
Abstract
Objectives
To determine if hemodynamic changes secondary to propofol administration are a result of direct myocardial depression as measured by global longitudinal strain (GLS). The authors hypothesized that propofol would cause a significant worsening in GLS, indicating direct myocardial depression.
Design
Prospective, observational.
Setting
Endoscopy suite at a single academic medical center.
Participants
Patients undergoing outpatient, elective endoscopic procedures at an outpatient clinic of a single tertiary care academic medical center.
Interventions
None.
Measurements and Main Results
Limited transthoracic echocardiograms were performed before and after patients received propofol for endoscopic procedures. Post-processing measurements included GLS, 2D (dimensional) ejection fraction (2D EF), and 3D EF. Using paired sample Student’s t test, no statistically significant change in GLS, 2D EF, or 3D EF was found despite statistically significant hypotension. In fact, there was a trend toward more negative GLS (improved myocardial function) in patients after receiving propofol.
Conclusion
We found propofol did not cause a reduction in systolic function as measured by GLS, a sensitive measure of myocardial contractility. Therefore, decreases in blood pressure after a propofol bolus in spontaneously breathing patients are likely due to decreased vascular tone and not impaired left ventricular systolic function. These results should be considered in the management of propofol-induced hypotension for spontaneously breathing patients.
Introduction
Dose-dependent hypotension is one of the most common side effects of propofol administration. 1 Propofol has classically been described as a cardiovascular depressant with decreases in cardiac contractility, cardiac index, and stroke volume index, all of which may contribute to resultant hypotension.2,3 However, a direct myocardial depressant effect from propofol has not been fully elucidated, as peripheral vasodilation has also been shown to be a cause of hypotension.4-6 The objective of this pilot study was to ascertain if direct myocardial depression contributes to the hemodynamic changes observed after propofol administration.
Multiple studies have investigated the effects of propofol on myocardial function. The results have been inconsistent and variable. In extracted left ventricular (LV) papillary muscles of rats, propofol did not cause changes in myocardial contractility. 7 A canine model found propofol had negative inotropic effects only at supratherapeutic doses, 8 and another found that propofol-induced vasodilation was the mechanism of decreased cardiac output.4,9 In human studies measuring cardiac output by thermodilution technique, propofol administration had no effect on cardiac output.10,11 However, similar studies found cardiac output was decreased significantly when propofol was given.12,13 Larsen and colleagues 14 used tissue-tracking Doppler to show a significant decrease in LV function after a propofol bolus. Measurement of global longitudinal strain (GLS) in patients with normal LV function under positive pressure ventilation showed that a propofol and midazolam induction diminished contractility. 15
The aim of this pilot study was to build on the above-mentioned studies with a few key differences. We measured myocardial function with LV GLS because it is a sensitive marker of systolic function that correlates well with 3-dimensional (3D) magnetic resonance imaging (MRI) measurements of ejection fraction (EF). 16 GLS is derived from speckle tracking that measures longitudinal shortening of the myocardium as a percentage (change in length proportional to baseline length). A normal value for GLS is <−18%, while >−16% is abnormal and −16% to −18% is borderline. 17 The closer this value moves to 0%, the more likely there is an abnormality in LV systolic function. 18 Additionally, patients in this study received only propofol for induction and maintained spontaneous respiration, removing 2 important confounding variables in prior studies. In this prospective, observational pilot study, we aim to show that weight-based propofol for sedation does not change GLS, which is a reflection of myocardial performance.
Methods
The study was approved by the local institutional review board. Written informed consent was obtained for all participants. Calculated a priori, a sample size of 10 would achieve 80% power to detect a mean of paired difference of 5.0% in GLS with an estimated standard deviation of difference of 5.0% with a significance level α of .05 using a 2-sided paired t test.
Study Population
Potential subjects undergoing elective, outpatient endoscopy procedures were approached for consent. Exclusion criteria were contraindications to transthoracic echocardiography (TTE), age less than 18 years, patients unable to consent, body mass index greater than 40 kg/m2, non-English speaking (due to lack of funding for interpreter services), cognitive impairment, or hemodynamic instability (heart rate >100 or <60 bpm [beats per minute], mean arterial pressure [MAP] <65 mm Hg, or hypoxemia as defined by pulse oximetry <90%).
Transthoracic Echocardiography
All the images were obtained using a commercially available ultrasound system (EPIQ CVxi, Philips Medical Systems) and a 1.5-MHz X-5 TTE Transducer. One of 2 advanced Focus Assessed Transthoracic Echocardiography (FATE)-certified cardiothoracic anesthesiologists performed a limited echocardiogram in the preoperative area. The echocardiographers were separate from the primary anesthesia team. Apical 4-chamber, 2-chamber, and 3-chamber views were obtained as well as a 4-beat, full-volume 3D acquisition of the LV. Patients were then taken to the procedure room and anesthesia was induced using propofol while maintaining spontaneous ventilation. Additional medications that were administered were patient specific (Table 1). No opioids were administered. During the pre- and post-examinations, all patients were in the left lateral decubitus position as is typical for endoscopic procedures. Immediately after loss of consciousness, as defined by the primary anesthesia team obtaining a loss of eyelash reflex, a second echocardiogram was performed by the same examiner acquiring the same set of views. The examination was completed after loss of consciousness and prior to the start of the endoscopic procedure and was limited to 2 minutes duration. The images were digitally saved for post-procedural processing in Digital Imaging and Communications in Medicine format (National Electrical Manufacturers Association).
Subject and Anesthesia Management Details a .
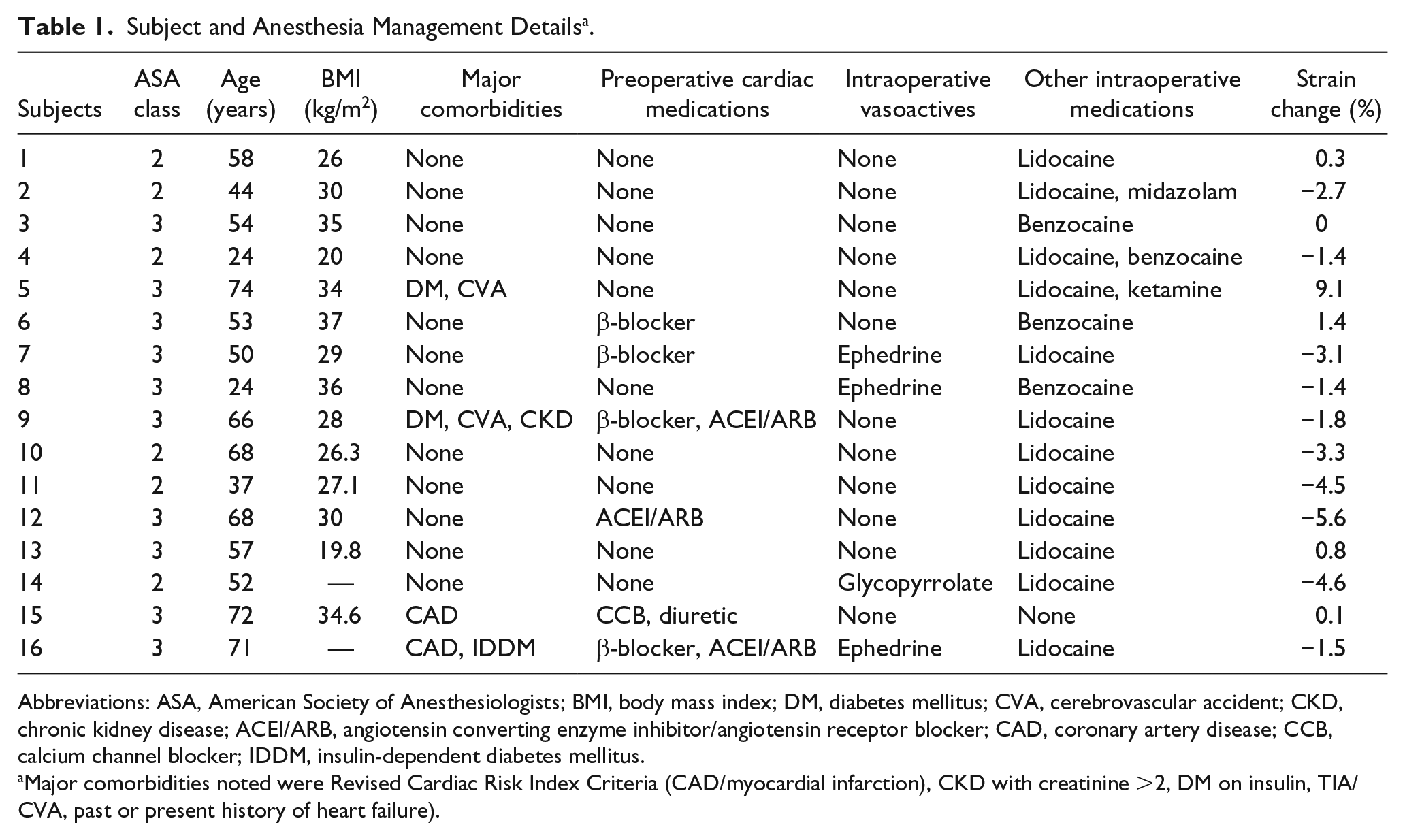
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; DM, diabetes mellitus; CVA, cerebrovascular accident; CKD, chronic kidney disease; ACEI/ARB, angiotensin converting enzyme inhibitor/angiotensin receptor blocker; CAD, coronary artery disease; CCB, calcium channel blocker; IDDM, insulin-dependent diabetes mellitus.
Major comorbidities noted were Revised Cardiac Risk Index Criteria (CAD/myocardial infarction), CKD with creatinine >2, DM on insulin, TIA/CVA, past or present history of heart failure).
Post-Processing Measurements
Post-procedural processing was completed by the same 2 anesthesiologists who performed the examinations. Using Simpson’s biplane summation of discs measurement, 2-dimensional (2D) EF, end-diastolic volume (EDV), and end-systolic volume (ESV) were determined. Three-dimensional EF, EDV, and ESV measurements were obtained from the 3D data set with commercially available software (3DQ_Advanced, Philips Medical Systems). GLS was determined using semi-automated analysis with commercially available software (AutoSTRAIN LV, Phillips Medical Systems) from the apical images. Both echocardiographers adjusted the automated calculations as appropriate to optimize measurement accuracy.
Statistical Analysis
A paired sample Student’s t test was used to assess the primary outcome of changes in GLS after propofol administration (Table 2). Additionally, changes in MAP, heart rate, 2D EF, 2D EDV, 2D ESV, 3D EF, 3D EDV, and 3D ESV were also assessed via paired sample t test. A P value less than .05 was a priori considered statistically significant. A linear regression analysis was performed to determine if the weight-based dose of propofol (mg/kg) correlated with the observed change in each variable. A correlation coefficient was obtained for the change in strain and weight-based propofol dose. Normal distribution for use of parametric statistical tests was not performed due to the small sample size and given that parametric tests are robust to slight departures from the normality assumption.
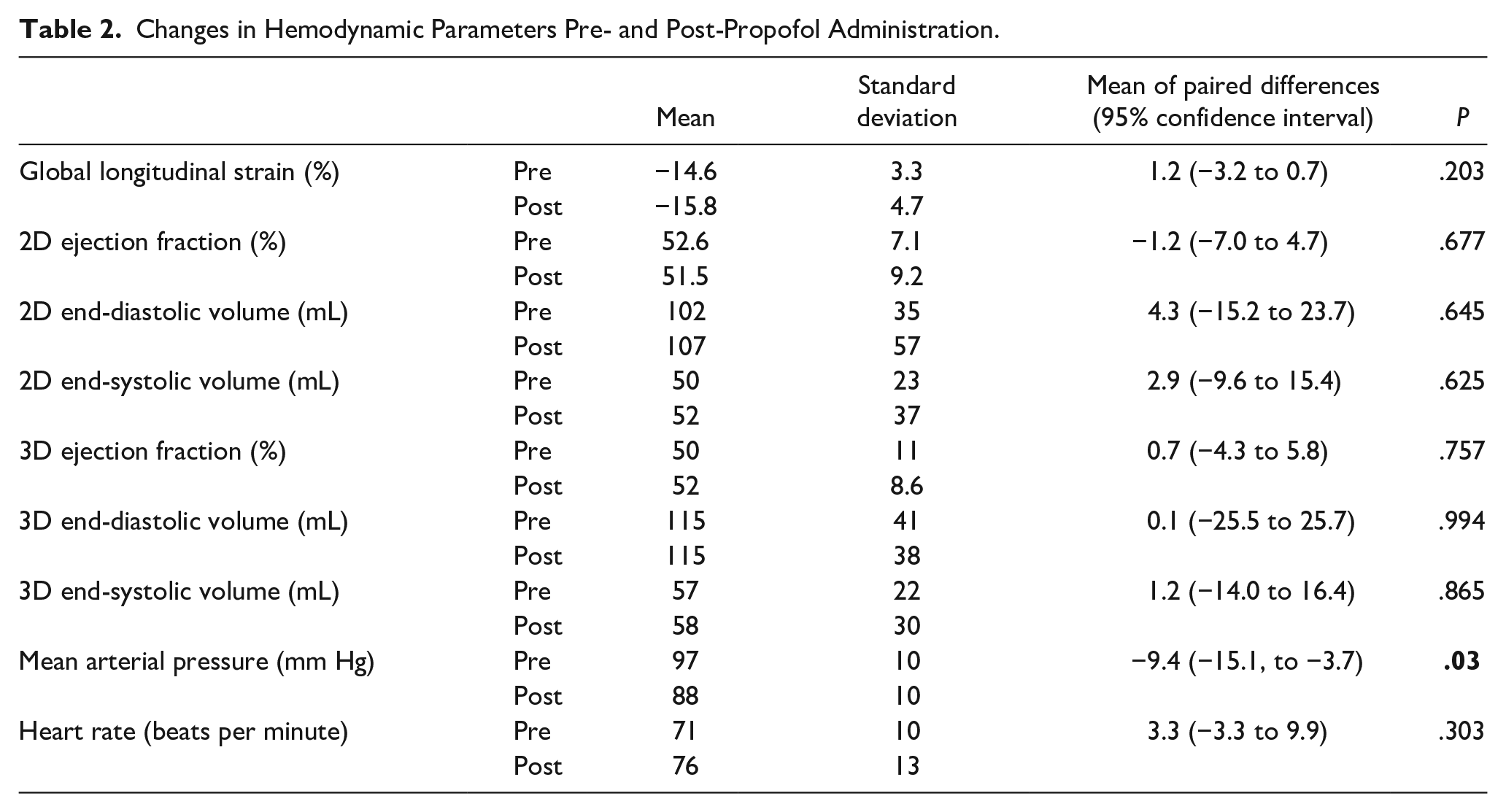
Changes in Hemodynamic Parameters Pre- and Post-Propofol Administration.
Results
Sixteen patients were included in this study. GLS became more negative (pre −14.6% standard deviation (±) 3.3%, post −15.8% ± 4.7%), although this was not statistically significant (P = .20). EF (pre 52.6% ± 7.1%, post 51.5% ± 9.2%), EDV (pre 102 ± 35 mL, post 107 ± 57 mL), and ESV (pre 50 ± 23 mL, post 52 ± 37 mL) measured by 2D also did not change (P = .67, P = .64, P = .62, respectively). There were also no significant differences in EF (pre 50% ± 11%, post 52% ± 8.6%), EDV (pre 115 mL ± 41 mL, post 115 ± 38 mL), and ESV (pre 57 ± 22 mL, post 58 ± 30 mL) by 3D (P = .75, P = .99, P = .86, respectively). The MAP did decrease significantly (pre 97 ± 10 mm Hg, post 88 ± 10 mmHg; P = .003), but heart rate did not change significantly (pre 71 ± 10 bpm, post 75 ± 13 bpm; P = .30).
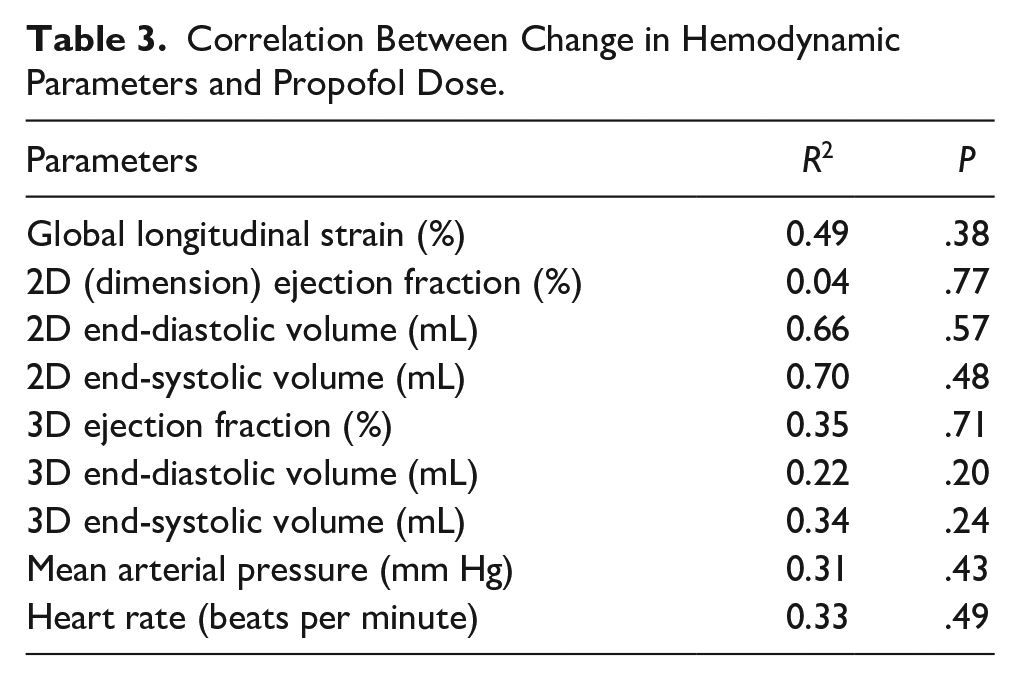
The linear regression analysis showed that the weight-based propofol dose did not significantly correlate with the changes observed in any variable (Table 3). The mean weight-based propofol dose was 1.14 mg/kg with a standard deviation of 0.4 mg/kg. Weight-based propofol dose did not correlate with change in strain with R2 0.0602 (Figure 1). Here, R2 denotes the strength of linear relationship between propofol dose and change in strain. Of note, no patients were excluded due to hemodynamic instability as defined by fluctuations of heart rate and MAP >10%. Vasopressors were not frequently used (Table 1).
Correlation Between Change in Hemodynamic Parameters and Propofol Dose.
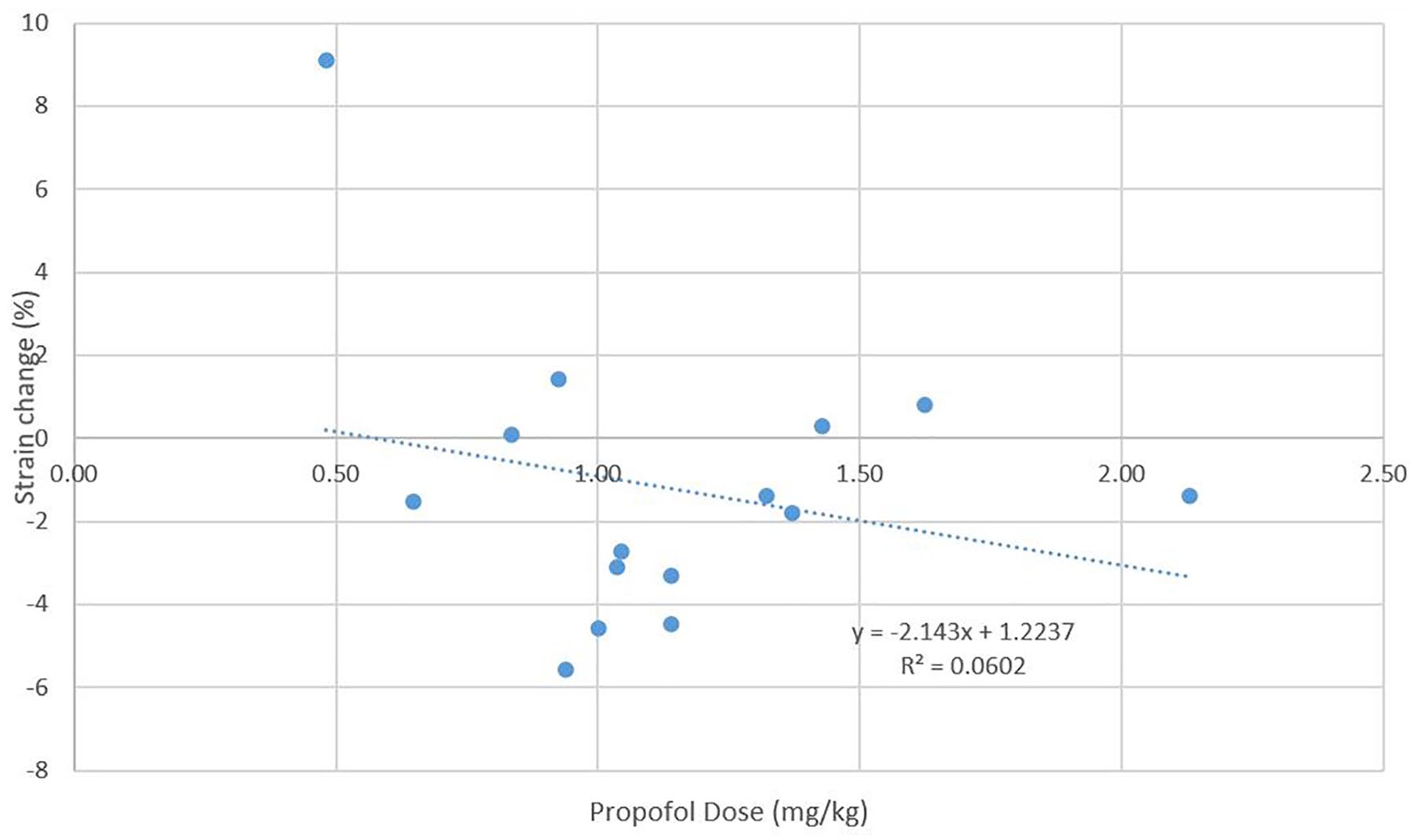
Strain change (%) as a function of propofol dose (mg/kg). Correlation coefficient, R2 0.0602.
Discussion
Our results indicate that low-dose propofol for sedation of spontaneously ventilating patients is unlikely to be a direct myocardial depressant. This counters previous work, which suggests propofol is a direct myocardial depressant.2,3,12-15 The combination of decreased MAP and unchanged GLS would suggest that this decrease in MAP may be solely due to a decrease in systemic vascular resistance. This theory does, in fact, agree with the findings of previous authors.4,9-11 Of note, the average MAP of the patients in this study was higher than the general population (97 mm Hg pre-propofol and 88 mm Hg post-propofol). We also found that heart rate did not increase in our patients despite a significant decrease in MAP. This may be due to 25% of our study population being on β-blocker therapy or due to propofol attenuating the normal baroreceptor reflex as has been found in prior studies. 19
These findings are clinically relevant in the treatment of propofol-induced hypotension. Based on our results, hypotension after low-dose propofol in normal to mildly reduced EF patients may be solely due to vasodilation and not negative inotropy. Therefore, for isolated low-dose propofol-induced hypotension, we would recommend treatment with intravenous fluids and vasopressors prior to inotropic support in healthy patients with normal to mildly reduced baseline ventricular function. Avoiding the use of vasopressors and inotropes when they are not necessary can eliminate potential adverse effects such as arrhythmias, splanchnic hypoperfusion, and lactic acid production. 20 Given the fact that venous dilation has been shown to occur at smaller propofol doses than arterial dilation, perhaps intravenous fluids should be preferred to vasopressors. 6 This information may also alter the anesthesiologist’s choice of medication for sedation in endoscopic procedures. In particular, propofol may be a better choice for patients with poor LV function because it is not a myocardial depressant as ketamine has shown to be. 21 Etomidate can cause adrenal suppression, which can be significantly detrimental in patients with reduced cardiac function despite its reported cardiovascular stability. 22 However, since we did not include such patients in our population, additional studies are needed to examine this further.
Our findings differ from prior studies. One possible reason is that we reduced some potential confounding factors. Prior studies with general anesthetic doses of propofol have found reduced cardiac function.12,15 However, positive pressure ventilation was used in those studies, which is known to decrease LV preload causing a decrease in cardiac output 23 and has also been shown to decrease myocardial contractility. 24 Perhaps, the findings are a result of positive pressure ventilation and not higher doses of propofol. However, it is possible the lower doses of propofol (mean weight-based dose of 1.14 mg/kg) used in our study explain the difference observed. Additionally, we used LV GLS as our measurement of myocardial contractility. Of the 3 forms of strain, longitudinal, radial, and circumferential, we measured longitudinal because the above mentioned “normal” values have only been referenced for longitudinal strain acquired from TTE. 17 GLS is a sensitive assessment of systolic function that can be useful in evaluating myocardial depression. 25 Semi-automated strain has been shown to be feasible, reproducible within a given software platform, 26 and correlates well with MRI measurements of EF. 16 Therefore, GLS should have the power to elucidate more subtle changes in systolic function; however, our study found no change. Last, we largely avoided concomitant medication administration. Patients in prior studies received medications such as benzodiazepines10,15 or morphine 13 that could alter myocardial function via direct action or a synergistic effect with propofol. In both human and rat models, opioids have shown to cause myocardial depression.27,28 Benzodiazepines also cause decreased myocardial contractility. 29
Our study had several limitations. A standardized weight-based dose of propofol was not used. The lack of standardization creates a possible confounding variable. Also, we used low-dose propofol to maintain spontaneous ventilation, which may hinder the ability to detect a dose-dependent effect. Another limitation is the sample size of 16 patients. A larger sample size would increase the ability to detect a more subtle difference in GLS or EF. The potential variability in image acquisition and post-processing calculations should also be discussed. Although the examiners are board certified in advanced perioperative transesophageal echocardiography and well-experienced in TTE, neither was blinded during the studies nor post-processing measurements. Inter- and intraobserver variability was not accounted for in the image acquisition nor the image analysis. However, we believe the semi-automated nature of GLS measurement mitigates some of this potential bias. Measurement of GLS can be affected in a few different ways. Irregular heart rates or rhythms, age, sex, and LV loading conditions can alter the calculation.17,30 None of these factors were considered in the statistical analysis due to the small sample size of the study. GLS measures frequently vary by software platform, which may limit comparison to absolute values of other platforms. 17 However, we used the same software throughout our study, which creates reliable and reproducible results. 30 Last, reliable TTE imaging and GLS measurements depend on a series of hemodynamic snapshots. Since image acquisition was limited to 2 time points, there may be changes over time that went undetected.
Our results yielded potentially clinically relevant implications and also encourages further investigation. A larger sample size could allow for comparisons among groups such as normal EF and low EF patients, as these groups may have a different physiologic response. Additionally, measurement of strain at standardized, incrementally increasing propofol doses could be performed to determine a dose-response curve. Finally, replicating this protocol with other common anesthetic agents such as etomidate and ketamine could help elucidate optimal sedation for patients to minimize direct myocardial depression.
Conclusion
This pilot study was conducted to ascertain the effects of propofol on myocardial function. We found that low-dose propofol for sedation of spontaneously ventilating patients with normal or mildly reduced LV ejection fraction did not cause a reduction in systolic function as measured by GLS, a sensitive measure of myocardial contractility. Therefore, decreases in blood pressure after a propofol bolus in spontaneously breathing patients are likely due to decreased vascular tone and not impaired LV systolic function. These results should be considered in the selection of anesthetic agents for these patients and the management of low-dose propofol-induced hypotension, though further investigation is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.