
Abstract
Complications and critical events during cardiopulmonary bypass (CPB) are very challenging, difficult to manage, and in some instances have the potential to lead to fatal outcomes. Massive cerebral air embolism is undoubtedly a feared complication during CPB. If not diagnosed and managed early, its effects are devastating and even fatal. It is a catastrophic complication and its early diagnosis and intraoperative management are still controversial. This is why the decision-making process during a massive cerebral air embolism represents a challenge for the entire surgical, anesthetic, and perfusion team. All caregivers involved in this event must synchronize their responses quickly, harmoniously, and in such a way that all interventions lead to minimizing the impact of this complication. Its occurrence leaves important lessons to the surgical team that faces it. The best management strategy for a complication of this type is prevention. Nevertheless, a surgical team may ultimately be confronted with such an occurrence at some point despite all the prevention strategies, as was the case with our patient. That is why, in each institution, no effort should be spared to establish cost-effective strategies for early detection and a clear and concise management protocol to guide actions once this complication is detected. It is the duty of each surgical team to determine and clearly organize which strategies will be followed. The purpose of this case study was to demonstrate that a massive air embolism can be rapidly detected using near-infrared spectroscopy monitoring and can be successfully corrected with a multimodal neuroprotection strategy.
Keywords
Introduction
Complications and critical events during cardiopulmonary bypass (CPB) are very challenging, difficult to manage, and, in some instances, have the potential to lead to fatal outcomes. 1 One of the most feared complications is massive cerebral air embolism due to its high risk of cognitive deficit, stroke, mortality, and morbidity.2,3 It is a catastrophic complication and its early diagnosis and intraoperative management are still controversial. This is why the decision-making process during a massive cerebral air embolism represents a challenge for the entire surgical, anesthetic, and perfusion team. All caregivers involved in this event must synchronize their responses quickly, harmoniously, and in such a way that all interventions lead to minimizing the impact of this complication.
Considering the gaps in the medical literature in this regard, we present a case of a patient with a history of pulmonary atresia with intact ventricular septum whose massive air embolism during CPB during her fifth surgical intervention was successfully managed. Furthermore, the interventions and actions taken during the intraoperative period for the management of the massive cerebral air embolism during CPB are presented.
Case Description
A 20-year-old female patient with a history of pulmonary atresia with intact ventricular septum treated with multiple palliative surgeries complained of progressive shortness of breath. The last of these surgeries was an interposition of a valved conduit from the right ventricle to the pulmonary artery at age of 12 years. On physical examination, the patient was in good general condition with a grade IV/VI systolic murmur in the second left intercostal space and without signs of heart failure. In addition to her congenital heart disease, the patient had a history of mild to moderate cognitive impairment. An institutional preoperative transthoracic echocardiogram was done and reported moderate systolic and diastolic dysfunction in the left and right ventricles, severe tricuspid regurgitation, and a pulmonary valve with both mild stenosis and severe insufficiency. No intracardiac shunts were detected in the preoperative transthoracic echocardiogram.
The patient was scheduled for a tricuspid valve repair and replacement of the valved conduit. The cardiac anesthesiologist, pediatric noninvasive cardiologist, and pediatric cardiac surgeons established the perioperative plan. Preoperative medications were optimized. Initial vital signs were within normal ranges with an oxygen saturation of 92% without oxygen supplementation. The anesthetic induction was carried out uneventfully with fentanyl, midazolam, etomidate, and vecuronium. Sevoflurane and fentanyl boluses were used for anesthesia maintenance before CPB. The patient was monitored with an arterial line, a central venous catheter in the right internal jugular vein, and near-infrared spectroscopy (NIRS) using an INVOSTM monitor with bilateral cerebral sensors in the frontal region and a somatic renal sensor, which were placed before anesthetic induction. Baseline values for regional oxygen saturation (rSO2) were the following: right frontal NIRS, 69%; left frontal NIRS, 64%; and somatic NIRS, 80%. A transesophageal echocardiography probe was placed as a complement to hemodynamic monitoring.
Femoral vessels were cannulated and CPB was initiated prior to conventional median sternotomy. A Sorin Stockert S5 Heart Lung Machine with an open venous reservoir was used for CPB. A level sensor was placed in the venous reservoir; for air entrance monitoring an air bubble detection device was placed after the venous reservoir and proximal to the roller pump. Venous drainage was considered to be appropriate; therefore, a vacuum assist device was not necessary. On CPB, anesthesia was maintained with isoflurane and fentanyl boluses as needed. During the dissection of the mediastinum, air bubbles were detected in the right cardiac chambers with the transesophageal echocardiogram. The surgeon was alerted, and he reported that the innominate vein was torn during dissection, and he proceeded to suture it. Air bubbles were not visible neither in the venous nor the arterial femoral cannulas.
Minutes later, an abrupt drop (approximately 50% from baseline) on the bilateral cerebral NIRS values was observed without a significant drop from baseline of the somatic NIRS, which remained above baseline values during the surgery (see Figure 1). Immediately, the left cardiac chambers and aortic root were checked with the transesophageal echocardiogram, and a massive number of bubbles was detected (see Figure 2 and Supplementary Video 1; available in the online version of the article). The pediatric cardiac surgeon and perfusion team were alerted to the event and a massive cerebral air embolism was considered to be the cause of the drop in the cerebral rSO2. Up until that moment the patient had been hemodynamically stable in CPB for approximately 20 minutes without vasopressors, in sinus rhythm, and with a mean arterial pressure (MAP) ranging between 50 and 60 mm Hg and NIRS values above baseline; the central line was closed, and no infusions were being administered when the air embolism was detected.

Near-infrared spectroscopy monitor that shows the values of cerebral and somatic tissue oxygenation through the anesthesia induction, cardiopulmonary bypass initiation, at the moment in which air is detected simultaneously in the left cardiac chambers on the transesophageal echocardiogram, and immediately after retrograde cerebral perfusion administration. D, right frontal sensor; I, left frontal sensor; S, somatic sensor.
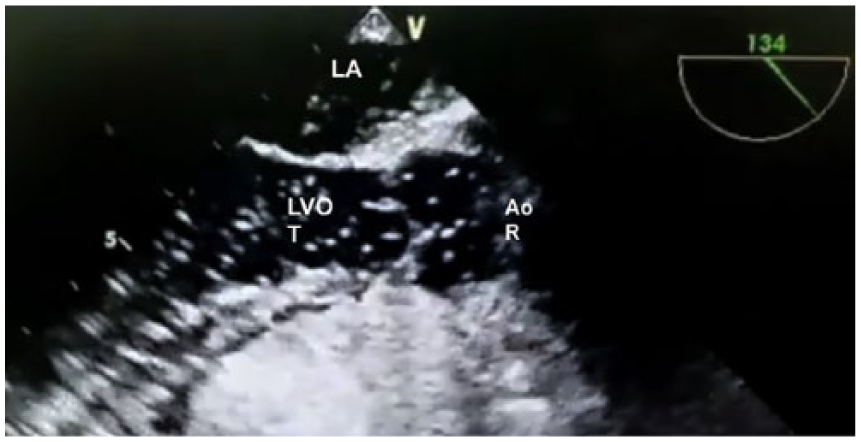
Long axis view of the left outflow tract that shows numerous bubbles of air. LA, left atrium; LVOT, left ventricle outflow tract; AoR, aortic root. See also Supplementary Video 1; available in the online version of the article.
The precise source of the air remains unknown, since no intracardiac shunts were previously described or shown in the transthoracic or transesophageal echocardiography, and air was neither observed when the circuit was inspected nor detected by the air bubble monitor on the arterial line of the CPB circuit. Once air was detected in the right cardiac chambers, the CPB circuit was inspected and no misconnections or disruptions that could explain air entrance were encountered. At the time, the surgeon continued with a thorough hemostatic control of structures in mediastinum but did not report any evident source of possible air entrance. Simultaneously, neuroprotection strategies were initiated as follows: the patient was positioned in deep Trendelenburg, a bolus of 30 mg/kg of methylprednisolone was administered, moderate therapeutic hypothermia was induced using an alpha stat strategy (target patient temperature: 24°C; temperature gradient during cooling: 6°C), and a bispectral index monitor (BIS) was placed at this point and used to quantify brain activity. This was targeted to remain at a 100% suppression ratio and a BIS score of 0 throughout the period of moderate hypothermia in order to achieve electrical brain silence with a continuous infusion of propofol that was started at the time. The team decided to target a MAP ≥70 mm Hg that was attained initially with phenylephrine boluses and then with norepinephrine infusion in order to optimize cerebral and coronary perfusion pressure. When the air embolism was detected the heart was still ejecting, but once the nasopharyngeal temperature reached 25°C to 24°C (30 minutes after the event) the heart went in to ventricular fibrillation until cardioplegia could be administered. The tear in the innominate vein was rapidly sutured and the pump sucker retrieved most of the blood; therefore, there was no massive amount of blood lost. However, we decided to transfuse 1 unit of packed red blood cells to optimize oxygen delivery and hemodynamic parameters including cerebral rSO2. All infusions were administrated directly in the venous reservoir through luer ports and B Braun perfusor space syringe pumps controlled infusion rates of noradrenaline (0.05-0.2 µg/kg/min titrated as needed) and propofol (100-200 µg/kg/min titrated by BIS values). The surgeon continued the dissection of mediastinum until the ascending aorta was released. At this point, an aortic root cannula was placed in order to vent air from the left cardiac chambers.
Given the massive number of air bubbles shown and the profound drop in cerebral rSO2 measured by NIRS, a consensus was reached by the anesthesiologist, surgeons, and perfusionist to administer retrograde cerebral perfusion (RCP) as a strategy to remove air emboli from the cerebral circulation. The arterial line of the CPB was disconnected from the arterial femoral cannula and connected to a 24-Fr right-angled metal venous cannula (Pacifico’s venous cannula) in the superior vena cava, and the aortic root vent was used to aspirate air bubbles. Inferior vena cava was snared and then RCP was administered for 2 minutes, with the flow rate adjusted to 300 mL/min in order to maintain 40 to 45 mm Hg of pressure in the arterial line of the circuit at a temperature of 25°C. Since the central venous line was in the right internal jugular vein, central venous pressure could not be measured to monitor and titrate RCP flow because the catheter was excluded once the tourniquet to secure the venous cannula was applied; therefore, pressure was measured off of a luer port located after the arterial line filter and proximal to the venous cannula in the superior vena cava.
Once the RCP was completed and the anesthesiologist confirmed the absence of air in the left heart chambers and aortic root with the transesophageal echocardiogram, surgery resumed. RCP was administered 40 minutes after the initial drop in cerebral rSO2 values, and as soon as it was completed, these values returned to normal. Blood gas analysis after RCP (20 minutes) at 24°C showed a PaO2 of 536 mm Hg, a PaCO2 24.5 mm Hg (corrected by temperature 43.3 mm Hg), and a lactate of 2.95 (see Table 1 for more details). Cerebral perfusion with an alpha stat strategy seemed preserved since cerebral rSO2 values rose steadily during cooling until they returned to baseline values after RCP was terminated. Conventional antegrade perfusion was reinitiated via the femoral cannulas because it was anatomically not possible to change to central cannulation. Approximately 90 minutes after the embolic event the surgeon was able to apply the aortic cross clamp and cardioplegia; after this, surgery continued as planned.
Arterial Blood Gas Analysis During CPB After Air Embolization and After RCP.
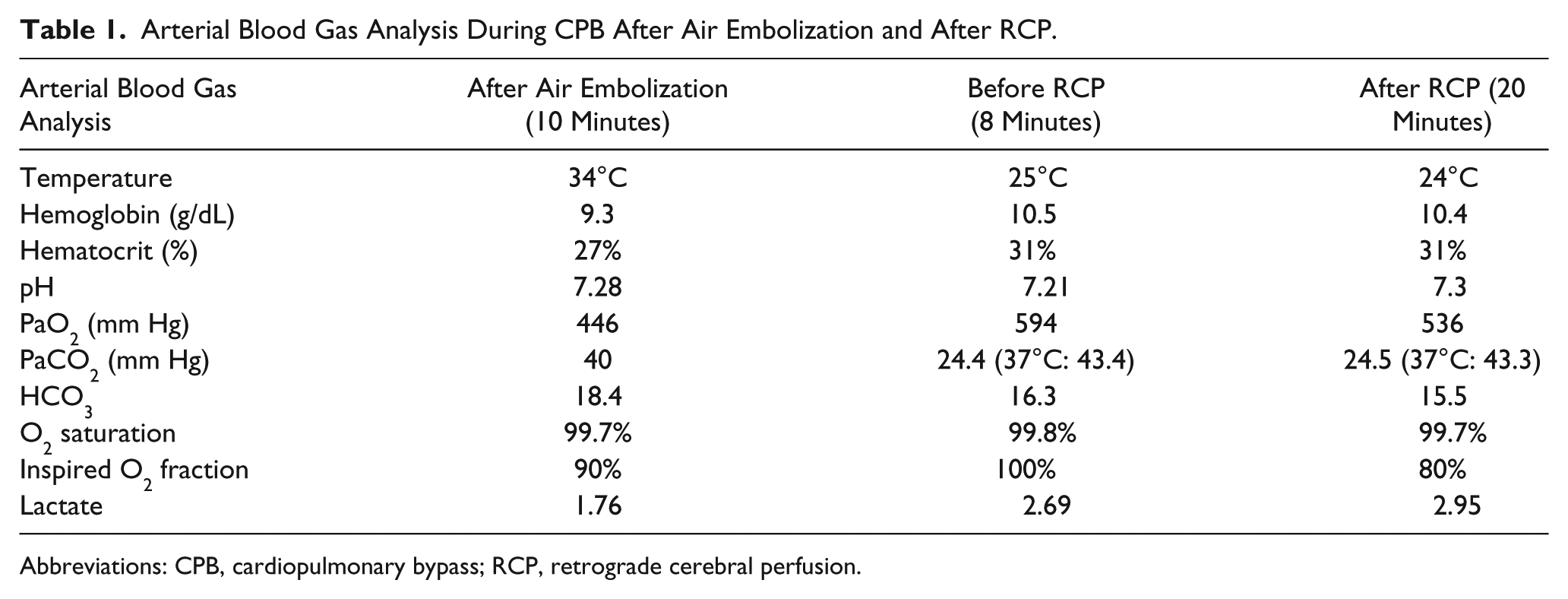
Abbreviations: CPB, cardiopulmonary bypass; RCP, retrograde cerebral perfusion.
Cerebral and somatic rSO2 values were held above baseline until the end of surgery. The patient was slowly rewarmed to a mildly hypothermic state (target temperature of 35°C) while carefully avoiding hyperthermia; the temperature gradient ranged between 5°C and 8°C during the rewarming phase. The propofol infusion was discontinued once mild hypothermia was achieved. The new conduit was interposed without any complication and the aortic clamp was released after conventional deaeration maneuvers and verification on transesophageal echocardiography that left ventricle and aortic root did not contain air bubbles (aortic cross-clamp time was 149 minutes). The patient was then weaned off CPB (CPB time was 279 minutes) with norepinephrine and milrinone drips for hemodynamic support.
The mediastinum was packed with compresses and a vacuum-assisted device was placed for delayed sternal closure because of coagulopathy and risk of cardiac tamponade. The patient was transferred to the cardiovascular intensive care unit under deep sedation with mechanical ventilation and vasoactive hemodynamic support. The sequence of intraoperative events is described in Figure 3.
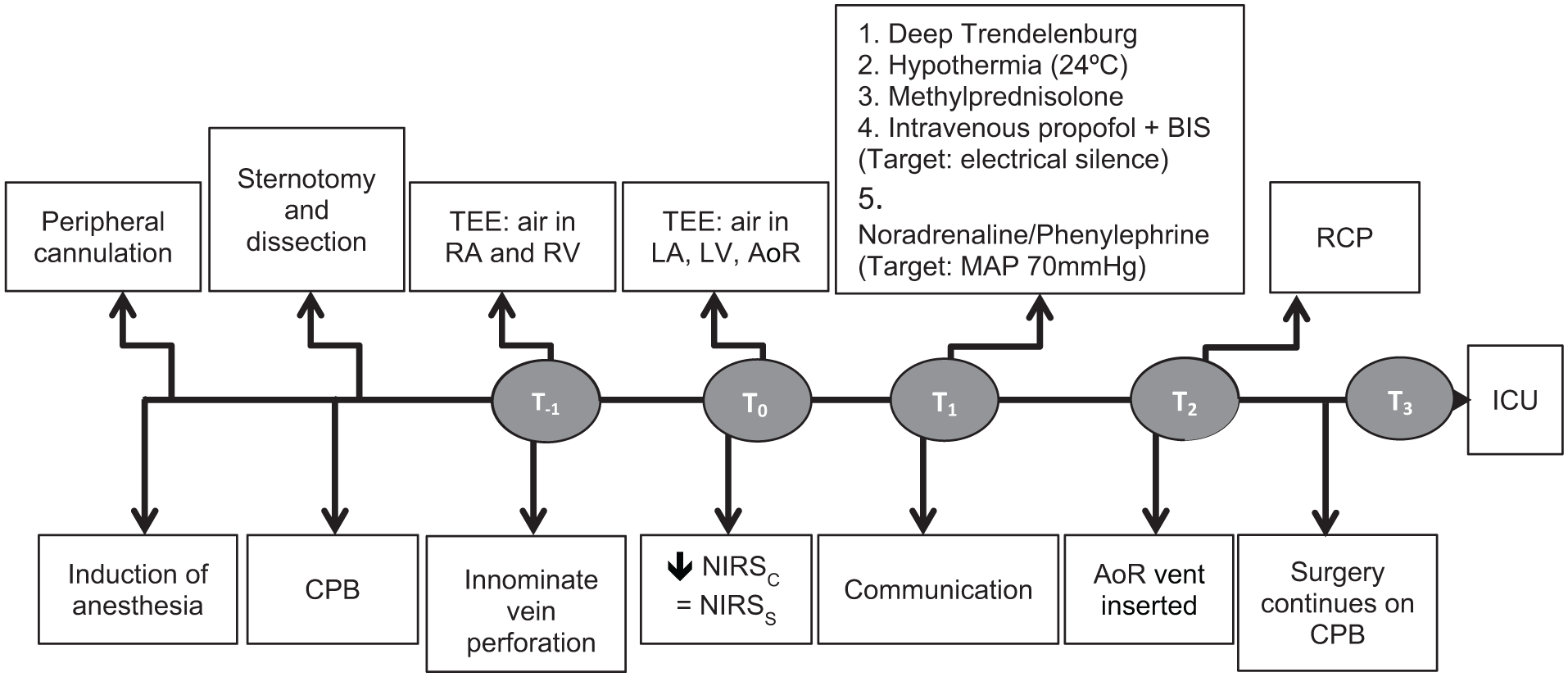
Timeline of important events during the intraoperative period. T−1: moment of air detection in the right heart chambers (5 minutes before cerebral embolization), T0: moment of massive cerebral air embolism detection, T1: 1 to 5 minutes after T0, T2: 40 minutes after T0; T3: end of surgery (420 minutes after T0). CPB, cardiopulmonary bypass; TEE, transesophageal echocardiography; RV, right ventricle; RA, right atrium; NIRSC, cerebral NIRS values; NIRSS, somatic NIRS values; LA, left atrium; LV, left ventricle; AoR, aortic root; BIS, bispectral index; MAP, mean arterial pressure; RCP, retrograde cerebral perfusion; ICU, intensive care unit.
The sternum was closed 24 hours after the initial postoperative period and the patient was awakened on the first postoperative day. Neither sensory or motor deficits nor signs of focalization were documented. A postoperative computed tomography scan on the 11th postoperative day did not show ischemic changes, and after a rigorous examination by the institutional neurologist, focal ischemic sequelae were ruled out (see Figure 4).
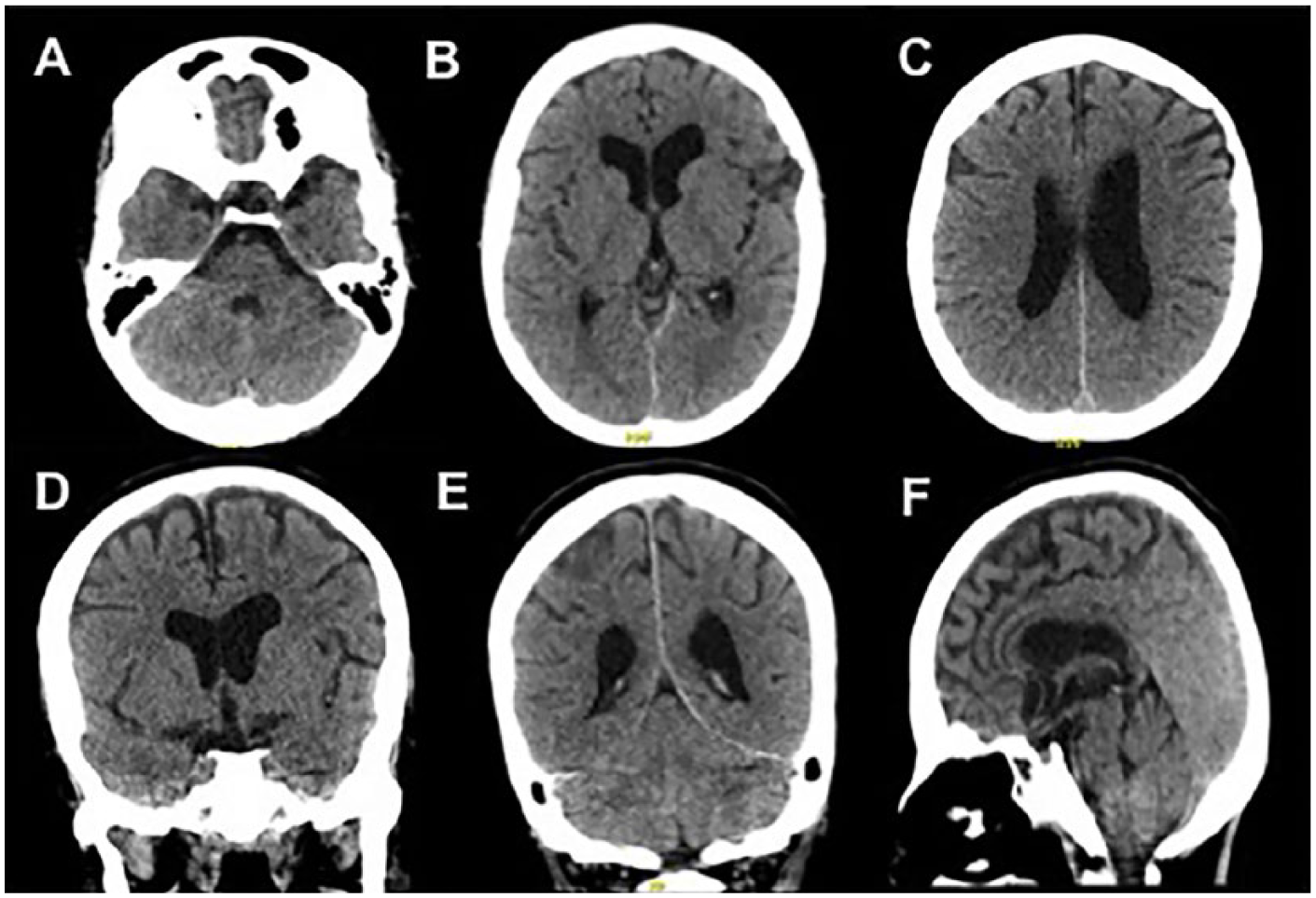
Noncontrast brain computed tomography scan on 11th postoperative day. (A-C) Axial reconstructions show normal cortical and subcortical differentiation of the cerebral and cerebellar parenchyma without any focal or diffuse lesions and with a normal appearance of the ventricular system and subarachnoid space. (D and E) Coronal reconstructions where the thalamic and cerebellar vermis is seen without any focal lesions. (F) Sagittal pons and corpus callosum of normal scanographic appearance.
The patient was discharged from the intensive care unit on the 12th postoperative day in good general condition, with a tracheostomy due to difficult ventilatory weaning secondary to physical deconditioning. Once neurological causes for difficult weaning were ruled out, the patient was put on proportional assist ventilation, which allowed the conditioning and improvement of ventilatory mechanics and ultimately allowed satisfactory ventilatory weaning. The patient did not suffer from encephalopathy and did not have any neurological deficits or signs of focalization. Finally, the patient was discharged from the hospital at 45 days postoperatively and currently is in good general condition and has returned to her normal daily life.
Discussion
Massive air embolisms during CPB are a catastrophic complication. Although the incidence is rare and ranges from 0.1% to 0.2%, 2 its effects can be devastating and even lethal for the patient once it occurs. 4 In our patient, no intracardiac shunts appeared in the preoperative echocardiogram. Transesophageal echocardiography during the intraoperative period did not show any visible intracardiac shunts either. At the moment of the incident, the surgical field was filled with adhesions, and a previous vascular lesion of the innominate vein with profuse bleeding also obscured a clear view of the anatomical structures. At this point, the main focus of the surgeon was bleeding and hemostatic control. Air entrance might have been related to other inadvertent vascular lesions during the dissection of the mediastinum that was addressed at the moment of hemostatic control. To this day, the source of air entering the left cardiac chambers remains uncertain, but both the perfusionist and the anesthesiologist ruled out malfunctions in the circuit of the CPB as the source.
After an air embolism is suspected, the question that should be addressed next is what to do? At our institution, it is the responsibility of the anesthesiologist to coordinate the actions and steps to follow with the surgical and perfusion team in an efficient and orderly manner. Currently, there is no algorithm or standard of care in the literature for the treatment and management of a massive cerebral air embolism during CPB. 5 In our case, we tried to address the problem with a multimodal approach by taking into account the multiple pathways and mechanisms that mediate tissue damage in this kind of ischemic brain injury in order to offer the best neurological protection strategy.
Neuroprotection is defined as any strategy that is intended to antagonize, interrupt, or reduce the sequence of harmful molecular or biochemical events that can generate irreversible neuronal death. 6 Multiple strategies have been investigated in experimental laboratory conditions with mixed results. However, they have seldom been successfully extrapolated to clinical scenarios. 6 Based on our experience and our knowledge of current literature on the pathophysiology of the event, we proposed a number of interventions to provide neuroprotection and diminish irreversible damage to cerebral tissue during the intraoperative period that are summarized below (see Figure 5):
Promptly identify the problem and its cause (NIRS, transesophageal echocardiography, and identify sources of air entry).
Limit the injury: prevent entry and embolization of more air (deep Trendelenburg position and limit sources of air entry).
Restore the oxygen supply-demand balance: decrease the consumption and metabolic requirement of cerebral oxygen (induced electric brain silence monitored by BIS and hypothermia).
Control proinflammatory pathways leading to injury produced by ischemia-reperfusion (steroids).
Improve tissue perfusion and optimize oxygen delivery (keep mean arterial blood pressures higher than usual with vasopressor support if necessary, avoid anemia, optimize fraction of inspired oxygen, and hold NIRS above baseline values).
Decide if mechanical removal of air emboli is pertinent (RCP or antegrade selective cerebral perfusion).
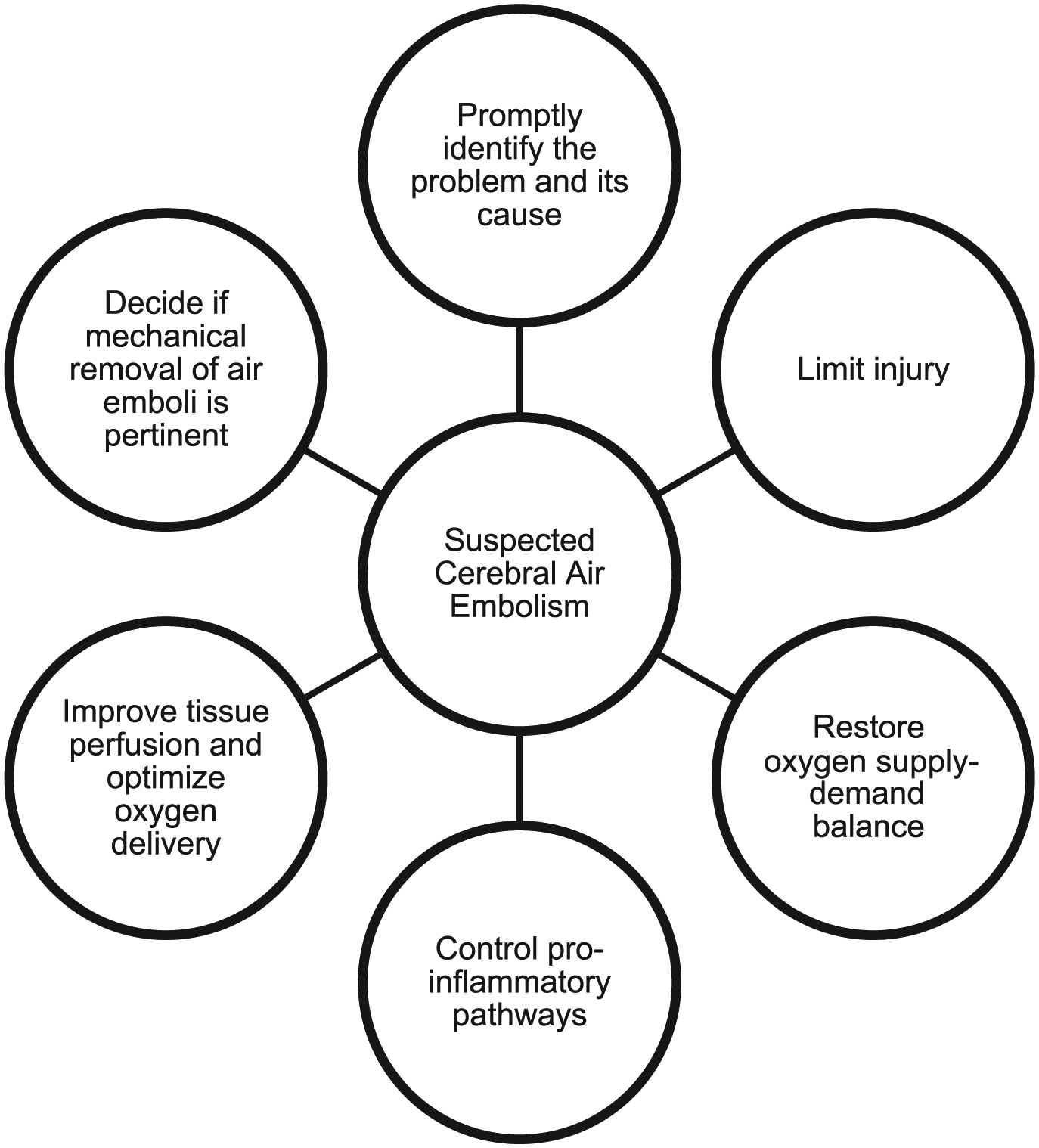
Approach to management of massive cerebral air embolism during cardiopulmonary bypass.
Sources of air embolism during CPB are diverse. However, the most common ones are air entrance through the surgical field with manipulation of large vessels or heart chambers and the components of the CPB circuit. 4 In our case, the source of air was not in the CPB circuit but in the surgical field due to a challenging anatomic scenario (a mediastinum with multiple adhesions). This situation allowed the undetected entry of a massive amount of air into cardiac cavities before it was possible to place the aortic root suction cannula. However, the rSO2 monitoring and transesophageal echocardiography made it possible to quickly identify a complication that most likely could not have been detected by the CPB air bubble sensor given the location of the device and the source of air entry in this scenario.
Both the NIRS and transesophageal echocardiography were critical tools in the rapid diagnosis of the situation and the direction of subsequent actions. Massive air embolisms can be identified from the surgical field by direct observation by the surgeon, direct viewing in the CPB circuit, via transesophageal echocardiography, or by CPB detection devices. 5 However, these means of detection may fail to identify an air entry point in the context of a complex surgical case such as ours. Permanent transesophageal echocardiographic evaluation during the entire surgery is not feasible; therefore, there are periods in which catastrophic events such as a massive cerebral air embolism can go unnoticed and early diagnosis can be delayed. Other diagnostic tools such as transcranial Doppler or jugular bulb saturation may be impractical and require significant operator expertise for routine clinical use. Hence, NIRS offers a noninvasive, safe, and easy-to-use alternative that provides information on regional cerebral metabolism and the balance of oxygen demand-supply in real time. 5
In our case, the information provided by the NIRS monitor was decisive since it allowed us to initiate actions for neuroprotection in a timely manner. Even though the somatic NIRS did change at the time of the incident, the maximum change in somatic rSO2 was 15% of the baseline value, which is not considered significant and, unlike cerebral rSO2, it never reached an absolute value below 40%. Once the bleeding from innominate vein was controlled, somatic rSO2 rapidly went to baseline values (80%) while cerebral rSO2 remained low for approximately 40 minutes. Cerebral oximetry has been used successfully to detect intraoperative embolic events for surgery involving the aortic root or the aortic arch. 7 As previously established by other authors, NIRS is a monitoring tool that detects alterations in cerebral oxygenation and the hemodynamic coupling between the oxygen supply and metabolic demand in a manner that is noninvasive, rapid, and sensitive. It does not represent any risks for the patient, and unlike other monitors such as the BIS, it is not modified by variations in temperature.8,9
The ability of NIRS to detect critical levels of cerebral hypoperfusion has been reported in the literature, and it can play a critical role in decision making. 10 Low values of cortical rSO2 indicate an alteration between cerebral perfusion and regional oxygen demands. Decreases to an absolute value of 50% or a reduction of 20% below the baseline can be considered cutoff points for critical rSO2 and have been associated with adverse neurological outcomes. 11 Our patient’s cerebral rSO2 dropped abruptly to almost 50% from baseline due to a massive air embolism in the cerebral circulation, and this monitor allowed us to identify the problem. NIRS technology has also been used in cardiac surgery to establish an association between cerebral oxygenation values and adverse outcomes (cognitive dysfunction, prolonged hospitalization, and cerebral ischemia). 9
In addition to the detection of ischemic events or alterations in the oxygen delivery-demand balance, another purpose for intraoperative rSO2 monitoring is to provide information on cerebral metabolic supply. In summary, NIRS enabled us to guide the decision-making process and ensure an adequate oxygen delivery based on our patient’s requirements. 12 In addition to NIRS, BIS was added to ensure the lowest cerebral metabolic consumption through induction of electrical silence during the critical event. Likewise, we established a goal for MAP ≥70 mm Hg because the use of high MAPs during CPB has shown beneficial effects on functional outcomes and, contrary to what one might think, low MAPs do not decrease the embolic burden on the central nervous system and worsen functional outcomes. 13
Regarding the cellular and molecular proinflammatory mechanisms that mediate ischemic injury, in vitro studies of cellular models of oxidative injury have established the neuroprotective effects of methylprednisolone, which suppresses autophagy and apoptosis in cells exposed to oxidative damage. 14 Therapy with steroids as a neuroprotection strategy is still under debate. However, in the case of CPB and an ischemic injury, there is evidence that suggests that their use reduces proinflammatory mediators, mitigates ischemia-reperfusion injury, limits cytotoxicity induced by hypothermia-rewarming injury, and might have beneficial effects on neurological outcomes.15-18 Beyond the pharmacological and physiological effects of propofol on cerebral metabolism, no clinical study to date has yet shown that propofol improves neurological outcomes after cerebral injury, and it may not be considered a neuroprotective agent alone. However, it might play a role in the context of a multimodal neuroprotection strategy for brain injury. 19 Induced deep hypothermia was used as a means of protecting the brain from ischemic injury by reducing oxygen demand and excitotoxicity. 20 It has been used for this purpose during CPB with favorable clinical results when hyperthermia after rewarming is avoided and mild hypothermia is targeted after CPB.20,21
In addition, RCP was also used to remove air emboli from cerebral circulation. This modality of perfusion does not guarantee adequate cerebral capillary flow or prevent ischemia; indeed, considering the hemoglobin level, the oxygen delivery rate was 46 mL/min at a 300mL/min flow, but this was sustained for only 2 minutes, and as stated before, cerebral perfusion was preserved since cerebral rSO2 values rose steadily and did not fall during and after RCP was terminated. However, it allows removal of air and debris from cerebral circulation and extends the safe period of circulatory arrest in deep hypothermia to more than 60 minutes.1,22 Although its use is not standardized, case reports have suggested administering RCP for 1 to 2 minutes at 28°C and with a pressure ranging from 20 to 40 mm Hg in the arterial line of the CPB circuit.22-25 Other authors have reported that RCP should be administered for 5 minutes with a flow of 300 to 500 mL/min while maintaining jugular venous pressure <25 mm Hg. 26 In our case, it was decided to titrate flow according to pressure in the arterial line in order to maintain pressure between 40 and 45 mm Hg and avoiding any increase above this range to prevent cerebral edema. Even though RCP is described in the literature as a fundamental part of the armamentarium of cerebral protection after a massive air embolism, the other neuroprotection strategies used were effective in preventing permanent neurological injury given that a satisfactory outcome for the patient was achieved in spite of surgical conditions that did not allow the immediate initiation of RCP.
A massive cerebral air embolism is undoubtedly a feared complication during CPB. If not diagnosed and managed early, its effects are devastating and even fatal. Its occurrence leaves important lessons for the surgical team that faces it. The best management strategy for a complication of this type is prevention. Nevertheless, a surgical team may ultimately be confronted with such an occurrence at some point despite all the prevention strategies, as was the case with our patient. That is why, in each institution, no effort should be spared to establish cost-effective strategies for early detection and a clear and concise management protocol to guide actions once this complication is detected. It is the duty of each surgical team to determine and clearly organize which strategies will be followed in a complication of this magnitude.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.