
Abstract
Coagulation management, and transfusion practice in liver transplantation (LT) have been evolving in the recent years due to better understanding of coagulation abnormalities in end-stage liver disease, and clinical management of LT patients. Avoidance of allogeneic blood components is feasible in some patients, but multi-modal coagulation therapies may be necessary in others who develop complex coagulopathy due to hemorrhage, hemodilution, hypothermia, and acid-base disturbances. Transfusions of plasma and cryoprecipitate remain to be the mainstay therapy for procoagulant factor replacement during LT. Clinical efficacy and safety of these products are limited by logistic issues (eg, thawing), and mostly noninfectious complications. Considering potential alternatives to conventional transfusion is thus important to improve hemostatic resuscitation in complex LT cases. The present review is mainly focused on procoagulant properties of plasma and platelet transfusion, and currently available plasma-derived and recombinant factor concentrates, and antifibrinolytic agents in LT patients. The role of viscoelastic coagulation tests to guide specific component therapies will be also discussed.
Keywords
Introduction
The liver is the major organ of synthesis of most coagulation factors and inhibitors. Patients with end-stage liver disease (ESLD), and those undergoing liver transplantation (LT) typically present with coagulation abnormalities on prothrombin time (PT) and international normalized ratio (INR).1,2 In the early days of LT, massive hemorrhage was not uncommon, and large amounts of allogeneic blood components were transfused to provide hemostatic resuscitation. Thromboelastography (TEG, Haemonetics, Niles, IL) as a point-of-care (POC) whole blood coagulation test proved to be useful in continuous monitoring of coagulation changes, and detection of systemic fibrinolysis.3,4 Intraoperative requirements of packed red blood cells (PRBC) and plasma used to be both over 10 units (U) in typical adult LT cases even when TEG was in use. Advances in surgical techniques, and implementation of transfusion protocols significantly reduced allogeneic blood transfusion in some LT centers,5,6 but transfusion rates remain to be high in some centers receiving high-risk donor organs, and severely ill recipients.7-9
Concomitantly reduced procoagulant and anticoagulant proteins result in the state of so-called “rebalanced hemostasis” in patients with ESLD.10-12 However, this state is so fragile, and plasma transfusion is often required after major blood loss and hemodilution during LT. The risk of pathogen transmission is low for allogeneic plasma, but it is still associated with noninfectious complications including transfusion-related circulatory overload (TACO), 13 and transfusion-related acute lung injury (TRALI). 14 Considering alternatives to conventional plasma transfusion is thus important to potentially improve hemostatic resuscitation in complex LT cases with moderate to severe coagulopathy. The aims of this article are (a) to discuss the limitations of conventional plasma and platelet transfusion, (b) to review hemostatic properties of currently available factor concentrates, and (c) to discuss the role of antifibrinolytic therapy in LT patients.
Limitations of Plasma Transfusion
Current transfusion practice patterns vary widely between institutions (Table 1). Indeed, a Canadian study reported that practice patterns were significantly different among 8 major LT centers for RBC, plasma, and platelets. 22 Even after adjusting for the estimated blood loss (EBL), there was still wide variability in the uses of plasma and platelets. It is often difficult to identify a uniform transfusion practice in an institution where different transfusion strategies were utilized among individual anesthesiologists without coagulation testing. 23 Furthermore, the literature shows that transfusion patterns may vary according to the method of intraoperative coagulation tests due to different turnaround times, and varied sensitivities to factor deficiency and fibrinolysis.15,19,24 A long turnaround time (30-45 minutes) hinders timely use of plasma according to PT/activated partial thromboplastin time (aPTT) in a centralized laboratory. 25 Whole blood POC tests are faster, but contact-activated (kaolin or ellagic acid) tests are less sensitive to dilutional coagulopathy and fibrinolysis than a tissue factor–activated test.19,24
Blood Product and Factor Concentrate Used in Liver Transplantation. a
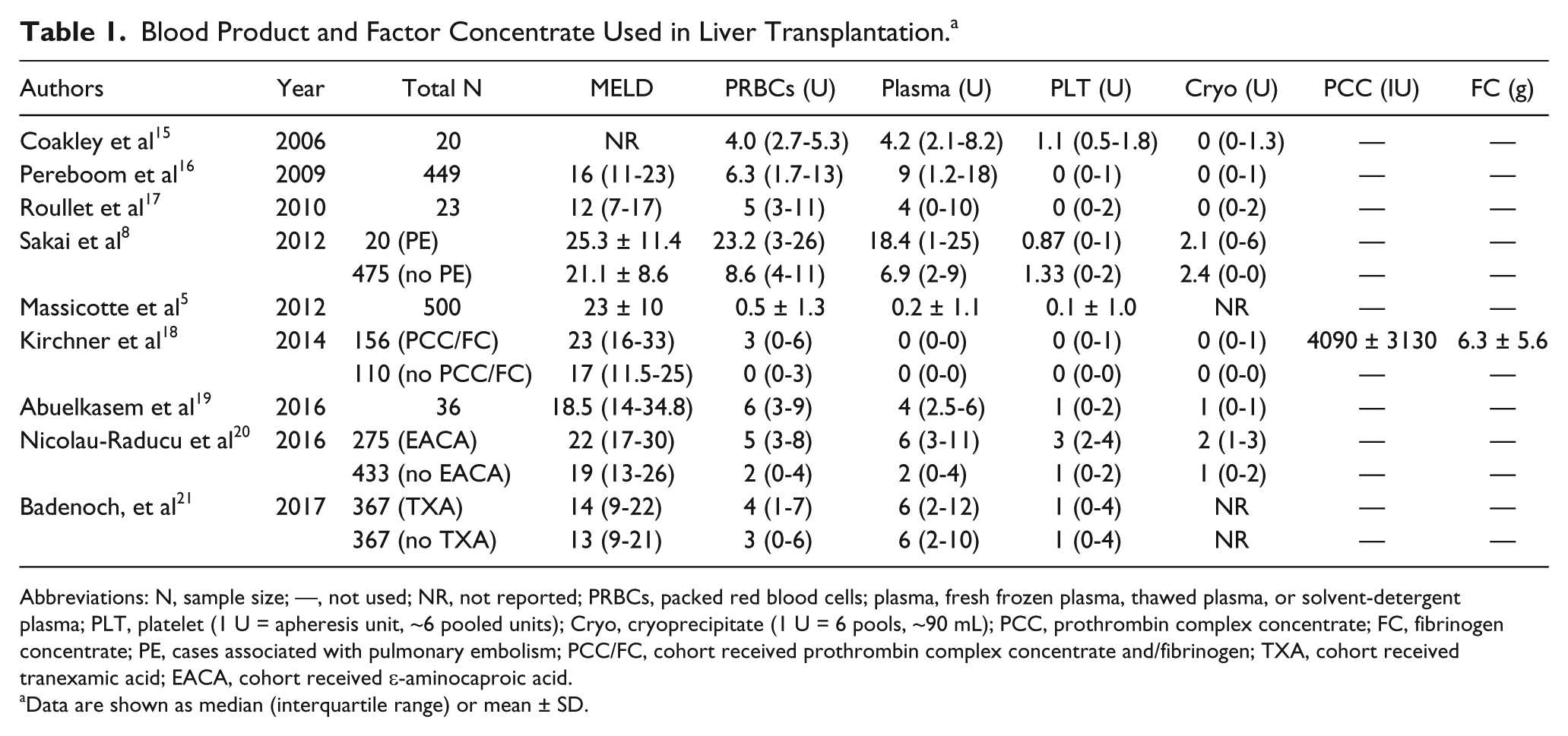
Abbreviations: N, sample size; —, not used; NR, not reported; PRBCs, packed red blood cells; plasma, fresh frozen plasma, thawed plasma, or solvent-detergent plasma; PLT, platelet (1 U = apheresis unit, ~6 pooled units); Cryo, cryoprecipitate (1 U = 6 pools, ~90 mL); PCC, prothrombin complex concentrate; FC, fibrinogen concentrate; PE, cases associated with pulmonary embolism; PCC/FC, cohort received prothrombin complex concentrate and/fibrinogen; TXA, cohort received tranexamic acid; EACA, cohort received ε-aminocaproic acid.
Data are shown as median (interquartile range) or mean ± SD.
In general, prethawed plasma units are only available at large medical centers, and the additional time required for thawing further delays the intervention. More importantly, each plasma unit is expected to increase procoagulant factors by 2% to 3%, 26 and thus large amounts of plasma are required to achieve clinically significant increments (15%-30%). This increases the risk of TRALI 14 as well as TACO, 13 and it may even paradoxically increase bleeding by elevating capillary and venous pressures.5,23 Hypocalcemia due to citrate overload, and hypothermia after large volume transfusion may hinder improvement in thrombin generation.27,28 Lactic acidosis may be worsened by impaired elimination during the anhepatic phase of LT 29 and severe acidosis can significantly disturb fibrin polymerization and thrombin generation. 30 Efficacy of plasma transfusion is thus limited in acidemia. 31
Some of these limitations of plasma can be potentially overcome by the use of a hemostatic component and factor concentrate containing specific coagulation factor(s) in conjunction with POC tests.
Limitations of Platelet Transfusion
Moderate thrombocytopenia (50-75 × 103/µL) is relatively common in patients with ESLD and has been reported in 64% to 84% of patients with cirrhosis.32-34 However, severe thrombocytopenia (<50 × 103/µL) is found in only 1% of patients, 35 and there is limited evidence suggesting the association between ESLD-related thrombocytopenia and periprocedural bleeding.33,36 The lack of bleeding tendency is partly attributed to elevated von Willebrand factor (vWF) levels in LT patients. Acute endothelial damage, reduced vWF clearance, and/or enhanced vWF synthesis contribute to elevated plasma levels of vWF.37,38 Conversely, ADAMTS-13 (A disintegrin-like and metalloproteinase with thrombospondin type-1 motifs 13), which cleaves multimers of vWF under high shear, may be deficient due to reduced hepatic synthesis, resulting in normal or enhanced thrombus formation at the site of vascular injury. 38
Thrombocytopenia in ESLD can be attributed to decreased platelet production due to bone marrow suppression or low hepatic production of thrombopoietin, which regulates the genesis and differentiation of megakaryocytes, a precursor of mature platelets.32,33 In addition, decreased platelet survival may be associated with splenic sequestration or portal hypertension, further contributing to thrombocytopenia in ESLD.32,33,39
Prophylactic platelet transfusion is a tempting therapeutic option in thrombocytopenia patients undergoing LT. 2 However, prophylactic platelet transfusion does not effectively improve platelet count40,41 or viscoelastic clot firmness. 42 Furthermore, it was shown in one retrospective study that intraoperative exposure to platelet transfusion during LT (n = 182) was associated with a higher early mortality due to TRALI or acute respiratory distress syndrome (ARDS) (odds ratio 12.2; 95% confidence interval, 1.5-98.6; P = .004) compared with nonexposure (n = 267). 16 Adverse effects of allogeneic platelet transfusion may be attributed to cytokines and microaggregates in platelet concentrates, possible pathogen contaminations, and ABO incompatibility.43,44 Another recent retrospective study involving 399 patients undergoing LT demonstrated that intraoperative platelet transfusion (n = 139) was associated with lesser 1-year graft survival (81.2% vs 89.9%; P = .02) as well as 90-day (91.9% vs 97.1%; P = .04) or 1-year overall survival (87.7% vs 94.2%; P = .04). 34 There was also an increased risk of mortality from sepsis at 90 days (2.88% vs 0.39%, P = .033) and 1 year (3.60% vs 0.39%, P = .012). These findings were independent of the degree of preoperative thrombocytopenia. Taken together, platelet transfusion should be reserved for actively bleeding patients during LT. Further improvements in platelet function testing are required in the assessment of abnormal levels of vWF and ADAMTS-13 in ESLD.
Fibrinogen-Rich Components
Fibrinogen is a large glycoprotein synthesized in the liver, and plays crucial roles in hemostasis, wound healing, and immunity.45,46 In hemostasis, fibrinogen supports platelet aggregation, and thrombin-cleaved fibrin and activated factor (F) FXIII (FXIIIa) polymerizes to form a clot. 47 Fibrinogen levels in end-stage liver disease (ESLD) are typically normal or elevated, 48 but they may be functionally defective due to dysfibrinogenemia.
The increased negative charge of fibrinogen molecules due to maldistribution or excess of sialic acid delay fibrin polymerization. 49 This can be detected on a fibrin-specific viscoelastic test as reduced clot firmness (Figure 1). There is a paradoxical observation that fibrin clots in dysfibrinogenemia are more tightly packed than normal fibrin despite the reduced fibrin polymerization. 49 Such alterations may partly explain the lack of established viscoelastic test threshold(s) for prophylactic fibrinogen intervention or bleeding prediction in LT. 50
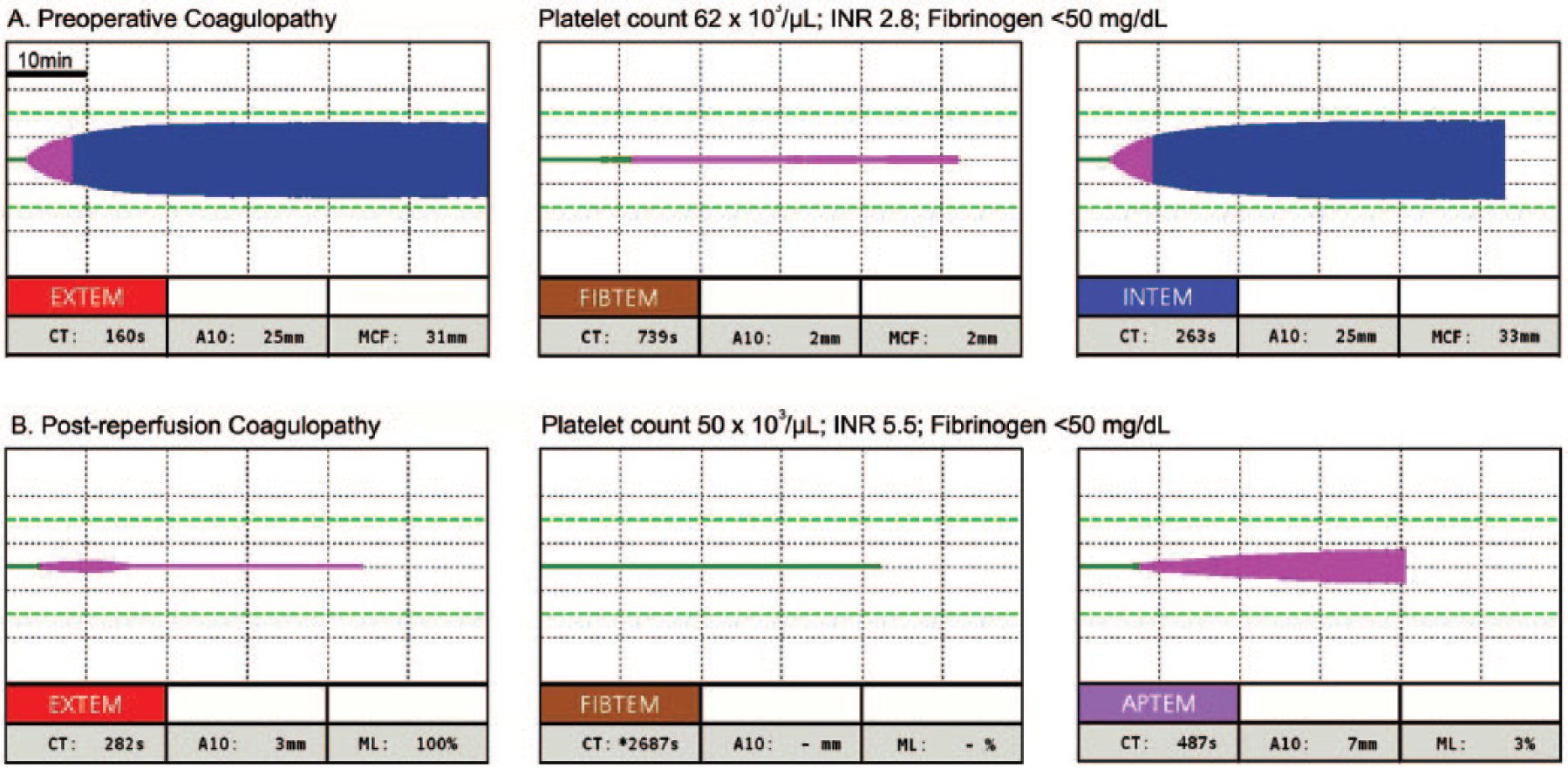
Diagnosis of coagulopathy on thromboelastometry. Thromboelastometry traces from 2 liver transplant patients are shown along with standard laboratory coagulation test data. (Panel A) Preoperative traces. Tissue factor-activated EXTEM clotting time (CT) is extensively prolonged (EXTEM, normal 35-80 seconds) as high INR, while INTEM-CT is only mildly prolonged (INTEM, normal 137-246 seconds). A10 (10-minure clot firmness) is reduced on EXTEM and INTEM, consistent with thrombocytopenia. Severe hypofibrinogenemia is shown on fibrin-specific clot firmness (FIBTEM, normal 7-24 mm). (Panel B) Post graft reperfusion traces. Most findings are similar to the panel A except for severe fibrinolysis (maximum lysis [ML] %, normal <15%). Note the clot dissolution in 10 min on EXTEM, and a flat-line on FIBTEM (ie, minimal fibrinogen). Fibrinolysis is resolved in vitro on APTEM with a plasmin inhibitor, aprotinin.
Intraoperative fibrinogen levels can be reduced rapidly due to hemorrhage followed by resuscitation with fibrinogen-poor fluids and components (eg, PRBC).3,4,51 Furthermore, systemic fibrinolysis can break down fibrin clots, and worsen bleeding, particularly after the graft reperfusion. 48 Cryoprecipitate has been the mainstay therapy for fibrinogen replacement since the early years of LT.3,4,48 Cryoprecipitate is derived from partially thawed fresh frozen plasma, yielding an average of 388 mg of fibrinogen per unit (~15 mL).47,52 It is presumed that each cryoprecipitate unit increases plasma fibrinogen level by about 10 mg/dL in a 60-kg patient, but there is significant variability among fibrinogen contents, ranging from 120 to 796 mg per unit. 47 In addition to fibrinogen, cryoprecipitate also contains 40% to 70% vWF (in comparison with normal plasma). 47 Repeated administration of vWF or FVIII-containing products has been associated with thrombosis in some patients with von Willebrand’s disease (vWD). 53 There might be a similar thrombotic risk after repeated doses of cryoprecipitate containing both vWF and FVIII, 54 but there is a paucity of data supporting the association of cryoprecipitate and vascular thrombosis during or after LT.55,56
Pathogen reduction processes are not routinely applied to cryoprecipitate, but it is feasible to produce cryoprecipitate units with sufficient fibrinogen (262 mg per unit) from pathogen-reduced plasma. 57 Prior to the transfusion, cryoprecipitate needs to be thawed, and each unit should be compatible with the recipient’s ABO blood type.58,59 These issues potentially hinder rapid availability and use of cryoprecipitate in major hemorrhage and massive transfusion. Clinical availability of cryoprecipitate is limited to the North America and the United Kingdom.58,60
Use of fibrinogen concentrate (FC) overcomes some of the limitations of cryoprecipitate. There are 2 commercially available products in the North America: Fibryga (Octapharma, Vienna, Austria) and RiaSTAP (CSL Behring, Marburg, Germany).61,62 Both FC products are indicated for the treatment of actively bleeding patients with congenital fibrinogen deficiency. Each FC vial contains approximately 1 g of purified, lypophilized fibrinogen, which can be stored at room temperature. 63 FC is reconstituted with 50 mL of distilled water for a rapid administration without thawing or blood type matching. 59 FC has been shown to increase viscoelasticity (ie, fibrin polymerization) on TEG with much less variability than cryoprecipitate after equipotent doses of fibrinogen, resulting in a more predictable increase in plasma fibrinogen levels. 59 Although FC products are manufactured from a large pool of human plasma, multiple safeguards are implemented in the manufacturing steps that mitigate pathogen transmissions, 64 and minimize allergic reactions and other transfusion-related reactions. 47
There is a paucity of data on the threshold fibrinogen level for replacement during LT. For the actively bleeding patient, administration of cryoprecipitate or FC is considered when plasma fibrinogen level falls below 100 to 130 mg/dL, or 10-minute amplitude of FIBTEM (FIBTEM-A10) is below 5 to 8 mm (Figure 1).17,18,65,66 Kirchner et al 18 have implemented a rotational thromboelastrometry (ROTEM; TEM International, Munich, Germany) based hemostasis protocol including maximal clot firmness of FIBTEM (FIBTEM-MCF) below 8 mm (A10 < 6 mm) for FC administration (Figure 1A). 65 FC was used at a mean dose of 6.3 g in 57.5% (n = 153) of 266 cases. In their study, prothrombin complex concentrate (PCC) was also used in 34.9% (n = 93) of patients according to the prolonged clotting time of EXTEM (EXTEM-CT) above 80 seconds (Figure 1A), while plasma transfusion was reserved for suspected FV and/or FXI deficiency. 65 They reported that 85.3% (n = 227) and 71.4% (n = 190) of LT cases were performed without plasma and platelet transfusion, respectively. Their low rates of allogeneic blood product usage support the usefulness of factor concentrates under pre-defined criteria on viscoelastic coagulation testing (Table 1).
Timing of administration should be carefully considered for the efficacy of FC. In a recent placebo-controlled randomized clinical trial of FC in LT, Sabate et al 67 hypothesized that preoperative supplementation of FC would reduce transfusion requirements during LT in patients with plasma fibrinogen below 290 mg/dL. The dose required to achieve a target fibrinogen dose of 290 mg/dL was calculated, and FC was given to the FC-treatment group, while saline was given to the control group. Intraoperatively, a rescue dose of FC was permitted in both groups if fibrinogen was below 100 mg/dL. FC-treated group (n = 48) received 3.54 g (median) preemptively, and 4.14 g (total) of fibrinogen in 24 hours, which was significantly higher than 2.58 g in the placebo group (n = 44). Notably, the majority of FC in the placebo group was given in the postoperative period, and no between-group difference was found for PRBC, plasma or platelet usage. 67 In their study, fibrinogen was replaced to the median of 220 mg/dL (FIBTEM A10, 11 mm) before surgery in the absence of bleeding. Intraoperative blood loss and hemodilution were not considered for the dosing, and this omission might have resulted in clinically non-significant difference in fibrinogen levels (ie, 20 mg/dL higher in the FC group) after the graft reperfusion. Supplementing fibrinogen after the graft reperfusion may prove to have better efficacy in restoring fibrin polymerization instead of preoperative supplementation when hemostasis is already present. 68
The risk of thromboembolic complication needs to be considered for any hemostatic intervention. In the LT population, hepatic artery thrombosis (HAT) is the most feared event, occurring at a rate of 3% to 9%. 69 HAT is associated with a re-transplantation rate of 53%, and a mortality rate between 27% and 58%.56,70 One series of 1192 consecutive LTs suggested that the greatest surgical risk factor for HAT was the type of arterial anastomosis, specifically a supraceliac graft interposition to the recipient’s aorta, 69 while a review of 634 consecutive patients found that accessory hepatic artery reconstruction and cytomegalovirus (CMV) infection to be significant predictors for HAT.55,56 Conversely, the patient’s age, indication of LT, surgical time, cold ischemic time, and volume of blood transfusion were not associated with HAT. 69 Sabate et al 67 did not find any increase in HAT after preemptive FC administration (2.2% vs. 6.8% in the study and placebo groups, respectively). Kirchner et al 18 reported that the incidence of HAT was 4.5% in LT patients receiving FC and/or PCC when compared with 3.6% in those who did not receive these concentrates (P = .73). 18 However, both of these studies were underpowered for the safety evaluation, and an adequately powered multicenter study on the use of FC in LT is warranted.
Prothrombin Complex Concentrate
PCC is a purified vitamin K–dependent factor concentrate derived from plasma. 71 It is produced from the supernatant of pooled cryoprecipitate, which undergoes ion-exchange chromatography to create a purified preparation containing either 3-factor (FII, FIX, and FX) or 4-factor PCC (FII, FVII, FIX, and FX).71,72 All PCC formulations undergo at least one form of viral reduction, although most undergo at least two steps (Table 2). 72 The dose of PCC is standardized to the FIX content, which is approximately 500 international unit (IU) per vial. Each vial is reconstituted with 20 mL of sterile water, giving a factor level of 25 IU/ml. Higher concentrations of factors in PCC compared with plasma (0.8-1.2 IU/mL) allow rapid recovery of vitamin K–dependent factors in warfarin-treated patients (Food and Drug Administration–approved indication) without circulatory overload.76,77 Reduced production of FII, FV, FVII, FIX, and FX are the hallmark of ESLD,78,79 and thus using 4-factor PCC may seem logical in restoring deficient factors except for FV.
Composition of Selected Factor Concentrates.
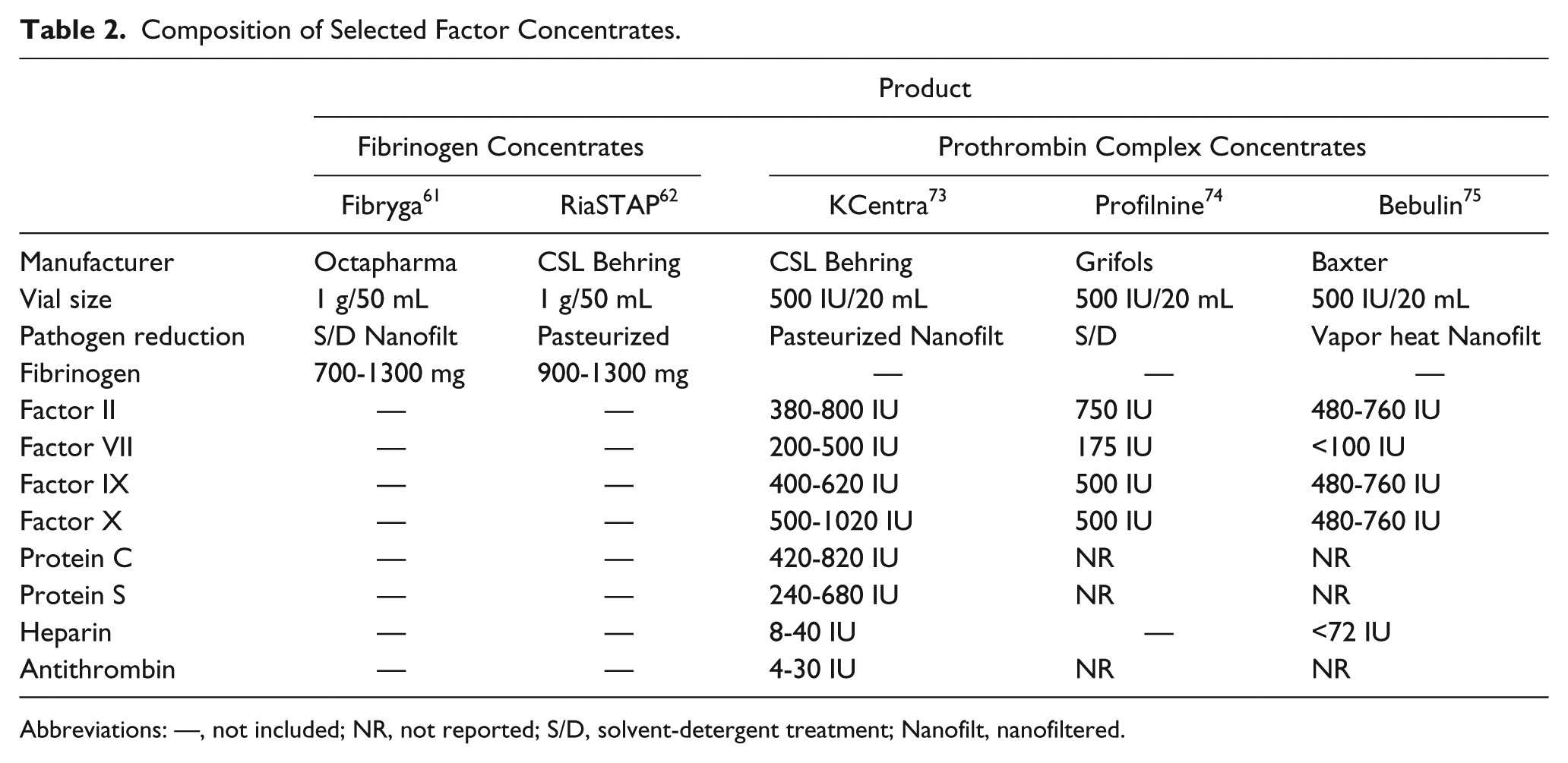
Abbreviations: —, not included; NR, not reported; S/D, solvent-detergent treatment; Nanofilt, nanofiltered.
Lorenz et al 79 reported a case series of PCC infusion in patients with severe liver damage suffering from active bleeding or undergoing invasive procedures (n = 22). The median dose of PCC was 25.7 IU/kg (1500 [1000-4000] IU), and an additional 2000 IU was administered in 5 patients. They observed similar recoveries (1.3-1.4 IU/kg) among FII, FIX, and FX, which were restored to the normal range. Clinical efficacy after the first PCC dose was judged to be “very good” (normal hemostasis) in 76% of patients, and in 5 others, efficacy was initially “satisfactory” (mildly delayed, but sufficient hemostasis), but “very good” after the second dose. No PCC-related adverse events including thrombosis occurred.
As mentioned above, Kirchner et al 18 applied a 25 IU/kg dose of PCC for EXTEM-CT above 80 seconds for active hemorrhage during 266 LT cases after restoring fibrinogen levels. PCC was used in 34.9% (n = 93) compared with the plasma transfusion in 14.7% (n = 39).
It has been demonstrated that thrombin generation (TG) in ESLD patients often remain normal despite prolonged PT/INR.10,11 The so-called “rebalanced hemostasis” in ESLD is partly related to decreased anticoagulant proteins, including antithrombin (AT), protein C, and protein S.10-12 However, “rebalanced” TG in ESLD tends to be easily perturbed by small amounts of exogenous anticoagulants as well as hemodilution.11,51,80
Indeed, Abuelkasem et al 51 showed that peak TG (median) was 186 nM before LT, which was below the normal range (234-296 nM). After the graft reperfusion, peak TG was further decreased to 121 nM due to hemorrhage and hemodilution as shown in low FX level (median, 28%). In their study, ex vivo additions of PCC (0.2 and 0.4 IU/mL) to LT plasma samples were shown to be more effective in restoring TG compared with the minimal effect of normal plasma (10% volume replacement, equivalent to 2-3 U in vivo). The TG response to PCC appears to be dose-dependent, and 0.4 IU/mL of PCC (equivalent to 20 IU/kg dose in vivo) put TG to supranormal levels in some samples. Preexisting AT deficiency (median, 25%-29%) in LT subjects delays the shutdown of procoagulant proteases such as FXa and thrombin. Therefore, it may be important to avoid extreme AT deficiency (10%-30%) prior to PCC administration because commercial PCC products contain minimal AT (Table 2).37,65 Although the risk of acute thrombosis is reportedly low after PCC administration,18,37 the association of low AT activity and portal vein thrombosis has been previously suggested in ESLD patients. 81
The safety data regarding PCC are limited to its main indication of acute warfarin reversal. The incidence of thrombosis with PCC is estimated to be 1.4% (95% confidence interval, 0.8%-2.1%) based on the 1032 warfarin-treated patients. 82 As mentioned above, Kirchner et al 18 did not observe statistically significant increases in composite thromboembolic events including HAT, portal vein thrombosis, and myocardial ischemia between FC/PCC-treated and nontreated cohorts (7.1% vs 4.5% in nontreated; P = .31).
The volume of infusion is much less with PCC compared with plasma transfusion, and the risk of volume overload is actually higher in the latter related in acute warfarin reversal. 83 Elevated central venous pressure may be considered to be a risk predictor of bleeding in LT.5,23
To date, there is no published randomized control trial of PCC on the efficacy and safety in LT. The PROTON trial is one such trial in Europe, but the results are not yet available. 84
Recombinant Factor VIIa
Recombinant activated FVII (rFVIIa; NovoSeven; Novo Nordisk, Bagsbaerd, Denmark) is a serine protease that mainly promotes the conversion and activation of FX to FXa, and FIX to FIXa. 85 The main indications of rFVIIa are limited to congenital bleeding disorders including hemophilia with inhibitors, and factor VII deficiency, but “off-label” uses in acquired bleeding conditions were very common in the early 2000s.86 -88 In the case of hemophilia, high doses of rFVIIa (>90 µg/kg) directly activates sufficient FX to promote TG, bypassing the need for FVIII or FIX. Clinical use of rFVIIa effectively shortens PT/INR in warfarin-treated patients because this test is highly sensitive to FVII levels.88,89 However, rFVIIa is ineffective as a warfarin reversal agent because TG is not restored due to lack of prothrombin and FX. 89
This is an important consideration when bleeding due to multifactorial vitamin K deficiencies is suspected in ESLD and LT patients. In a population of patients undergoing partial hepatectomy, randomization to a single preoperative dose of rFVIIa (20 or 80 µg/kg) failed to demonstrate any difference in the number of patients transfused or the volume of blood products. 90 Similarly, in patients undergoing LT, the use of a single preoperative dose (20, 40, or 80 µg/kg) of rFVIIa had no effect on the volume of blood products transfused. 91 A follow-up study using more frequent dosing (60 and 120 µg/kg repeated every 2 hours) did show a small decrease in the number of patients requiring transfusion, but there was no reduction in the number of PRBC transfusion. 92 Taken together, there is no data to support routine use of rFVIIa in LT, and PT/INR is not a useful measure of its indication or efficacy in ESLD patients.
Antifibrinolytics
The liver is involved in the synthesis and breakdown of many proteins involved in fibrinolysis pathway. There appears to be a dynamic rebalancing of these proteins in ESLD. 93 Increased tissue plasminogen activator (tPA) levels are countered by elevated plasminogen activator inhibitor-1 (PAI-1), even in severe ESLD (Child’s class C). Plasminogen and α2-antiplasmin (plasmin inhibitor) are both decreased, but the latter effect is more dominating, and fibrin becomes more prone to fibrinolysis in severe ESLD.
Unlike the trauma-associated profibrinolytic state which is associated with a high mortality, 94 systemic fibrinolysis during LT is often transient, and it is not a major predictor of mortality. Systemic fibrinolysis is most commonly observed in the late anhepatic stage and postreperfusion period when tPA is released from the vascular bed, but is not cleared by the liver (Figure 1B). 48 In this regard, use of antifibrinolytics during LT seems logical, and there is clinical evidence to support this practice.95,96
Aprotonin, a direct plasmin inhibitor, was the first antifibrinolytic agent used during LT, 97 and many subsequent studies have established the association between intraoperative fibrinolysis, bleeding and increased transfusion during LT. 98 Clinical use of aprotinin has essentially ceased since 2007 when it was withdrawn from the market due to the high rate of mortality in high-risk cardiac surgery. 99 It is difficult to assess actual clinical impact(s) of antifibrinolytic therapy in LT from the early publications because aprotinin is no longer used, and surgical and blood conservation techniques have been significantly advanced in the recent years. 100 Currently, tranexamic acid (TXA) is used worldwide, while ε-aminocaproic acid (EACA) is limited to North America. The meta-analysis by Molenaar et al 101 indicated that TXA infusion (10 mg/kg/h) consistently reduced PRBC and plasma transfusions compared with the placebo. Prophylactic TXA administration (bolus, 30 mg/kg plus infusion at 16 mg/kg/h) has been also documented by Massicott et al 5 in 200 LT patients to whom minimal blood products were administered (Table 1).
Antifibrinolytic therapy is sparingly used at other institutions for fear of intravascular or graft thrombosis. Nicolau-Raducu, et al 20 compared EACA-treated (n = 275), and nontreated patients (n = 433) during LT at a single institution. Clinical decision to use EACA was based on TEG evidence of fibrinolysis, and the average dose was 6.6 ± 2.7 g followed by 1 g/h infusion. It is notable that EACA-treated patients had higher Model for End-Stage Liver Disease (MELD) and INR values compared with the nontreated cohort (MELD, 22 vs 19, and INR, 1.8 vs 1.6; P < .0001 for both). Their study indicated that EACA-treated patients received larger amounts of PRBC, plasma, platelet, and cryoprecipitate. Furthermore, the subgroup analysis showed much higher transfusion requirements in patients who required repeated bolus injections, or prolonged infusion (total EACA dose, 5-10 or >10 g). They failed to find any difference in thromboembolic events (hepatic thrombosis, myocardial infarction, stroke, and early HAT) between EACA and non-EACA groups. Their findings concur with the recent propensity-matched cohort study by Badenoch et al 21 in which decreased PRBC and plasma requirements were found in TXA-treated (n = 367) versus matched nontreated cohort without increased HAT, portal vein, and other venous thromboses (Table 1).
Intracardiac thrombosis (ICT) and pulmonary thromboembolism (PE) are potentially fatal complications during LT, occurring at an estimated rate of 0.36% to 4.0%.8,102,103 ICT/PE seems to occur infrequently, but the reported intraoperative and overall mortality rates are high (30%-55% and 45%-68%, respectively).8,103,104 The causal association between antifibrinolytic therapy and ICT/PE has not been established,8,103,104 but declotting attempts by intravenously administered tPA can be hindered by TXA or EACA.102,105 The occurrence of ICT/PE is typically within 30 minutes of graft reperfusion,8,105 and thus early diagnosis with transesophageal echocardiogram, and withholding antifibrinolytics during this period should be considered in high-risk LT cases.
Conclusion
Clinical coagulation studies in the recent years lead to better understanding of coagulopathy in patients with ESLD. Prophylactic plasma transfusion is rarely indicated in minor procedures, but therapeutic plasma transfusion is still required in a portion of LT patients. Multifactorial coagulation defects may be diagnosed in a timely fashion using POC viscoelastic coagulation tests. Cumulating clinical studies and experiences suggest that it is feasible to restore hemostasis using POC-guided FC and PCC administrations in the majority of LT patients. Antifibrinolytic therapy is an important adjunct to stabilize fibrin clots. All these interventions have potentials for thromboembolic complications, and thus they should be used according to the pre-agreed institutional protocol, and judicious coagulation monitoring. Future studies are warranted to elucidate complex balances of coagulation during LT, and to optimize goal-directed transfusion and factor concentrate therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KAT has served on clinical trial data monitoring committees for Octapharma.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.