
Abstract
Atrial fibrillation is the most common cardiac arrhythmia in adults affecting almost 6 million adults in the United States. The 2 most common comorbidities associated with atrial fibrillation are heart failure and thromboembolic events. Heart failure symptoms may be treated with rate control, antiarrhythmic medications or by catheter ablation. Unfortunately, despite optimal medical management, thromboembolic events still occur. Recently, there has been a great deal of interest and innovation in finding an alternative to chronic anticoagulation. Several percutaneous left atrial appendage occlusion devices have been developed over recent years, some of which have proven to be noninferior to anticoagulation in preventing strokes in atrial fibrillation patients. The 2 most widely used left atrial appendage occlusion devices are the WATCHMAN (Atritech Inc, Plymouth, MN, USA) and the LARIAT (SentreHEART, Palo Alto, CA, USA) devices. After a detailed description of the procedures, the anesthetic considerations of each procedure and management of specific adverse events are discussed within this review.
Atrial fibrillation (AF) is the most common cardiac arrhythmia in adults, affecting about 6 million adults in the United States. The incidence and prevalence of AF is expected to double in the next 10 years, attributable to both an increase in the elderly population as well as the improved management of typical comorbidities such as hypertension, diabetes, and obesity. 1 The most common complications associated with AF are heart failure and thromboembolic events. 2 Heart failure symptoms are treated with rate control and antiarrhythmic medications or by catheter ablation. Despite optimal medical management, thromboembolic events may still occur.
Atrial Fibrillation–Related Stroke
Stroke is the third most common cause of death and the leading cause of serious disability in adults within the United States. About 15% to 20% of strokes each year in the United States can be attributed to AF. 3 AF-related strokes are usually severe, lead to permanent disability, and necessitate institutional care more often than with patients who have strokes unrelated to AF. 4
The pathophysiology of AF is characterized by disorganized electrical activity in the atria resulting in a quivering motion instead of organized forceful contractions. The incomplete ejection of blood from the atria into the ventricles causes stasis of blood especially within the left atrial appendage (LAA). The LAA is a trabeculated cul-de-sac, and more than 90% of thromboses in nonvalvular AF and 60% of thromboses in valvular AF originate from this pouch. 5
Anticoagulation for Atrial Fibrillation
AF patients can be stratified according to their CHA2DS2-VASc score (Table 1) for their risk of thromboembolic events. 6 For scores ≥2, oral anticoagulation is recommended. Vitamin K antagonists (eg, warfarin) and non–vitamin K antagonists (eg, dabigatran, apixaban, and rivaroxaban) are clinically effective in preventing strokes in high-risk AF patients.7-9 Unfortunately, maintaining a narrow therapeutic window, patient noncompliance, and major side effects like bleeding have limited the long-term effectiveness of chronic anticoagulation in preventing strokes. 10
CHA2DS2-VASc Score. a
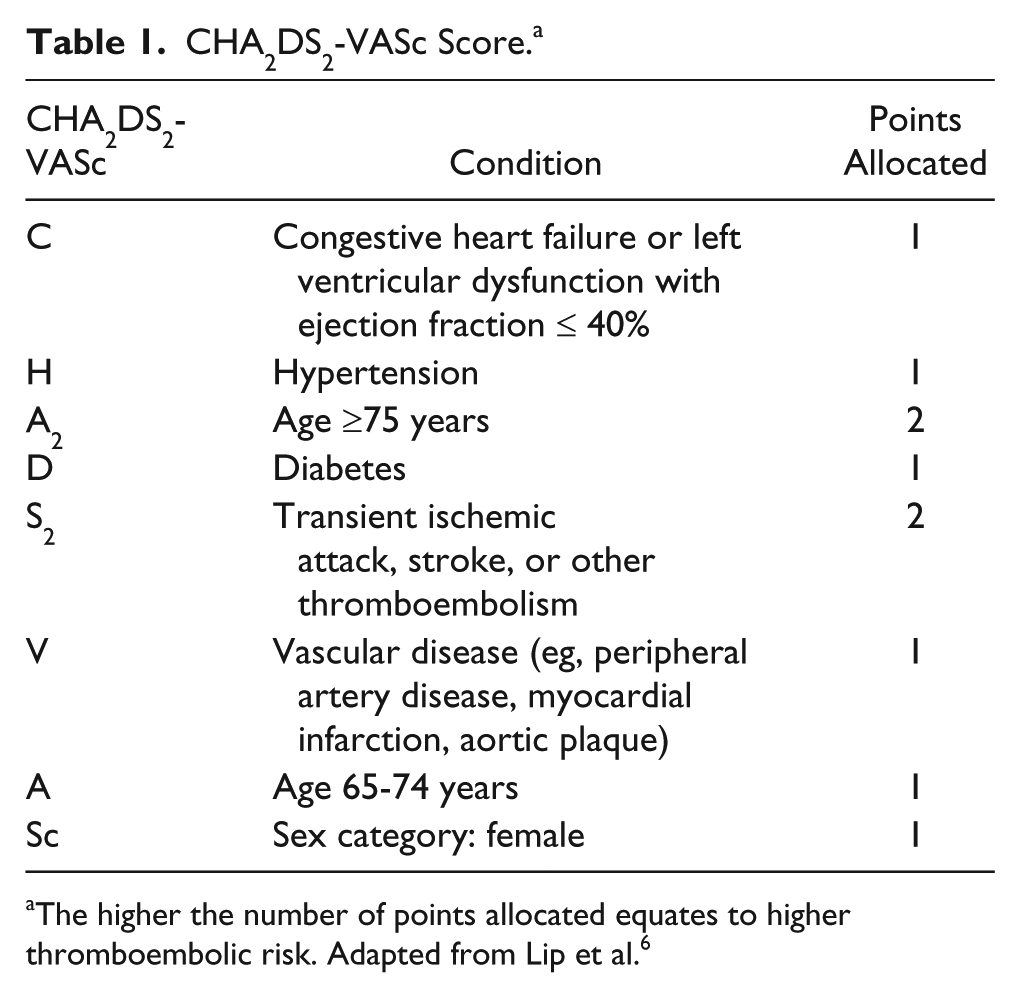
The higher the number of points allocated equates to higher thromboembolic risk. Adapted from Lip et al. 6
LAA Occlusion Devices
Recently, there has been a great deal of interest and innovation in finding an alternative to anticoagulation. Several open and percutaneous LAA occlusion devices have been developed over recent years, some of which have proven to be noninferior to anticoagulation in preventing strokes in AF patients. 11 In this article, we review the most common techniques for percutaneous LAA occlusion and the anesthetic management of patients undergoing these procedures.
Approach for LAA Ligation
There are several different methods for excluding or excising the LAA: (1) an open approach to surgically excise or suture off the LAA in patients undergoing mitral valve surgery or as an adjunct to the maze procedure, (2) an open approach to place an epicardial clip over the LAA via thoracotomy or thoracoscopy, (3) a percutaneous endovascular endocardial approach to deploy an occlusion device from inside the LAA (eg, WATCHMAN device), and (4) a percutaneous epicardial approach that ligates and excludes the LAA externally (eg, LARIAT device). 12
In patients with AF or LAA thrombus undergoing cardiac surgery without the maze procedure, concomitant surgical suturing or stapling of the LAA is usually considered a prophylactic procedure to prevent future ischemic strokes. However, a recent retrospective study reported that LAA closure during coronary artery bypass grafting and/or mitral valve surgery actually increased the risk of postoperative AF nearly 4-fold and did not significantly reduce the risk of subsequent ischemic stroke or mortality. 13 The study did not address whether patients who underwent LAA exclusion were continued on anticoagulation. Additionally, several studies have suggested that a communication between the left atrium and LAA may remain in up to 50% of patients undergoing surgical LAA excision.14-18 These findings have made alternative approaches for LAA occlusion more appealing.
Development of Percutaneous Devices for LAA Occlusion
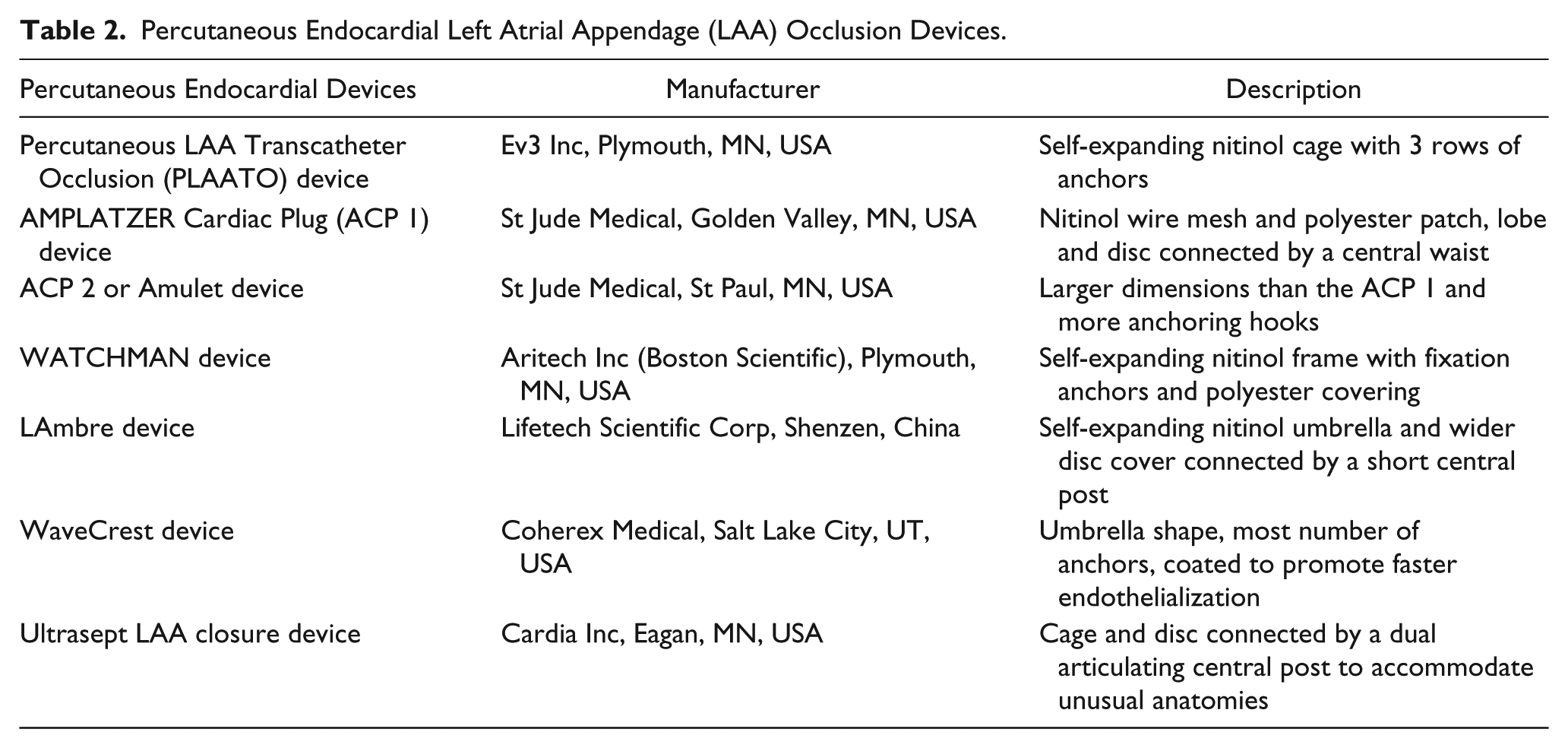
The first percutaneous endocardial device for LAA occlusion was the Percutaneous LAA Transcatheter Occlusion (PLAATO) device. PLAATO withdrew from the market in 2006. The next generation of endocardial devices comprised the AMPLATZER Cardiac Plug (ACP), the ACP2 or Amulet, and the WATCHMAN device. The original ACP no longer has US Food and Drug Administration (FDA) approval for use in the United States, but the Amulet is used widely in Europe and is being trialed in the United States. 19 Newer endocardial LAA occluders include the LAmbre, WaveCrest, and Ultrasept LAA closure devices. However, none of these newer devices are currently available for commercial use in the United States. 20 A brief description of each of these percutaneous endocardial LAA occlusion devices can be found in Table 2.
Percutaneous Endocardial Left Atrial Appendage (LAA) Occlusion Devices.
Endocardial devices require at least a short duration of perioperative anticoagulation for epithelialization to occur and involve some risk of device embolization or infection. In contrast, epicardial LAA occlusion devices do not leave behind any foreign bodies within the heart that need to epithelialize or that can embolize. There are several devices that can deliver a suture or clip over the LAA via a surgical incision (ie, sternotomy, thoracotomy, or thoracoscopy), and there are ongoing investigations to find a way to do so with percutaneously.
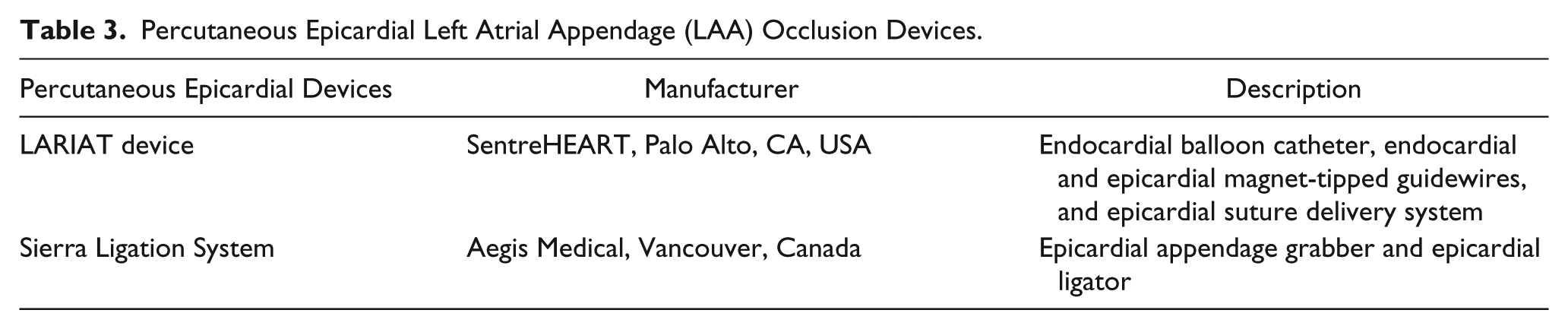
The percutaneous epicardial LAA occlusion devices include the LARIAT and the Sierra Ligation System. The LARIAT device is technically a hybrid procedure in that it involves endo- and epicardial access whereas the Sierra device is completely epicardial. The LARIAT device has been studied much more comprehensively. The Sierra device just recently received FDA approval to initiate clinical trials. 20 A brief description of each of these percutaneous epicardial LAA occlusion devices can be found in Table 3.
Percutaneous Epicardial Left Atrial Appendage (LAA) Occlusion Devices.
Because the techniques and devices used for LAA exclusion are continuously evolving, there are few articles that provide a complete and comprehensive overview of the field. However, the review articles from Bedeir et al, 12 Jazayeri, et al, 19 and Romero et al 20 collectively describe all of the different methods available on the market as well as in trial currently.
Among the percutaneous approaches currently available on the market, the most widely used endocardial device is the WATCHMAN and the most commonly used epicardial device is the LARIAT. 21 After a detailed description of each of these procedures, the anesthetic management of patients undergoing each procedure will be discussed.
WATCHMAN LAA Occlusion Device
Data from the WATCHMAN LAA Closure Technology for Embolic PROTECTion in Patients with Atrial Fibrillation (PROTECT AF) clinical trial showed that the WATCHMAN LAA closure is a safe and effective alternative to anticoagulant treatment to reduce the risk of AF-related stroke. This technology was found to be noninferior to warfarin for the combined endpoint of stroke, systemic embolism, and death among patients with nonvalvular AF who were eligible for warfarin therapy and had a CHADS2 stroke risk score of ≥1. 22 The Prospective Randomized EVAluation (PREVAIL) trial demonstrated an overall 95% success rate for implanting the WATCHMAN device (93.2% for new physicians), and the reported overall 7-day serious procedure- and device-related complication rate was 4.5%. 23
Based on the results from these 2 trials, the FDA approved the WATCHMAN device in 2015 for use as an LAA closure device to reduce the risk of stroke in patients with nonvalvular AF. It remains the only percutaneous LAA closure device approved by the FDA for this purpose. According to data from a prospective registry of 3822 patients who underwent the WATCHMAN procedure since its approval, procedural success was about 95.6% and the complications rates for pericardial tamponade, device embolization, procedure-related stroke, and mortality were 1.02%, 0.25%, 0.08%, and 0.08%, respectively. 24
Description of Procedure
The WATCHMAN device is a self-expanding nickel-titanium frame structure equipped with 10 fixation barbs and a permeable polyester fabric on the left atrial side that eventually epithelializes to seal off the LAA (Figure 1). Although the fixation barbs offer some device stability, the primary way that the WATCHMAN device stays in place is by radial forces created from compression of the device. To create adequate compression, the implanted device is sized to be 8% to 20% wider than the largest transesophageal echocardiography (TEE) measurement of the LAA orifice. The WATCHMAN device is currently available in 5 different sizes.

WATCHMAN device. Digital image (How the WATCHMAN device works: http://www.watchman.com/how-watchman-device-works.html).
The femoral vein is cannulated in the groin and a transseptal sheath is advanced from the right atrium into the left atrium. A guidewire is inserted into the left upper pulmonary vein (to avoid trauma to the LAA) and the WATCHMAN access sheath is exchanged over it. A pigtail catheter is inserted through the sheath and into the left upper pulmonary vein as well. Under fluoroscopic and TEE guidance, the pigtail catheter and access sheath are withdrawn and repositioned into the distal point of the LAA. The pigtail catheter is then removed and the WATCHMAN device is inserted through the sheath. After reconfirming the delivery catheter position, the device is deployed by retracting the access sheath and the delivery catheter. The device remains tethered to a core wire. Once the device position, anchor, and seal are verified, the device is released and the delivery apparatus is removed (Figure 2). 25
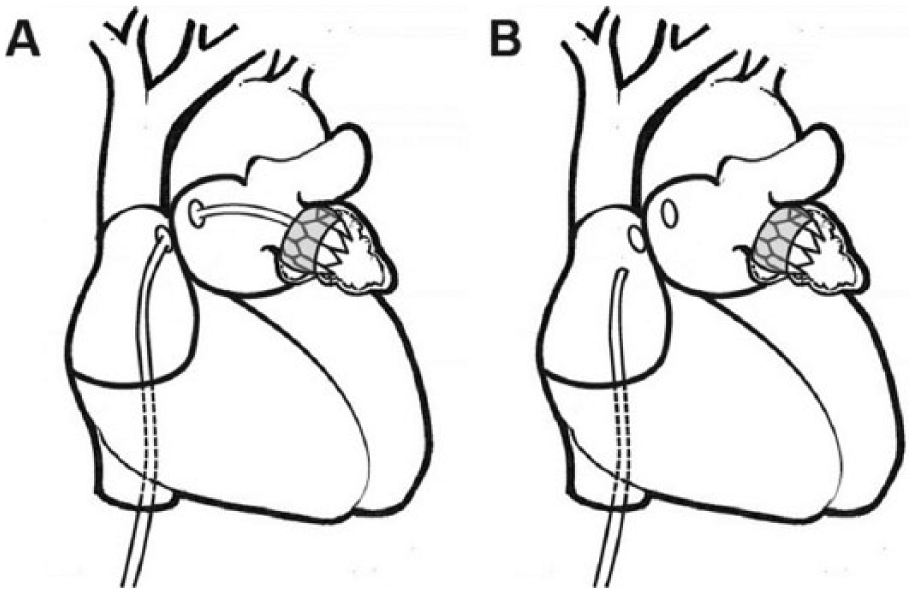
(A) Transseptal puncture with the WATCHMAN device sheath positioned in the left atrial appendage (LAA). (B) LAA exclusion by the WATCHMAN device and removal of the device sheath.
Procedural risks include pericardial effusion, major bleeding, procedure-related ischemic stroke or hemorrhagic stroke, air embolism, and device embolization. Device-related risks include implant failure, incomplete closure, and device-related thrombus.
To confirm adequate LAA exclusion after the procedure, TEE is performed at least prior to discharge and also 45 days after the procedure. Color Doppler flow ≤5 mm around the device has been established as a standard for confirming adequate LAA exclusion. 23
LARIAT LAA Occlusion device
The LARIAT device has 510k clearance from the FDA for soft tissue closure during surgical procedures. The LARIAT device is frequently used off-label for LAA exclusion for stroke prevention in patients with AF. Although there are no published data about the LARIAT from any prospective randomized trials, there are published clinical results from a single center, prospective observational study and a multicenter retrospective study that demonstrate the potential of the LARIAT as a method of LAA closure to prevent AF-related strokes. These studies showed consistent trends of efficacy and safety for LAA closure with successful LAA closure rates reported as 91% to 100% in some studies and serious adverse events noted in 2% to 5% of cases.26,27
Further validation of these findings is currently underway. The aMAZE trial is an active multicenter, prospective, randomized controlled trial that is investigating the safety and efficacy of the LARIAT device and to determine if LAA ligation in conjunction with pulmonary vein isolation and ablation improves maintenance of sinus rhythm in patients with AF. 28
Description of Procedure
The LARIAT procedure requires pericardial access and placement of an epicardial sheath as well as endovascular access for a transseptal puncture and placement of an endocardial wire. The pericardial space is entered via a subxiphoid approach using a micropuncture needle. Once the pericardium is entered and a guidewire is placed in the pericardial space, serial dilations are performed prior to insertion of the pericardial sheath. The sheath is advanced over the guidewire and positioned so that it is on the superior side of the right ventricle and the curve is directed posteriorly.
The femoral vein is cannulated in the groin so that a transseptal puncture can be performed. Once the transseptal sheath is in place, a magnet tipped endocardial wire is placed into the most anterior and superior aspect of the LAA (Figure 3). Positioning can be confirmed by fluoroscopy, TEE, and an LAA angiogram with manual injections of contrast.
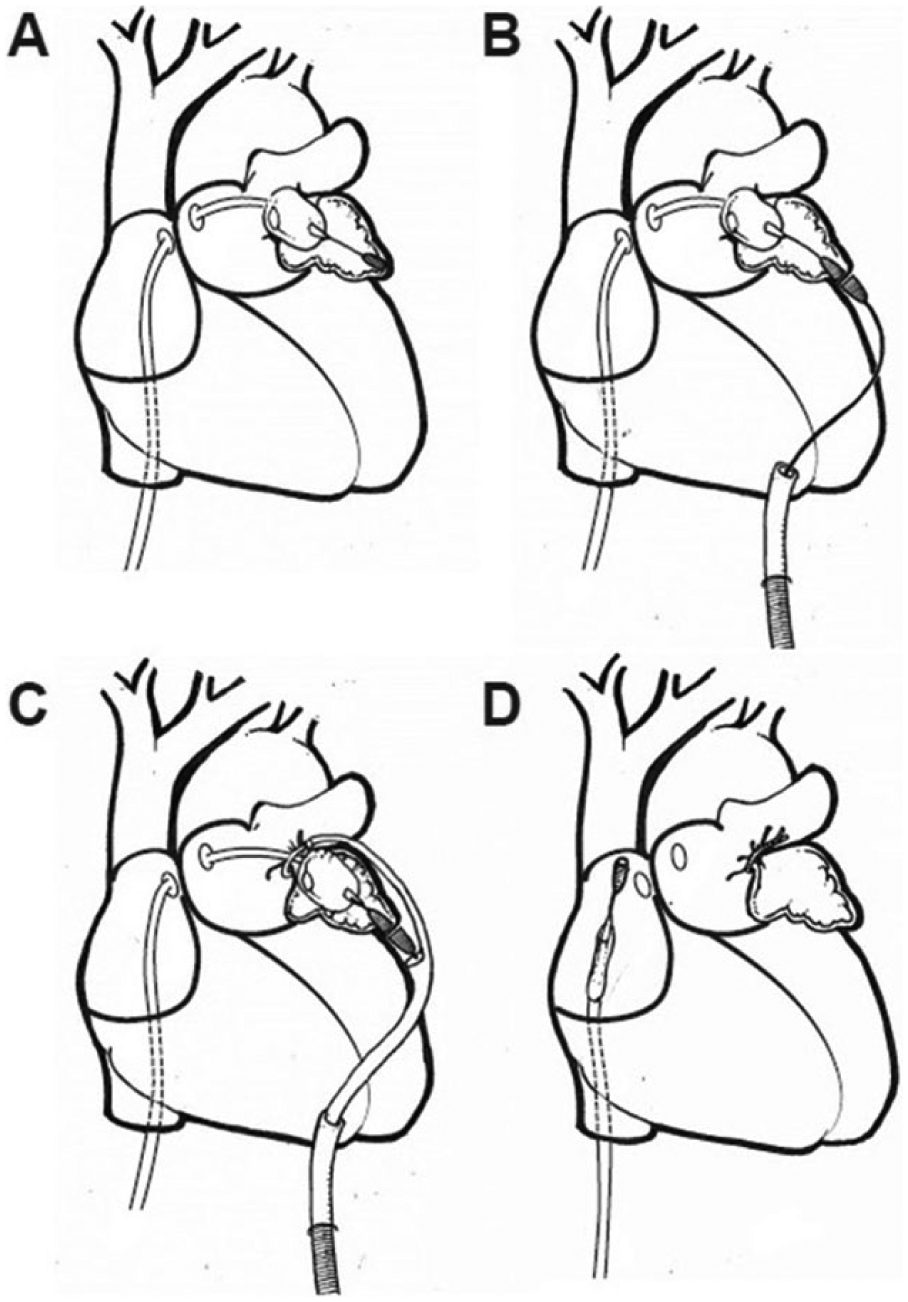
(A) Transseptal puncture with magnet-tipped endocardial wire and balloon catheter. (B) Magnet-tipped epicardial wire connected to the endocardial wire. (C) LARIAT snare tightened around the left atrial appendage (LAA) ostium. (D) LAA exclusion by the LARIAT device and removal of sheath and wires.
A magnet-tipped epicardial wire is then placed into the epicardial sheath and allowed to connect with the endocardial wire (Figures 3 and 4). The LARIAT snare and device is aligned over the LAA with the aid of fluoroscopy and a contrast-filled balloon catheter that is placed at the LAA ostium. The snare is then closed. After complete closure of the LAA is confirmed via angiogram and TEE, the preloaded suture is tightened. The 2 magnet-tipped wires and LARIAT device are removed prior to complete release of the suture. 29
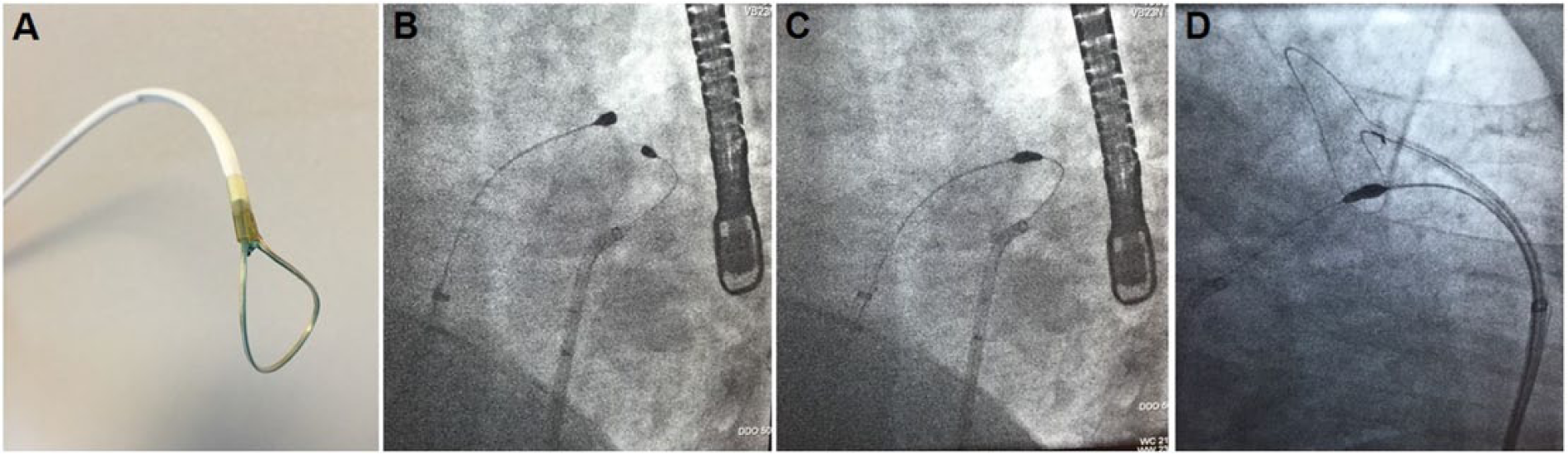
(A) LARIAT device with snare and preloaded suture. (B, C). Fluoroscopic view of magnet-tipped wires connecting across the left atrial appendage (LAA) wall. (D) Fluoroscopic view of LARIAT snare positioned over LAA ostium prior to tightening.
Procedural risks include pericardial effusion or hemopericardium, puncture of the right ventricle or LAA, laceration of epicardial vessels, air embolism, and postoperative pericarditis. Device-related risks include implant failure and incomplete closure. Since there is no residual device that remains within the heart, there is no risk for device embolization or device-related thrombus. Because of the need for epicardial access to the LAA, the LARIAT procedure can be technically more challenging in some patients, especially due to the variability in size, morphology, and orientation of the LAA within the general population.
To confirm adequate LAA exclusion, TEE is performed, at minimum, prior to discharge as well as 30 days, 90 days, and 1 year after the procedure to measure any blood flow between the left atrium and LAA. Color Doppler flow of ≤1 ± 1 mm has been established as a standard for confirming adequate LAA exclusion. 28
Preoperative Evaluation for Anesthesia
A thorough history and physical should be obtained from the patient prior to proceeding with an LAA occlusion procedure. Special attention should be directed toward pertinent cardiac history such as whether the AF is paroxysmal versus chronic, duration of AF, associated valvular abnormalities, comorbidities, CHA2DS2-VASc score, and whether the patient is on any antiarrhythmic medications or anticoagulation. Marginal renal function is of concern because of the use of intravenous contrast during fluoroscopy. Because of the risk of bleeding during percutaneous LAA occlusion procedures, any anticoagulation beyond aspirin should be stopped for an appropriate amount of time prior to the day of surgery with confirmation on the morning of surgery of complete reversal. 28
A recent electrocardiogram (ECG) should be reviewed. A preoperative computed tomography (CT) scan should be performed to determine LAA size and position. Additionally, TEE is imperative to determine the presence of an intracardiac thrombus and to diagnose any valvular abnormalities that may alter anesthetic induction and maintenance. An echocardiogram may also provide additional information regarding any unusual anatomy that could influence the cardiologist’s approach.
If an intracardiac thrombus is detected preoperatively, anticoagulation should be started or continued. Serial TEEs should be performed until the thrombus is no longer present before proceeding with a percutaneous LAA occlusion procedure. Patients with a history of an atrial septal defect repair, atrial septal defect closure device, or an aneurysmal interatrial septum should not undergo an LAA occlusion procedure that involves a transseptal puncture. 25
The LARIAT procedure requires that the LAA be freely mobile within the pericardial space. Therefore, previous open heart surgery is an absolute contraindication to performing a LARIAT. Relative contraindications include pericarditis, uremia, radiation therapy, and constrictive body habitus (eg, morbid obesity, pectus excavatum, etc). 29
Choice of Anesthetic
Because the WATCHMAN and LARIAT procedures both require continuous TEE monitoring, they are traditionally performed with general endotracheal anesthesia (GETA) in the USA. However, a recent European survey suggests that several institutions have performed percutaneous LAA occlusion procedures with monitored anesthesia care (MAC) instead. 30 Unfortunately, there is little information regarding the choice of medications, dosages, whether an anesthesiologist is present, or the success rate of the LAA occlusion procedure.
Chan et al 31 reported on 11 patients who underwent either a WATCHMAN or an ACP device implantation. Each patient underwent the procedure under conscious sedation with intravenous midazolam and fentanyl as well as continuous TEE monitoring. The study showed a 100% success rate for procedure completion and no procedure-related complications from using conscious sedation. 31 Limitations of this study are that it was a small study, it was not randomized with a GETA control group to compare procedure times, and it did not address any metrics for patient satisfaction.
While continuous TEE monitoring is one of the limitations to choosing MAC over GETA, some institutions have reports successful use of catheter-based intracardiac echocardiography (ICE) instead of TEE. A recent study from Frangieh et al 32 demonstrated successful deployment of the WATCHMAN device under MAC and with fluoroscopy and ICE guidance. According to their procedure protocols, the ICE catheter can be inserted through the transseptal sheath so that only one transseptal puncture is necessary. Although the procedure success rate from ICE imaging was comparable to those from TEE imaging, the procedure times with ICE were longer and LAA measurements for device size selection were still obtained from a preprocedure TEE. 32
The literature that does exist regarding the use of MAC or conscious sedation during an LAA occlusion procedure almost exclusively pertains to the WATCHMAN device or another percutaneous endocardial device. There is little information regarding MAC for patients undergoing a LARIAT procedure at this time, although it potentially could be possible with adequate local infiltration at the groin and subxiphoid catheter entry points.
Ultimately, the patient must tolerate the presence of the TEE probe, be able to lay flat for the duration of the procedure, and lay still during key intraoperative events like transseptal puncture and device deployment. Several clinical scenarios may definitively preclude the use of MAC during either procedure. The cardiologist’s experience in performing the procedure as well the institution’s history of complications should be taken into consideration. If there is a potentially difficult groin cannulation or a contraindication to having an unsecured airway (eg, obstructive airway or increased aspiration risk), GETA is the better option. The choice of anesthetic should be discussed by both the anesthesiologist and the cardiologist.
At our institution, percutaneous endocardial and epicardial LAA occlusion procedures are performed under GETA. Induction and maintenance medications are at the discretion of each anesthesiologist. Continuous TEE monitoring is performed by either the anesthesiologist or a member of the cardiology team. Short acting muscle relaxants are used with the intent to extubate all patients at the end of the procedure.
Intraoperative Management
Routine monitors are utilized for an LAA occlusion procedure. Defibrillator pads should be applied to the patient in case of prolonged arrhythmias. ECG leads and defibrillator pads should be applied so as to not interfere with fluoroscopic imaging. Although this procedure may be performed with a noninvasive blood pressure cuff, an arterial line is generally preferred because of the likelihood for arrhythmias and the potential for acute cardiovascular decompensation. Central venous access is not necessary as long as adequate large bore peripheral intravenous access can be obtained.
Fluid resuscitation may be necessary in the setting of arrhythmias and/or poor cardiac filling. The use of crystalloid and colloid fluids is at the discretion of the anesthesiologist but must be used judiciously in consideration of the patient’s comorbidities and underlying cardiac function. Both procedures carry a risk of pericardial effusion and major bleeding. As a result, an active type and screen should be ordered. Compared with the WATCHMAN procedure, the LARIAT procedure involves a somewhat higher risk for bleeding because of the additional pericardial access. Therefore, an active type and cross should be ordered with blood products available in the room. Detection of pericardial effusion, hemopericardium, and/or cardiac tamponade can be done continuously by TEE and fluoroscopy.
TEE Assessment of the LAA
Intraoperative fluoroscopy may not be adequate alone for assessing LAA anatomy, especially if there are multiple overlying lobes or complex orientation. Therefore, intraoperative TEE is extremely important during any LAA exclusion procedure. CT scans and 3-dimensional reconstructions may be obtained at the discretion of the cardiologist to complement intraoperative fluoroscopy and TEE.
Assuming there are no contraindications to placement, a TEE probe should be inserted and the LAA should be viewed in at least 4 different multiplane views to assess LAA ostium size, LAA shape, LAA depth, number of lobes, and position. There is an excellent video article from Möbius-Winkler et al 33 that delineates the appropriate views for assessing the LAA. Although the article specifically refers to the WATCHMAN device and procedure, the TEE views described are applicable to any LAA exclusion procedure.
The TEE views ideal for assessing the LAA are (1) 0°-20° corresponding to the mid-esophageal (ME) 4-chamber view; (2) 45°-60° ME mitral commissural view; (3) 90° corresponding to the ME 2-chamber view; and (4) 120°-135° corresponding to the ME aortic valve long-axis view. Although these views generally correlate with standard TEE perioperative views, minor adjustments need to be made in order to visualize the LAA optimally. The 0° and 135° views usually yield the largest LAA ostial diameter measurements. The ostium should be measured from the superior edge of the mitral valve annulus to the limbus of the left upper pulmonary vein or to the ligament of Marshall (ie, Coumadin ridge).25,33
The WATCHMAN device is available in 5 different sizes (21-, 24-, 27-, 30-, and 33-mm diameters). Since it relies on some degree of compression for stability, the WATCHMAN device will not accommodate maximum LAA ostium sizes that are <17 mm or >31 mm. In addition, the WATCHMAN device measures the same dimension in both diameter and height. Therefore, the LAA depth must be able to accommodate the chosen device size. 25 The LARIAT procedure may not be successful if the LAA is too large (>45 mm in width), has multiple lobes directed at different angles, lies behind the pulmonary artery, or if the heart is rotated posteriorly. 29
Key Intraoperative Events
WATCHMAN
Because of FDA mandates, all physicians who are implanting the WATCHMAN device must undergo thorough knowledge-based and procedure-based training, including simulation. All WATCHMAN implantations must also be performed with a Boston Scientific–employed and –trained clinical specialist in attendance. In addition to helping the clinician maintain procedural standards and potentially troubleshoot the device, he or she also documents device characteristics, procedural performance, and release criteria measurements for an online prospective registry. 24
Prior to transseptal puncture, heparin should be given in a 100 unit/kg dose to achieve a goal activated clotting time (ACT) of at least 250 seconds. The puncture can be guided by fluoroscopy or by TEE via ME bicaval or 4-chamber views.
Positioning of the WATCHMAN device within the LAA both prior to and after deployment is crucial and is performed with the aid of fluoroscopy and TEE. When the pigtail catheter and access sheath are positioned into the distal point of the LAA, a multiplane TEE sweep from 0° to 135° should be performed multiple times to confirm proper positioning. 33 There is a risk of arrhythmias and of LAA rupture as the device is advanced into the LAA and during device expansion.
After the WATCHMAN device is deployed and before it is released from the core wire, appropriate position, anchor, size, and seal must be confirmed. To verify device position, fluoroscopy and TEE are used to confirm that the plane of maximum device diameter is at or is just distal to the orifice of the LAA and that it spans the entire LAA ostium. If the device is too shallow, the device is at risk for embolization. If the device is too distal, the LAA may have an incomplete seal and residual flow into the LAA. To verify device anchor, the physician performs a “tug test” in which the access sheath and delivery catheter are withdrawn 1 to 2 cm away from the device to create tension. The deployment knob is then gently retracted and released. Proper anchoring will show the device and LAA moving in unison. To verify device size, the maximum diameter of the WATCHMAN device is measured from the same TEE views from which the original LAA ostium sizes were measured. The device diameter should be 8-20% smaller than its original dimension consistent with appropriate device compression. Finally, to verify adequate LAA seal, color Doppler flow is used to show no color flow around the device. Small leaks around the device are permissible if they are ≤5 mm. If a color Doppler flow leak >5 mm or a physical gap >3 mm is detected around the device, then the device should be fully collapsed and repositioned. The device position, anchor, size, and seal should be confirmed once again after the device is released from the core wire.25,33
If the device needs repositioning after full deployment and release and if the device is still in the LAA, it can be retrieved and collapsed with the delivery catheter. The risk of complete device embolization is increased if the WATCHMAN device is undersized or if the LAA has unusual morphology, too large an ostium diameter, or is too shallow to accommodate the device height. If the device embolizes to the left atrium or left ventricle, it can be difficult and dangerous to attempt snaring the device within the heart. Instead, the device may be maneuvered anterograde into the aorta using coronary catheters. Percutaneous retrieval can then be attempted in the descending aorta. However, if that is not successful, an open surgical approach may be necessary. 34
LARIAT
During pericardial puncture, entry of the guidewire, and serial dilations, the patient may exhibit arrhythmias such as left bundle branch and premature ventricular contractions. In addition, there is a risk of right ventricular compression, myocardial puncture, hemopericardium, and subsequent tamponade. It is imperative that the cardiologist never advance the epicardial sheath within pericardium unless it is over a guidewire or the LARIAT device itself so as to avoid myocardial puncture. 29
If myocardial puncture does occur, a pigtail drain should be placed in the pericardium. A small right ventricular perforation can cause a self-limited drainage of about 30 to 50 mL of blood. The pigtail can be removed at this point, but a safety guidewire should be left in place in case bleeding reoccurs later during the procedure. If there is continued bleeding, cardiothoracic surgical backup should be notified immediately. Surgical exploration may be required to assess the extent of laceration and to perform a definitive repair. 29
Prior to transseptal puncture, heparin should be given in a 100 unit/kg dose to achieve a goal ACT of at least 250 seconds. The puncture can be guided by fluoroscopy and TEE via ME bicaval or 4-chamber views.
While the LARIAT snare and device are being appropriately aligned over the LAA by the cardiologist, the anesthesiologist should remain vigilant about detecting new arrhythmias and poor cardiac filling. It is also important that the magnet-tipped wires do not disconnect and that they remain in their original positions. If inappropriate tension is placed on the epicardial wire, it can pull the endocardial wire through the wall of the LAA leading to a hemopericardium. If this occurs, the procedure can be aborted and the patient may be managed conservatively with a pericardial drain. Alternatively, the hemopericardium can be managed with a pericardial drain, blood transfusion as needed, repositioning of the wires, and completion of the LARIAT procedure. Ligation of the LAA would stop any further bleeding.
After the LARIAT snare is closed, complete LAA exclusion is confirmed by left atrial angiogram and by TEE color Doppler flow ≤1 ± 1 mm on cross section. It is important for the LARIAT device not to move while the suture is being tightened because this can lead to a laceration or avulsion of the LAA or left atrium. Again, cardiothoracic surgical backup should be notified immediately in the case of brisk bleeding.
Postoperative Management
At the conclusion of either procedure, the cardiologist may let the ACT drift back to normal gradually or reverse the effects of heparin with the administration of protamine. An ACT should be measured to confirm reversal. Assuming the patient remains hemodynamically stable, the patient should be extubated so that a neurologic exam can be performed to rule out any procedure-related strokes. The patient is monitored overnight for development of a pericardial effusion or groin hematoma. Postoperative pain after either procedure is most commonly from groin cannulation and/or presence of a pericardial drain. Nonnarcotics should be sufficient, but narcotics may be added as needed.
After a WATCHMAN procedure, patients should be monitored closely for a pericardial effusion which could further deteriorate into cardiac tamponade. Early and late effusions can be the result of both overt trauma to the LAA from guidewires and catheters or from the device anchors penetrating the thin walls of the LAA. A transthoracic echocardiogram should be performed prior to discharge to rule out an effusion and to confirm device position. If the device cannot be visualized from a subxiphoidal view, then fluoroscopy or TEE should be utilized to confirm device position. 34
After a LARIAT procedure, a pigtail catheter is prophylactically left within the pericardial space overnight in case of fluid accumulation and to prevent cardiac tamponade. A transthoracic echocardiogram is performed prior to removal of the catheter to rule out any pericardial effusions.
The LARIAT procedure entails an increased risk for pericarditis and Dressler syndrome than the WATCHMAN procedure. This is attributed to the inflammatory response that occurs after the LAA is ligated. Colchicine twice daily is generally started on the day of the procedure and continued for 3 to 4 weeks. 35 The dose may be adjusted if patients experience gastrointestinal side effects. If patients do manifest signs or symptoms of pericarditis, nonsteroidal anti-inflammatory drugs and oral corticosteroids may be added. 28 No studies to date have shown if pericardial injection of anti-inflammatory medications can reliably prevent postoperative complications.
Incomplete LAA exclusion after a LARIAT procedure is defined by color Doppler flow of >2 ± 1 mm. 28 Because these leaks are typically central and concentric, some case reports have reported successful leak closure with the use of vascular plugs or septal occluders.36,37
Postoperative Anticoagulation
The risk of thrombus after a WATCHMAN or LARIAT procedure remains low. Because the true incidence is not known and because there have been case reports documenting post-procedure thrombus formation for each device, patients are typically anticoagulated for at least a short period of time.
WATCHMAN patients are anticoagulated with aspirin and warfarin for at least 45 days while the device epithelializes. At that point, if TEE demonstrates stable device position and color Doppler flow around the device is ≤5 mm, then patients are transitioned to aspirin and clopidogrel for up to 6 months. After that, patients may be considered for transition to only aspirin. 23 Of special note, endocarditis prophylaxis should be given to patients during the initial 6 months after WATCHMAN implantation. The cardiologist may extend the period of prophylaxis at his or her discretion. 25
LARIAT patients were originally thought to not require anticoagulation immediately after the procedure because there was no device left behind that needed to epithelialize. However, there have been a few case reports showing evidence of early small thrombus formation at the suture site as well as partial re-openings with communicating flow between the left atrium and LAA. As a result, anticoagulation with warfarin is generally continued for at least 1 to 3 months both to prevent early thrombus formation and to confirm complete occlusion.38-40
Patients may remain in AF even after LAA exclusion. Although the majority of thrombi in AF patients originate from the LAA, not all do. Without medical therapy or ablation to eliminate AF, patients with high CHA2DS2-VASc scores may still be at risk for ischemic strokes. In other words, an LAA exclusion procedure does not eliminate the risk of ischemic stroke completely. However, in the specific population of patients who cannot tolerate long term anticoagulation, an LAA exclusion procedure does decrease the risk of ischemic stroke significantly.
Conclusion
As the prevalence of AF continues to rise in the aging population, the need to manage the risk of thromboembolic events remains increasingly important. Several percutaneous LAA occlusion devices have been shown to be noninferior to anticoagulation in appropriately selected patients. As their safety profiles continue to improve, the use of these devices will continue to increase as well. It is important for anesthesiologists to be familiar and comfortable with the appropriate perioperative management of patients undergoing either endocardial or epicardial percutaneous LAA closure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.