
Abstract
Tracheal bronchus (TB) occurs in 0.1–3% of the population as an accessory bronchus that originates in the trachea, typically supplying the right upper lobe. The presence of a TB can pose unique airway challenges, particularly during procedures that require lung isolation. Here, we describe a case of TB with difficult lung isolation. Careful examination with fiberoptic bronchoscopy permitted double lumen tube positioning without obstruction of the TB. A second case is presented where the presence of TB did not affect anesthetic management. Implications of TB for airway management and strategies for successful one-lung ventilation are discussed.
Keywords
Introduction
Tracheal bronchus (TB) occurs in 0.1–3% of the population as an accessory bronchus that originates in the trachea, typically supplying the right upper lobe (RUL).1-3 Most often, the takeoff is <2 cm proximal to the carina but it can be higher.
4
The TB is characterized as “displaced” when the affected lung segment is supplied solely by the accessory bronchus or as “supernumerary” when it occurs concurrently with the usual bronchial supply.
5
Anatomical classification based on the distance of the TB takeoff from the carina (Figure 1) has also been used.3,6 Other systems of classification have been used but these are unlikely to be of significance to the anesthesiologist in practice.6-8 Patients are typically asymptomatic although may present with recurrent RUL pneumonia.
5
TB can be associated with other congenital abnormalities, such as Down syndrome, VACTERL association, and tracheoesophageal fistula, among others.
9
In children, TB is usually discovered during bronchoscopy for pulmonary pathologies. In asymptomatic adults, it is often discovered incidentally on CT imaging or upon fiberoptic bronchoscope (FOB) assisted placement or troubleshooting of a double lumen tube (DLT) for surgery with one lung ventilation (OLV).
10
Here, we describe a case of tracheal bronchus causing difficult lung isolation. A second patient with tracheal bronchus not impacting the anesthetic plan is also described. Written HIPAA authorization was obtained for both patients prior to writing of this report. This manuscript adheres to the applicable EQUATOR guidelines for case reports by using the CARE and Anaesthesia Case Report (ACRE) checklists. Simple classification system for TB. Type 1 TB has an accessory bronchus that arises greater than 2 cm from the true carina. Narrowing of the trachea distal to the TB takeoff can result in the appearance of a “false carina” as the accessory bronchus may be as large or larger than the distal trachea in diameter. Type 2 TB also arises greater than 2 cm from the carina but without distal narrowing of the trachea. Type 3 TB arises within 2 cm of the carina. TB, tracheal bronchus.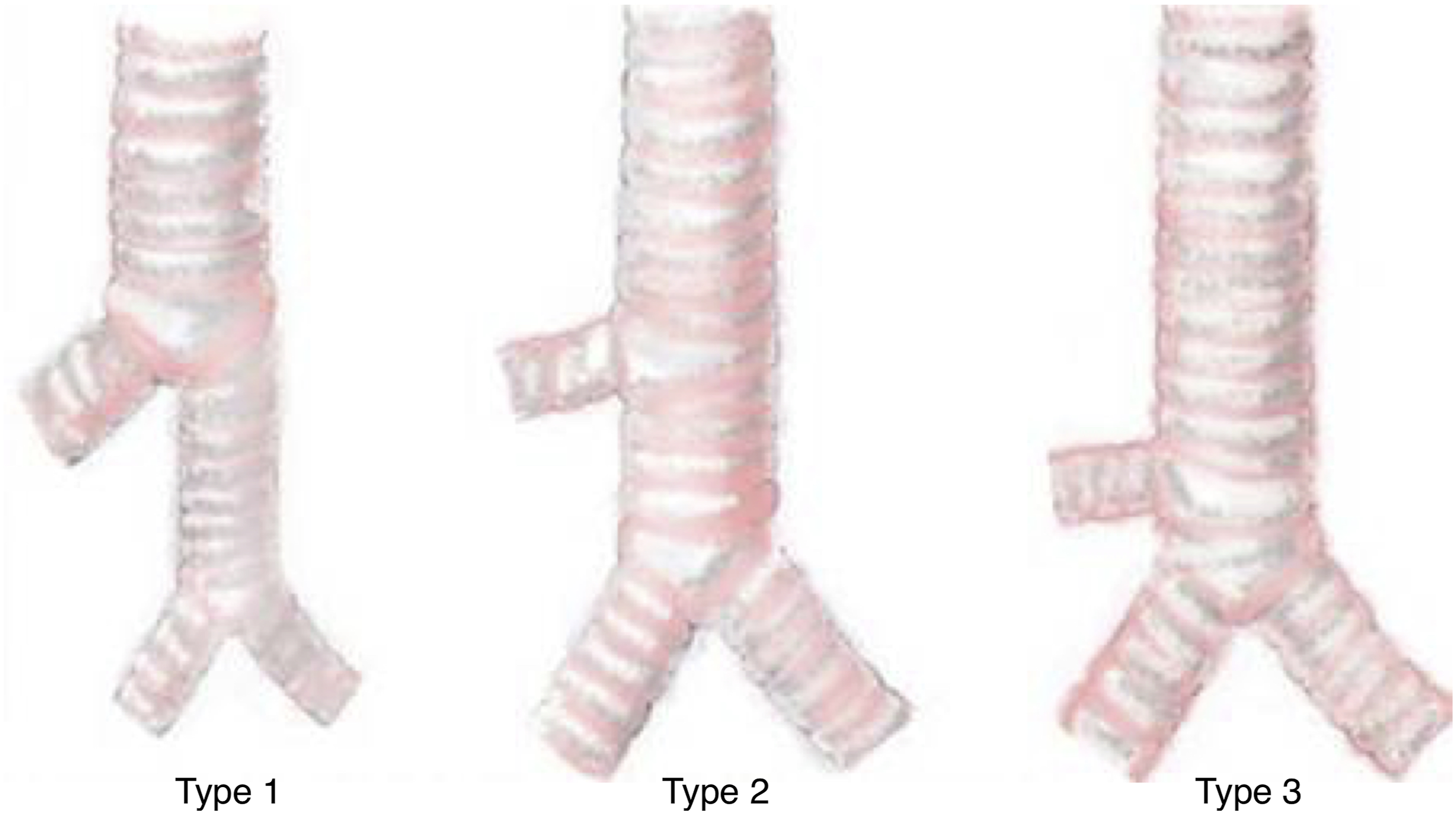
Report
Case 1
A 66-year-old woman with a history of gastroesophageal reflux disease and severe mitral regurgitation presented for minimally invasive mitral valve repair via right anterior mini-thoracotomy requiring OLV. After unremarkable induction of general anesthesia, a 37F left DLT was placed through the glottic opening under direct laryngoscopy. The DLT was then advanced under direct FOB guidance until the endobronchial lumen was appropriately positioned in the left main bronchus. After right mini-thoracotomy, the surgeon observed partially inflated right lung despite right lung isolation. FOB examination did not reveal DLT malposition. The DLT was then partially retracted and careful FOB examination revealed a right TB with its origin 3–4 cm proximal to the carina. The DLT was then repositioned with the tracheal lumen orifice above the origin of TB, while still achieving acceptable bronchial cuff position in the left main bronchus. Following this, lung isolation was achieved with successful deflation of right upper lobe. Further operative course and recovery was uneventful. When imaging studies were looked at retrospectively, careful examination of the patient’s postoperative chest radiographs revealed the subtle presence of the right TB though this was not described in the radiologist’s report (Figure 2A). There were no other imaging studies of the chest for review. The presence of a tracheal bronchus can be subtly distinguished on postoperative chest radiograph in patient #1 (A). Arrow indicates the tracheal bronchus orifice. Computed tomography scan coronal slice demonstrating tracheal bronchus to the right upper lobe in patient #2 (B).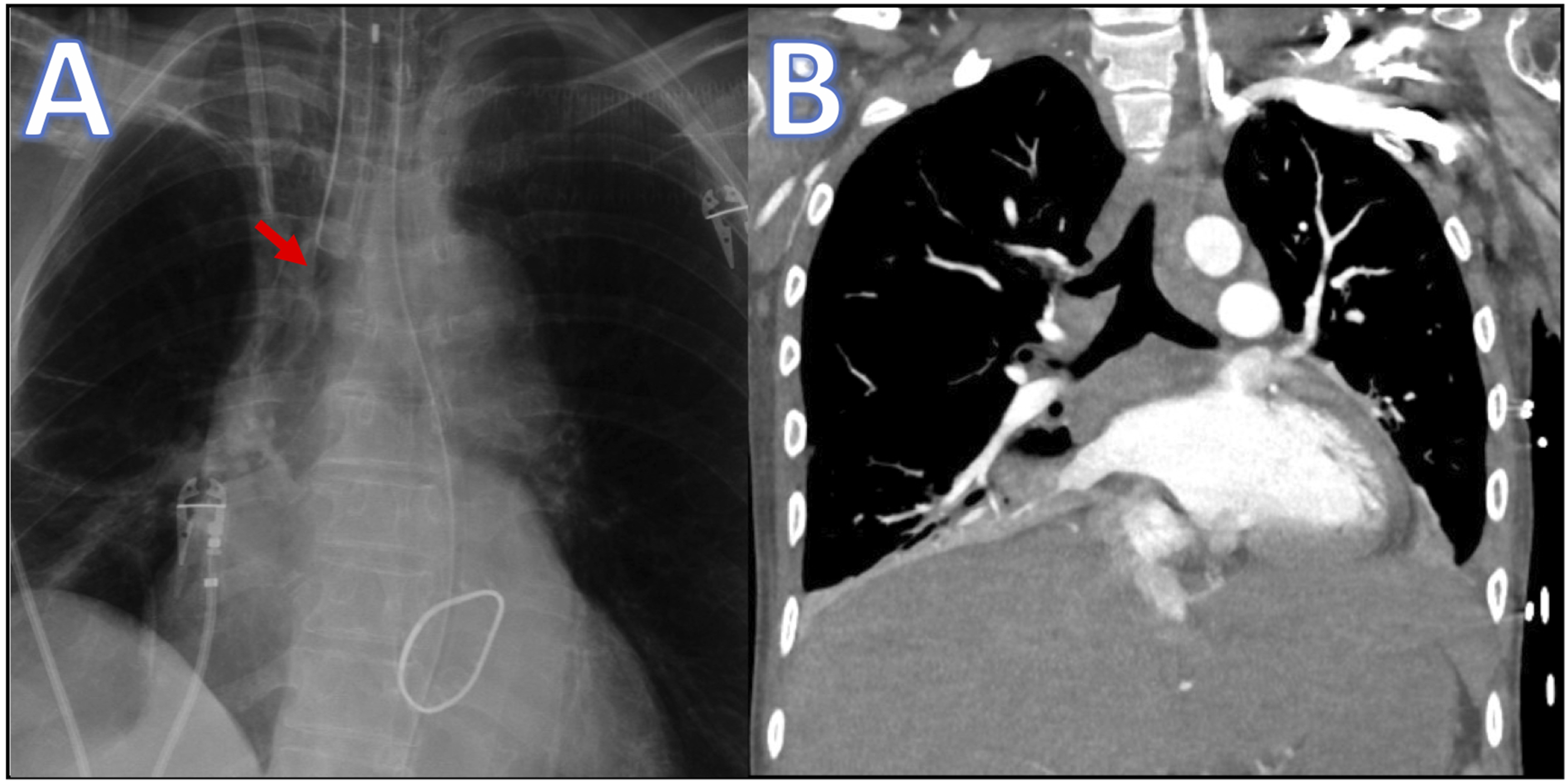
Case 2
A 35-year-old man with a history of intellectual disability, seizures, and frequent admissions for aspiration pneumonia who was now status post gastric tube placement, presented to the operating room for conversion to gastrojejunostomy tube. Rapid sequence induction was performed with propofol, fentanyl, and succinylcholine with easy insertion of an 8.0 mm endotracheal tube (ETT). During the procedure, the anesthesiology resident retrieved the patient’s most recent computed tomography (CT) scan to review for educational purposes and noted the presence of a right tracheal bronchus (Figure 2B), which had not been previously identified by the anesthesia team. There was no evidence of issues with ventilation and the ETT was presumed to be adequately positioned and adjustments were not made. The operative course was uneventful, and the patient was extubated at the end of the case and brought to the recovery area at his baseline condition. Retrospective review of the patient’s imaging showed the known presence of the right TB, which was included in the radiologist’s report of previous CT imaging.
Discussion
Tracheal bronchus poses unique challenges to ventilation, particularly during OLV. If the tracheal cuff of a left DLT obstructs, or is distal to the TB takeoff, the RUL will fail to ventilate during two-lung ventilation or when ventilating the right lung. This can lead to RUL atelectasis, which may be a source of poor oxygenation during or after OLV. Alternatively, when ventilating the left lung in isolation, the RUL may fail to collapse while ventilating the endobronchial lumen. In these situations, TB should remain on the differential diagnosis and careful fiberoptic examination can confirm the diagnosis and permit adjustment of tube position to avoid TB obstruction (Figures 3A and 3B). When DLT retraction would preclude adequate position of the endobronchial cuff, for example, in the presence of a very proximal TB takeoff, alternatives to DLT placement may be needed. For right-sided surgery, a single lumen tube with a bronchial blocker in the right main stem bronchus and a second bronchial blocker
11
or Fogarty catheter
12
in the tracheal bronchus can be used (Figure 3C). For left-sided surgery, consider the use of a single lumen tube with a bronchial blocker in the left main bronchus (Figure 3D).3,13 If replacement of a DLT during surgery is difficult, lowering tracheal cuff pressure may permit collapse of the RUL while permitting adequate left-sided OLV.
10
However, this approach must be taken with great caution to avoid permitting oral secretions to enter the trachea past a partially deflated tracheal cuff. A malpositioned double lumen tube with the tracheal cuff obstructing the opening to the tracheal bronchus, as described in case 1 (A). An appropriately positioned double lumen tube with the tracheal cuff proximal to the tracheal bronchus takeoff, achieved in case 1 by careful withdrawal of the endotracheal tube under fiberoptic guidance (B). When tracheal bronchus anatomy does not permit adequate positioning of a double lumen tube, a single lumen tube with a bronchial blocker in the right main stem bronchus and a second bronchial blocker in the tracheal bronchus can be used for left lung ventilation (C). For right lung ventilation in this setting, a single lumen tube with a bronchial blocker in the left main stem bronchus can be used (D).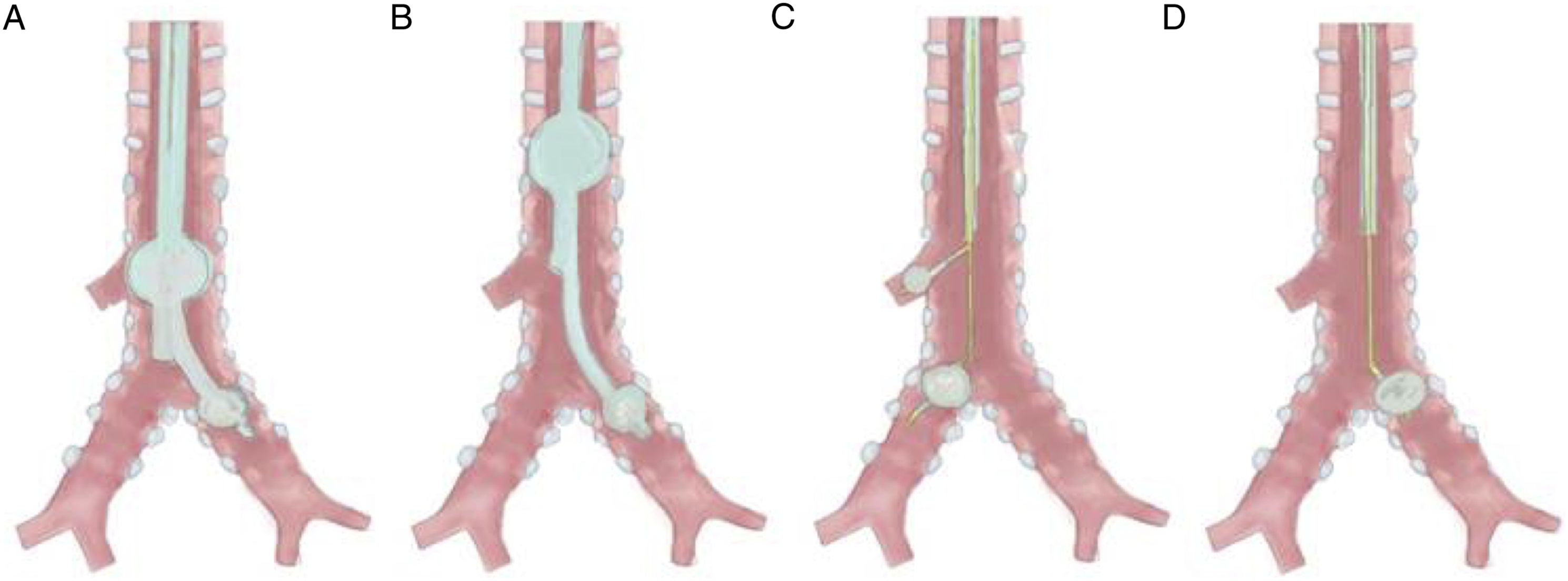
Right-sided DLT can theoretically be used with TB but are also prone to problems with ventilation and lung isolation. When ventilating the tracheal lumen, the RUL may fail to collapse if the TB takeoff is obstructed by or proximal to the tracheal cuff—a highly likely scenario considering that TB is usually found within 3–4 cm of the carina. Alternatively, when ventilating the endobronchial lumen, the RUL may not ventilate in the presence of a “displaced” type TB. Accordingly, a left DLT should be used whenever possible in the presence of TB. When a left DLT is contraindicated or cannot be adequately placed, a single lumen ETT can be used in combination with bronchial blockers or Fogarty catheters, depending on the operative side, as described above (Figures 3C and 3D).
TB also poses implications for single lumen tubes, including accidental TB intubation leading to atelectasis of remaining lung or obstruction of the TB takeoff by the tracheal cuff causing RUL atelectasis or post-obstructive pneumonia. 14 Inability to ventilate secondary to presumed inadvertent TB intubation has also been described. 2 Solutions include careful placement with rotation of ETT tip away from TB orifice and ensuring ETT cuff position above the TB origin using fiberoptic guidance.2,4
Though the range of incidence of TB in the literature ranges from 0.1–3%, in a retrospective study of 9781 multidetector CT images the overall incidence was 0.31% (approximately 1 in 300 patients). 15 Thus, while uncommon in the general population, anesthesiologists who regularly perform cases requiring OLV are likely to encounter TB at some point in their careers. Knowledge of methods to troubleshoot difficult lung isolation due to TB can permit adequate OLV in these patients. In case 1, an incidentally discovered TB was found to be the cause for failed RUL collapse during OLV. Adjustment of the DLT position under FOB guidance permitted RUL collapse and adequate OLV. No CT images were available for review preoperatively, which likely would have changed the airway management to either more precise placement of a left DLT or use of bronchial blockers. It is a common technique for anesthesiologists to place a DLT “blindly” with confirmation of position with FOB—a technique that would seem more likely to result in a missed TB. Surprisingly, the DLT in case 1 was inserted under continuous FOB guidance but TB was still missed. Possibly, the initial placement of the DLT through the glottis may have placed the bronchial lumen distal to the TB. Thus, when continuous FOB is employed, if the FOB is inserted through the bronchial lumen to guide the tube into the left mainstem, the tip of the tube can be below the TB takeoff making it impossible to visualize. This is the most likely scenario in our case; however, it cannot be ruled out that the right-sided TB was simply missed while attention was directed at guiding the FOB and DLT into the left mainstem bronchus. Alternatively, the carina may be mistaken for a “false carina” between the trachea and tracheal bronchus with either FOB-guided insertion or blind insertion with FOB confirmation. This highlights the importance of vigilance for unexpected tracheal anatomy. However, routine use of FOB-guided advancement of a DLT would reasonably better equip the anesthesiologist for diagnosis of rare pathologies, such as TB. In case 1, TB was subtly present on retrospective review of the patient’s preoperative chest radiograph. However, this was not described in the radiologist report and would most likely be missed by an anesthesiologist if its presence was not already known. Even when CT imaging is available, this can be missed by the anesthesiologist, as demonstrated by case 2. Although the patient in case 2 did not require alterations in airway management, this certainly could have been required. This further demonstrates the importance of a thorough preoperative review of the chart including relevant imaging. In this way, the anesthesiologist can be prepared to manage the airway of a patient with a TB—whether it is known or yet to be discovered.
Footnotes
Acknowledgments
The authors would like to thank Aseel Walker, M.D., Department of Anesthesiology, Hartford Hospital, Hartford, CT, USA, and Janet Maurice, Digital Marketing Consultant, PROMODOGG LLC, for creating the illustrations. We also thank Jeffrey Gross, M.D., Professor and Chair, Department of Anesthesiology, UConn Health, Farmington, CT, USA, for his thoughtful comments on the manuscript in its preparation.
Abbreviations
CT, computed tomography; DLT, double lumen tube; ETT, endotracheal tube; FOB, fiberoptic bronchoscope; OLV, one lung ventilation; RUL, right upper lobe; TB, tracheal bronchus
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.