
Abstract
Background
Transcatheter edge-to-edge repair (TEER) with MitraClip is a safe and effective alternative to surgical mitral valve repair/replacement in patients with high operative risk. Pleth Variability Index (PVI) is a non-invasive, dynamic index based on analysis of the respiratory variations in the plethysmographic waveform recorded transcutaneously by the pulse oximeter.
Objectives
The objective of the study was to evaluate if the hemodynamic effect of improved left-sided output after successful transcatheter mitral valve repair would lead to a significant change in PVI, and if it would correlate with the decrease in left atrial pressure (LAP).
Design
Prospective, observational cohort study (ClinicalTrials.gov NCT03993938).
Setting
Single academic hospital in Detroit, Michigan (USA), from October 2019 to February 2021.
Participants
The authors included adult patients with severe mitral regurgitation who underwent successful MitraClip placement.
Measurements and Main Results
Of 30 patients, all components of the LAP (a wave, v wave, and mean) decreased significantly after successful MitraClip placement (P < .01). The median (IQR) PVI increased from 21 (11-35) to 23 (13-38) after clip placement; however, this change was not statistically significant (P = .275). No significant correlation between change in PVI and change in LAP was observed (P = .235).
Conclusions
In patients with severe mitral regurgitation, successful MitraClip resulted in a significant reduction in LAP without a significant change in PVI. A larger sample size may provide more insight on the utility of using PVI as an indicator of LAP change in patients with mitral regurgitation.
Introduction
Mitral valve disease, especially mitral regurgitation, is one of the most commonly encountered valvular heart pathologies. 1 Although surgery is the preferred therapy for primary severe mitral regurgitation, about 50% of patients have prohibitive risk factors, such as age and/or comorbidities. 2 Transcatheter mitral valve repair using transcatheter edge-to-edge repair (TEER) with MitraClip® (Abbott Vascular, Menlo Park, CA) is a safe and effective alternative to surgical mitral valve repair/replacement for patients with severe mitral regurgitation and high risk for operative morbidity and mortality.3-6 Successful TEER requires intraprocedural quantification of mitral regurgitation by echocardiography and hemodynamic monitoring. 7 Use of transesophageal echocardiography (TEE) is standard during TEER procedures. Some TEE measures of mitral regurgitation are qualitative or semiquantitative, and there can be significant inter-operator variability with assessments. Studies show that accurate TEE assessment after MitraClip therapy is limited by acute changes in annulus geometry, multiple jets, and eccentric regurgitation.8,9 Thus, TEE alone may not reflect a comprehensive hemodynamic assessment during MitraClip procedures.
Left atrial pressure (LAP) is frequently used in conjunction with TEE for quantitative assessment before and after TEER. LAP should decrease significantly after TEER completion due to the reduction in mitral regurgitation. 10 LAP in MitraClip is measured using a transseptal sheath prior to the insertion of the clip delivery system and is repeated using the steerable guide catheter. Studies indicate that intraprocedural LAP monitoring translates into a superior intraprocedural result and a greater reduction in mitral regurgitation severity. 7 However, it has also been shown that LAP monitoring should ideally be performed continuously rather than as a static measurement before and after TEER, which can burden the procedure with an additional invasive apparatus for the measurement. 11 This is due to the dynamic nature of the left atrial hemodynamics and the influence of loading conditions as well as the shape and function of the left atrium and left ventricle which would be more reliably monitored with a continuous indicator. 7
The Pleth Variability Index (PVI) is a non-invasive, dynamic index based on analysis of the respirophasic variations in the plethysmographic waveform recorded transcutaneously by the pulse oximeter. 12 Studies have shown that PVI is accurate in predicting fluid responsiveness in mechanically ventilated adult patients,13,14 and has been shown to predict volume expansion induced changes in cardiac index interoperatively during cardiac surgery. 15 We hypothesized that the hemodynamic effect of improved cardiac output after successful TEER would lead to the better conductance of the respirophasic variations leading to a change in the PVI, and that the percentage of change (ΔPVI) would correlate with the percentage of change of the gold standard index, the LAP (ΔLAP). This could lead to the use of PVI as an additional non-invasive index to optimize MitraClip placement.
The primary aim of this study was to correlate ΔLAP and ΔPVI after successful MitraClip. The secondary aims included comparing the LAP and PVI values before and after MitraClip, and to evaluate the effect of possible confounders including rhythm and co-existing valvular abnormalities.
Materials and Methods
This prospective, observational cohort study was approved by the Henry Ford Hospital Institutional Review Board (IRB #13004) and was registered at ClinicalTrials.gov (NCT03993938, Principal investigator: Ashwin Vaidyanathan MD, Date of registration: June 21, 2019) prior to patient enrollment. Patients with moderate-to-severe mitral regurgitation (3+ and 4+) undergoing transcatheter mitral valve repair with MitraClip (Abbott Vascular, Santa Clara, CA) were recruited for the study between October 2019 and February 2021. The Institutional Review Board granted a waiver of informed consent because of the observational nature of the study and because the study followed standard-of-care management for MitraClip placement. Patients without successful MitraClip placement were excluded from the study. Successful MitraClip placement was defined as intraprocedural clip deployment with post-clip mitral regurgitation grading of less than or equal to 2+ on TEE. 16 This manuscript adheres to the applicable STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines.
The Masimo Radical-7 (Masimo Corporation, Irvine, CA) probe was attached to the patient’s finger along with standard American Society of Anesthesiologists monitors at the start of the procedure. All patients received general anesthesia with endotracheal intubation. Baseline hemodynamic parameters including heart rate, systemic blood pressure, and PVI value (from the Radical-7 probe) were recorded by the anesthesia provider after endotracheal intubation and prior to the start of the procedure. Arterial lines were placed by the proceduralist for some patients, based on comorbidities such as low ejection fraction.
Right femoral vein access was obtained under ultrasound guidance, and right heart catheterization was performed. The MitraClip delivery system was steered under TEE guidance. Intraprocedure LAP (a wave, v wave, and mean) was recorded by the proceduralist prior to and after MitraClip deployment. For each measurement of the LAP, 3 readings of the PVI at 1-minute intervals were recorded. The average of these 3 PVI readings was recorded as the PVI mean. If post-clip deployment mitral regurgitation was found to be greater than mild based on TEE assessment, the process was repeated with additional clip(s) to reach mild mitral regurgitation. The hemodynamic variables during the successful clip attempt were recorded for statistical analysis.
Statistical Analysis
Patient Demographics.
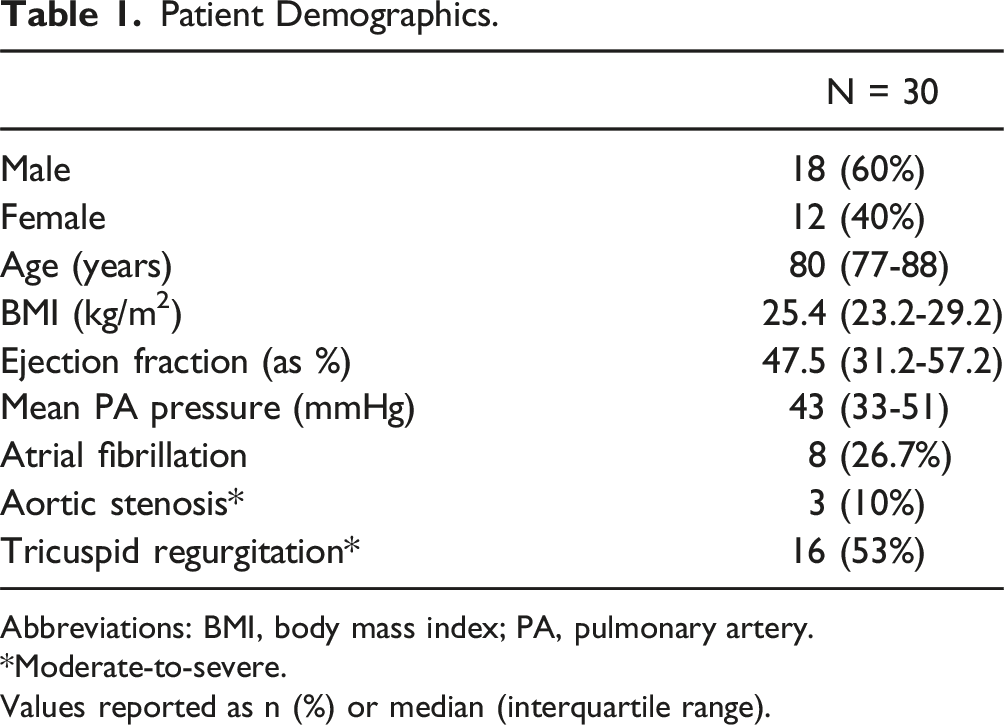
Abbreviations: BMI, body mass index; PA, pulmonary artery.
*Moderate-to-severe.
Values reported as n (%) or median (interquartile range).
Results
Socio-Demographic and Baseline Parameters
A total of 32 patients who underwent TEER with MitraClip between October 2019 and February 2021 were recruited. Two patients were excluded due to unsuccessful MitraClip procedure. The remaining 30 patients were included for statistical analysis (18 [60%] male and 12 [40%] female). The median age was 80 (IQR, 77-88) years. The median patient BMI (body mass index) was 25.4 kg/m2 (IQR, 23.2-29.2). The major underlying rhythms were sinus and paced rhythms (73.3%) with 8 patients (26.7%) having a diagnosis of atrial fibrillation (Table 1).
A total of 23 (77%) patients had pre-procedure severe mitral regurgitation and 7 (23%) had moderate-to-severe mitral regurgitation. There were 2 patients who had co-existing moderate aortic stenosis and one patient had severe aortic stenosis.
Procedural Parameters
The mean ± SD procedure duration defined as the time from intubation to placement of successful MitraClip was 152 ± 34 minutes. The mean ± SD intraprocedure tidal volume was 7.1 ± .5 mL/kg with a positive end-expiratory pressure of 5 cm H2O. There were 14 patients who received a single clip, 13 who required a second clip, and 3 patients who required a third clip for a successful procedure. A median of 800 (IQR, 700-1000) mL of intravenous crystalloids were administered over the duration of the procedure, and 3 patients required the initiation of intraprocedure vasopressor infusion (norepinephrine) due to systemic hypotension. There was one patient who had new onset atrial fibrillation at the time of MitraClip placement, which was cardioverted to sinus rhythm. Post-procedure mitral regurgitation severity was trace in 21 patients (70%), with the remaining 9 patients having mild mitral regurgitation.
Left Atrial Pressure
The LAP (v wave) before MitraClip placement ranged from 8 to 68 with a median of 23 mmHg, the LAP (a wave) ranged from 2 to 33 with a median of 13 mmHg, and the LAP (mean) ranged from 3 to 34 with a median of 13 mmHg. There was a significant reduction in all 3 components of the LAP (v wave, a wave, and mean) after successful placement of the MitraClip, with the v wave value showing the greatest significant change (P < .001) with a median reduction of 26.1% (Figure 1). Box-and-whisker plot of left atrial pressure (v wave and mean) before successful clip deployment (“pre-MitraClip”) and after clip deployment (“post-MitraClip”).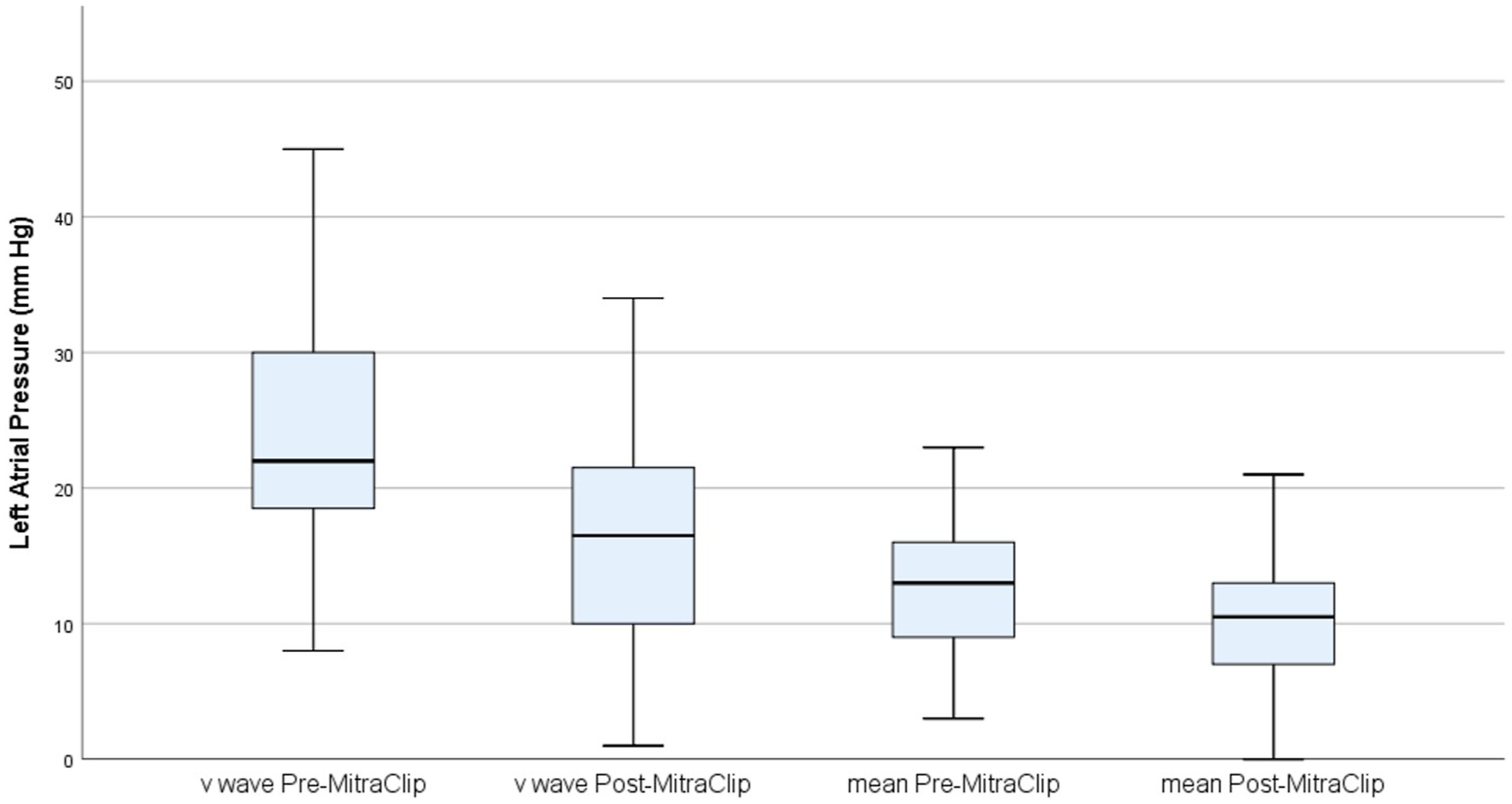
Pleth Variability Index
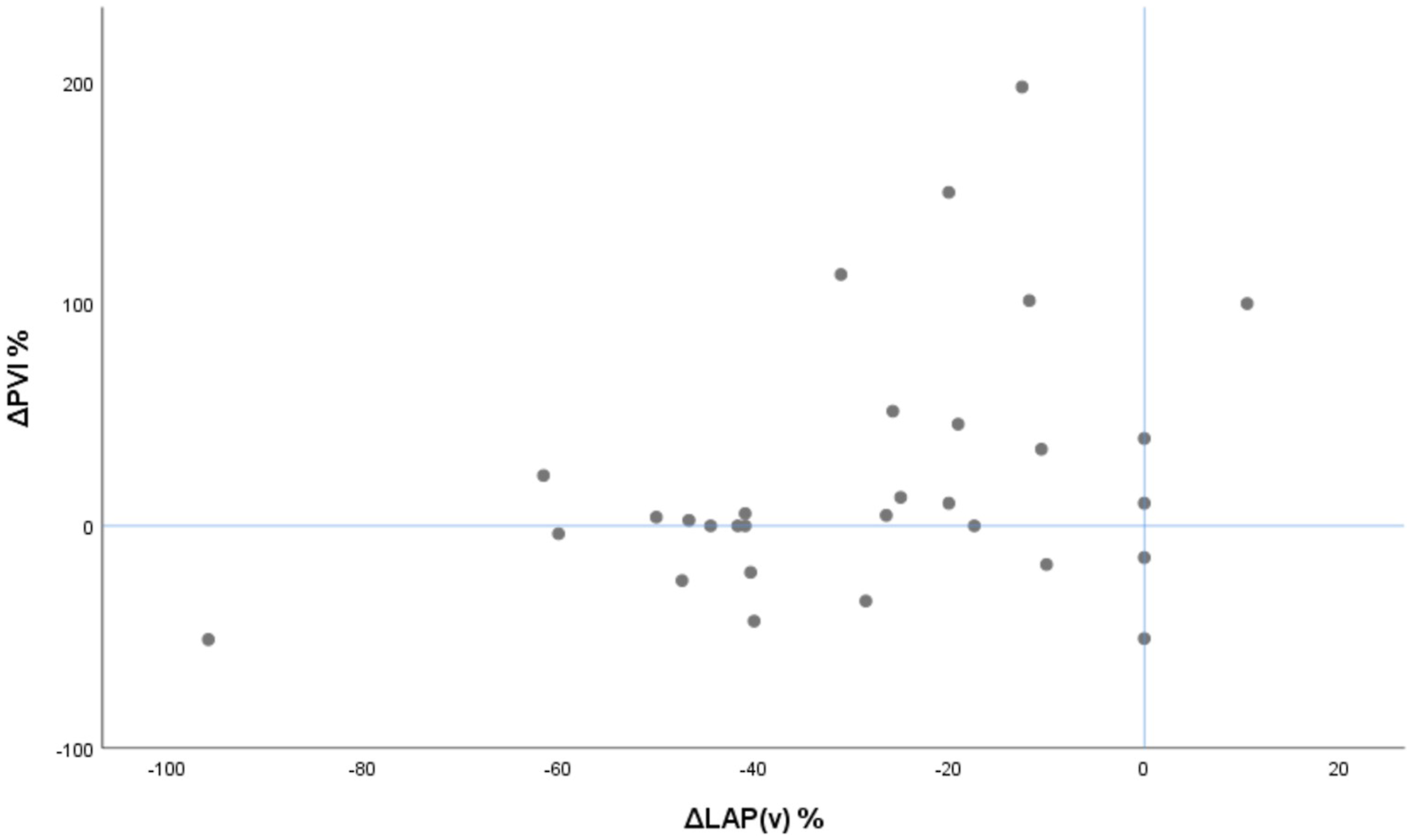
The pre-procedure PVI values ranged from 6 to 49, with a median (IQR) of 21 (11-35). After successful placement of MitraClip, the overall median PVI value increased to 23 (13-38); however, this change in PVI was not statistically significant (P = .275) (Figure 2). The Spearman correlation between ΔLAP (v wave) and ΔPVI was not statistically significant (P = .235) (Figure 3). If the patients with atrial fibrillation were excluded from the analysis, the ΔLAP (v wave) and ΔPVI correlation was still not statistically significant (P = .117). Subgroup analysis comparing median PVI values in patients with atrial fibrillation and PVI values in patients without atrial fibrillation did not show any statistically significant difference between groups (P = .078). Box-and-whisker plot of PVI value before successful clip deployment (“pre-MitraClip”) and after clip deployment (“post-MitraClip”). Scatter plot of LAP v wave percentage change with PVI percentage change.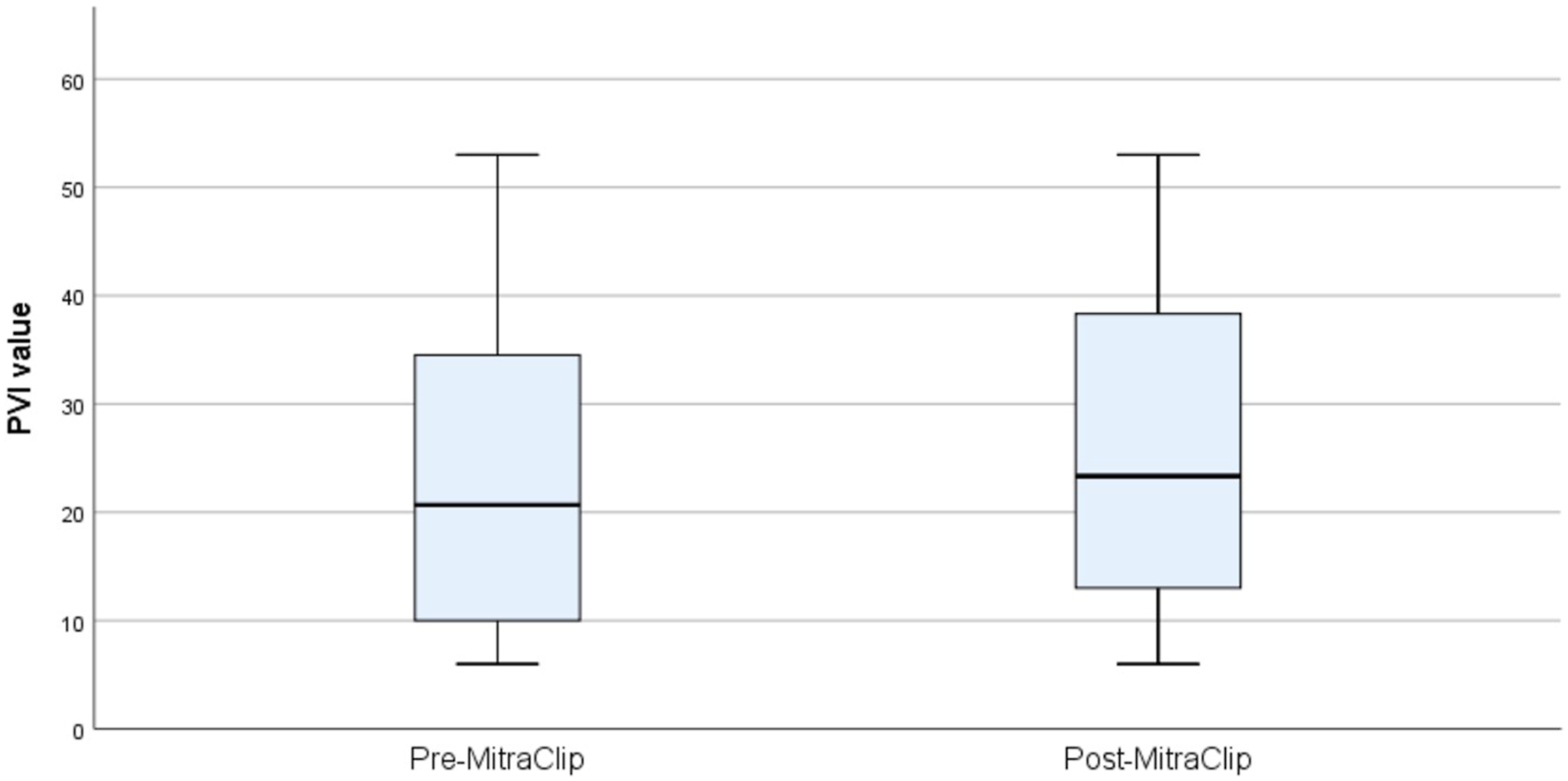
Discussion
To our knowledge, our analysis is the first to compare the PVI, a non-invasive dynamic indicator of volume status, with directly measured intracardiac pressures (LAP) during MitraClip. A statistically significant reduction in all 3 components of the LAP (v wave, a wave, and mean) was found following successful MitraClip insertions, agreeing with findings well described in the literature.7,17 The PVI value was observed to increase after MitraClip placement, but this change was not statistically significant and the increase did not significantly correlate with changes in LAP.
Improvement of systolic forward flow and cardiac output following successful MitraClip is associated with more favorable clinical and anatomic outcomes including all-cause mortality at 3 years. 18 These hemodynamic changes associated with MitraClip are more important predictors of clinical outcomes than the echocardiographic improvement of mitral regurgitation. 7 The improvement in systolic forward flow associated with a reduction in LAP and regurgitant volume as described in our study would theoretically better allow the transmission of respirophasic changes onto the plethysmographic waveform which determines the PVI value. 15 As such, the PVI value would be expected to increase after the improvement of mitral regurgitation. However, while LAP decreased significantly in our study, there was no significant change in PVI.
While LAP decreased significantly, concurrent improvement in stroke volume and cardiac output was not reflected in PVI. Correction of MR during MitraClip has been associated with increased afterload, which may be one potential confounder. 19 PVI also correlates poorly to fluid responsiveness in aortic surgeries due to diastolic dysfunction, which occurs frequently in severe mitral regurgitation. 20 Also, plethysmographic waveform is determined by arterial and venous distensibility and not dependent on stroke volume alone. 21 Chronic mitral regurgitation especially with co-existing systemic hypertension has been associated with reduced arterial elasticity and resultant arterial stiffness. This chronic change in the vasculature in this patient population may be an important consideration against the utility of PVI and use of plethysmographic-based indices to predict volume responsiveness.
Limitations
This study is limited by the small sample size, and the role of potential confounders influencing left atrial hemodynamics including atrial fibrillation and volume status. Although PVI has not been thoroughly studied in atrial fibrillation, parameters such as pulse pressure variation, systolic pressure variation, and stroke volume variation, which rely on similar principles, have been shown to be unreliable when estimating volume status in patients with atrial fibrillation. 13 We included patients with atrial fibrillation in our study, to evaluate the trend in PVI rather than the absolute value, and no significant differences in PVI were detected in patients with or without atrial fibrillation in our sample. The precise role of each individual confounding factor with potential use of adjusted regression models could not be evaluated in this study due to the small sample size. In addition, although we did not record LAP or PVI continuously, by measuring the LAP and PVI at the key pre- and post-MitraClip endpoints, we wished to provide a first-look at the potential utility of this dynamic indicator which could be easily expanded to continuous monitoring.
Conclusion
A continuous, non-invasive hemodynamic monitor could be highly beneficial during MitraClip procedures. In the present study, MitraClip placement resulted in a significant reduction in LAP. However, there was not a concomitant change in PVI to suggest utility of this device in this context. While further exploration may provide more insight into the utility of using PVI as a tool to ensure successful MitraClip placement, this study suggests caution in the use of non-invasive indicators for complex hemodynamic states.
Footnotes
Acknowledgments
We acknowledge the entire department of anesthesiology at Henry Ford Hospital, Detroit, MI for their support and assistance with patient recruitment, and data collection. We appreciate the assistance provided by Xiaoxia Han, PhD, with statistical analysis and by Karla Passalacqua, PhD, with manuscript proofreading. No AI or ChatGPT was used or No part of the paper was “generated.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.