
Abstract
This year marked a number of milestones in critical care. As vaccines for the SARS-CoV-2 virus became widely available and were confirmed to be exceptionally effective against severe illness and hospitalization, we were then faced with new variants and the resource-intense responses necessary to combat them. Despite challenges new and old, we have persevered and continued to provide excellent care to our patients while pushing the boundaries of clinical research. This article is a collection of studies published in 2021 relevant to critical care, with a specific focus on cardiothoracic critical care. To ignore the impact of the COVID-19 pandemic would do a disservice to our colleagues, many of whom have made incredible breakthroughs in novel therapies to the coronavirus, and yet we present additional themes of delirium, acute kidney injury, lung transplant, advances in ECMO as well as biomarkers of sepsis.
Introduction
This review is a selected list of publications chosen to highlight key themes relevant to cardiothoracic critical care in 2021. A PubMed search was conducted with focus terms of cardiac surgery, thoracic surgery, heart transplantation, and lung transplantation crossed with critical care. Additional filters were chosen specifically to include year 2021 as well as manual filters to include search terms of anesthesiology and surgery. We subsequently manually reviewed the remaining 772 articles for representation in this review. A number of major themes were identified for specific discussion, including sedation and postoperative delirium, advances in diagnosis, treatment and prognosis of acute kidney injury following cardiac surgery, advances in treatment and examination of outcomes in heart and lung transplantation, novel biomarkers for sepsis in the cardiac surgery population, a comparison of resuscitation strategies, and carbon dioxide removal via an extracorporeal circuit in acute respiratory distress syndrome. Therapeutic advances in the treatment of COVID-19 were queried separately.
Postoperative Delirium
Postoperative delirium (POD) remains an important topic in clinical research, as up to 53% of patients who undergo major surgery have been shown to experience some level of cognitive dysfunction. 1 Multiple publications over the last year attempted to identify predictors of postoperative delirium, examining risk factors throughout the perioperative period.
Risk and Prevention
Although management strategies have been identified that reduce the incidence or severity of POD, some factors appear to be non-modifiable but nonetheless useful for risk stratification. In a meta-analysis of fourteen publications that included over 13,000 participants, specific factors in each phase of the perioperative period were identified that may increase the likelihood of POD. 2 The risk of POD positively correlated with age which increased by year, with age greater than 65 being most significantly associated. Other factors included preoperative diagnoses of carotid artery stenosis and diabetes. One factor that was protective against POD was greater preoperative left ventricular ejection fraction (LVEF).
One potentially modifiable condition in the preoperative period that has immense impact on POD is depression. In a systematic review and meta-analysis of seven publications including over two thousand patients, it was identified that 26% of the study population had POD and that approximately 9% of the total study population had a preoperative diagnosis of depression. Across all seven of the studies there was a clear association between the diagnosis of preoperative depression and the development of POD. 3 The association of preoperative depression and POD had an odds ratio of 2.31, suggesting that the identification and initiation of treatment prior to major surgery could have significant impact on a large surgical population, though prospective trials are necessary to validate these findings.
Intraoperative and postoperative factors also seem to have some influence on the development of POD. A review of pooled data from four separate publications showed that every 1-minute increase in aortic cross clamp time increased the odds ratio of POD by 1%, though the endpoint was not statistically significant. This data, when combined with data from two additional studies, also identified that every hour a patient spent on the ventilator was associated with a higher risk of developing POD. When this same data was evaluated to look at days spent in the ICU, it was identified that every day spent in the ICU raised the odds ratio by 40% for the development of POD. 2
Sedation Strategy
It has been well established that sedation increases the likelihood of the development of POD. 4 Nevertheless, sedation does play an important role in the management of ICU patients, particularly those arriving from the operating room following major cardiac surgery. A recent review of fifteen studies that included over 2800 patients identified that the use of dexmedetomidine provided adequate sedation with a potential reduction in the development of POD by up to 44% when compared to opioids and other sedating medications. 1 In a recent double-blinded randomized controlled trial, researchers compared dexmedetomidine to a true control, normal saline. After analyzing the results from the 102 study participants, dexmedetomidine showed some benefit, including a reduced length of stay and improved pain scores. Interestingly, when compared to normal saline, dexmedetomidine did not provide any statistically significant reduction in POD. A separate meta-analysis of thirteen publications showed that, when compared to other medications, dexmedetomidine decreased the amount of time patients spent on the ventilator and reduced the amount of postoperative complications after cardiac surgery. 5
Steroids
In 2021, multiple reviews of the available literature were done to determine if steroid administration could be an effective way to reduce POD. Glucocorticoid administration is postulated to reduce the risk of POD by reducing the degree of the inflammatory response, particularly in major cardiac surgery. In a recently published longitudinal study, 116 patients were assessed on postoperative day six and then 4 years after surgery for any degree of POD. The researchers performed multiple neurological assessments, including a mini-mental state exam and a Rey auditory verbal learning test, prior to surgery to establish a clear baseline and these same tests were performed at follow up. While preoperative administration of dexamethasone showed some benefit in reducing POD at the 6 day and 4-year mark, it did not reach statistical significance. 6 In another review covering over 8000 patients it was determined that while administration of glucocorticoids did not reduce POD, they did reduce time on the ventilator, as well as time in the ICU––two factors that we know greatly contribute to the development of POD. 7 The meta-analysis did not show any significant impact on blood sugar, wound healing or gastric injury in the trial group compared to the control group––possibly indicating that the administration of steroids may provide some benefit without a significant detrimental effect.
Acute Kidney Injury
Diagnosis
Early detection of acute kidney injury (AKI) in the cardiac surgery population remains a subject of intense study. AKI has been reported in up to 40% of cardiac surgical patients, and for the 13% of those progressing to the need for renal replacement therapy (RRT), AKI is an independent risk factor of morbidity and mortality. 8 Unfortunately, current definitions rely on serum creatinine measurements and urine output, which may result in a diagnostic delay of 1–3 days. While there has been significant interest in biomarkers which may provide advanced warning of renal injury, these methods can be expensive, can require longer processing time, and have limitations on the timing of bioassay performance. Silverton et al performed a feasibility trial with a device providing noninvasive, real-time measurement of urine oxygen partial pressure, a measure previously shown to be predictive of postoperative AKI in cardiac surgical patients. 9 Using a prototype investigational urinary oximeter placed between the collection bag and urinary catheter, they monitored oxygen content and flow rate throughout the intraoperative period and into the ICU, with the device being removed no later than 24 h following separation from cardiopulmonary bypass (CPB). Data analysis was limited to flow rates at or above an arbitrary threshold of 0.5 cc/kg/h, as accuracy at lower flow rates was unknown and it was posited that below this rate would be classified as AKI even without additional supporting data. The primary outcome measure was incidence of AKI by Kidney Disease: Improving Global Outcomes (KDIGO). 10 Of the 91 devices applied (118 patients were enrolled with 18 declining and an additional 9 excluded for non-patient factors), 86 of these completed the study, with 5 device malfunctions preoperatively. Data from the ICU was excluded given a high rate of oliguria in these patients, and an additional 16 were excluded from analysis for the same issue on CPB. Their data revealed that a mean urinary oxygen partial pressure cutoff of less than 25 mmHg following CPB was associated with AKI. Notably, these measurements were available 2 days prior to significant serum creatinine elevation, providing an earlier alert as to the presence of a developing AKI. While the exploratory nature of this study means that their results will need extensive validation prior to application in clinical use, the feasibility of these measurements provides a promising new method to identify acute kidney injury earlier in cardiac surgery patients.
Intervention
With the potential to detect AKI more rapidly, more attention is being paid to strategies to reduce the severity of this morbid complication. The KDIGO guidelines provide a bundle of recommendations for this purpose. Its early implementation has been demonstrated to reduce the occurrence of AKI in cardiac and major abdominal surgical patients when using a biomarker-based approach to identify those at high risk in two single center RCTs, though these were relatively small studies.11,12 Zarbock et al set out to determine the feasibility of implementing such a bundle for high-risk patients undergoing cardiac surgery in a multicenter trial. 13 Their randomized controlled, multicenter, parallel-group trial was conducted in 12 centers around Europe. Using the urinary biomarkers tissue inhibitor of metalloproteinases-2 (TIMP-2) and insulin growth factor-binding protein 7 (IGFBP7), they identified those patients at high risk for AKI following cardiac surgery. Of the 1,447 patients screened, 280 were enrolled. Exclusion criteria included patients with preexisting AKI, need mechanical circulatory support, chronic dialysis dependency, pregnancy, or breastfeeding, known glomerulonephritis/interstitial nephritis/vasculitis, chronic kidney disease (CKD), or kidney transplant within 1 year. Those enrolled were randomized to control or the KDIGO bundle, consisting of avoidance of nephrotoxic agents, prevention of hyperglycemia, optimization of hemodynamics and perfusion pressure, functional hemodynamic monitoring if necessary and close monitoring of renal function. Adherence to the bundle was significantly higher in the intervention arm. The incidence of AKI within 72 h of surgery was not statistically different between the groups; however, the incidence of moderate to severe AKI was significantly lower in the intervention group. Interestingly the use of RRT was higher in the intervention group at day 90. As a feasibility study, the project was a success, demonstrating a significant increase (65.4% compared to 4.2%) in adherence to a previously validated bundle to potentially reduce the occurrence of AKI following cardiac surgery. This data suggests a potential role for both the KDIGO bundle and a biomarker-based identification of high-risk patients in reducing kidney injury following cardiac surgery.
Prognosis
Despite early detection and treatment strategies, 2–5% of cardiac surgery patients will incur AKI necessitating renal replacement therapy (RRT), which confers up to a 50% risk of mortality.14,15 Failure to recover to independence off RRT can place considerable quality of life restraints on patients and family members. No models currently exist to predict the chances of renal recovery in cardiac surgical patients, which can make conversations concerning the initiation of therapy challenging. Hu et al set out to build a predictive model based on retrospective analysis of data from the Effect of the Intensity of Continuous Renal Replacement Therapy on patients with cardiac surgery-associated Acute kidney Injury (CRITERIA) study. 16 This single center investigation over 3 years was designed to compare survival between two dosages of hemofiltration in patients older than 18 years with AKI following cardiac surgery and deemed by the treatment team to require RRT, with those patients previously requiring RRT and those with a diagnosis of CKD prior to surgery excluded. Multivariable logistic regression analysis showed that mechanical ventilation, baseline eGFR, hypertension, sepsis, MAP, and BMI stratification were the best predictors of renal recovery. Low BMI was a negative predictor of recovery, a similar finding to studies showing decreased odds after percutaneous coronary intervention and in the elderly. The authors posited that critical illness patients present with hypermetabolism and high energy consumption, and that low BMI patients have less efficient immune systems and are prone in inflammation. Limitations of the model include a relatively low sample size and single center nature of the original study, as well as the non-standardized approach to cessation of renal replacement therapy in the medical community. While this predictor will require validation on a larger scale, it provides a promising framework to guide shared decision making between the nephrologist, intensivist, the patient, and their family.
Lung Transplantation
Complications
Central airway stenosis (CAS) is a serious complication of lung transplantation resulting in significant morbidity and mortality. Strategies to mitigate this complication include bronchial artery anastomosis, topical application of hypoxia inducible factor stabilizers, and hyperbaric oxygen. Kraft and colleagues performed a randomized controlled trial comparing hyperbaric oxygen to usual care in patients demonstrating extensive airway necrosis at 4 weeks post-transplantation. The trial was stopped early as there was no difference between usual care and hyperbaric oxygen in the rates of acute cellular rejection, stenting, or CAS. The time to stent placement was significantly shorter in the hyperbaric oxygen group (P < .05). Interestingly, patients that developed CAS and received stenting had significantly elevated HMOX1 and VEGFA expression at 4 weeks (P < .05).
Another serious but uncommon complication after lung transplantation is pulmonary artery obstruction. Kumar et al performed a systematic review and meta-analysis to determine the prevalence of this complication after lung transplantation. 18 After looking at 34 full text citations, the prevalence of pulmonary artery obstruction was 3.66% (n = 1696). The prevalence was higher in single lung transplantation. The most common causes were reduction of the pulmonary artery lumen (63.93%) and distortion or kinking due to donor-recipient size mismatch (24.59%). The authors found the mortality of obstruction to be 22.54%. There are no recommendations regarding transesophageal echocardiography (TEE) assessment of the pulmonary artery during the lung transplantation. The authors found a pressure gradient of 57 mmHg, velocity of 2.6 m/s, and pulmonary artery diameter of .78 cm as useful guides for intraoperative TEE assessment
Therapy
Surfactant is a crucial component of normal lung health maintenance and changes in surfactant in lung transplantation have been well described. However, surfactant is not routinely used in clinical lung transplantation. Ali and colleagues performed a systematic review and meta-analysis of 6 clinical studies and 29 pre-clinical studies with a primary outcome of the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2). 19 The clinical studies demonstrated significantly improved oxygenation in recipients of surfactant therapy during lung transplantation (P < .01). Analysis of the pre-clinical studies similarly demonstrated a significantly higher PaO2/FiO2 (P < .01).
Heart Transplantation
Donor Heart Preservation
In order to expand the donor pool for heart transplantation there has been increased interest in donation of after circulatory death (DCD). One of the challenges to heart transplantation in general and DCD specifically is minimizing ischemic-reperfusion injury (IRI). Hydrogen sulfide (H2S) is an endogenous signaling molecule that has been implicated in cardioprotective effects in models of IRI. Ertugruli et al conducted a systematic review and meta-analysis to evaluate the cardioprotective effects of H2S in postconditioning against IRI. 20 After looking at 16 rodent model studies, they found a significant effect that H2S limited infarct size (P < 00.001). H2S may offer a valuable target for novel cardiac preservation therapies.
Risk Stratification
Matkovic et al sought to determine the effect of preoperative pulmonary artery hypertension (PAH) as a result of left-sided heart failure (HF) on long-term survival after heart transplantation. 21 They conducted a prospective, observational trial that included 44 patients and compared those with a preoperative diagnosis of PAH to those without a preoperative diagnosis of PAH. The groups were well-matched and those with preoperative PAH had a significantly higher 30-day mortality (P < .05). Interestingly, right heart catherization values of pulmonary vascular resistance index (PVRI) and transpulmonary gradient (TPG) were found to be independent predictors of lower 30-day survival after heart transplantation.
Outcomes
As of February 2022, severe acute respiratory syndrome coronavirus 2 diseases (COVID-19) has infected over 400 million people across the globe, 22 and even with vaccination, immunosuppressed patients remain at high risk. Granger et al reported a case series of 39 heart transplant (HT) recipients from 3 French transplant centers as well as a systematic review and meta-analysis of outcomes in HT patients with COVID-19. 23 Of the 39 patients, 74.4% had their immunosuppression reduced while 33.3% required mechanical ventilation and 25.6% died. Additionally, 43.6% of patients developed acute kidney injury and 15.4% required RRT. The authors’ meta-analysis looked at 41 published studies and found the overall mortality of heart transplantation patients with COVID-19 to be 22.1%. Preexisting diabetes mellitus and CKD stage III were associated with death.
Postoperative Management
Iron deficiency is common in end-stage heart failure and prone to persist post-transplant for a myriad of reasons. Heart transplant recipients also have decreased exercise tolerance despite normal graft function. Brautaset Englund and colleagues performed a randomized, placebo-controlled, double-blind trial comparing iron supplementation (ferric derisomaltose 20 mg/kg) vs placebo on exercise tolerance in heart transplant recipients. 24 Iron deficiency was defined as ferritin <100 μg/liter or 100-300 μg/liter with transferrin saturation of <20%. There was no difference in oxygen consumption between those receiving iron supplementation and placebo at 6 months. However, iron levels and quality of life were both significantly higher in the treatment group with no increase in adverse events.
Calcineurin inhibitors improve survival after heart transplantation, but are associated with adverse effects such as nephrotoxicity, hypertension, metabolic disease, and allograft vasculopathy. They are also causatively linked to left ventricular hypertrophy (LVH). LVH in the allograft at 1 year is an adverse prognostic marker. Anthony et al performed a prospective, randomized, open label study comparing low-dose everolimus plus low-dose tacrolimus to standard dose tacrolimus starting at 12 weeks post-transplantation. 25 They primarily followed LVH as the change in left ventricular mass (LVM) by cardiovascular magnetic resonance imaging. There was a significant decrease in LVM (P < .001). There was no significant difference in blood pressure, renal function, frequency of rejection, or frequency of infections.
Extracorporeal Carbon Dioxide Removal
Lung protective ventilation is a cornerstone of the treatment of acute respiratory distress syndrome (ARDS). While this therapy has been shown to reduce mortality, it can be complicated by respiratory acidosis. McNamee et al designed a multicenter, randomized, allocation-concealed, open label clinical trial comparing lower tidal volume ventilation with CO2 removal facilitated by extracorporeal carbon dioxide removal (ECCO2R) with normal low tidal volume ventilation. 26 Lower tidal volumes were achieved in the intervention group, but there was no significant difference in 90-day mortality between the two groups. There were significantly fewer ventilator-free days in the intervention group, but otherwise no significant difference in duration of ventilation, need for ECMO at day 7, mortality at day 28, or duration of ICU stay. There were more serious adverse events in the intervention group: 31 vs 9%.
Prothrombin Complex Concentrate vs Fresh Frozen Plasma
It is not uncommon for postoperative resuscitation after cardiac surgery to include blood products. Looking at a way to more efficiently achieve hemostasis and minimize the amount of blood products administered provides both short- and long-term benefits for patients, as every unit of blood product given has the potential to cause a complication.
In a recent randomized pilot study, 101 individuals undergoing cardiac surgery were separated into two groups––one to initially receive four factor pro thrombin complex concentrate (PCC) and the other fresh frozen plasma (FFP)—in order to evaluate the hemostatic effects in the resuscitation. 27 The researchers looked at the overall amount of hemostatic therapies each individual received after initiation of the intervention at specific time points, including the 60-minute, 4-hour, and 24-hour marks. Their findings showed that at the 4-hour and 24-hour time points, the PCC group had received less hemostatic therapies compared to the FFP group and that, overall, the PCC group received 42% fewer blood products. This means that the PCC group had less exposure to foreign products and therefore lower likelihood of complications. It also suggested that rapid correction of coagulopathy with concentrated factors may save additional resuscitation later in the clinical course. Although this trial was small, it does shed light on the potential benefits for the use of four factor PCC. The advantages that PCC provides come from its reliable, constant and measured degree of factor concentration as well as less volume.
Procalcitonin Levels Following Cardiac Surgery
Key Articles for Critical Care 2021.
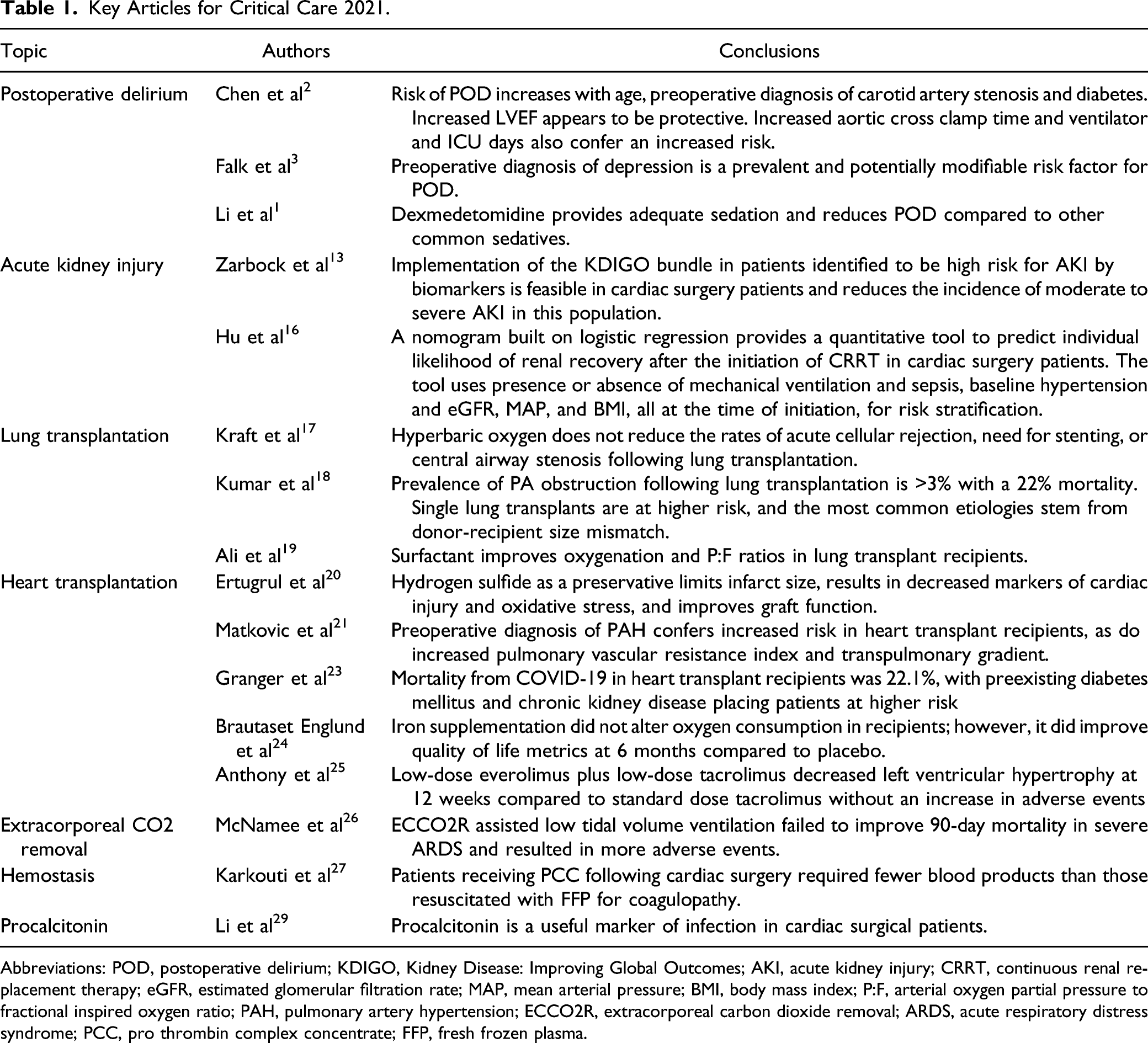
Abbreviations: POD, postoperative delirium; KDIGO, Kidney Disease: Improving Global Outcomes; AKI, acute kidney injury; CRRT, continuous renal replacement therapy; eGFR, estimated glomerular filtration rate; MAP, mean arterial pressure; BMI, body mass index; P:F, arterial oxygen partial pressure to fractional inspired oxygen ratio; PAH, pulmonary artery hypertension; ECCO2R, extracorporeal carbon dioxide removal; ARDS, acute respiratory distress syndrome; PCC, pro thrombin complex concentrate; FFP, fresh frozen plasma.
COVID-19
The COVID-19 pandemic has continued to stress hospitals and intensive care units (ICUs) over the past year, with repeated surges frequently overwhelming hospital capacity and resources. Moreover, the demand for non-COVID care has increased, which may be the result of lockdowns, hesitancy to pursue treatment, or delay of surgery as sequelae of COVID-19 burden on healthcare systems. 30 Intensivists remain on the frontlines caring for large numbers of critically ill COVID-19 patients, while now also facing an increased number of non-COVID patients in the ICU. In the procedural realm, the optimal timing and management of tracheostomies for COVID-19 patients remains a frequent question for intensivists, surgeons, and anesthesiologists.
Last year, the RECOVERY trial identified dexamethasone as one of the few medications to provide a mortality benefit in critically ill COVID-19 patients. 31 Use of dexamethasone later in the disease course is postulated to reduce inflammatory-mediated lung injury, particularly in patients requiring invasive mechanical ventilation. 31 This widely available and inexpensive medication is now adopted as standard of care worldwide. 31 Here, we continue our review of medical therapies, as well as recent meta-analyses of tracheostomy outcomes in COVID-19 patients.
Baricitinib
Baricitinib is a selective inhibitor of Janus kinase (JAK)1/JAK2 which results in intracellular cytokine pathway inhibition, as well as interfering with the function of protein kinase 1 and subsequent cellular viral entry and infectivity. 32 This agent was identified by artificial intelligence as a potential intervention in COVID-19, and the results of the Adaptive COVID-19 Treatment Trial 2 (ACTT-2) found a reduced time to recovery and more rapid clinical improvement when co-administered with remdesivir, particularly in patients requiring oxygen supplementation. 32 Although this study suggested a mortality benefit at 28 days, it was underpowered to determine a significant result. The COV-BARRIER trial was designed as a double-blind, placebo-controlled trial to evaluate for benefit and safety of baricitinib plus standard of care vs standard of care alone in 1,502 patients across 101 centers in 12 countries. 33 Hospitalized COVID-19 patients requiring supplemental oxygen were randomized 1:1 to receive 4 mg/day enteral baricitinib (2 mg/day for patients with renal impairment and eGFR between 30 and 60 mL/min/1.73 m2) for up to 14 days or until hospital discharge vs placebo. Patients age 18 and older with confirmed COVID-19 were included if they had evidence of pneumonia or symptomatic COVID-19 infection, at least 1 elevated inflammatory biomarker (C-reactive protein, d-dimer, lactate dehydrogenase, or ferritin), and required supplemental oxygen. Exclusion criteria were patients requiring invasive mechanical ventilation at the time of enrollment, immunosuppressing medications, neutropenia, lymphopenia, prior COVID-19 convalescent plasma or intravenous immunoglobulin, elevation of liver enzymes or severely impaired renal function (eGFR <30 mL/min/1.73 m2). The primary endpoint was the proportion of patients to progress to requiring high-flow supplemental oxygen, noninvasive or invasive mechanical ventilation, extracorporeal membrane oxygenation or death at 28 days; results revealed no significant difference in the baricitinib vs standard of care group (27.8 vs 30.5% respectively; odds ratio .85, 95% confidence interval .67–1.08, P = .18). Incidence of adverse outcomes was similar between the two groups. Notably, the results from the RECOVERY trial were released during the COV-BARRIER study, with the standard of care changing significantly to include routine use of dexamethasone. This may have altered the results of the COV-BARRIER study and is a limitation of this investigation. Nonetheless, these results support the safety profile of baricitinib in COVID-19 patients. 33
Prostacyclin
Autopsy results from COVID-19 patients note pulmonary microvascular thrombosis and endotheliopathy, with severe pulmonary injury. 34 Patients with endotheliopathy have elevated levels of circulating soluble thrombomodulin (sTM), a biomarker associated with a prothrombotic phenotype in COVID-19 infection. 34 Prostacyclin released by endothelial cells results in a dose-dependent vasodilatory effect, as well as causing platelet inhibition. Both mechanisms are beneficial in severe COVID-19 respiratory failure. Johansson et al. enrolled 80 patients in a Danish multicenter, randomized, blinded, parallel-grouped exploratory trial to investigate the safety and efficacy of intravenous prostacyclin vs placebo in mechanically ventilated patients with COVID-19. Patients were included if they were 18 years or older, had confirmed COVID-19 infection, required invasive mechanical ventilation and had and documented endotheliopathy as measured by an elevated level of sTM (>4 ng/mL). 34 Exclusion criteria included patients who were intubated for longer than 72 h at time of enrollment, pregnancy, withdrawal from active therapy, known hypersensitivity to prostacyclin, enrolled in an alternative prostacyclin trial within 30 days, life-threatening bleeding, known severe heart failure or suspected acute coronary syndrome. Patients were randomized to receive an infusion of prostacyclin 1 ng/kg/min for 72 h vs placebo. The primary outcome of ventilator-free days at 28 days was 5 days in the placebo group vs 16 days in the prostacyclin group. However, there were large standard deviations for both groups (12 and 10 days respectively, 95% CI −5 to 21, P = .07). Secondary outcomes of 28-day and 90-day mortality were need for renal replacement therapy, vasopressors, ventilator-free days at 90-days, and safety outcomes similarly yielded no significant benefit. There was, however, an improvement in sequential organ failure assessment (SOFA) score (5.7 prostacyclin vs 6.7 placebo, adjusted difference 1.1; 95% confidence interval .28–1.92, P = .009). 34 The safety of prostacyclin in COVID-19 patients with severe respiratory failure is supported by this study, though a higher powered study is needed to evaluate for efficacy.
Tracheostomy
The prolonged requirement for invasive mechanical ventilation in some COVID-19 patients presents a unique challenge in the setting of a global pandemic, where high demand for limited resources such as ventilators and ICU beds has forced healthcare systems to enact crisis standards of care in extreme circumstances. Tracheostomies in patients with prolonged respiratory failure have previously been demonstrated in the non–COVID-19 population to facilitate weaning from sedation and the ventilator, resulting in decreased number of days in the ICU as well as reduced incidence of ventilator-associated morbidity. Two meta-analyses from the past year evaluated for similar findings in the COVID-19 population.35,36
Ferro et al reviewed 39 studies from the United States, the United Kingdom, Spain, Italy, China, and India which investigated outcomes following tracheostomy in COVID-19 patients. 35 Included studies were those specific to COVID-19 that included outcome data for mortality, timing of decannulation, weaning of mechanical ventilation, and complication rates. The authors excluded small case series of less than 10 patients. There was no significant difference in mortality, complication rate, or timing to decannulation depending on if the tracheostomy was performed as a surgical or percutaneous procedure. Early tracheostomy (defined as occurring less than 14 days from intubation) vs those performed after day 14 did not reveal a mortality benefit nor did it predict time to decannulation. 35 While the authors attempted to evaluate rates of nosocomial infection to healthcare workers participating in the procedure, there was insufficient data to perform an analysis. The latter finding is notable and supports the effectiveness of personal protective equipment (PPE) during these aerosol-generating procedures. 35 This meta-analysis was limited by incompleteness and variability in reported data in the 39 included studies, as well the possibility of selection bias in a rapidly emerging disease process.
Key COVID-19 Critical Care Articles for 2021.
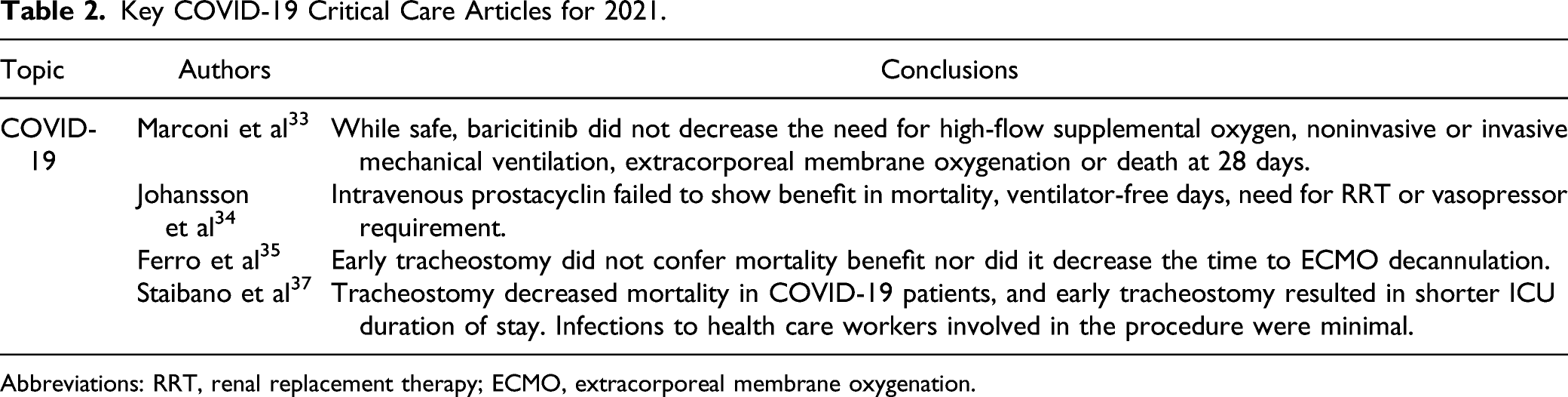
Abbreviations: RRT, renal replacement therapy; ECMO, extracorporeal membrane oxygenation.
Conclusion
This past year has seen the growth of literature on a number of issues pertaining to the care of cardiac surgical patients. Postoperative delirium continues to be an area of intense focus. Early diagnosis and intervention of acute kidney injury is slowly integrating into everyday care. Strategies to expand the transplant donor pool continue to develop while year-over-year we increase our capacity to better care for these patients postoperatively. We continue to make advancements in the recognition and treatment of postoperative sepsis, resuscitation, and ECMO-based therapies. Our armamentarium of tools to combat COVID-19 and its worst effects is growing. While this is not a comprehensive review of all relevant topics, we hope it will guide and inform busy clinicians on the latest discoveries and observations pertinent to their practice as well as to provide hope for the future of therapeutics in critical care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.