
Abstract
The management of children with a borderline ventricle has been debated for many years. The pursuit of a biventricular repair in these children aims to avoid the long-term sequelae of single ventricle palliation. There is a lack of anesthesia literature relating to the care of this complex heterogenous patient population. Anesthesiologists caring for these patients should have an understanding on the many different forms of physiology and the impact on provision of anesthesia and hemodynamic parameters, the goals of biventricular staging and completion as well as the pre-operative, intra-operative, and post-operative considerations relating to this high-risk group of patients.
Introduction
Whether a complex biventricular repair is preferred over single ventricle palliation in children with a borderline ventricle has been a topic of debate for over a decade. 1 The debate has typically addressed children with borderline left heart disease but has also addressed other forms of congenital cardiac disease with a functional single ventricle such as unbalanced atrioventricular canal defect, double outlet right ventricle, complex transposition of the great arteries and pulmonary atresia with intact ventricular septum. In addition, patients with complex intracardiac anatomy (e.g. straddling of atrioventricular valves) may be potential candidates for a biventricular repair strategy.
The primary incentive of pursuing a biventricular repair in this heterogeneous group of patients is to avoid the long-term sequalae of single ventricle palliation. This is particularly important in patients with other high-risk comorbidities such as heterotaxy and Trisomy 21, who both have poorer outcomes with single ventricle palliation.2,3 Unfortunately, long-term survival after the Fontan procedure has not improved significantly over the last decade 4 leaving many patients, families and cardiologists seeking alternative therapies. Our institution has a large population of local and referred patients who are failing to progress on the single ventricle pathway to Fontan palliation. Some palliated single ventricle patients develop complications such as plastic bronchitis or protein-losing enteropathy, and most Fontan patients will have end-organ dysfunction including Fontan associated liver disease. 5 Other palliated single ventricle patients develop severe cyanosis related to high pulmonary vascular pressures, veno-venous collaterals, atrioventricular valve regurgitation and/or ventricular dysfunction, and pulmonary vein disease. While cardiac and/or lung, liver or kidney transplantation can be considered, there is a significant shortage of available organs. Importantly, single ventricle patients may also have contraindications to cardiac transplantation such as pulmonary hypertension or high panel reactive antibody titers.
Our institution has a busy biventricular repair program that continues to grow significantly in both volume and complexity. The aim of this review article is to provide an overview of the selection, evaluation and implementation of biventricular repair strategy which includes primary biventricular repair, staging to a biventricular repair, and conversion of a single ventricle palliation to a biventricular repair. We will detail the specific anesthesia concerns and challenges associated with the care of these patients.
Variation in Patient Anatomy
The majority of single ventricle patients actually have two ventricles one of which is small. This may be the left or the right ventricle (see Figure 1). Left heart hypoplasia is a spectrum of disease. Children with the most severe disease (ie. hypoplastic left heart syndrome with aortic and mitral atresia) will typically proceed down the single ventricle palliation pathway whereas those with milder forms of left heart hypoplasia (ie. aortic stenosis or coarctation) may undergo a biventricular repair that addresses the aortic or valvular obstruction. However, many patients will have what is considered “borderline” left heart hypoplasia. There is also a subset of patients with a small right ventricular size, such as patients with pulmonary atresia and intact ventricular septum and patients with left dominant atrioventricular canal defects. In addition, there are some patients who have complex anatomy which may require extensive surgery to create a biventricular circulation including multiple intracardiac baffles, straddling valvular tissue, and arterial switch or aortic root translocations. Traditionally these patients have been managed with single ventricle palliation procedures as the extent of the procedures necessary to achieve a biventricular circulation tend to be extremely complex and require specific surgical expertise in creating complex baffles, as well as valve repair. Variations in anatomy in patients undergoing biventricular repair. Patients who present for biventricular repair can be broadly grouped into 3 categories: complex anatomy with 2 adequately sized ventricles, small right ventricular and small left ventricular congenital heart disease. These categories are not mutually exclusive as there is some overlap. Patients who have small right or left sided ventricles often require staging catheterization or surgical procedures to encourage growth of the ventricle. DORV = Double Outlet Right Ventricle; PA/IVS = Pulmonary Atresia/Intact Ventricular Septum; AVC = Atrioventricular Canal; PFO = Patent Foramen Ovale; HLHS = Hypoplastic Left Heart Syndrome; AS = Aortic Stenosis.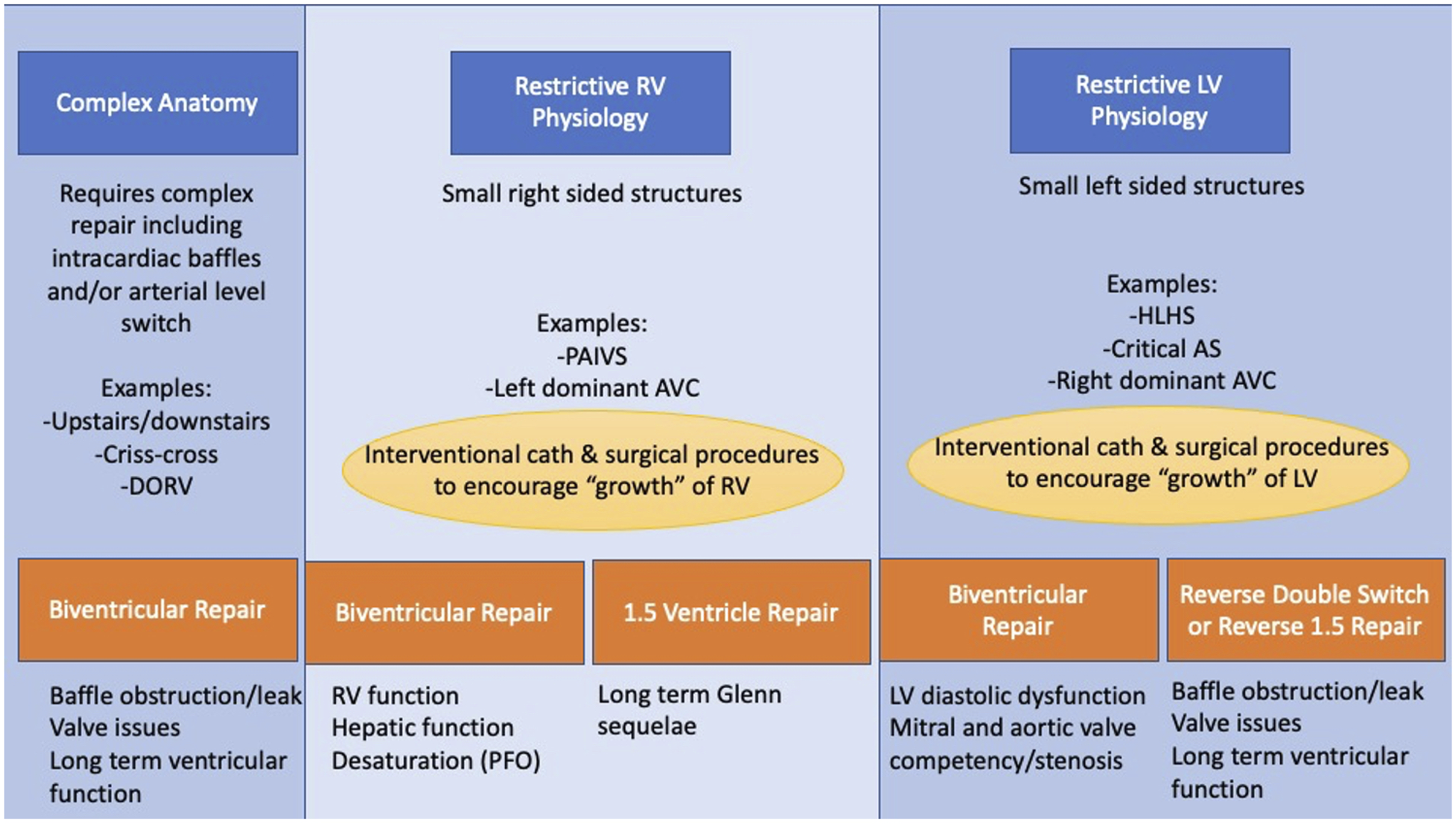
Assessment of the Adequacy of the Left Ventricle for Biventricular Repair and Growth of the Left Ventricle
Borderline left heart disease is defined by Z-scores between −5 and −2 of the aortic valve, mitral valve, and left ventricular end-diastolic volume as well as the presence of endocardial fibroelastosis (EFE). It has been demonstrated that a pre-operative left ventricular end-diastolic pressure (LVEDP) measurement at cardiac catheterization of greater than or equal to 13 mmHg is an independent predictor of mortality, heart transplant, or biventricular take-down. 6 The appearance of the mitral valve, including the structure of the papillary muscles and chords, are also important factors when considering the suitability of the left ventricle to be able to support the systemic circulation. The appearance of the left ventricle is also considered, as a non-apex forming, extremely hypertrophied left ventricle less likely to be able to tolerate a biventricular circulation. The difficulty is that no single feature is absolutely a guarantee of success or failure of a biventricular repair. Rather, there is a constellation of features which suggests that a biventricular repair would be feasible or not. In those patients in whom there is concern about the size of the left ventricle, staging procedures are often undertaken. These staging procedures attempt to volume load the left ventricle and may involve one or more maneuvers including restriction of the atrial septum, placement of a systemic to pulmonary artery shunt, or partial closure of ventricular septal defects to encourage the growth or dilation of the left ventricular cavity. In patients with large inlet ventricular septal defects, it may be possible to place the intraventricular patch on the right side of the heart to allow the newly septated heart to have a larger left ventricular volume.
Assessment of the Adequacy of the Right Ventricle for Biventricular Repair and RV Rehabilitation
Although the majority of literature published in recent years on biventricular repair strategies has focused on children with borderline hypoplastic left ventricles, a similar clinical approach can be pursued in those with small right ventricles. A borderline right ventricle is defined as a Z-score between −5 and −2 of the right ventricle and associated atrioventricular valve. The use of atrial septal restriction is also a key component of encouraging growth of the right ventricle through increasing flow across the right atrioventricular valve. 7 This is an important strategy given that biventricular conversion is associated with a higher risk of mortality in patients with left dominant atrioventricular canal defects. 7 Although the addition of a systemic to pulmonary shunt to volume load a hypoplastic left ventricle can result in favorable growth conditions, options to volume load the right ventricle are much more limited. In patients with a superior cavopulmonary anastomosis, volume loading with inferior vena cava blood flow may be sufficient to induce growth of the right ventricle for eventual biventricular conversion. 7
Patients With Adequate Ventricular Size, but Complex Anatomy
Patients with complex anatomies, but with reasonably balanced ventricles such as patients with double outlet right ventricle or some forms of transposition of the great arteries are evaluated for the potential for repair while considering issues related to baffle feasibility including left ventricular or right ventricular outflow tract obstruction. Extensive imaging is performed including cardiac magnetic resonance imaging (MRI), or cardiac computerized tomography (CT) in patients with pacemakers, to best pre-operatively predict the size and types of baffles required. Some of these patients will also require additional procedures such as an arterial switch or aortic root translocation in addition to the necessary intracardiac repair. Many of these patients have heterotaxy, and have complex venous anatomy such as anomalous pulmonary venous return, interrupted inferior vena cava, or persistent left superior vena cava. In addition to a comprehensive surgical plan, management of the complex anatomy during cardiopulmonary bypass must be considered as well. Due to the overall complexity of these operations, some are performed in stages.
Timing of Biventricular Repair
Candidates can be evaluated for candidacy for biventricular repair from fetal life to early adulthood. Some patients are seen during fetal life and interventional procedures may be performed to attempt to halt the progression of aortic stenosis.
8
A summary of the patient populations considered for possible biventricular repair is shown in Figure 2. Consideration must be given to the overall size and age of the patient, especially when complex baffles and/or there are valve repairs required. Generally, while some primary biventricular repairs and some staging procedures are performed in infancy, the majority of children will not be ready for completion of a biventricular repair until they are at least one year of age. Variations in presentation for biventricular repair. Patients may present at any point on the single ventricle palliation pathway for consideration for a biventricular repair. Some patients are considered for a single stage repair, but the majority will benefit from undergoing a staged approach to encourage ventricular recruitment prior to a final completion biventricular repair. The issues encountered with these various different circulations are listed. PA = Pulmonary Artery; APC = Aortopulmonary Collateral; AVV = Atrioventricular Valve; SVC = Superior Vena Cava; IVC = Inferior Vena Cava; RA = Right Atrium; RV-PA = Right Ventricle–Pulmonary Artery.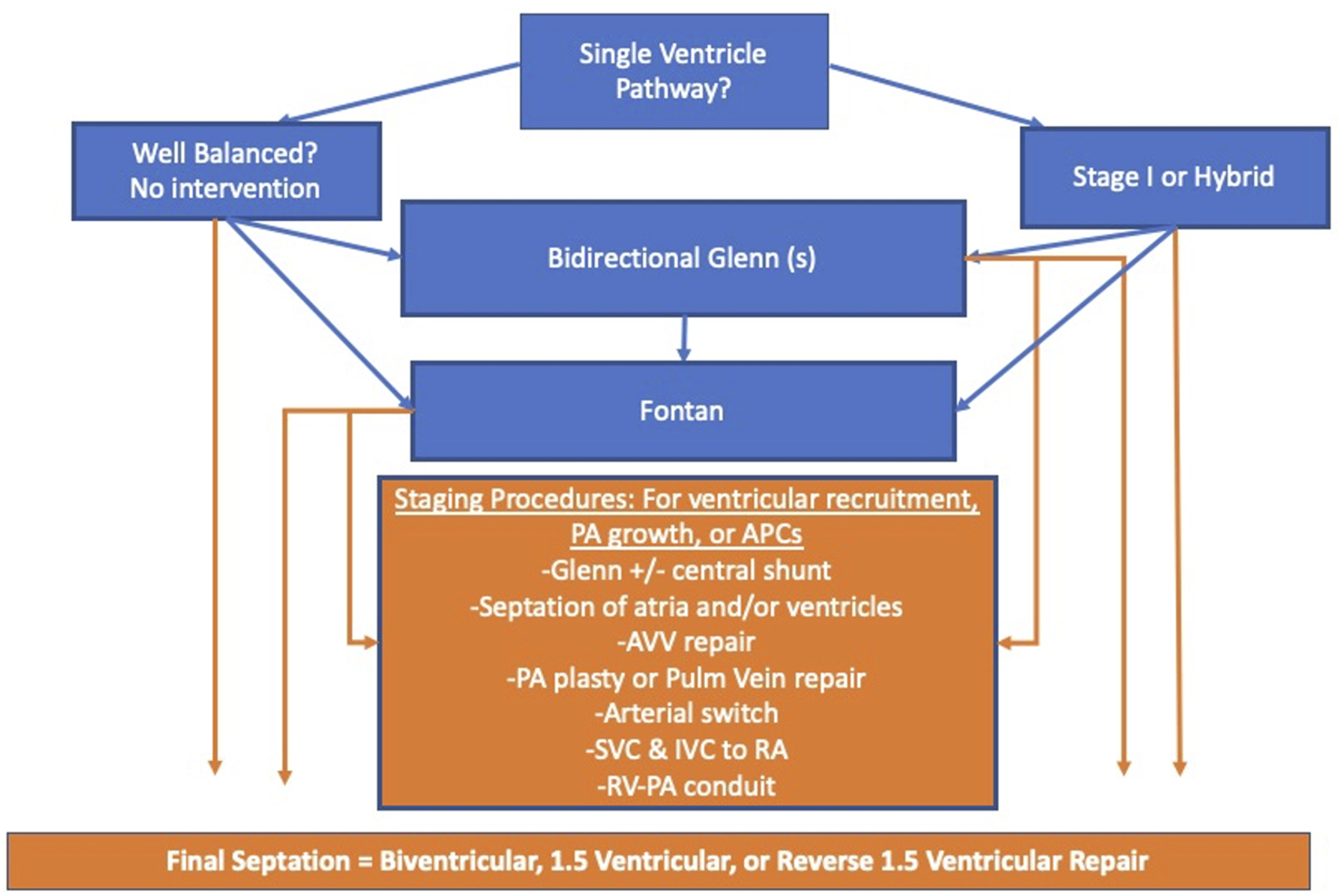
The precise timing of the completion of a biventricular repair is patient specific and varies considerably. Current evidence suggests that in the majority of patients, significant growth of the hypoplastic ventricle does not occur after 12 months following atrial restriction. 9 Therefore, patients may require a systemic to pulmonary artery shunt or a right ventricle to pulmonary artery shunt to encourage flow to the ventricles to encourage growth. 9 Although previous studies have suggested that older age is associated with decreased potential for ventricular growth and recruitment, more recent experience has refuted this. 9
There is a growing experience with biventricular conversion for patients considered to have a sub-optimal Fontan circulation. 10 Of the 23 patients studied, 8 were elective conversions with the remaining 15 converted due to “failing Fontan physiology” (defined as Fontan pressures >15 mmHg and/or associated sequalae). A combination of staged and primary biventricular conversion procedures were undertaken in this patient group depending on the degree of ventricular hypoplasia present with end-diastolic volume cut-offs of 62.5 ml/m2 determining the approach. 10 The median age of patients was 10 years at the time of eventual biventricular conversion. This suggests that conversion at a relatively late age may be feasible. As expected, the overall survival was significantly improved in those patients with elective conversion rather than conversion in the presence of failing Fontan physiology (100% vs 67%).
The Complex Biventricular Repair Program at Boston Children’s Hospital
The Complex Biventricular Repair Program at Boston Children’s Hospital was formally established in 2014 although an active strategy of pursuing biventricular repair has been in existence since the late 1990s. The program is composed of a multi-disciplinary team of cardiac surgeons, cardiologists, cardiac anesthesiologists, and nursing staff that meet on a weekly basis to formally discuss patients considered for the program. Since the formal commencement of the program, the team has reviewed 850 patients as of 2021 (Emani SM, personal communication) with 80% of these being referrals from outside institutions or directly from families.
11
Detailed discussions include review of all relevant imaging and physiologic data. For patients who have not had adequate imaging or testing, patients are asked to come to Boston for a full evaluation. Not all patients are candidates for a biventricular repair, nor do all patients and families decide to ultimately proceed with a biventricular strategy. The options are thoroughly discussed at conference and the parents are presented with the results of these discussions including both the known and unknown risks of single ventricle palliation and a biventricular repair strategy (see Figure 3). Breakdown of underlying cardiac anatomy of patients reviewed by the Complex Biventricular Repair Team at Boston Children’s Hospital from 2014 to 2018 for consideration of biventricular staging and/or repair.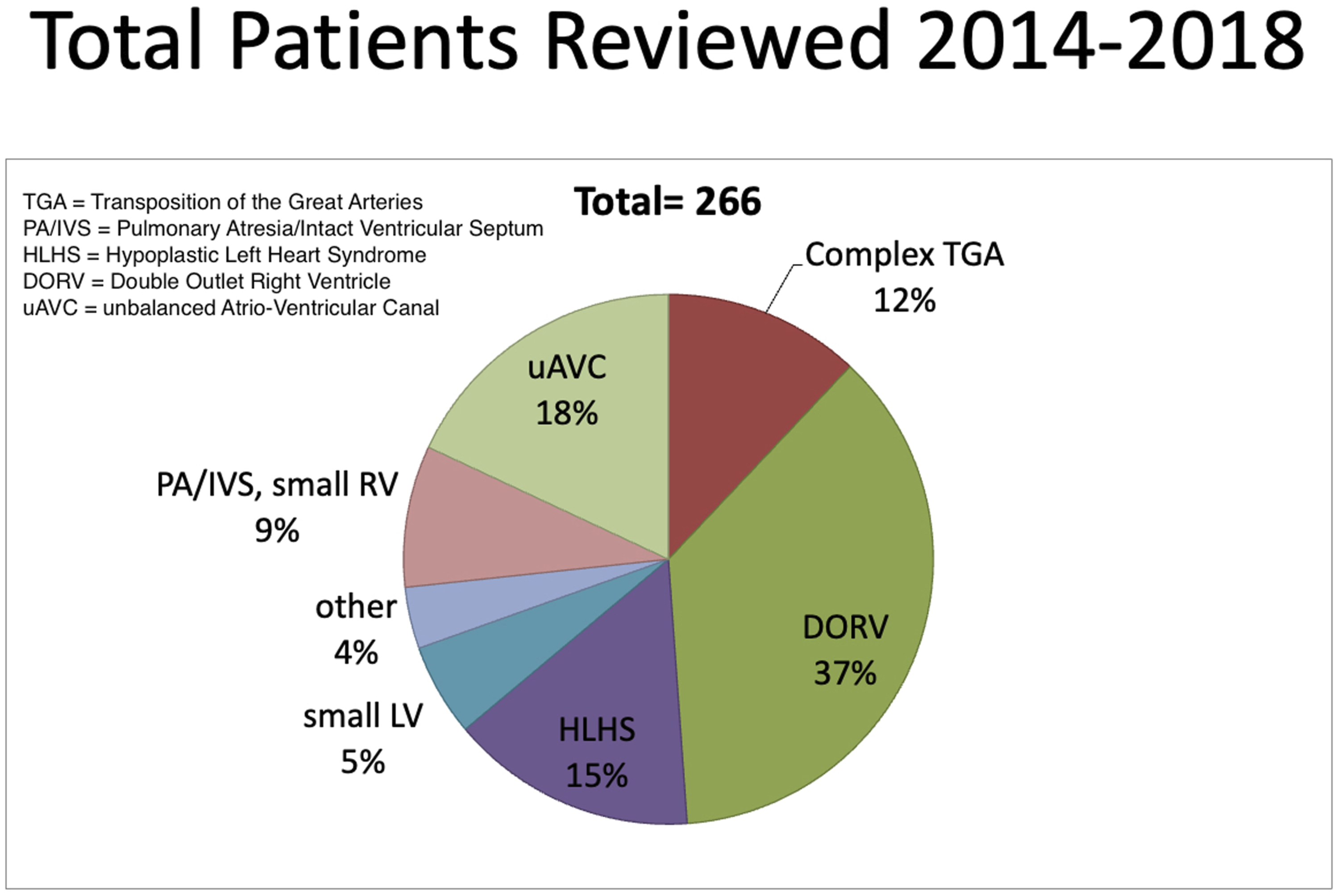
Experience Within Our Institution
The primary concept behind embracing a biventricular staging approach in patients with border left heart hypoplasia is the potential for left ventricular growth over time. For this to occur in infants and children, appropriate flow and loading conditions must be provided.
The definition and accurate measurement of effective growth remains problematic and challenging. Preferably, “growth” should involve an increase in ventricular mass in addition to volume. 11 The growth of a ventricle should not necessarily be equated with an increase in size as dilation of the ventricle with increased end-diastolic ventricular pressures following biventricular repair can be detrimental. Also, the resection of endocardial fibroelastosis (EFE), an important component of our institution’s approach, increases the size of the ventricle yet does not indicate an increase in growth. To complicate matters further, those patients with hypoplastic left heart syndrome are known to have intrinsic abnormalities of the myocardial extracellular matrix that is not addressed by strategies of encouraging ventricular growth.
A staging approach may decrease the risk of severe left or right atrial hypertension. In the case of high left atrial pressures, high pulmonary pressures can lead to risk of acute pulmonary hemorrhage. It is also notable that the consequences of development of pulmonary hypertension secondary to left atrial hypertension can be substantial with the potential to no longer be a suitable candidate for heart transplantation or salvage conversion to single ventricle palliation. Elevated right atrial pressures can cause desaturation through residual atrial level shunting, RV dysfunction, or liver dysfunction.
Primary Versus Staged LV Recruitment
The management of patients with a borderline ventricle has slowly transitioned from previously being considered a dichotomous decision (single ventricle palliation or primary biventricular repair) to consideration of undergoing staged ventricular recruitment. Neonatal biventricular repair in these patients is often a high-risk procedure with significant uncertainty regarding the potential for subsequent ventricular growth and function. 12 The reintervention rate is high and any salvage procedures undertaken in this neonatal population with either single ventricular palliation procedures or institution of mechanical circulatory support are associated with significant risk. 13
In order to avoid this challenging conundrum, our program has focused on a process of staged ventricular recruitment. This involves initially proceeding along the single ventricle palliation pathway with additional measures undertaken to promote ventricular growth at different points in time. Both patients undergoing a surgical Stage 1 or hybrid Stage 1 procedure may be considered candidates for biventricular conversion. The experience of biventricular conversion in patients following hybrid Stage 1 has been described previously. 14 The decision to further pursue eventual biventricular repair is then re-assessed on an ongoing basis when, or if, the patients is deemed an appropriate candidate.
Specific Procedures in Biventricular Staging
ASD Restriction
Restriction of flow across the atrial septum is an important component of staged ventricular recruitment and has been shown to be the primary predictor of ventricular growth (measured by indexed LV end-diastolic volume). 13 In the absence of valvular pathology, flow across an atrial septal defect (ASD) is dependent upon the differences in diastolic compliance of the left and right ventricles. By restricting this flow, both systemic and pulmonary venous blood returns to their corresponding ventricle and results in increased volume loading of the hypoplastic ventricle. Although the presence of a large ventricular septal defect (VSD) limits the potential to volume load the hypoplastic ventricle, restriction of the ASD without closure of the VSD still results in a significant increase in ventricular size. 15 It has been hypothesized recently that the promotion of blood flow through the atrioventricular valve to a hypoplastic ventricle results in ventricular growth irrespective of the exact means of accomplishing this. The presence of antegrade flow across the atrioventricular valve and resultant wall shear stress on the myocardium (with the inflow jet directed at the ventricular apex) may explain the increase in ventricular size seen in patients both with and without large VSDs. Without any restriction at the level of the atrial septum, measures of increasing either pulmonary or systemic venous return would only serve to increase flow through the dominant ventricle and, in the setting of borderline left ventricles with accessory pulmonary blood flow, no increase in ventricle size has been demonstrated. 16 Typically, a 4 mm fenestration is placed within the atrial septal patch, although this may be increased in size in patients at increased risk of atrial hypertension. 11
Endocardial Fibroelastosis
Endocardial fibroelastosis, a diffuse white fibrous tissue lining the endocardium, 17 is often seen in children with left heart obstructive disease. 18 Both moderate and severe EFE has been demonstrated to be a strong predictor of mortality following biventricular repair.18,19 Although transthoracic echocardiography can suggest the presence of EFE with hyper-reflective endocardium, it is not diagnostic and possesses several limitations. 20 The use of myocardial delayed-enhancement cardiac MRI demonstrates a pattern of hyper-enhancement of the endocardial aspect of the left ventricle, papillary muscles, chordae tendinae, and mitral valve leaflets and it is the key diagnostic modality for surgical planning and monitoring of EFE as it is able to ascertain both the location and depth of EFE in children with left heart obstructive disease. 20 Although our program has undertaken an aggressive approach to EFE resection, we acknowledge that other institutions have chosen not to perform resection of EFE on the basis of concerns for persistent diastolic dysfunction despite adequate relief of EFE. 21
Additional Pulmonary Blood Flow (“Super Glenn”)
In the setting of borderline left heart structures, the use of a targeted increase in pulmonary blood flow provides additional flow into the left ventricle via the mitral valve. The “Super Glenn” involves a superior cavopulmonary connection to the right pulmonary artery and an additional source of pulmonary blood flow to the left pulmonary artery (either modified Blalock Taussig shunt or right ventricle-pulmonary artery conduit) with an intrapulmonary septation with a fenestrated patch between the two sources of pulmonary blood flow. The use of a fenestrated patch (or occasionally an external band) prevents pulsatile flow in the superior vena cava. The atrial septum is also fenestrated with additional procedures typically undertaken simultaneously to address any obstruction to inflow or outflow from the left ventricle. 22 For patients who have previously undergone Stage 1 repair with placement of a Sano conduit, this conduit may be kept intact to provide the additional source of pulmonary blood flow. Data recently published from our program demonstrated a statistically significant increase in indexed left ventricular dimension. 22 That said, the use of the Super Glenn has the risk of providing excessive pulmonary blood flow, left atrial hypertension, and pulmonary hypertension that may exclude the potential for the child to revert to single ventricle palliation or even heart transplantation. The volume load on the single ventricle is also important, and while the desired effect is ventricle growth, patients must be closely monitored for the development of valvular regurgitation.
1.5 Ventricle Repair
In patients with hypoplastic right ventricle, an alternative approach to either a single ventricle palliation or biventricular repair is the 1.5 ventricle repair. This involves a superior cavopulmonary connection and a fully septated heart. Thus, the inferior vena cava venous return is to the right ventricle which provides antegrade pulmonary blood flow. The addition of the superior cavopulmonary connection decreases right ventricular volume loading without decreasing the left ventricular volume load. The presence of the right ventricular output maintains pulsatile flow to the pulmonary circulation and an ability to increase cardiac output. This technique may be used when a fenestrated ASD alone does not result in adequate growth of the small right ventricle, the right atrial pressure is too high, or if patients have low arterial oxygen saturation. There may be a role for a staged approach to this repair with recruitment of the right ventricle which may include resection of right ventricular muscle bundles in patients with hypertrophied right ventricles as is present in pulmonary atresia with intact ventricular septum. There is evidence to suggest there may be superior outcomes with 1.5 ventricular repair compared to single ventricle palliation. 23 The long-term complications of a superior cavopulmonary anastomosis in the 1.5 ventricular repair are unknown. In some instances, take-down of the superior cavopulmonary anastomosis at a future procedure allows completion of the biventricular repair. 24
“Reverse” Double Switch
In recent years, an alternative strategy utilized in a limited numbers of patients is the so-called “reverse” double switch procedure. This approach is utilized in patients with hypoplastic left ventricles unable to proceed along the biventricular conversion pathway or who have undergone a Fontan procedure. This operation involves using the right ventricle to support the systemic circulation and the left ventricle as the sub-pulmonary ventricle by performing an atrial and arterial switch operation. The experience with conversion of two patients with failed Fontan palliation to this circulation has recently been published. 25 If the left ventricle (sub-pulmonary ventricle) is not adequate then a superior cavopulmonary anastomosis is either left in place or constructed. This reverse 1.5 ventricle repair creates a septated 1.5 ventricle circulation with a sub-pulmonary left ventricle.
Valves
The valvular repairs needed for many patients in a biventricular conversion pathway can be complex. Patients with borderline left ventricles often have unicommissural or bicomissural aortic valves in association with a hypoplastic aortic annulus. In the neonatal period, there are limited options for aortic valve repair/reconstruction and the available approaches are generally best deferred until the child is older. In this circumstance, initial palliation may include a Damus-Kaye-Stansel anastomosis if there is no other obstruction to left ventricular outflow. A Ross procedure is also an option in neonates, but still remains technically challenging and is generally deferred until the child is older and of greater size. 11
Mitral valve repair is also a challenge due to the presence of varying degrees of obstruction at the subvalvular, valvular, or supravalvular level. Patients with single papillary muscle or fusion of the papillary muscles to the ventricular wall may require splitting of the LV papillary muscles and division of chordal attachments and delamination. Repair of valve stenosis may involve a commissurotomy and resection of additional fibroelastic tissue on the leaflets. Any supravalvular mitral membrane can cause obstruction and should be carefully resected. In those patients where adequate mitral valve repair is not feasible, placement of a stented bovine jugular graft (Melody) in the mitral position has been utilized. Once placed, this valve allows for progressive dilation in the cardiac catheterization laboratory which may delay the need for definitive replacement. 26
Specific Anesthesia Aspects
The development of the Complex Biventricular Repair Program at our institution has led to a steady influx of complex patients requiring involvement of the cardiac anesthesia team. These patients require the care of a cardiac anesthesiologist for extensive non-invasive imaging with echocardiography and cardiac MRI, cardiac catheterization for both diagnostic and interventional purposes, and surgical intervention in the cardiac operating room. The majority of referrals to the biventricular repair program present after at least one, if not multiple, previous surgical interventions. As a consequence, these patients have typically had many cardiac procedures and often have endured prolonged hospital admissions. A substantial number of these patients have significant non-cardiac comorbidities. With many referrals to our program coming directly from families, we have also found that the families are generally very well informed and motivated to pursue the biventricular repair pathway.
Non-Invasive Imaging
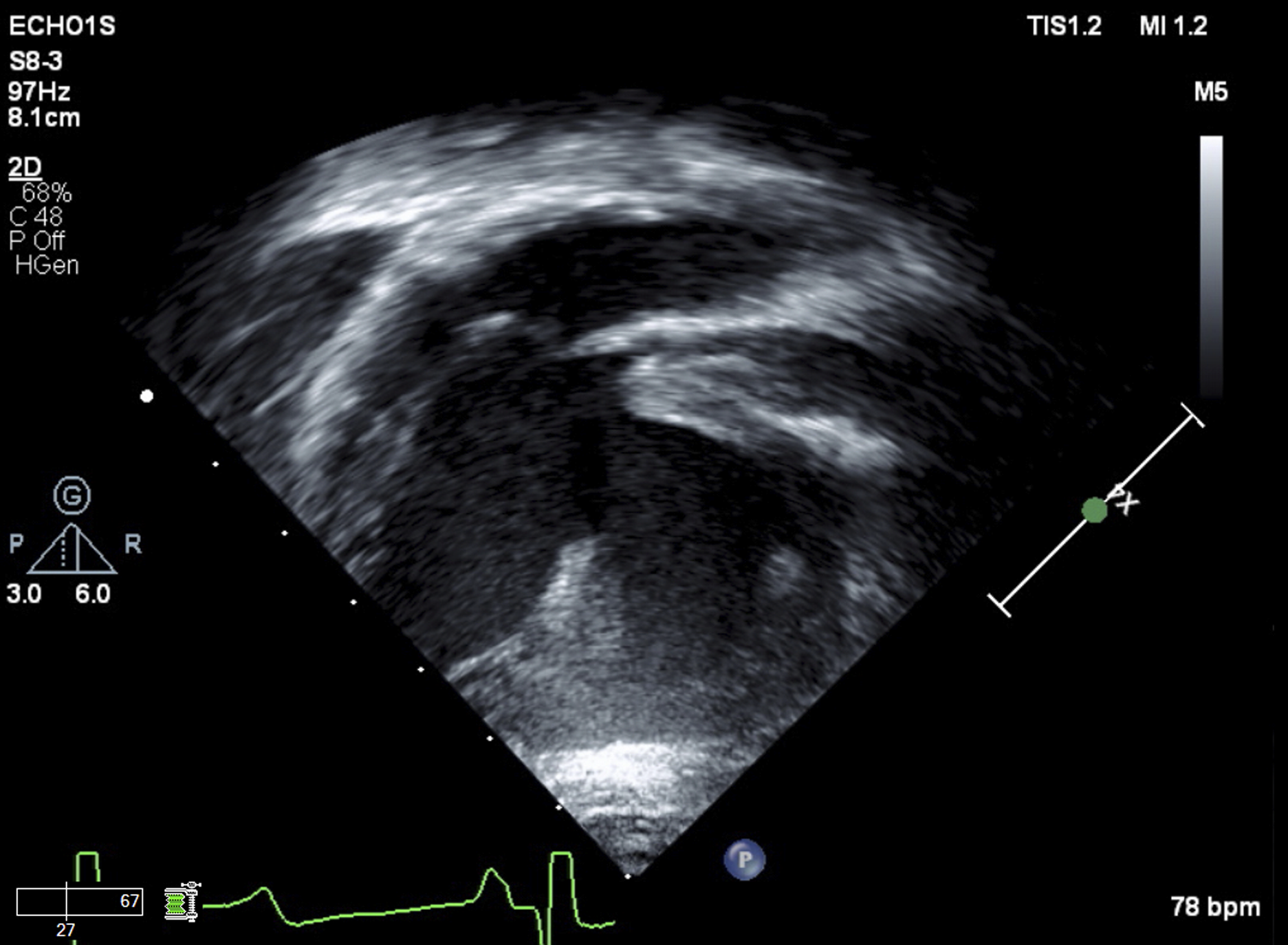
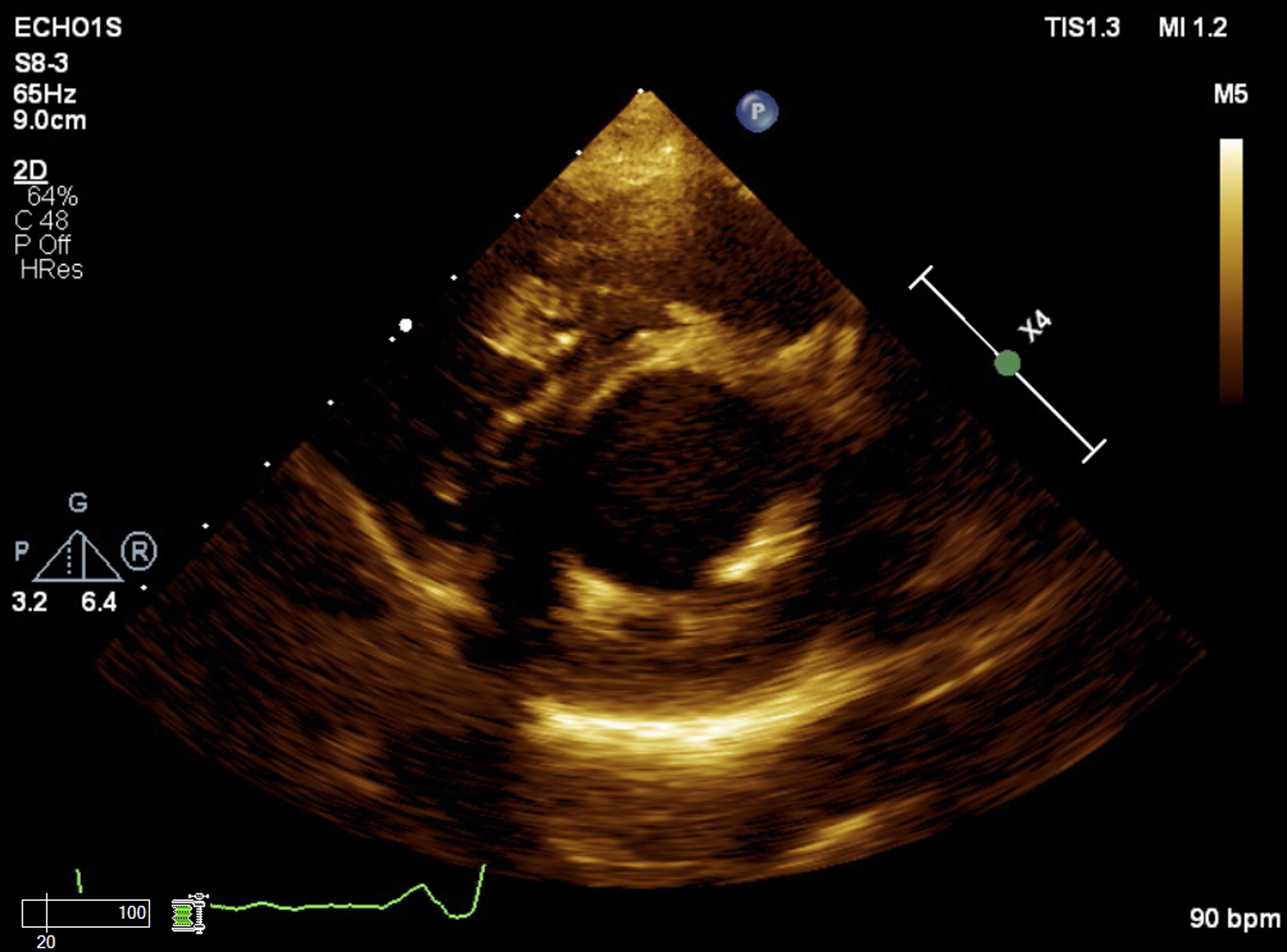
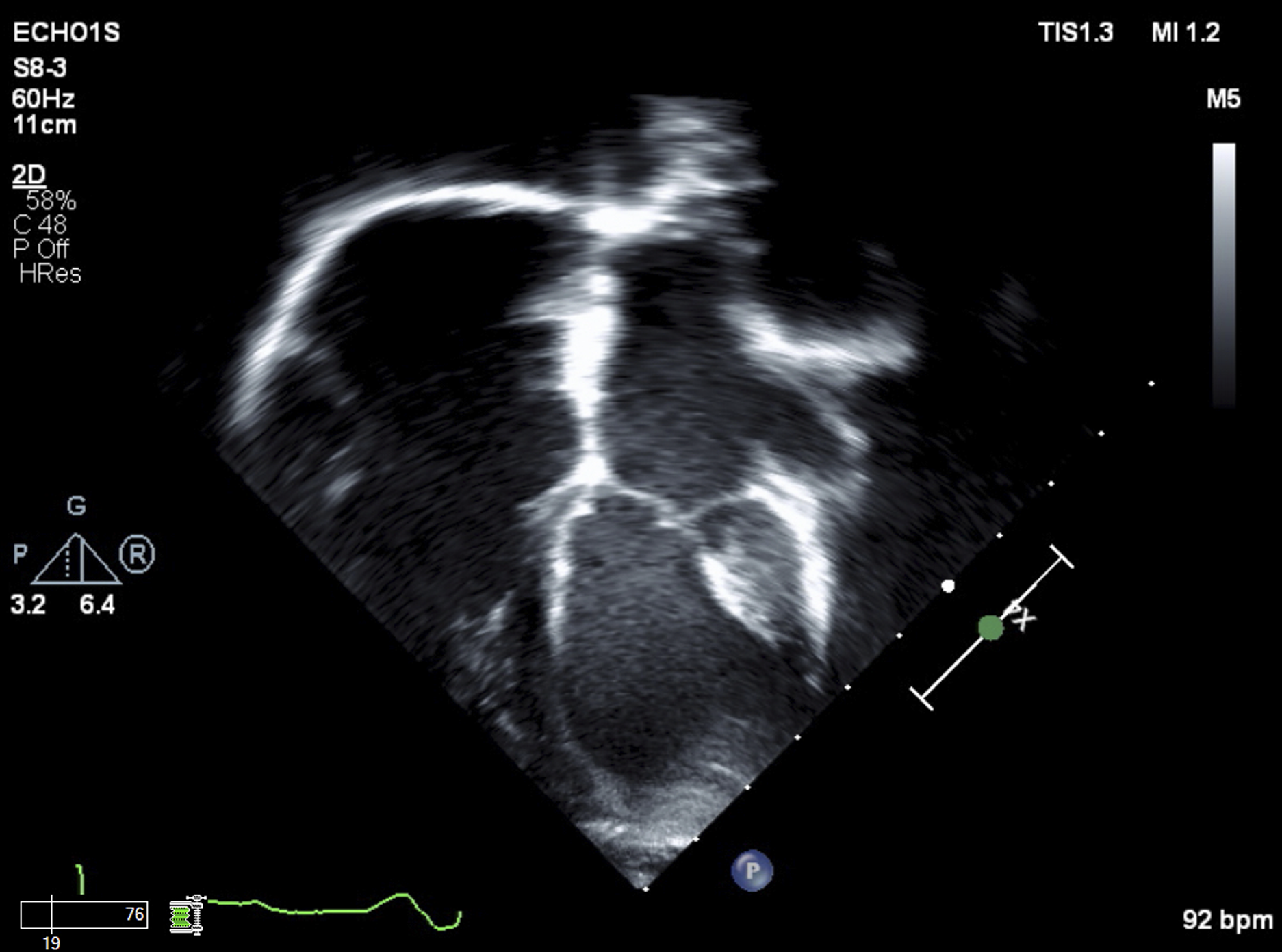
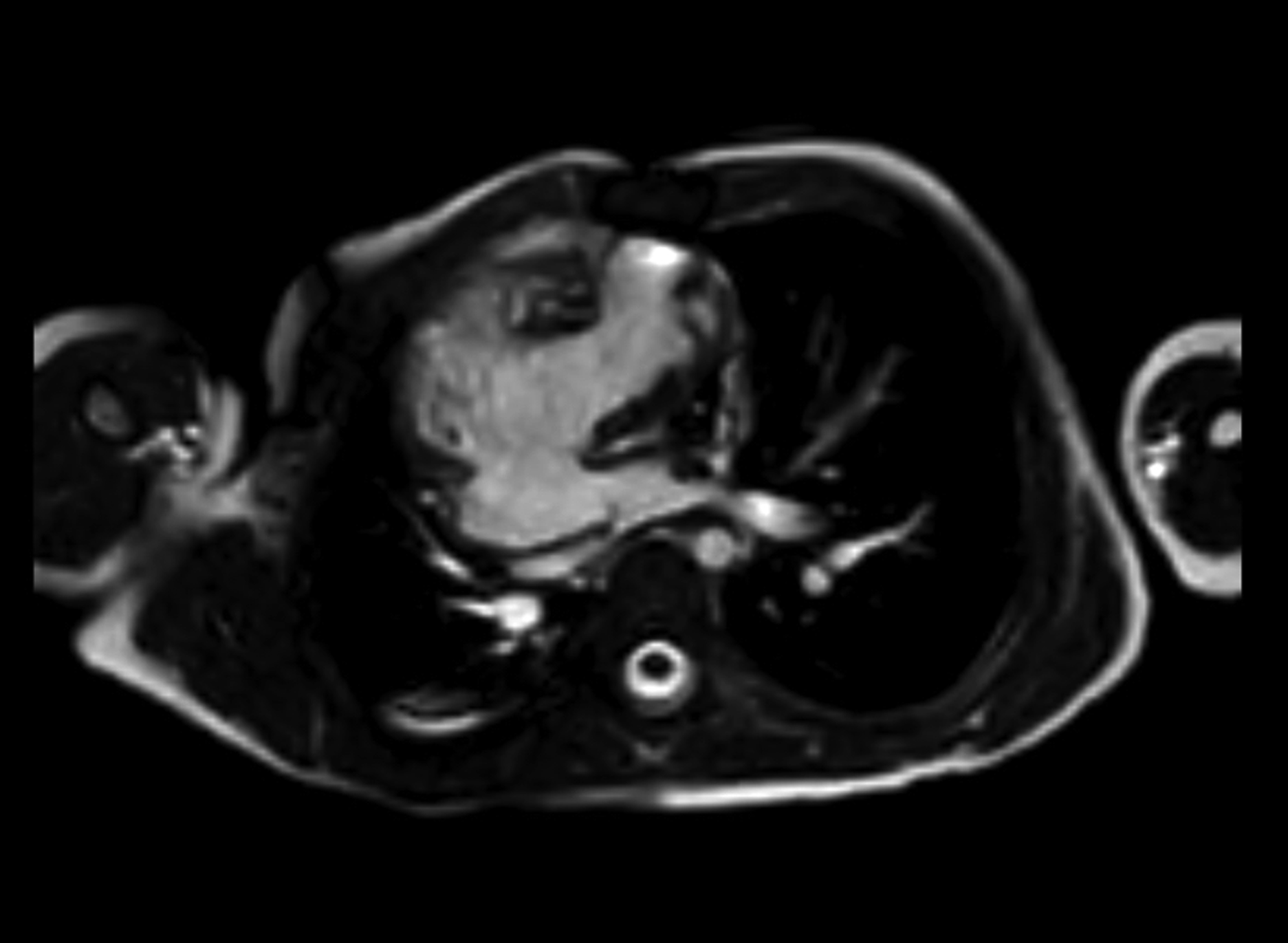
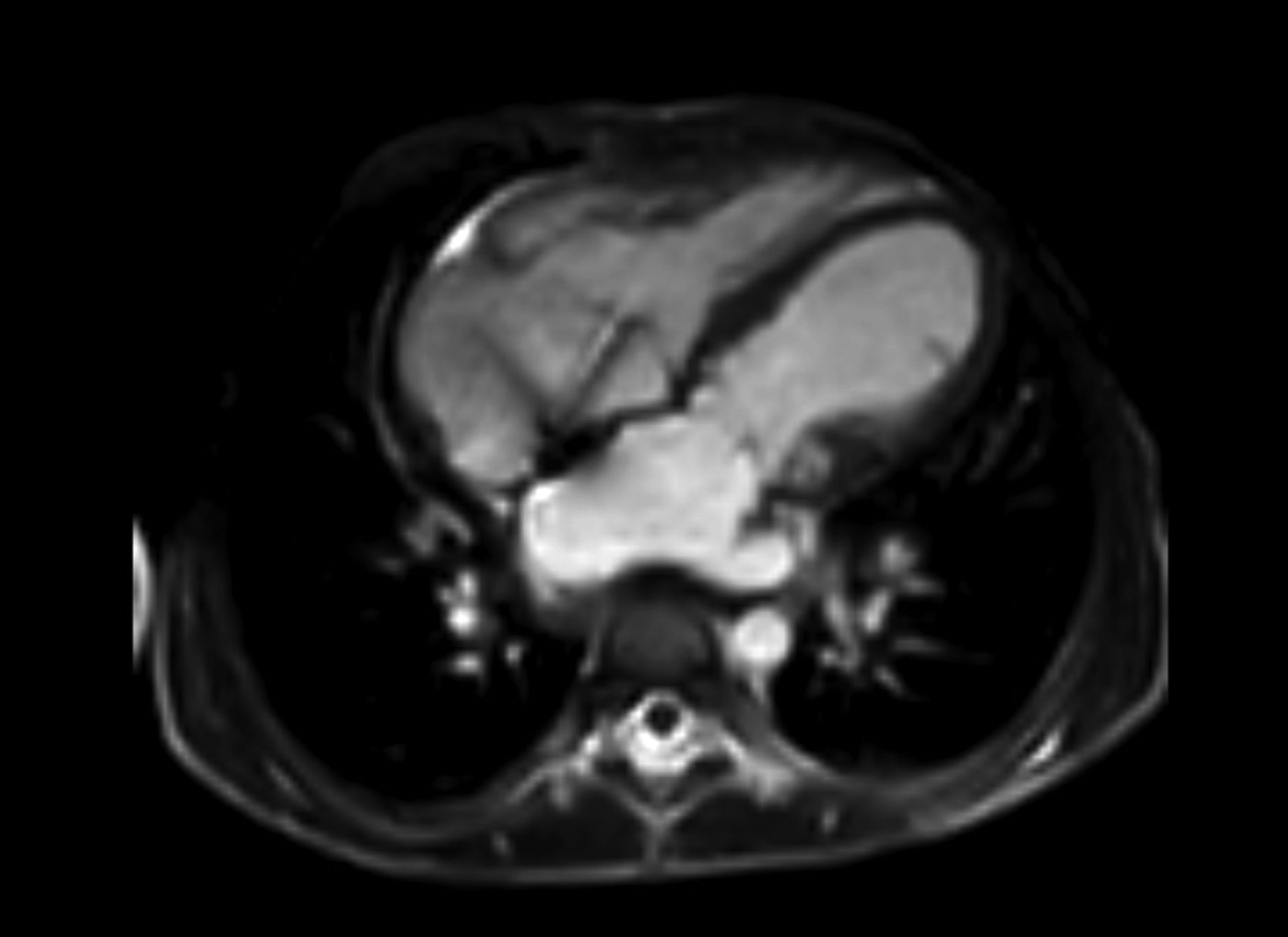
The use of non-invasive imaging, predominantly transthoracic echocardiography (Images 1, 2, 3, and 4) and cardiac MRI (Images 5 and 6) are important in the evaluation of patients undergoing consideration for biventricular staging/repair or conversion. A comprehensive echocardiographic examination provides important anatomic and function assessments with key areas of interest being systolic and diastolic biventricular function and evaluation of valve pathology. The cardiac MRI aims to quantify ventricular volumes, trans-mitral inflow, semilunar outflow, as well as the presence and extent of EFE. As most patients seen in our program are of infant/toddler age, these imaging studies are obtained under general anesthesia. Ferumoxytol, an off-label MRI contrast agent typically used in the treatment of anemia, is increasingly being used in selected patients rather than the usual gadolinium-based contrast agent. Ferumoxytol based imaging allows for improved image quality and decreased need for breath-holding during imaging.27,28 The majority of our cardiac MRIs are performed with general endotracheal anesthesia to facilitate acquisition of extended, end-expiratory breath-holding sequences. Borderline Right Ventricle Short Axis view on Transthoracic Echocardiography. Borderline Right Ventricle Long Axis view on Transthoracic Echocardiography. Borderline Left Ventricle Short Axis view on Transthoracic Echocardiography. Borderline Left Ventricle Long Axis view on Transthoracic Echocardiography. Borderline Right Ventricle 3-chamber view on Cardiac MRI. Borderline Left Ventricle 4-chamber view on Cardiac MRI.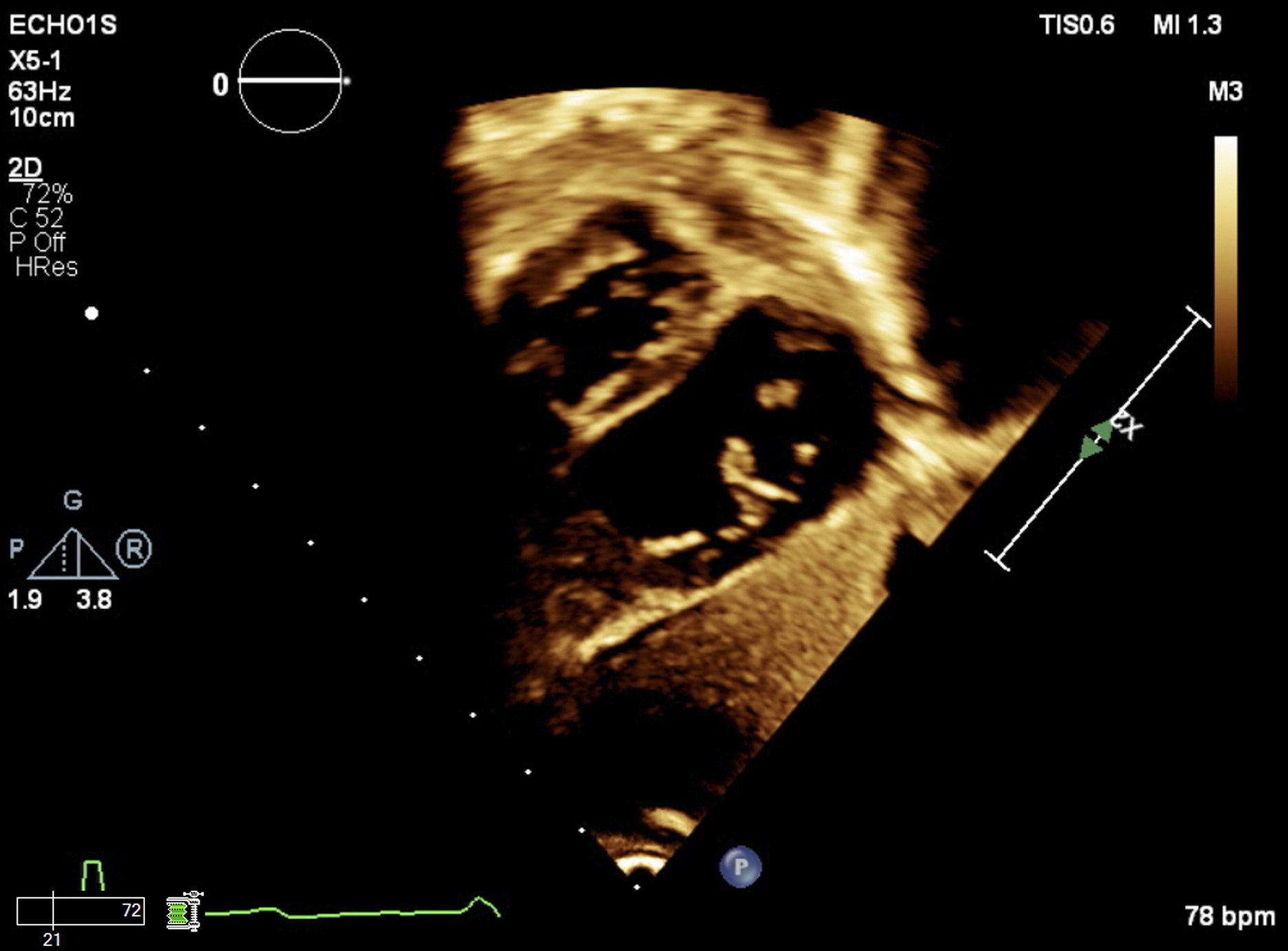
Cardiac Catheterization
Many of these patients live a great distance away from our institution and we are often consulted as to whether it would be possible for all pre-operative evaluation procedures (ie. echocardiography, cardiac MRI and cardiac catheterization) to take place on the same day to minimize inconvenience and costs to families. Our preference has been to undertake the echocardiography and cardiac MRI on the first day followed by cardiac catheterization the following day. This strategy has evolved over the last 3–4 years for several important reasons. The duration of general anesthesia associated with performing 3 complicated procedures is generally in excess of 5–6 hours and many of the patients managed this way ultimately required hospital admission rather than discharge home or to a local hotel. In addition, the logistics of scheduling the 3 procedures in one day without there being a period during which the child remains under anesthesia without a procedure being performed are prohibitively difficult. This process also allows synthesis of the cardiac MRI and echocardiographic data into the catheterization plan by the surgical, cardiology, and anesthesia teams. In addition, catheterization derived assessment of pulmonary vascular resistance can be artificially elevated due to the accumulated atelectasis that accrues following the multiple, extended, expiratory breath holds required to obtain the comprehensive cardiac MRI data. Furthermore, volume administration during the MRI and prior to cardiac catheterization may influence hemodynamic measurements, particularly the assessment of ventricular diastolic pressures.
Judicious fluid administration is essential with close monitoring of the volume given during the case. The impact of fluid boluses on the hemodynamic findings of the catheterization procedure should also be kept in mind and discussed with the interventional cardiologist to allow for accurate interpretation of the results of the procedure. If regular diuretics are held on the morning of the procedure then strong consideration should be given to administration of intravenous diuretics in the immediate post-procedural period. Our preference has been to embrace early use of inotrope infusions delivered in dilute concentrations via a dedicated peripheral intravenous catheter that is carefully monitored throughout the case for any signs of extravasation. It is very rare to place a peripheral arterial line at our institution for these patients as we are able to monitor central aortic pressures continuously (once the cardiologist has gained arterial access) for most of the case. We almost never place a central venous catheter during the cardiac catheterization. Our preference is also to undertake the cardiac catheterization under general endotracheal anesthesia with prompt extubation at the conclusion of the procedure.
Operative Management
The patients presenting for biventricular repair are amongst our most complex cases seen in the cardiac operating room. These are procedures of significant duration with long cardiopulmonary bypass and cross-clamp times. They have often had multiple previous procedures and may have significant anxiety relating to healthcare interactions as well as display tolerance to usual premedication dosages. As mentioned previously, a significant proportion of these patients have traveled from either interstate or overseas to our institution and are highly educated regarding their child’s congenital heart disease and the options for management available. They have also commonly had multiple interactions with different congenital heart disease programs that impact on their expectations relating to this procedure.
As with induction of general anesthesia for the cardiac MRI and catheterization procedures, the choice of induction method is decided by the cardiac anesthesiologist and we would stress that a thorough understanding of that particular patient’s anatomy and physiology is more important than a standardized method of induction. In the absence of intravenous access, the administration of a heavy oral (or intramuscular) premedication of ketamine and midazolam followed by supplementation with spontaneous breathing inhalation of sevoflurane not to exceed 4% inspired concentration is utilized to obtain intravenous access. Due to multiple previous operative procedures, obtaining intravenous and intraarterial access can often be challenging. Our current preference is to attempt radial or ulnar arterial access and then, if unsuccessful, proceed to place an axillary arterial line. Although a femoral arterial line may be used, care should be taken. The femoral artery is an end-artery and placing a line which may be in-situ for a prolonged period does put the lower limb at risk. Occlusions from previous line placement (whether relating to past operative procedures or catheterizations) should be evaluated using ultrasound and are not uncommon. The choice of endotracheal tube size should be carefully evaluated in the setting of anticipated prolonged intubation with care to avoid excessive pressure on the tracheal mucosa. Precautions relating to previous sternotomies and the risk of significant bleeding and inability to rapidly proceed on to cardiopulmonary bypass should be taken, including adequate large bore intravenous access and a plan for rapid institution of peripheral bypass if required. All patients receive an internal jugular central venous line unless there is an obstruction present. The catheter provides measurement of central venous, cavopulmonary or common atrial pressures depending on the patient and is useful in comprehensive analysis of post-cardiopulmonary bypass hemodynamics. In addition, superior vena cava oxygen saturation can be used as a mixed venous saturation surrogate measurement. These catheters should, however, be removed as soon as feasible in the post-operative period. If the need for prolonged central venous access is anticipated in the post-operative period, consideration should be given to placement of intracardiac lines or a cuffed tunneled central venous catheter in the operating room.
Cardiopulmonary bypass techniques vary based on the proposed operative procedure. The surgeons will use moderate hypothermia in most cases, although some patients may require deep hypothermia for both myocardial and end-organ protection, to allow for low-flow or circulatory arrest if needed. Circulatory arrest may be required if there is injury to a structure on sternal re-entry, to repair the aortic arch, for repairs involving the pulmonary veins, or for excessive pulmonary venous return. Induced ventricular fibrillation in association with decompressed ventricular cavities can be used to minimize cross-clamp times. Hepatic hypoperfusion due to the presence of major aortopulmonary collaterals during bypass can present a challenging scenario, particularly in certain Fontan patients with borderline hepatic function. Coiling is often undertaken during the pre-operative cardiac catheterization in order to prevent this. Multiple doses of cardioplegia may be necessary if a long cross-clamp time is required.
In the immediate post-bypass period, atrial and post-capillary pulmonary hypertension is expected due to small ventricular cavity size and ventricular diastolic dysfunction. Ventricular systolic dysfunction has not typically been a significant challenge despite the long cardiopulmonary bypass runs. There may be a need for inotropic support and drug selection should be individualized based on the patient’s particular needs as regards heart rate, inotropy, lusitropy, and afterload. It is not uncommon to have to “switch” inotropes when the effects of a particular agent such as tachycardia prove to be detrimental to the patient’s physiology and hemodynamics. Although ventricular systolic dysfunction may be improved with the use of inotropes, there are currently no potent lusitropic agents available. 29
Dopamine, epinephrine, norepinephrine, and milrinone, alone or in combination, have all been used effectively in our institution. Milrinone should only be employed after careful consideration is given to the target systemic vascular resistance for a particular patient as the vasodilator effects of this agent predominate over its inotropic properties.30,31 An intracardiac pressure monitoring line for the relevant atrium (depending if hypoplastic right or left ventricle) is placed and transduced prior to weaning off bypass. Due to the uncertain location of conduction pathways in these patients, arrhythmias and/or atrioventricular block is common and should be addressed early with temporary epicardial pacing. We have found it essential to aggressively treat and manage arrhythmias to maintain atrioventricular synchrony. Heart block is problematic because unipolar ventricular pacing with temporary wires does not produce a normal ventricular contraction pattern and can compromise ventricular performance. Use of bipolar leads, analogous to the approach employed in cardiac resynchronization therapy (CRT) may need to be considered. If it is suspected that low cardiac output and/or peripheral vasoconstriction results in an inaccurate representation of central aortic pressure on the peripheral arterial line waveform, transduction of central aortic pressure from the surgical field may be necessary to make informed decisions regarding volume and inotrope administration. Transesophageal and epicardial echocardiography are utilized to assess the completeness of the surgical repair including atrioventricular and semilunar valve function, baffle/conduit patency and residual VSD, ventricular filling and contractility function, and the direction and size of the shunt through the atrial fenestration. If significant residual lesions are detected, a thoughtful discussion regarding whether the lesions should be addressed in the operating room or the catheterization suite should be conducted.
There may be significant bleeding following termination of CPB and it can be exceptionally difficult to manage, due to the presence of poor ventricular compliance in these often-small ventricles. Overzealous volume replacement should be avoided and administration should be guided by constant surveillance of atrial pressures. We usually aim for a hematocrit greater than 35% and our surgeons pursue aggressive hemostasis prior to leaving the operating room. Consideration should be given to the fact that overzealous administration of coagulation factors places the patient at risk for thrombotic complications including central venous thrombus and fenestration closure. 32 We utilize thromboelastography obtained during rewarming on CPB and following protamine administration to guide platelet transfusion and to estimate the effect of plasma transfused with platelets on the fibrinogen concentrations. 33
Management in the Cardiac Intensive Care Unit
The anticipated post-operative course in the cardiac intensive care unit varies greatly depending on the specific surgical procedure. On one end of the spectrum, a patient undergoing a brief procedure to provide an accessory source of pulmonary blood flow can be expected to advance to early extubation, whereas those undergoing a long, complex biventricular conversion should be anticipated to require a longer duration of ventilatory and hemodynamic support. Ventilator management should be directed toward target blood gases with the lowest possible mean airway pressure. This requires judicious use of positive end-expiratory pressure (PEEP), an I:E ratio of 1:2.5–1:3, a low respiratory rate, and tidal volumes of 8–10 ml/kg. This is particularly important in patients with impaired sub-pulmonary ventricular function and those with limited pulmonary blood flow or a high dead space to tidal volume ratio. Atrial hypertension secondary to ventricular diastolic dysfunction is very common in this patient population. Rapid, large fluid boluses are very poorly tolerated and should be avoided if possible. Any fluid administration should be done while carefully monitoring the atrial pressures and assessing the pulse pressure trace for evidence of preload recruitable stroke work.
The use of sedation, analgesia, and continuous muscle relaxation is typical after biventricular conversion patients in the early post-operative period, with an expected prolonged period of low cardiac output and vasoactive requirements. Severe end-organ complications relating to this period with renal and hepatic dysfunction, gastrointestinal ischemia and even limb ischemia can occur but are rare. Altered temperature regulation is often seen in biventricular staging and conversion with the occurrence of fevers commonly in the first 72 hours. We institute a protocol of close temperature monitoring with active cooling to maintain normothermia or mild hypothermia. Arrhythmias or tachycardia may not be well tolerated. Patients require atrioventricular synchrony if possible, and patients are often placed on AAI settings with a backup rate in the post-operative setting. Patients who develop sudden arrhythmias are at significant risk of deterioration and require urgent management and correction.
The need for reinterventions in the post-operative course is not uncommon. In particular, premature closure of the atrial fenestration may require a return to the catheterization laboratory for re-establishment of an atrial septal defect. The atrial fenestration should be closely evaluated by echocardiography if concerns of excessively high or increasing atrial pressures. Consideration should also be given to the presence of major aortopulmonary collaterals and the need for coiling in the setting of increased left atrial pressures if these have not been addressed pre-operatively. If the patient fails to progress as expected, the possibility that there is a residual lesion burden, such as residual shunts, any valve stenosis or regurgitation, and/or outflow tract obstructions should be entertained. Patients with hypoplastic right ventricles undergoing conversion to a biventricular circulation are vulnerable to prolonged periods of right atrial hypertension that can result in hepatic and renal dysfunction and right ventricular failure, particularly in the presence of a low mean arterial pressure. It may be necessary to perform a superior cavopulmonary anastomosis to decrease right-sided volume load. In the setting of no addressable residual lesions and poor hemodynamics, consideration should be given to take-down of the biventricular repair to an intermediate stage to facilitate clinical improvement.
Future Innovations
There are several new and innovative modalities that are currently being explored. 3D printing (with data obtained from cardiac MRI) to facilitate complex surgical planning and management has been used, but it is expensive and requires considerable time to create. Novel software which can 3D model the heart and allow the surgeon to rotate/alter it in real-time before and during the procedure is under development. In the cardiac catheterization laboratory and in the operating room, use of conductance catheter technology both before and after a fluid challenge (5-10 ml/kg depending on the physiology) is used to obtain ventricular pressure-volume loops to characterize compliance and ventriculoarterial coupling (see Figure 4). Example of ventricular pressure-volume loops obtained during cardiac catheterization. This patient is a 4 year old with severe aortic stenosis that underwent staged palliation to a Super Glenn circulation as part of biventricular staging. The figure shows left ventricular pressure-volume loops prior to their biventricular conversion with baseline in yellow, caval occlusion in red and atrial septal defect occlusion in blue. It demonstrates abnormal diastolic function related to impaired passive filling, diminished systolic function with dP/dT max of 685 mmHg/s (normal systemic LV would be ∼1200 mmHg/s) and highly abnormal diastolic function in response to volume challenge.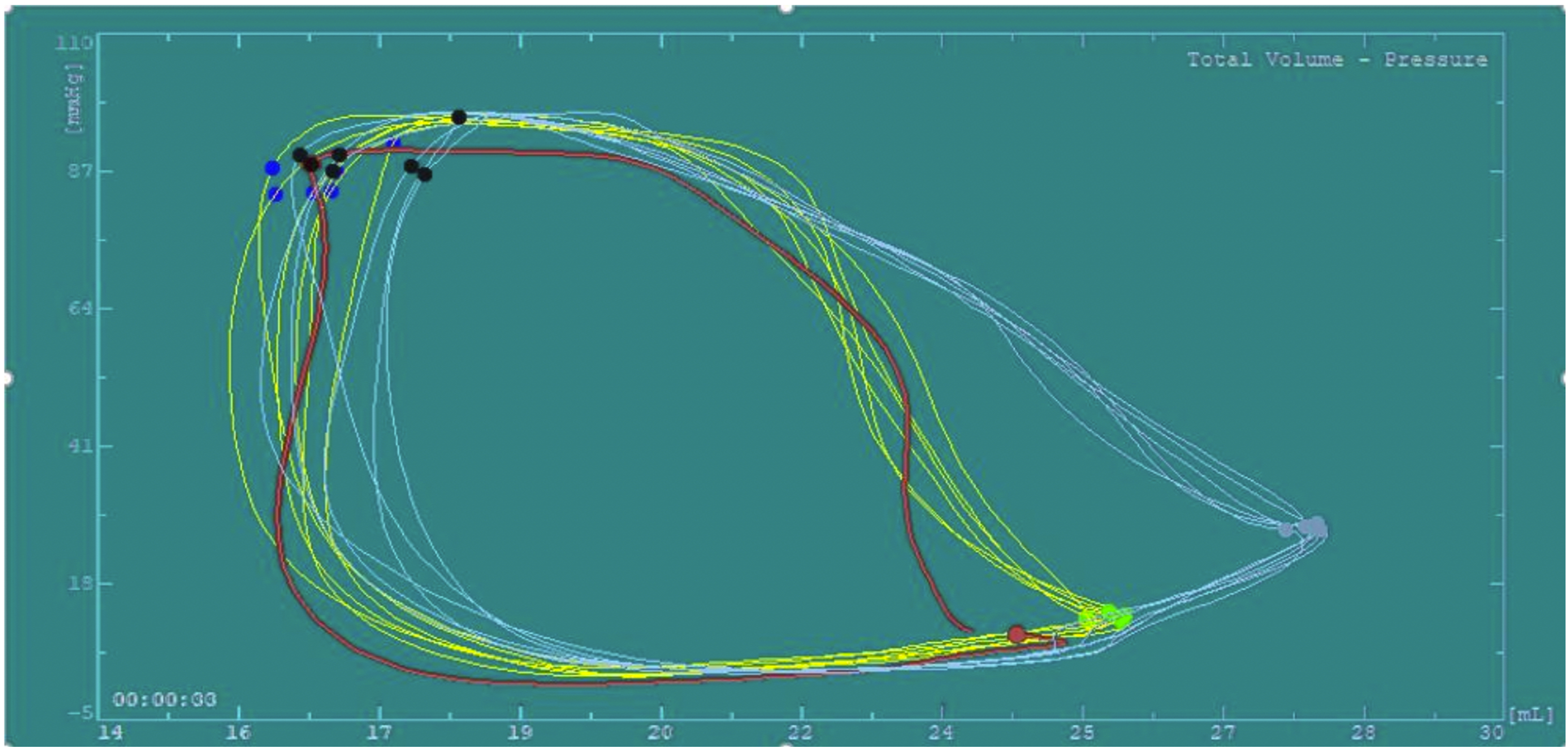
Intra-operative electrophysiological mapping in the operating room is being used to decrease the risk of damage to the conduction system and subsequent post-operative heart block. 34 This is performed on an empty, beating heart and using a 16-electrode grid catheter while supported with moderately hypothermic cardiopulmonary bypass. This mapping requires close collaboration between the cardiac surgeons and electrophysiology cardiologists and the use of 3D heart models to enhance this mapping is being explored.
The novel use of mitochondrial transplantation is another innovation that may serve to mitigate the effects of ischemia-reperfusion injury in this high-risk patient population. This technique has been studied since the early 2000s with transplantation of fresh, viable mitochondria from non-ischemic tissue (typically either pectoralis major or rectus abdominis skeletal muscle). 35 The mitochondria are isolated from the skeletal muscle sample in a process that takes under 30 minutes and that can be performed in either the cardiac operating room or cardiac intensive care unit. The isolated mitochondria are then injected directly into the affected areas of myocardium (often guided by echocardiography). Alternatively, they can also be administered intravascularly either via direct intracoronary injection or aortic root injection. The mitochondrial transplantation has been shown to increase myocardial adenosine triphosphate (ATP) levels and improve mitochondrial protein pathways required for cellular respiration. Following an ischemic event with subsequent revascularization, this treatment modality may improve myocardial function and recovery. 36 The use of mitochondrial transplantation is in the early stages of use in the biventricular staging patients with compassionate use only as a rescue therapy. Its role in the future management of biventricular repair patients is yet to be determined.
Conclusions
Biventricular repair is considered in patients who are born with hypoplastic right or left ventricles, as well as patients with complex anatomy. Anesthesiologists must be familiar with the various physiologies encountered in this heterogenous patient population and understand the goals of biventricular staging and completion. Ultimately, more studies are needed to define the indications and provide long-term survival and functional outcomes data.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.