
Abstract
Anesthesia providers are frequently exposed to radiation during routine patient care in the operating room and remote anesthetizing locations. Eighty-two percent of anesthesiology residents (n = 57 responders) at our institution had a “high” or “very high” concern about the level of ionizing radiation exposure, and 94% indicated interest in educational materials about radiation safety. This article highlights key learning points related to basic physical principles, effects of ionizing radiation, radiation exposure measurement, occupational dose limits, considerations during pregnancy, sources of exposure, factors affecting occupational exposure such as positioning and shielding, and monitoring. The principle source of exposure is through scattered radiation as opposed to direct exposure from the X-ray beam, with the patient serving as the primary source of scatter. As a result, maximizing the distance between the provider and the patient is of great importance to minimize occupational exposure. Our dosimeter monitoring project found that anesthesiology residents (n = 41) had low overall mean measured occupational radiation exposure. The highest deep dose equivalent value for a resident was 0.50 mSv over a 3-month period, less than 10% of the International Commission on Radiological Protection occupational limit, with the eye dose equivalent being 0.52 mSv, approximately 4% of the International Commission on Radiological Protection recommended limit. Continued education and awareness of the risks of ionizing radiation and protective strategies will reduce exposure and potential for associated sequelae.
Introduction
Anesthesia providers may be exposed to radiation in the operating room (OR) and out-of-OR locations. This is most often due to the frequent use of intraoperative or intraprocedural mobile radiography, fluoroscopy, and computed tomography. For example, one study found that even though individual anesthesia providers received relatively small episodic exposures, the aggregate radiation exposure to members of an anesthesia department doubled after staffing an electrophysiology laboratory. 1 Routine radiation monitoring may be warranted for anesthesia providers who frequently work in areas where fluoroscopy is used to obtain real-time moving images of the interior of the patient. 2
Physician education in radiation safety is important to protect patients and providers. A national survey of urology trainees found insufficient protective equipment usage and occupational radiation monitoring as well as inadequate resident education in radiation safety. 3 A survey of resident physicians at a large academic medical center demonstrated inadequate knowledge of radiation safety across specialties and postgraduate training years. 4 A survey of US vascular surgery trainees revealed inconsistent formal radiation safety training but found that those who had received formal training were more knowledgeable and were more likely to monitor exposure and practice dose reduction strategies. 5 A radiation safety educational program for orthopedic surgery residents led to decreased radiation exposure to residents and patients, 6 and an online course on the safe use of fluoroscopy for radiology residents decreased patient dose without affecting diagnostic quality. 7
Anesthesiology residents in our department were surveyed electronically in 2014. Of the 57 of 78 (73%) residents who responded, 82% had a “high” or “very high” level of concern about occupational ionizing radiation exposure, and 94% of resident respondents indicated interest in educational materials about radiation safety (Table 1). The needs assessment also revealed a preference for the curriculum on radiation safety to be presented as a formal classroom-based didactic lecture presentation and also be made available as a written handout distributed to all anesthesiology residents.
Anesthesiology Resident Radiation Safety Survey Results (57 Respondents, 73% of All Residents). a
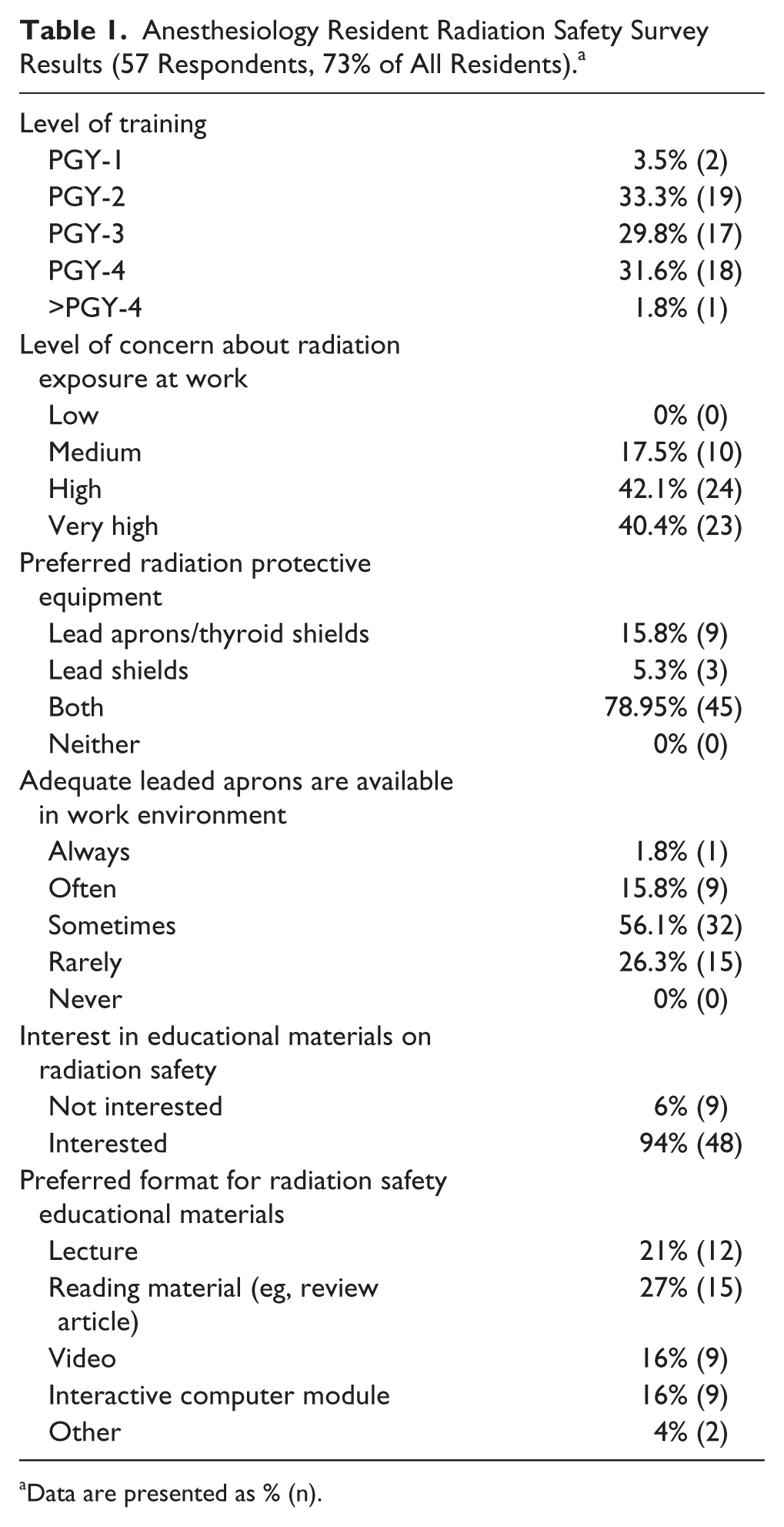
Data are presented as % (n).
The goal of this article is to summarize the key learning points for radiation safety related to basic physical principles, effects of ionizing radiation, radiation exposure measurement, occupational dose limits, radiation and pregnancy, sources of radiation exposure, factors affecting occupational exposure such as positioning and shielding, and monitoring. This information may be useful as a curriculum for other trainees and practicing physicians. Resident-led projects to improve access to lead aprons and to measure exposure are also described to illustrate how knowledge about radiation safety was used to improve the work environment.
Physical Principles
X-rays are produced when a high voltage (50-150 kVp) is applied to a tungsten target in an X-ray tube and electrons, or current, flow through the X-ray tube. A heated filament (cathode) releases electrons, which are accelerated using an electrical potential gradient, known as voltage, in a tube toward a tungsten target (anode). The flow of electrons from the cathode to the anode is referred to as current. When the electrons interact with the anode most of the energy creates heat but some of the energy creates X-rays. Increasing tube current (mA) increases the quantity of X-rays, whereas increasing the voltage (kVp) increases the number of X-ray photons produced per unit time and the penetrating power of X-rays. 8
Effects of Ionizing Radiation
The adverse effects of ionizing radiation can either be deterministic, stochastic, or both. 9 Deterministic effects are measured by the peak dose and refer to cell death at the tissue level. These effects cause predictable tissue damage when the dose of radiation exceeds a certain threshold, and may result in skin erythema and desquamation, lens opacities and cataracts, bone marrow suppression, gonadal injury and sterility, and organ atrophy. For example, the incidence of lens opacities among interventional cardiologists is 5-fold higher than controls and is correlated with occupational exposure. 10 Stochastic effects are measured by the effective dose and refer to radiation-induced DNA damage and subsequent mutations that are linked to the induction of cancer or other genetic effects. Stochastic effects are cumulative with a long latency period, and the probability of the adverse effect increases with dose. There is no “safe” dose below which possible malignancy or genetic damage will not occur.
Radiation Exposure Measurements
Radiation exposure is defined as the quantity of X-rays or gamma radiation required to produce an amount of ionization (electric charge) in air at standard temperature and pressure. When an individual is exposed to radiation, only a portion will be absorbed by the body, while the remainder is reflected or scattered.
The absorbed dose is the amount of ionizing radiation energy absorbed by a unit mass of material, and is measured in the SI unit gray (Gy). One Gy is the deposit of 1 joule of radiation energy in 1 kg of matter. The equivalent dose refers to the absorbed dose multiplied by a radiation weighting factor (wR) specific to the type of radiation and accounts for biologic “harmfulness” of different types of radiation. For diagnostic X-rays, the weighting factor is equal to 1. The equivalent dose is measured in the SI unit Sievert (Sv). The effective dose, also measured in Sieverts, is the weighted sum of equivalent doses in all specified tissues and organs. It is calculated by multiplying the equivalent dose to each organ by a weighting factor (WT) determined by the organ’s radiosensitivity and is used to estimate overall long-term stochastic risk 11 (Table 2). 12 Although the estimated dose targets the portion of the body exposed, it is not possible to directly calculate and can only be estimated.
International Commission on Radiological Protection Recommended Tissue Weighting Factors.
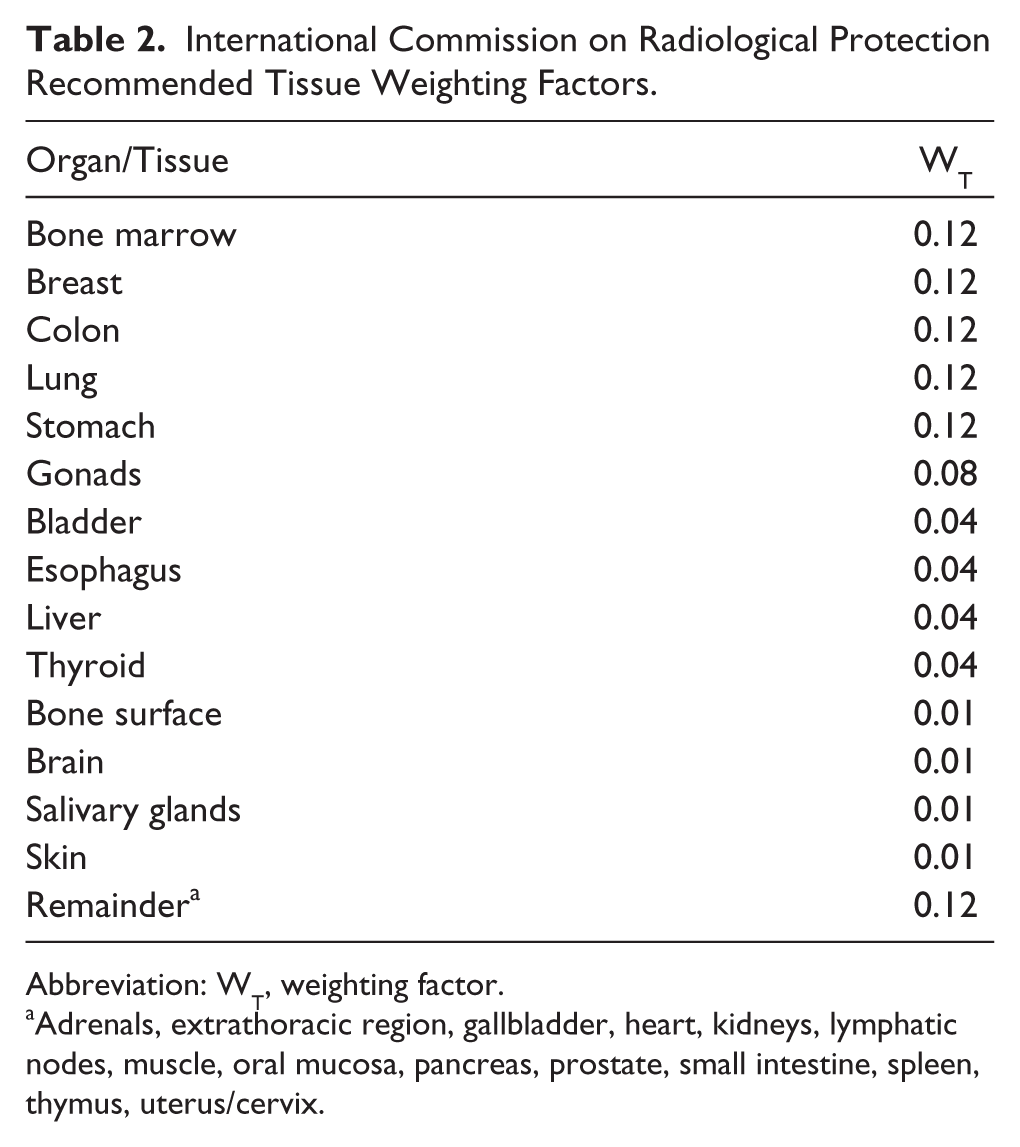
Abbreviation: WT, weighting factor.
Adrenals, extrathoracic region, gallbladder, heart, kidneys, lymphatic nodes, muscle, oral mucosa, pancreas, prostate, small intestine, spleen, thymus, uterus/cervix.
On average, individuals are exposed to approximately 1 to 3 mSv of natural background radiation from cosmic and terrestrial sources annually. Typical patient doses vary by imaging modality (Table 3). 13 One minute of fluoroscopy is approximately equivalent to 100 to 1000 chest radiographs. 14
Average Patient Radiation Doses by Imaging Modality.
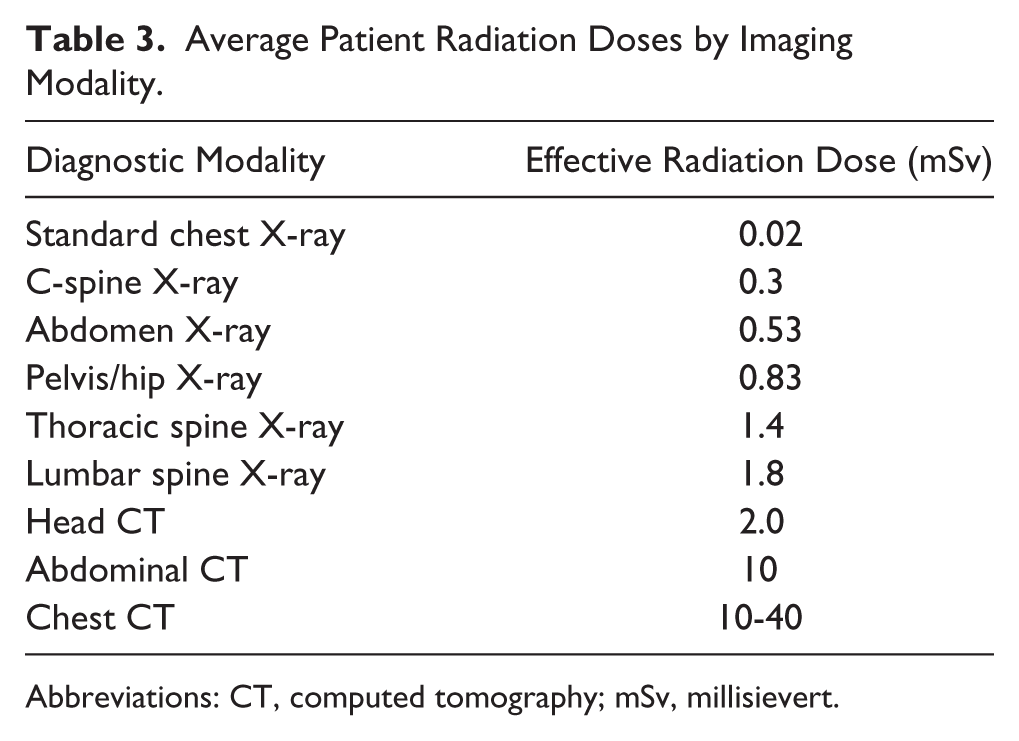
Abbreviations: CT, computed tomography; mSv, millisievert.
Occupational Dose Limits
Recommended maximum safe doses have been established based on epidemiological studies of atomic bomb survivors and radiation workers. In the United States, individual state governments set occupational dose limits. However, most use the National Council on Radiation Protection and Measurements’ recommended effective dose limit of 50 mSv in any given year and a lifetime limit of 10 mSv times the individual’s age in years. 15 In the European Union, the dose limits recommended by the International Commission on Radiological Protection (ICRP) are used. Individual countries have set stricter limits, such as Germany’s 400-mSv lifetime dose limit.
The recommended equivalent dose limit is 500 mSv per year for skin (averaged over 1 cm2 of the most irradiated area of skin) and extremities. 16 In 2011, the ICRP proposed a new equivalent dose limit for ocular lens of 20 mSv per year averaged over 5 years, not exceeding 50 mSv in any single year (which was decreased from the previous limit of 150 mSv per year). 17 The World Health Organization recommends investigation when monthly exposure reaches 0.5 mSv for effective dose, 5 mSv to the lens of eye, or 15 mSv to the hands or extremities. 18
Radiation and Pregnancy
The National Council on Radiation Protection and Measurements recommends an occupational fetal radiation exposure of less than 5 mSv for the entire pregnancy or less than 0.5 mSv per month of pregnancy. 15 The ICRP recommends an exposure of less than 1 mSv for the entire pregnancy. In the United States, workers who do not wish to declare their pregnancy are not required to do so.
Preconception irradiation of either parent’s gonads has not been shown to result in increased risk of cancer or malformations in offspring. 19 Compared to control populations exposed to background radiation (<1 mGy over the gestational period), embryos or fetuses exposed to fewer than 50 mGy of radiation during gestation have no increased risk of induced miscarriages, cancer, or congenital malformations.
In doses exceeding 500 mGy, the potential noncancer health effects of prenatal radiation exposure include death, miscarriage, growth retardation, neuromuscular deficiencies, severe mental retardation, and brain and major malformations. The first trimester is the period of highest risk. Threshold doses for these deterministic effects are well above those received by health care professionals wearing appropriate personal protective equipment. The probability of live birth without malformation or cancer is reduced by 0.002% following conception exposure of 0.5 mSv and by 0.1% following exposure of 10 mSv. In utero exposure to ionizing radiation (>6% in doses above 500 mGy) is associated with increased risk of childhood malignancy, especially leukemia (Table 4). 8
Probability of Bearing Healthy Children as a Function of Radiation Dose.
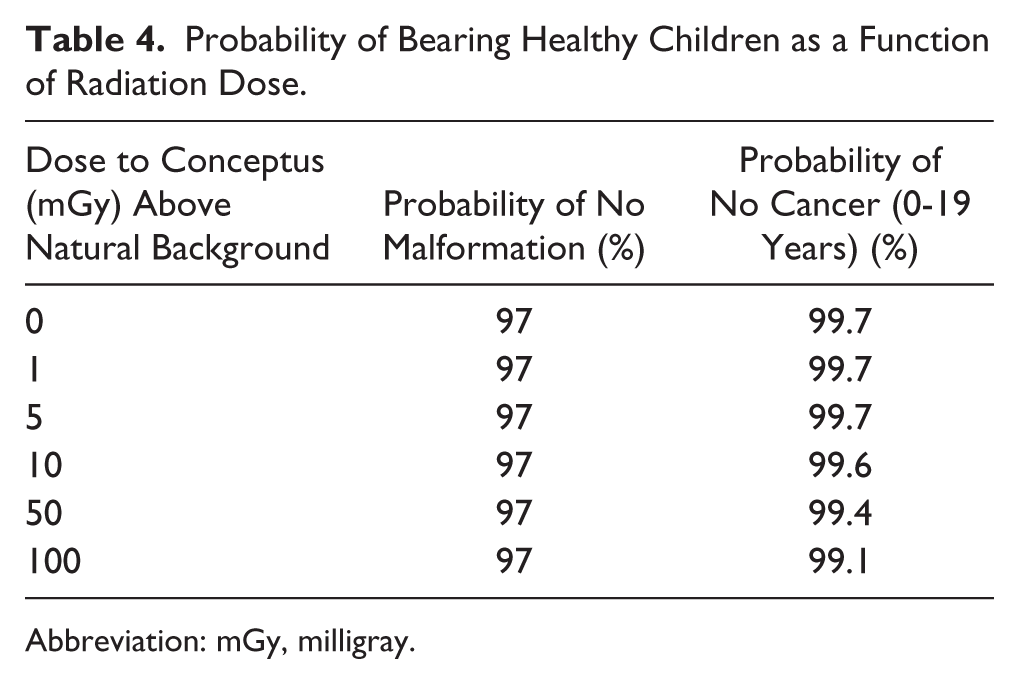
Abbreviation: mGy, milligray.
Sources of Exposure
For every 1000 photons that reach the patient, approximately 100 to 200 are scattered, 20 reach the image detector, and the rest are absorbed. 11 Sources of occupational exposure can be divided into direct exposure from the primary X-ray beam, scattered radiation from the patient body surface, and leakage X-rays emitted from the X-ray tube in areas other than the primary beam. 16
Of these 3 sources, scattered radiation from the patient composes the majority of occupational exposure. In other words, scattered radiation is the main source of radiation with the primary source of scatter being the patient. Thus, utilizing a lead shield as the only means of personal protective equipment may be less effective than the combination of a lead shield and lead apron to minimize personal exposure to scattered radiation. The scattered radiation dose is 1/1000 of the entrance skin dose at 1 meter from the center of the X-ray field. Larger patients generate more scatter due to the increased voltage and current of X-ray beams necessary for better visualization.
Leakage X-rays contribute minimally to occupational radiation exposure. Equipment is required to be checked periodically for radiation leakage. Regulations limit maximum equipment leakage levels to 1 mGy per hour at 1 meter from the X-ray tube for maximum tube potential and current.
Typical fluoroscopy doses are 0.001 to 0.01 mGy per hour at the operator’s position. Whereas the dose output of X-ray units is regulated, the dose to the patient is not regulated or typically measured. 8 Steps can be taken to minimize patient exposure including placing the patient as far from the X-ray tube and as close to the image intensifier as possible.
Factors Affecting Occupational Exposure
Nonmodifiable factors affecting occupational exposure can be related to the procedure and patient, such as complexity of the procedure and body size of the patient. It is crucial for the proceduralist to minimize the radiation dose in as many ways as possible, including minimizing fluoroscopy time and the number of acquired images and taking advantage of user-selected radiation dose reduction features of the imaging equipment. Practitioners utilizing ionizing radiation as part of a procedure should adhere to the principle of ALARA (“as low as reasonably achievable”) to achieve adequate imaging to properly perform the procedure. 11
While previous studies of orthopedic surgeries utilizing intraoperative fluoroscopy suggested minimal exposure to anesthesia providers,20,21 a study of endovascular thoracoabdominal aortic aneurysm repairs found large variation in exposure among OR personnel, with the dosimeter located on the anesthesia machine itself receiving 15 times the dose of the scrub nurse. 22 At one pediatric hospital, anesthesiologists working in the OR received minimal exposure to radiation, but those working in the cardiac catheterization laboratory received significantly higher exposure, with dosimetric readings ranging from 0.2 to 1.8 mSv per month. 2 Another study of anesthesia providers demonstrated that over a period of 6 months, the combined net radiation exposure was 0.28 mSv for endoscopic retrograde cholangiopancreatography procedures and 2.32 mSv in the cardiac catheterization suite. 23 This highlights the need for monitoring to quantify exposure and methods to decrease personnel exposure. For anesthesia providers, modifiable factors to reduce exposure include optimizing positioning and shielding.
Positioning
The power of the radiation beam is attenuated according to the inverse square law (1/distance2). Therefore, maximizing distance from the radiation beam and the patient to the extent possible is important as exposure is thought to be minimal at a distance of more than 36 inches. 20 This safe distance may be compromised if the anesthetizing location is quite small, which limits the ability to adequately distance oneself from the source of radiation. In fact, most of the exposure to anesthesia providers is from scatter off of the patient on the side of the beam.
The power of reflected radiation is inversely related to the angle between the radiation beam and the target. Importantly, at the same distance from the field, the exposure on the side of the X-ray source far exceeds that on the side of the image intensifier, which allows an image to be displayed on a monitor (Figure 1). 24 Often the interventionalist performing the procedure is positioned on the side of the image intensifier, leaving the anesthesia provider closer to the X-ray source.
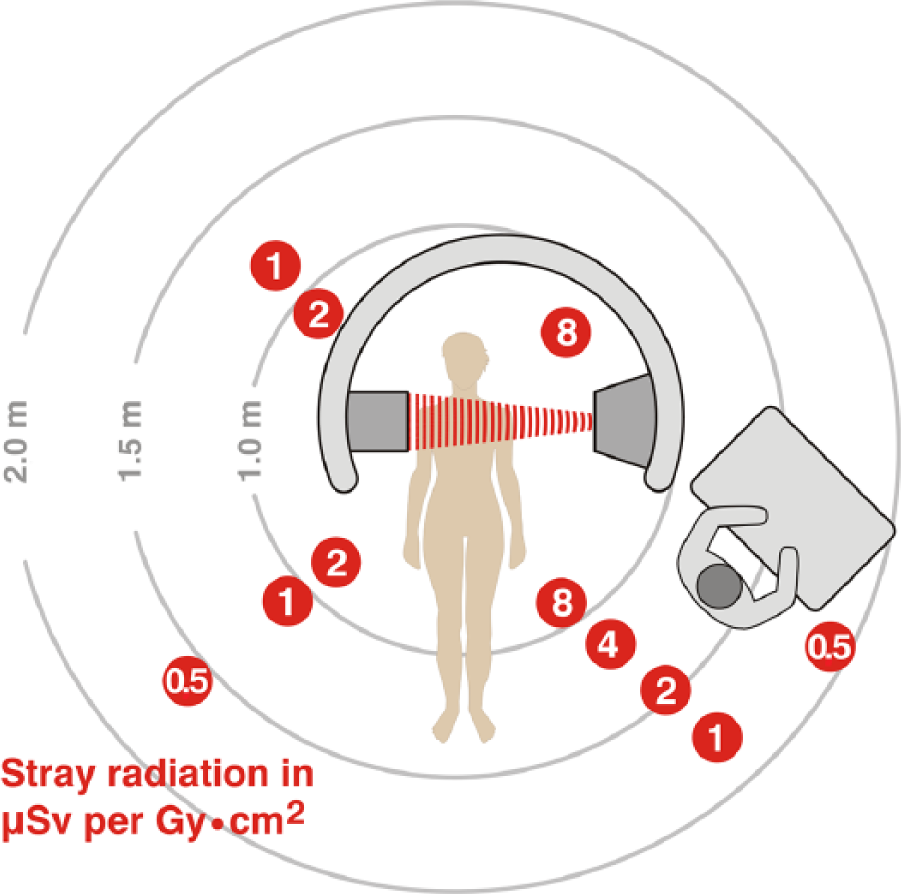
Distribution of scatter radiation from a lateral X-ray source showing higher concentrations of scatter on the side with an X-ray source. Units are µSv radiation exposure to personnel per Gy cm2 of total radiation emitted by the X-ray tube. This figure was modified and used with permission from Valentin. 24
Shielding
Appropriate shielding is important in protecting individuals from radiation exposure. This includes structural shielding embedded into the walls of the procedural suite. Mobile, transparent leaded acrylic shields offer protection from direct exposure but are of limited value in protection from scatter. Equipment-mounted shielding includes leaded drapes and leaded acrylic shields suspended from the fluoroscopy table or scanner. Personal protective shielding equipment includes aprons, thyroid shields, eyewear, and gloves. 16
Aprons
Traditionally aprons were made of lead-impregnated vinyl and rubber. Newer aprons are made of lighter-weight materials including barium, tungsten, tin, and antimony (alone or as composite with lead). Aprons are typically 0.25 mm lead-equivalent; when wrapped around, the double thickness provides 0.5 mm lead equivalence anteriorly. The transmission of 70 to 100 kVp X-rays is 0.5% to 5% through 0.5 mm lead and 0.6% to 6.8% through 0.5 mm lead-equivalent composite and lead-free aprons. A lead apron covers only approximately four fifths of the active bone marrow. Other vulnerable sites, such as the eyes, must also be protected. Aprons should be stored on hangers with minimal folds and inspected under fluoroscopy annually to detect deterioration and defects. 25
One cannot necessarily assume that the facility will have appropriate shielding resources in place. For example, at our medical center, the 2014 resident survey indicated that there were not enough lead aprons readily available in the ORs (Table 1). Even if a lead apron is available for use, it may not be the appropriate size (eg, paucity of smaller sizes) or design (eg, aprons leaving the back exposed).
A quality improvement project in 2014 was undertaken at our institution to diagnose and address the root cause problem of lead apron access. The resulting intervention was multifaceted but included making the existing lead aprons in the OR suite more easily accessible instead of being locked away. Also, additional sets of lead aprons, particularly smaller sizes, were purchased specifically for anesthesiologist use. These aprons were maintained by anesthesia technicians in the anesthesia workroom and taken out by a formal sign out system to minimize loss. This scenario illustrates the need to study the particular problem at each facility as it will likely differ depending on the facility.
Eyewear
The eye is one of the most sensitive organs to radiation exposure. In 2011, the ICRP proposed a new equivalent dose limit for ocular lens of 20 mSv per year averaged over 5 years, not exceeding 50 mSv in any single year (decreased from previous limit of 150 mSv per year). 17 Radiation protective eyewear is important as studies have shown that in the neuro-interventional radiology suite, the scattered radiation exposure (likely due to the lateral beam) to the anesthesia provider’s eyes can be up to 3 times that of the interventionalist. 26
Prescription glasses made of plastic offer inadequate protection (5% reduction in radiation exposure) while those made of optical glass offer modest protection (30% to 40% reduction). Leaded eyeglasses generally provide 0.5 or 0.75 mm lead-equivalent protection (98% reduction) but can be compromised by backscatter from the head and lack of lateral eye shielding.16,25
Since various modes of shielding provide additive protection, combining multiple shielding modalities (eg, shields, aprons, eyewear, drapes) will minimize exposure. In our 2014 survey of residents, almost 80% reported using leaded aprons with thyroid shields in addition to lead shields when working in rooms utilizing radiation (Table 1).
Monitoring
Dosimeters to measure personal exposure are available to personnel working in high-risk radiation exposure areas. The most common type of dosimeter is the film badge, which has a radiation-sensitive film loaded into a plastic holder containing filters that allow the identification of type of radiation exposure. Film badges are heat and moisture sensitive. Alternatively, optically stimulated luminescent dosimeters can be used instead of film badges. These thermoluminescent dosimeters contain small chips of lithium fluoride or calcium fluoride crystals. They are small and can be loaded into plastic rings to measure finger exposure. They are also heat sensitive.
Dosimeters are person specific and must not be shared. They are usually assigned to monitor a period of up to 3 months. If recorded exposures reach 10% of allowable limits, then they are exchanged monthly. When a single dosimeter is worn, it is placed outside a shielded garment or thyroid collar. When 2 dosimeters are worn in the case of pregnancy, one is placed at collar level outside the lead apron or thyroid collar and the other at waist level under the lead apron. 8 The shielded waist dosimeter is used to estimate fetal dose. This may be an overestimate of actual fetal dose because it does not account for attenuation by the mother’s tissues.
Resident-Led Dosimeter Project
We implemented an opt-in radiation dosimeter program for the anesthesiology residents. The Institutional Review Board reviewed this program and granted exemption since this initiative was deemed quality improvement and did not meet the federal regulatory definition of research. Fifty-one residents initially agreed to participate and were given a ring dosimeter for 3 months to measure shallow dose exposure, which was then exchanged for a thermoluminescent dosimeter to measure deep, eye, and shallow dose exposure for the subsequent 3 months. All residents also received an occupational radiation safety lecture by Health Physics and were given instructions on dosimeter usage. After dropouts, full exposure data were collected from 41 residents from August 1, 2015, to February 1, 2016 (Table 5).
Dosimetry Data Results From Anesthesiology Residents (Units in mSv).
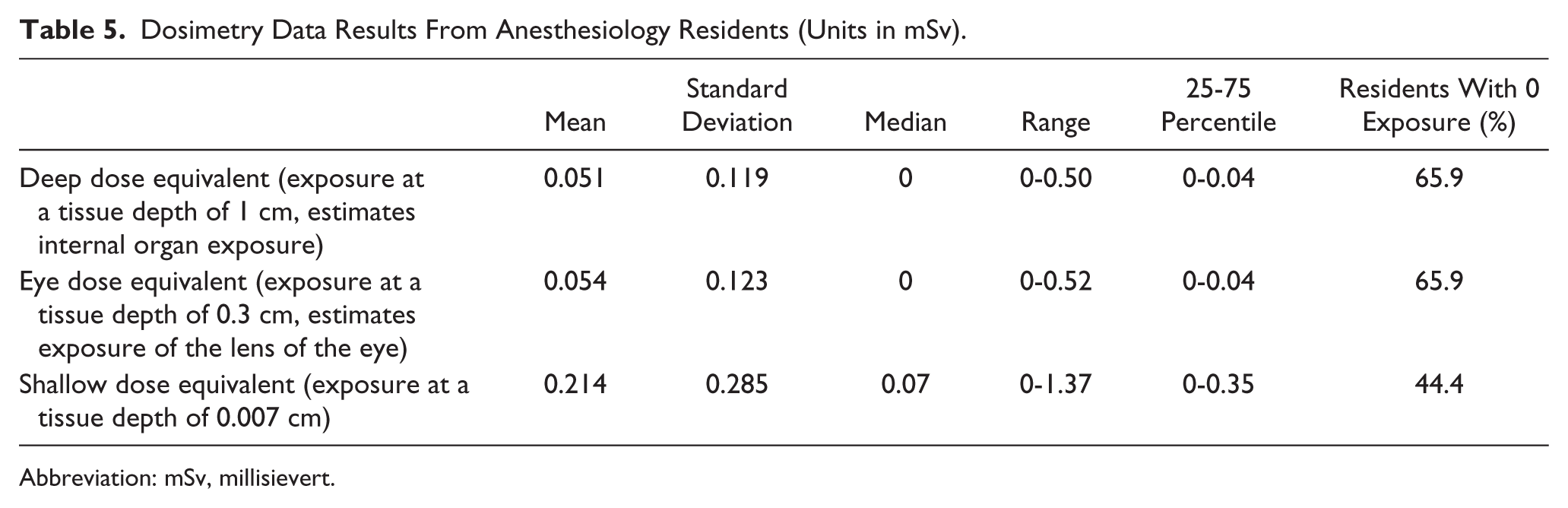
Abbreviation: mSv, millisievert.
The measurements indicated that the anesthesiology residents had low overall measured occupational radiation exposure. The highest deep dose equivalent value recorded by one resident was 0.50 mSv over a 3-month period, approximately 10% of the ICRP occupational limit, with the resident also having the highest eye dose equivalent of 0.52 mSv, which is approximately 4% of the ICRP recommended limit.
Conclusion
Anesthesia providers are frequently exposed to radiation during routine patient care in the operating room and remote anesthetizing locations. Anesthesiology residents are concerned about radiation exposure and desire further education about radiation safety, especially common sources of radiation exposure and methods to minimize exposure. Our quality improvement project involving resident exposure and published studies suggest that occupational radiation doses are generally well below the recommended threshold. However, continued education and awareness of the risks, improvements in radiation shielding, and increasing distance from the source of ionizing radiation will reduce exposure and potential for associated sequelae.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.