
Abstract
Interactions between the cardiovascular and respiratory systems are complex and profound. General anesthesia, muscle relaxation, and positive-pressure ventilation all impose physiological effects on cardiovascular function. In patients presenting for pulmonary resection, additional effects resulting from positioning, 1-lung ventilation, surgical procedures, and contraction of the pulmonary vascular bed may impose an additional physiological burden. For most patients with adequate pulmonary and cardiovascular reserve, these effects are well tolerated. However, the cardiothoracic anesthesiologist may be asked to provide anesthetic care for patients with significantly reduced cardiac function who require potentially curative pulmonary resection for lung cancer. These patients present a major perioperative challenge and a thoughtful approach to intraoperative management is required. The authors review a case of a patient with severely impaired biventricular function who presented for elective pulmonary lobectomy in an attempt to effect a curative resection of lung cancer and present a discussion of physiological and pathophysiological considerations for clinical management.
Keywords
Introduction
Interactions between the cardiovascular and respiratory systems are complex and profound. General anesthesia, muscle relaxation, and positive-pressure ventilation (PPV) all impose physiological effects on cardiovascular function. In patients presenting for pulmonary resection, additional effects resulting from positioning, 1-lung ventilation (OLV), surgical procedures, and contraction of the pulmonary vascular bed may impose an additional physiological burden. For most patients with adequate pulmonary and cardiovascular reserve, these effects are well tolerated. However, the cardiothoracic anesthesiologist may be asked to provide anesthetic care for patients with significantly reduced cardiac function who require potentially curative pulmonary resection for lung cancer. These patients present a major perioperative challenge, and a thoughtful approach to intraoperative management is required. We review a case of a patient with severely impaired biventricular function who presented for elective pulmonary lobectomy in an attempt to effect a curative resection of lung cancer and present a discussion of physiological and pathophysiological considerations for clinical management.
Case Presentation
The patient was a 61-year-old man with a medical history notable for reactive airway disease, benign prostatic hypertrophy, alcoholism, tobacco abuse, and a dilated cardiomyopathy characterized by severe biventricular dysfunction with a history of congestive heart failure (CHF). He had recently undergone a nuclear stress imaging study, which revealed a left-ventricular ejection fraction (LVEF) of 8%. Cardiac catheterization demonstrated normal coronary perfusion with an LVEF of 10%. At the time of his cardiac evaluation, he was severely symptomatic, able to ambulate only 15 m on a level surface, and experienced moderately severe dependent edema. Medical therapy for heart failure included carvedilol, lisinopril, digoxin, and furosemide, and these had produced significant improvements in the signs and symptoms of CHF. Additional medications included aspirin and albuterol.
The patient was admitted on the morning of surgery for a scheduled bronchoscopy, mediastinoscopy, and thoracoscopic right upper lobectomy for lung mass thought to be a bronchogenic carcinoma. Results of pulmonary function testing were as follows: FEV1 (forced expiratory volume in 1 s) = 101% predicted; FEV1/FVC (forced vital capacity) = 83%; and diffusing capacity for carbon monoxide (DLCO) = 88% predicted. On admission, his vital signs were as follows: blood pressure (BP) = 110/82; pulse = 98; SpO2 = 95% on room air; weight = 82 kg; and body mass index = 22. Laboratory studies were significant only for hemoglobin 12.1 g/dL. He appeared comfortable seated in an upright position and denied recent dyspnea or orthopnea, but he remained very sedentary. On examination, auscultation revealed distant breath sounds and mild bibasilar crackles, but no murmurs, rubs, or gallops were appreciated.
A frank discussion with both the patient and attending surgeon regarding the risks and benefits of surgery and anesthesia revealed that the patient understood and accepted these risks and wished very much to proceed with elective surgery with a curative intent.
In the operating room, the patient was lightly sedated with 2 mg IV midazolam, and left radial artery cannulation was performed under local anesthesia. After preoxygenation, intravenous induction of general anesthesia was accomplished with 10 mg etomidate, 50 mg rocuronium, and 100 µg sufentanil. The trachea was easily intubated with a 39 French left double lumen endotracheal tube under direct laryngoscopy and position confirmed by fiber-optic bronchoscopy. Mild hypotension was initially treated by infusion of epinephrine at 2 to 6 µg/min. Additional inotropic support was achieved by intravenous infusion of milrinone 0.375 µg/kg/min. Inhalational delivery of epoprostenol (Flolan) was initiated at 50 ng/kg/min to promote pulmonary vasodilation and right ventricular (RV) afterload reduction. After the induction of anesthesia, a central venous catheter was placed in the right internal jugular vein under ultrasound guidance, and a transesophageal echocardiography (TEE) probe was placed for continuous monitoring of cardiac function. Intraoperative echocardiographic examination revealed severely impaired biventricular function, severely dilated left ventricle, moderately dilated right ventricle, moderate mitral regurgitation, and mild tricuspid regurgitation (Figure 1). A small but observable improvement in biventricular systolic function was observed with the initiation of inotropic therapy (epinephrine and milrinone) and inhaled pulmonary vasodilator therapy. General anesthesia was maintained with 0.7% to 1.9% sevoflurane and midazolam.
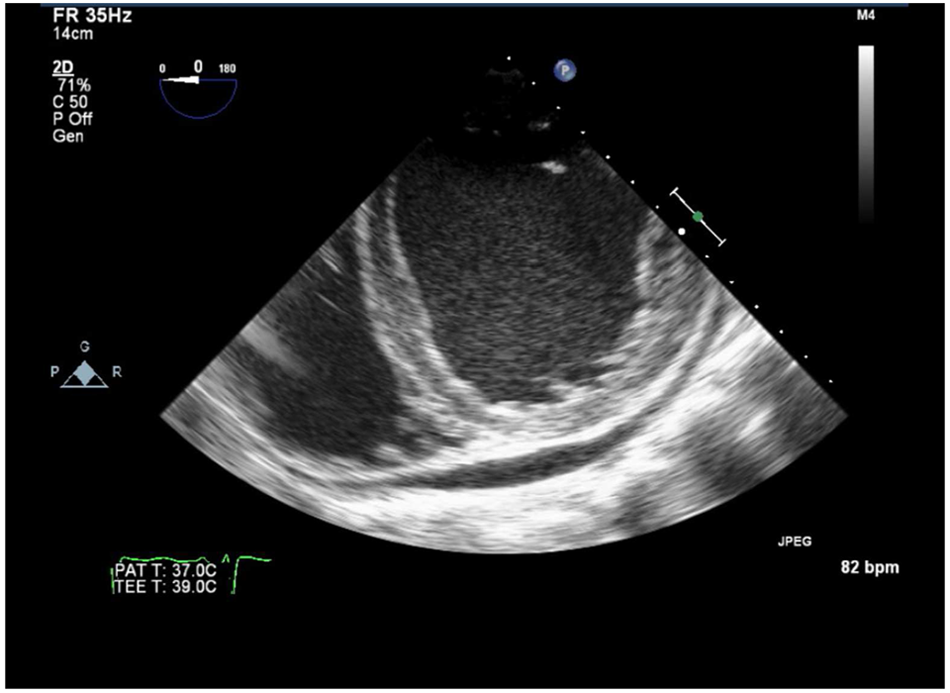
Transesophageal echocardiogram (TEE), midesophageal short-axis view (TG-SAX): this view illustrates biventricular enlargement with thinned myocardium and spontaneous echo contrast “smoke” in the left ventricle. A small pericardial effusion is also present.
OLV was easily achieved via the endobronchial lumen of the double-lumen endotracheal tube, and surgical conditions were deemed to be optimal. Efforts were made to minimize pleural insufflation pressure. Delivered tidal volumes during OLV were approximately 5 cc/kg, and peak pressures were below 30 cm H2O throughout. Positive end-expiratory pressure (PEEP) of 5 cm H2O was applied throughout the OLV period.
SpO2 values ranged from 92% to 100% during OLV. Lobectomy proceeded via a thoracoscopic approach and was concluded without complication. The nondependent lung was reinflated gently with continuous positive airway pressure (CPAP) at the conclusion of surgery, and 2-lung ventilation resumed at that time. After confirmation of neuromuscular recovery, the patient was emerged and extubated. Transport was to an intensive care unit dedicated to the care of surgical patients after cardiothoracic surgery. His recovery was complicated only by moderate postoperative hypercarbia treated with bilevel positive airway pressure and left basilar atelectasis, which responded to pulmonary toilet therapies. On postoperative day 3, he was transferred to a step-down unit and was discharged home without additional complication on postoperative day 4.
Cardiorespiratory Interaction: Effects of Spontaneous Ventilation Versus PPV
Spontaneous ventilation affects the physiology of the cardiovascular system largely through phasic changes in intrathoracic pressure (ITP) and lung volume as a result of diaphragmatic motion and can be understood based on the effects of these pressure/volume changes on venous return, ventricular interdependence, and ventricular loading phenomena.
In general, negative ITP accompanying spontaneous ventilation promotes an increase in venous return to the right heart, which transiently elevates RV end-diastolic volume. Because both ventricles share a common septum, an increase in RV end-diastolic volume tends to limit LV filling and, thus, LV stroke volume (LVSV). This phenomenon has been termed direct ventricular diastolic interdependence 1 and under normal conditions results in a small decrease in systolic arterial pressure. An exaggerated example of this diastolic interdependence resulting in decreased LVSV and arterial BP is referred to as pulsus paradoxus (>10 mm Hg) and commonly accompanies cardiac tamponade, 2 which magnifies the effect because of greatly increased coupling resulting from pericardial constraint.
The net effect of a negative-pressure lung inflation on LVSV ultimately depends on a balance between the 3 primary effects on cardiac function: an increase in LV afterload achieved by increasing transmural aortic pressure, a reduction in LV preload as a result of leftward shift of the interventricular septum after augmented RV filling (parallel interdependence), and a delayed augmented LV preload, again because of increased RV filling (serial interdependence). Under normal conditions, augmented venous return leading to improved LVSV is likely to be the net result of these changes. 3
The administration of a positive-pressure breath results in a small and transient increase in systolic arterial BP (known as Δ up) and then a transient decrease in BP (Δ down). The former results from both a decrease in LV afterload (decrease in transmural aortic pressure in a manner inverse to that of spontaneous inspiration) and a transient increase in pulmonary venous return to the left atrium by mechanical inflation of the lung parenchyma.4-6 The latter effect (Δ down) reflects a delayed reduction in LV preload resulting from positive-pressure inspiration impeding venous return several cardiac cycles previously. Phasic changes in arterial BP may also result from ventricular interdependence phenomena, whereby inspiratory decrements in RV filling permit enhanced LV diastolic dimension, SV, and arterial BP 7 with the inverse changes occurring during expiration. Ventilation may also affect ventricular function and cardiac output through effects on LV and RV afterload. Under normal conditions, spontaneous inspiration is associated with a greater decrease in ITP than in intraluminal thoracic aortic pressure because of the continuity of the thoracic aorta with arteries outside the thorax. This tends to increase transmural aortic pressure, increasing LV afterload.8-10 Inspiration affects RV afterload differently because (1) unlike the systemic arterial circulation, the entire pulmonary vasculature lies within the thorax and (2) RV afterload largely depends on pulmonary vascular resistance (PVR), which in turn varies with lung volume. Specifically, RV afterload appears to depend on the amount of lung residing within West zones 1 and 2 in which the alveolar pressure is great enough to cause physical compression of alveolar capillaries. 11
PPV has effects on LV afterload that are generally the inverse of those associated with spontaneous ventilation. An increase in ITP with a positive-pressure breath decreases transmural aortic root pressure, decreasing LV afterload. Unloading the LV favors LV ejection in patients with ventricular dysfunction and will be discussed below. As noted above, RV afterload tends to increase at higher lung volumes, specifically reflecting partial (West zone 2) or complete collapse (West zone 1) of the pulmonary vasculature. This observation appears to be true whether lungs are inflated spontaneously or with positive pressure. Patients mechanically ventilated for respiratory failure because of acute respiratory distress syndrome (ARDS) frequently develop pulmonary hypertension, which is further augmented by high airway pressures and pulmonary hyperinflation. Iatrogenic augmentation of RV afterload in this context may lead to RV dilation and acute cor pulmonale,12,13 which has been associated with increased mortality in ARDS. 14 Recent attention to protective ventilation strategies in these patients, which emphasize lower tidal volumes and airway pressures, may have led to a reduced incidence of cor pulmonale in ARDS. 15 Recognition of these heart lung interactions underlies recent emphasis on RV “protective” ventilation strategies in mechanically ventilated patients.
The effect of steady-state increases in ITP by the administration of PEEP or CPAP on cardiac function is complex and has been comprehensively reviewed. 16 The effect of positive-pressure lung inflation in general, and PEEP in particular, on cardiovascular function relates primarily to effects on ITP and lung volume. The extent to which a given alveolar pressure increases ITP is in turn related to compliances of the lung and chest wall, 16 both of which can be substantially altered in disease states such as acute lung injury. In normal hearts, PEEP may impede venous return and cardiac preload, particularly under conditions of hypovolemia. 17 Whereas the RV preload is adversely affected initially, the series linkage of ventricles leads to a decline in LV filling within several beats (series coupling). The mechanism by which venous return declines under conditions of PEEP is not entirely clear. The simplest explanation for PEEP-induced decrements in venous return is a reduction in the pressure gradient for return—that is, an ITP-mediated increase in right atrial pressure without a concomitant increase in mean systemic filling pressure. However, experimental studies and clinical observations provide evidence for parallel increases in right atrial pressure and mean systemic filling pressure, thus preserving the gradient for venous return.18-20 Although not entirely clear, it appears that PEEP may elicit constriction or compression of conducting veins leading to an increase in venous flow resistance. 18 This concept is consistent with the experimental observation of inferior vena cava collapse with PEEP administration in a canine model 21 and a high collapsibility index of the superior vena cava, 22 which in turn may be related to volume status. 23
PEEP appears to affect RV and LV afterload without an appreciable effect on cardiac contractility. The effects of PEEP on LV and RV afterload parallel those of PPV in general—that is, a decrease in LV afterload via effects on transmural aortic pressure and an increase in RV afterload by augmenting lung inflation and PVR.
The degree to which PPV in general and PEEP in particular lead to elevated PVR and RV afterload augmentation depends on whether the primary effect is to recruit atelectatic alveoli or to overdistend those alveoli that are adequately ventilated. At low lung volumes below functional residual capacity (FRC), PVR is elevated because of compression of extraalveolar vessels. If PEEP is applied under these conditions, resolution of atelectasis and an increase in lung volume toward FRC would be expected to diminish PVR and RV afterload, potentially augmenting RV performance.24,25 At lung volumes above FRC, alveolar vessels are compressed and PVR rises. 26 In patients with advanced pulmonary disease requiring mechanical ventilation, this latter effect appears to predominate. Echocardiographic study of patients with ARDS have demonstrated a high incidence of cor pulmonale attributable to RV outflow impedance, 15 a factor that directly limits RVSV 13 and has been linked to PEEP settings. 27 Indeed, lung volume–dependent effects of PEEP have been observed in clinical studies of patients with respiratory failure. Application of PEEP leads to a decline in pulmonary artery pressures (PAPs) when alveolar recruitment results. 28 PEEP-induced impairment of RV stroke index is inversely correlated with lung recruitment in ARDS. 29 This finding may explain why pulmonary recruitment maneuvers used to treat atelectasis may promote RV dilation and LV collapse. 30
Cardiorespiratory Interaction in Patients With Cardiomyopathy
It is now understood that cardiovascular and pulmonary disease states affect the nature of cardiopulmonary interactions and response to respiratory interventions. Under normal cardiovascular conditions, the application of PPV and the resultant increase in ITP limits cardiac preload via decreased venous return, resulting in the previously discussed decrements in cardiac output via the Frank Starling mechanism. Thus, the normal heart is said to be “preload dependent.” Hypovolemic states and pulmonary hyperinflation may also present with similar responses to PPV. However, if cardiac contractile function is profoundly compromised, effects on ventricular afterloading may predominate, particularly because patients with CHF are often hypervolemic. Indeed, the response to incremental increases in ITP differs between patients with normal heart function and those with significant dysfunction. 31
It is now well appreciated that increases in ITP associated with PPV and CPAP may lead to improvement in cardiac function, especially in disease states. It should be noted that lung volume rather than airway pressure itself determines ITP during PPV. 32
Thus, alterations or abnormalities in lung or chest wall compliance ultimately contributes to the relationship between an applied airway pressure and increases in intrathoracic, intrapleural, and intrapericardial pressures.
Most of the available data relating cardiorespiratory interactions to cardiac function in disease states comes from investigations and clinical observations in acute heart failure, obstructive sleep apnea (OSA), and ventilator weaning.
The application of PEEP has been found to improve hemodynamics in most33,34 but not all 35 experimental studies of patients with poor ventricular reserve. Discrepancies may be attributable to a number of factors not controlled in these studies: (1) unreported differences in pulmonary compliance and the resultant degree of pulmonary inflation/hyperinflation with attendant increase in RV afterload, (2) severity of preexisting RV dysfunction and pulmonary hypertension, and (3) pretreatment differences in volume status. In patients with LV dysfunction and CHF requiring mechanical ventilation, the application of PEEP adversely affected cardiac output in patients with low pulmonary capillary wedge pressure but improved cardiac output in those patients with elevated filling pressures. 33
Elevation of ITP by mechanical ventilation in both animal and clinical studies augments cardiac function.36,37 In a canine model of heart failure, the phasic application of high-frequency jet ventilation timed to coincide with cardiac systole in a canine heart failure model augmented LVSV more effectively than when applied during diastole. 38 This phenomenon was not abolished by pericardiectomy. Additional support for ITP-mediated improvements in ventricular function comes from studies of CPAP in patients with ventricular dysfunction. The application of CPAP in patients with heart failure predominantly affects filling pressures39-41 but may also augment LVEF 42 and cardiac output.31,43,44 The primary hemodynamic effect of CPAP in patients with normal contractile function appears to result from a decrease in LV preload, whereas in patients with impaired LV contractile function, decreases in LV end-diastolic volume are associated with significant improvements in LVEF. 42
Evidence for additional mechanisms by which the application of CPAP or bilevel positive airway pressure may improve cardiac function comes from studies of patients with OSA and weaning from mechanical ventilation. Recent evidence points to the potential of these modalities to modulate cardiac function by cardiorespiratory interaction. In studies of patients with OSA and heart failure, the application of CPAP resulted in clinical improvements of OSA, reduced LV end-systolic diameter, and increased LVEF, from 25% to 33.8%. 45 Though the improvement in cardiac function is likely multifactorial, CPAP is believed to decrease cardiac afterload in OSA patients with heart failure by attenuating negative intrapleural pressure swings and reducing systemic BP. 46 Similar dramatic improvements in LV function have been observed in patients with idiopathic dilated cardiomyopathy CMP and OSA. 47
OLV: Effect on Cardiac Preload, Afterload, and Systolic Function
OLV is frequently used to improve surgical exposure for procedures within the thorax, including pulmonary resection surgeries. The specific effects of OLV per se on the cardiovascular system and hemodynamics are often difficult to assess from clinical studies because it is typically accompanied in the clinical context by changes in body positioning (usually lateral decubitus), surgical incisions of the chest wall and pleura (thoracotomy and thoracoscopy), mechanical compression of the lung in the operative hemithorax, pleural insufflation, hypercapnia, and the delivery of anesthetic agents, all of which may potentially affect hemodynamic function. Perhaps these factors help explain the wide variation seen in animal and clinical studies of OLV and hemodynamics. The initiation of OLV has been correlated with an increase,48-51 decrease,52-54 and no change54-60 in cardiac output in patients undergoing OLV.
Through the mechanisms discussed for 2-lung ventilation, the selective application of PPV to 1 lung is likely to result in reduction in LV afterload to the extent that ITP is increased. The degree to which ITP increases during OLV is in turn affected by the surgical approach. Pressure within the ventilated hemithorax will be largely affected by ventilatory parameters and lung and chest wall compliance. During thoracoscopic surgery, pressure within the operative hemithorax is largely a function of pleural insufflation pressure. Though not conclusively demonstrated, a reduction in LV afterload may occur during OLV with an open chest (thoracotomy) and is supported by observations of an increase in cardiac output 50 under these conditions and reduced aortic regurgitation with the onset of OLV. 61 Systemic vasodilation, which may accompany an increase in ITP, 16 further contributes to a decrease in LV afterload. A decrease in systemic vascular resistance (SVR) with the onset of OLV has been reported in some studies.49-50
OLV affects LV preload via decrements in filling through direct effects on venous return as well as phasic and steady-state ventricular interdependence phenomena and septal shift. Thus, pulse pressure variation occurs during OLV and continues to predict fluid responsiveness during OLV and pulmonary resection. 62 More dramatic increases in lung volume and ITP associated with recruitment maneuvers63,64 and higher levels of PEEP and CPAP during OLV are associated with a decrement in cardiac output.50,63 The hemodynamic effects of recruitment maneuvers are observed even under open-chest conditions64,65 and appear to decrease LV diastolic dimensions. 65 Under greatly exaggerated conditions of dynamic hyperinflation, complete cardiovascular collapse can result. 66
The selective delivery of oxygen to 1 lung results in alveolar hypoxia in the nonventilated lung. Through an oxygen-sensing mechanism present in pulmonary vascular smooth muscle cells, alveolar hypoxia leads to an increase in arterial vasomotor tone, decreasing blood flow to regions not participating in gas exchange. This adaptive mechanism promotes an improvement in ventilation perfusion matching by decreasing intrapulmonary shunting and venous admixture. One potential consequence of hypoxic pulmonary vasoconstriction (HPV) involving an entire unventilated lung is an increase in PVR as a result of the contraction of the pulmonary vasculature. Within the normal lung, the low-pressure, high-capacitance vasculature is well known to buffer changes in blood volume. This characteristic of the pulmonary vasculature may explain the variable and generally modest increases in PVR that result from OLV. In addition, underlying alterations in PVR and loss of pulmonary vasculature from diseases such as chronic obstructive pulmonary disease, common in thoracic surgery patients, may contribute to the variability seen in these studies.
Despite buffering effects, increases in PVR and PAPs can occur with the onset of OLV,48,52 creating conditions of increased afterload for the RV. This in turn causes an increase in RV dimensions during both systole 55 and diastole.52,55 The former is likely a direct result of increased afterload; the latter may represent a compensatory preload reserve effect. 55 The degree to which RV afterload is increased after the onset of OLV is likely to be affected by the degree to which HPV contracts the pulmonary vascular volume of the nonventilated lung; hypercapnia 67 ; the method of oxygen delivery to the nonventilated lung50,52; surgical factors, including pleural insufflation, thoracotomy, and direct lung compression; and specific anesthetics.49,54 In a clinical study, the partial recruitment of nondependent lung tissue during OLV by the application of high-frequency PPV normalized the pulmonary vascular resistance index (PVRI) and RV end-diastolic volume index and improved RVEF by 33% compared with CPAP. 52
Though the evidence is incomplete, it appears that under normal conditions, cardiac output is not dramatically altered by the institution of OLV, though other concurrent factors such as pleural insufflation may profoundly affect hemodynamics. The primary hemodynamic effects of OLV per se are the result of effects of augmented RV afterload and decrements in RV function (Figure 2). It also appears likely that the fundamental and previously discussed cardiorespiratory interactions remain active during OLV, though attenuation of these effects by open thoracotomy seems likely.
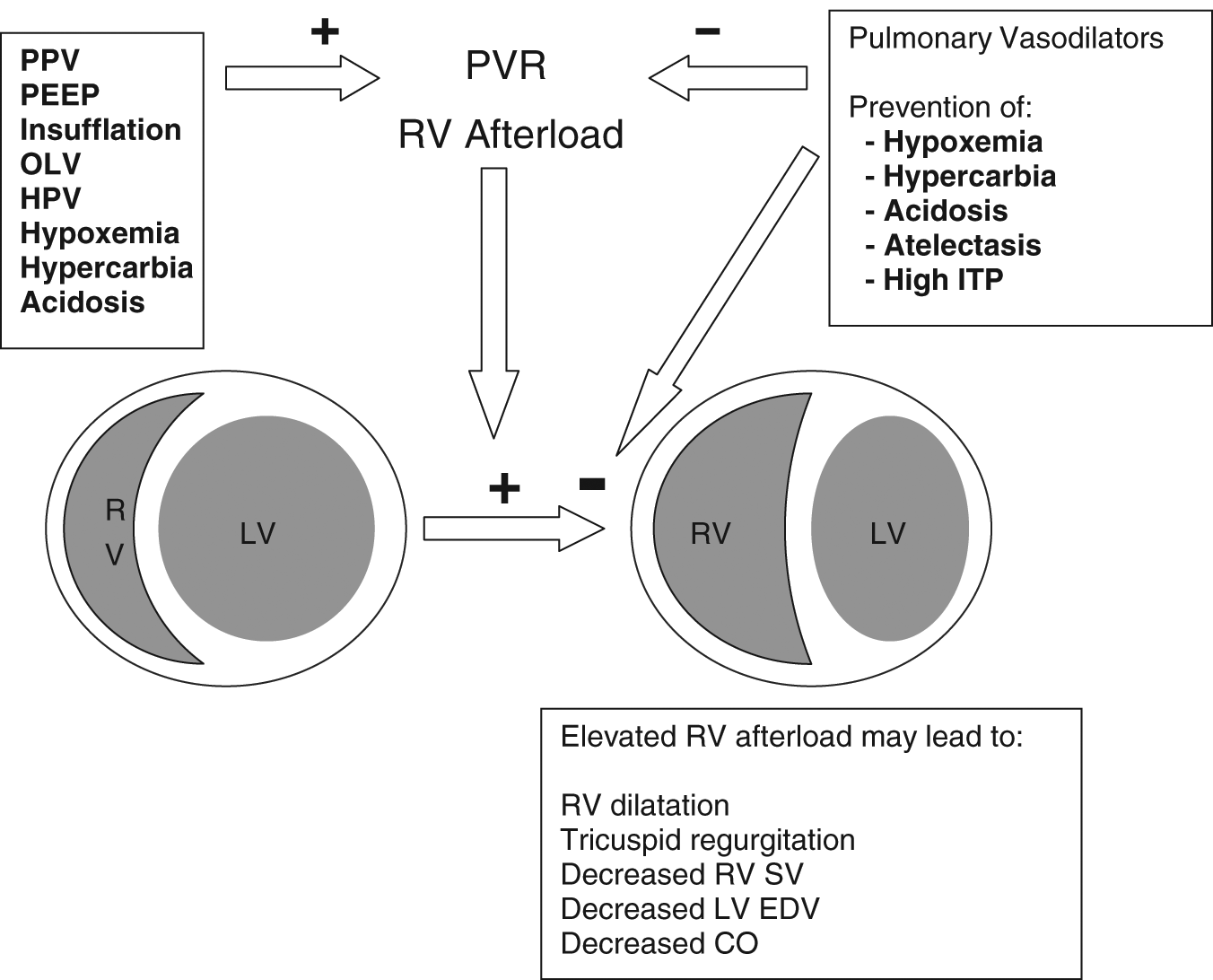
Schematic representation of intraoperative factors that may affect right ventricular (RV) function during thoracic surgical procedures. Ventilatory factors, including positive-pressure ventilation (PPV) and positive end-expiratory pressure (PEEP) as well as hemithoracic insufflation, have the potential to adversely affect pulmonary vascular resistance (PVR) through effects on intrathoracic pressure (ITP). Hypoxic pulmonary vasoconstriction (HPV), acidosis, hypercarbia, and hypoxemia may directly augment PVR, which increases RV afterload. Elevated RV afterload may lead to decreased RV stroke volume (SV), RV dilation, and decrements in LV output via parallel and series ventricular interdependence effects. These adverse effects may be mitigated, at least in part, by optimal control of ventilatory parameters, prevention of gas exchange and pH abnormalities, and inhalational pulmonary vasodilator therapy.
Effect of OLV on Cardiac Function in Patients With Cardiomyopathy
The clinical effects of OLV in human patients with systolic ventricular dysfunction have not been studied systematically, and the scant available information in the English language literature comes from case reports, with most patients having only LV dysfunction,68,69 dysfunction of mild to moderate severity, 70 and/or mechanical circulatory support. 69 Leonard and Myles 68 describe the anesthetic management of a patient with impaired LV systolic function (LVEF = 25%) who underwent thoracotomy and pulmonary lobectomy under total intravenous anesthesia. They describe a slight reduction of arterial BP after induction and during OLV, which was treated with metaraminol. Neither cardiac output nor mean PAP changed significantly during this period. These results are consistent with those seen in the patient we presented above. Though we did not directly measure cardiac output in our patient, TEE examination revealed mildly improved biventricular function with the institution of inodilator therapies and no observable change in the size or function of either ventricle with the institution of OLV or with low-pressure pleural insufflation. The very limited available information suggests that OLV per se does not greatly perturb hemodynamic function in the adequately preloaded heart under optimal conditions of inotropic and pulmonary vasodilator support. Nevertheless, care should be taken to avoid iatrogenic pulmonary hyperinflation, hypercarbia, and of course, hypoxemia, all of which could further exacerbate increases in PVR and RV afterload. This is likely to be particularly important in patients who also have preexisting severe RV dysfunction.
Surgical Implications
Patient Positioning
Patients who are undergoing pulmonary resection are frequently placed in the lateral position depending on the side of operation. Historically, there has been conflicting evidence regarding the effects of body position on hemodynamics. Animal studies demonstrated that the change from the supine to lateral position caused an increase in intracardiac pressures and cardiac ouput. 71 Fujise et al 72 found that in humans, the degree of hemodynamic changes with positioning differs between the right and left lateral decubitus positions. They found an increase in preload and cardiac index (CI) and a decrease in SVR, with these changes being more pronounced when patients were placed in the right lateral decubitus position. 72 These findings would explain why many patients with heart failure are more comfortable or have less symptoms when placed in the lateral position (trepopnea), particularly the right lateral decubitus position. 73 It is still unclear how this phenomenon affects patients undergoing thoracic surgery because these effects may be offset by those of hemithoracic insufflation.
Hemithoracic Insufflation
The effects of positive-pressure insufflation during thoracoscopy should be seriously considered by the cardiothoracic anesthesiologist. Surgeons use positive-pressure hemithoracic insufflation as a means to hasten lung collapse and to optimize exposure of intrathoracic structures. 74 However, insufflation of the hemithorax is not without possible hemodynamic compromise because it creates a pathophysiological state similar to that of a tension pneumothorax. In an experimental porcine model, hemithoracic insufflation pressures of 5 mm Hg during both 2-lung ventilation and OLV resulted in decreased CI, mean arterial pressure, and LV stroke work index and increased PAP and central venous pressure (CVP).75,76 Similar results were observed in a clinical study that demonstrated hemodynamic deterioration with insufflation pressures >5 mm Hg and inadequate surgical exposure in a majority of patients at lower insufflation pressures. 76
Results from human studies of hemithoracic insufflation effects on hemodynamics are mixed. Wolfer et al 77 demonstrated that slow increases in insufflation pressure (up to 14 mm Hg) were well tolerated, with an increase in CVP but no significant changes in mean arterial pressure, heart rate, arterial oxygen saturation, or end-tidal CO2.
Additional evidence to support the video-assisted thoracoscopic (VATS) approach in patients with cardiomyopathies comes from reports of VATS epicardial lead implantation for resynchronization therapy.78,79 It should be noted that neither study involving resynchronization therapy discusses whether insufflation was used in these procedures. Byhahn et al 80 demonstrated that in patients undergoing total endoscopic coronary artery bypass grafting, the use of insufflation pressures of 10 to 12 mm Hg unilaterally were well tolerated without any change in LV or RV function. Although thoracoscopic approaches in general appear to be reasonably safe in patients with cardiomyopathy, the absence of definitive data with regard to hemithoracic insufflation in this patient population should prompt a cautious approach, particularly in patients with severe RV dysfunction.
Oxidative Stress
It is now well appreciated that OLV and subsequent lung expansion generates reactive oxygen species (ROS), in what has been referred to as atelectasis reexpansion syndrome.81,82 The damage that occurs at the cellular level commences with hypoxia and is worsened during reoxygenation of the lung. ROS interact mostly with endothelial cells and may initiate tissue dysfunction by destroying antioxidant defense mechanisms. 83
Studies have also shown that the heart and lung are directly and adversely affected by ROS. 83 Oxidative stress appears to cause arrhythmias and increases the incidence of pulmonary hypertension and acute respiratory failure. 83 Arrhythmia formation is thought to be a result of the hydroxyl radical and hyperoxynitrate, both by-products of oxidative stress.84,85 These products alter electrophysiology and the mechanical properties of myocytes 85 and inhibit sarcolemmal Na/ATPase activity. 86 A more recent study suggests that there may be a biochemical basis for these perioperative changes in myocardial reserve. 87 Heerdt and colleagues used a swine model to demonstrate that the oxidative stress associated with pulmonary lobectomy resulted in a profound reduction in sarcoplasmic endoreticular calcium adenosine triphosphate subtype 2a activity. 86 The latter compound plays a key role in myocyte calcium cycling, and therefore, activity reduction was associated with nitrotyrosine incorporation into myocardial proteins and a decrement in the contractile property of isolated myocardial trabeculae. 87
ROS may also play a role in the development of pulmonary hypertension.88-90 The NADPH oxidase pathway produces superoxide, which is increased during reperfusion. 84 Superoxide increases 5-hydroxytryptamine-induced pulmonary vasoconstriction. Endothelin-1 (a potent vasoconstrictor) activity is also stimulated by ROS. 90
Although definitive clinical evidence is lacking, experimental data suggest that oxidative stress and resultant ROS may impair cardiac function and increase PVR. Though small changes in these parameters may be well tolerated in the healthy patient, the likelihood of significant hemodynamic derangements in the patient with severe biventricular dysfunction should be considered during this period.
Contraction of the Pulmonary Vascular Bed
Pulmonary resection inevitably results in contraction of the pulmonary vascular bed. RV dysfunction is a potential physiological consequence, particularly in patients with preexisting cardiac dysfunction. Hemodynamically significant complications usually arise 48 to 72 hours postoperatively, suggesting a multiphasic response to lung resection. Postoperatively, resting mean PAPs and PVR return to baseline values, whereas RVEF decreases over several days.91,92 Despite decrements in RVEF, RVSV is generally preserved after major lung resection.92,93 An echocardiographic study of the RV after pulmonary resection confirmed RV dilation and dysfunction during the early postoperative period. 94
In both early and late postoperative periods, PAPs at rest and during activity were higher than preoperative values. 95 However, the PAPs at rest and during activity were higher in the late postoperative period compared with those in the early postoperative period, suggesting a deterioration of the pulmonary vascular bed over time. 95 Based on these results, it was concluded that even though clinical symptoms remained stable, the condition of the pulmonary vascular bed did not improve. 95
In the absence of relevant data in the cardiomyopathy population, it is reasonable to conclude that detrimental effects of surgery on the pulmonary vascular bed and resultant effects on PVR are more likely to exacerbate RV dysfunction in this population.
Anesthetic Management
Preoperative Assessment
Preoperative evaluation prior to lung resection is essential for risk stratification. Most patients scheduled to undergo lung resection are current or former smokers and are thus at elevated risk for cardiac, pulmonary, and vascular disease processes. Initial evaluation should include a thorough history and physical, review of radiographic findings, evaluation of pulmonary function tests, and assessment of cardiopulmonary status. Morbidity and mortality in this patient population is largely from respiratory complications; cardiac complications account for approximately 15%.96,97 Though not well studied, severe preoperative cardiac disease is likely to increase these risks.
The most commonly used spirometric test to determine perioperative pulmonary risk is the FEV1. 98 Classically, an FEV1 greater than 80% predicted or greater than 2 L has been considered adequate for pneumonectomy and a FEV1 greater than 1.5 L for lobectomy. The most valuable single test for postthoracotomy respiratory complications is the predicted postoperative (ppo) FEV1. 96 The ppo FEV1 is calculated as follows: ppo FEV1% = preoperative FEV1% × (1 − [Percentage functional lung tissue removed]/100). Patients with ppo FEV1 greater than 40% are considered to be at average risk for respiratory complications; major respiratory complications and postoperative ventilatory support have been associated with ppo FEV1 values of 40% and 30%, respectively. 97
Diffusion capacity across the alveolar capillary interface is also widely used in predicting perioperative risk, particularly in patients who have borderline spirometric results. DLCO is a useful test in determining gas exchange capacity of the lung. 99 Studies have shown that DLCO is a strong predictor of mortality when expressed as the percentage ppo. 99 Patients undergoing surgical resection with a DLCO less than 40% are at high risk for perioperative cardiopulmonary complications and have increased mortality.98,99
Cardiopulmonary status can be assessed in many ways, and all patients undergoing lung resection should have some assessment of their cardiopulmonary reserves. Formal cardiopulmonary exercise testing is used to calculate maximal oxygen consumption (VO2max). Information obtained from cardiopulmonary exercise testing includes exercise ECG, heart rate response to exercise, minute ventilation, and oxygen uptake per minute. 98 A VO2max less than 10 mL/kg/min is indicative of high risk for perioperative death and cardiopulmonary complications.97-99 Other tests can be used to assess a patient’s cardiopulmonary status, including stair climbing and 6-minute walking tests98,99; however, it should be noted that there is variability in how these tests are performed and interpreted.
The unilateral pulmonary arterial occlusion (UPAO) test is a more useful test to evaluate patients who are at high risk for RV failure after pulmonary resection. As previously stated, lung resection causes not only a decrease in lung volume but also a decrease in the size of the pulmonary vascular bed. The UPAO test thus mimics this loss of pulmonary vascular volume and allows for estimation of postoperative right heart function. This test is performed by placing a pulmonary arterial occlusion catheter in the pulmonary arterial trunk on the side that is to be resected and evaluating right-heart hemodynamics. 100 The variables measured before and during the test are the cardiac output, CI, and the mean PAP (mPAP). The total pulmonary vascular resistance index (TPVRI) is then calculated as follows:

One study concluded that the occluded TPVRI was the only predictor of postoperative cardiopulmonary complications, and the author recommended that lobectomy should be contraindicated in patients with an occluded TPVRI ≥ 900 dynes. 101 Other studies suggest that the preoperative functional limits include not only TPVRI but also mPAP and CI, using the following values as functional limits TPVRI < 700 dyne sec cm−5 m−2, mPAP < 30 mm Hg, and CI > 2.0 L min−1 m2. 101 The UPAO may not be necessary as part of a routine workup for patients undergoing pulmonary resection but is of value in patients with known cardiac dysfunction or those with insufficient cardiopulmonary status on routine testing.
Other organ systems should be thoroughly evaluated, and patients should be counseled on smoking cessation prior to surgery.
Management of General Anesthesia
The goals of anesthetic management in patients with cardiomyopathy include maintenance of normovolemia, avoidance of medications that cause myocardial depression, and prevention of increased ventricular afterload that could tip the balance toward frank failure in an already jeopardized heart. Managing OLV in this patient population only adds to the complexity in the challenge to maintain a balance between optimal lung protection ventilation strategies (optimal minute ventilation, avoidance of barotrauma, minimizing PVR, optimal lung isolation, and appropriate oxygenation) and support of ventricular function (inotropic intervention, afterload reduction, maintenance of coronary perfusion, and stabilization of rhythm). In patients with low-output states with or without congestive symptoms, inotropic agents, vasodilators, and diuretics can be used to facilitate a more desirable physiological state on the Frank-Starling curve (see Table 1).
Table of recommendations of interventions and medications for patients at risk of ventricular failure during one lung ventilation. Adapted from Forest P, and Overgaard C, et al.
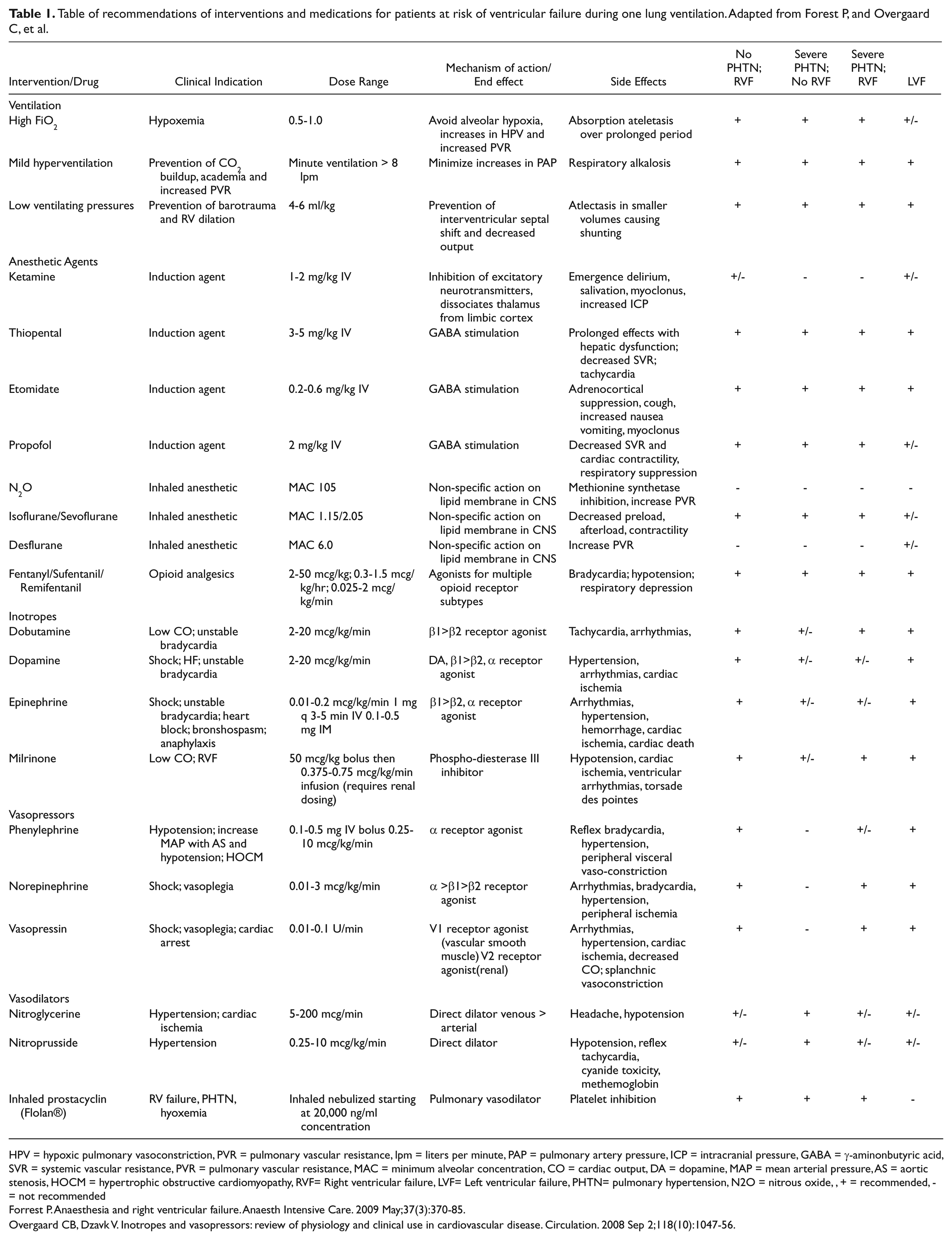
HPV = hypoxic pulmonary vasoconstriction, PVR = pulmonary vascular resistance, lpm = liters per minute, PAP = pulmonary artery pressure, ICP = intracranial pressure, GABA = γ-aminonbutyric acid, SVR = systemic vascular resistance, PVR = pulmonary vascular resistance, MAC = minimum alveolar concentration, CO = cardiac output, DA = dopamine, MAP = mean arterial pressure, AS = aortic stenosis, HOCM = hypertrophic obstructive cardiomyopathy, RVF= Right ventricular failure, LVF= Left ventricular failure, PHTN= pulmonary hypertension, N2O = nitrous oxide, , + = recommended, - = not recommended
Forrest P. Anaesthesia and right ventricular failure. Anaesth Intensive Care. 2009 May;37(3):370-85.
Overgaard CB, Dzavk V. Inotropes and vasopressors: review of physiology and clinical use in cardiovascular disease. Circulation. 2008 Sep 2;118(10):1047-56.
Inhaled anesthetics
Inhaled volatile anesthetics may alter ventricular function by reducing preload and contractility. RV failure can occur as a result of acute elevations in PVR caused by hypoxia, hypoventilation, atelectasis, and high ventilating pressures. It appears that halothane, isoflurane, and sevoflurane do not affect PVR unfavorably.101,102 However, PVR can be increased by both desflurane and nitrous oxide, and these agents should be avoided in patients at risk of RV failure—that is, those with preexisting RV dysfunction and severe pulmonary hypertension.103-106 There has also been speculation that the use of epidural analgesia allows the use of a less-volatile anesthetic during OLV, which in turn might have less impact on attenuating HPV, thereby improving oxygenation and minimizing increases in PVR. 107 Although volatile anesthetics appear to inhibit HPV in vivo and in vitro, they appear to have no major impact on oxygenation during OLV, and the type of anesthetic (inhalational vs total intravenous) by itself does not affect oxygenation during OLV. 108 Other factors such as lung mechanics may play a larger role in gas exchange.
Opioids
Of the short-acting opioids commonly used during thoracic surgery, fentanyl and sufentanil have minor effects on pulmonary hemodynamics. Remifentanil may cause a reduction in pulmonary vascular tone through histamine and opioid receptor pathways. 109
Intravenous anesthetics
Etomidate is known for its stable hemodynamic profile and is often advocated as the induction agent of choice in patients with depressed cardiac function. However, etomidate is known to cause adrenal insufficiency, and its use in critically ill patients is controversial. 110 Though arterial pressure is maintained during etomidate anesthesia, there is concern for augmented LV afterload, which could potentially adversely affect myocardial function in patients with preexisting systolic dysfunction. 111
Thiopental can reduce RV contractility and SVR but does not change PVR. Ketamine may have a safer hemodynamic profile than etomidate in critically ill patients but can increase PVR and myocardial work. 112
Propofol is known to depress ventricular filling pressure and contractility, but these effects can be reversed with inotropic support. Direct effects of propofol on PVR are minimal, but it can produce pulmonary vasoconstriction on activation of α-adrenoreceptors.101,113,114
Inotropes
Optimal use of inotropes during cardiac dysfunction and heart failure remains controversial. Nevertheless, they are used for improving cardiac output by enhancing contractility and chronicity, decreasing SVR, and enhancing diuresis through increased renal blood flow. Dobutamine, dopamine, and epinephrine all improve SV, increase heart rate, and decrease filling pressure. However, they increase myocardial stroke work and oxygen consumption.115,116 Nevertheless, dobutamine appears to have an advantage in this regard by proportionally increasing coronary blood flow.117,118 Additionally, beta-adrenergic receptor responses may be blunted in heart failure, leading to a low efficacy of these agents. Epinephrine can increase arterial and venous pulmonary pressures through direct pulmonary vasoconstriction and increase in blood flow. 116 Milrinone, acting through a non-β-adrenergic pathway, does not have an associated diminished efficacy or tolerance. As a selective phosphodiesterase-3 inhibitor, it produces less tachycardia than catecholamines, decreases filling pressure and SVR (vasodilation), and increases SV through direct positive inotropy, resulting in less cardiac oxygen consumption. 116 It also enhances diastolic relaxation (lusitropy) and causes relatively more RV afterload reduction through pulmonary vasodilation (Table 1). 116
Vasopressors
Norepinephrine, phenylephrine, and vasopressin stimulate arterial and arteriolar vasoconstriction, resulting in increased mean arterial pressure. This serves to increase right and left coronary blood flow and improve ventricular function, thereby increasing LV and RV output. 101 Additionally, in RV ischemia during pressure overload, increasing LV afterload with these agents produces an interventricular septal shift back to the RV that may improve LV output and, conceivably, RV output.101,119 Norepinephrine, a powerful α1-agonist, primarily increases systolic, diastolic, and pulse pressures. It can increase coronary perfusion through increases in diastolic pressure but can be cardiotoxic, inducing apoptosis if used as an infusion for a prolonged period. 116 Norepinepherine is also commonly used for low BP because of vasoplegia. 115 It appears to be more effective (increase in cardiac output) than phenylephrine during conditions of RV failure caused by pressure overload rather than in chronic pulmonary hypertension.101,120 Phenylephrine, an α-agonist, is often used as a bolus for correction of sudden severe hypotension. Although it may lead to increased RV coronary perfusion pressure, it may worsen RV function in patients with chronic pulmonary hypertension similarly to norepinephrine because of direct coronary vasoconstriction and/or pulmonary arterial vasoconstriction. 121 Vasopressin can produce potent systemic vasoconstriction and pulmonary vasodilation through stimulation of nitric oxide (NO) in the pulmonary endothelium. 122 The effects of vasopressin are relatively unaffected by hypoxic and acidotic conditions compared with those of norepinephrine, and it is often more useful for refractory hypotension in patients with pulmonary hypertension (see Table 1). 116
Pulmonary vasodilators
RV failure results from anatomic and physiologic impediments to normal RV ejection. The causes are extensive but typically relate to an elevation in PVR, either as the primary cause of RV failure or as a contributing factor in patients with an already dysfunctional right ventricle. 123 Reduction of PVR is therefore a primary focus of prevention and treatment for RV failure in these patients. It is evident that the efficacy of vasodilator therapies is related to the severity of vasoconstriction in the pulmonary circulation. 124
Pulmonary vasodilating agents may be administered enterally (phosphodiesterase inhibitors sildenafil and bosentan), intravenously (calcium channel blockers, adenosine, magnesium, nitroglycerin, phosphodiesterase inhibitors, and prostanoids), or inhalationally (inhaled NO [iNO], prostacyclin, iloprost, nitroprusside, nitroglycerine, and milrinone) (Table 1). The inhalational delivery of vasodilators produces predominant or exclusive pulmonary vasodilation depending on the pharmacokinetic and pharmacodynamic properties of the drug. Their effects are predominantly seen in well-ventilated lung regions, minimizing overall ventilation-perfusion mismatch. iNO and prostacyclin both produce pulmonary vasodilation, decreasing PVR and improving oxygenation with minimal systemic effects. They are effective in treating pulmonary hypertension caused by vascular disease, ARDS, acute lung injury, RV failure complicating cardiac surgery, and Eisenmenger’s syndrome. iNO works through a receptor-mediated increase in cyclic guanosine monophosphate (GMP), causing vasodilation and inhibition of smooth muscle cell proliferation. It is administered through a delivery system that minimizes the formation of nitrogen dioxide. 125 Despite dramatic improvement in physiology seen with iNO, there is still lack of evidence for distinct outcome benefits. 126 Inhaled prostacyclin (Flolan) works through a receptor-mediated increase in cyclic AMP causing vasodilation, antiproliferation of smooth muscle cells, and inhibition of platelet aggregation. Because it is more easily administered and considerably less expensive than iNO, inhaled prostacyclin has found use in cardiothoracic surgery. 127 Inhaled milrinone has also been used in cardiothoracic surgery, with evidence to support its use as an inhaled agent.128,129
Intraoperative Monitoring
Intraoperative invasive monitoring is essential to interpret and treat hemodynamic fluctuations that occur during OLV in patients with compromised ventricular function. Direct visualization of RV and LV function with echocardiography also assists in the assessment of ventricular dysfunction and response to treatment with appropriate medications.
Invasive Arterial Catheterization
Invasive systemic arterial BP monitoring assists in managing rapid variations in BP caused by ventricular dysfunction and respiratory effects of mechanical ventilation. Additionally, responsiveness to inotropes and vasoactive agents can be managed more appropriately with beat-to-beat assessment and monitoring of trends. The arterial waveform can be a sensitive indicator of preload dependence and can predict fluid responsiveness through variations in systolic BP and pulse pressure. 130
Pulmonary Artery Catheterization
Although it has not been shown that use of the pulmonary artery catheter (PAC) leads to improved rates of mortality or hospitalization, 131 it still remains a reliable tool to assess RV function, particularly when used in conjunction with echocardiography. The PAC can directly measure PAP, pulmonary capillary wedge pressure, and right atrial pressure and calculate cardiac output, mixed venous oxygen saturation, pulmonary artery resistance, and RV stroke work. Acute increases in PAP signal a rising PVR, whereas a rising CVP signals RV failure and falling cardiac output in the absence of hypovolemia, tamponade, or excessive PEEP.101,123 Additionally, a decrease in PAP can also reflect RV failure and a decrease in ejection fraction. 132 Notably, a right ventricle without preexisting hypertrophy typically cannot generate systolic PAP >50 to 60 mm Hg, though a right ventricle that is chronically hypertrophied usually can tolerate a significantly elevated PAP. 123
The PAC can also assist in assessing response to treatment with inotropes and vasoactive drugs. An appropriate response to inhaled vasodilators would be a decrease in CVP and an increase in cardiac output, with or without a significant change in PAP.
Echocardiography
TEE allows for direct inspection of the heart and can be used to determine the cause of hemodynamic instability resulting from contractility, valvular, and/or volume derangements. Although the right heart structures are less well visualized with TEE because of their anterior location, TEE can still provide useful information about RV function and response to therapy. Global and regional function of the ventricles can be assessed by calculating the ejection fraction or fractional area change and analyzing segmental wall motion abnormalities of the left ventricle. Global RV function can be assessed using the tricuspid annular plane systolic excursion. 133 It is calculated as the end-systolic to end-diastolic fractional shortening of RV length and is usually about 35%. 134 In normal patients, the systolic excursion is >25 mm. Doppler assessment of mitral inflow and pulmonary vein flow allows for assessment of LV diastolic function, whereas tricuspid inflow and hepatic vein flow allows for detection of RV diastolic function. Additionally, interventricular septal shift can determine volume overload (diastolic septal flattening) as opposed to pressure overload (systolic septal shift) of the right ventricle. Other characteristics of RV failure on echocardiogram include a dilated right ventricle, increase in tricuspid regurgitation with regurgitant peak velocities >2.5 m/s, dilated right atrium, and blunted systolic hepatic vein flow patterns. Pulmonary hypertension could manifest as a dilated and hypertrophied right ventricle (>5 mm at end diastole), dilated right atrium, dilated main pulmonary artery, interventricular systolic septal shift, and interatrial septal shift (bowing) into the left atrium, with or without significant tricuspid regurgitation.
Postoperative Analgesia
Pain control is of paramount importance for optimal outcomes in the thoracic surgical patient. Thoracic epidural analgesia has been widely used for postoperative pain management, attenuation of the postoperative stress response and associated systemic sympathetic activity, and improved pulmonary function. There is evidence to support the use of thoracic epidural analgesia in improving heart function in patients with heart failure secondary to ischemic cardiomyopathy and in minimizing adverse perioperative cardiac events.135-137
Pain associated with thoracotomy is often severe and debilitating. Although thoracoscopic surgery (VATS) utilizes smaller incisions in the chest wall, pain control must still be considered. Both thoracotomy and VATS procedures have been associated with the development of chronic pain. 138 Pain after thoracic surgery is multifactorial, resulting from direct incisional trauma, stretching of ligaments, rib retraction, and nerve injury, all of which may trigger sympathetic and inflammatory responses that are associated with the development of chronic pain. Multimodal approaches to the treatment of these diverse causes are the most effective approach. 138
A combination of local anesthetics, opioids, and NSAIDs are most frequently used in thoracic surgery patients. Local anesthetics can be delivered into the thoracic epidural, paravertebral, subarachnoid, or interpleural spaces or injected in proximity to intercostal nerves. Epidural analgesia remains the “gold standard” approach and is used routinely because it provides reliable and effective analgesia with few side effects.138,139 The thoracic paravertebral block is the most effective alternative to thoracic epidural analgesia.138,139
Conclusion
We have presented a case of a patient with severely impaired biventricular function for elective pulmonary lobectomy and have briefly reviewed physiological and management considerations. Although generally challenging to manage in the perioperative context, severe cardiac dysfunction may be particularly problematic in the thoracic surgical patient. Interactions between the cardiovascular and respiratory systems, effects of general anesthesia, PPV, hemithoracic insufflation, OLV, and contraction of the pulmonary vascular bed all serve to increase the complexity and implications of management decisions. As this patient population ages and as advanced therapies for heart failure prolong survival, we are more likely to face similar management scenarios. Thus, an understanding of the pathophysiological principles that govern interactions between cardiovascular function and anesthetic and surgical exposures becomes more important in optimizing outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.