
Abstract
This review focuses on the literature published during the calendar year 2021 that is of interest to anesthesiologists taking care of children and adults with congenital heart disease. Four major themes are discussed, including cardiovascular disease in children with COVID-19, aortic valve repair and replacement, bleeding and coagulation, and enhanced recovery after surgery (ERAS).
Keywords
Introduction
The 2021 literature was searched via the US National Library of Medicine PubMed database using the terms congenital heart disease (CHD), anesthesia, cardiac surgery, cardiopulmonary bypass (CPB), pediatric cardiology, adult congenital heart disease, coagulation, and COVID-19. From the resulting articles, we chose 4 prominent themes to highlight: cardiovascular disease in children with COVID-19, aortic valve repair and replacement, bleeding and coagulation, and enhanced recovery after surgery (ERAS). This review will highlight relevant research in these areas.
COVID-19 and Cardiovascular Disease in Children
The effects of COVID-19 and COVID-19 vaccines on the cardiovascular system
The SARS-CoV-2 virus is unusual among coronaviruses in its frequent association with cardiovascular and thromboembolic complications. (Table 1) The virus may damage myocardial and vascular cells either directly or as a secondary effect of a maladaptive hyperinflammatory immune response. Cardiovascular damage from COVID-19 is relatively common in adults of all ages and elevated cardiac enzymes have been demonstrated in up to 20% of hospitalized adults with COVID-19. 1 In children, infection with SARS-CoV-2 can also result in a post-infectious Multisystem Inflammatory Syndrome in Children (MIS-C) which typically presents 2–6 weeks after initial infection. MIS-C shares many features with severe acute COVID-19 and can present with ventricular dysfunction, coronary aneurysms, and cardiovascular shock along with other non-cardiovascular manifestations. Feldstein et al evaluated the characteristics and outcomes in children and adolescents with MIS-C and severe acute COVID-19. Compared to children with severe acute COVID-19, children with MIS-C were younger, more likely to be non-Hispanic black, and more likely to have cardiorespiratory (56 vs 8.8%) or cardiovascular without respiratory involvement (10.6 vs 2.9%). Children with severe acute COVID-19 were more likely to have respiratory without cardiac involvement. Forty-five percent of patients with MIS-C vs 9% of patients with severe acute COVID-19 required vasopressor support. Mortality rate was similar; 1.9% of the children with MIS-C and 1.4% of the children with severe acute COVID-19 died during the hospitalization. Of the children with MIS-C with reduced ventricular function (34%) and coronary aneurysms (13.4%), 91 and 79.1%, respectively, normalized within 30 days. 2
Key 2021 Articles on COVID-19 and Heart Disease.
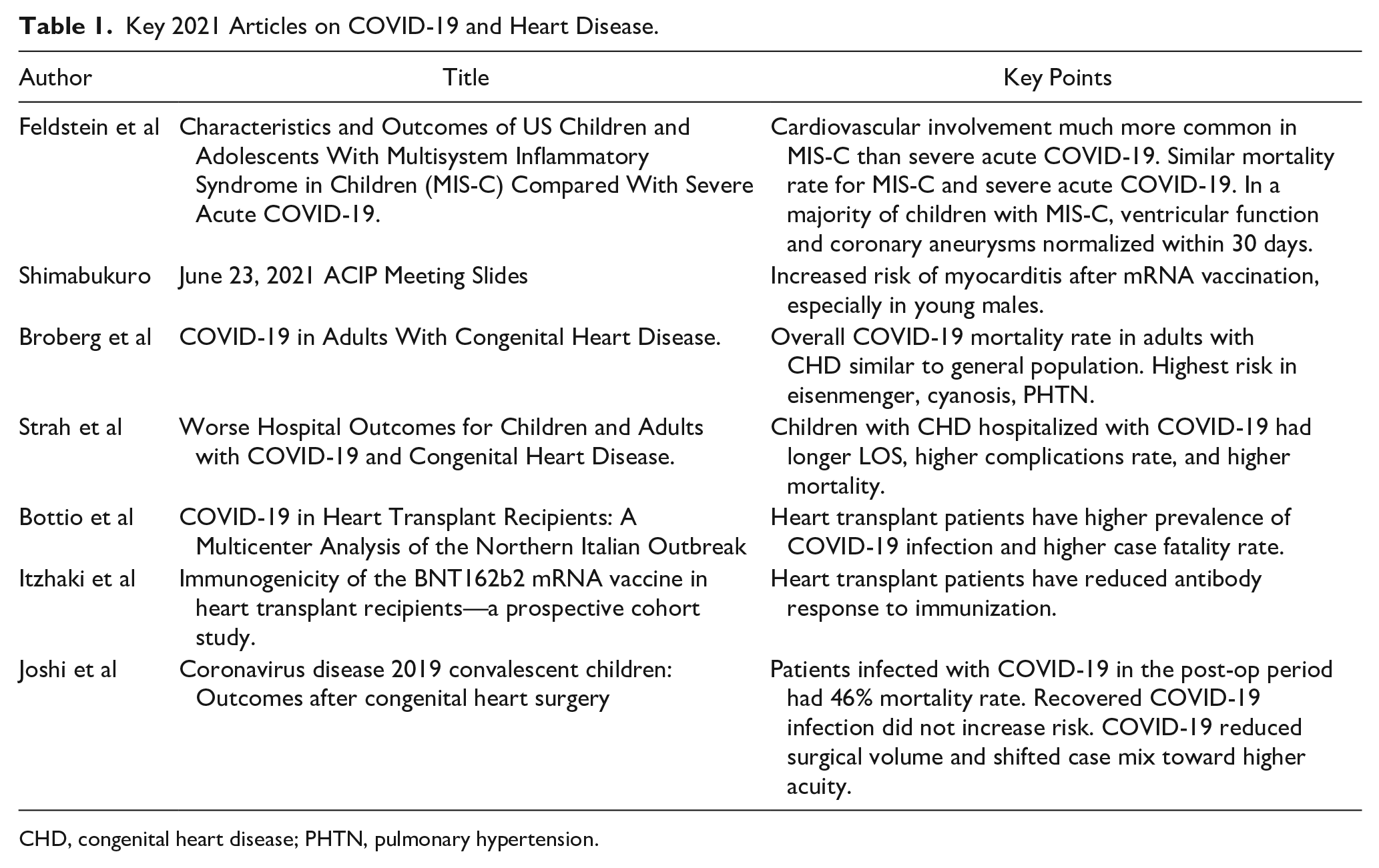
CHD, congenital heart disease; PHTN, pulmonary hypertension.
Although vaccination has dramatically reduced the risk of morbidity and mortality from COVID-19, mRNA vaccines have been shown to be associated with cardiovascular complications in certain groups of patients. Utilizing safety data generated by the Vaccine Adverse Event Reporting System (VAERS) for vaccine doses administered prior to June 11, 2021, the Advisory Committee on Immunization Practices (ACIP) found 1,226 reports of myocarditis, most occurring 2–3 days after the second vaccine dose. Overall, the rate of reported myocarditis was 18.1 per million doses in 12–17 year olds and 15.9 for 18–24 year olds with a dramatically higher reporting rate in young males vs young females. 3 (Table 2) Other sources have confirmed these preliminary findings. The United States military reported an incidence of 8.2 cases of myocarditis per 100,000 male service members and an Israeli study utilizing a large national data set demonstrated an average of 2.7 cases of myocarditis per 100,000 vaccinated patients overall.4,5
Myocarditis/Pericarditis risk following mRNA COVID-19 Vaccination.
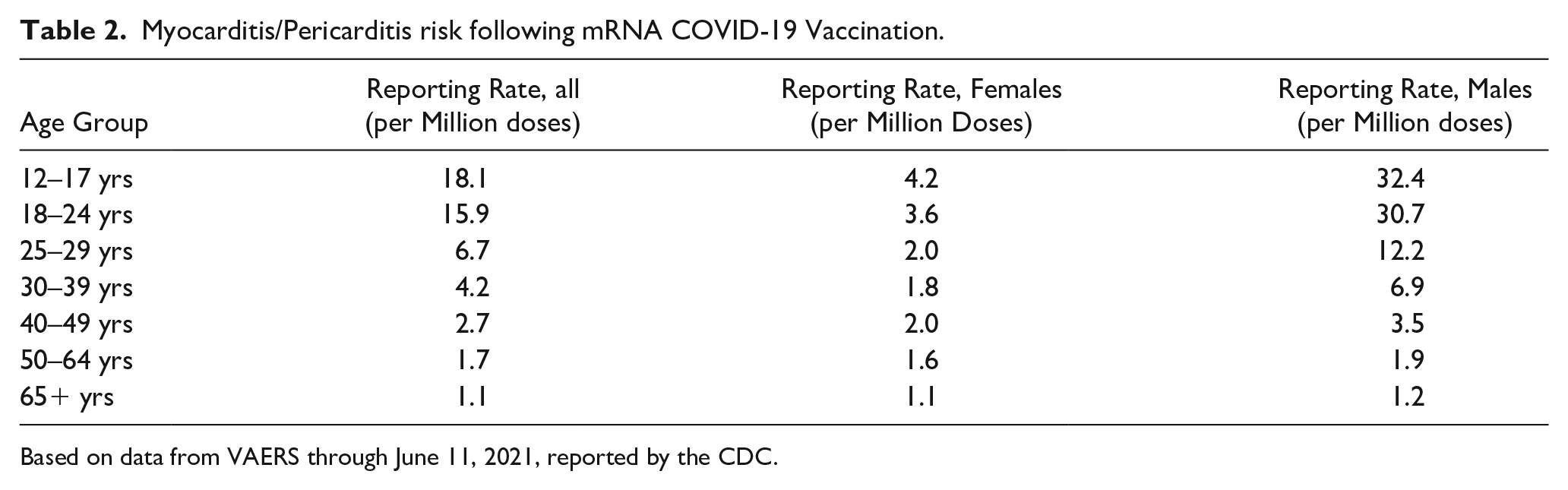
Based on data from VAERS through June 11, 2021, reported by the CDC.
Unlike the cardiovascular manifestations of COVID-19, vaccine-related myocarditis is generally benign and self-limited. Thus, comparison of the rates of complications and associated morbidity of vaccination vs COVID-19 infection clearly favors universal vaccination in teenagers and young adults. 1
COVID-19 in Congenital Heart Disease
As baseline hypertension and cardiovascular disease are thought to play a role in COVID-19 related cardiac complications, pediatric and adult patients with congenital heart disease (CHD) may be at increased risk of morbidity and mortality. In a large study from 58 international adult CHD centers including patients with various type of CHD, Broberg et al found a COVID-19 case fatality rate of 2.3%, similar to the cumulative case fatality rate across all global populations. Male sex, diabetes, cyanosis, pulmonary hypertension, renal disease, heart failure, and higher physiologic disease stage were associated with increased risk of mortality in this population, whereas anatomic complexity, type of defect, systemic ventricular dysfunction, and systemic hypertension were not. The highest risk of mortality was observed in patients with Eisenmenger physiology (13%), cyanosis (12%), and pulmonary hypertension (10%). 6
In a database study from the United States, Strah et al demonstrated that children with CHD are at higher risk of COVID-19 complications than healthy children. In their cohort of nearly 10,000 children hospitalized with COVID-19, children with CHD had a longer length of stay (22 vs 6 days), higher complication rate (6.9% vs 1.1%), and higher mortality (3.8% vs .8%). 7
COVID-19 in Heart Transplant Patients
Patients who have undergone heart transplantation represent a particularly high-risk group for complications from COVID-19 infection due to their comorbidities and immunosuppression. In one study conducted by Bottio et al 8 during the height of the pandemic in Northern Italy before the introduction of vaccines, heart transplant patients had both a higher prevalence of infection (18 vs 7 cases per 1,000) and higher case fatality rate (29.7 vs 15.4%) compared to the general population.
Ideally, the availability of effective vaccines should substantially decrease the risk of mortality, but unfortunately there is significant evidence that transplant patients mount a suboptimal response to vaccination. Itzhaki et al studied the antibody response to vaccination in 42 heart transplant patients who received the Pfizer vaccine. They demonstrated that only 15% of patients had positive antibody titers after the first dose and only 49% had positive titers in response to the 2-dose vaccination series. Anti-metabolite immunosuppression (mycophenolate mofetil) was associated with decreased immunogenic response to vaccination. 9 However, there is emerging evidence that a third vaccine dose enhances the immunogenic response in solid organ transplant recipients and may help improve outcomes in this vulnerable group. 10
COVID-19 in Heart Surgery
The COVID-19 Pandemic has had a profound effect on hospital resource utilization and surgical case volumes around the world. Joshi et al conducted a survey of congenital heart surgery programs in Brazil and found that nearly all centers experienced decreased surgical volume with over 70% of programs reporting significantly decreased volume, resulting in a shift in case mix toward more complex surgery with an associated increase in mortality rates. The authors also evaluated the impact of preoperative and postoperative COVID-19 infection on surgical outcomes. They found that children who have previously recovered from COVID-19 had no higher rate of adverse surgical outcomes than children without recent COVID-19 infection; however, in patients who were infected with COVID-19 in the postoperative period, the mortality rate was 46%. 11 (Table 2)
Aortic Valve Procedures
The surgical treatment of aortic valvulopathies in children and adults has recently been transformed by new and improved versions of old procedures such aortic valve repairs, the Ozaki procedure, and the Ross procedure (Table 3).
Key 2021 Articles on Aortic Valve Procedures.
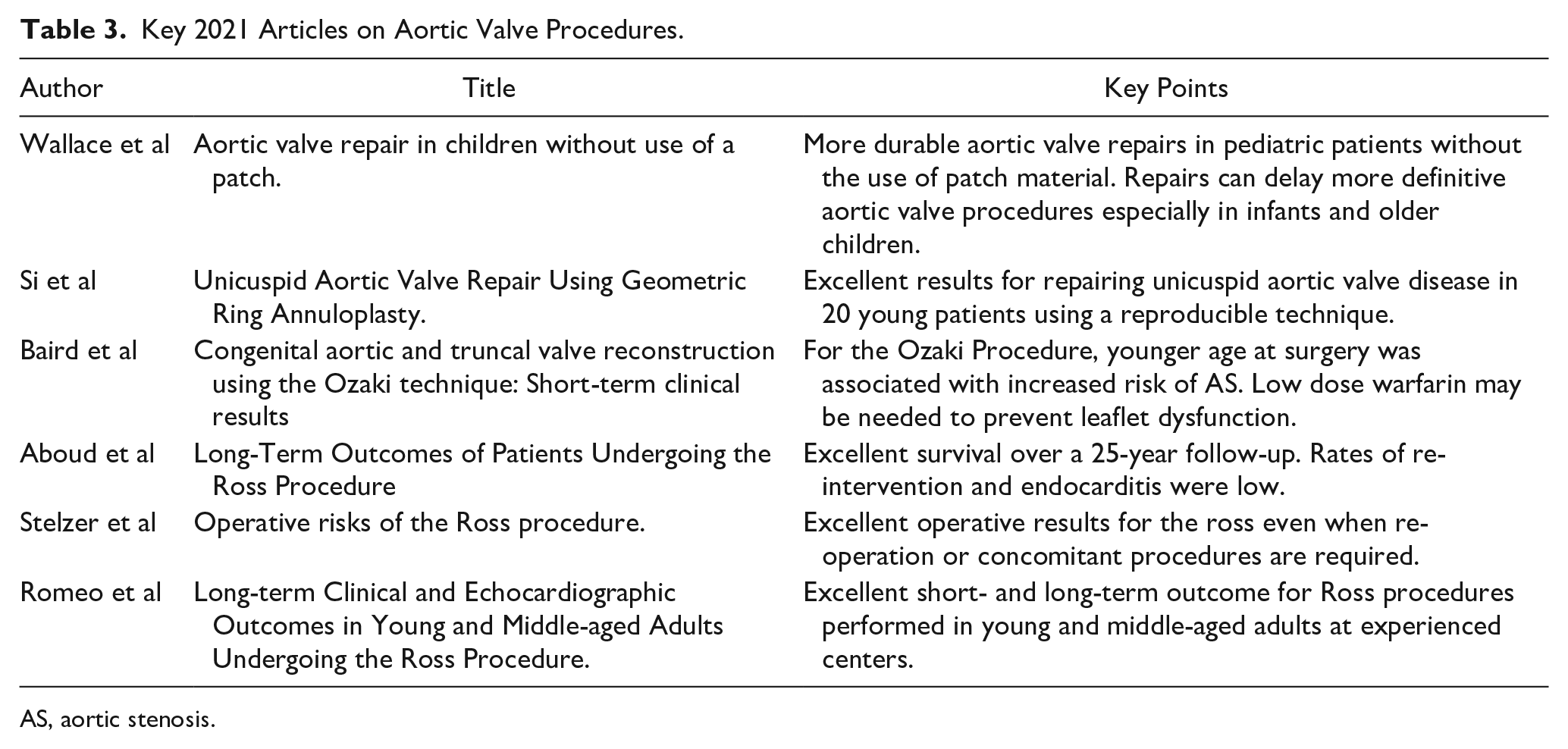
AS, aortic stenosis.
Mechanical and bioprosthetic aortic valves and aortic homografts have been used reliably for years with apparently good results. Mechanical valves have been touted as the valve of choice in pediatric patients whenever possible because of their durability, but long-term data demonstrates that these valves are associated with decreased long-term survival and increased morbidity.12,13 Mechanical aortic valve replacement in young patients has a major impact on the duration and quality of life. Patients fall off their expected survival curves within 10–17 years of surgery compared to their peers due to complications of additional cardiac operations, endocarditis, valve thrombosis, and anticoagulation.12,14,15 (Table 4)
Comparison Between Aortic Valve Replacement Options.
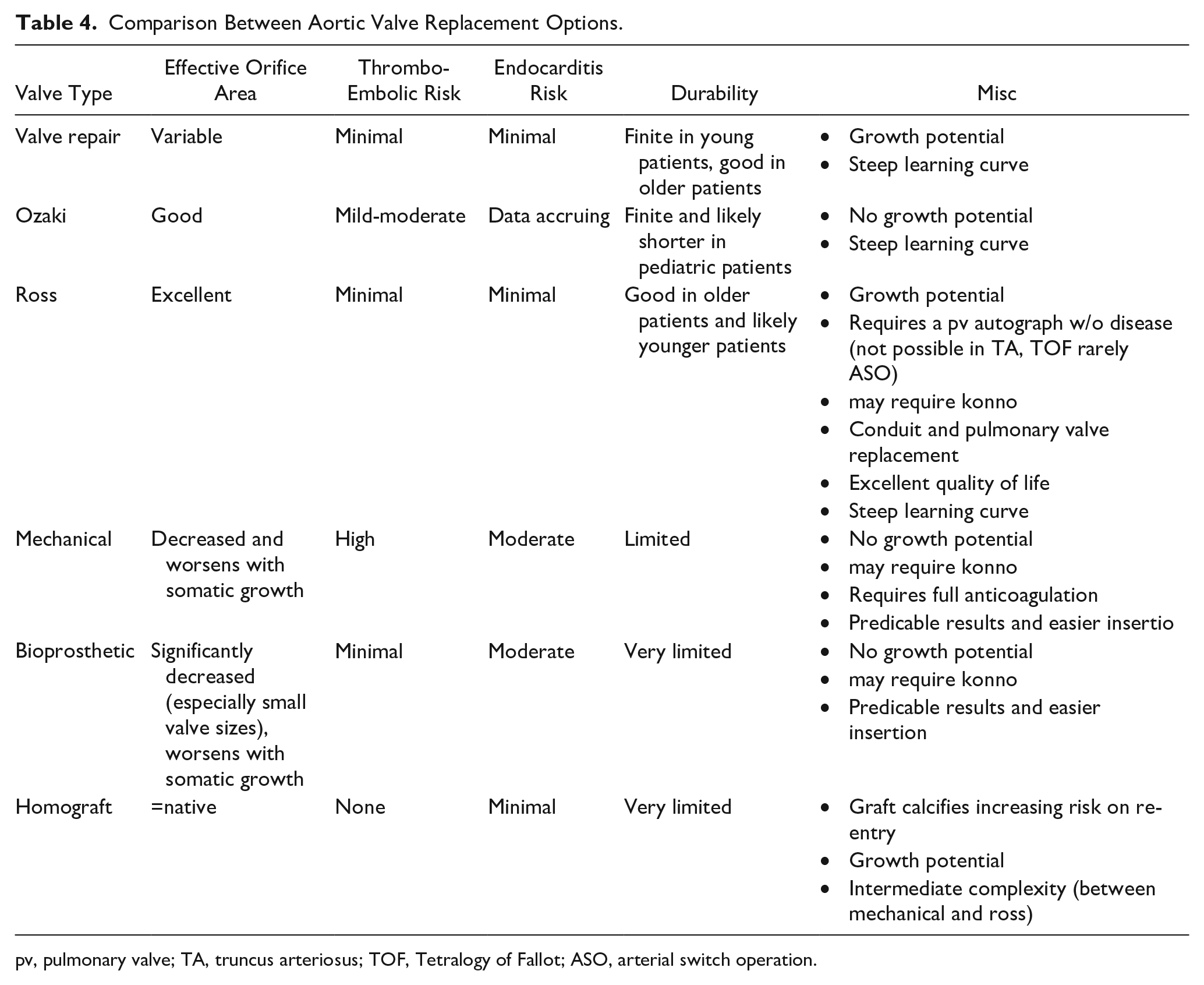
pv, pulmonary valve; TA, truncus arteriosus; TOF, Tetralogy of Fallot; ASO, arterial switch operation.
Aortic Valve Repair
Aortic valve repair theoretically offers an ideal solution for pediatric patients. However, despite acceptable early results, long-term results have historically been less promising with some series reporting a reoperation rate as high as 46% at 7.5 years. 16 A group in Melbourne recently demonstrated improved long-term results for aortic valve repair in 102 patients including 25 neonates and 17 infants. Only 47% of those operated on as neonates and 40% of those operated on as infants or older children required a second aortic valve procedure (usually a Ross) at 15 years. Neonatal survival was 98% at 10 years and survival for the entire cohort was 95% at 15 years. 17 The authors recommend initial surgical repair over transcatheter procedures in very young patients because the valve is less likely to be repairable after balloon dilation, and surgical repair has been shown to delay the need for subsequent intervention compared to balloon valvuloplasty. 18 Importantly, re-operative surgery was delayed for 7 years even in patients with only suboptimal repair. This surgical approach is reminiscent of the treatment strategies employed for mitral valve disease in pediatric patients.
In adolescents and young adults, aortic valve repair techniques with or without root replacement are now being performed routinely in patients with aortic insufficiency (AI) secondary to unicuspid and bicuspid valve disease with excellent early and late results.19,20
Ozaki Procedure
The Ozaki procedure uses a template to create a neoaortic valve from bovine pericardium or glutaraldehyde treated autologous pericardium which is then sewn to the native aortic root, maximizing the effective orifice area. Baird et al report on short-term results with this procedure in 57 patients aged .7-25 years, with a mean age of 12 years. They reported an 88% freedom from moderate or greater AI or aortic stenosis (AS) at 2 years and 91% freedom from reoperation at 1.5 years. Notably, the 4 patients with post op moderate AS all had their procedures at a younger age compared to those without AS. 21 Ozaki recently reported on 850 adult patients. There was 96% freedom from reoperation and 93% freedom from moderate or greater AI at a mean follow up of 53 months. 22 However, there are concerns about performing this procedure in pediatric patients as there is no growth potential of the leaflets, and valve degeneration and calcification are likely similar to bioprosthetic valves. It is also important to note that this procedure may not eliminate the need for warfarin anticoagulation. There has not yet been sufficient follow up in children to endorse this procedure over a Ross or mechanical valve replacement. 23
Ross Procedure
There has been a resurgence of enthusiasm for the Ross procedure based on multiple reports of excellent short- and long-term results.13,24,25 Major concerns include the high surgical complexity and risk of degeneration of the aortic autograft and the pulmonic homograft. However, surgical improvements that limit dilation of the autograft, the use of acellular homografts, and the availability of percutaneous pulmonic valve replacement address some of these limitations. Romeo et al evaluated the long-term mortality and re-intervention data on 1431 patients between 18 and 65 years undergoing the Ross procedure in 5 experienced centers. Early post op mortality was .7%, and 10 and 15 year survival was 95.1 and 88.5%, respectively. Freedom from autograft and homograft intervention was 92 and 97%, respectively, during that time. 26
Conclusion
In summary, recent research suggests that whenever possible a valve repair is preferred over valve replacement. AI is more treatable with valve repair in older patients whereas AS in this group often requires valve replacement. In young children, an adequate result is acceptable as it delays the need for re-operative surgery. When valve repair fails or is not feasible, a Ross procedure is likely the next best option with good quality of life and similar life expectancy to that of sex- and age-matched controls for at least 15 years after surgery. The role of the Ozaki procedure is unclear at this time, but it may play a role in children with truncal valve disease where the Ross procedure is not an option.
Bleeding and Coagulopathy
Perioperative bleeding and coagulopathy remain a significant source of morbidity and mortality in congenital cardiac surgery. Data from the National Heart, Lung, and Blood Institute Recipient Epidemiology and Donor Evaluation Study-III from 2013 to 2016 show that children undergoing CBP are frequently transfused. Of 185 single ventricle patients, 81% received red blood cells (RBCs), 79% received platelets, 86% received plasma, and 56% received cryoprecipitate. Patients in this cohort were transfused at a median intraoperative hemoglobin of 13.5 g/dL. 27
Antifibrinolytic Dosing
Antifibrinolytic medications such as tranexamic acid (TXA) and aminocaproic acid have become mainstays in cardiac surgery. Despite their widespread use, there remains considerable dosing heterogeneity in pediatrics. Siemens et al evaluated the efficacy of high-dose (>50 mg/kg cumulative) and low-dose (<50 mg/kg cumulative) TXA regimens in a systematic review and meta-analysis of 12 randomized controlled trials. While there was a larger decrease in postoperative blood loss in the higher dose group (10 vs 5.4 mL/kg), the reduction was not statistically significant. Both dosing strategies led to a reduction in RBC and FFP transfusion compared with placebo. There was also no difference is transfusion between patients who received continuous vs bolus dosing. 28 A review by Hovgesen et al 29 of 50 studies evaluating the efficacy of different TXA doses across all pediatric surgical disciplines also demonstrated efficacy of lower dose TXA. This research supports the use of the lowest efficacious dose of TXA and highlights the need for development of a standardized dosing regimen in pediatrics.
Viscoelastic Testing
Pediatric patients, particularly neonates and young infants, frequently receive empiric transfusion of blood products after separation from bypass. Point of care viscoelastic testing using thromboelastography (TEG) or rotational thromboelastography (ROTEM) has shown promise in decreasing unnecessary transfusion of blood products by providing qualitative information regarding clot formation and stability. 30 While these tests can help distinguish between coagulopathy and inadequate surgical hemostasis, the tests take up to 30–45 minutes to complete, and the results may lag behind the need to make immediate clinical decisions. Visual assessment of the surgical field is often used to guide initial transfusion decisions, but visual inspection may not reliably distinguish between surgical and coagulopathic bleeding and may lead to excessive and inappropriate transfusion. In a prospective blinded study, Restin et al examined the ability of surgeons to distinguish between coagulopathic and surgical bleeding using a clinical intraoperative bleeding score. In their cohort of 49 patients, bleeding was scored numerically by the surgeon every hour and compared with simultaneous ROTEM measurements. Severe bleeding (score 5–8) was seen at 24 time points and correlated to abnormal ROTEM values only 58.3% of the time. Transfusion based on the visual bleeding score in this study would have resulted in a 1.7-fold increase in blood product administration. 31 In a single center retrospective study of 537 surgical patients, Emani and colleagues evaluated whether early TEG testing could predict post-bypass bleeding. They found good correlation (r = .76) between rewarming and post-protamine values of maximum amplitude (MA), a marker of platelet function and fibrinogen concentration. They also demonstrated that a rewarming MA of less than 45 mm compared to an MA of 45 mm or more was associated with a 38 vs 22% incidence of attaining the composite bleeding outcome (blood product transfusion, recombinant factor VIIa use, and surgical re-exploration). 32
In addition to TEG and ROTEM, preoperative multiple impedance platelet aggregometry (Multiplate) has shown promise in predicting platelet transfusion requirements in adults undergoing cardiac surgery. Multiple studies this year investigated the role of Multiplate in pediatric cardiac surgery. Harris et al examined whether Multiplate testing preoperatively could predict bleeding in a retrospective single center cohort of 225 patients. While there was a statistically significant improvement in their predictive model using preoperative testing in combination with clinical characteristics, this translated to an increase in identification of only .9% of children at risk for bleeding intraoperatively and only .4% postoperatively. 33 Di Gregorio investigated the use of Multiplate in a retrospective case-controlled study of 31 children and found that the platelet function tests were not significantly different between bleeders and non-bleeders. 34 Dieu et al 35 investigated the use of Multiplate as a POC test post-CPB as compared to ROTEM and found no significant difference between the tests in predicting which patients required a platelet transfusion but did find an association between platelet transfusion and maximum clot firmness (MCF) (regression coefficient = −.348 [95% confidence interval −1.006 to −.028]; P = .039).
Current guidelines from the Pediatric Critical Care Transfusion and Anemia Expertise Initiative (TAXI), Pediatric Critical Care Blood Research Network (BloodNet), and Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) make a weak recommendation to use viscoelastic testing in the intraoperative and postoperative periods to guide platelet and plasma transfusion (grade 2B). The group also recommended standardization of bleeding endpoints in future studies to allow for more robust meta-analysis and comparison between studies. 36 (Table 5)
Key 2021 Articles on Bleeding and Coagulopathy.
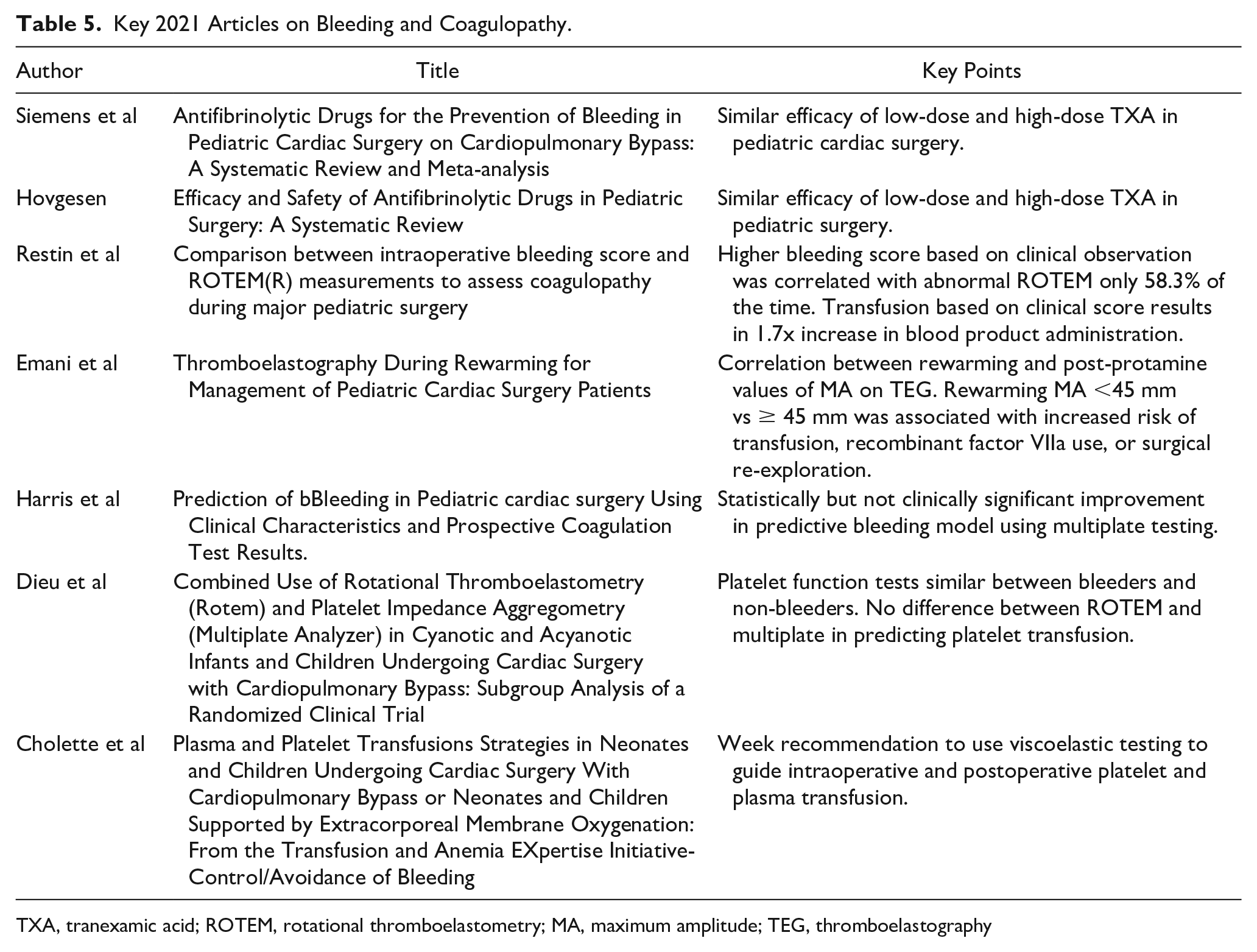
TXA, tranexamic acid; ROTEM, rotational thromboelastometry; MA, maximum amplitude; TEG, thromboelastography
Enhanced Recovery After Pediatric Cardiac Surgery
Enhanced recovery after surgery (ERAS) programs are multidisciplinary, multimodal perioperative pathways which aim to expedite the patient’s return to baseline after surgery. 37 Improved outcomes have been demonstrated for numerous adult and pediatric surgeries, including pediatric cardiac surgery. (Table 6)
Key 2021 Articles on ERAS in Cardiac Surgery.
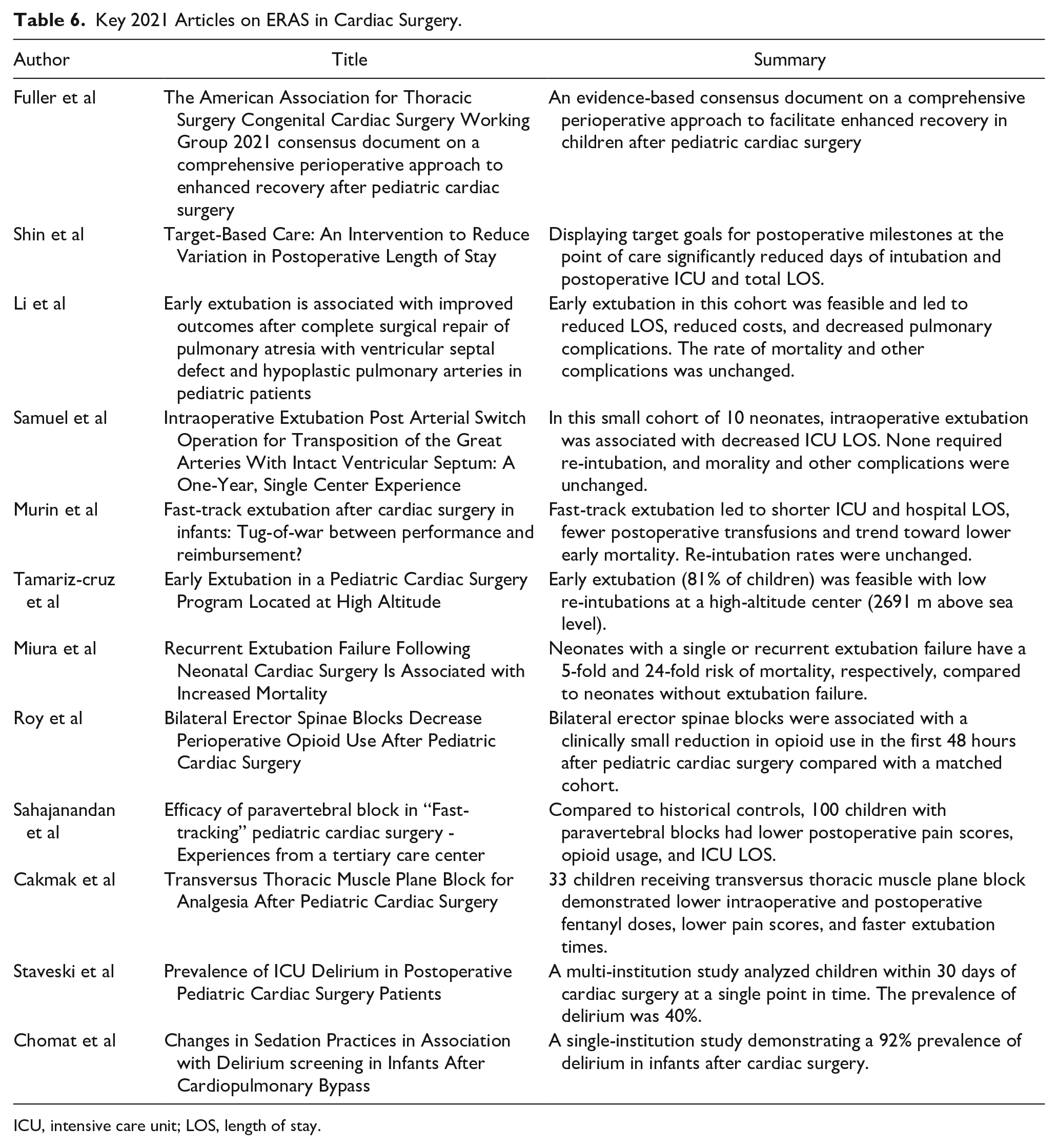
ICU, intensive care unit; LOS, length of stay.
In 2021, the American Association for Thoracic Surgery (AATS) Congenital Cardiac Surgery Working Group published a consensus document on a comprehensive perioperative approach to enhanced recovery after pediatric cardiac surgery. Based on published data and expert opinion, the working group proffered 29 recommendations to facilitate enhanced recovery after pediatric cardiac surgery. The authors emphasize that ERAS programs require careful and strategic multidisciplinary planning and must be tailored to the individual institution. Once integrated, it is critical to have a quality assurance infrastructure to regularly evaluate and fine-tune each subcomponent of the ERAS program based on outcomes. Another point of emphasis, considering the high acuity and mortality inherent to congenital heart disease, is that the ERAS pathway will require modifications for individual children with mitigating risk factors (e.g.,, open chest, residual lesions, and pulmonary hypertension) or when inadequate staffing or available clinical expertise would jeopardize safety. The guidelines highly recommend immediate or early extubation as a component of ERAS in select patients and highly recommend application of protocol-based multimodal analgesia with limited intraoperative use of respiratory depressants. The authors recommend postoperative delirium screening and sedative/analgesic strategies that limit delirium. Lastly, the guidelines state that peripheral regional anesthesia or neuraxial anesthesia may be an effective opioid-sparing analgesic modality. 38
Target-Based Care
Shin et al instituted a target-based care intervention for ten different congenital heart surgeries. Targets of expected time to extubation, intensive care unit (ICU) length of stay (LOS), acute care LOS, and hospital LOS for each child were visibly displayed at bedside. This simple intervention, essentially a visible reminder of the timeline for milestone goals, markedly reduced interpatient variation between the pre- and post-intervention cohorts. Notably, children post-intervention had .7 fewer days intubated, .97 fewer ICU days, and 1.18 fewer total LOS days. 39
Early Extubation
Over the past decade, data have supported early extubation (EE) as an important component of ERAS.38,40,41 Reported benefits across studies include decreased LOS, decreased costs, and hemodynamic benefits realized with return of spontaneous ventilation and reduced sedation. In 2021, Li et al retrospectively analyzed 113 children undergoing pulmonary atresia with ventricular septal defect (VSD) and hypoplastic pulmonary arteries at a mean age of 2.5 years old who were extubated early. The children were propensity matched with peers experiencing prolonged ventilation. EE was associated with a significant decrease of ICU LOS, hospital LOS, medical costs, and pulmonary complications. 42 Samuel et al reported successful intraoperative extubation of 10 consecutive neonates undergoing arterial switch operation for D-transposition of the great arteries with intact ventricular septum. These patients were compared to a control group undergoing the same procedure prior to the change in extubation practice. Neonates who were intraoperatively extubated had a shorter hospital LOS with no difference in morbidity. Importantly, none of the intraoperatively extubated neonates required re-intubation. 43
Murin et al reported the results of 182 infants <7 kg who were fast-track extubated within 8 hours of surgery. After propensity matching to pairs who were not fast-tracked, fast-track infants had shorter ICU LOS (1.8 vs 4.2 days), hospital LOS (7 vs 10 days), lower postoperative transfusion rates: 61 vs 77%, and a trend toward lower early mortality. Reintubation rates did not differ. 44 Tamariz-Cruz et al published the outcomes of EE after pediatric cardiac surgery in the relatively high altitude of Mexico City, located at 2691 m (8828 ft.) above sea level. Of their 478 children, 66% were extubated in the operating room, and an additional 15% were extubated within 24 hours after surgery. Those who were extubated early had significantly lower mortality, reintubation, infection, and both ICU and hospital LOS. Importantly, the exclusion criteria for EE in this study included weight <10 kg, age <30 days, and CPB times >90 minutes. These exclusion criteria place those at greatest risk of prolonged hospital course and postoperative complications in the non-EE group. 45 Miura et al reported that extubation failure is associated with increased mortality following neonatal cardiac surgery. Over 1000 neonates at a single institution were studied. Predicted mortality with recurrent extubation failure it was 29%, with single extubation failure it was 6.5%, and with no extubation failure it was 1.2%. Reintubation due to cardiovascular reasons was the greatest predictor of heightened mortality. 46
Although these studies suggest a benefit to EE, the retrospective, single-institution nature of these studies presents a significant risk of selection bias. For example, a hemodynamically unstable child may be kept intubated for a longer period, and any accrued morbidity or prolonged LOS may be more accurately attributed to the cardiovascular issue rather than prolonged intubation. Without proper randomized controlled trials, we are thus left with association rather than causality between EE and improved outcomes.
Regional Anesthesia
Regional anesthesia is another important subcomponent of ERAS at many institutions. Several publications in 2021 have broadened our understanding of the role of regional anesthesia in a multimodal analgesic plan. Roy et al reported a prospective cohort study of 10 children receiving a bilateral erector spinae plane block (ESPB) with catheters at the end of surgery. Children in the ESPB cohort received less opioids in the first 48 hours, but the clinical difference was small. Pain scores were also slightly higher in the ESPB cohort at half of the time intervals during the first 48 hours. 47 While 2 prior studies have demonstrated efficacy of ESPB in cohorts of 40 and 50 children, larger studies are needed to confirm the efficacy of ESPBs in pediatric cardiac surgery.48,49 Sahajanandan et al reported an analysis of 100 children under the age of 8 years receiving a paravertebral block (PVB) vs 100 historical matched controls undergoing a range of cardiac surgeries. In the PVB group, time to extubation and ICU LOS were shorter, intraoperative and postoperative opioid use was lower, and postoperative pain scores were lower. 50 Cakmak et al reported the efficacy of transversus thoracic muscle plane block (TTPB), a fascial plane block which provides analgesia of the anterior branches of the T2 to T6 intercostal nerves. Thirty-three children received a single-shot TTPB (.25 mL/kg of .25% bupivacaine bilaterally between fourth and fifth ribs) prior to sternotomy and were compared to 37 children without the block. Pain scores were significantly lower in the TTPB group despite receiving significantly lower intraoperative doses of fentanyl. The time to extubation was also significantly lower in the TTPB group than in the non-TTPB group. 51
Post-Operative Delirium
Two publications in 2021 studied the burden of delirium after pediatric cardiac surgery. Staveski et al prospectively enrolled 181 children at 27 North American cardiac ICUs, and a 1 day, point-prevalence study of delirium was conducted on all children who had undergone cardiac surgery in the past 30 days. The spot prevalence of delirium was 40%. Modifiable risk factors associated with a positive delirium screen were higher pain score at time of screen, total opioid exposure, pain medication or sedative administered in the previous 4 hours, no progressive physical therapy or ambulation schedule, and parents absent from the bedside. 52 Chomat et al 53 reported a delirium prevalence of 92% in infants after cardiac surgery, supporting prior research stating infants are at the highest risk for delirium after CPB.
Additional data are needed to guide intraoperative and postoperative multimodality analgesic and sedation regimens that limit delirium, improve LOS, and lead to increased patient and family satisfaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.