
Abstract
We describe the novel combined use of a fiberoptic bronchoscope and a Fuji Uniblocker placed outside the endotracheal tube (ETT) for removal of a retained BioGlue polymerized tissue fragment (2.8 × 0.8 cm) from the right main bronchus (RMB). The patient was a trauma victim who presented with a diffuse axonal injury, cervical spine and maxillofacial injuries, and a flail chest, and the procedure we describe took place following the surgical repair of a disrupted left main bronchus. Endoscopic retrieval using different sizes of grasping forceps and a Dormia basket failed to remove the foreign body (FB). Under combined GlideScope videolaryngoscopic and bronchoscopic guidance, a 9.0 F Uniblocker was introduced outside the ETT, placed into the RMB beyond the FB, initially inflated, and then gradually increased in volume during withdrawal from the RMB into the trachea so as to trap the FB between the tip of the ETT and the blocker balloon. The ETT, bronchoscope, blocker catheter, and the FB were then removed from the glottis as a single unit. The FB was then removed using Magill forceps with the aid of a GlideScope. We conclude that the combined use of a GlideScope, bronchoscope, and an Uniblocker placed outside the ETT can be an effective method for removal of a retained FB.
Keywords
Introduction
Retained tracheobronchial foreign bodies (FBs) in adults is an occasional problem that can result in cough, wheeze, edema, granulation tissue formation, atelectasis, 1 bronchiectasis, 2 and pneumonia. 1 Rigid bronchoscopy remains the standard method to remove large and central aspirated FBs because it offers superior airway control, suction, and extraction capabilities. 3 However, the presence of an unstable cervical spine or oral/maxillofacial trauma may preclude its use. 3 In such cases, flexible bronchoscopy using forceps, snares, or baskets can be a potential alternative.1,4 Fogarty catheters and balloon-tipped catheters intended for angioplasty have been described for the removal of bronchial FBs.5,6 The balloon-tipped catheter is used to trap the FB near the bronchoscope tip, with subsequent simultaneous withdrawal of both the catheter and bronchoscope. However, the use of these catheters can be complicated by tracheobronchial disruption or catheter tip embolization 5 as they have poorly compliant balloons and thin catheter shafts, respectively. Similarly, the Arndt wired-tip endobronchial blocker was successfully used for retrieval of an aspirated FB in a trauma patient. 7
The “torque control” Fuji Uniblocker (Fuji Systems Corporation, Tokyo, Japan), a flexible blocker shaft with soft open-lumen tip, can be easily manipulated and positioned to separate patient’s lungs during thoracic procedures. The enclosed 9.0 F Uniblocker compliant balloon can accommodate a maximum inflation volume of 8.0 mL, making it a potential alternative to remove aspirated FBs. Of note, the 9.0 F (3.0 mm) outer diameter of the Uniblocker precludes its use through the endotracheal tube (ETT) alongside the flexible bronchoscope (>3.7 mm outer diameter) or through its working channel.
In this report, we show how the combined use of the bronchoscope, GlideScope videolaryngoscope (VL; Verathon Inc, Bothell, WA), and Fuji Uniblocker can be used to remove a retained bronchial FB, as illustrated in the management of a trauma patient with cervical spine and maxillofacial injury after repair of ruptured left main stem bronchus (LMSB).
Case Report
A 29-year-old, 167 cm, 70 kg soldier was referred from another hospital to our tertiary center after falling from a great height. He suffered from diffuse axonal injury, a fracture of the second cervical spine vertebra, as well as fractures to both maxillary sinuses, and to the base of the skull. He also suffered from a left flail chest, bilateral hemopneumothoracies, and a disrupted LMSB. His previous medical history was unremarkable.
Physical examination revealed a Glasgow Coma Scale score of 5/15 and severe bilateral surgical emphysema extending from the neck to groin. He was intubated with a 7.0-mm ETT, while SIMV-PC (synchronized intermittent mandatory pressure control ventilation) was initiated with a fraction of inspired oxygen (FiO2) of 0.4. The cervical spine was immobilized with a cervical collar, and the right (radial) artery and subclavian veins were catheterized. Pleural drainage was accomplished using bilateral chest tubes. Sedation was provided using fentanyl 120 µg/h.
The respiratory rate was 20/min, resting heart rate (HR) 82/min, blood pressure 144/74 mm Hg, and arterial oxygen saturation (SpO2) 92% on a FiO2 of 0.4. Examination of the other systems revealed no abnormalities. His preoperative airway examination revealed an interincisor distance of approximately 3.0 cm, an immobilized neck flexion and extension, and bilateral peripharyngeal emphysema.
Chest radiography showed bilateral pneumothoracies, a pneumomediastinum, and collapsed left lower lung lobe. Transthoracic echocardiography and an electrocardiogram showed no abnormalities. Hemoglobin concentration was 9.5 g/dL, albumin level was 2.6 g/dL, and serum glutamic oxaloacetic and glutamic pyruvic transaminase enzymes were 158 U/L and 75 ULl, respectively. Lactic acid was 2.5 mmol/L, and serum creatinine phosphokinase and myoglobin levels were 5647 U/L and 440 U/L, respectively. The patient’s electrolytes, creatinine, and cardiac troponin levels were normal. Arterial blood gas analysis was normal apart from an arterial oxygen tension (PaO2) of 63 mm Hg.
Computed tomography (CT) scan demonstrated an extensive pneumomediastinum and surgical emphysema, a disrupted LMSB, and bilateral pneumothoracies.
Brain CT demonstrated a fracture at the skull base extending to the right carotid canal and to the anterior and medial maxillary sinuses with multiple hypodense foci seen within the left centrum semiovale, representing sequela diffuse axonal injury. A CT perfusion study demonstrated no evidence of mismatch and CT angiography showed no evidence of injury of the right internal carotid artery.
The patient underwent a surgical repair of the disrupted LMSB through a left thoracotomy. During surgery, BioGlue (CryoLife, Kennesaw GA), a 2-component surgical adhesive composed of purified bovine serum albumin and glutaraldehyde, was applied externally to seal an air leak from the anastomotic line. However, bronchoscopic examination through the placed right double lumen endobronchial tube revealed a totally obliterated LMSB lumen, which required revision of the bronchial anastomosis with extraction of the previously dispensed BioGlue. After the surgery, the patient was ventilated in the surgical intensive care unit.
On the second postoperative day, the patient remained intubated with an 8.5-mm ETT, the respiratory rate was 20/min, the HR 80/min, blood pressure 176/86 mm Hg, and SpO2 96% with a FiO2 of 0.7. Arterial blood gas analysis was as follows: pH 7.407, PaCO2 47.8 mm Hg, HCO3 29.4 mmol/L, and PaO2 83.9 mm Hg with a PaO2/FiO2 ratio of 119.9.
A bedside bronchoscopic examination demonstrated a patent LMSB, an intact anastomotic suture line, and a retained piece of a polymerized BioGlue (2.8 × 0.8 cm) in the right main bronchus (RMB; Figure 1).
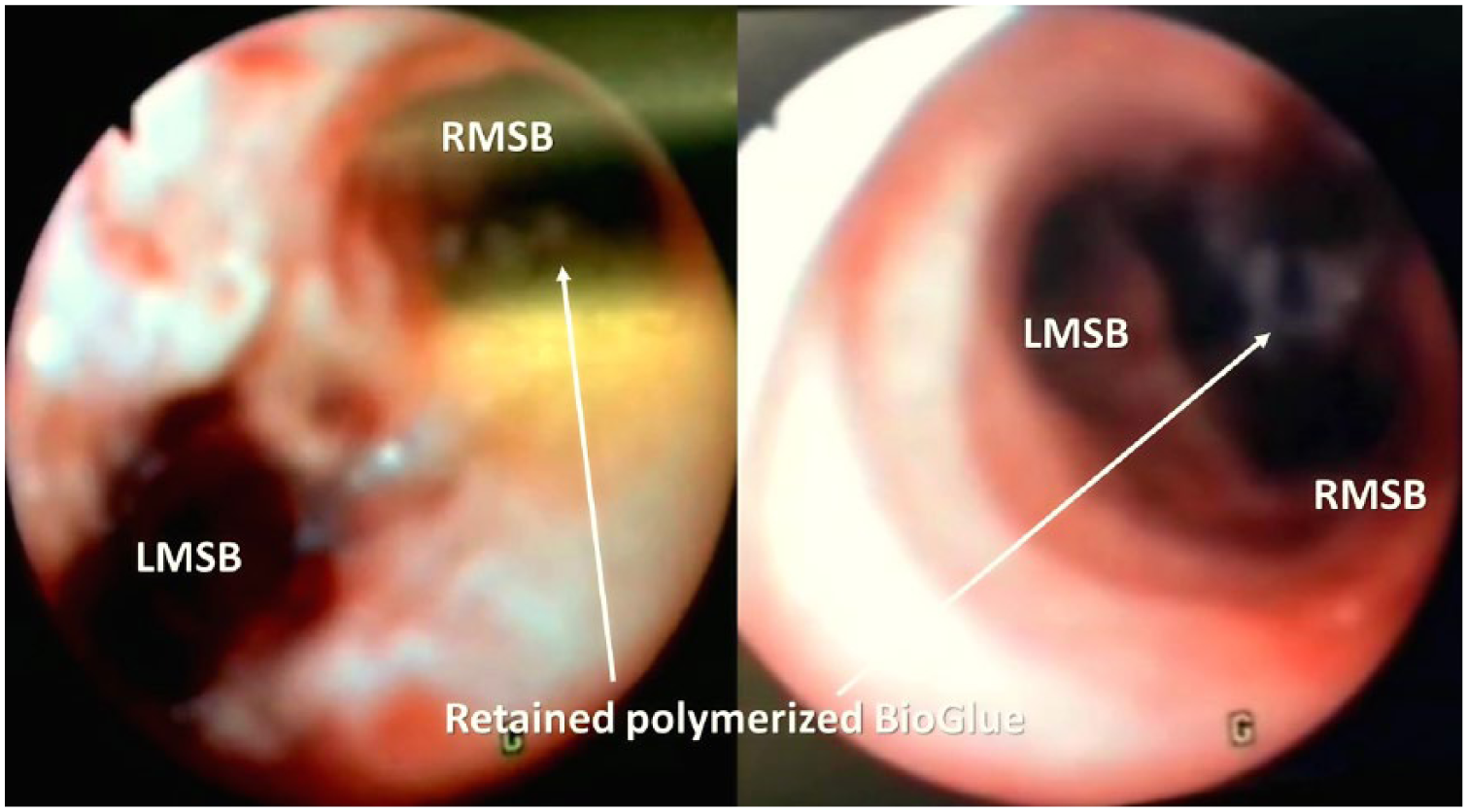
Bronchoscopic images showing the retained polymerized BioGlue foreign body in the right main stem bronchus. LMSB, left main stem bronchus; RMSB, right main stem bronchus.
Multidisciplinary discussions involving a cardiothoracic surgeon, an intensivist, anesthesiologists, and the family were carried out, emphasizing the need for extraction of the retained polymerized BioGlue because the possibility of local hypersensitivity reaction such as swelling or edema, or tissue necrosis, infection, or mineralization. The presence of a cervical spine fracture and cervical immobilization with the associated need to avoid potentially harmful extreme neck extension precluded the use of a rigid bronchoscope. Flexible bronchoscopic extraction of the FB at bedside was offered as the best management option in view of the minimally invasive technique and the critical condition of the patient. Written informed consent was obtained.
Patient monitoring included electrocardiography, pulse oximetry, invasive arterial blood and central venous pressure measurements, and capnographic monitoring. Sedation was provided using fentanyl, and cisatracurium 14 mg was administered for muscle relaxation.
Repeated trials using a 5.0-mm fiberoptic bronchoscope (FOB; Karl Storz Endoskope, Tuttlingen, Germany) and different sizes grasping forceps and Dormia baskets were performed, but they failed to extract the retained FB beyond the carina. Laryngoscopy was performed using a GlideScope VL, where subsiding surgical emphysema was observed.
Subsequently, a multidisciplinary discussion involving the proceduralists (thoracic surgeon and anesthesiologists) was carried out, emphasizing the need for extraction of the retained FB using a balloon-tipped 9.0 F Fuji Uniblocker that was introduced through the glottis outside the ETT, under GlideScope VL guidance (Figure 2a and b), then placed into the right main stem bronchus beyond the retained FB under FOB visual guidance using the FOB placed through the ETT (Figure 3a). The cuff of the Fuji Uniblocker was initially inflated, then withdrawn from the RMB into the trachea with progressive inflation to trap the FB between the tip of the ETT and blocker balloon (Figure 3b). The ETT, bronchoscope, blocker catheter, and the FB were then removed from the glottis as a single unit under combined GlideScope VL and bronchoscopic guidance. The FB was then removed from the posterior surface of pharynx with Magill forceps, while the glottis was visualized via the GlideScope VL. After removal of the FB, tracheal intubation was accomplished with an 8.5-mm ETT using the GlideScope VL with the bronchoscope reintroduced to rule out any potential damage (see the Online Supplementary Video; available in the online version of the article). A 5.0-mm FOB rather than a pediatric FOB was used to enable combined use of the 9.0 F Fuji Uniblocker and forceps to remove the retained bronchial FB in case of failure with the use of the former. This precluded the passage of a 9.0 F Fuji Uniblocker through the 8.0-mm ETT.
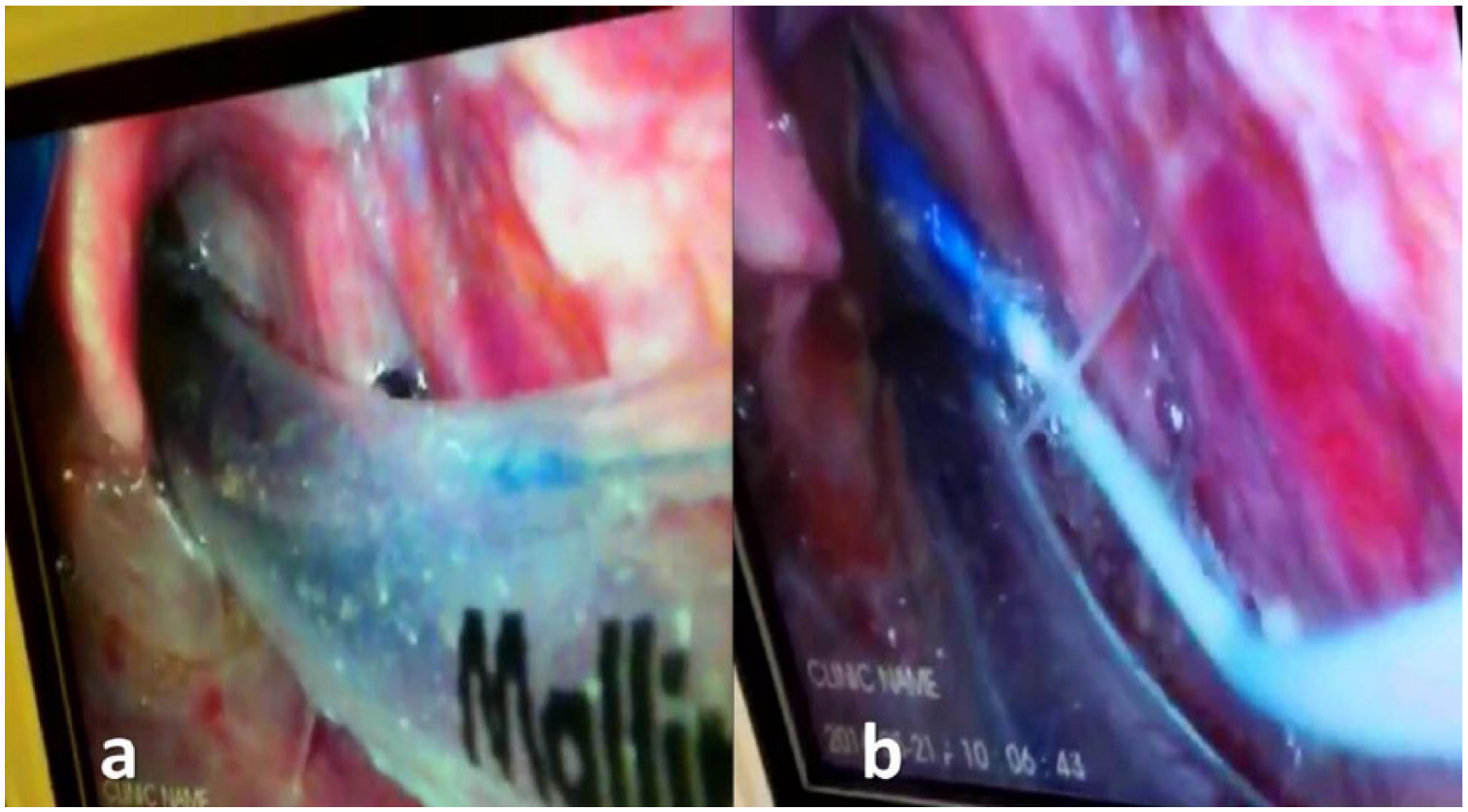
Photograph showing (a) GlideScope videolaryngoscopic visualization of the glottis (b) with introduction of the tip of the 9.0 F Fuji Uniblocker alongside the endotracheal tube through the glottis.
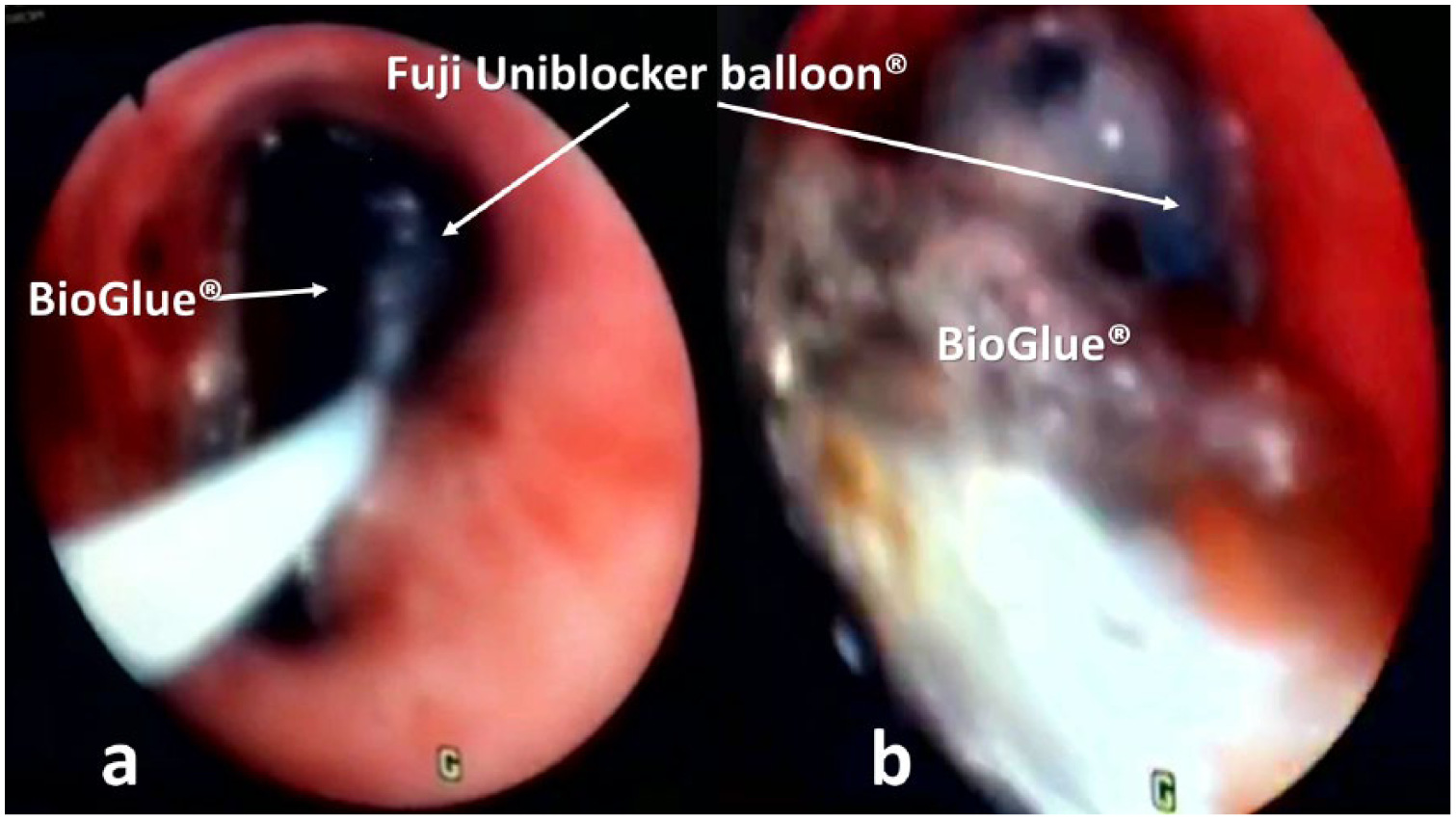
Photograph showing (a) the positioning of the 9.0 F Fuji Uniblocker into the right main stem bronchus beyond the retained foreign body under direct bronchoscopic visualization vision. (b) Withdrawal of the Fuji Uniblocker with progressive inflating its cuff balloon from the right main stem bronchus into the trachea with trapping of the retained polymerized BioGlue foreign body between the tip of the tracheal tube and blocker balloon.
Cervical immobilization and mechanical ventilation were continued throughout the procedure. The vital signs of the patient remained stable throughout the procedure except for transient mild bradycardia (HR = 50/min) and mild hypoxemia (SpO2 of 90%) after extubation, which improved with a bag-mask ventilation before reintubation.
Discussion
Rigid bronchoscopy is considered the gold standard for FB extraction from the tracheobronchial tree, as it provides control of the airway during the procedure and allows instruments to be passed through its lumen. 3 However, the presence of a cervical spine fracture with neck immobilization and maxillofacial trauma discourages its use. A flexible bronchoscope can sometimes substitute for a rigid bronchoscope and is can be particularly useful for removing FBs from distal airways and upper lobe bronchi because of the smaller diameter and greater flexibility in comparison with a rigid bronchoscope.1,4
Different instruments can be used in combination with flexible bronchoscope for extraction of aspirated tracheobronchial FB, such as forceps, baskets, snares, and balloons, with the choice depending on the nature of the FB and the availability of the instruments.1,4 Dropping or fragmentation of FB during its retrieval may be life threatening, which depends both on the nature of the FB and the experience of the bronchoscopist.
In the present case, the retained bronchial tissue glue, which was used for sealing the noted air leak during surgical repair of the ruptured left main bronchus, was discovered during routine fiberoptic bronchoscopy following the procedure. There are several potential adverse events related to the existence of the BioGlue in the tracheobronchial tree that may mandate urgent removal, including airway obstruction, edema, infection, adhesions, and tissue necrosis. An initial attempt to retrieve the FB using forceps and Dormier baskets was unsuccessful because the FB was too soft to be grasped, with the potential risk of fragmentation; this made it similarly difficult to be engulfed using the Dormier basket.
The Fogarty balloon-tipped embolectomy catheter has been used for the retrieval of aspirated FBs from the tracheobronchial tree.5,8,9 However, the thin shaft and the low-volume, high-pressure balloon can lead to complications such as bronchial rupture, tip embolization, and catheter disruption, particularly with repeated attempts. 9 The adjustable guide loop of the Arndt wire-guided endobronchial blocker has been used to grab an aspirated tooth from the tracheobronchial tree in a trauma patient. 10 However, in the present case, it was considered to be difficult to grab the elongated, thin polymerized BioGlue sheet, with added risks of sample fragmentation by the sharp nylon loop, particularly in the view of the initial failure using the Dormier basket. We used a 5.0-mm FOB to allow the use of the Fuji Uniblocker and forceps because of concerns about potential risks of pushing the FB deeper into the right main stem bronchus during insertion of the blocker. The use of the GlideScope added some novelty in addition, as it provided a good laryngoscopic view without unduly stressing the cervical spine. Note that while conventional balloon-tipped catheters were too soft to pass through the vocal cords with an ETT in situ, the Fuji Uniblocker was stiff enough to be pushed through the larynx alongside the ETT.
To the best of our knowledge, this is the first report on using the Fuji bronchial Uniblocker in FB extraction. Although the technique was previously described, the use of Fuji Uniblocker is rather unique. The Fuji Uniblocker is available in sizes 5 F and 9 F and offers advantages over a Fogarty catheter in the terms of utilizing a high-volume, low-pressure cuff, having a torque control mechanism to facilitate its placement beyond the aspirated FB, and having an inner lumen for potential suction and oxygenation.
We described a 5-step approach to remove a FB from the tracheobronchial tree in an intubated patient. First, a size 9.0 F Fuji Uniblocker was inserted outside the ETT guided with a GlideScope VL. Second, the blocker’s tip was introduced into the RMB beyond the retained FB and then inflated with air, preventing distal displacement. Third, the FB was removed gradually into the trachea with incrementally increasing the balloon volume. Fourth, the blocker, FB, and the ETT were removed as one unit under vision with a flexible bronchoscope. Finally, the FB was extracted from the pharynx using Magill forceps after ruling out residual material using a flexible bronchoscope.
Conclusion
In conclusion, the combined use of a GlideScope, bronchoscope, and Uniblocker placed outside the ETT could offer an effective method for removal of a retained foreign body.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.R. El-Tahan received free airway device samples from Ambu in April 2014 and from Airtraq in March 2015 for use in another three studies. He has no direct financial or other interests in Ambu or Airtraq (in the context of this and other studies.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.R. El-Tahan received free airway device samples from Ambu in April 2014 and from Airtraq in March 2015 for use in three previous studies. He has no direct financial or other interests in Ambu or Airtraq (in the context of this and other studies).
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.