
Abstract
Alpha-gal syndrome (AGS) is an IgE-mediated hypersensitivity to galactose-α-1,3-galactose, an oligosaccharide found in mammalian tissues, including bovine or porcine-derived bioprosthetic valves and heparin. Concerns exist regarding perioperative hypersensitivity reactions in patients with AGS undergoing cardiac surgery involving xenogeneic materials. We present three patients with documented AGS who underwent transcatheter aortic valve replacement (TAVR) using bovine or porcine-derived bioprostheses. All patients underwent a preoperative evaluation by allergists, and two received no pharmacological pre-treatment. Intraoperative heparin administration was without adverse reactions in all cases. Postoperative courses were uncomplicated, with no evidence of immediate or delayed allergic responses. Follow-up periods ranged from 4 to 6 years without structural valve deterioration attributable to AGS. These cases demonstrate that patients with AGS can safely undergo TAVR with bovine or porcine-derived valves and heparin, provided they are appropriately evaluated and monitored. Despite theoretical concerns, perioperative hypersensitivity appears to be rare in this population, supporting the feasibility of xenogeneic valve use in AGS patients.
Introduction
Alpha-gal syndrome (AGS) is an increasingly recognized IgE-mediated allergy to the carbohydrate epitope galactose-α-1,3-galactose (“alpha-gal”), found in most non-primate mammalian tissues. 1 The condition is most often triggered by bites from the Lone Star tick (Amblyomma americanum) in the United States. It leads to delayed anaphylactic or allergic responses following ingestion or parenteral exposure to mammalian-derived products (including red meat, gelatin, bovine/porcine tissues, and heparin). 2
Epidemiologic evidence indicates that AGS is more prevalent than previously appreciated. The Centers for Disease Control surveillance data identified approximately 90,000 suspected cases between 2010 and 2022, with estimates suggesting up to 450,000 Americans may have developed AGS during this period, particularly in the southeastern, mid-Atlantic, and central United States. These regions parallel the expanding geographic range of A. americanum. 3 Because porcine and bovine-derived materials are ubiquitous in cardiac anesthesia and surgery (bioprosthetic valves, pericardial patches, heparin, gelatin-based agents), patients with AGS represent a unique perioperative management dilemma, given both xenogeneic tissue and mammalian-derived anticoagulants may trigger immunologic risk.
For patients requiring cardiac surgery, specifically those undergoing aortic valve replacement or transcatheter aortic valve replacement (TAVR), AGS poses dual concerns: the risk of hypersensitivity reactions and potential consequences for long-term bioprosthetic durability in the context of immune activation. Yet only a handful of perioperative reports describe the course of AGS patients undergoing surgical bioprosthetic valve replacement, and none detail long-term outcomes following a transcatheter approach. 4
In all three cases presented, patients had severe symptomatic aortic valve disease requiring intervention, and the multidisciplinary heart team determined that the benefits of TAVR outweighed the theoretical risk of hypersensitivity. Surgical and transcatheter bioprosthetic valves remain the standard of care for many elderly patients, and currently available alternatives free of mammalian-derived tissue are limited.
We therefore present a case series of three patients with documented AGS who successfully underwent TAVR with mammalian-derived bioprosthetic valves and standard heparin anticoagulation, highlighting perioperative management strategies, outcomes, and implications for long-term follow-up in this emerging patient population.
Cases
Case 1
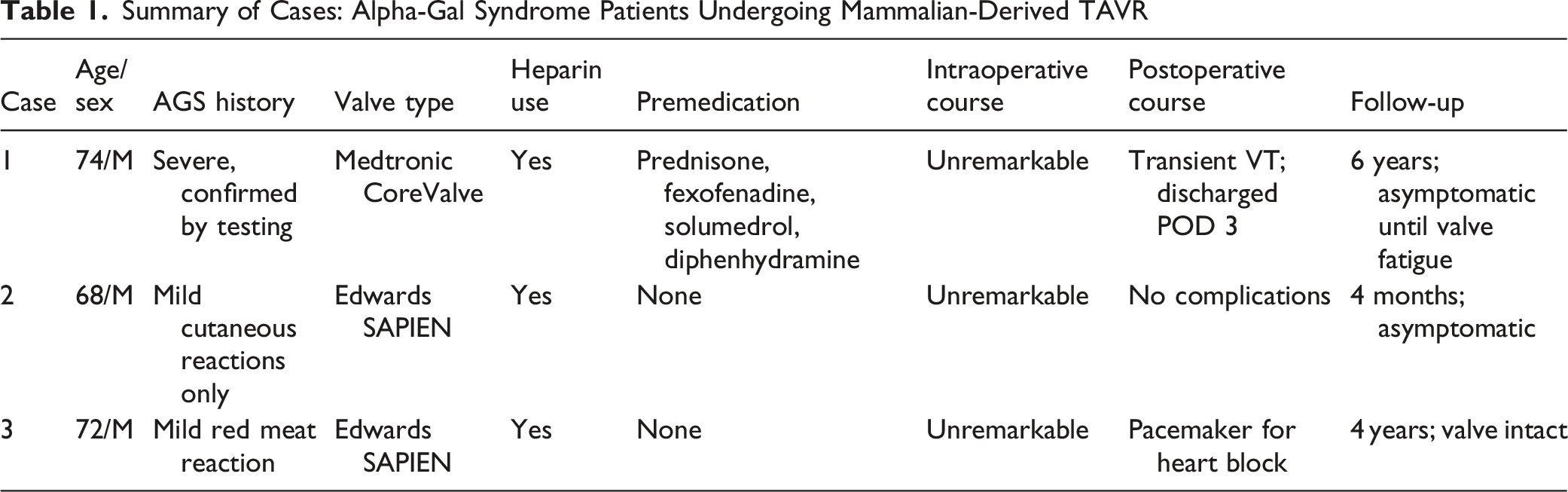
A 74-year-old male with AGS and critical aortic stenosis underwent TAVR with a 29 mm Medtronic CoreValve ® (Minneapolis, MN) with no evidence of paravalvular leak on postoperative echocardiogram. The patient had a prior history of delayed allergic reactions following mammalian meat ingestion, which prompted formal allergy evaluation and confirmatory testing for AGS, and perioperative prophylactic premedication included prednisone, fexofenadine, solumedrol, and diphenhydramine. Intraoperative unfractionated heparin was tolerated without adverse reaction.
Postoperatively, the patient experienced a transient episode of ventricular tachycardia that was self-resolving. He was discharged on postoperative day 3 and followed regularly. Six years later, he developed severe aortic regurgitation likely related to structural valve degeneration and prosthetic fatigue. Although a contribution from chronic immune-mediated processes related to AGS cannot be completely excluded, there was no definitive evidence linking AGS to accelerated valve degeneration in this case. The patient was offered a replacement of his prosthetic valve, but the patient declined. No allergic or hypersensitivity reactions were reported throughout his course.
Case 2
A 68-year-old male with AGS, hypertension, hyperlipidemia, paroxysmal atrial fibrillation, atrioventricular block, mast cell syndrome, and aplastic anemia (receiving bi-weekly transfusions) underwent TAVR with a 26 mm Edwards SAPIEN ® valve (Irvine, CA) with no evidence of paravalvular leak on postoperative echocardiogram. Despite a history of mild cutaneous reactions to red meat, he had no history of anaphylaxis. No preoperative pharmacologic prophylaxis was administered.
The intraoperative course was unremarkable, and the patient tolerated intravenous heparin without reaction. The postoperative period was uncomplicated, and he remains symptom-free on cardiology follow-up roughly 4 months after the procedure, without allergic manifestations.
Case 3
A 72-year-old male with AGS (previous mild red-meat reaction), Type 2 diabetes mellitus, BMI 32, and hypertension underwent TAVR with a 26 mm Edwards SAPIEN ® valve (Irvine, CA) for severe aortic stenosis with no evidence of paravalvular leak on postoperative echocardiogram. No perioperative prophylaxis was given.
The intraoperative course was uncomplicated. Postoperatively, the patient developed complete heart block requiring permanent pacemaker implantation, attributed to the anatomical location of valve placement rather than hypersensitivity. At 4-years of follow-up, he remains asymptomatic with preserved valve function and no allergic sequelae.
Discussion
Alpha-gal syndrome (AGS) is an IgE-mediated delayed hypersensitivity reaction directed against the carbohydrate epitope galactose-α-1,3-galactose (α-gal), which is extensively expressed in non-primate mammalian tissues. Sensitization is most commonly attributed to Lone Star tick bites in the United States, which introduce α-gal through salivary glycoproteins and stimulate the formation of specific IgE antibodies. 5 When patients are re-exposed to α-gal, by either the consumption of mammalian products or exposure to medical materials such as bioprosthetic heart valves or porcine-derived heparin, they can develop systemic allergic reactions. 6 Unlike most food allergies that appear within minutes, reactions in AGS tend to occur several hours later, typically between 3 and 8 hours, due to the lipid-based absorption and transport of the allergen. 7 The immune response to xenogeneic cardiac tissue, however, isn’t identical to that from dietary exposure. Processing steps involved in preparing bioprosthetic valves, including fixation, decellularization, and sterilization, alter the α-gal epitope sufficiently to reduce its immunogenicity, which may help explain why hypersensitivity is less common during procedures like transcatheter aortic valve replacement (TAVR). 8 Evidence of long-term tolerance of mammalian-derived prosthetic valves in these patients provides further evidence to support this claim.
The decision to proceed with TAVR in these patients was based on a careful multidisciplinary risk-benefit assessment. Given the severity of symptomatic aortic valve disease and the absence of readily available non-mammalian valve alternatives, the potential benefits of valve replacement were felt to outweigh the theoretical risk of hypersensitivity. Additionally, previously published reports suggest that clinically significant perioperative reactions remain relatively uncommon, particularly with contemporary extensively processed bioprosthetic valves.
Comparison With Prior Studies
Summary of Cases: Alpha-Gal Syndrome Patients Undergoing Mammalian-Derived TAVR
Considerations
Several factors may explain the absence of allergic reactions in our patients. Modern TAVR valves undergo extensive decellularization and glutaraldehyde fixation, processes that markedly reduce α-gal antigenicity. Although glutaraldehyde fixation has been standard for surgical valves for decades, current-generation TAVR valves, which have been commercially available since 2011-2014, incorporate more aggressive decellularization and anticalcification treatments than earlier surgical bioprostheses. It is therefore possible that earlier reports of hypersensitivity reflected exposure to less-processed valve tissue, whereas contemporary transcatheter valves contain substantially lower levels of residual immunogenic epitopes. 12 Experimental data have shown that α-gal-free or enzymatically treated xenografts provoke significantly less IgM- and IgE-mediated immune activation, correlating with improved bioprosthetic durability.13,14 Moreover, delayed hypersensitivity may not be efficiently triggered by the limited antigen exposure that occurs during TAVR, as opposed to systemic exposure to heparin or parenterally administered bovine-derived agents. Variability in α-gal IgE titers among individuals also likely contributes to heterogeneous clinical responses. 15 Heparin presents a unique challenge because, although it is porcine in origin, its antigenic α-gal content may vary by manufacturer and lot. 16 Prior studies demonstrated that up to 50% of AGS patients with high IgE titers may develop hypersensitivity to high-dose heparin during cardiopulmonary bypass, particularly in those with recent tick sensitization. 17 In contrast, low-dose heparin used during TAVR may fall below the threshold for reaction.
Recent advances in xenogeneic tissue engineering have focused on the development of genetically modified pigs that lack expression of the α-gal epitope. Alpha-gal–deficient (“GalSafe”) pigs have received U.S. Food and Drug Administration approval for food and biomedical applications, and their tissues are being actively investigated for use in implantable medical devices, including bioprosthetic heart valves. Preclinical studies suggest that α-gal–negative porcine tissues provoke less IgM- and IgE-mediated immune activation and may exhibit reduced calcification compared with conventional porcine xenografts. At present, however, no commercially available transcatheter or surgical heart valve marketed by major manufacturers, including Edwards Lifesciences or Medtronic, is derived from genetically modified α-gal–deficient porcine tissue. As such, current clinical practice continues to rely on extensively processed conventional porcine bioprostheses. The emergence of α-gal–free valve technologies may ultimately alter recommendations for patients with AGS, but further clinical validation is required. 18
Clinical Implications
Our findings highlight the importance of a coordinated team approach in caring for AGS patients who require cardiac procedures. Taking a thorough allergy history and checking α-gal IgE levels ahead of time may help identify patients at higher risk and inform how we manage them perioperatively. 19 For patients who have had recent reactions or have positive α-gal titers, it is reasonable to give corticosteroids, H1 and H2 blockers, and a leukotriene inhibitor before the anticipated procedure. 20 In higher-risk cases, or when cardiopulmonary bypass is needed, non-heparin anticoagulants like bivalirudin or argatroban can be used instead. However, they are more difficult to reverse and require close monitoring. 21 Clear multidisciplinary communication among anesthesia, cardiology, allergy, and surgical teams is also important to minimize perioperative risk and avoid unexpected intraoperative reactions. Additionally, heparin skin testing may help identify tolerance preoperatively when the clinical history is not clear. 22
Study Limitations
This case series is limited by its small sample size, retrospective design, and absence of uniform α-gal IgE quantification. Given the rarity of AGS and the heterogeneity of clinical presentations, the lack of systematic allergy testing and follow-up precludes definitive conclusions regarding long-term valve durability or the protective effect of decellularization. 23 We are also unable to rule out the possibility of subclinical hypersensitivity or delayed, immune-driven changes in the valve over an extensive period of time. Prospective studies that combine biochemical valve analysis with immunologic profiling will be crucial for better understanding these potential links.
Future Directions
Future investigations would ideally establish multicenter registries to capture procedural and immunologic outcomes of AGS patients undergoing cardiac surgery and TAVR. Laboratory studies assessing residual α-gal antigenicity in commercially available bioprostheses, as well as the efficacy of α-gal–negative xenografts, could further inform device selection. It would be helpful to have standardized perioperative guidelines that cover premedication, heparin testing, and postoperative monitoring to make these procedures safer for patients. Taken together, these steps could improve how we assess risk and might eventually allow for more personalized approaches to cardiac surgery for the increasing number of patients with α-gal sensitization.
Conclusion
Patients with alpha-gal syndrome can safely undergo TAVR with mammalian-derived valves and heparin when appropriately evaluated and monitored. Despite theoretical hypersensitivity risk, no immediate or delayed allergic reactions occurred in this series, suggesting that xenogeneic bioprostheses remain a viable option for AGS patients requiring valve replacement. Notably, one patient underwent successful prophylactic premedication following preoperative allergy evaluation, while the remaining patients tolerated the procedure without prophylaxis or hypersensitivity reactions.
Footnotes
Ethical Considerations
This study is exempt from Institutional Review Board (IRB) review because it did not involve human subjects research as defined by federal regulations. Therefore, formal ethical approval and informed consent were not required.
Consent to Participate
The requirement for written informed consent was waived due to the retrospective nature of the study and the use of de-identified data.
Consent for Publication
Written informed consent for publication of clinical details was obtained from all patients included in this case series. In cases where patients were deceased or unable to provide consent, written informed consent was obtained from the patient’s legally authorized representative or next of kin. Copies of the written consent forms are available for review by the Editor of this journal upon request.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.