
Abstract
High-dose opioid use in cardiac anesthesia has been challenged due to its association with increased postoperative complications. We retrospectively compared postoperative opioid consumption in a cohort of adult cardiac surgery patients who received low, moderate, or high doses of intraoperative opioids. We also examined variability in intraoperative opioid use among cardiac anesthesiologists. Within our cohort, we categorized patients into “lower opioid recipients” (LOR), “mid opioid recipients” (MOR), or “higher opioid recipients” (HOR) based on the distribution of intraoperative opioids administered in morphine milligram equivalents (MME) within our cohort. After summarizing their demographics and clinical characteristics, we assessed the association between their intraoperative opioid dose group and our outcomes of interest including postoperative opioid consumption. A total of 6390 patients who underwent cardiac surgery between 2014 and 2022 met our inclusion criteria. Our multivariable models indicated that the HOR group was significantly associated with less postoperative opioid consumption relative to the LOR (MME: Mean Ratio (MR) = 0.51 (0.47, 0.56), P < 0.001; MME/kg: MR = 0.51 (0.48, 0.55), P < 0.001) and the MOR (MME: MR = 0.53 (0.50, 0.57), P < 0.001; MME/kg: MR = 0.55 (0.55 (0.51, 0.58), P < 0.001). Among patients undergoing elective adult cardiac surgery, higher doses of intraoperative opioids were associated with lower postoperative opioid consumption. Marked variability in opioid administration was observed among cardiac anesthesiologists, where higher intraoperative opioid use remains a common practice. This highlights the need for precise distinction between high and low dose opioid techniques.
Keywords
Introduction
High-dose opioid use has traditionally been a cornerstone of cardiac anesthesia. 1 This has primarily been because opioids in high doses remain relatively free of hemodynamic side effects that are considered detrimental to patients with critical cardiac pathology. 2 This practice has been challenged due to the consequences of increased postoperative complications, including but not limited to delirium, respiratory depression, postoperative nausea and/or vomiting, gastrointestinal ileus, and higher risks of long-term opioid dependence. 3
While patient-reported pain scores guide postoperative opioid administration, intraoperative administration varies and is often provider-dependent, with widely variable administration practices across different institutions.4,5 Furthermore, it has been reported that low-dose opioid anesthesia can be safely administered when compared with higher-dose practices in adult cardiac surgery.6-8 Therefore, there has been a building consensus to shift towards judicious opioid usage, perioperative opioid stewardship, and multimodal analgesia (MMA) strategies.9,10 This change in practice emphasizes the need to standardize intraoperative opioid dosing as a part of low-dose opioid-sparing strategy that could optimize pain control after cardiac surgery.
Unfortunately, factors that drive intraoperative opioid administration in adult cardiac surgery have not been carefully examined. Burns et al reported that substantial variations (20-43%) exist due to differences among providers and centers. 11 The variety of enhanced recovery after surgery (ERAS) bundles in cardiac surgery across different centers only adds to these differences. In the absence of a standardized definition of opioid-sparing anesthetic in published studies and the lack of distinction in what constitutes low- vs high-dose intraoperative opioids, providers may opt to continue the practice with which they are most familiar.
Therefore, we conducted this study to determine if there were differences in postoperative opioid consumption and relevant secondary outcomes in adult patients undergoing cardiac surgery who received lower, moderate, or higher doses of intraoperative opioids. We also examined variability in intraoperative opioid use over time and among individual cardiac anesthesiologists.
Methods
Design, Setting, and Participants
After obtaining institutional review board approval (Pro00104705), we performed a retrospective review and included all patients ≥18 years of age undergoing non-transplant and non-ventricular assist device (VAD) cardiac surgery with cardiopulmonary bypass (CPB) via a midline sternotomy at our single large tertiary academic center between January 1, 2014 and December 31, 2022. The study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) recommendations. We excluded patients who underwent emergency surgery, had opioid/substance abuse history, had absent or only zero pain scores, had surgery via an incision other than midline sternotomy, or underwent additional surgeries within the initial 72 hours after the index operation.
Abstracted data from the electronic medical record included baseline characteristics such as age, sex, race, body mass index (BMI), American Society of Anesthesiologists physical status (ASA PS) score, tobacco use, chronic pain status, surgery date, and type. Additionally, perioperative variables included intra- and postoperative opioid consumption in morphine milligram equivalents (MME), duration of surgery, postoperative pain scores, postoperative duration of mechanical ventilation (MV), intensive care unit (ICU) and hospital lengths of stay (LOS), and postoperative antiemetic usage.
Definition of Cut-Off Values
Previous publications that aim to assign “high” or “low” opioid dose status to patients vary drastically in threshold values,5-8,11 which prompted our decision to define our intraoperative opioid groups using a data-driven method. We obtained our thresholds from the lower and upper quartiles of intraoperative opioid dose (in MME) within our cohort. As such, “lower opioid recipients” (LOR) includes the lowest 25% of our cohort (65 MME or less), “higher opioid recipients” (HOR) includes the top 25% of our cohort (113 MME or more), and “mid opioid recipients” (MOR) includes the remaining 50% of patients (receiving 66-112 MME).
Statistical Analysis
Patient Demographics and Baseline Characteristics Summarized for Our Entire Cohort and by Intraoperative Opioid Administration Group. Continuous Variables Were Summarized as Mean (SD) or Median [IQR], and Categorical Variables Were Summarized as Frequency (%)
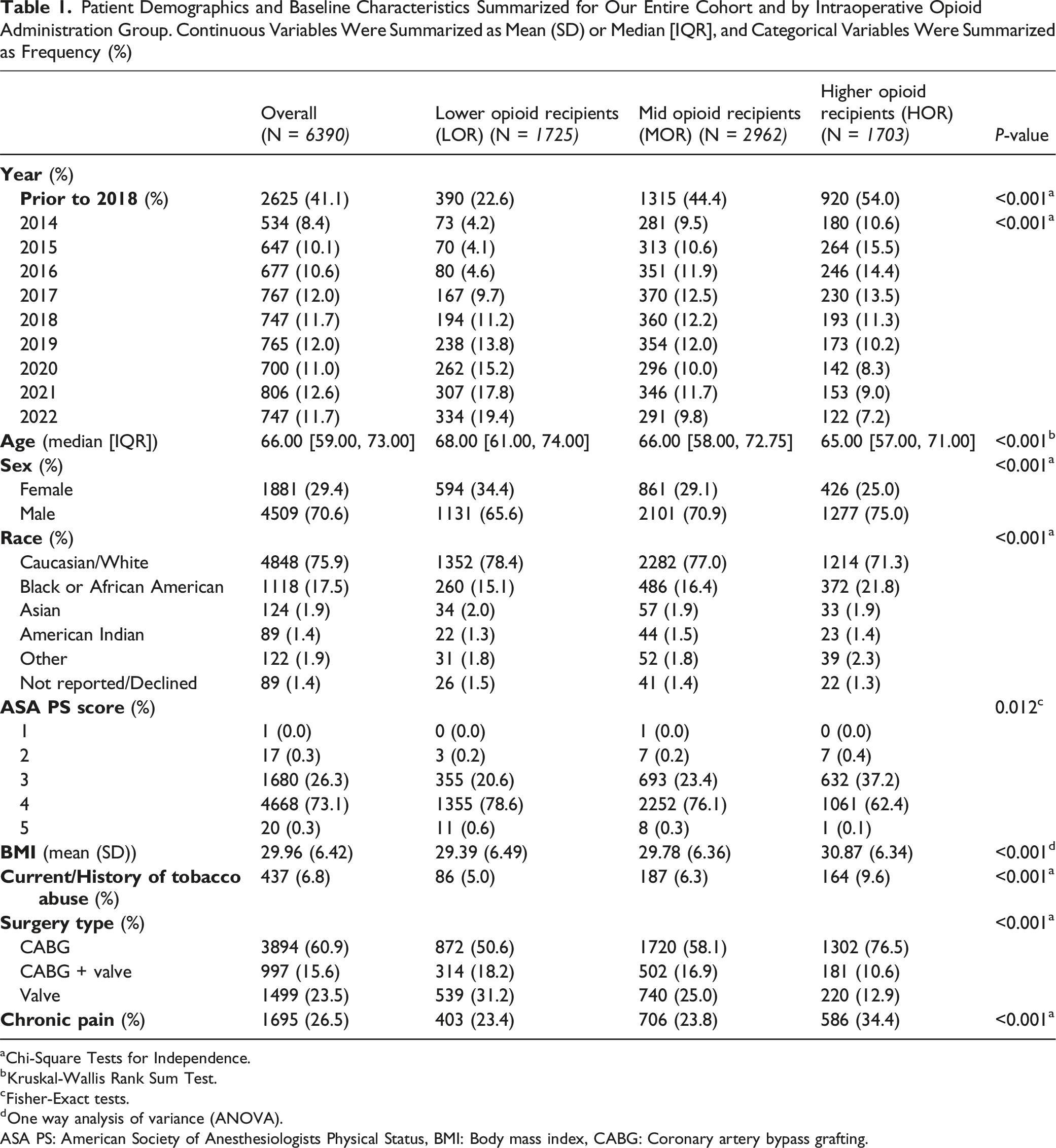
aChi-Square Tests for Independence.
bKruskal-Wallis Rank Sum Test.
cFisher-Exact tests.
dOne way analysis of variance (ANOVA).
ASA PS: American Society of Anesthesiologists Physical Status, BMI: Body mass index, CABG: Coronary artery bypass grafting.
Patient Intraoperative and Postoperative Characteristics Summarized for Our Entire Cohort and by Intraoperative Opioid Administration Group. Continuous Variables Were Summarized as Mean (SD) or Median [IQR], and Categorical Variables Were Summarized as Frequency (%)

aSignificant differences between groups were determined via Kruskal-Wallis rank sum tests, Chi-Square Tests for Independence
bUsing Bupivacaine or ropivacaine.
cIncludes NSAIDs (ketorolac), lidocaine, and magnesium sulfate.
dFisher-Exact tests.
eIncludes NSAIDs (ketorolac, ibuprofen), ketamine, lidocaine, and magnesium sulfate.
fIncludes gabapentin and pregabalin.
CPB: Cardiopulmonary bypass, ICU: Intensive Care Unit, MME: Morphine milligram equivalents, MV: Mechanical ventilation.
Primary Outcome: Total Postoperative Opioid Consumption in the First Three Postoperative Days (72 hours) in MME
Secondary Outcomes: Total postoperative opioid consumption in the first three postoperative days (72 hours) in MME/kg, duration of MV (from ICU admission to extubation), ICU and hospital LOS, as well as postoperative pain scores and antiemetic use in the first three postoperative days (72 hours).
We assessed the association between intraoperative opioid administration and our outcomes of interest with multivariable regression models adjusting for the patient’s age, sex, race, ASA PS score, tobacco use, intraoperative multimodal analgesia use, surgery year, type of surgery (coronary artery bypass graft (CABG), valve, CABG + valve), and duration. Total postoperative opioid consumption was shifted by a constant, log-transformed, and assessed via linear regression, while our length of stay outcomes were evaluated with negative binomial regression. The results are reported as mean ratios (MR) and Rate Ratios (RR), respectively. To assess the duration of MV, we ran an accelerated failure time (AFT) model as opposed to a Cox proportional hazards model to reflect our primary interest more accurately in ventilation times and not risk of extubation. Using the “survival” package in R (version 4.4.0), our AFT model included a specified log-normal distribution and used the first 24 hours post-op to determine censorship. As such, the reported results are time ratios (TR). Meanwhile, we used a linear mixed-effects model with a random intercept for each patient to evaluate pain scores collected over the first three postoperative days, and logistic regression to evaluate postoperative antiemetic administration. We reported the beta coefficients and odds ratios (OR) for these models, respectively. All reported estimates obtained from our multivariable regression models include a 95% confidence interval.
Additionally, we examined the variability of intraoperative opioid administration in our cohort by calendar year and by individual cardiac anesthesiologists who were involved in at least 50 surgeries between 2014 and 2022. Upon observing some variation in intraoperative opioid administration within these identified anesthesiologists, we conducted a sensitivity analysis that replicated the multivariable models previously discussed while also adjusting for the anesthesiologist’s years of experience at the time of the patient encounter. This experience was defined as the number of years that had passed since their reported graduation year from residency.
Finally, to evaluate the robustness of our results, we performed a secondary analysis in which we replicated the models run on our full cohort and our subset of patients treated by our identified anesthesiologists with intraoperative opioids treated as a continuous predictor (MME and MME/kg).
Results
A total of 9559 patients underwent cardiac surgery with CPB (other than cardiac transplantation and VAD implantation) via a midline sternotomy at our hospital between January 1, 2014 and December 31, 2022. After applying all exclusion criteria, a final cohort of 6390 patients was included in the study (Figure 1). Flow diagram showing our study cohort. CPB: Cardiopulmonary bypass, VAD: Ventricular assist device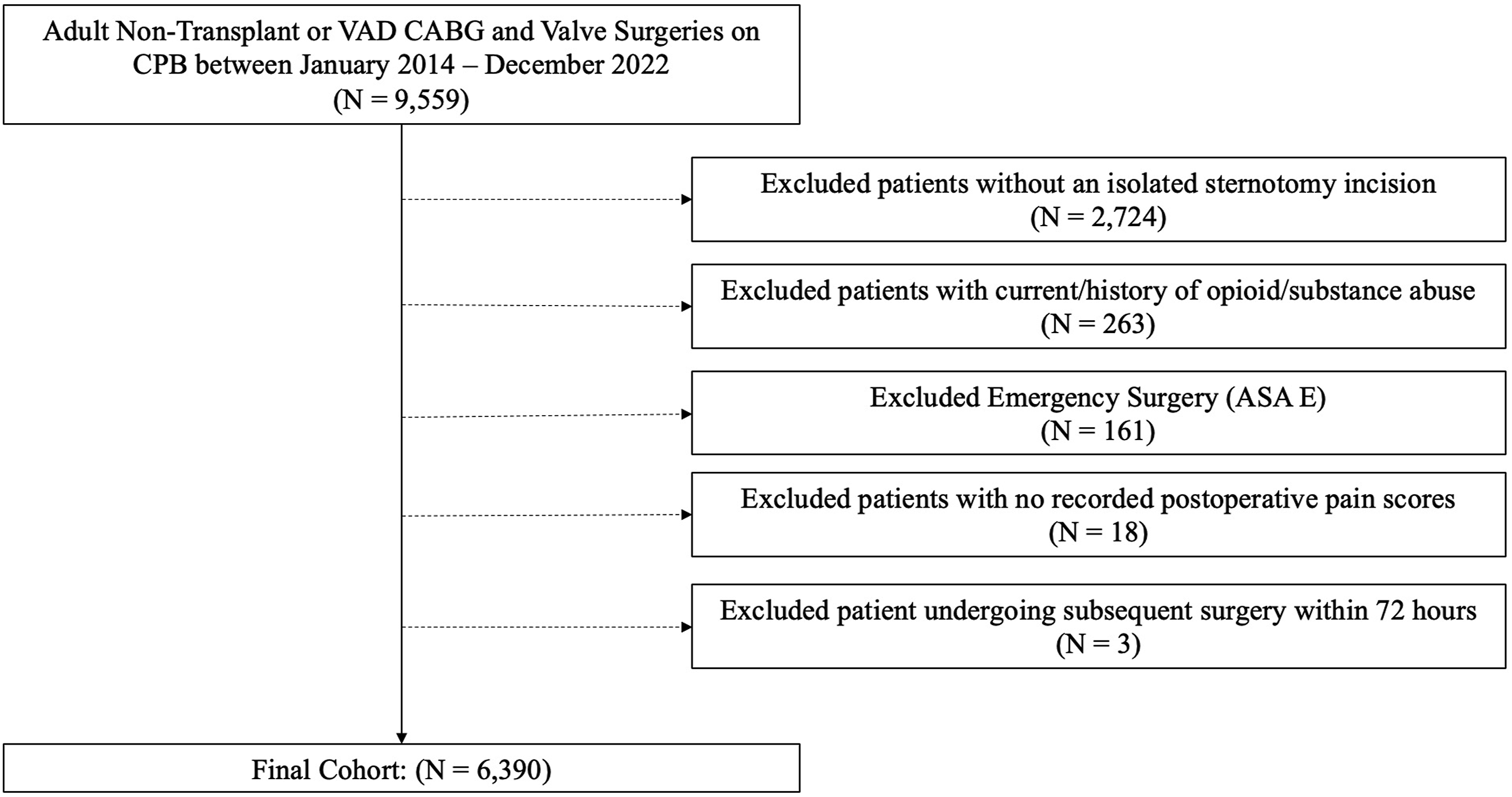
Compared to the LOR group, patients in the HOR group were younger (65 years old [57-71] vs 68 [61-74], P < 0.001), more male (75% vs 65.6%, P < 0.001) non-Caucasian/white patients (Caucasian/white patients: 71.3% vs 78.4%, P < 0.001). The HOR group also had more patients with an ASA PS score of 3 (37.2% vs 20.6%, P = 0.003), more CABG patients (76.5% vs 50.6%, P < 0.001), more patients with current or former tobacco abuse (9.6% vs 5%, P < 0.001), and a higher BMI (30.87 (SD = 6.34) vs 29.39 (SD = 6.49); P < 0.001) (Table 1). Further, 54% of patients in the HOR group had surgery in the early study period prior to 2018, compared to 22.6% of LOR (P < 0.001) (Table 1, Figure 2). Percentage of intraoperative HOR and LOR by year. HOR: Higher opioid recipients, LOR: Lower opioid recipients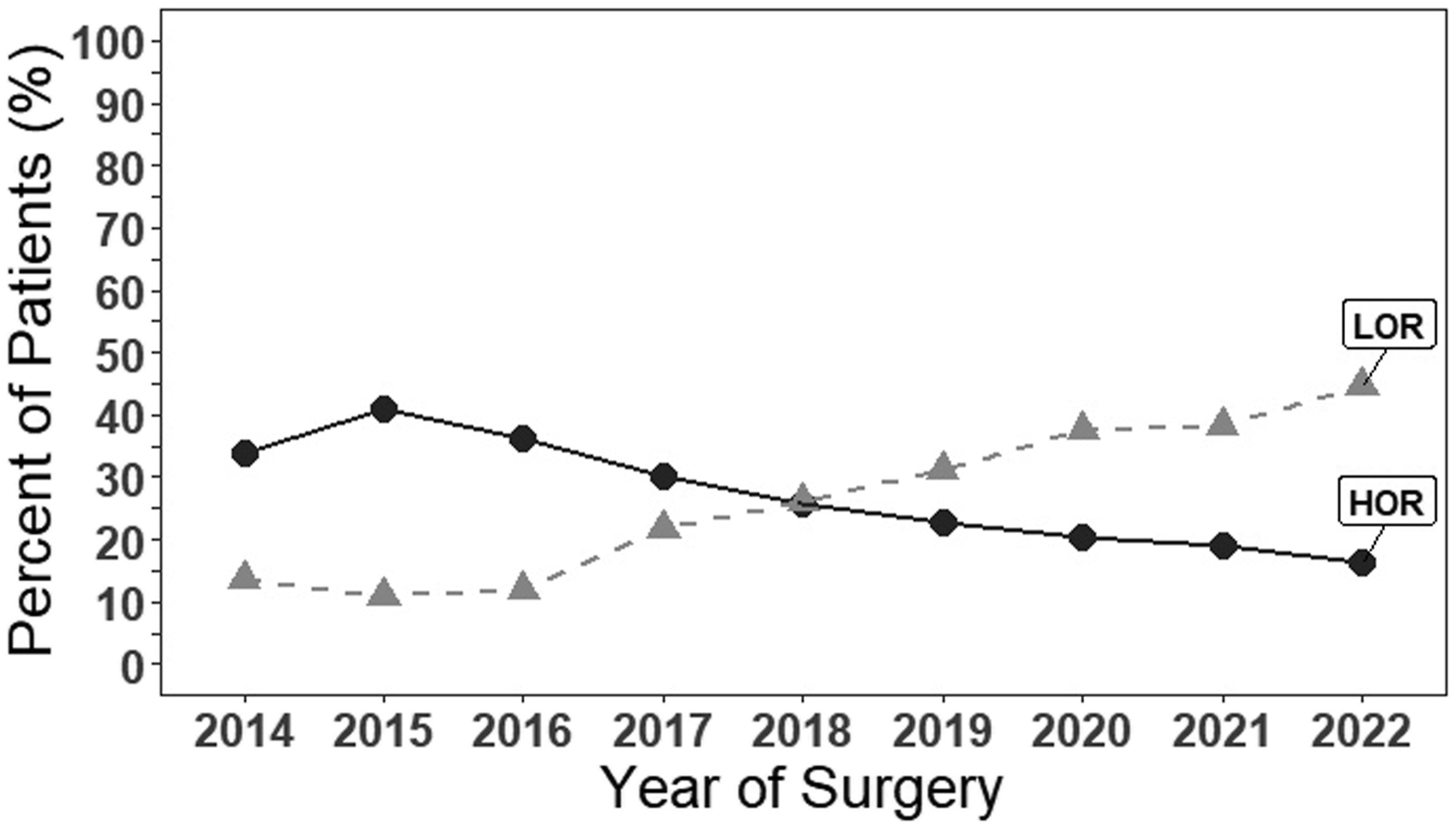
Similarly, relative to the MOR group, patients in the HOR group were younger (65 [57-71] vs 66 [58-73], P = 0.001), more male (75% vs 70.9%, P = 0.010) non-Caucasian/white patients (Caucasian/white patients: 71.3% vs 77%, P = 0.002). The HOR also had more patients with an ASA PS score of 3 (37.2% vs 23.4%, P = 0.003), more CABG patients (76.5% vs 58.1%, P < 0.001), more patients with current or former tobacco abuse (9.6% vs 6.3%, P < 0.001), and a higher BMI (30.87 (SD = 6.34) vs 29.78 (SD = 6.36); P < 0.001). Only 44.4% of MOR had surgery before 2018 compared to 54% of HOR (P < 0.001). (Table 1, Supplemental Table 1).
Patients in the LOR group were older (68 [51-74] vs 66 [58-73], P = 0.001) with fewer male patients (65.6% vs 70.9%, P = 0.010) compared to the MOR group. The LOR group also had fewer CABG patients (50.6% vs 58.1%, P < 0.001) and only 22.6% of LOR patients had surgery before 2018 compared to 44.4% MOR (P < 0.001). No differences were seen in race, ASA PS score, BMI, or tobacco abuse (Table 1, Supplemental Table 1).
Regarding perioperative variables between patient groups, the HOR group had a higher administration rate of non-opioid analgesics intraoperatively compared to MOR (41.7% vs 14.9%, P < 0.001) and LOR (41.7% vs 24.3%, P < 0.001). The HOR also had longer surgery duration compared to MOR (8.27 hours [7.22-9.59] vs 7.45 [6.45-8.65], P < 0.001) and LOR (7.35 [6.33-8.60], P < 0.001), as well as a shorter CPB duration relative to MOR (2.30 hours [1.82-2.92] vs 2.35 [1.88-3.13], P < 0.001) but not LOR (2.35 [1.88, 3.05], P = 0.051). Meanwhile, compared to MOR, the LOR had a higher administration rate of non-opioid analgesics intraoperatively (24.3% vs 14.9%, P < 0.001) but no differences in surgery duration (P = 0.142) or CPB duration (P = 0.198). (Table 2, Supplemental Table 1).
Pairwise Contrasts for Intraoperative Opioid Group Extracted From Multivariable Regression Results
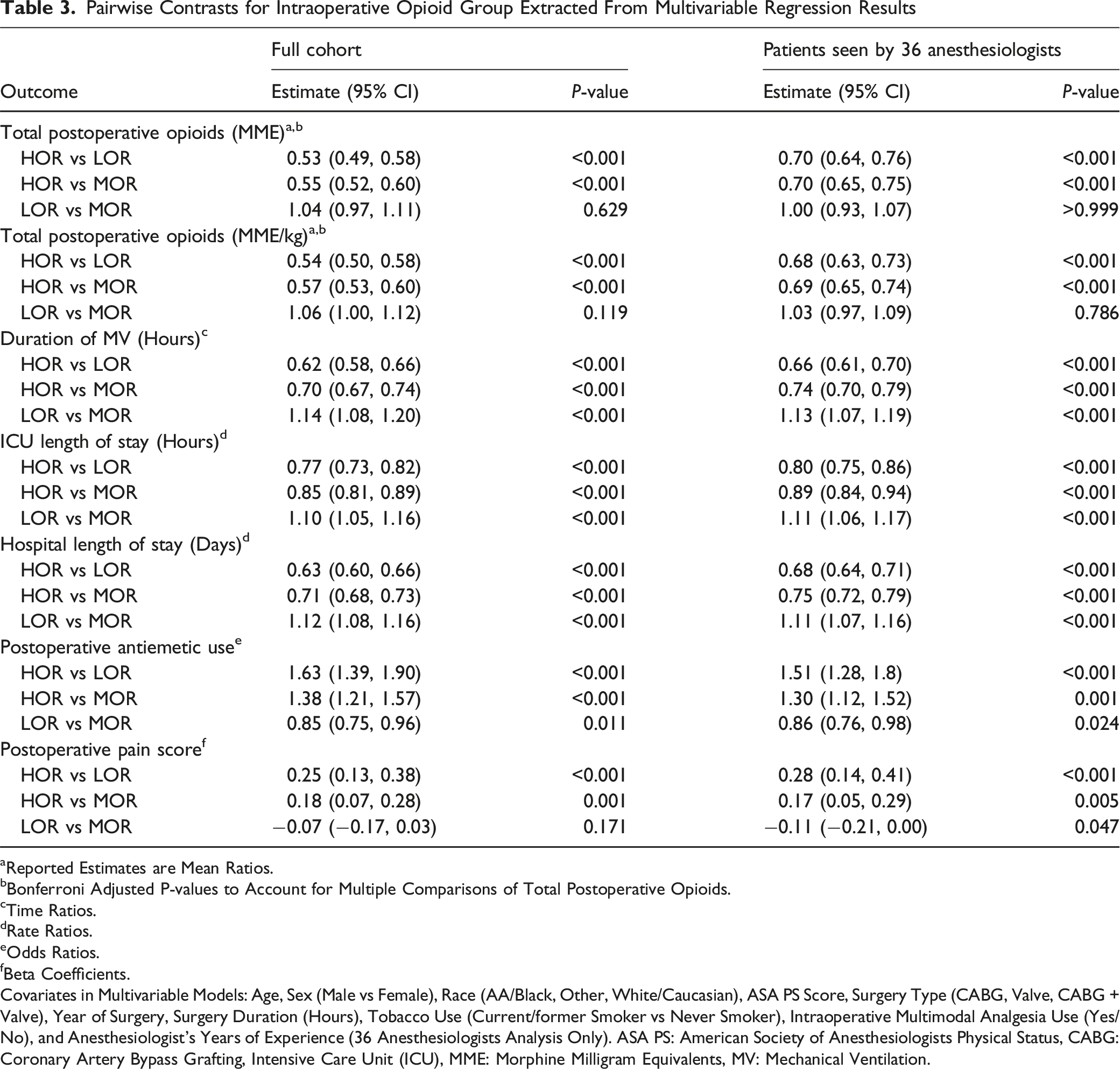
aReported Estimates are Mean Ratios.
bBonferroni Adjusted P-values to Account for Multiple Comparisons of Total Postoperative Opioids.
cTime Ratios.
dRate Ratios.
eOdds Ratios.
fBeta Coefficients.
Covariates in Multivariable Models: Age, Sex (Male vs Female), Race (AA/Black, Other, White/Caucasian), ASA PS Score, Surgery Type (CABG, Valve, CABG + Valve), Year of Surgery, Surgery Duration (Hours), Tobacco Use (Current/former Smoker vs Never Smoker), Intraoperative Multimodal Analgesia Use (Yes/No), and Anesthesiologist’s Years of Experience (36 Anesthesiologists Analysis Only). ASA PS: American Society of Anesthesiologists Physical Status, CABG: Coronary Artery Bypass Grafting, Intensive Care Unit (ICU), MME: Morphine Milligram Equivalents, MV: Mechanical Ventilation.
The HOR group is also associated with a 38% reduction in MV compared to the LOR group (TR = 0.62 (0.58, 0.66), P < 0.001), as well as a 23% and 37% reduction in ICU (RR = 0.77 (0.73, 0.82), P < 0.001) and hospital LOS (RR = 0.63 (0.60, 0.66), P < 0.001), respectively. Further, the HOR group is associated with an average of 0.25 point (95% CI: 0.13, 0.38) increase in postoperative pain scores and has 1.63 (95% CI: 1.39, 1.91) times the odds of postoperative antiemetic use. When comparing HOR to MOR, we continue to see similar relationships. The HOR group is associated with a 30% reduction in MV compared to the MOR group (TR = 0.70 (0.67, 0.74), P < 0.001) and a 15% and 29% reduction in ICU (RR = 0.85 (0.81, 0.89), P < 0.001) and hospital LOS (RR = 0.71 (0.68, 0.73), P < 0.001), respectively. The HOR group is also associated with an average of 0.18 point (95% CI: 0.07, 0.28) increase in postoperative pain scores (P < 0.001) and has 1.38 (95% CI: 1.21, 1.57) times the odds of postoperative antiemetic use relative to the MOR group.
Meanwhile, the LOR group is associated with a 13% increase in MV compared to the MOR group (TR = 1.13 (1.07, 1.19), P < 0.001) and an 11% increase in both ICU (RR = 1.11 (1.06, 1.17), P < 0.001) and hospital LOS (RR = 1.11 (1.07, 1.16), P < 0.001). No significant associations were found for postoperative pain score (Beta = −0.07 (−0.17, 0.03), P = 0.171) but LOR did have decreased antiemetic use (OR = 0.85 (0.75, 0.96), P = 0.011) (Table 3).
A total of 36 anesthesiologists were identified who performed at least 50 surgeries during the study period, spanning from 2014 to 2022. They were assigned a random number from 1 to 36 to maintain anonymity, and the variability in intraoperative opioid administration was demonstrated by showing the percentage of patients who qualified for the HOR group (Figure 3). In our sensitivity analysis, we replicated our multivariable models amongst the patients seen by only these anesthesiologists and adjusted for their years of experience at the time of the encounter. We found that the direction and size of the effects are similar, except for the comparison between LOR and MOR regarding postoperative pain. Percentage of intraoperative higher opioid recipients (HOR) by all 36 anesthesiologist who performed at least 50 surgeries during the study period. For this plot, the anesthesiologist’s years of experience was defined based on the first patient encounter observed within the time frame of our cohort. The dashed line represents the average percent of patients belonging to the HOR across the 36 anesthesiologists, which was 27%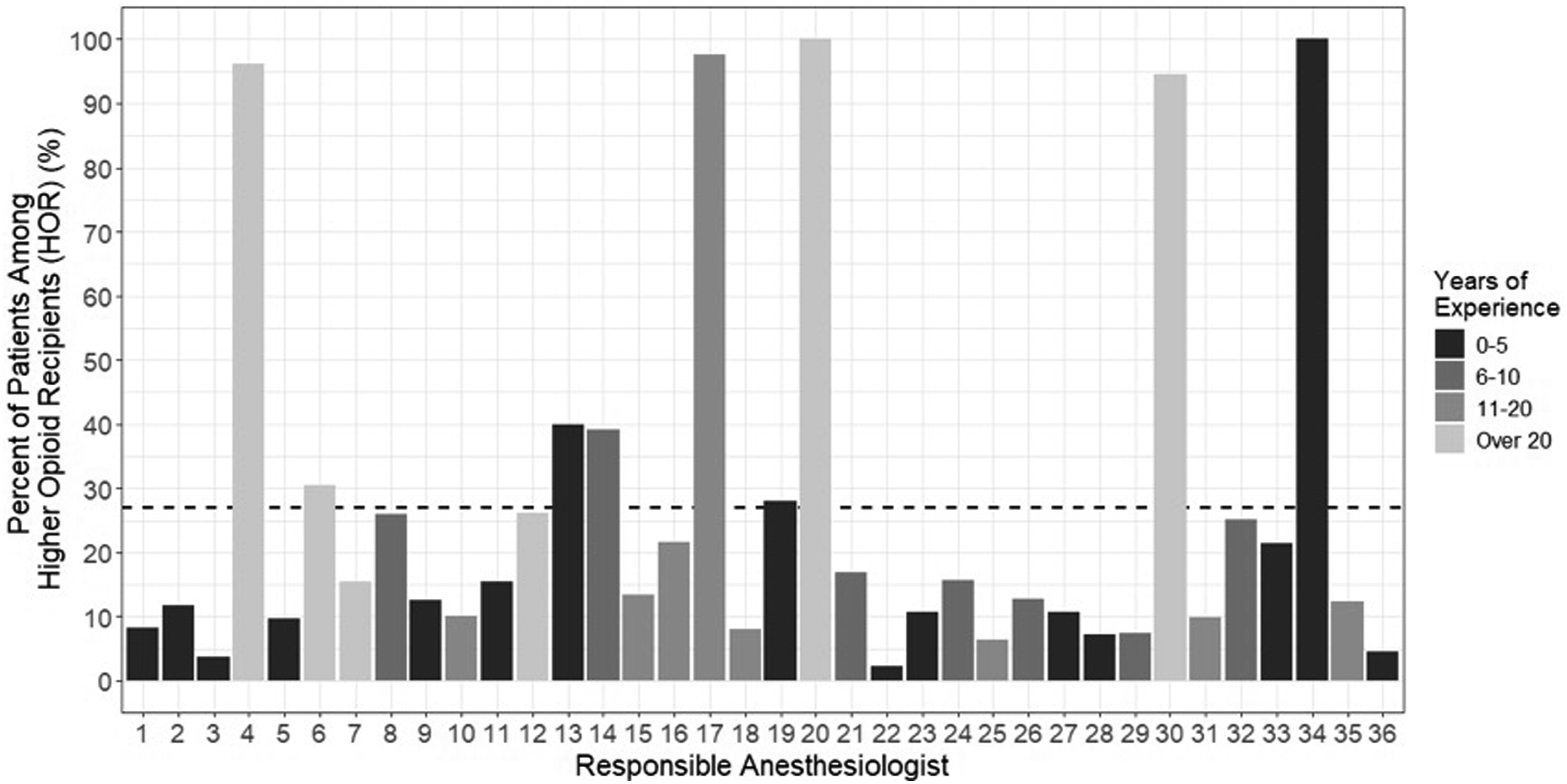
Finally, our secondary analysis using intraoperative opioids as a continuous predictor indicates increases in total intraoperative opioids (MME and MME/kg) are significantly associated with decreases in total postoperative opioids (MME and MME/kg), decreases in duration of MV, decreases in postoperative hospital and ICU length of stays, and increases in postoperative antiemetic use (Supplemental Table 2). As for postoperative pain scores, we found that intraoperative opioids measured in MME were significantly associated with increases in postoperative pain but did not find a significant association when intraoperative opioids were measured in MME/kg (Supplemental Table 2). Thus, except for postoperative pain scores, the size and direction of the effects seen when we treat both MME and MME/kg intraoperative opioid administration as a continuous predictor are like those seen when comparing our HOR vs LOR, HOR vs MOR, and LOR vs MOR groups.
Discussion
In this study, we evaluated intraoperative opioid administration in non-transplant and non-VAD cardiac surgery with CPB via a midline sternotomy over a 9-year period. We divided patients into “lower opioid recipients” (LOR) including the bottom 25% of our cohort, “higher opioid recipients” (HOR) including the top 25%, and “mid opioid recipients” (MOR) including the remaining 50% of patients. The intraoperative HOR were more likely to be younger, male, non-Caucasian/White, relatively healthier (ASA PS score ≤3), have a higher BMI, have a current or history of tobacco use, have underwent CABG surgery, and have had surgery performed earlier in the study period compared to the other two groups. Interestingly, HOR had a decrease in total postoperative opioid consumption, as well as reduction in duration of MV and ICU and hospital LOS compared to the other two groups after adjusting for other covariates. We also observed marked variability in intraoperative opioid administration among adult cardiac anesthesiologists at our institution, where around 14% administered higher doses of intraoperative opioids to over 90% of their patients.
While high-dose opioids have been one of the defining characteristics of a cardiac anesthetic for over 40 years, we expect this practice will become increasingly historical with the availability of contemporary, non-opioid analgesic agents. The opioid crisis in the United States accelerated the decline in the use of high-dose opioids. It began with the clinical push to make pain the “fifth vital sign,” meaning that physicians ensured that liberal administration and prescription of opioids reduced patients’ perception of pain.12,13 Unfortunately, opioid use begets higher opioid use, which in part is due to central sensitization of opioid receptors, increasing the requirement for more medication to produce the same biological effect. 14 Additionally, using high-dose opioids to treat acute pain carries the risk of developing a dose-dependent hyperalgesia and allodynia, 15 and it increases the risk of persistent opioid use 90 days after cardiac surgery. 16 Those concerns might explain the decline of intraoperative HOR over the 9-year study period, suggesting a shift in practice towards being less liberal with intraoperative opioids.
Another accelerator of this shift in opioid use, whether institutional or national, is the widespread implementation of ERAS programs. ERAS bundles are based on the aggregation of marginal gains, where a sum of evidence-based process interventions can achieve earlier return to preoperative physiologic function, improve outcomes in cardiac surgery,17-19 and reduce duration of MV and ICU and hospital LOS.20,21 The multimodal analgesia (MMA) opioid-sparing approach for pain management is one of those bundles, which employs the synergistic effect of non-opioid analgesics and regional anesthetic techniques to reduce perioperative opioid use in cardiac surgery.22,23 One of the essential elements of cardiac ERAS programs is the elimination of unnecessary variations in perioperative care delivery. 24 While the initial focus was on ERAS pre- and postoperative bundles, the emphasis is now shifting to intraoperative management and the role of the cardiac anesthesiologist. 25
In contrast to the growing consensus in the literature, our intraoperative HOR group was associated with lower total postoperative opioids and shorter duration of MV and ICU and hospital LOS. Higher intraoperative opioid doses may indicate better control of pain signals during surgery. By effectively suppressing nociceptive input, intraoperative analgesia may limit central sensitization and reduce the amplification of postoperative pain, which could ultimately lower the need for opioids after surgery. Alternatively, this discrepancy may have other explanations that merit consideration. First, we note that association does not imply causation, and this association may reflect residual confounding by case complexity. For example, lower-risk patients may receive higher opioid doses, which is very difficult to capture in a retrospective study such as ours. Furthermore, slight variation in individual anesthesiologist practice patterns, including comfort with higher-dose regimens may also contribute to our unique findings. Finally, unmeasured clinical factors (i.e., intraoperative hemodynamic stability, surgical efficiency, or postoperative pathways adherence) may partially account for the observed relationship. It is also worth pointing out that patients in the HOR group had higher mean pain scores compared to the other two groups, which is probably not clinically significant because it remained <4/10, which generally reflects adequately controlled pain. These findings highlight the need for individualized pain management plans rather than decreasing opioids arbitrarily, which is likely the wrong clinical approach. If that decrease in opioids is not associated with MMA optimization, it may be followed by an increase in postoperative opioid consumption, which in turn can be more detrimental to duration of MV and ICU and hospital LOS.
There are two possible explanations for this discrepancy between our findings and other studies on outcomes after high-dose intraoperative opioids. First, the lack of a standardized definition for high vs low dosage makes comparison of outcomes more challenging. In our study, patients were labeled as HOR if they received more than 113 MME intraoperatively, which was lower than that of high-dose opioid recipients in other studies. For example, Rong et al used a higher cutoff limit of >2 mg/kg of MME, 6 Wong et al used >20 mcg/kg of fentanyl mcg equivalents, 7 and Fisher et al reported on patients receiving a mean of 1139 fentanyl mcg equivalents. 5 A second reason is the lack of a standardized definition of MMA, which is typically defined as achieving adequate pain relief using several pain medications and regional techniques that work via different mechanisms. For example, Stepan et al reported outcomes on patients receiving high-dose opioids (8-10 mcg/kg of fentanyl mcg equivalents), which is lower than the opioid dose in our HOR group, but their patients received intraoperative lidocaine and ketamine boluses followed by lidocaine and dexmedetomidine infusions. 8 Similarly, Grant et al reported outcomes on patients receiving high-dose opioids (>50 MME), which is also much lower than the opioid dose in our HOR group. However, their patients received five non-opioid interventions including preoperative gabapentin and acetaminophen, intraoperative dexmedetomidine and ketamine infusions, in addition to intraoperative regional serratus anterior plane block. 11 It is difficult to compare patients who received vastly different regimens of MME. For example, compared to our study, patients in the Grant et al study were more likely to receive acetaminophen (47% vs 11%), ketamine infusions (57% vs 5%), dexmedetomidine infusions (17.5% vs 8%), and regional blocks (28.4% vs 4.3%). 11
Unlike postoperative pain, where opioid administration is mostly dictated by patients’ pain scores on a pain numeric rating scale, intraoperative opioid administration is determined mainly by the provider’s subjective estimation of analgesic needs of their patients. Similar to previous studies, patients in the HOR group were more likely to be younger, healthier (ASA PS 3), with higher BMI and longer surgery duration.26,27 Similar sex disparities were previously reported, where females received lower doses of opioids, 26 despite reporting more surgical pain. 28 While racial disparities were previously reported, where Caucasian/white patients received more opioids for postoperative pain, 28 other health systems have reported no racial disparities, particularly if standardized management pathways were used. 29 Additionally, patients in the HOR group also received more non-opioid analgesics, reflecting a subjective concern about adequate pain control in patients with the previously mentioned baseline characteristics, where those patients were given more intraoperative opioid and non-opioid analgesics.
Understanding practice variations among anesthesia providers and their related patient outcomes would provide a unique insight into the daily practices of providers that directly influence patient outcomes. 30 Previous studies have reported substantial variations in intraoperative opioid administration across cases, which were not attributed to patient and surgical characteristics, but rather to provider and institutional practices.4,5 We included all adult cardiac anesthesiologists who provided care to a considerable number of patients and observed marked variability in intraoperative opioid administration, where several of the cardiac anesthesiologists administered high-dose intraoperative opioids in over 90% of their patients.
Our study was conducted retrospectively at a single academic tertiary center. Findings were observational and may be confounded by many factors including patient selection and provider preference. Our study was also limited by the lack of a formal ERAS program for cardiac surgery, and no new ERAS elements were adopted during the study period. Therefore, our results, which include low utilization of regional blocks in midline sternotomy patients, may differ from institutions that use regional blocks more routinely. Intraoperative opioid use was divided according to predetermined cutoffs, which neither capture the complexity of variations in dose, timing, and type of opioid used, nor consider the type of general anesthesia induction or maintenance agents (inhalational agents vs total intravenous anesthesia). We reported our opioid consumption in MME for improved standardization, but the exchange rates used to calculate opioid dosage are approximate, and MME conversion tables and calculators have inherent inaccuracies and marked variability in calculation methods. 31
In conclusion, among patients undergoing elective adult cardiac surgery via midline sternotomy at a single academic center, higher doses of intraoperative opioids were associated with lower postoperative opioid consumption, which may have contributed to faster recovery. Marked variability in opioid administration was observed among cardiac anesthesiologists, with several using a high-dose opioid technique. While higher intraoperative opioid use has been decreasing over time, its use remains a common practice in cardiac anesthesia, which highlights the need for standardized definitions of multimodal analgesia and precise distinction between high and low dose opioid techniques.
Supplemental Material
Supplemental Material - Variations in Intraoperative Opioid Use in Cardiac Surgical Patients With Midline Sternotomy
Supplemental Material for Variations in Intraoperative Opioid Use in Cardiac Surgical Patients With Midline Sternotomy by Negmeldeen Mamoun, MD, PhD, Morgan A Rosser, MS, Kamrouz Ghadimi, MD, Crosby Culp, MD, Bryan Chow, MD, Katherine Sun, MD, Sharon McCartney, MD, and Michael Manning, MD, PhD in Seminars in Cardiothoracic and Vascular Anesthesia.
Footnotes
Author Contributions
Negmeldeen Mamoun, MD, PhD: Role: This author helped design and implement the study and write the manuscript. Attestation: This author approved the final manuscript. Morgan A Rosser, MS: Role: This author helped design and implement the study and write the manuscript. Attestation: This author approved the final manuscript. Kamrouz Ghadimi, MD: Role: This author helped write the manuscript. Attestation: This author approved the final manuscript. Crosby Culp, MD: Role: This author helped design and implement the study and write the manuscript. Attestation: This author approved the final manuscript. Bryan Chow, MD: Role: This author helped design and implement the study and write the manuscript. Attestation: This author approved the final manuscript. Katherine Sun, MD: Role: This author helped design and implement the study and write the manuscript. Attestation: This author approved the final manuscript. Sharon McCartney, MD: Role: This author helped design and implement the study and write the manuscript. Attestation: This author approved the final manuscript. Michael W Manning, MD, PhD: Role: This author helped design and implement the study and write the manuscript. Attestation: This author approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.