
Abstract
Critical events during cardiopulmonary bypass (CPB) can challenge the most experienced perfusionists, anesthesiologists, and surgeons and can potentially lead to devastating outcomes. Much of the challenge of troubleshooting these events requires a key understanding of these situations and a well-defined strategy for early recognition and treatment. Adverse situations may be anticipated prior to going on CPB. Atherosclerosis is pervasive, and a high plaque burden may have implications in surgical technique modification and planning of CPB. Hematologic abnormalities such as cold agglutinins, antithrombin III deficiency, and hemoglobin S have been discussed with emphasis on managing complications arising from their altered pathophysiology. Jehovah’s witness patients require appropriate techniques for cell salvage to minimize blood loss. During initiation of CPB, devastating situations leading to acute hypoperfusion and multiorgan failure may be encountered in patients undergoing surgery for aortic dissection. Massive air emboli during CPB, though rare, necessitate an urgent diagnosis to detect the source and prompt management to contain catastrophic outcomes. Gaseous microemboli remain ubiquitous and continue to be a major concern for neurocognitive impairment despite our best efforts to improve techniques and refine the CPB circuit. During maintenance of CPB, adverse events reflect inability to provide optimal perfusion and can be ascribed to CPB machine malfunction or physiological aberrations. We also discuss critical events that can occur during perfusion and the need to monitor for organ perfusion in altered physiologic states emanating from hemodilution, hypothermia, and acid–base alterations.
Keywords
Introduction
Managing patients on cardiopulmonary bypass (CPB) can be challenging in unusual situations, particularly when the problem is unanticipated or the team members have not previously experienced these problems. Usually difficulties encountered may emanate from an underlying preexisting condition of the patient or from problems related to the surgery and/or conduct of CPB. Inadequacies in management are often multifactorial and may be a reflection of deficiencies in core competencies in one or more areas of patient care, medical knowledge, communication, practice-based learning, and or system-based practice. The objectives of this review article are to describe situations or incidents that may be encountered infrequently and recommend management strategies derived from current evidence or expert opinion.
Adverse Situations Identifiable Before Going on CPB
Severe Aortic Atherosclerosis
Ascending aortic atherosclerosis has been recognized as the most important risk factor for perioperative stroke and postoperative neurobehavioral changes. Ascending aortic atherosclerosis places the patient at risk for significantly reduced survival rate and could be responsible for spontaneous embolic stroke during their intraoperative and postoperative periods. 1 Cerebral emboli may be composed of atherosclerotic debris, calcium, air, fat, platelet thrombi, or CPB tubing. 2 Increased awareness of the dangers of severe ascending aortic atherosclerosis is critical in order to avoid the devastating complications from stroke and possibly postoperative neurocognitive dysfunction. The usual technique employed for going on CPB involves the surgical manipulation of the aorta for cannulation, application of clamps, and the delivery of cardioplegic solution. The construction of proximal anastomoses for coronary artery bypass grafts, or valve replacement or repair, can also produce a shower of atherosclerotic debris in the circulation. The challenge is to recognize such hazardous situations and attempt to select a section of the ascending aorta for instrumentation that displays limited or no atherosclerotic changes.
Intraoperative assessment by palpation of the ascending aorta is unreliable. However, intraoperative transesophageal echocardiography (TEE) of proximal ascending aorta and epiaortic ultrasound (EAS) are considered more reliable tools in the diagnosis of ascending aortic atherosclerosis. These imaging modalities help diagnose and determine the location, thickness, and anatomic structure of the aortic atheroma. High-grade atheromas are at risk for plaque disruption and embolization and include grade 4, sessile atheroma protruding at least 5 mm into the aortic lumen, and grade 5, mobile protruding atheroma. The presence of mobile components or ulceration and calcification in the atheroma are also associated with a higher risk for thromboembolism. 3 Even the presence of moderate atherosclerosis (aortic plaque thickness 3 to 5 mm), of the ascending aorta, has the potential for causing delayed postoperative stroke. The ascending aorta showing moderate atherosclerosis on EAS prior to aortic cannulation can produce new lesions showing mobile atheromatous plaques at the sites of aortic instrumentation following aortic decannulation. The incidence of these new lesions was reported to be as high as 33.3% if the plaque thickness exceeded 4 mm, but only 0.8% when it was less than 3 mm. These newly formed lesions were mediated by intimal injury from clamping or cannulation of the ascending aorta and occurred in 3.4% as found in a study of 472 patients who underwent cardiac surgery. 4 Other mechanisms that can disrupt a stable atheroma during CPB could include a sandblasting effect caused by the erosive effect of the high-velocity jet from an aortic cannula. 5
Although the superiority of EAS for evaluation of aortic atherosclerotic lesions is clearly established, 6 it is still unclear whether appropriate surgical modifications guided by the findings of EAS translates into an actual reduction of early postoperative stroke rate. Several small-scale studies using EAS criteria to screen for high-risk patients requiring avoidance of aortic manipulation have shown a decrease in stroke rate or neurocognitive dysfunction.7,8 In a prospective, randomized study the use of EAS resulted in modifications to the intraoperative surgical management in 29% of patients randomized to EAS compared with 12% of patients who were randomized to manual assessment by palpation of the ascending aorta. Interestingly, the use of EAS was not associated with any alterations in the NIH stroke scale or with a decrease in transcranial Doppler (TCD) detected cerebral embolization before or during CPB compared with patients randomized to manual aortic palpation. 9
Since the manipulation of the ascending aorta is routine and often unavoidable in patients undergoing cardiac surgery with CPB, the routine use of TEE and EAS is recommended to minimize the devastating and disabling consequences of stroke and neurologic injury. These imaging modalities are an accurate, easily accessible tool and allow for sensitive point-of-care diagnosis of atherosclerosis. 10
Nevertheless, TEE has certain limitations, as it does not always visualize plaques present in the distal ascending aorta and proximal aortic arch due to air-filled trachea and left main bronchus interposed between esophagus and distal ascending aorta. EAS is the most sensitive method for detecting high-grade ascending and arch aortic atheromas at the time of surgery, thereby allowing changes to the intraoperative plan and technique for CPB. These modifications would include changing the ascending aorta cannulation site to axillary artery or other alternative sites for CPB, avoiding partial occlusion clamps for proximal bypass graft anastomosis by using a “single cross-clamp” technique, the avoidance of aortic cross-clamping by using ventricular fibrillatory arrest during surgery, using all arterial bypass grafts to avoid proximal anastomosis, performing circulatory arrest and replacing the ascending aorta, or by conversion to off-pump surgery. 11
The reduction of emboli and neurologic injury during CPB requires a multidisciplinary approach with advances in perfusion technology, CPB techniques, and surgical strategies geared toward preventing neurologic injury during cardiac surgery. One of these strategies typically employed during off-pump coronary artery bypass grafting (CABG) includes the “no-touch” technique. This technique avoids using all types of clamps in the aorta. Antegrade cardioplegia cannot be provided, and no grafts are anastomosed to the aorta. As such pedicled arterial grafts for myocardial revascularization (eg, internal mammary artery or gastroepiploic artery) serve as conduits for coronary bypass grafts. No touch techniques in patients with severe atherosclerosis (aortic wall thickness >5 mm) may avert an increase in the incidence of stroke. While performing off-pump CABG, partial clamping of nondiseased segments is permissible in case of mild atherosclerotic lesions located in the posterior wall of the ascending aorta. 12 This technique is also considered safe and effective as it avoids clamp injury or atheroembolism in patients with a calcified aorta. 13
Other surgical strategies advocated for the avoidance of thromboembolic events include utilizing the axillary artery for arterial cannulation. Axillary cannulation is preferred in patients with extensive high-grade aortic atherosclerosis as it provides adequate arterial inflow and minimizes the risk of retrograde atheroemboli and stroke. 14 Axillary cannulation also provides a safe and feasible alternative to the femoral artery in aortic dissection, as it reliably provides antegrade aortic flow through the true lumen decreasing the risk of visceral organ malperfusion. 15
Circulatory arrest with/without cerebral perfusion in combination with deep hypothermia may also be considered when the aorta has severe atherosclerosis. Mild hypothermia along with selective antegrade cerebral perfusion (ACP) has been used in circulatory arrest, but optimal flow rates and time limitations are unknown. 16 Results from 1002 patients receiving unilateral or bilateral ACP while undergoing complex aortic arch repair reveal that using mild systemic hypothermia (28°C to 30°C) is a safe option and make deep hypothermia nonessential for aortic arch replacement. Unilateral ACP offers similar brain and visceral organ protection as bilateral ACP and may be safer in that it minimizes the risk of embolism arising from surgical manipulation on the arch vessels. 17 A cannula tip directed toward the aortic arch (standard direction) is likely to generate high flow velocity and turbulence, which may adversely affect an aneurysmal wall or a severely atherosclerotic aortic arch. The effect of cannula tip direction on flow within the transverse arch has been studied by performing hydrodynamic analysis using particle image velocimetry in glass perfusion models of healthy and aneurysmal aortic arches. The study suggests that directing the tip of the aortic cannula toward the aortic root instead of standard direction may be beneficial in aneurysmal aortic arch disease as a slower and less turbulent flow is generated in the transverse arch. 18
Hematological Concerns
Cold Agglutinins (CA)
Cold agglutinins are serum antibodies directed against antigens on the red blood cells that become active at low blood temperature, thus resulting in increased blood viscosity, microvascular occlusion, red cell hemolysis, or clumping and agglutination of red blood cells. Although cold agglutinin disease is a rare condition, the risk to patients necessitates an increased awareness of cold agglutinins and screening.
In CA the thermal amplitude is the highest temperature at which an antibody binds to red blood cells, and a subsequent drop in temperature below this threshold leads to an exponential increase in antibody activity. Rewarming reverses antibody activity but activates the complement system leading to hemolysis in patients. The antibody binding and complement fixation are effective at low temperature whereas complement is more lytic at higher temperature. For hemolysis to occur, the temperature must be low enough for the cold agglutinins to activate but warm enough for the complement fixation to occur. 19
Both monoclonal and polyclonal cold agglutinins account for CA. Polyclonal antibodies are transient and occur following acute infections such as mycoplasma, infectious mononucleosis, or cytomegalovirus and may be responsible for acute life-threatening intravascular hemolysis.20,21
Patients with CA are rarely symptomatic since CA activation most often occurs at temperatures well below the usual range of body temperature. However, the hypothermic environment during CPB, with low systemic (22° to 36°C) and coronary (as low as 8° to 12°C) temperatures are likely to trigger adverse sequelae in the presence of cold-active antibodies. Cold agglutinin screening is performed in some centers before cardiac surgery, as prolonged hypothermic CPB can cause lethal complications of hemolysis, microvascular occlusion, and organ failure. Adverse outcomes such as myocardial infarction, stroke, or acute renal failure may be attributed to another cause if the presence or clinical suspicion of CA has been missed. Thus, the clinical suspicion for CA is aroused in patients who have not been previously screened for CA but now manifest signs of hemoglobinuria. In addition, agglutination may be seen in the cardioplegia delivery system as the blood is cooled.21,22
In a review of literature, the authors noted that the presence of CAs did not promote the institution of a unique care plan that meaningfully improved patient CPB outcomes. In the review, the presence of CAs was noted in 0.3% of patients. The surgical team’s response was variable with only one third of patients avoiding hypothermia on CPB. After further antibody verification the initially identified CA-positive patients were found to have true cold agglutinins in only 43% of the cases. As such, modification of CPB to avoid hypothermia did not decrease adverse events. 23 A distinction was made by the authors between patients with CA and those with cold hemagglutinin disease. 24 CA patients harbor the cold agglutinins only, whereas those with cold hemagglutinin disease have true cold hemagglutinins, which is responsible for agglutination or hemolysis of blood at low temperatures. Since there is a paucity of evidence looking at randomized appropriate interventions to CA/cold hemagglutinin disease, we recommend that all these patients be managed with normothermic goals. Management goals in CA-positive patients are to maintain the patient’s blood temperature above the thermal amplitude throughout their hospitalization including the use of normothermic CPB with warm myocardial preservation techniques to prevent fatal complications. Patients with cold agglutinin disease should undergo laboratory testing to obtain precise information in dealing with CA antibodies. CA titers, thermal amplitude, and hematology consultation are helpful before cardiac surgery 24 (Table 1).
Strategies for Managing Patients with Cold Agglutinins.
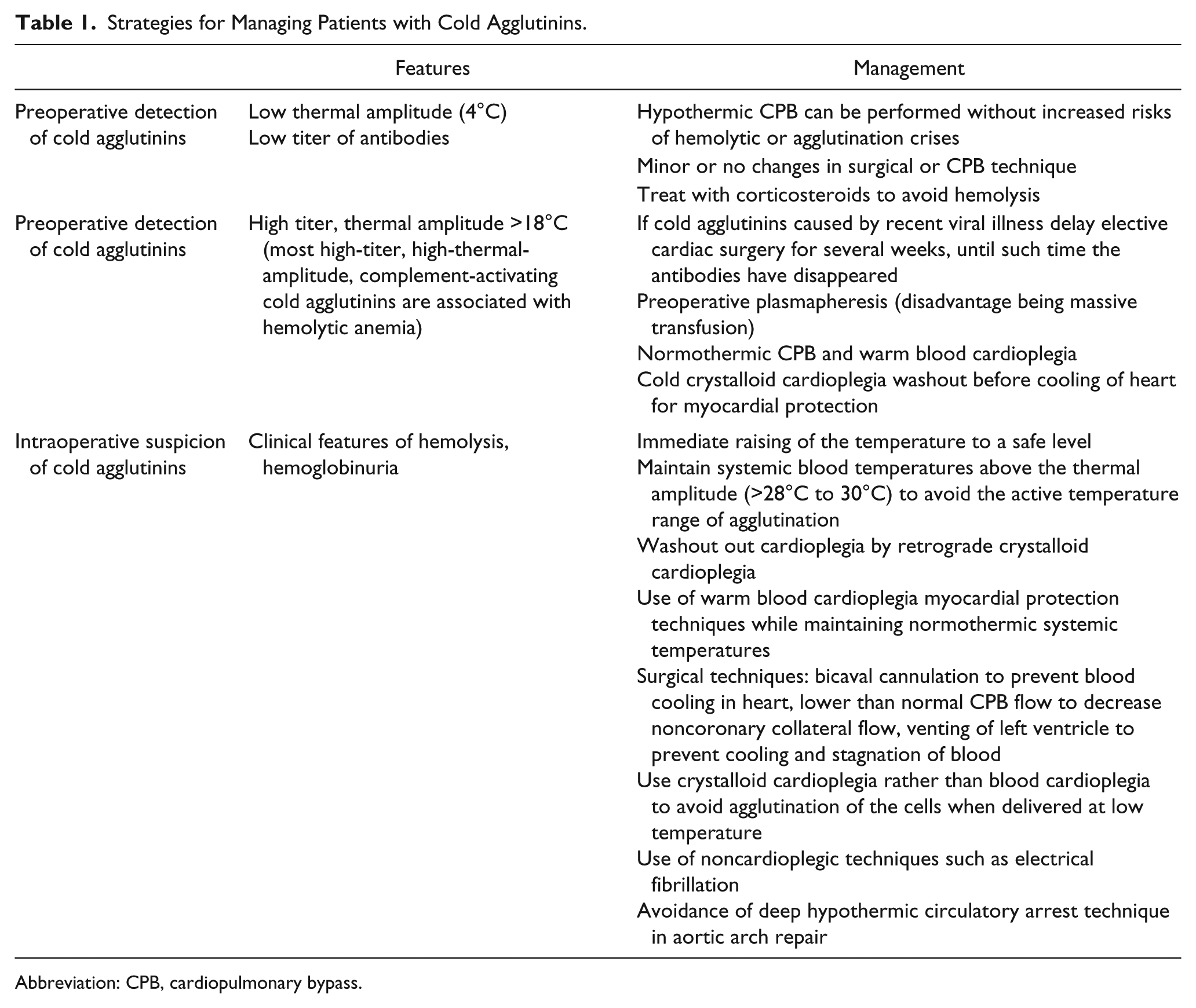
Abbreviation: CPB, cardiopulmonary bypass.
Antithrombin III Deficiency
Normal blood coagulation depends on the delicate balance between the procoagulant system and the inhibitors of coagulation, of which antithrombin (AT) is the most important. AT is a serine protease inhibitor synthesized in the liver and functions by binding and irreversibly neutralizing thrombin as well as factors IX, X, XI, XII, kallikrein, and plasmin. In the circulation, AT exists in a form with low inhibitory activity. However, in the presence of heparin, its activity is accelerated at least a thousand times. Although AT affects multiple coagulation factors, only its action on thrombin and factor Xa has clinical significance. 25 Patients who have a deficiency in AT levels are at increased risk of thromboembolic events. In the operating room, these patients exhibit a resistance to heparin administration and are at higher risk for not only developing thrombi during CPB but also for developing a consumptive coagulopathy due to activation of inflammatory and hemostatic pathways, increasing the risk for neurologic injury as well as excessive bleeding after separation from bypass. 26
AT deficiency can be congenital or acquired. Congenital AT deficiency is an uncommon autosomal dominant disorder—prevalence anywhere between 1 in 500 and 1 in 5000 has been reported. Although more patients have qualitative rather than quantitative factor defects, it is far more common for patients with quantitative defects to exhibit symptoms. Acquired forms arise from increased factor consumption, loss from the intravascular compartment (nephrotic syndrome or renal failure), or liver failure. 25 Mild factor deficiencies are not associated with clinical symptomatology. AT activity does not become clinically important until levels fall below 50%. The normal range is over 80% activity. 26 In the cardiac surgical population, acquired deficiencies, secondary to increased consumption, are more common. The natural activity of heparin and AT forms AT–heparin complexes, which are rapidly cleared. Prior to CPB, heparin is usually given as a bolus dose of 300 to 400 units/kg, 3 to 5 minutes prior to initiation of bypass. This bolus dose creates a large number of heparin–AT complexes, and after rapid clearance, the AT level is reduced by 30%. Dilution by the CPB circuit further decreases the AT level. 27 If AT levels are not restored, heparin resistance, or the failure of a specific heparin dose to produce a prolonged activated coagulation time, may occur. Multiple other factors can contribute to heparin resistance in this population of patients. These include endocarditis, the presence of an intra-aortic balloon pump, shock, thrombocytosis, and previous heparin exposure, among others. Only rarely does heparin resistance lead to visible clot in the CPB circuit—the far more important result is the activation of inflammatory and hemostatic mechanisms, which leads to thrombin formation, platelet and factor consumption, and excessive fibrinolysis. These sequelae produce a prothrombotic state, placing the patient at risk for embolic neurologic injury. 28
A common treatment of heparin resistance is to administer more heparin. While this practice may produce adequate anticoagulation as measured by the activated clotting time, it further exacerbates the AT deficiency via the pathway described above. 29 Another option for treating AT deficiency is the administration of fresh frozen plasma (FFP). However, this has been found to be inferior compared with the use of AT concentrate. Large disparities have been found in AT levels measured in patients treated with FFP versus those treated with AT concentrate. 26 Some studies have shown that AT supplementation in the presence of heparin resistance leads to statistically significant improvement in biochemical hemostatic markers. This may indicate improvements in outcomes based on decreased platelet activation and factor consumption; however, outcome studies have failed to bear out clinical improvements such as decreased chest tube output and decreased transfusion requirements.28-30
A 75 µg/kg bolus dose of recombinant AT over 10 to 20 minutes effectively treats low AT levels pre-CPB, and it is helpful in managing patients with both congenital and acquired AT deficiency.27,28,31 With the other risks involved with the administration of FFP (alloimmunization, transfusion related lung injury, volume overload, etc), the use of these products for the treatment of low AT levels should be discouraged. A few prospective studies have shown that AT levels below 58% post-bypass are predictive for higher chance of re-exploration, adverse neurological outcomes, thromboembolic events, and prolonged intensive care unit stays. 32 Post-bypass AT levels are correlated with low pre-bypass AT levels, prolonged CPB time, and preoperative heparin use. 33 Postoperatively, AT levels will continue to decline. The rate of decline depends on the extent of tissue disruption and hemorrhage. AT levels will reach their lowest 3 days postoperatively and return to normal by the fifth postoperative day. Beyond this time period, supplementation of AT levels is no longer required. 34
Blood Transfusion in a Jehovah’s Witness
Because of their beliefs, cardiac surgery and its associated large-volume blood loss, along with potentially long bypass times and microvascular bleeding, are particularly dangerous for Jehovah’s Witnesses (JW). Since randomized controlled trials are impossible with this population, the strategies used to minimize blood loss and prevent transfusion come from case reports and retrospective analysis. These strategies rely on 3 principles: (a) correcting preoperative anemia, (b) minimizing perioperative blood loss, and (c) using lower hemoglobin-based transfusion triggers. 35
Multiple medical, surgical, and perfusion strategies that allow JW to undergo cardiac surgery safely have been described in the literature. From a medical standpoint, the use of preoperative erythropoietin injections, folic acid, and iron supplementation to increase preoperative hemoglobin level (goal >15 g/dL) has been shown to be potentially beneficial. In addition, a detailed discussion regarding what factor concentrates, if any, are acceptable to the patient is necessary. 35 The use of antifibrinolytics during the case can minimize clot breakdown and further blood loss. Normovolemic hemodilution and controlled hypotension can be employed to further minimize blood loss, as long as end-organ perfusion is not compromised. 36 In addition to these items, strict volume management strategies must be used. Trendelenburg positioning and vasoactive drugs can be successfully used to maintain hemodynamic stability, as well as help with the desires for strict volume control. Fluid overload from liberal intravenous administration should be avoided, since it is associated with coagulopathy and poorer long-term outcomes. 37
Perfusion strategies include the use of minimal-perfusion circuits, small prime volumes, and retrograde autologous priming. A concern with minimal-perfusion circuits is their ability to handle air entrainment (see section on Micro Air Embolism), although there are circuits that incorporate an auto-sensor for air entrainment and stop venous inflow to allow for manual de-airing if entrainment is detected. Retrograde autologous priming is another blood conservation technique that may be considered to limit the severity of hemodilution during CPB and decrease perioperative transfusions. The use of small prime volumes and retrograde autologous priming, in which 800 to 1000 cc of the patient’s blood is used to displace the prime solution in the CPB circuit, by gravity drainage into the venous limb, or passive pressure gradients in the arterial limb, allow for less hemodilution and prime volumes as low as 100 to 200 mL. 38
In addition, there are multiple surgical techniques that can be employed to minimize blood loss during cardiac surgery. Off-pump bypass has been noted to preserve hemoglobin levels and prevent platelet dysfunction associated with CPB. If valve surgery is required, consideration should be given to transfemoral or transapical techniques, if possible, as these techniques allow for avoidance of CPB altogether. Having senior surgeons perform these surgeries, with absolutely meticulous attention to hemostasis, leads to better outcomes. 35 Discard suction and laparotomy pads should not be used, as these techniques do not allow for salvage of lost blood. 37 Avoiding hypothermia has also been shown to be helpful in the prevention of blood loss, as has the use of bone wax, fibrin glue, and other hemostatic agents. 35 When microvascular bleeding occurs, the use of recombinant factor VIIa should be considered early in this population. 30
The group headed by El-Essawi et al documented their experience with 29 JW patients over a 5-year period. Using minimized perfusion techniques, their patients’ mean hemoglobin after bypass was 10.1 g/dL. 33 The group led by Emmert et al described 0% mortality with 16 JW over a 5-year time span, again utilizing some of the previously mentioned techniques. 30 In addition, numerous case reports exist in the literature showing that cardiac surgery can be performed in the JW population safely and without large increases in morbidity and mortality.36,37
Problems Encountered During Initiation of CPB
Malperfusion Syndrome During Aortic Cannulation in Type A Aortic Dissection
Malperfusion syndrome has been described as the situation where there are low pressures in both radial arteries and a high back pressure in the arterial cannula utilized for CPB. The cause of organ malperfusion during CPB in aortic dissection is from the dissection of the organ vessels themselves or by compression of the origin of these vessels by the false lumen. Patients undergoing surgery for type A aortic dissection may have preexisting organ malperfusion or may develop intraoperative malperfusion with initiation of CPB. Intraoperative malperfusion syndrome may be diagnosed by TEE and monitoring both radial arteries, which may produce a loss or decrease in pressures on initiation of CPB. Diagnosing malperfusion is critically important as complications from aortic cannulation can compromise cerebral perfusion. Additional tools used as part of the multimodality assessment for detection of cerebral ischemia would include Doppler monitoring, near-infrared spectroscopy (NIRS), and electroencephalography (EEG). Monitoring of TCD serves a dual purpose in that it provides a quantitative description of cerebral microemboli as well as measure velocity of the middle cerebral artery (MCA) through temporal-bone ultrasonic windows. TCD does not directly measure cerebral blood flow (CBF) since the flow velocity of red cells is influenced by vessel diameter. However, a change in TCD velocity does correlate closely with a change in CBF allowing instantaneous recognition of cerebral hypoperfusion. 39
While various cannulation routes have been used for the systemic perfusion, not a single route is considered perfect. 40 As such, the optimal cannulation site for repair of acute ascending aortic dissection continues to be controversial. The traditional approach for aortic access during CPB is by femoral cannulation as it can be performed expeditiously in patients with hemodynamic instability. In a review of the subject initial femoral artery cannulation has been considered an acceptable risk in patients undergoing repair of type A aortic dissection. In this study, 104 of 107 patients underwent surgery without perfusion abnormalities whereas only 3 patients developed intraoperative malperfusion. 41
However, femoral cannulation is not a fail-safe technique. Malperfusion from flow directed in a false lumen from dissection of the femoral artery is a distinct possibility. 42 Surgeons have considered alternate cannulation sites for antegrade perfusion as there are continuing concerns with malperfusion from retrograde femoral perfusion causing embolization of thrombi and atheromatic debris within the true lumen. The presence of a dissection of the femoral artery, severe atherosclerotic aortic disease, and lower limb ischemia are thus considered contraindications to retrograde femoral artery cannulation.
Antegrade perfusion through the axillary artery is preferred in type A aortic dissection.43,44 However, even axillary artery dissection is not completely safe as it can lead to antegrade carotid dissection and cerebral malperfusion if there is subsequent dissection of the subclavian or brachiocephalic trunk. Approximately 5% of patients required alternate cannulation as problems may be encountered following axillary cannulation. 45
Another technique, transapical aortic cannulation (TAC), consists of the insertion of the arterial cannula through the apex of the left ventricle and the aortic valve with the tip lying within Sinus of Valsalva. TEE guidance is needed for correct cannula placement. CBP is quickly established using this technique and it provides a more physiological method of delivering antegrade arterial flow while assuring perfusion of the true lumen in aortic dissection. 46 Wada et al described TAC in 138 patients with type A aortic dissection. A flexible cannula was inserted through the left ventricular apex and across the aortic valve and positioned in the ascending aorta under TEE guidance. CPB flow was adequate and there was no need to change site of cannulation. 47
Direct aortic true lumen cannulation is a promising standard arterial cannulation technique whereby antegrade perfusion can be easily achieved with temporary circulatory arrest. Cessation of circulation is first achieved by draining venous blood into the CPB system followed by transection of the dissected ascending aortic to identify the true lumen. 48 The manipulation can be performed within 30 seconds and no technical problems or permanent neurologic disorders were encountered in a series of 176 patients. 49
Detection and Prevention of Gaseous Microemboli During CPB
The occurrence of massive air embolism has been nearly eliminated due to increased awareness of etiologies and technological advances. 50 However, existing CPB circuits do not offer good protection from gaseous microemboli (GME) that can inadvertently enter the bypass circuit both from the surgical field and during interventions performed by the perfusion technician. GME are generated from the components of the extracorporeal circuit and/or during surgical manipulation in open heart procedures. These sources are the major culprits in the delivery of GME leading to adverse neurologic sequelae. GME formed in the CPB circuit can contribute to the risk of cerebral injury during CPB. A correlation was seen between intraoperative GME intensity and neurocognitive tests, suggesting that the level of GME may be responsible in determining the psychological outcome after CABG with CPB. 51 The design of the oxygenator and reservoir and the use of vacuum-assisted venous drainage (VAVD) have an influence on the delivery of existing GME to the patient. Bubble oxygenators have historically been the most commonly reported source with GMEs. Subsequent changes in design along with chemical defoaming agents, arterial line filtration, and maintenance of a low gas-to-blood flow ratio of 1:1 significantly reduced the numbers and sizes of GME produced by bubble oxygenators. Membrane-type blood oxygenators, however, have not been commonly implicated as a source of GME. 52
GME is quantifiable by means of a TCD, which monitors the quality of extracorporeal perfusion and tracks microemboli in CPB circuits. It has been noted that up to 1000 microemboli per second at flow rates ranging from 0.2 to 6.0 L/min can occur. 53 Significant neuropsychological injury has been attributed to increased loads of GME, and this makes for a compelling case for strict observance of practices aimed in reducing the incidence of GMEs. GME exacts its toll by triggering inflammatory changes and subsequent disruption of the cerebral microcirculation, vascular endothelium, and the blood–brain barrier.
Venous air is not completely removed in open hard-shell venous reservoirs. Microbubbles were measured in 3 different reservoirs (Maquet, Sorin, and Medtronic) at different levels after the reservoir and after the arterial filter with a GAMPT BCC200 detector. The authors noted a lower reservoir level resulted in a moderate rise in microbubbles passing the reservoir. Bubble volume from the Sorin reservoir was markedly lower after the arterial filter than from the Medtronic and Maquet reservoirs. The minimum levels recommended by the manufacturers were safe. 54
The use of cardiotomy suction causes an amplification of systemic inflammatory response and a resulting coagulopathy, as well as exacerbation of the microembolic load. This leads to a tendency toward increased blood loss, transfusion requirement, and organ dysfunction. Filtration techniques should be used to remove GME from cardiotomy suction. These are larger bubbles, consist of air (mostly nitrogen), and hence are more stable. It is appropriate to reconsider routine use of cardiotomy suction in on-pump coronary artery surgery. 55
Centrifugal pump (CP) and roller pump (RP) designs are the main arterial pumps used in CPB. GME can be produced by vaporous cavitation, which occurs when a vacuous space is created in blood, within the negative pressure regions that develop behind the roller pump heads. However, in a recent meta-analysis comparing outcomes in RP and CP, there was no reported pump-related malfunction or mishap. There was no significant difference for hematological variables, postoperative blood loss, transfusions, neurological outcomes, or mortality. 56 Pulsatility of flow during CPB leads to GME increment by splitting and size diminishing of the existing bubbles but not by additional gas production. Increased pump flow rate and pulsatile flow during CPB has the potential to deliver more GME at post-pump site. 57
Vacuum-assisted venous drainage is usually applied to optimize venous drainage during bypass. The major advantages of VAVD are a significant decrease in CPB prime volume, which helps improve blood conservation and prevent drawbacks of transfusion (immunomodulation, infection). However, there have been concerns regarding an increased incidence of gaseous microemboli. These drawbacks are usually avoidable through appropriate training of perfusionists. 58
Air emboli can be introduced when the cardiac chambers are opened to the atmosphere for valvular, atrial septal, or ventricular septal repair. Air entrainment can occur from aortic, venous cannulation sites or with placement of a left atrial or left ventricular vent cannula.
Blood obtained during cardiotomy suction (CS) is a source of lipid rich emboli and has the ability to cause a pronounced systemic inflammatory response and a resulting coagulopathy if re-infused. Similar to GME, the large particulate load of microemboli can cause microcirculatory derangements. CS blood contains fat, bone, lipids, and other debris from the surgical field that enters the CPB circuit, ultimately obstructing the microcapillary circulation of the patient. CS blood administered through a cell saver before return to the CPB circuit significantly reduced blood lipid content and thereby the inflammatory effects compared with filtering only. 59 On the other hand, processing large quantities of blood with a cell saver produce thrombocytopenia and/or dilution of coagulation factors leading to bleeding with high rates of blood transfusion.
Processing of shed (CS) blood with cell saver before transfusion of may limit cerebral microembolization and reduce cognitive decline after surgery. 60 More recently, large studies have shown that, while CS blood is undesirable because of its pathological potential, the direct re-infusion of CS and residual pump volume (RPV) after CPB potentially lowers the risk of transfusion and is no more harmful to the patient than the re-infusion of cell salvage-processed CS after CPB. 61 The issue of dealing with CS and RPV at present is unclear in the absence of high-quality evidence and is influenced by institutional preference.
Troubleshooting issues related to air embolism and neurologic complications first requires a heightened awareness among perfusion technicians, surgeons, and anesthesiologists. The design of the oxygenator and reservoir and real-time monitoring of gaseous microemboli in the arterial and venous line have all had a significant impact in the reduction of GME. Gravity-assisted drainage in a primed line leads to significantly less emboli as compared with the use of VAVD with a higher negative pressure (−40 mm Hg) in an unprimed line. As such the safe use of VAVD necessitates refinement of perfusion techniques. These include utilization of oxygenator and arterial filters with sufficient air handling capabilities, use of low set intensity vacuum to assist in full venous return, and the real-time monitoring of gaseous microemboli in the arterial and venous lines.62,63 Other techniques such as the use of smaller venous cannulae, shorter circuit tubing, and lower priming and blood transfusion volumes can increase the risk of arterial gaseous microemboli and blood trauma.
The concept of using hypobaric oxygenation during CPB to reduce dissolved gases in blood holds great potential for limiting end-organ damage by drastically reducing GME delivery. Variable subatmospheric pressures were applied to 100% oxygen sweep gas in standard hollow fiber microporous membrane oxygenators to oxygenate and denitrogenate blood in animal models. Compared with current practice standards of oxygen/air sweep gas, hypobaric oxygenation reduced GME volumes to achieve their near-total elimination during CPB. 64
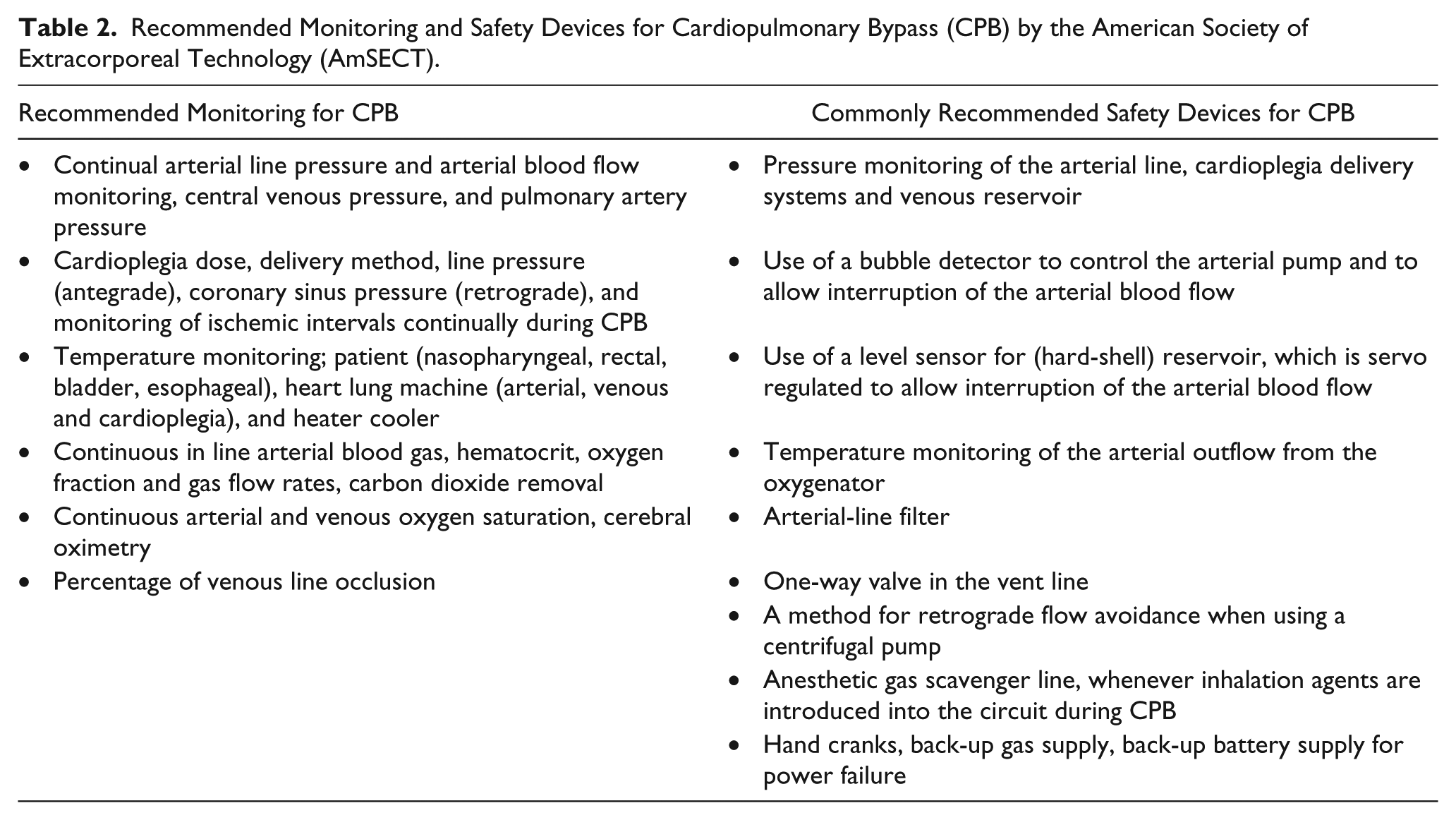
The American Society of Extra Corporeal Technology (AmSECT; http://www.amsect.org) recommends development of an institutionally based protocol for conduct of CPB. Safety devices, monitoring, and communication are emphasized, and the perfusionist is encouraged to use a checklist for each CPB procedure. Monitoring and safety devices can prevent or attenuate problems inherent to perfusion and are considered the standard of care as shown in Table 2.
Recommended Monitoring and Safety Devices for Cardiopulmonary Bypass (CPB) by the American Society of Extracorporeal Technology (AmSECT).
Novel microemboli detectors, such as the Emboli Detection and Classification (EDAC) Quantifier (Luna Innovations, Roanoke, VA) and Bubble Counter Clinical 200 (GAMPT, Zappendorf, Germany), have helped perfusion technicians to discover the sources of entrained air and reduce the source of unrecognized air emboli. The use of EDAC quantifiers that have a higher sensitivity as a detection modality have been linked to higher counts during events such as CPB initiation, heart manipulations, insertion and removal of clamps, and the administration of drugs. The clinical significance of these microemboli and what practices may be used to reduce GME incidence require further study. 65
Although patients on CPB have had neurocognitive deficit attributed to GME in the postoperative period, the management is largely preventative. TCD is largely a research tool and is not routinely used during CPB. Both the EDAC and Gampt have been used in a clinical setting for monitoring basal GME production but have major limitations as they partially count microbubbles at higher flow rates, and studies regarding their use have not been fully validated. 66 Microemboli attributed to the performance of CPB cannot be completely eliminated by its avoidance. Several randomized studies have failed to show a difference in the frequency of postoperative neurocognitive dysfunction in patients undergoing surgery with and without the use of CPB.67,68
Difficult Situations During Maintenance of CPB
Massive Air Embolism During CPB
As mentioned earlier, massive air embolism is a rarity with technologic advancements in the circuitry of CPB and increased awareness of the consequences of massive arterial air embolism. Severe neurological injury or death from direct occlusion of arteries and perivascular inflammation still remains a major concern, and as such, the team must employ multiple safeguards. Massive air embolism can occur from multiple etiologies related to equipment failure or inadequate techniques (Table 3).
Causes of Massive Air Embolism During Cardiopulmonary Bypass.
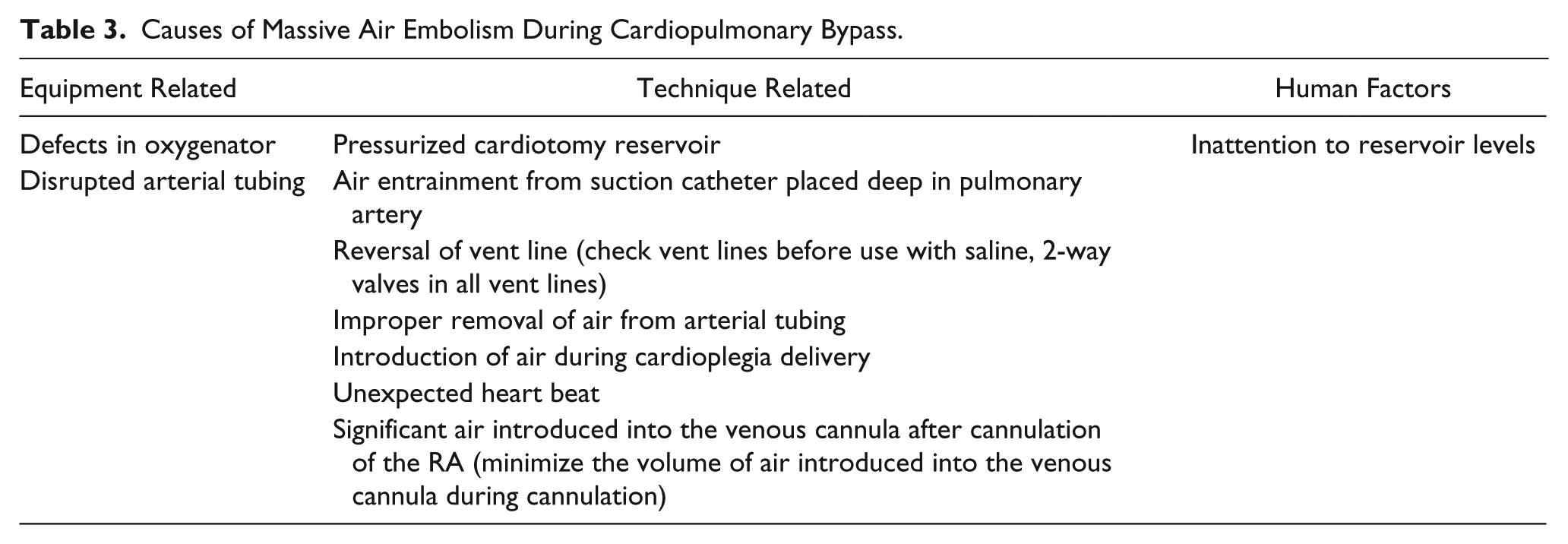
Since these events are catastrophic in nature, appropriate modification of certain perfusion techniques may need to be reconsidered. The volume of air present in the venous cannula after cannulation of the right atrium bears a positive correlation with the level of TCD-quantified emboli in the middle cerebral arteries. 69
Preventative measures include establishing and updating perfusion checklists, performance of crisis management/simulation scenarios, and creation of clear lines of communication along with defined responsibilities of personnel.
Given the fact that massive air embolism is an acute event, there may not be sufficient time to allow induced hypothermia of the brain to benefit from hypothermia’s neuroprotective effects. The concept of retrograde cerebral perfusion (RCP) was first introduced to treat air embolism during CPB. RCP is presently used to prevent cerebral rewarming and extend the safe hypothermic arrest time. The brain is retrogradely perfused through the superior vana cava with flows maintained between 200 and 500 mL/min, while maintaining the patient CVP <25 mm Hg. Blood return to the pump is by cardiotomy suction, and the surgeon should visualize retrograde flow from the aortic arch vessels. RCP does not provide adequate cerebral capillary blood flow or prevent cerebral ischemia, but it facilitates the removal of air and debris from the cerebral circulation and extend the safe period of profound hypothermic circulatory arrest to more than 60 minutes. However, even the use of RCP during controlled conditions such as hypothermic circulatory arrest at 12° to 18°C, the technique is still unable to fully meet cerebral oxygen demands 70 (Table 4).
Treatment of Massive Air Embolism.
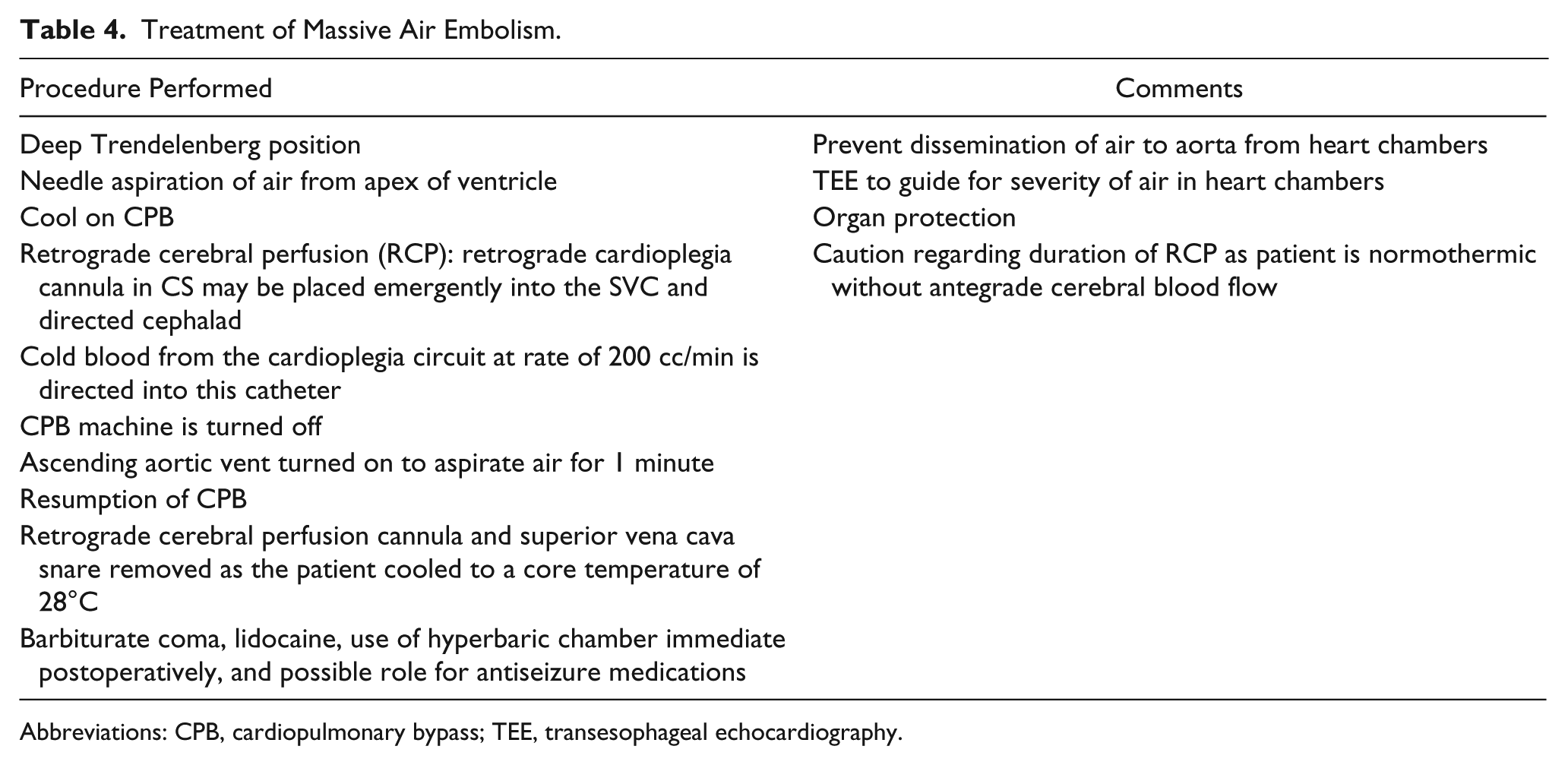
Abbreviations: CPB, cardiopulmonary bypass; TEE, transesophageal echocardiography.
Critical Events Related to CPB Machine/Pump Failure on CPB
Reversal of Roller Blood Pump Rotation
During the loss of power, hand cranking of the CPB has been noted to play a role. However, hand-cranking devices may be unsafe in an emergency situation for managing electromechanical failure of the older CPB equipment with roller pumps. Hand cranking may cause a reverse rotation of the roller pump head, leading to accidental air entrainment. Modifications in the designs of the hand-cranking device of newer CPB machines include an ergonomic design to prevent fatigue and incorporation of a ratchet-style device with 1:2 transmission (Cobe, Stockert, and Jostra heart-lung consoles), along with fluorescent markers to improve visualization in dark. These devices also prevent reverse roller pump rotation. Other pump-related causes are noted in Table 5. 71
CPB Machine/Pump Issues.
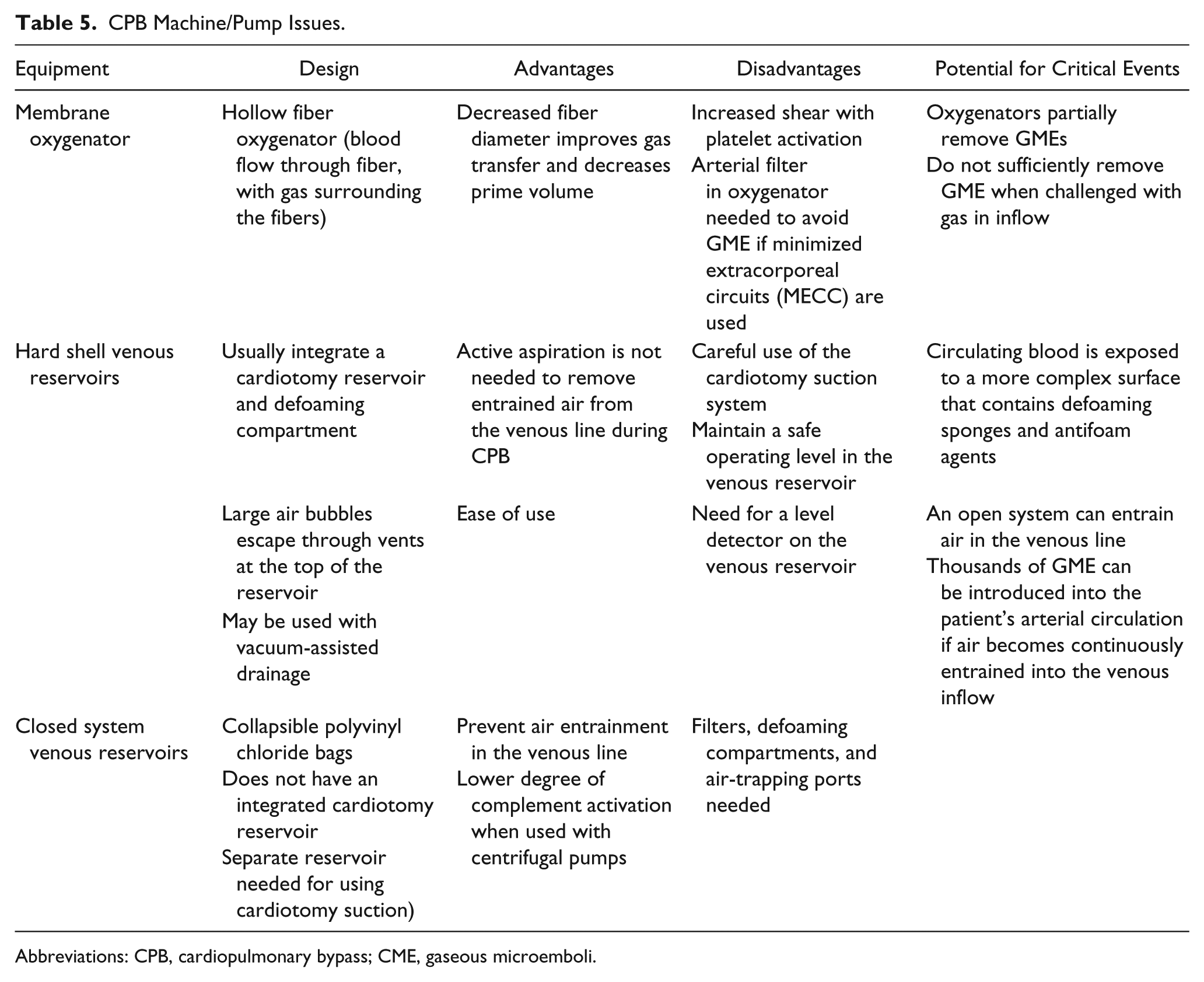
Abbreviations: CPB, cardiopulmonary bypass; CME, gaseous microemboli.
Perfusion technicians operating the CPB machine may be lulled to some degree of complacency as technologic advances have evolved to make conduct of CPB an extremely safe undertaking with a high degree of success. CPB machine malfunctions could rapidly spiral into a potentially life-threatening situation when least expected, and anesthesiologists and perfusion technicians are obligated to perform routine pre-use checks including maintaining a check lists for anesthesia machine and CPB equipments. 72
Power Outage in the Operating Room During CPB
Electrical failure during CPB has been reported to occur in 1 of every 1500 cases. 73 Interruption of power supply in the operating room suites could follow a natural catastrophe such as storms, fires, earthquakes, or explosions. It is a rare event but one that the anesthesia care team and perfusion technicians should be prepared to handle in a speedy and appropriate manner. Advanced planning or simulation practice in anticipation of such critical events should be a part of quality improvement process.
Electrical failure is particularly perilous for the cardiac surgical patient during CPB. Apart from the usual monitoring equipment, operating room lights, electrocautery, and overhead paging, the CPB pump and heat exchanger will also be inoperative. With prolonged period of power failure and power restoration uncertain a decision needs to be made regarding terminating the cardiac surgical procedure if feasible. The situation is difficult as the heart may be in asystole after having received a dose of cardioplegia infusion, and the patient will remain hypothermic with cooling maintained during CPB. Since warming of the patient is not possible during power interruption, hand cranking of the arterial pump should be continued to maintain circulation. Hand cranking is effective but exhaustive and extra personnel will need to be allotted. The perfusionist conducting the bypass should supervise the correct rotation of the pump. Additional members of the team will need to be deployed to observe the blood level in the oxygenator reservoir as all blood level sensors and bubble detectors will be inoperable. The mean arterial pressure (MAP) is monitored by means of an aneroid Tycos gauge and this should be maintained at prefailure level. The surgeon can intermittently palpate the aorta to access efficiency of hand cranking. 74
The patient will need support with inotropes via a battery-operated infusion pump with reestablishment of some degree of perfusion and appearance of electromechanical activity of the heart. The lungs are manually ventilated with 100%. Oxygen and monitoring is continued with the battery-operated transport monitor. Most modern heart–lung machine pump consoles are equipped with built-in battery back-up units.
Priorities for the patient on CPB during a power outage include restoring adequate systemic perfusion following pump failure. Typically, a clamp is immediately placed on the venous tubing since venous return will continue to drain into the reservoir resulting in exsanguination. In situations where there is adequate cardiac contractility, limiting venous return will help heart in resuming systemic perfusion. If, however, the heart is in a hypothermic and noncontractile state, mechanical perfusion by hand cranking the pump is essential. There are issues surrounding hand cranking, especially with regard to air entrainment. However, the adequacy of hand cranking is estimated by the venous saturation monitor, which is powered by battery. 74
In addition to the pump unit requiring portable battery pack built into the machine, other CPB machine functions used for cardioplegia administration, cardiotomy suction, and left ventricular vent will require a battery pack source or a hand crank. The length of battery life is affected by the pump speed, circuit pressure, boot stiffness, and the number of pumps utilized. Centrifugal pumps have been shown to reduce drain on the battery when compared with roller pumps. 73 Of note, the patient may be unable to be rewarmed via the heater/cooler unit of the bypass circuit that is dependent on electrical power. The heater/cooler unit of the bypass circuit requires considerable electrical power for pumping water to the oxygenator and for generating heat for rewarming. Protocols for preventative maintenance, necessary equipment, battery backup, and guidelines for the successful management of such accidents during CPB should be discussed during simulation drills (Table 6).
Effective Strategies Used to Manage Patient on CPB During a Power Outage.
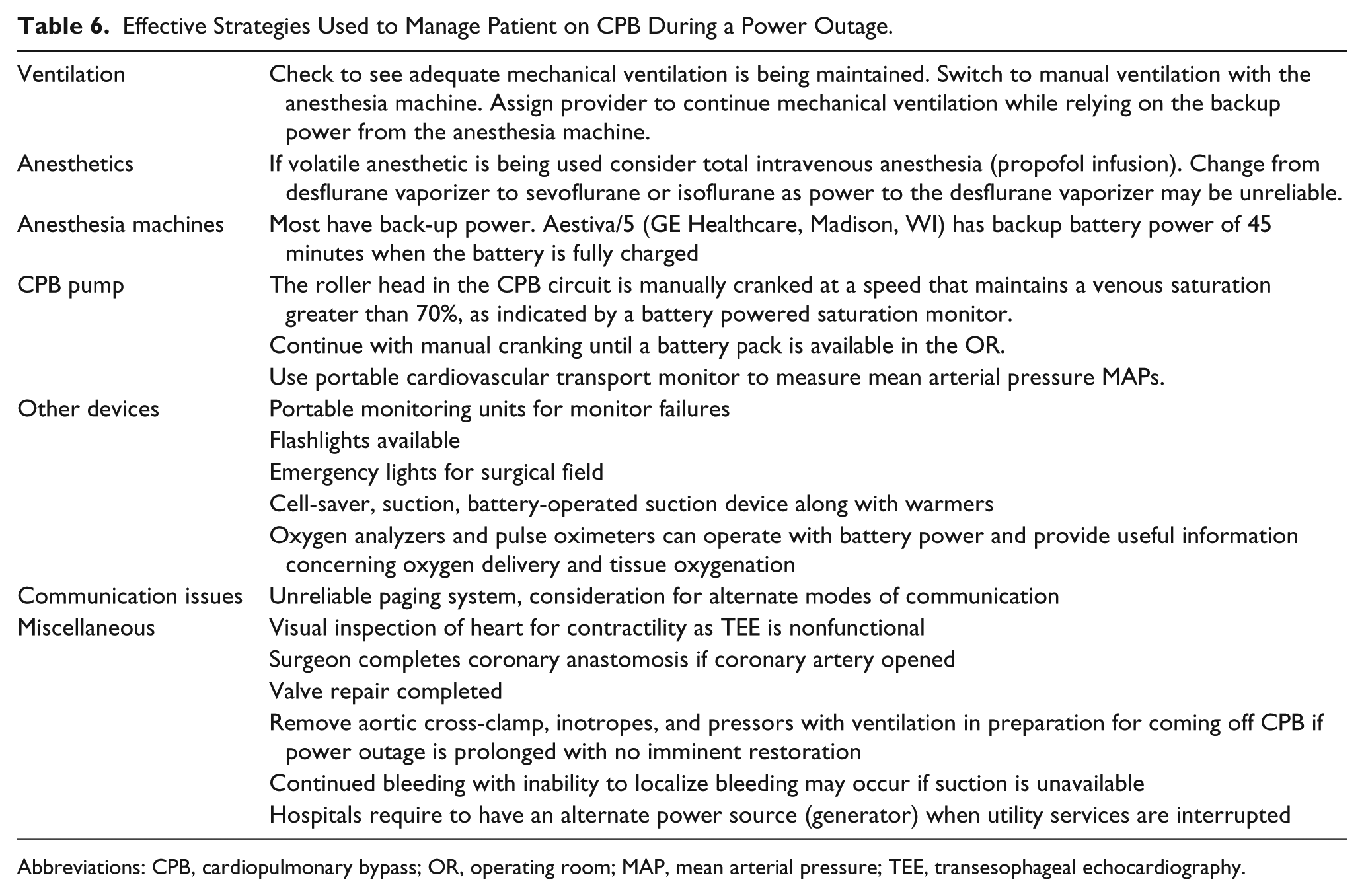
Abbreviations: CPB, cardiopulmonary bypass; OR, operating room; MAP, mean arterial pressure; TEE, transesophageal echocardiography.
Critical Events Related to Perfusion on CPB (Table 7)
Critical Events Related to Perfusion on CPB.
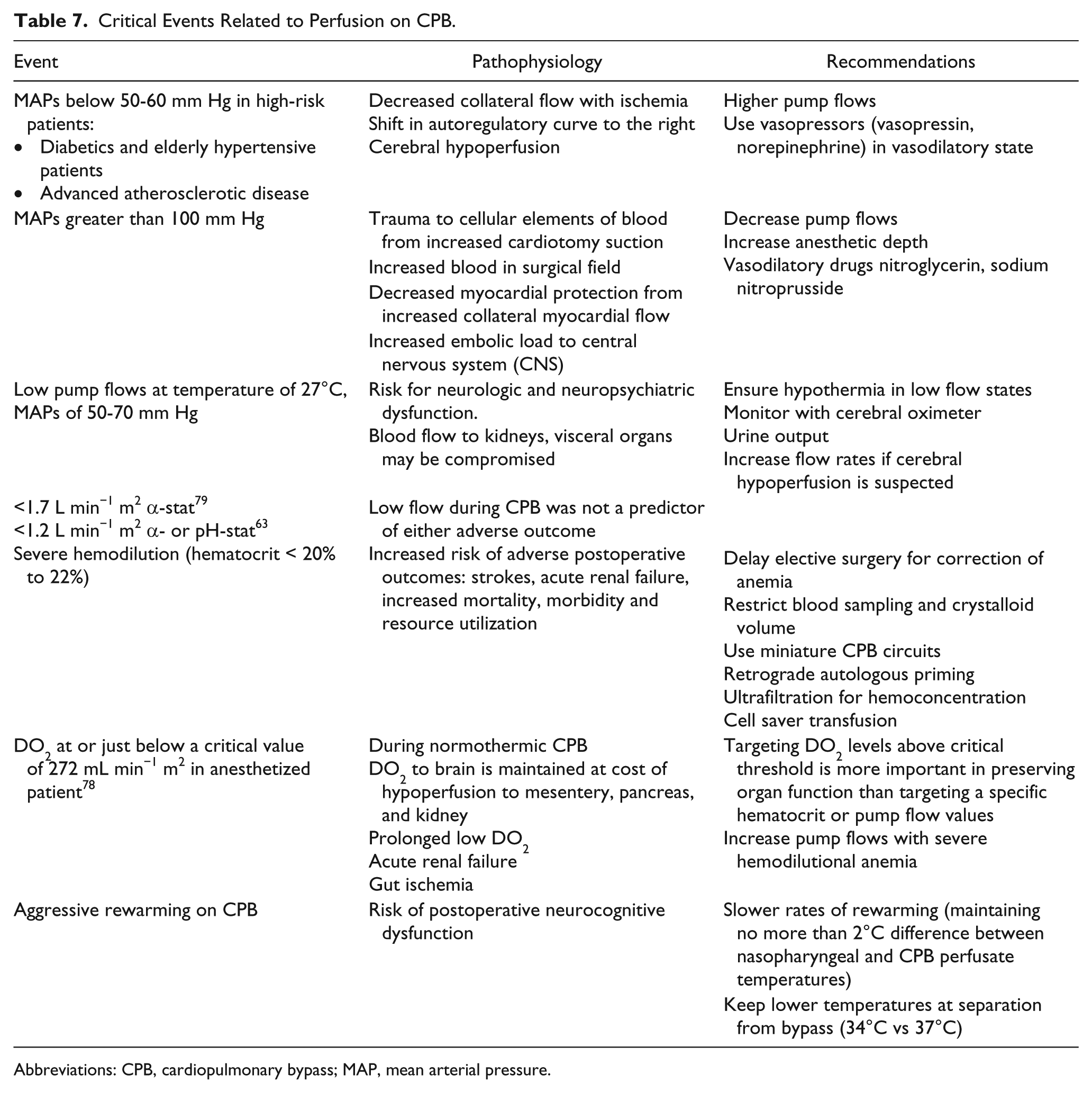
Abbreviations: CPB, cardiopulmonary bypass; MAP, mean arterial pressure.
Optimal Pump Flow
There is no consensus regarding optimal pump flows during CPB as most investigators have studied the process using different acid–base management and cerebral blood flow (CBF) measurement techniques. The pump flow rates set during CPB varies in most centers and is based on institutional practice. Calculation of initial flow rates is based on body surface area (BSA) and temperature management strategy. Flow rates of 2.2 to 2.5 L min−1 m2 approximate the cardiac index (CI) of normothermic patient with normal hematocrit. Lower flow rates of 1.2 L min−1 m2 in hypothermic states are suitable as there is less hypertension from increased blood viscosity. CBF typically remains relatively constant at pump flow rates of 1.0 to 2.4 L min−1 m2 when hypothermic bypass is used. There is no evidence of minimum safe flows during normothermic or hypothermic CPB states. 75 However, the following factors should be taken into consideration if organ hypoperfusion is suspected or proven during CPB. These include BSA, extent of hypothermia, acid–base balance status, whole-body oxygen consumption, use of neuromuscular blockade agents, oxygen content of blood (hemoglobin concentration and saturation, PaO2 and SaO2), depth of anesthesia, and organ ischemic tolerance.
Hematocrit During CPB
There are concerns that in the absence of CPB guidelines for lower limits of hematocrit during CPB, accepting extreme hemodilution may contribute to postoperative organ injury including renal injury after cardiac surgery. 76 Defoe observed a strong inverse relationship between hematocrit levels on bypass and in-hospital mortality and need for intra-aortic balloon pump support. 77 Habib et al also noted that mortality, major morbidity, and resource utilization were significantly increased and hinged on low hematocrit values. 78 An independent, direct association was noted between degree of hemodilution during CPB and risk of perioperative stroke. 79 Hemodilution during CPB to a hematocrit of less than 24% is associated with an increased likelihood of renal injury (including acute renal failure) and worse operative outcomes. In addition, the effect is worsened by prolonged CPB time and intraoperative blood transfusion. 80
Unfortunately, employing blood transfusion to counter hemodilution is, by its nature, fraught with inherent hazards. Data have emerged that consistently show perioperative blood transfusion and its association with adverse outcome. 81 Allogeneic blood transfusion is not without known risks from transfusion reactions, immunosuppression, infections, and perioperative inflammation from raised cytokine levels.82-84 Traditionally blood transfusions have been endorsed in patients with low hematocrit (<8 g%) to counteract the further drop from hemodilution and the ongoing perioperative blood losses. In a retrospective study where all confounding variables were adjusted by constructing a propensity score the 30-day and 1-year mortality, transfused patients showed a significantly higher hazard ratio of 1.88. 85
Careful pre-CPB planning should prevent excessive hemodilution. If possible, elective surgery should be delayed in order to restore red cell mass with use of iron and erythropoietin. Other techniques such as limiting the volume of crystalloids pre- and post-CPB and reducing frequency and volume of blood sampling in the perioperative periods are ways of avoiding and/or worsening hemodilution. Retrograde autologous priming techniques also reduce the volume of prime required.
Oxygen Delivery
The overall margin of safety with organ perfusion during CPB is essentially related to systemic oxygen delivery and its determinants, the pump flow rate, and oxygen content. These parameters also determine tissue oxygenation, and in the clinical setting oxygen content and delivery can be adjusted. For example, an extremely low hematocrit will adversely impact systemic oxygen delivery (low oxygen content) and can be managed by blood transfusion or hemoconcentration by using ultrafiltration.
With the onset of CPB the systemic oxygen content is reduced primarily from hemodilution (Hb between 7 and 8 g%) and from reduced oxygen delivery from restriction of pump flows (2.2-2.4 L min−1 m2). Reducing whole-body oxygen consumption by instituting hypothermia and paralytics will lower demand and the amount of oxygen extraction that occurs at the tissue level.
The safe margin between oxygen delivery and demand is narrowed in situations involving low CPB flow and inadequate cooling as there is impaired total oxygen delivery with no concomitant decrease in oxygen demand. Initially this is physiologically compensated by increasing oxygen extraction until the limits of critical oxygen delivery (DO2) is reached (DO2 = 330 mL min−1 m2 in anesthetized patient). Further deterioration in oxygen delivery limits availability of oxygen, and the tissue is more dependent on anaerobic metabolism, thus leading to lactic acidosis.
Hypothermia
While advocating neuroprotective strategies during CPB with the notion of circumventing critical events, one should realize that many of our daily practices in CPB management are based on assumptions from observational studies without sound reference to evidence-based medicine. Thus, endorsing hypothermia to deter organ ischemia has not been sufficiently supported in the literature. For example, a recent review of randomized trials evaluating neuropsychological function post-CPB failed to reveal any advantage related to temperature of systemic perfusion. 86
Hypothermia is, however, associated with a reduced stroke rate. Unfortunately, this benefit is offset by a trend toward an increase in non-stroke-related perioperative mortality and myocardial damage. 87
The lack of evidence to routinely support hypothermia has led to more controversy. Systemic normothermia and continuous warm cardioplegia may be favorable in providing myocardial protection. In fact, normothermic techniques have been reported to lower the incidence of perioperative myocardial infarction, cardiac arrhythmias, and post-CPB low cardiac output syndromes. 88 However, a recent review showed that the risk of stroke, cognitive decline, atrial fibrillation, use of inotropic support or intra-aortic balloon pump, myocardial infarction, and acute kidney injury after cardiac surgery were not significantly different between the normothermic (>34°C) and hypothermic (≤34°C) groups.
Hyperthermia
Perfusionists typically monitor blood temperature at the point of exit of blood from the oxygenator. Blood enters the circulation by way of the ascending aorta and quickly reaches the brain, so excessive heating must be avoided. During the phase of rewarming, pump flows are often transiently lowered to allow application or removal of aortic clamps. The resulting cerebral hypoperfusion, increased embolic activity coupled with cerebral hyperthermia can increase patient’s vulnerability to developing CPB-associated neurocognitive dysfunction. Cerebral hyperthermia (brain temperature >37°C) in particular creates cerebral ischemia from an oxygen supply and demand mismatch, widening any preexisting cerebral ischemic penumbral zone and increasing production of free radicals.
Temperature measurement of the arterial and venous blood is necessary to keep the arterial venous gradient less than 10°C to prevent bubble formation as the blood warms. During the rewarming phase of CPB, temperature recorded at nasopharyngeal, esophageal, bladder, and rectal sites underestimates the jugular bulb (JB) temperature (representing actual brain temperature). Because of the ease of access, nasopharyngeal temperature is preferred as a surrogate of brain temperature. However, the nasopharyngeal and arterial inflow temperatures are the closest to JB temperatures, with an average gradient of 1°C to 2°C. Therefore, in patients who are at high risk for developing postoperative neurocognitive dysfunction, slow rewarming with nasopharyngeal temperatures not exceeding 37°C is recommended.89,90
Overwarming at the end of CPB as seen in JB and nasopharyngeal temperatures exceeding 38°C is common after deep hypothermia. Aggressive rewarming can potentially offset any potential neuroprotective gains obtained from hypothermia during CPB. A surface-warming device in combination with limited rewarming (nasopharyngeal of 35°C) was compared to control group (warmed to nasopharyngeal temperature of 37°C). In this study the peak JB temperatures during the rewarming phase were significantly lower in the surface-rewarming group compared with the control group at the end of CPB but returned to normal in the ensuing 4 hours. Limited rewarming during CPB, when used in combination with surface warming, can be another option in preventing cerebral hyperthermia while minimizing the risk of postoperative hypothermia 91 (Table 7).
Summary
The purpose of this review is to describe the various challenges faced during CPB that can result in adverse outcomes. CPB entails multiple facets related to coagulation, cannulation, perfusion, and requires expertise from perfusionists, surgeons, and anesthesiologists for its success. Even a routine CPB run will require advance planning and discussion so that the patient’s underlying conditions and the technical complexities of the procedure are appropriately addressed. Perfusion mishaps can be sudden and unanticipated, resulting in strokes and multiple organ dysfunction, which could be devastating.
To avoid critical events during CPB, education of and teamwork to keep up with technological advances are important. Safety initiatives should include having a checklist, well-defined communicated goals, and vigilance. The use of monitors, protocols, and safety devices, however, cannot supplant vigilance, as human errors can occur in unlikely scenarios. The guidelines in perfusion practice should also include familiarity and understanding of perfusion machines and circuitry, evidence-based perfusion practices, and emergency crisis drills.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.