
Abstract
The first stage of surgical treatment for hypoplastic left heart syndrome (HLHS) includes the creation of artificial systemic-to-pulmonary connections to provide pulmonary blood flow. The modified Blalock-Taussig (mBT) shunt has been the technique of choice for this procedure; however, a right ventricle–pulmonary artery (RV-PA) shunt has been introduced into clinical practice with encouraging but still conflicting outcomes when compared with the mBT shunt. The aim of this study is to explore mathematical modeling as a tool for describing physical profiles that could assist the surgical team in predicting complications related to stenosis and malfunction of grafts in an attempt to find correlations with clinical outcomes from clinical studies that compared both surgical techniques and to assist the anesthesiologist in making decisions to manage patients with this complex cardiac anatomy. Mathematical modeling to display the physical characteristics of the chosen surgical shunt is a valuable tool to predict flow patterns, shear stress, and rate distribution as well as energetic performance at the graft level and relative to ventricular efficiency. Such predictions will enable the surgical team to refine the technique so that hemodynamic complications be anticipated and prevented, and are also important for perioperative management by the anesthesia team.
Introduction
The treatment of hypoplastic left heart syndrome (HLHS) involves a sequence of complex, staged surgical procedures. During the first stage (Norwood operation), the goal is to provide pulmonary blood flow after closing the ductus arteriosus.1-3 To accomplish this, the modified Blalock-Taussig (mBT) shunt, consisting of an artificial connection between the innominate and the right pulmonary arteries, has been the procedure of choice for many years.4,5 However, a surgical shunt between the right ventricle and the pulmonary artery (RV-PA) was recently proposed as a modification to the Norwood operation (Sano procedure). 6 There have been reports of better postoperative hemodynamic profiles and more adequate pulmonary diastolic pressure 7 related to a lack of pulmonary run-off with the Sano intervention, which translate into greater hospital survival, although there is no apparent effect on mid- or long-term survival.8-11 In some high-risk patients with prematurity, low birthweight, severe valvular insufficiency and noncardiac conditions, a hybrid operation consisting of stenting of the ductus arteriosus and banding of the branch pulmonary arteries, is used as an alternative, with conflicting evidence of improved survival. 12
The explanation for this prognostic discrepancy might lie in the unique physical characteristics of types of shunts used in the treatment of HLHS. The purpose of this article is to explore the mathematical analysis of the physical properties that determine flow patterns that could affect early and late complications after a modified Blalock-Taussig or Sano procedure. To conduct a rational analysis, studies that used computational tools and theoretical approaches were reviewed and summarized, and the possible clinical implications are discussed.
Mathematical Models and Computational Fluid Dynamics
With advancements in surgical approaches to both palliate and treat congenital heart disorders, growing interest in the development and application of mathematical models for complex heart physiologies has emerged in recent years. Because both the modified Blalock-Taussig and Sano interventions involve the interaction between the heart and systemic and pulmonary circulation, a general mathematical model serves as a first step for the description of the whole system in these cases. Mathematical modeling is an integral part of physics and is used to describe theories that are based on experimental evidence. When this principle is to be applied to human biological systems, the limitations of experimental accessibility emerge as a barrier. However, in recent years, a great deal of interest in using mathematical models to predict the performance of complex physiologic processes, such as those related to the cardiovascular system, has encouraged the development of technologies that can mimic in vivo biomechanics of the heart and blood vessels. 13
The biomechanical aspects of the cardiovascular system are particularly complex due to the interaction between solid (heart muscle/valves and blood vessels) and fluid (blood) mechanics. 14 These interactions are dynamic in structure and properties. As a result, mathematical models must involve multiple variables and require the utilization of computational tools. Physical quantities, such as stress and strain, which are difficult to measure in vivo given their dynamic nature, can now be processed by the combination of high-tech data acquisition (eg, magnetic resonance imaging, spiral tomography) and computer-based 3-dimensional geometric reconstruction algorithms.15,16 To further complicate matters, in situations where surgical 2-ventricle repair of HLHS as a primary or as a staged procedure, when assessments of arterial and mixed venous oxygen saturations are inaccurate to estimate fractional flow between pulmonary and systemic circulations, mathematical modeling of transitional circulations must include the contribution of both ventricles to predict hemodynamic profiles after the operation. 17
Windkessel models, which present an electrical analogy to fluid flow, have been successful for effectively modeling the cardiovascular system in terms of the interactions between the cardiac pump and arterial/venous conduits.18-23 When vascular branching and natural or artificial anastomoses are included in the circuit, complicated physical interactions between blood and vessel walls determine the overall performance of the system. At the level of vascular anastomoses, most mathematical models have traditionally assumed that both blood vessels and grafts are rigid-walled conduits through which incompressible non-Newtonian fluid flows in a laminar fashion. However, to develop a more realistic approach, flow must respond to the interaction between blood and elastic conduits, which are both defined by independent differential equations. This allows for pressure and flow velocities, as well as tissue displacement at any point of geometric computational domain, to be calculated. 24 With this type of model, we are able to determine arterial wall stress secondary to blood movement, taking into consideration that pressure, velocity, and tissue displacement vary with time and position given the pulsatile nature of the flow. 25
There is general agreement that local mechanical fluid dynamics at the level of anastomosis, including those where artificial grafts are used in the arterial vasculature, determine the development of intimal hyperplasia.26,27 Conditions that favor hyperplasia include turbulent flow and intraluminal stress distribution and are compounded by the thrombogenic properties of an artificial graft in contact with blood.28-30 Because anastomotic flow properties and stress distribution along the vessel wall are strongly influenced by the geometrical configuration of the vessel-graft arrangement, it is essential to employ anatomically accurate geometric modeling. 31 In particular, intimal hyperplasia, which occurs along suture lines and is a key element in graft failure, is associated with a compliance mismatch between the graft material and the arterial wall.32-34 This aspect can also be thoroughly investigated by analyzing shear stress distribution using a realistic model that includes geometrical frameworks, flow and vessel wall aspects, and a numerical analysis.35,36 This multifactorial model requires the application of complex technologies in the field of computational fluid dynamics (CFD).
CFD is a field of biomechanics that is based on computer simulations and uses numerical methods to analyze and solve problems related to fluid flow and heat transfer. 37 CFD is the main tool used to provide detailed solutions to flow in vascular systems, with many of these solutions providing insights about properties related to pathophysiological processes. The physical properties of fluid motion can be described by partial differential equations (governing equations) that are solved by conversion through high-level computer programming languages. 38 The computations describe fluid behavior through numerical simulations utilizing programs developed on high-speed digital computers to generate numerical solutions. 39 The foundation of CFD lies in Navier-Stokes equations, which describe the motion of viscous fluids. These equations contain expressions of fluid, energy, and mass conservation. CFD technology uses discretization and numerical methods to solve the equations. CFD codes consist of 3 components: preprocessing, solver, and postprocessing. 40 During the preprocessing phase, a fluid flow problem is introduced into the computer. This includes defining the geometry; grid generation (the most critical step in determining accuracy); fluid properties (blood as a non-Newtonian fluid with shear-dependent viscosity); and boundary conditions at the inlet and outlet (blood pressure, flow, and temperature) (Figure 1). During the solver phase, a finite volume method is used to find mathematical solutions to unknown flow variables that are approximated and discretized for an algebraic solution. This step is time consuming and depends on the calculating capacity of the computer. Finally, in the postprocessing stage, graphic visualization of the computational results is made available.
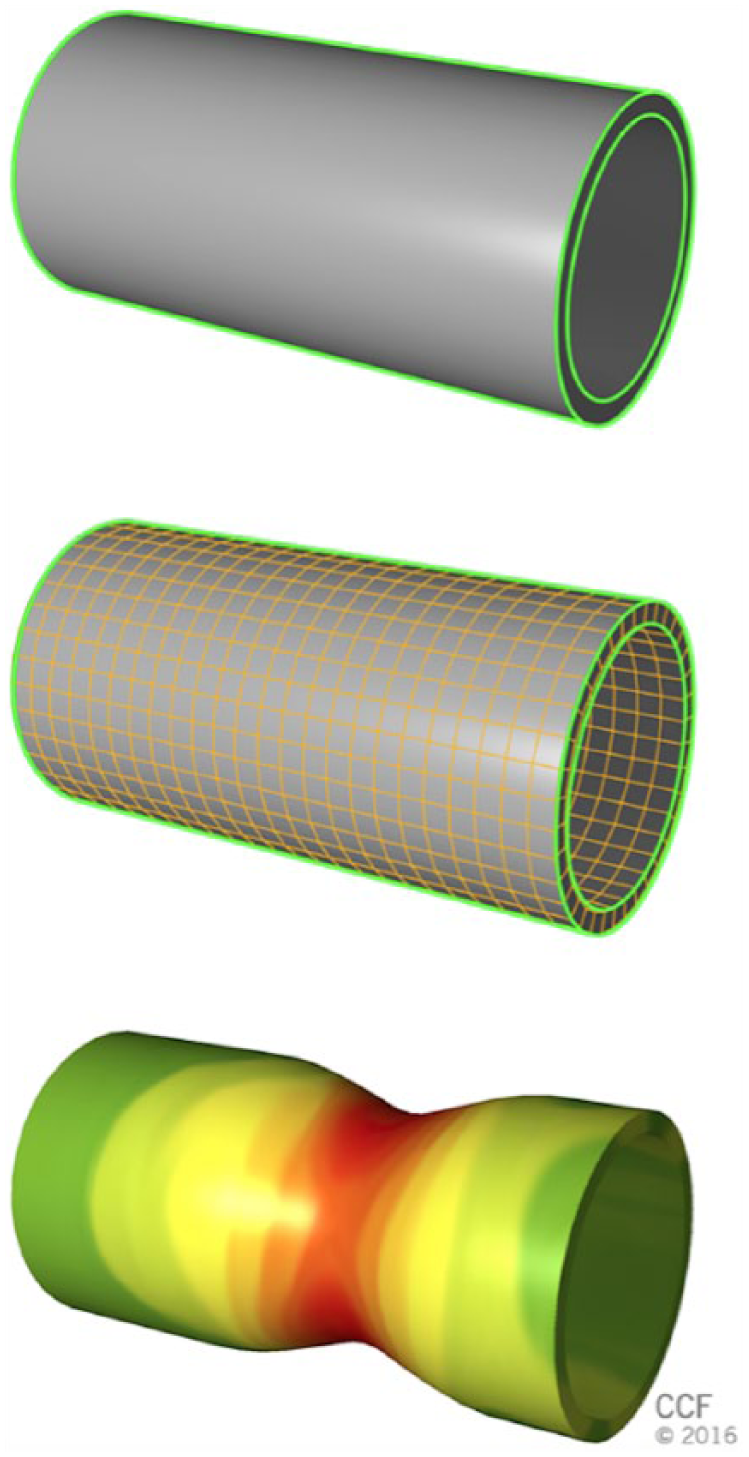
Steps of processing in computational fluid dynamics (CFD). (A) Definition of geometry of the vessel to be studied. (B) Creation of the grid and definition of boundaries. (C) Analysis and display of solutions for the different variables under study.
Modified Blalock-Taussig Shunt: Geometrical Framework and Pressure-Flow Patterns
The modified Blalock-Taussig shunt comprises an artificial systemic-to-pulmonary connection that is achieved by the interposition of a polytetrafluoroethylene (PTFE, GoreTex) graft between a subclavian artery and a pulmonary artery (left or right) and is used to provide palliation in some congenital heart defects. 41 Potential complications associated with the procedure include stenosis of the graft, insufficient or excessive pulmonary flow, distortion of the pulmonary artery, and limited flow due to the graft’s inability to adapt to patient growth. 42 To mitigate these complications, some amount of preoperative prediction of hemodynamic profiles in and around the connection is possible and is a valuable tool to understand the pathophysiology of factors related to the development of postoperative thrombosis, hyperplasia, and stenosis.43,44
Because the aim of an mBT shunt is to establish and maintain pulmonary blood flow through an implanted graft, flow distribution between the systemic circulation and the pulmonary vascular bed is critical. Liu et al developed a model based on CFD with flow velocities obtained by echocardiography and pressure wave reflections from peripheral vessels as boundary conditions and found a significant drop in pressure across the shunt, with 40% of blood flow distributed from systemic to pulmonary circulation in one cardiac cycle and a ratio of pulmonary flow through the shunt to systemic flow (Qp/Qs) of 0.724.45,46 Studies have suggested that the optimal Qp/Qs ratio for maximum oxygen delivery is between 0.5 and 1, 47 which confers physiologic plausibility to the mBT. Pressure drop through the shunt has been documented by different studies that used Doppler and models with steady state/rigid walls and pulsatile flow.48-50 Migliavacca et al, by means of a computational fluid-structure interaction approach based on finite element analysis, documented that the pressure decrease occurs at the level of pulmonary anastomosis and that distensibility at the pulmonary artery–anastomosis site determines the pressure drop only when it is not fully distended, which happens when the pulmonary artery pressure is lower than 5 mm Hg.51,52
In addition to the pressure drop across the mBT shunt, other factors also determine the short- and long-term performance of the shunt. These include both geometric factors and the distribution of shear stress and energy loss. Using 3-dimensional simulations, Song et al 53 studied the impact of shunt size and geometry on flow, shear stress, and energy transfer, taking into account the degree of pulmonary artery hypoplasia. In this study, pulsatile flow was simulated, the shunt was modeled perpendicular to the pulmonary artery and the diameter of the graft was evaluated from 3 to 5 mm. The flow characteristics were modeled with the finite element method to discretize the continuous flow into cells on a mesh that underlined the geometry of the system, for which a computer solved differential equations, and the boundary conditions were obtained from information derived from cardiac catheterizations of patients who had received mBT shunts for Fontan palliation. They documented a Reynolds number below 2300, which allowed the use of Poiseuille’s law to calculate maximal wall shear stress. The results of the study showed that the 5-mm shunt carried the lowest energy loss but the highest shear stress, while the 3-mm shunt had high energy loss with low shear stress. Interestingly, maximum shear stress was found at the level of distal anastomosis, which corresponds to the site of pressure drop in other studies. 54 The relationship between shear stress and intimal hyperplasia has been widely studied. In systemic vessels, both high and low shear stress have been associated with intimal hyperplasia,55-58 whereas low shear stress and turbulent flow have been identified as triggers of intimal hyperplasia in pulmonary circulation. 59 These findings stress the importance of optimal graft size and geometry to fine tune the shear stress, because this factor plays a pivotal role in stenosis on the pulmonary side of the anastomosis. Regarding thrombosis of the graft, high shear stress induces erythrocyte aggregation and platelet activation.60-62 Waniewski et al 63 investigated shear stress with different geometric configurations and graft diameters and its impact on flow patterns associated with thrombosis and stenosis. The study simulated pulsatile flow through a system of the left subclavian artery, left pulmonary artery and a graft obtained from computed tomography scan images that used two shunt diameters (3 and 4 mm) and 2 graft shapes (curved and straight). Computer simulations showed complex flow patterns and low-pressure areas at the anastomosis and a high shear rate with all configurations, particularly with the 3-mm graft, whereas pathologically low shear stress (<1 Pa) was found in the pulmonary artery distal to the graft outlet and on the downstream part of the subclavian artery. On the other hand, high wall shear stress (>3.5 Pa) was present on the upstream part of the subclavian artery, in the graft, and in the pulmonary artery at the graft outlet. Two interesting aspects from this study deserve mention. First, high shear rates persisted during diastole with expected lower velocities and therefore longer platelet-vessel wall contact, resulting in greater platelet activation. 64 Second, graft shape was not a determinant factor for shear stress/rate and flow patterns, which is in agreement with other studies that indicate that the diameter plays a more critical role in mBT shunt performance.43,44,65
Finally, in terms of geometric configuration, the effect of the angle between the arteries and the graft on flow has been analyzed in several studies. The studies agree that the influence of the angle between the subclavian artery and the shunt conduit is less relevant than the diameter. The ideal angle is between 60° and 90°, with angles of approximately 110° associated with excessive pulmonary flow and angles of approximately 30° leading to significant pressure drops.65-67
Mathematical Modeling to Compare mBT and Sano Operation
With the advent of the RV-PA shunt, several studies have shown improvements in short-term morbidity variables and a consistent increase in aortic diastolic pressure and pulmonary artery growth.68,69 The improved diastolic pressure is associated with the decreased diastolic run-off phenomenon (diastolic steal) and improved coronary perfusion. A review of postmortem Norwood cases at Children’s Hospital in Boston revealed that impaired coronary perfusion and maldistribution of pulmonary blood flow were the causes of death in 63% of cases. 70 The hemodynamic differences were documented with echocardiogram and Doppler ultrasound by Ohye et al, 71 and findings such as these have encouraged the application of mathematical modeling to the comparative analysis of mBT and RV-PA shunts in cyanotic congenital heart defects.
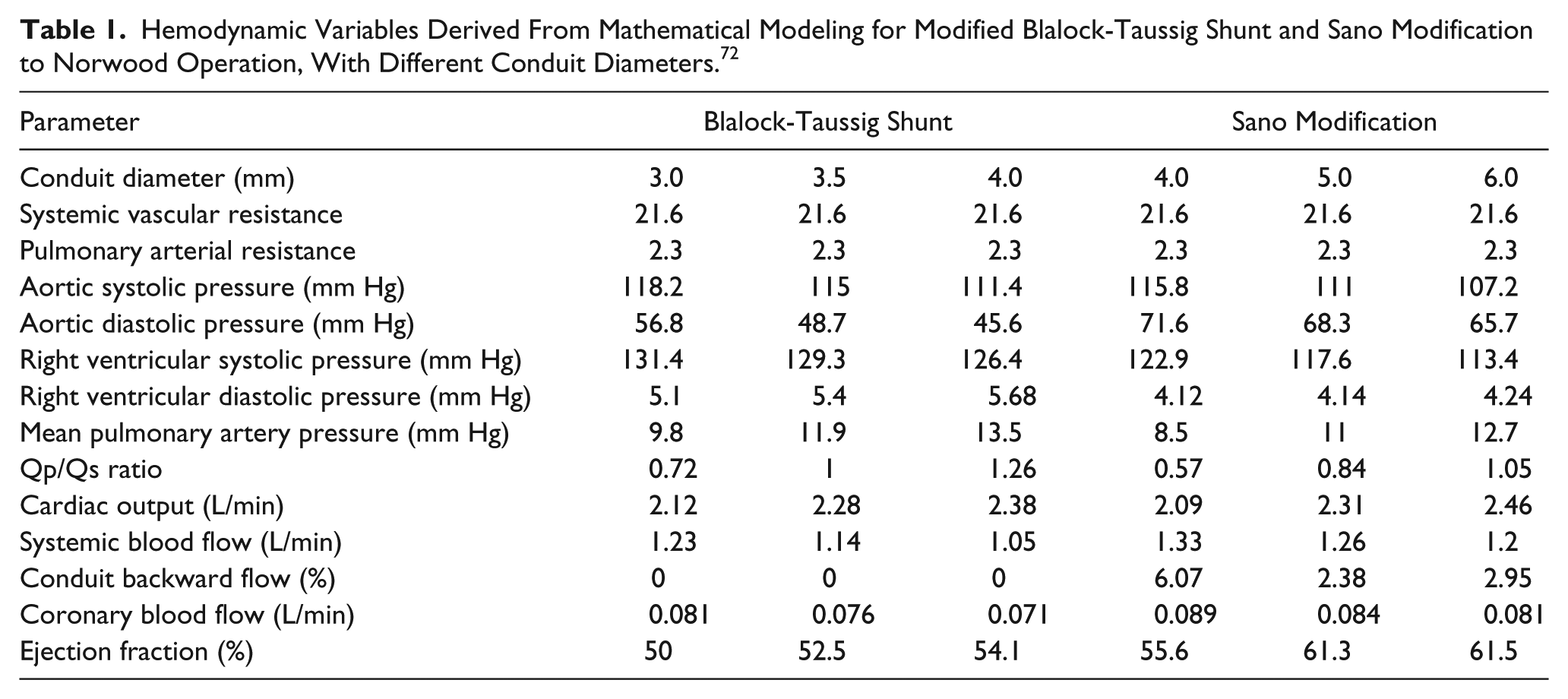
Bove et al 72 used lumped parameter models as part of a CFD analysis to compare the hemodynamic performance of mBT and RV-PA shunts. In this study, time-varying elastances to model cardiac cavities, nonlinear resistances to model valvular structures, and linear resistance to model a nonrestrictive atrial septal defect based on data from 28 patients were used. 73 They found that with an RV-PA shunt, there is higher diastolic aortic pressure, decreased mean pulmonary artery pressure for a comparable shunt diameter (Table 1), a lower Qp/Qs ratio, higher coronary perfusion pressure, lower stroke work, and higher mechanical efficiency. Interestingly, the effect of the RV-PA shunt on pulmonary diastolic pressure and coronary perfusion translates into 2 beneficial consequences that have potential clinical impact. First, decrease in the afterload improves the mechanical performance of the single ventricle and pulmonary blood flow to a point only comparable with high-diameter mBT grafts. Second, the lack of diastolic run-off improves the oxygen supply-demand ratio for the myocardium.
Hemodynamic Variables Derived From Mathematical Modeling for Modified Blalock-Taussig Shunt and Sano Modification to Norwood Operation, With Different Conduit Diameters. 72
Migliavacca et al 74 applied a multiscale model to reconstructive cardiac surgery to analyze the differences between mBT and Sano conduits. They used a finite volume method with hydraulic nets representing coronary, pulmonary, and systemic circulation that were identical for both models. A multiscale approach was utilized to couple the 3-dimensional models with the hydraulic circulatory nets, and a comparison with catheterization postoperative data was then carried out. Their results were consistent, with higher diastolic aortic pressure, lower pulmonary artery pressure, lower pulmonary-to-systemic flow, higher coronary perfusion pressure, and minimal regurgitant flow in the Sano conduits. These data were closely correlated with clinical findings. An aspect of clinical relevance was that predicted cardiac output is comparable only when the RV-PA graft has a greater diameter than the mBT graft, which must be taken into consideration when choosing the graft. Regarding pulmonary flow direction, RV-PA shows deceleration and even reversal during diastole, whereas mBT generates forward flow throughout the cardiac cycle. 75
Mroczec et al 76 used a finite element method for computer simulations based on anatomical detail obtained from echocardiographic and angiographic studies to compare the Norwood operation with mBT versus the RV-PA shunt. The Qp/Qs ratios were 0.92 in the RV-PA conduit and 1.5 in the mBT shunt, with more pulsatile flow and diastolic reversal in 20% of the cardiac cycle in the former. Regarding shear stress, in the mBT shunt it was maximal at the connection between the shunt and the pulmonary artery during mid-systole, whereas for the RV-PA shunt, it was found at the proximal and distal fragments. 3 Finally, they showed decreased ventricular stroke work with comparable systemic flow; however, neither the impact of ventriculotomy on ventricular performance nor the effect of systemic and pulmonary vascular resistances on ventricular function was investigated. 77
Mathematical models for both atria and the single ventricle are similar, with the difference lying on the value parameters within each model when we compare mBT and RV-PA shunt. For the 3 cardiac chambers (cc), time-varying elastance describes systolic and diastolic pressure-volume relationships, with a minimum value of 0 at diastole and 1 at systole. Assuming a linear relationship between chamber pressure and volume, elastance for atria and ventricle can be expressed as a product of a pulsatile activation time function (Acc(t)) and a purely volume elastance term (E*cc(Vcc)):

For the single ventricle, a second-order polynomial function can be adopted to take into consideration the nonlinear elastance reduction with increasing volume:

At diastole, during filling, all cardiac chambers fill at an exponential pressure-volume function, reflecting the restrictive effect of the pericardium.
The vascular system is divided into 2 subsystems connected by the systemic-to-pulmonary shunt. Each of these divisions consists of anatomical compartments, assumed to have constant compliance (C) and instantaneous local pressure (P(t)) and volume (V(t)). With these assumptions, the equations for conservation of mass and momentum can be applied to the model to describe the vascular system.


where δP(t) is the instantaneous pressure applied to the compartment ends, Q(t) is the instantaneous flow rate, R is the viscous resistance, and L is the inertance.
The application of the aforementioned equations, to incorporate the hypoplastic heart and the systemic and pulmonary vasculature to the model, allows the researchers to calculate different hemodynamic variables to compare mBT and RV-PA shunt under different geometrical conditions (Table 1).
Comparison of mBT and RV-PA shunt are easily visualized by means of imaging derived from CFD analysis. 72 In Figure 2, the velocity profiles in different cross-sections of mBT (Figure 2A) and RV-PA conduit (Figure 2B) are presented. The difference between the 2 types of connections is that in RV-PA shunt the flow is lower and there is diastolic reversal, evidenced by the opposite direction of the convexity between the profiles.
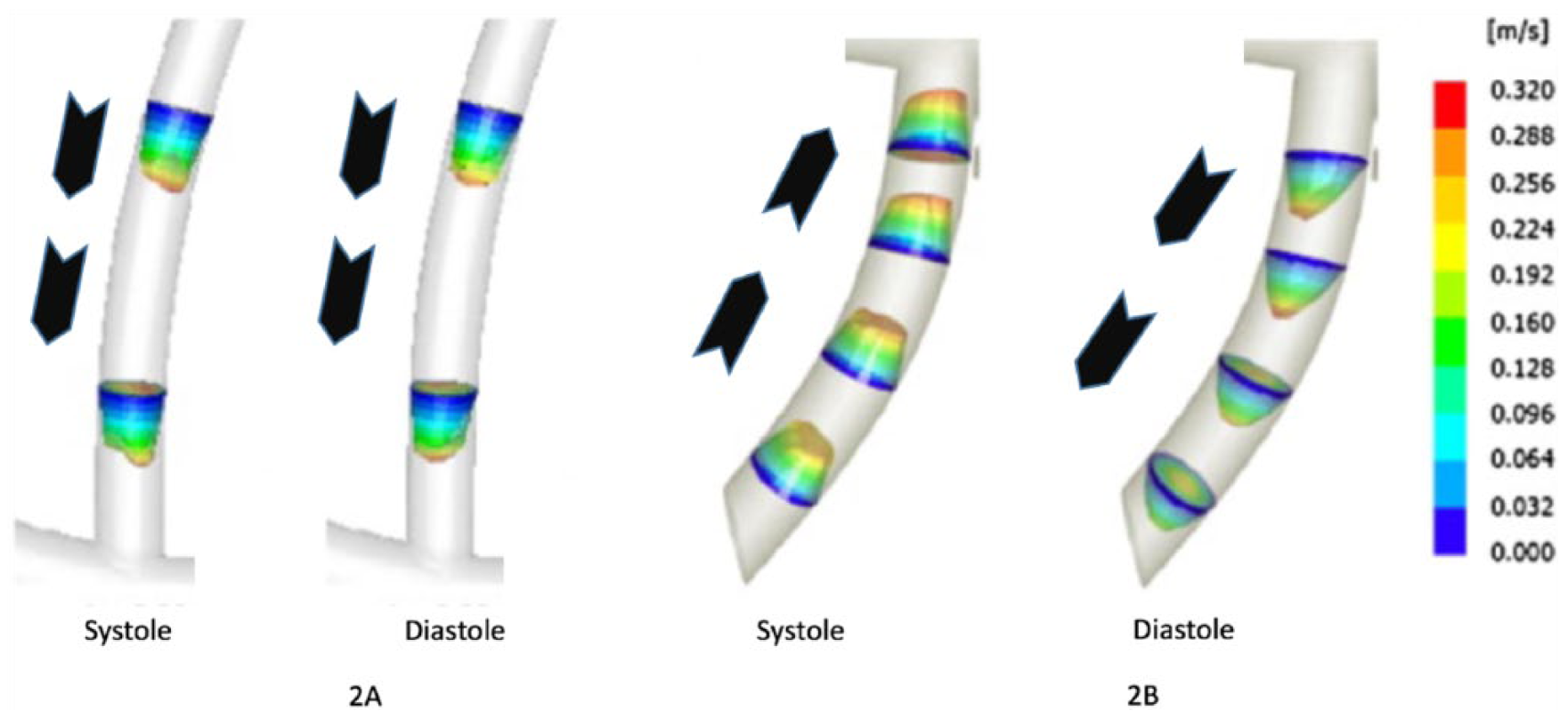
Velocity profiles along pulmonary-to-systemic shunt conduits during systole and diastole: (A) Blalock-Taussig shunt in systole (left) and diastole (right). (B) Sano modification in systole (left) and diastole (right). The arrows illustrate duration of flow during different phases of the cardiac cycle.
Finally, after the original description of the Sano procedure in 2003, new modifications have been implemented. 78 Addition of a cuffed PTFE tube to the distal main pulmonary artery and distal arch plasty for the neoaortic reconstruction (Brawn’s modification), complicate modeling, and future studies using CFD to predict shear stress and hemodynamic profiles in patients undergoing these novel procedures will shed light regarding flow distributions in both pulmonary and systemic circulations.
Clinical Studies Comparing mBT and Sano Procedure
Surgical repair of hypoplastic left heart syndrome comprises three stages. During stage I, or the Norwood procedure, the pulmonary blood flow can be provided from either a modified Blalock-Taussig shunt connecting the subclavian or innominate artery to the pulmonary artery or a RV-PA connection (Sano shunt). During stage II, pulmonary blood flow is provided through an anastomosis between the superior vena cava and the pulmonary artery. At this stage, the previous shunt (mBT or Sano) is removed. During stage III, or the Fontan procedure, pulmonary and systemic circulations are separated once the inferior vena cava is anastomosed to the pulmonary artery. Figure 3 shows the anatomic features of mBT and Sano connections.
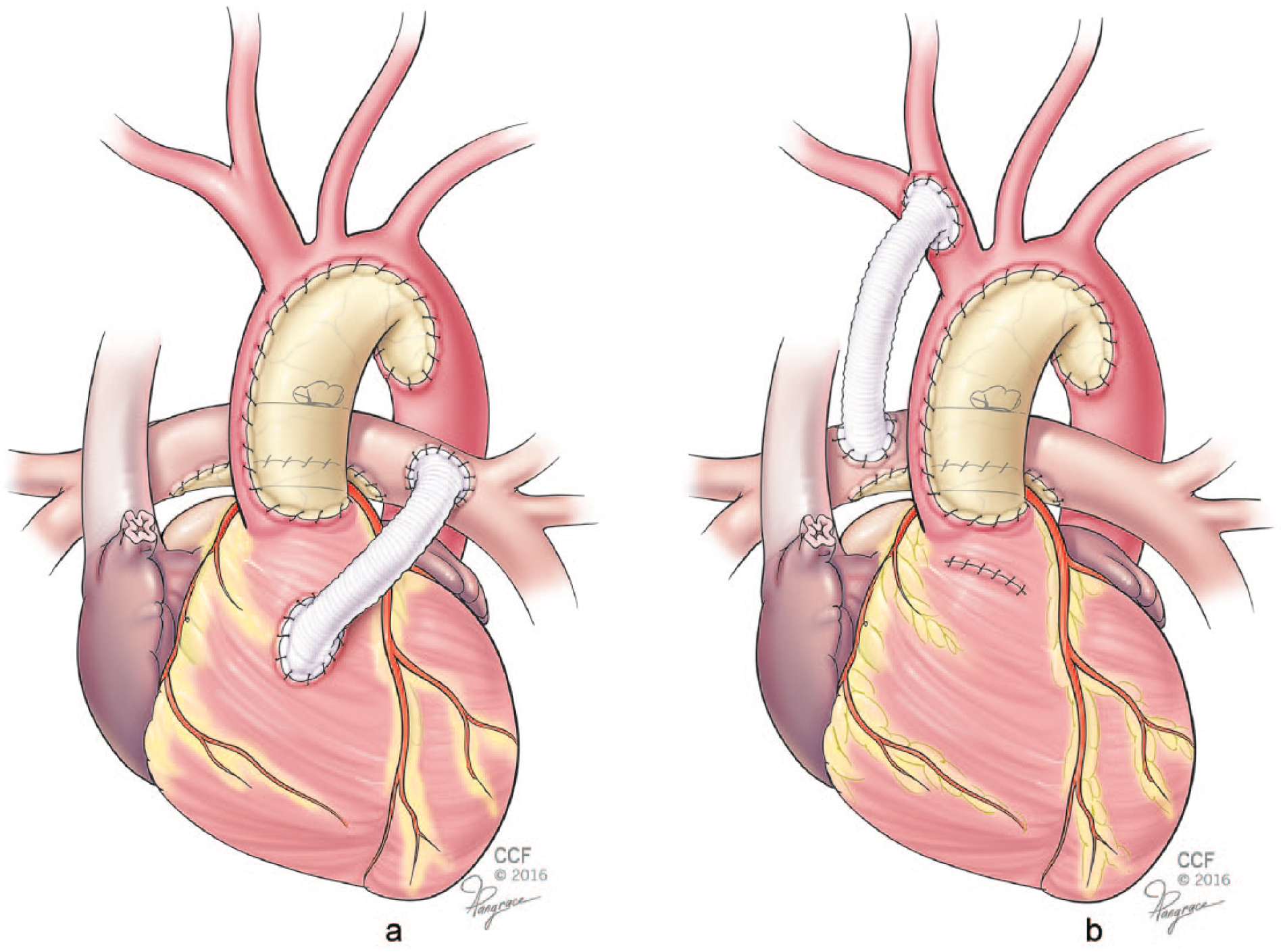
Shunt connections during Norwood procedure. (A) Right ventricle to pulmonary artery graft (Sano shunt). (B) Subclavian to pulmonary artery graft (Blalock Taussig shunt).
Using an mBT shunt during the Norwood procedure provides continuous pulmonary blood flow in systole and diastole. However, a diastolic runoff into the lower resistance pulmonary circulation may lead to a coronary steal phenomenon, which can be responsible for adverse outcomes, such as myocardial ischemia, low cardiac output and death after the Norwood procedure.79,80 The Sano shunt, on the other hand, provides pulmonary flow without the risk for diastolic run-off and has been associated with a more stable perioperative transition and lower mortality.81-83 However, some disadvantages have been described in association with a right ventricle-pulmonary artery shunt, including the negative effect of ventriculotomy on right ventricular function, a risk for ventricular aneurysm formation, the development of arrhythmias and volume overload secondary to regurgitation from a nonvalved RV-PA conduit.84,85
Currently, there is debate on which of these shunt alternatives has better clinical outcomes during the Norwood procedure (stage I). Initial reports have been restricted to small, nonrandomized retrospective analyses that showed conflicting results with limited follow-up.83,85,86 Ohye et al, 9 in a randomized multicenter study, analyzed 555 infants with single ventricles who underwent Norwood operations and showed a higher rate of transplant-free survival at 12 months in the RV-PA shunt group than in the mBT group. However, this difference became nonsignificant after 12 months. Patients with RV-PA shunts had more complications and received more unintended cardiac interventions during the 12-month observation period. 9 More recently, 2 retrospective studies comparing the Sano procedure and mBT also demonstrated a higher rate of shunt interventions in the Sano group. In contrast to mBT, which is a short, straight connection between 2 vessels, the proximal end of a Sano shunt involves heart structures and therefore can be affected by normal growth or dilatation of the right ventricle and by the effect of sternal compression; both factors may be responsible for the observed increase in interventions during interstage repair in patients with a single ventricle who underwent Sano palliation.7,10
Despite the vast experience acquired during decades of performing mBT on patients with single ventricle physiology, as well as on those with biventricular circulation nonamenable to an initial complex repair, mortality rates are still as high as 7.2%. 87 In a retrospective analysis of 174 neonates with single ventricle malformations undergoing mBT, the presence of extracardiac malformations, associated chromosomal abnormalities, pulmonary atresia with intact interventricular septum (PAIVS), and atrial isomerism were found to be significant risk factors for mortality.88-91 The rate of reintervention in patients with mBT shunt varies from 10% to 17% and has been associated with the presence of extracardiac malformations, low weight, and heterotaxy syndrome.88,92,93
Sano modification of the Norwood procedure is not free of complications. The most feared adverse event is conduit stenosis and dysfunction, which occurs with an incidence of 22% to 23% and contributes to overall interstage mortality.94 -96 Other complications include perioperative arrhythmias that are more common than in mBT, 97 hypocontractile ventricular state, 98 and the development of ventricular pseudoaneurysm.99,100
The classic Norwood procedure and Sano modification have shown benefits as well as complications in patients with HLHS. Overall, definite evidence of one procedure being significantly better than the other is lacking, mainly due to the retrospective nature of most studies that evaluated clinically relevant outcomes. 101 The choice of technique must be individualized according to anatomical and clinical factors.
Clinical Implications and Anesthetic Considerations
Morbidity and mortality after a stage I Norwood procedure have significantly decreased in recent years because of advances in perioperative care and the introduction of new surgical techniques, with Sano modification being the most relevant.83,102-105 Mortality after stage I palliation with adjuvant mBT has remained steady and significant for years, 106 indicating that further refinement of surgical technique is difficult to achieve. Studies using CFD for modeling graft-vessel interactions in mBT have shown that the effect of diameter on flow patterns and shear stress/rate distribution is greater than that of other variables, such as the angle of incidence and the shape of the graft. 63 In that regard, the one factor that surgeons should take into consideration when performing mBT is the diameter that best suits the size of aorta and pulmonary artery in a particular child, 107 and mathematical modeling with computer-assisted dynamics might be considered in assisting this task. 108
Retrospective reports have shown evidence of better short-term survival with an RV-PA shunt compared with an mBT shunt.6,8,82 However, clinical studies published to date that compared both techniques have important limitations in terms of their retrospective nature, long-term patient follow-up, and the independent effect of recent advances in perioperative technologies and care on clinical outcomes.109-112 Moreover, when RV-PA shunt patients are compared with contemporary mBT shunt controls, survival rates are comparable. 113 The lack of a significant difference in clinical course could be related to multiple factors that are difficult to separate from each other. We think that the physical profile illustrated by CFD simulations of both mBT and Sano procedures highlights the physiological plausibility as well as their significant drawbacks. Performance of mBT as an adjuvant to the Norwood operation offers the possibility of creating an artificial short conduit that simulates the ductus arteriosus but lacks the vasoactive and dynamic adaptation to fluctuations of systemic and pulmonary circuits. As a result, systemic and coronary blood flow as well as pulmonary arterial circulation can become either insufficient or excessive. This deficient physiologic adaptability of mBT makes it clinically impossible to regulate flow to both circulations all the time. A consequence of the artificial connection of mBT is the creation of a microenvironment of abnormal shear stress/rate distribution and a flow pattern that favors thrombosis and intimal hyperplasia, which could lead to graft failure. 45 On the other hand, the Sano shunt, even though it is free of diastolic pulmonary run-off and is effective in providing pulmonary blood flow with an acceptable Qp/Qs ratio, 76 involves a ventriculotomy with unpredictable consequences. Menon et al demonstrated decreased systolic RV deformation at the ventriculotomy site that persisted after stage-2 palliation and declined RV systolic function. 114 On the other hand, Wilder et al 115 showed an improved 6-year survival rate associated with no significant RV dysfunction. Finally, Ghanayem et al 116 measured hemodynamic variables in a retrospective study of patients undergoing RV-PA shunting and showed a lack of significant hemodynamic benefits. 116
The Pediatric Heart Network randomized clinical study showed a better transplant-free survival rate at 12 months with RV-PA shunts compared to mBT shunts. However, it also showed a higher rate of unintended cardiovascular interventions, including balloon dilatation and stent placement in the graft or in the pulmonary artery as well as performance of a rescue mBT shunt.9,117 These interventions are secondary to graft stenosis, which is present in approximately 40% of cases and is mainly located at the proximal anastomosis to the right ventricle.84,86,118 A possible explanation for the early stenosis of the RV-PA shunt might be related to the high shear stress applied to the anastomosis between the graft and the right ventricle. 3 This situation is complex and compounded by the bidirectional flow that occurs during the cardiac cycle, 76 which creates stasis that favors platelet aggregation and the development of a local inflammatory response, 119 particularly in cases of hyperviscosity and altered coagulation. 120 Another potential consequence of poor flow secondary to stenosis of the proximal anastomosis of RV-PA shunt is the pressure drop at the distal end of the graft, which leads to underdevelopment of the pulmonary artery and adds difficulty to the second stage of surgical repair. This effect can be mitigated by proximal valve-like hood modification and other techniques.121,122
Approximately 50% of the mortality cases after modified Norwood operation occur within the first 48 postoperative hours. 123 Fatalities are associated with a combination of low cardiac output and imbalance between pulmonary and systemic flow. 124 When a Norwood operation is performed, systemic and pulmonary circulations run in parallel through modified Blalock-Taussig or right ventricle to pulmonary artery connections. Under these circumstances, pulmonary vascular resistance is determined by both the pulmonary vascular bed and the artificial shunt. The anesthesiologist is able to manipulate the vascular bed component by means of changes in inspired fraction of oxygen and nitric oxide as well as ventilation. As the pulmonary resistance falls, the main resistor in the system becomes the shunt. In this context, knowledge of the anticipated geometrical characteristics of the connection helps the anesthesiologist to plan strategies to modify systemic vascular resistance. For instance, in light of a CFD-predicted low flow through a potentially stenotic shunt, maintenance of systemic vascular resistance becomes critical to perfuse the lungs, whereas in patients with an adequately sized shunt, a sudden drop in pulmonary vascular resistance will make it too large leading to an overflow situation. On the other hand, because the main goal for the anesthesiologist when approaching a patient after a Norwood procedure is to maintain pulmonary blood flow, it is imperative to avoid hypovolemia, significant hypercarbia, triggers of pulmonary hypertension crises, such as inadequate anesthesia, and development of elevated mean airway pressure.
Although geometrical features of artificial connections and anatomy in general after Norwood procedures, are not routinely evaluated by anesthesiologists, variables such as aortic annular area and effective shunt area are independent predictors of perioperative morbidity and mortality, 125 and as such, must be taken into consideration by the anesthesia provider when planning strategies to manage these patients.
Conclusion
Both mBT and RV-PA shunt techniques are useful adjuvants to the stage I Norwood operation for palliative management of patients with HLHS. Preference for one or the other procedure depends largely on institutional and individual experience. Currently, there are no clinical data to conclusively favor either technique. Mathematical modeling to display the physical characteristics of the chosen surgical shunt is a valuable tool to predict flow patterns, shear stress, and rate distribution as well as energetic performance at the graft level and relative to ventricular efficiency. Such predictions will enable the surgical team to refine the technique so that hemodynamic complications be anticipated and prevented, and are also important for perioperative management by the anesthesia team. Future research is warranted in fields such as the development of interfacing between image acquisition and computer fluid dynamics technologies, real-time application of CFD to surgical procedures, and feeding of the analysis systems by all disciplines involved in perioperative care of these complex patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.