
Abstract
There has been a paradigm shift toward “fast-track” management with early extubation (EE) in cardiac surgery. Our retrospective, matched case-control study wishes to define the benefits of EE in pediatric congenital heart surgery. We examined 50 consecutive pediatric cardiac surgery patients extubated in the operating room (February 2009 to July 2009) against a control group of delayed-extubation patients. No significant differences were found in preoperative variables except heart failure medication. Significant intraoperative variables included the following: blood products (363 vs 487 mL, P = .023), morphine (62% vs 6%, P < .0001), and inotropes (16% vs 60%, P < .0001) given. Postoperatively significant differences included hospital stay and lower inotrope scores in the early-extubation group (14.89 vs 31.68, P < .0001). The reintubation rate was not significant. EE patients have equivalent hemodynamic profiles shown by a decreased necessity for inotropic support. We conclude that EE is feasible in low-/medium-risk pediatric congenital heart surgery patients.
Introduction
Improved understanding of preoperative and postoperative physiology and advances in perioperative management strategies have resulted in significant improvements in hospital survival in children with congenital heart disease undergoing open-heart surgery. 1 There has been a paradigm shift in the perioperative management of these patients, from slow weaning of mechanical ventilation and inotropes in the intensive care unit (ICU) to a “fast-track” management strategy to promote early extubation (EE), ambulation, and hospital discharge. Many clinicians previously believed that the need for inotropic support also meant that ventilator support was automatically required. 2 Cardiac surgery studies have demonstrated that EE reduces the duration of ICU and hospital stay.2,3 The feasibility of EE in the majority of congenital heart lesions has been shown. 4 EE in the pediatric population is associated with reduced ICU and hospital stay, with no increase in morbidity or mortality. 2 In addition, 1 study reported decreased postoperative pulmonary complications. 5
Our institution initiated an EE protocol in January 2009. The aim of this study was to analyze the impact of this protocol as compared with matched case-control patients. Outcome measures included reintubation rate (failed strategy), postoperative hemodynamics, inotrope score, and narcotic use.
Methods
The research ethics board at our institution approved the study and waived the requirement for patient/parent consent. The study population consisted of 50 consecutive patients who underwent cardiac surgery using cardiopulmonary bypass (CPB) and met the criteria for EE from February 2009 to July 2009 (EE group). In this study, EE was defined as the extubation that happened in the operating room (OR). Patients who were extubated after arrival to the ICU were excluded from the study group. All patients from the initiation of the EE protocol were included. The procedures are shown in Table 1.
Diagnoses and Procedures in the Early-Extubation Group and Control Group.
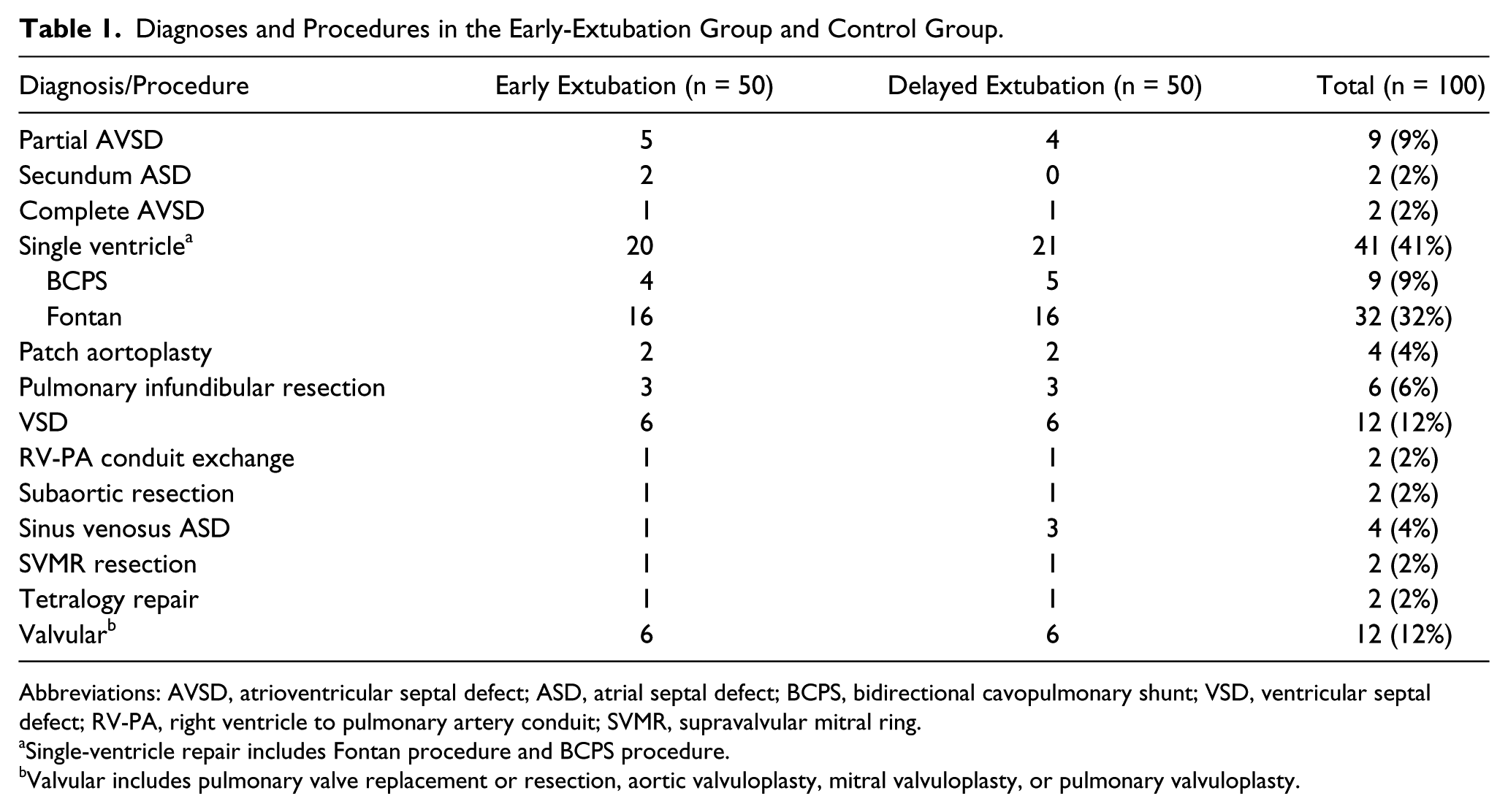
Abbreviations: AVSD, atrioventricular septal defect; ASD, atrial septal defect; BCPS, bidirectional cavopulmonary shunt; VSD, ventricular septal defect; RV-PA, right ventricle to pulmonary artery conduit; SVMR, supravalvular mitral ring.
Single-ventricle repair includes Fontan procedure and BCPS procedure.
Valvular includes pulmonary valve replacement or resection, aortic valvuloplasty, mitral valvuloplasty, or pulmonary valvuloplasty.
Indications for and Contraindications to EE
All patients were reviewed in the multidisciplinary preoperative conference. Based on the data presented, an attending anesthesiologist listed the potential candidates for EE in the OR. The absolute contraindications included severe pulmonary hypertension, preoperative respiratory failure, known difficult airway, open sternum at the end of surgery, ongoing bleeding, and significant ventricular dysfunction. Relative preoperative contraindications included neonates and major chromosomal and/or genetic abnormalities. EE for patients with chromosomal and/or genetic abnormalities was evaluated on a case-by-case basis, based on the complexity of the surgical procedure and their airway status.
Case Match Control Study
A control patient was matched to each EE group patient based on primary diagnosis and procedure, body weight, age, major chromosomal abnormalities, and past surgical interventions when possible (Table 2). Control patients were defined as those who underwent operation before January 2009 and were treated with routine anesthesia and extubation protocol, defined as the delayed-extubation (DE) group. Routine management prior to 2009 included transfer to the ICU intubated and ventilated, with anesthetic management favoring higher doses of fentanyl (20-50 µg/kg) and additional sedation as necessary. In 2009, the OR team initiated attempts to identify appropriate patients preoperatively and establish intraoperative safety criteria, which considered factors such as bleeding, respiratory failure, hemodynamic instability, and arrhythmias, in order to commit to a process of extubation prior to leaving the OR. A previous initiative involved the use of a propofol infusion to facilitate EE. 6 This strategy had not been sustained. Other preoperative factors, including prematurity, comorbidities, hemoglobin level, oxygen saturation, use of congestive heart failure medications and nutritional status, American Society of Anesthesiologists (ASA) score, Risk Adjusted Classification for Congenital Heart Surgery (RACHS) score, 7 and presence of recent infection, were taken into consideration for matching.
Preoperative Variables.
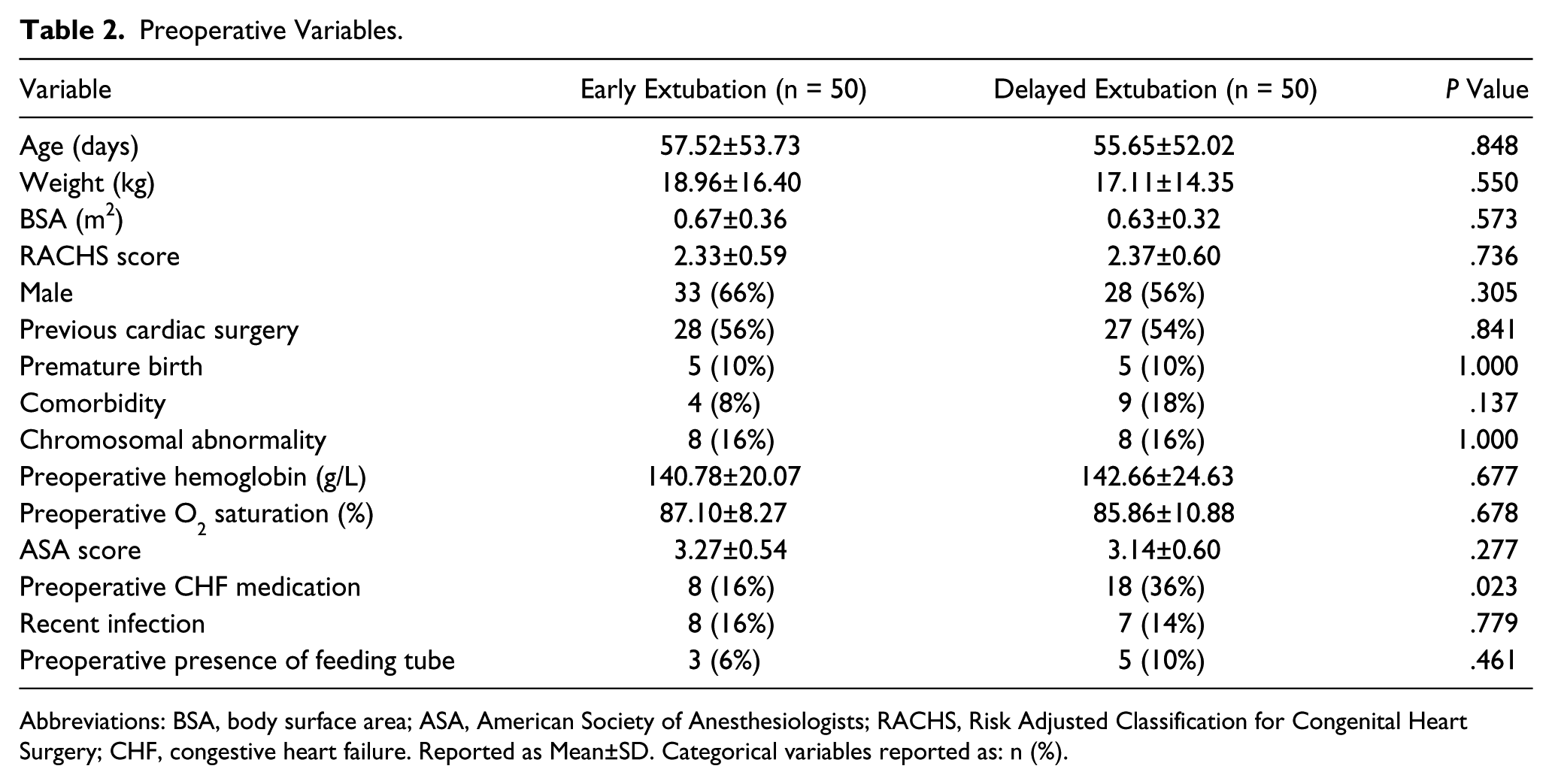
Abbreviations: BSA, body surface area; ASA, American Society of Anesthesiologists; RACHS, Risk Adjusted Classification for Congenital Heart Surgery; CHF, congestive heart failure. Reported as Mean±SD. Categorical variables reported as: n (%).
Anesthesia, Perfusion, and Surgical Strategies
Outside the neonatal period, patients were premedicated with oral benzodiazepines. All patients underwent inhalation induction with sevoflurane and maintenance with air/oxygen and isoflurane up to 1 minimum alveolar concentration. Routine invasive monitoring (arterial and jugular catheterization) and intravenous access were obtained. Fentanyl was given in incremental doses depending on the patient response. Rocuronium or pancuronium was used for paralysis and to facilitate endotracheal intubation. Tranexamic acid was given as an antifibrinolytic drug.
All operations were performed under mild or moderate hypothermic CPB. CPB was established with ascending aortic and bicaval cannulations in all cases. The hematocrit was kept at or >25% during CPB. Modified ultrafiltration was routinely performed for 10 to 15 minutes after termination of CPB. Additional blood was transfused to patients with residual cyanosis to maintain a hematocrit >30%. Transesophageal echocardiography was undertaken to assess ventricular function and residual intracardiac lesions. The final decision for EE was made by consensus between surgeons and anesthesiologists prior to chest closure. The criteria for EE included stable hemodynamics with standard doses of inotropes, normal oxygenation and gas exchange, the absence of hemodynamically significant residual lesions or ventricular dysfunction, and reasonable hemostasis with no concern for ongoing bleeding.
Assessment of Impact of EE on Postoperative Variables
Intraoperative data included hemodynamics, the amount of blood products transfused, significant intraoperative complications, CPB time, aortic cross-clamp time, serum lactate levels at the end of surgery and the use of inotropes. Postoperative data included rate of reintubation as well as data from the ICU, including vital signs, hemodynamics, duration of ventilation, inotrope use, pain medications and pain scores, fluid balance, postoperative blood products received, and chest tube drainage. A version of the Vasoactive-Inotrope Score was used to calculate postoperative use of inotropes as follows: 1 × dopamine dose (µg/kg/min) + 15 × milrinone dose (µg/kg/min) + 100 × epinephrine dose (µg/kg/min) + 100 × norepinephrine dose (µg/kg/min).8-10 Repeated variables were assessed every 8 hours for 48 hours postoperatively, with total ICU stay and hospital stay calculated.
In addition, a subanalysis was conducted differentiating between biventricular and single-ventricle patients. Single-ventricle patients underwent Fontan procedures and bidirectional cavopulmonary shunts (BCPS). All other patients had biventricular repairs.
Data Collection and Statistical Analysis
The records assessed consisted of anesthetic charts, perfusion records, operative notes, and echocardiography reports. The patients’ discharge summaries, preoperative cardiovascular surgery conference summaries, and preoperative forms were reviewed. Electronic charting systems in CIMS (Clinical Informatics and Management System) were also used to collect postoperative ICU information.
The statistical software system SAS (version 9.2, Cary, NC) was used for all statistical analyses. Continuous data were presented as means ± standard deviations, and categorical data were presented as proportions. The Student t test and analysis of variance with adjustment for multiple comparisons were used to compare continuous variables, and the χ2 test was used to compare categorical variables. An associated P value of <.05 was considered significant.
Results
Preoperative Variables
There were no differences in preoperative variables between the groups, except for the frequency of preoperative heart failure medication (P = .023, Table 2), which was higher in the DE group.
Intraoperative Variables
All patients received balanced anesthesia with fentanyl for analgesia. There were no differences in aortic cross-clamp time and CPB time between the groups (P = .634 and .244, respectively). The EE group received significantly less blood product intraoperatively (363 vs 487 mL in the DE group, P = .023, Table 3). There were no differences in hemodynamics and other parameters at the end of surgery between the groups. Intraoperative use of inotropes was significantly less in the EE group (16% vs 60% in the DE group, P < .0001). Morphine was given significantly more often in the EE group (P < .0001).
Intraoperative Variables.
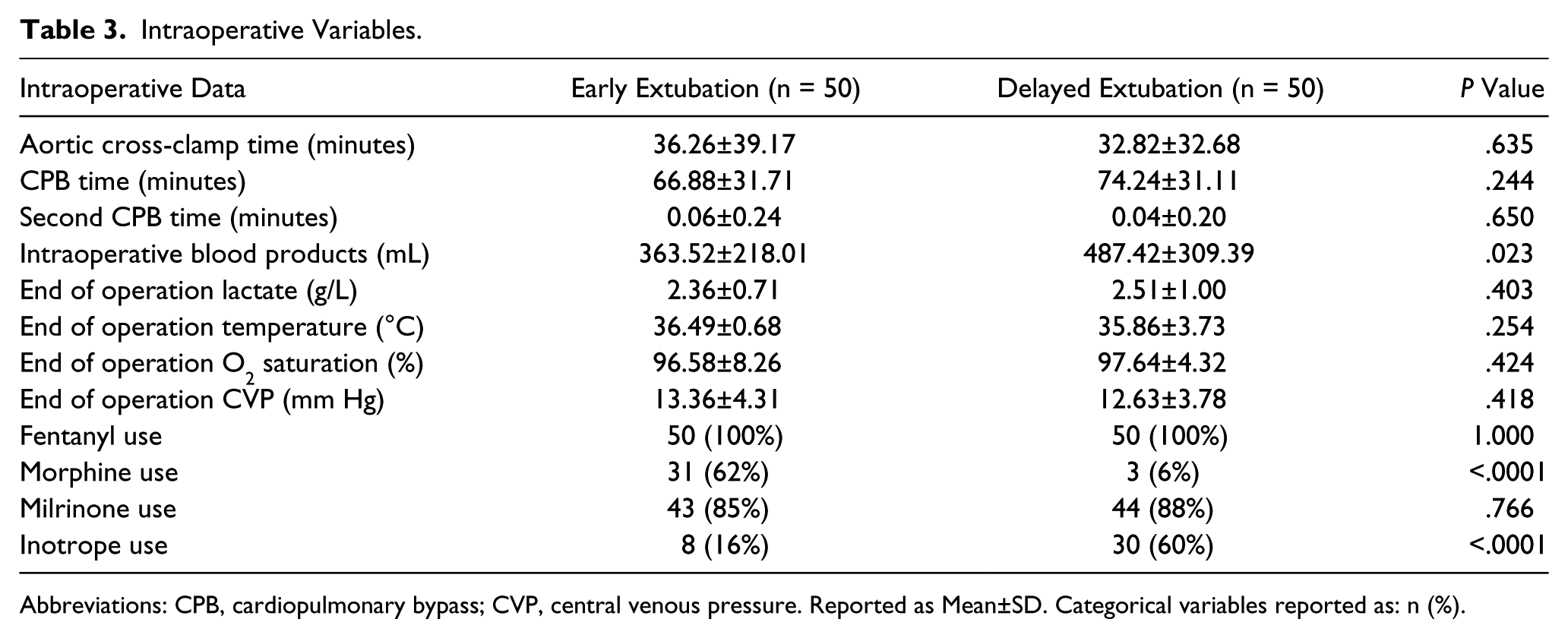
Abbreviations: CPB, cardiopulmonary bypass; CVP, central venous pressure. Reported as Mean±SD. Categorical variables reported as: n (%).
Postoperative Variables
Four (8%) patients in the EE group were reintubated in the OR. This was a result of apnea in 1 patient (ventricular septal defect closure), stridor in 1 patient (Fontan procedure), and insufficient alertness in 2 patients (atrioventricular septal defect repair and BCPS). All patients were then transferred to the ICU after reintubation, with no further complications. All patients were subsequently extubated within 3 to 18 hours. In the control group, 2 (4%) patients (BCPS) required reintubation because of desaturation (one for atelectasis and the other for tachyarrhythmia). Both patients had been extubated on the first postoperative day. There was no statistical difference in reintubation rates between the groups (P = .400).
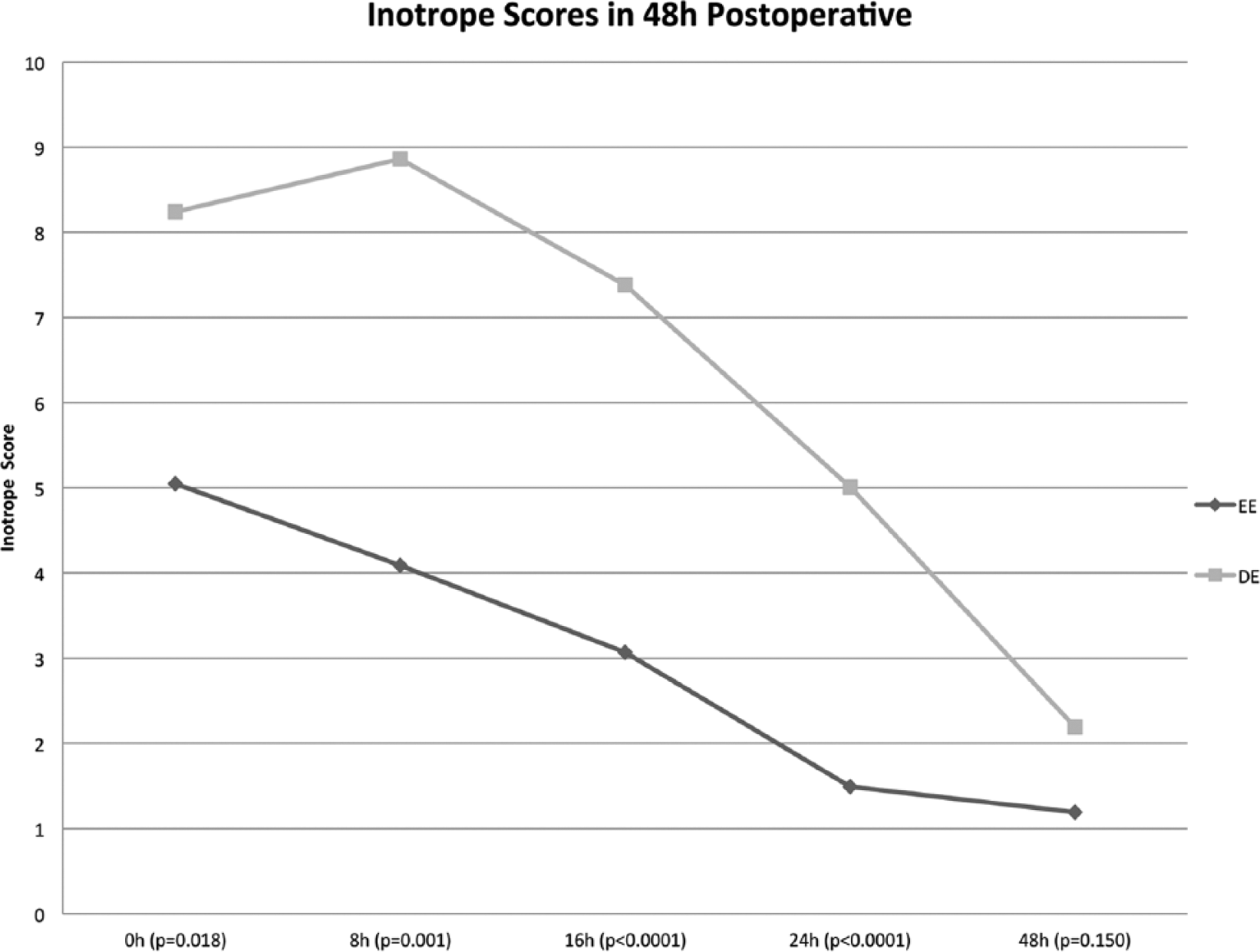
Inotrope scores at each time point in the first 24 hours and subsequent total inotrope scores were significantly less in the EE group compared with scores for those in the DE group (P < .0001, Figure 1). The duration of hospital stay was significantly shorter in the EE group (P = .047). Immediate postoperative central venous pressure (CVP) was not significant between the 2 groups (Table 3), and no significant difference was found in postoperative CVP pressures in the ICU (10.32 vs 10.77, P = .335, Table 4).
Postoperative Variables.
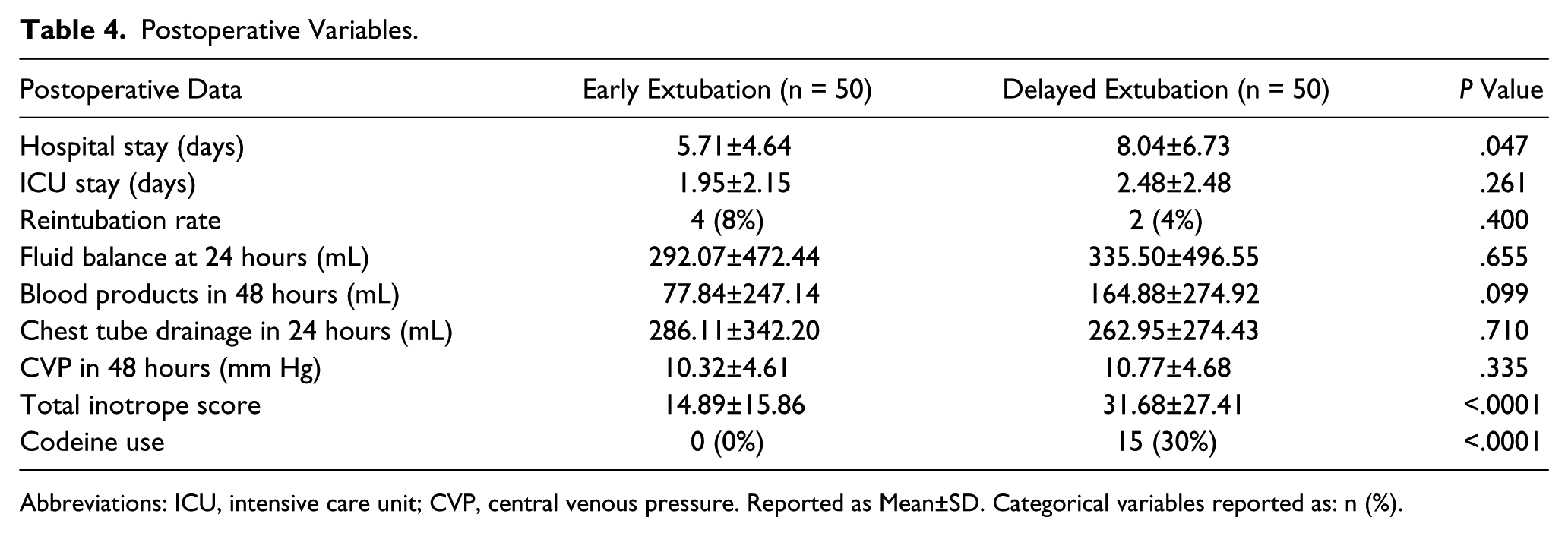
Abbreviations: ICU, intensive care unit; CVP, central venous pressure. Reported as Mean±SD. Categorical variables reported as: n (%).
Single-Ventricle Palliation
Of the entire cohort, 41 underwent single-ventricle palliation (Table 5); 20 patients were in the EE group and 21 in the DE group. Blood products given in the ICU were found to be less in single-ventricle patients in the EE group as compared with control single-ventricle patients (mean 65 vs 202 mL, P = .038). As in the analysis of all patients, no significant difference was found in immediate postoperative CVP, and ICU inotrope scores were similarly lower in the EE group. Of 6 patients who were reintubated, 4 were single-ventricle patients; 2 were in the EE group and 2 in the DE group.
Data for Single-Ventricle Patients (Fontan and BCPS).
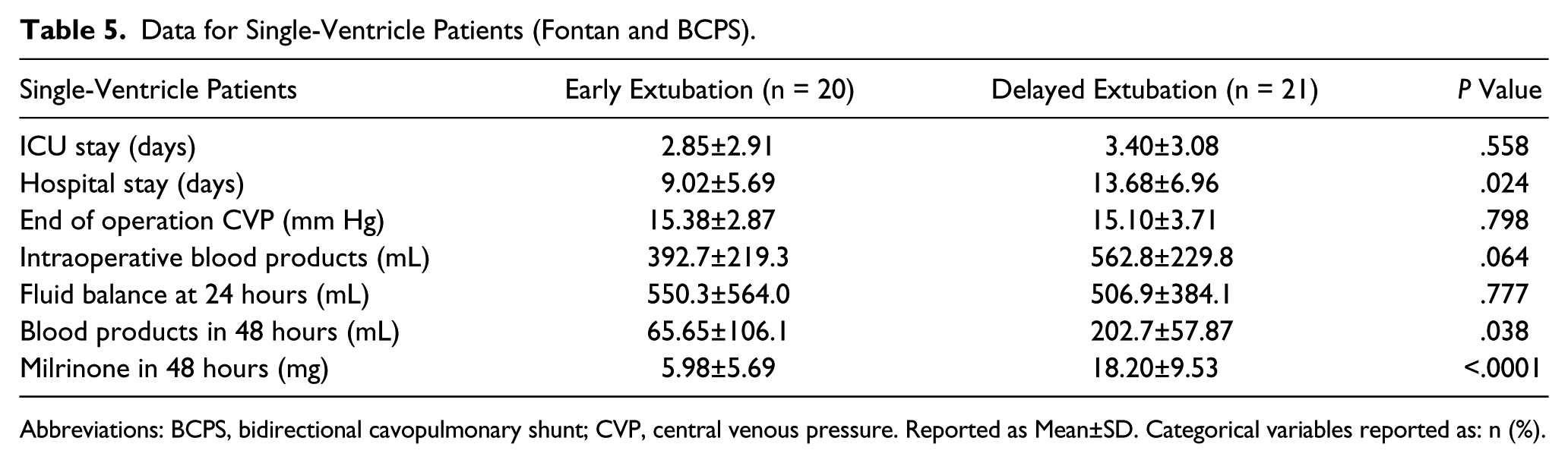
Abbreviations: BCPS, bidirectional cavopulmonary shunt; CVP, central venous pressure. Reported as Mean±SD. Categorical variables reported as: n (%).
Discussion
EE is routine practice following many adult cardiac surgery procedures. The pediatric congenital heart disease population is more varied and the surgery much more diverse. The purpose of our study was to examine the effects of a new initiative of EE on patient outcomes. We reviewed the impact of EE on immediate postoperative hemodynamics, inotrope administration, blood transfusion, and pain medication requirements. Case complexity and comorbidity were assessed through ASA and RACHS scoring systems. We confirmed previously reported benefits that include decreased hospital length of stay and faster ICU discharge times.2,3 We showed less inotrope use in the EE group. The demonstration of decreased inotrope scores with equivalent hemodynamics may indicate some degree of hemodynamic benefit following EE. The reintubation rate showed no significant difference between the groups. The subanalysis showed that the patients with single-ventricle physiology did not demonstrate greater hemodynamic benefits to EE than the main EE group, although a strong conclusion cannot be drawn based on the small number of patients in this subgroup.
Hemodynamic Advantages and Disadvantages of EE
Potential hemodynamic advantages of EE in the OR include increases in venous return and resultant increases in cardiac output. The negative intrathoracic pressure gradient would be particularly beneficial in patients with single-ventricle physiology who undergo cavopulmonary connection or patients with biventricular physiology who have restrictive physiology. Potential dose reductions of intraoperative anesthetic agents may be related to less adverse effects on myocardial performance in addition to greater ease in maintaining normal vascular tone, thereby allowing more favorable systemic blood pressures. Extubation has been shown to be associated with intrinsic catecholamine release and increases in heart rate and systolic blood pressure in the acute postoperative period.11-13 Potential disadvantages include carbon dioxide retention as a result of insufficient ventilation, which may lead to respiratory acidosis and subsequent increases in pulmonary vascular resistance. Though possibly beneficial in the recovery period, less sedative agents in the immediate postoperative period may result in increases in systemic vascular tone, which may result in excessive afterload to the systemic ventricle.
EE and Inotropes
A notable finding in this study was less inotrope requirement in the EE group compared with DE patients, regardless of the type of procedure. In other words, the EE group had equivalent hemodynamics to the DE group with less inotropic support. This fact can be explained by the potential physiological advantages of EE listed above: increases in venous return and cardiac output, intrinsic catecholamine release, and increased sympathetic stimulation and subsequent adequate vascular tone. It would be relevant to measure actual cardiac output and catecholamine levels in future studies to examine the possible positive effect of EE on those parameters. There was no evidence of adverse effects caused by EE on hemodynamic parameters in this study. Nonetheless, the study population essentially had normal ventricular function, allowing possibly better tolerance of imperfect ventilation and carbon dioxide retention. Hemodynamic advantages or disadvantages of EE in patients undergoing more complex procedures and/or with reduced ventricular function are still to be examined.
EE and CVP
We initially speculated that the CVP could be lower in the EE group because of the negative intrathoracic pressure gradients after EE. However, the results showed equivalent CVP at the end of surgery as well as in the ICU. The same trend was seen both in biventricular and single-ventricular physiologies. The results indicate that CVP may not simply be altered by the ventilator status but rather determined by multiple factors, including preload and volume status, venous vascular tone, and the right-ventricular diastolic performance. It is possible, but not likely, that the DE group did not require ventilation with significant positive airway pressures by the time of ICU admission. Although the vast majority of patients in the DE group were extubated within 24 hours, most patients left the OR in a surgical plane of anesthesia. In conclusion, there was no obvious effect of EE on CVP in this study.
Reintubation and Safety
Four (8%) patients in the EE group and 2 (4%) patients in the DE group required reintubation, but there was no statistical difference. Of those in the EE group, all were successfully extubated within 18 hours. There were no complications related to reintubation. This likely reflects the learning curve among the anesthesiologists in assessing the optimal degree of sedation and analgesia for children undergoing cardiac surgery. Given the lack of related complications, the short time to a final successful extubation, and the small number of failed extubations in the EE group (8%), we could conclude that EE was safe. Of note, 4 (66%) of 6 patients needing reintubation were single-ventricle patients, although extubation failure did not seem to be directly related to single-ventricle and cavopulmonary physiology. It is true that patients who undergo single-ventricle palliation have more significant physiological changes than patients with biventricular repair. Therefore, it is possible that a relatively subtle respiratory failure results in significant clinical consequences. Further studies are needed to define the risks and benefits of EE in patients with single-ventricle physiology.
EE and Length of Hospital Stay
Patients in the EE group had shorter hospital lengths of stay (5.71 ± 4.64 days vs 8.04 ± 6.73 days, P = .047) and observed shorter stays in the ICU (1.95 ± 2.15 days vs 2.48 ± 2.48 days, P = .261). Extubation in the OR can simplify patient management, resulting in fewer postoperative complications and a decreased necessity for subsequent procedures, thereby resulting in less-costly care. Multiple studies support the association between earlier extubation and decreased length of stay.3,14-17
Study Limitations and Future Directions
Limitations of this study include the following: the EE group had significantly less bleeding and transfusion requirements compared with the DE group, which may positively affect the postoperative parameters of the EE group compared with the DE group. Also, the EE group had significantly fewer patients with heart failure medication preoperatively, which may be related to less inotrope requirement. We did not measure cardiac output or catecholamine levels. The inability to completely match the patient’s preoperative characteristics may influence the difference between the groups, which is a limitation of the study design. Further research into the specific physiological benefits of EE in this population is needed. Detailed hemodynamic parameters, including cardiac output, could be included in future studies. Future directions will include assessment of the impact of EE on specific patient groups who may obtain the most benefit from spontaneous ventilation—for example, those with single-ventricle physiology—with a larger patient cohort.
Conclusion
We conclude that EE can be accomplished in low- to medium-risk pediatric congenital heart surgery patients without adverse effects. EE patients have hemodynamic profiles equivalent to those of DE patients with significantly less inotropic support. Single-ventricle patients are also candidates for EE, with findings similar to those in biventricular patients. EE patients have shorter hospital and ICU stays, leading to more efficient resource utilization. The benefits found in this study show the need for further investigation to facilitate defined guidelines.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.