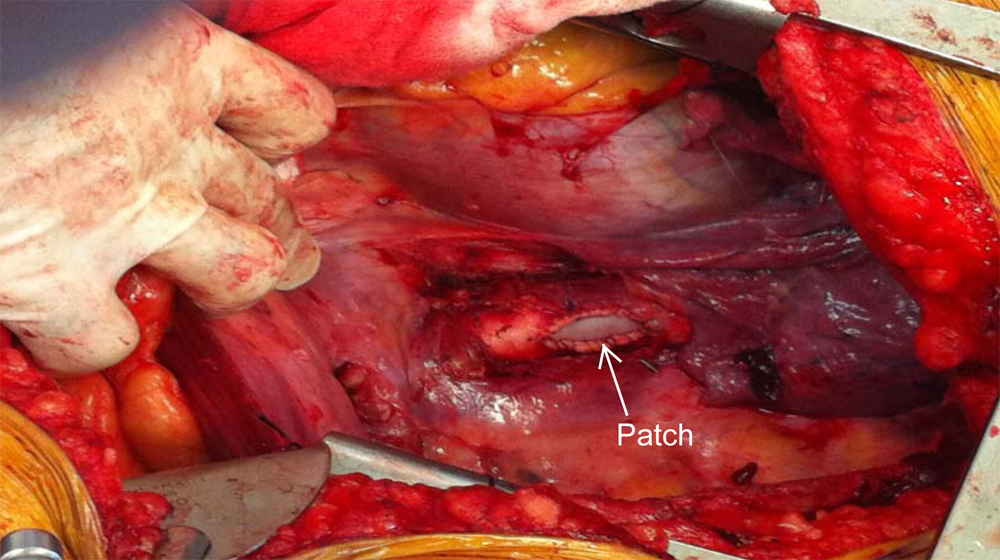
Use of intraoperative transesophageal echocardiography to guide surgical excision allowed minimal surgical manipulation of the patient’s thoracic aorta. The aortotomy was closed with a small patch, avoiding replacement of the aortic segment with a tubular graft
Discussion
Although various case reports have been reported in the literature,1-5 consensus guidelines for the management of a mobile thoracic aortic thrombus are lacking. Although these cases are rare, an initial conservative strategy has been advocated, while reserving more invasive management for patients who are unresponsive to medical therapy or evidence for significant systemic embolization.2,3 Medical management strategies have mainly involved the use of heparin, while reserving surgery for patients who continue to embolize despite therapy.3,4 Invasive management strategies have involved not only open thoracotomy and thrombectomy but also the use of endovascular therapy.1,6
The use of TEE has been advocated in the diagnosis and management of thoracic aortic thrombi that are a potential source of systemic embolization. TEE has been emphasized to be a reliable method of diagnosing thoracic aortic diseases and for identification of aortic thrombi. 5 The use of TEE is “real time,” allowing evaluation of the mobility of a particular thrombus. In addition, this modality allows the avoidance of intravenous contrast. It has been advocated that any systemic embolism without an obvious cardiac source should prompt a thorough evaluation of the thoracic aorta as a potential source. 7
Although there have been several reports on the use of preoperative TEE in the diagnosis of a thoracic aortic thrombus, the use of intraoperative TEE to guide surgical management of aortic thrombus has been limited to endovascular techniques.1,2,6,8,9 In our case, the proximity of the stalk of the thrombus to the left subclavian artery made determining the area of placement of the cross-clamp critical. Because of the intimate relationship of the thoracic esophagus with the thoracic aorta, we were able to precisely pinpoint the location of the stalk; the surgeon was then easily able to palpate the TEE transducer in the esophagus and note its relationship to the thoracic aorta. This allowed the surgeon to perform a mini-aortotomy and thrombectomy; thus, we were able to avoid prolonged cross-clamp placement, performance of a large aortotomy, possible aortic replacement with a graft, and the potential for significant blood loss.
Footnotes
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.