
Abstract
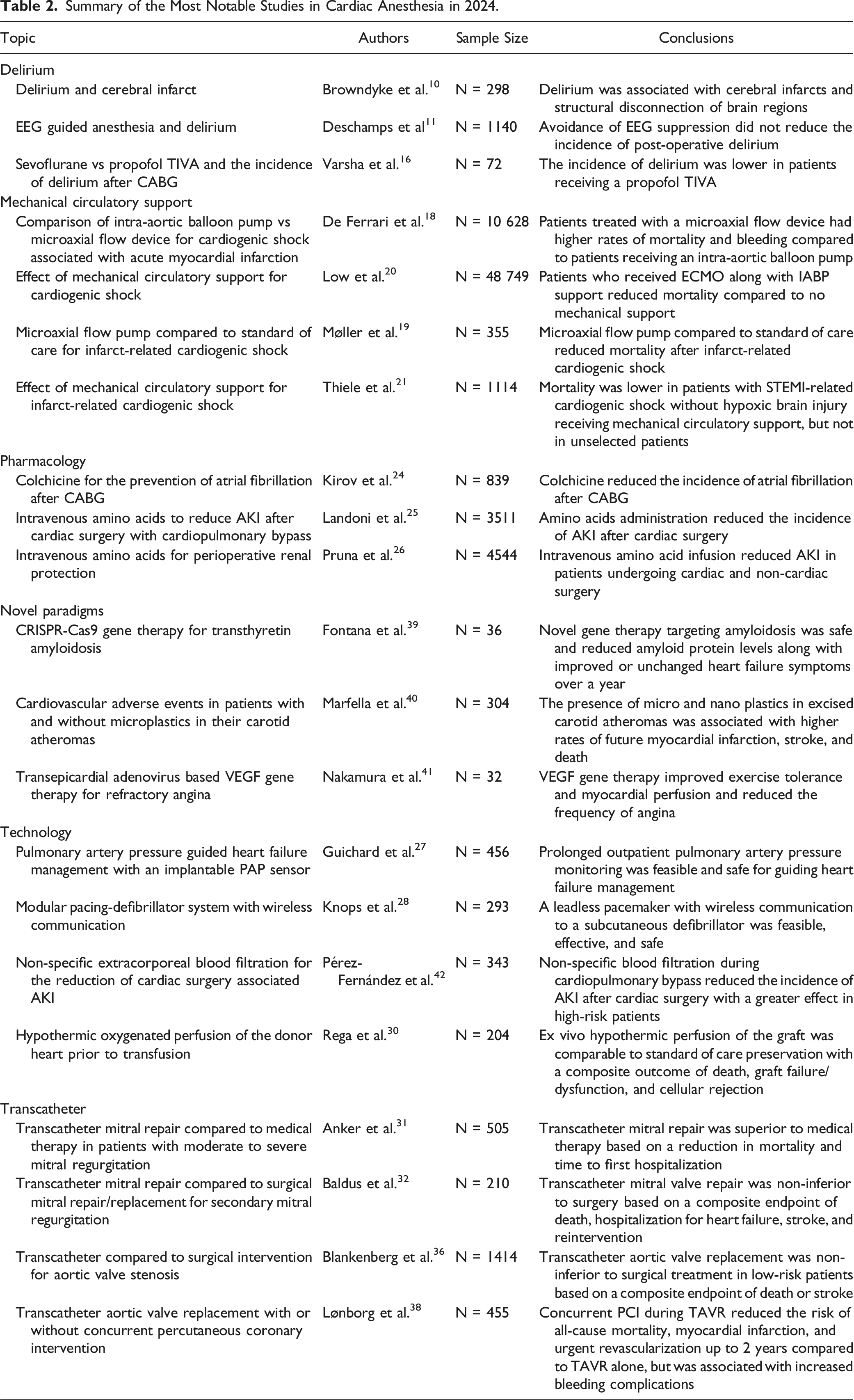
The research findings relevant for Cardiac Anesthesiology studies published in 2024 involved key innovations in devices and gene therapy in addition to the expansion of transcatheter techniques for valve repair or replacement. We reviewed 447 relevant articles and selected 21 as the most noteworthy studies published in 2024. Themes that emerged from our review include the etiology and prevention of delirium or outcomes after mechanical circulatory support. Robust clinical outcome data now supports the use of microaxial flow devices for mechanical circulatory support for cardiogenic shock due to acute myocardial infarction. Pharmacology development presents colchicine as anti-inflammatory medication to prevent atrial fibrillation or intravenous amino acids for kidney protection after cardiopulmonary bypass. Technological advances include implantable wireless pacing-defibrillator devices, pulmonary artery pressure monitoring in heart failure patients, extracorporeal blood purification for preventing acute kidney injury and hypothermic oxygenated perfusion of the donor heart in heart transplantation. Transcatheter interventions on mitral or aortic valve were gaining advances over surgical procedures. Novel paradigms included treatments with gene therapy for cardiac amyloidosis or refractory angina and the emerging risk of microplastic exposure in cardiovascular events.
Keywords
Introduction
Cardiac Anesthesiology continues to evolve to keep pace with advances in surgical technique and mechanical support. Cardiac surgery and perioperative care are fascinating fields with high stakes, high reward, and continuously evolving to provide safer and better care for patients. Researchers publish over a million studies indexed by PubMed from more than 5000 journals each year 1 creating a substantial challenge for the clinicians to keep up to date on impactful research. This review aims to identify key studies pertinent to cardiac anesthesiology and provide readers with a concise summary of research that holds the potential to influence patient care in the near future. Overarching themes that emerged from our review of research in 2024 include the etiology and prevention of delirium, outcomes after mechanical circulatory support, pharmacology advances through drug repurposing comparative effectiveness of anesthetics, novel paradigms for treatment with gene therapy and the emerging risk of microplastic exposure, and technological advances with implantable wireless devices. Clinical trials of transcatheter techniques demonstrate clear benefits of the technique over traditional open surgical approaches for treating most uncomplicated single valve pathologies.
Search Terms, PubMed Query, and the Number of Articles Identified by the Search.
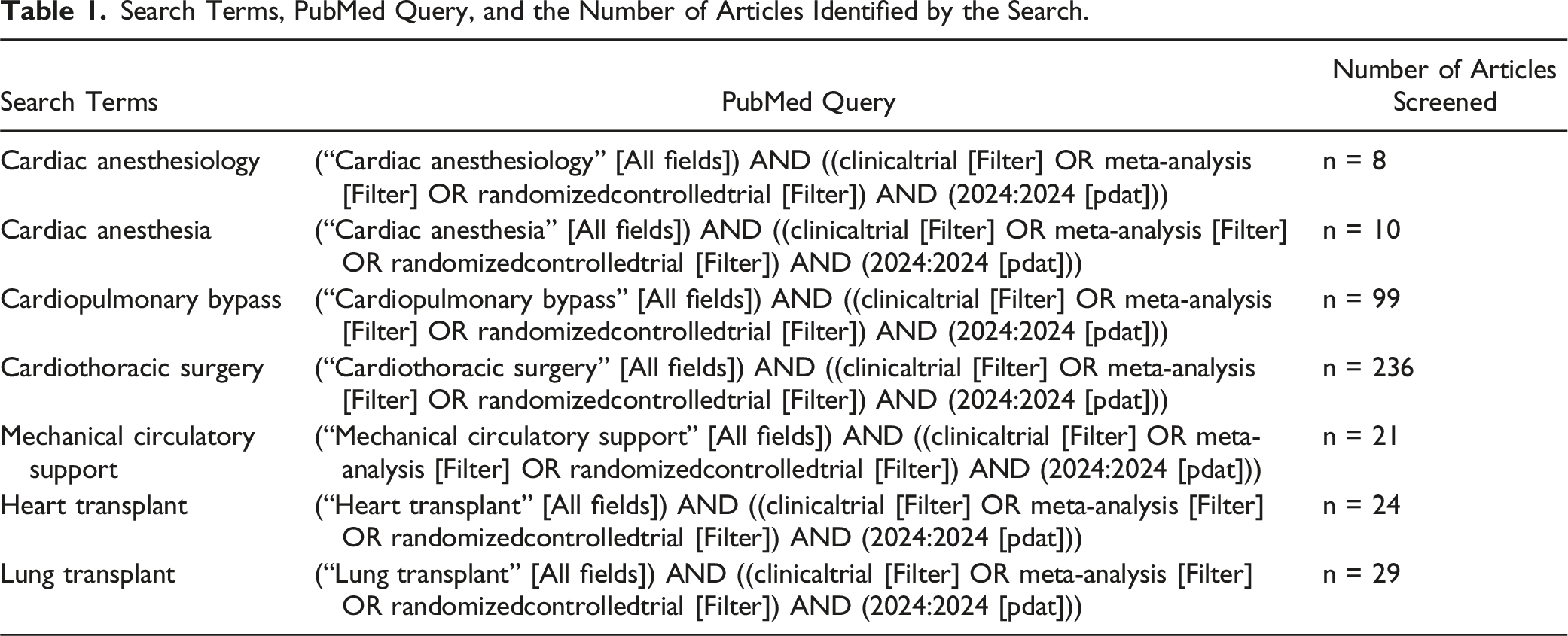
We also reviewed the contents of the most prominent clinical journals to identify 20 impactful and relevant studies which may not have been captured by our search terms: the New England Journal of Medicine, the Journal of the American Medical Association, and the Lancet. For each of the studies, we report the available statistical results provided by the authors for reference with the total sample size denoted as “N =” and any subgroup sample sizes as “n =”.
Summary of the Most Notable Studies in Cardiac Anesthesia in 2024.
Delirium
Post-operative delirium is an acute state of confusion and decreased awareness that often fluctuates and may manifest as hyperactivity or hypoactivity. A recent meta-analysis of 23 studies (N = 14 849 patients) found that the incidence of delirium after cardiac surgery is 11.8.% 7 Many factors contribute to the risk of post-operative delirium, but it is unclear what the best preventative strategy would be to reduce the incidence of delirium. Many interventions tested in clinical trials designed to prevent delirium after cardiac surgery have been ineffective.8,9 Two notable studies in 2024 focused on the etiology of delirium to support the development of more effective interventions. The first measured the degree of structural disconnection in the brain and the incidence of delirium after cardiac surgery 10 and the second tested whether greater anesthetic depth is a clinically significant risk factor for developing delirium after cardiac surgery. 11 The third study addressed the question whether total intravenous anesthesia with propofol was beneficial for reducing the incidence of delirium compared to inhalational anesthesia with sevoflurane in cardiac anesthesia.
Infarct-Related Structural Disconnection and Delirium in Surgical Aortic Valve Replacement Patients
Cerebral embolism and ischemia after cardiac surgery are known causes of clinically apparent cerebral infarction, especially after aortic valve surgery. Previous studies found that even patients without clinical evidence of cerebral infarction still demonstrate new brain lesions identified with magnetic resonance imaging. 12 It is unknown whether these subclinical brain lesions are associated with delirium after cardiac surgery. Browndyke et al. completed a secondary analysis 10 of a prospective randomized controlled trial comparing a standard aortic cannula, an aortic cannula with a mechanical filter, and an aortic cannula with suction filtration in 383 patients. The mechanical filter and suction device groups experienced lower rates of post-operative delirium and higher rates of acute kidney injury (AKI) and arrhythmias compared to the standard cannula group. There was no difference in the degree of brain injury detected by MRI in the primary study prior to the secondary analysis by Browndyke et al. 13 The purpose of this secondary analysis was to determine if there was an association between infarcts that compromise brain region connectivity and post-operative delirium. They excluded patients who experienced a clinically apparent stroke and included the remaining 298 patients with complete neuroimaging. They identified the location of the post-operative brain lesions and compared the images to an atlas of healthy controls to quantify the impact of the lesions on brain connectivity. All the patients undergoing aortic valve surgery had evidence of preoperative brain lesions, but the locations and connectivity did not differ between patients who did or did not develop delirium after surgery. Patients who experienced delirium after surgery were more likely to have lesions that disrupted connectivity to the right cerebellum and the right temporal lobe. Subclinical brain lesions are common after cardiac surgery and injury to the white matter connecting the right cerebellum and right temporal lobe are associated with an increased risk of delirium. Mechanical filtration and suction provide some protection, but brain ischemia remains a significant problem after cardiac surgery. Improved techniques for reducing cerebral emboli have the potential to reduce the incidence of post-operative brain injury and delirium. Reducing cerebral emboli with these specialized cannulas in combination with other techniques such as monitoring cerebral oxygen delivery and avoiding potentially neurotoxic medications may be a beneficial approach for reducing delirium in future studies.
Electroencephalography-Guided Anesthesia and Delirium in Older Adults After Cardiac Surgery: The ENGAGES-Canada Randomized Clinical Trial
Anesthetics induce a reversible loss of consciousness to facilitate surgery but may be associated with prolonged disruptions in cognition after surgery that predispose patients to delirium. Intra-operative electroencephalography (EEG) monitoring allows for the determination of anesthetic depth and allows for monitoring the patient response to anesthetic dosing. Anesthesia induced cognitive dysfunction is dose and exposure time dependent, but it is unknown whether EEG guidance of anesthetic dosing is effective for reducing the incidence of delirium after cardiac surgery. Deschamps et al. completed a prospective randomized controlled trial (N = 1140 patients) comparing the incidence of delirium in patients receiving EEG guidance to excessive anesthetic depth compared to usual care without EEG guidance during cardiac surgery with cardiopulmonary bypass (CPB). The study included patients aged 60 years or older at 4 hospitals in Canada. Clinicians in the intervention group were encouraged to decrease the volatile anesthetic concentration to minimize EEG suppression. The control group received usual care without intra-operative EEG monitoring information available to providers. The patients and the outcome assessors were blinded to group assignment. There was a statistically significant decrease in the median EEG suppression time in the intervention group of −7.70 (−10.61 to −4.67) minutes and lower minimum alveolar concentration (MAC) of volatile anesthetic of −0.14 MAC (−0.15 to −0.13). There was no difference in clinical outcomes between the groups with 18% of both groups experiencing delirium in the first 5 post-operative days. These results demonstrated that volatile anesthetic dosing during cardiac surgery with usual care generate comparable clinical results with or without EEG guidance and that a limited reduction in burst suppression time is not sufficient for preventing delirium.
These results differ from previous work in non-cardiac surgery demonstrating a lower risk of delirium in patients exposed to less anesthetic.14,15 Despite the negative results, EEG monitoring during surgery provides a useful index of a patient’s individual response to anesthetic dosing and allows for the detection of limited brain activity changes in response to intra-operative events. The study by Deschamps et al. may have been underpowered to detect rare adverse events that would impact clinical outcomes. Future studies may determine whether there are other beneficial applications of monitoring intra-operative EEG results to guide clinical management.
Comparison of Propofol-Based Total Intravenous Anesthesia vs Volatile Anesthesia With Sevoflurane for Post-operative Delirium in Adult Coronary Artery Bypass Grafting Surgery: A Prospective Randomized Single-Blinded Study
The exact mechanism by which intravenous and volatile anesthetics produce unconsciousness is unknown, but the predominant theory is that they work by potentiating gamma-aminobutyric acid (GABAa) receptors. Propofol and sevoflurane are among the most commonly used anesthetics and they differ in their potency, effect sites, and specificity. Previous work observed a lower incidence of delirium in elderly patients receiving propofol compared to volatile anesthetics after non-cardiac surgery. 17 It is unknown whether propofol is associated with lower rates of delirium after cardiac surgery. Varsha et al. completed a prospective randomized trial (N = 72 patients) comparing patients undergoing CABG with CPB who received sevoflurane or propofol-based total intravenous anesthesia. 16 Patients received EEG-guided anesthetic care to target a Bispectral index (BIS) between 40 and 60. The co-primary outcomes were the incidence of delirium measured by the Confusion Assessment Method for the intensive care unit (CAM-ICU) method on post-operative day 1 and 2 and the Montreal Cognitive Assessment performed on post-operative day 7. They observed that patients receiving sevoflurane anesthesia had a higher risk of developing delirium (OR 1.72, 95% CI, 1.13 to 2.62, P = .03) and post-operative cognitive dysfunction (OR 1.63, 95% CI, 1.01 to 2.62, P = .04). Unfortunately, the principal investigator performed the post-operative assessments which increased the risk of bias. The preliminary results are encouraging, but further studies are required to demonstrate reproducibility of the work and any possible clinical significance.
Mechanical Circulatory Support
The deployment of microaxial flow devices for left ventricular unloading during cardiogenic shock is becoming a more common therapy due to the expansion of percutaneous techniques and refinement of the technology. Despite the theoretical benefits it is still unclear which patients with which types of cardiogenic shock will benefit from microaxial flow devices. The following articles address this knowledge gap through a retrospective study, a meta-analysis, and an interventional clinical trial.
MI2AMI-CS: A Meta-Analysis Comparing Impella and IABP Outcomes in Acute Myocardial Infarction-Related Cardiogenic Shock
De Ferrari et al. completed a meta-analysis of 8 studies (N = 10 628 patients) with acute myocardial infarction-related cardiogenic shock comparing the outcomes of patients receiving either an intra-aortic balloon pump (IABP) or a microaxial flow device, specifically, the Impella (Abiomed Inc., Danvers, Massachusetts, USA). 18 The primary result was that patients with cardiogenic shock following acute myocardial infarction treated with an Impella had a higher incidence of mortality (57% vs 46%, OR 1.44, 95% CI, 1.29 to 1.60, P < .001) and major bleeding episodes (30% vs 15%, OR: 2.93, 95% CI, 1.67 to 5.13, P < .001) compared to patients treated with an IABP.
The study results seem to suggest that Impella use is inferior to IABP therapy for patients in cardiogenic shock secondary to acute myocardial infarction, but these results may be misleading since the available data is predominantly from retrospective studies with a high risk of bias. Also, the clinical trial data precedes the recent widespread clinical implementation of Impella placement. More specifically, two of the 8 studies were randomized controlled trials, representing only 73 of the total patients; the remaining 6 studies were observational.
Microaxial Flow Pump or Standard Care in Infarct-Related Cardiogenic Shock
Møller et al. completed an international prospective randomized trial of patients (N = 355 patients) with ST elevation myocardial infarction and cardiogenic shock. 19 They compared those who received standard of care revascularization and vasopressor support to patients who received the standard of care with an Impella Cardiac Power (CP) (Abiomed Inc., Danvers, Massachusetts, USA). The primary outcome was death from any cause at 180 days. The study included adult patients with cardiogenic shock diagnosed in the cardiac catheterization laboratory or within 12 hours after cardiac catheterization. The patients also had to be hypotensive with a systolic blood pressure less than 100 mmHg, have a lactate greater than 2.5 mmol per liter, and a left ventricular ejection fraction less than 45%. The study excluded patients who experienced out-of-hospital cardiac arrest or coma.
Patients in the intervention group were treated with the Impella CP (Abiomed Inc., Danvers, Massachusetts, USA) at highest tolerated performance level up to 3.7 liters per minute for 48 hours or until a complication occurred. The primary result was that patients treated with an Impella CP had significantly lower all-cause mortality at 180 days compared to the standard of care (HR 0.74, 95% CI, 0.55 to 0.99, P = .04). The intervention group also had significantly more adverse events including major bleeding, limb ischemia, sepsis, and a new requirement for renal replacement therapy (24.0% vs 6.2%, RR 4.74, 95% CI, 2.36 to 9.55). Overall, the number needed to treat was 8 and the number needed to harm was 6. Subgroup analyses revealed a clear benefit for males, patients with hypotension, and patients with multivessel coronary artery disease. The study included primarily males (80%) so it was likely underpowered to detect outcome differences for females. The study required 10 years to complete enrollment despite inclusion of 14 centers in 3 countries. A key innovation of this work is that the researchers focused on patients with a high likelihood of benefit. They excluded patients with sufficient cardiac output to prevent serious end organ injury and patients with a very low chance of survival due to anoxic brain injury. This strict inclusion and exclusion strategy demonstrated the efficacy of targeting mechanical circulatory support to patients most likely to benefit. The study also highlighted the current limitations of the technology since the intervention resulted in serious harm despite preventing death. One caveat is that the patients in the control group may not have survived long enough to develop complications. The intervention group also experienced a greater need for renal replacement therapy indicating that the non-physiological blood flow from the device may predispose patients to renal injury either directly or indirectly. Despite the complications, mechanical circulatory support with an Impella CP (Abiomed Inc., Danvers, Massachusetts, USA) is life-saving for a selected group of patients, and this study supports the continued adoption and refinement of the therapy.
Mechanical Circulatory Support for Cardiogenic Shock: A Network Meta-Analysis of Randomized Controlled Trials and Propensity Score-Matched Studies
Low et al. completed a meta-analysis of 38 studies (N = 48 749 patients) with cardiogenic shock to compare the effect of different mechanical circulatory support devices on patient outcomes. 20 The meta-analysis included patients requiring treatment for cardiogenic shock with the following 8 interventions listed in descending order by sample size: IABP (n = 20 031), medical therapy only (n = 14 011), Impella (Abiomed Inc., Danvers, Massachusetts, USA; n = 9047), extracorporeal membrane oxygenation (ECMO, n = 3847); ECMO and IABP (n = 1466), ECMO and Impella n = 300; centrifugal pump ventricular assist device (n = 40; and IABP and Impella (n = 7). The authors assessed 40 different pairs of comparisons between the studies. Overall, cardiogenic shock resulted in death for 32.5% of patients. Only combined treatment with ECMO and an IABP was associated with lower mortality compared to medical therapy (OR 0.54, 95% CI, 0.33 to 0.86). ECMO alone was associated with a higher mortality compared ECMO with IABP (OR 1.78, 95% CI, 1.19 to 2.68). These findings were robust and did not change with multiple sensitivity analyses. The available data does not seem to support mechanical circulatory support alone as an effective means for reducing mortality associated with all-cause cardiogenic shock compared medical therapy.
Temporary Mechanical Circulatory Support in Infarct-Related Cardiogenic Shock: An Individual Patient Data Meta-Analysis of Randomized Trials With 6-Month Follow-Up
Thiele et al. completed a meta-analysis of 9 studies (N = 1114 patients) experiencing acute myocardial infarction-related cardiogenic shock comparing patients who received percutaneous mechanical circulatory support or a control treatment. 21 The research included patient level data allowing more detailed analysis than is typically possible with study level meta-analysis. The original authors of the clinical trials participated in the meta-analysis and worked to expand patient follow-up when possible to standardize the primary outcome metric of all-cause mortality at 180 days. Four of the studies compared veno-arterial extracorporeal membrane oxygenation (VA-ECMO) to standard of care, and 5 studies compared left ventricular unloading devices to the standard of care. The key questions the researchers addressed were (1) does any type of active mechanical circulatory support for acute myocardial infarction-related cardiogenic shock reduce mortality compared to the standard of care?; (2) does the type of mechanical circulatory support impact patient mortality?; and (3) does targeted patient selection influence the effect of mechanical circulatory support?
The key findings of this study were that active mechanical circulatory support did not reduce all-cause mortality at 180 days after acute myocardial infarction with cardiogenic shock (HR 0.87, 95% CI, 0.74 to 1.03). However, patients with ST elevation cardiogenic shock without risk of hypoxic brain injury had a reduction in mortality with mechanical circulatory support (HR 0.77, 95% CI, 0.61 to 0.97). The type of mechanical circulatory support did not influence this result, but patients without hypoxic brain injury, a lactate level of 5 mmol/liter or more, systolic blood pressure less than 80, and a Thrombosis in Myocardial Infarction (TIMI) flow less than 3 who received active mechanical circulatory support had a lower mortality than similar patients receiving the standard of care. Bleeding complications and peripheral limb ischemia were high in patients receiving active mechanical circulatory support (bleeding OR 2.64, 95% CI 1.91 to 3.65; peripheral limb ischemia OR 4.43, 95% CI, 2.37 to 8.26). These results support the targeted application of mechanical circulatory support in a specific subset of patients as opposed to a broader application of the therapy to all patients in cardiogenic shock due to acute myocardial infarction.
Pharmacology
Pharmaceutical development typically requires an average of 10 years for drug discovery and $1 billion in development costs. 22 These costs can be prohibitive and limit which conditions and patients receive the benefit of drug development. One strategy to overcome this barrier is to repurpose existing drugs for new indications. 22 The key innovations in pharmaceuticals for conditions relevant for cardiac surgery and anesthesia apply this concept by studying existing drugs in new contexts. Two of the following articles assess the efficacy of colchicine for improving outcomes after cardiac surgery and the efficacy of intravenous amino acids for reducing the incidence of AKI following cardiac surgery
Colchicine in Patients With Coronary Disease Who Underwent Coronary Artery Bypass Surgery: A Meta-Analysis of Randomized Controlled Trials
Cardiac surgery with CPB results in a substantial inflammatory response reaction secondary to tissue injury and exposure to the CPB circuit and non-physiological mechanical stress on the blood. Excessive inflammation is associated with adverse effects such as further tissue injury, vascular permeability, and impaired vasomotor tone. Colchicine is a potent anti-inflammatory medication extracted from plants and has been used to treat joint swelling since 1500 BCE. 23 Colchicine remains a key treatment for joint inflammation due to gout, but it is not routinely used for preventing adverse outcomes in cardiac surgery. It is unknown whether non-specific inhibition of inflammation with colchicine is beneficial for patients undergoing cardiac surgery with CPB. To address this gap, Kirov et al. completed a meta-analysis of 5 prospective randomized trials of colchicine compared to placebo or usual care for the prevention of atrial fibrillation after coronary artery bypass grafting of N = 839 patients. 24 The meta-analysis included 3 multisite studies and 2 single site studies with 140 patients and 360 patients. The analysis demonstrated a lower risk of atrial fibrillation with colchicine treatment (RR 0.54, 95% CI, 0.40 to 0.73). The dose and frequency of the treatment varied between the individual studies but they all included preoperative or perioperative administration and repeat dosing post-operatively. This meta-analysis supports colchicine use as a potentially effective treatment to prevent post-operative atrial fibrillation after cardiac surgery and supports the paradigm of anti-inflammatory prophylaxis prior to cardiac surgery. The individual studies in the meta-analysis were neither designed nor powered for measuring less frequent adverse events, but the pronounced risk reduction for atrial fibrillation observed in this meta-analysis supports future trials designed to determine if colchicine is effective for preventing other adverse outcomes.
A Randomized Trial of Intravenous Amino Acids for Kidney Protection
Landoni et al. completed a multisite prospective randomized trial comparing intravenous amino acids to placebo for the prevention of AKI after cardiac surgery (N = 3511 patients). 25 The study included adult patients undergoing elective cardiac surgery with CPB who had a preoperative creatinine measurement and excluded patients with planned treatment with renal replacement therapy or an estimated glomerular filtration rate less than 30 mL/ minute/ 1.73 m2 of body surface area. The intervention group received a continuous infusion of 2 g/kg of ideal body weight/day of intravenous balanced amino acid mixture or a Ringer’s solution placebo started upon operating room admission and discontinued upon ICU discharge for up to 3 days after surgery. The primary outcome was the incidence of any AKI by the Kidney Disease: Improving Global Outcomes (KDIGO) creatinine criteria within 7 days of surgery. Treatment with intravenous amino acids resulted in a reduction in the incidence of AKI compared to control (RR 0.85, 95% CI, 0.77 to 0.94). The occurrence of Stage 3 AKI was significantly less in the amino acid group (RR 0.56, 95% CI, 0.35 to 0.87). The groups were not different in any of the secondary outcomes.
This study is remarkable because current preventative strategies for AKI consist of usual supportive care and avoidance of nephrotoxic agents. The mechanism of renal protection with intravenous amino acids is unknown, but preliminary work indicated that amino acids increase the glomerular filtration rate through vasodilation. 25 Whether renal vasodilation is a viable general therapeutic approach or something that is specific to intravenous amino acid induced vasodilation is unknown. Regardless, AKI after cardiac surgery remains a significant problem and the study by Landoni et al. expands the prophylactic paradigm for perioperative renal protection.
Amino Acid Infusion for Perioperative Functional Renal Protection: A Meta-Analysis
Pruna et al. completed a meta-analysis of 15 studies testing intravenous amino acids for renal protection after surgery (N = 4544 patients). 26 Eight of these studies included 3979 patients undergoing cardiac surgery with the results primarily from the Landoni et al. 25 The remainder of the studies included patients undergoing orthopedic, urological, abdominal, and obstetric procedures. The meta-analysis demonstrated that perioperative intravenous amino acid treatment reduced the incidence of AKI and reduced the hospital length of stay. These findings were robust on sensitivity analysis and support intravenous amino acids as a reproducible perioperative renal protective strategy.
Technology
Technological advancement is a key driver in medical innovation and often applies innovations from other fields in a new medical context. This year, the most prominent innovations relevant to cardiac surgery and anesthesia involved novel applications of wireless technology that enable outpatient pulmonary artery pressure monitoring, as well as a leadless pacemaker and defibrillator system. Other innovations included an innovative filter for continuous renal replacement system and a novel perfusion system to provide active blood flow during the transport of a donor heart for transplantation.
Seated Pulmonary Artery Pressure Monitoring in Patients With Heart Failure: Results of the PROACTIVE-HF Trial
Guichard et al. completed a prospective single arm multisite open-label trial (N = 456 patients) with chronic heart failure who received a seated pulmonary artery pressure monitoring system with clinical intervention based on the mean pulmonary artery pressure (mPAP) obtained. 27 This system transmits the mPAP wirelessly to clinicians managing the patient’s heart failure. The study included adult patients with at least 3 months of heart failure with NYHA class 3 symptoms who were stable on guideline directed medical therapy (GDMT) and required hospitalization for heart failure in the past 12 months. The clinicians were instructed to target a mPAP between 5 and 20 mmHg using GDMT with diuretic agents and vasodilators. The primary outcome was the incidence of hospitalization for heart failure or death at 6 months, and efficacy was defined against an expected event rate of 0.43 events per patient at 6 months. The primary result was a lower event rate at 6 months (0.15 per patient, 95% CI, 0.12 to 0.20, P < .0001). Importantly, the complication and device failure rates met the pre-specified safety thresholds. This study demonstrates that ambulatory remote monitoring of the mPAP may prevent hospitalization for heart failure and provides support for devices that transmit hemodynamic data remotely to clinicians to improve patient outcomes.
A Modular Communicative Leadless Pacing-Defibrillator System
Technological innovation with improving wireless technology and miniaturization has enabled the development of a novel modular pacing and defibrillator system in an effort to avoid the potential complications associated with transvenous lead platforms. This system combines a leadless pacemaker with a subcutaneous implantable cardioverter-defibrillator that communicates wirelessly to provide both anti-tachycardia and bradycardia pacing. Knops et al. completed a multisite prospective single group study (N = 293 patients) who received a leadless pacing-defibrillator system. 28 The study included patients with an existing defibrillator that required removal and were at high risk for monomorphic ventricular tachycardia. The primary performance endpoints were maintenance of communication between the pacemaker and the defibrillator system along with pacing thresholds. Safety outcomes included freedom from device related complications at 6 months, including hospitalization or death related to the device. At 6 months, 8.6% of patients experienced a system-related complication. Half of the complications (9 out of 18) occurred during the procedure to implant the system, and the other half were related to the system performance during follow-up. Overall, 97.5% (lower boundary of the one-sided 98.8% CI, 94.2%) of patients did not experience a system-related complication and 98.8% (lower boundary of the one-sided 97.5% CI, 97%) of patients received systems that met the performance goal. These results exceeded the expected benchmarks, but longer-term follow-up and larger studies are warranted.
Extracorporeal Blood Purification and Acute Kidney Injury in Cardiac Surgery: The SIRAKI02 Randomized Clinical Trial
AKI after cardiac surgery is a common problem associated with an increased risk of morbidity and mortality. 29 The etiology of cardiac surgery associated AKI is multifactorial with renal ischemia and direct nephrotoxicity from oxidative stress, systemic inflammation, and cell-free hemoglobin and free iron toxicity following hemolysis. Removal of these toxic substances during cardiac surgery has the potential to reduce the incidence of cardiac surgery associated AKI. Pérez-Fernández et al. completed a prospective randomized trial (N = 343 patients) to determine the effect of non-specific extracorporeal blood purification during CPB compared to usual care on the incidence of AKI after cardiac surgery. The study included adults scheduled for elective cardiac surgery with an expected CPB time greater than 90 minutes and excluded patients with chronic kidney disease stage 4 or 5. The intervention group received continuous kidney replacement therapy with a non-specific membrane filter and ultrafiltration as needed. The control group received the standard of care and ultrafiltration per the perfusionist’s discretion. The primary outcome was the incidence of AKI between randomization and 7 days after cardiac surgery. The intervention group had a significantly lower incidence of AKI after surgery (28% vs 40%, P = .03). The groups did not differ in secondary outcomes but subgroup analysis revealed that the intervention was more beneficial for patients with diabetes, chronic kidney disease, or a left ventricular ejection fraction less than 40%. In an exploratory analysis comparing cytokine levels, only TNFα and IL-8 were significantly lower in the intervention group (P < .05). This trial provides direct evidence in support of non-specific extracorporeal blood purification during CPB to reduce AKI by removing inflammatory mediators. However, the AKI incidence in the intervention group remained high at 28% which also supports the concept that AKI has a multifactorial etiology.
Hypothermic Oxygenated Perfusion of the Donor Heart in Heart Transplantation: The Short-Term Outcome From a Randomized, Controlled, Open-Label, Multicentre Clinical Trial
Rega et al. completed a prospective randomized open-label study (N = 204 patients) to determine the effect of hypothermic oxygenated perfusion of the donor heart prior to transplantation compared to static cold storage on heart transplantation outcomes. 30 The intervention group received hypothermic perfusion with the following key steps: flushing the graft with cold cardioplegia through a self-deairing aortic cannula, adding antibiotics and insulin, and adding a unit of cross-matched allogenic red blood cells. The control group received static cold storage per usual care. The primary outcome was time to first event of a composite of cardiac-related death, moderate or severe primary graft dysfunction, acute cellular rejection, or graft failure requiring the use of mechanical circulatory support or re-transplantation within 30 days after transplantation. There was not a statistically significant difference in the primary outcome between the groups (HR 0.56, 95% CI, 0.32 to 0.99 P = .06). A subgroup analysis revealed that the intervention group had a significant reduction in the incidence of primary graft dysfunction within 24 hours compared to the control group (11% vs 28%, RR 0.39, 95% CI, 0.20 to 0.73). This study demonstrates that hypothermic perfusion of donor hearts prior to transplantation is feasible and may be effective for reducing the risk of early primary graft dysfunction. These results are not sufficient to support a new standard of care but they should encourage further study and refinements in technique. If successful, this approach may expand the availability and safe storage time of donor organs which would improve access for patients on the heart transplantation wait list.
Transcatheter Interventions
Percutaneous transcatheter techniques for valve replacement or repair continue to revolutionize the treatment of valvular disorders by providing definitive therapy without the need for sternotomy and cardiopulmonary bypass. This may reduce the recovery time and complication rates of the procedures, while also allowing treatment for patients with prohibitive surgical risk factors. In 2024, various investigations into transcatheter techniques added further insight into their utility for patients with low- and high-surgical risk.
Transcatheter Valve Repair in Heart Failure With Moderate to Severe Mitral Regurgitation
In the RESHAPE-HF2 trial, Anker et al. completed a multisite prospective randomized trial in patients with heart failure and moderate to severe mitral regurgitation (MR) to determine the effect of transcatheter edge-to-edge mitral valve repair (TEER) along with goal-directed medical therapy compared to medical therapy alone (N = 505 patients). 31 The events per 100 patient-years of the 2 groups were compared. The intervention group showed a lower rate (37 compared to 58.9 events per 100 patient-years) of first or recurrent hospitalization for heart failure or cardiovascular death at 24 months (RR, 0.64, 95% CI, 0.48 to 0.85, P = .002). Patients of the intervention group were in better health status also at 12 months as measured by the Kansas City Cardiomyopathy Questionaire-Overall Summary (KCCQ-OS).
Transcatheter Repair vs Mitral Valve Surgery for Secondary Mitral Regurgitation
Baldus et al. completed a prospective multisite randomized trial (N = 210 patients) comparing transcatheter repair to surgical repair for secondary mitral regurgitation. 32 This non-inferiority trial conducted in Germany, assigned patients with heart failure and functional MR despite medical therapy to undergo either TEER or surgical mitral valve repair or replacement. The study showed that TEER was non-inferior to mitral valve surgery with respect to a composite of death, rehospitalization for heart failure, stroke, reintervention, or implantation of an assist device at 1 year (RR, 0.74, 95% CI, 0.41 to 1.34, P = .3).
Based on this data, anesthesiologists will likely see an increasing number of patients with heart failure and functional MR for presenting TEER. Although general anesthesia is traditionally used, conscious sedation and deep sedation are increasingly recognized as safe and effective alternatives for TEER, offering benefits such as reduced ICU length of stay and lower anesthetic requirements.33-35
Transcatheter or Surgical Treatment of Aortic Valve Stenosis
Blankenberg et al. completed a multisite prospective randomized trial of patients with severe, symptomatic aortic stenosis and low- to intermediate-surgical risk (N = 1414 patients) to determine the effect of a transcatheter (TAVR) vs surgical (SAVR) approach to the treatment of aortic valve stenosis. 36 They found that TAVR with either balloon expandable valve (BEV) or self-expanding valve (SEV) was non-inferior to SAVR with respect to death from any cause or stroke at 1 year (HR, 0.54, 95% CI, 0.36 to 0.80, P < .001). In addition to positive results for the combined primary outcome, the TAVR group had a significantly lower all-cause mortality than the SAVR group (2.6% vs 6.2%, HR 0.43, 95% CI, 0.24 to 0.73). These results support TAVR as the preferred first line therapy for eligible patients.
Long-term outcome data (10 years or more) and risk of severe structural valve deterioration is not completely determined in TAVR compared to SAVR. In the NOTION (Nordic Aortic Valve Intervention) trial, patients with severe aortic stenosis and lower surgical risk were randomized to TAVR or SAVR. The risk of major clinical outcomes such as all-cause mortality, stroke, or myocardial infarction was not different 10 years after treatment (HR, 1.0, 95% CI, 0.7 to 1.3, P = .9). Severe structural valve deterioration occurred in 1.5% and 10% after TAVI and SAVR, respectively (HR 0.2, 95% CI, 0.04 to 0.7, P = .02). 37 This study suggests further shift in aortic stenosis treatment toward TAVR in a patient population with low risk to surgical aortic valve replacement.
PCI in Patients Undergoing Transcatheter Aortic Valve Implantation
Lønborg et al. completed a prospective multisite randomized open-label trial (N = 455 patients) to determine the effect of concurrent percutaneous coronary artery intervention (PCI) during TAVR compared to TAVR alone. 38 The study included patients with severe symptomatic aortic stenosis and 1 or more coronary artery stenoses defined as a fractional flow reserve of 0.80 or less or a 90% occlusion. The study excluded patients with an expected survival less than 1-year, renal failure with a glomerular filtration rate less than 20 mL/ minute/ 1.73 m2 of body surface area, acute coronary syndrome within the past 2 weeks, and left main coronary artery disease. PCI was performed most commonly as a staged procedure prior to TAVR, and this sequence occurred for 74% of the patients in the intervention group. The remaining 26% of patients underwent PCI at the time of TAVR or within 2 days. The primary outcome was a composite endpoint of death from any cause, myocardial infarction, or urgent revascularization at 1 year. The researchers also assessed the safety endpoints of bleeding, stent thrombosis, and acute kidney failure. The main result was that patients who received PCI at the time of TAVR had a lower risk of a major adverse cardiac event (MACE) at 1 year (26% vs 36%, HR 0.71, 95% CI, 0.51 to 0.99, P = .04). However, patients in the intervention group were more likely to experience a bleeding event (28% vs 20%, HR 1.51, 95% CI, 1.03 to 2.22). This study supports PCI alongside TAVR for patients with a severe coronary lesion to reduce the risk of MACE, but this approach must be balanced with the additional risk of bleeding. The optimal timing of PCI remains unclear due to the inconsistent timing of PCI before or after TAVR in this study.
Novel Paradigms
The emergence of novel diagnostic and therapeutic paradigms relevant for cardiac surgery and anesthesia are rare and may not result in sustained changes in practice. This year we identified 3 studies with the potential for a paradigm shift. Two of these studies demonstrate the maturation of gene editing technology applied to cardiac disease, and the third described the potential harm of ubiquitous micro and nanoplastics present in the environment.
CRISPR-Cas9 Gene Editing With Nexiguran Ziclumeran for ATTR Cardiomyopathy
Fontana et al. completed a phase 1 open-label trial (N = 36 patients) with transthyretin amyloidosis and cardiomyopathy treated with nexiguran ziclumeran, a CRISPR-Cas9 gene editing therapy which decreases transthyretin levels. 39 The primary outcome was the safety and pharmacodynamics of the intervention measured by the serum transthyretin level up to 12 months after therapy. The secondary outcomes included cardiac biomarkers (N-terminal pro-B-type natriuretic peptide and high sensitivity cardiac troponin T levels), the 6-minute walk distance and New York Heart Association (NYHA) heart failure class. All patients experienced a rapid decrease in transthyretin levels after treatment at 12 months (−90%, 95% CI, −93% to −87%). The treatment was not associated with a significant change in cardiac biomarkers or 6-minute walk distance. Most patients (33 out of 36) either improved or remained at the same NYHA class at 12 months.
Overall, the interim results of the study suggest that nexiguran ziclumeran has an acceptable safety profile, dramatic impact on transthyretin levels, and possible clinical benefits. The study follow-up period will continue up to 27 months to determine if the treatment effect is durable and has a clinically significant impact. The study is an impressive demonstration of the rapid clinical translation of Crispr-Cas 9 gene editing technology in addition to the virus-free delivery method with hepatotropic nanospheres. If the efficacy and safety profile of the gene editing and nanotechnology-based delivery method is confirmed it could enable targeted treatments for diseases that have a genetic etiology. This would be a transformative innovation in clinical management of disease with the potential to bridge the gap between the massive trove of basic science research and clinical medicine.
Microplastics and Nanoplastics in Atheromas and Cardiovascular Events
Marfella et al. completed a prospective multisite observational study (N = 304 patients) with asymptomatic carotid disease undergoing carotid endarterectomy to determine the association between the presence of mircoplastics and nanoplastics (MNPs) in carotid atheromas and patient outcomes. 40 They separated the patients into 2 groups based on the whether there were MNPs present in the excised plaque and documented clinical outcomes during a 34-month follow-up period. Within the cohort, 58.4% of patients had detectable MNPs. The primary endpoint was a composite of stroke, myocardial infarction, or death from any cause and was adjusted for known cardiovascular risk factors. The patients with MNPs in their plaque had a significantly higher risk of morbidity and mortality (HR 4.53, 95% CI, 2.00 to 10.27, P < .001). The plaques with detectable MNPs had higher levels of proinflammatory cytokines and lower levels of collagen compared to plaques without plastic. Electron microscopy revealed that the plastic particles had a spiked shape and were mostly in the submicron size range. This study demonstrates a clear association between patient outcomes and the presence of MNPs in atheromatous carotid plaques. Future work is necessary to clarify whether the presence of MNPs causes disease leading to increased cardiovascular risk or whether this is an incidental finding.
Angiogenic Gene Therapy for Refractory Angina: Results of the EXACT Phase 2 Trial
Nakamura et al. completed a multicenter open-label trial with 32 patients who received transepicardial gene therapy with XC001 to treat refractory angina. 41 XC001 is an adenoviral vector encoding for vascular endothelial growth factor which promotes angiogenesis. The treatment is administered by 15 direct intramyocardial injections of 0.1 mL each through a mini thoracotomy. The primary hypothesis is that stimulating new cardiac vessel growth will relieve anginal symptoms and improve exercise tolerance. The phase 2 study was designed to assess safety and efficacy at 12 months after treatment. The clinical outcomes were exploratory and not formally tested, but patients demonstrated improvements in anginal symptoms and improved exercise tolerance which supports a sustained biological effect for up to 12 months. The treatment was safe and did not produce measurable off-target or systemic effects. This study is a proof-of-principle for endogenous revascularization through a biological treatment. The current paradigm of revascularization for coronary artery disease is largely a mechanical approach with endovascular stenting or coronary artery bypass grafting with surgery. Promoting new vessel growth has the additional advantage of not relying on endogenous conduits that may experience restenosis requiring reintervention. In this study preliminary positron emission tomography imaging of the ischemic myocardium before and after treatment demonstrated that the perfusion deficit likely decreased. This study demonstrated that epicardial gene therapy to stimulate the production of vascular endothelial growth factor is feasible and may result in cardiac angiogenesis. This finding will need to be replicated in a definitive randomized trial powered for efficacy prior to approval and implementation of the therapy into clinical practice.
Conclusions
Relevant research for Cardiac Anesthesiology in 2024 included work leading to a better understanding of delirium, robust outcomes data for patients requiring mechanical circulatory support for cardiogenic shock, expanded eligibility of transcatheter techniques for lower risk patients, technological advancements including wireless pacemaker-defibrillator systems and outpatient pulmonary artery pressure monitoring, and the clinical application of gene editing techniques. Improved donor organ storage with active perfusion may also reduce primary graft dysfunction and improve outcome after heart transplantation. These innovations will shift clinical practice directly by impacting patients’ preoperative status and indirectly through the increased application of transcatheter techniques for low-risk patients. Therefore, it is likely that higher risk patients requiring multiple high-risk challenging procedures will be a greater proportion of the patients undergoing open cardiac surgical procedures with cardiopulmonary bypass.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by National Heart, Lung, and Blood Institute of the National Institutes of Health under award number 5K23HL151882.