
Abstract
Objectives
Vasopressor choice potentially contributes to postoperative delirium due to differences in end-organ perfusion. This study seeks to determine the rates of postoperative delirium after perioperative phenylephrine, ephedrine, or norepinephrine administration.
Design
Retrospective, propensity-score matched multicenter database study.
Participants
Patients aged 60 and older undergoing surgery of the integumentary, musculoskeletal, respiratory, hematologic/lymphatic, gastrointestinal, genitourinary/reproductive, endocrine, or sensory organ systems.
Interventions
Perioperative vasopressor administration (phenylephrine, ephedrine, norepinephrine).
Measurements and Main Results
The primary outcome was the incidence of postoperative delirium based on ICD-10 diagnostic codes within seven days of surgery. After propensity score matching, there was no difference in the rate of postoperative delirium between phenylephrine and norepinephrine (OR 0.97; 95% CI 0.61–1.54; P = .9065) or between ephedrine and norepinephrine (OR 0.74; 95% CI 0.41-1.32; P = .3062). Phenylephrine was associated with a higher rate of postoperative delirium when compared to ephedrine (OR 1.30; 95% CI 1.05–1.60; P = .0162), although absolute risk difference was small (0.05%).
Conclusions
This study highlights the potential influence of vasopressor selection on postoperative neurocognitive outcomes in older adults. Understanding the physiologic and pharmacologic mechanisms underlying these associations may help guide individualized intraoperative management and reduce delirium risk in clinical practice.
Introduction
Postoperative delirium is a common neurological complication of anesthesia, characterized by transient alterations in consciousness, cognition, and awareness. It has been associated with adverse outcomes, including increased mortality and 1-year cognitive decline.1,2 The incidence of postoperative delirium is significantly influenced by intraoperative factors such as cerebral deoxygenation and hypotension, both of which can compromise cerebral perfusion and contribute to acute cognitive dysfunction.3,4 Vasopressor selection may contribute to this risk. Phenylephrine has previously been associated with increased postoperative delirium compared to ephedrine.5,6
Although phenylephrine and ephedrine have been compared in this context, norepinephrine is another commonly used agent with unclear effects on postoperative delirium. Comparisons between norepinephrine and ephedrine have primarily focused on outcomes such as nausea and hypotension, as these agents are commonly used in anesthetic practices.7,8 However, to our knowledge, the rates of postoperative delirium among all three agents have not been compared.
This multi-center, large database retrospective study aims to investigate the effects of norepinephrine compared to ephedrine and phenylephrine, administered on the day of surgery, on the incidence of postoperative delirium. We hypothesize that the incidence of postoperative delirium is similar following the administration of ephedrine vs norepinephrine on day of surgery due to similar mechanisms of action, and both vasopressors will have lower rates of postoperative delirium when compared to phenylephrine.
Methods
Data and Ethical Considerations
The TriNetX research network is a database that complies with the Health Insurance Portability and Accountability Act and relevant US federal regulations. It contains de-identified electronic medical records from 72 healthcare organizations across the United States, including academic medical centers and community hospitals. The data is de-identified in order to protect patient privacy; the identities of participating organizations and their specific contributions to the dataset are kept confidential to prevent potential re-identification of data. This study received a Determination of Non-Human Subjects Research (Protocol #30442) and was registered in ClinicalTrials.gov (NCT06844201).
Study Design
This retrospective analysis utilized data from 2005 to 2025, collected on October 29th, 2025, from the TriNetX US Collaborative Network. This study was designed to assess the impact of intraoperative norepinephrine use on the development of postoperative delirium, with phenylephrine and ephedrine included as comparators. To demonstrate the validity of the dataset and methodology, a comparison between intraoperative phenylephrine and ephedrine use was also conducted, as this relationship has been previously studied and characterized in the literature.5,6
Cohort Selection
Our inclusion criteria consisted of patients aged 60 years and older who underwent surgery of the integumentary, musculoskeletal, respiratory, hematologic/lymphatic, gastrointestinal, genitourinary/reproductive, endocrine, or sensory organ systems and were either administered norepinephrine, ephedrine, or phenylephrine on the day of surgery. Patients must not have received more than one of these vasopressors on the day of surgery in order to isolate the effects of each individual vasopressor. Patients who underwent surgical procedures of the neurovascular or cardiovascular systems were excluded in order to isolate noncardiac, nonneurosurgical postoperative delirium. Those who were administered epinephrine or dopamine on the day of surgery were also excluded in order to avoid confounding by other medications and exclude patients with increased illness severity. In order to isolate the effects of intraoperative vasopressor use and minimize confounding from patients requiring postoperative hemodynamic support, individuals who were administered phenylephrine, ephedrine, or norepinephrine seven days before or after the day of surgery were excluded. We also excluded patients with a diagnosis of sepsis, severe sepsis, other sepsis, streptococcal sepsis, hypotension, shock, or blood transfusion within seven days before and after surgery to exclude patients who may be more acutely ill compared to other patients or may require nonoperative vasopressor use. Finally, patients with a prior history of disorientation or unspecified dementia were excluded for homogeneity (Figure 1). Flow diagram of cohort selection from the TriNetX US collaborative network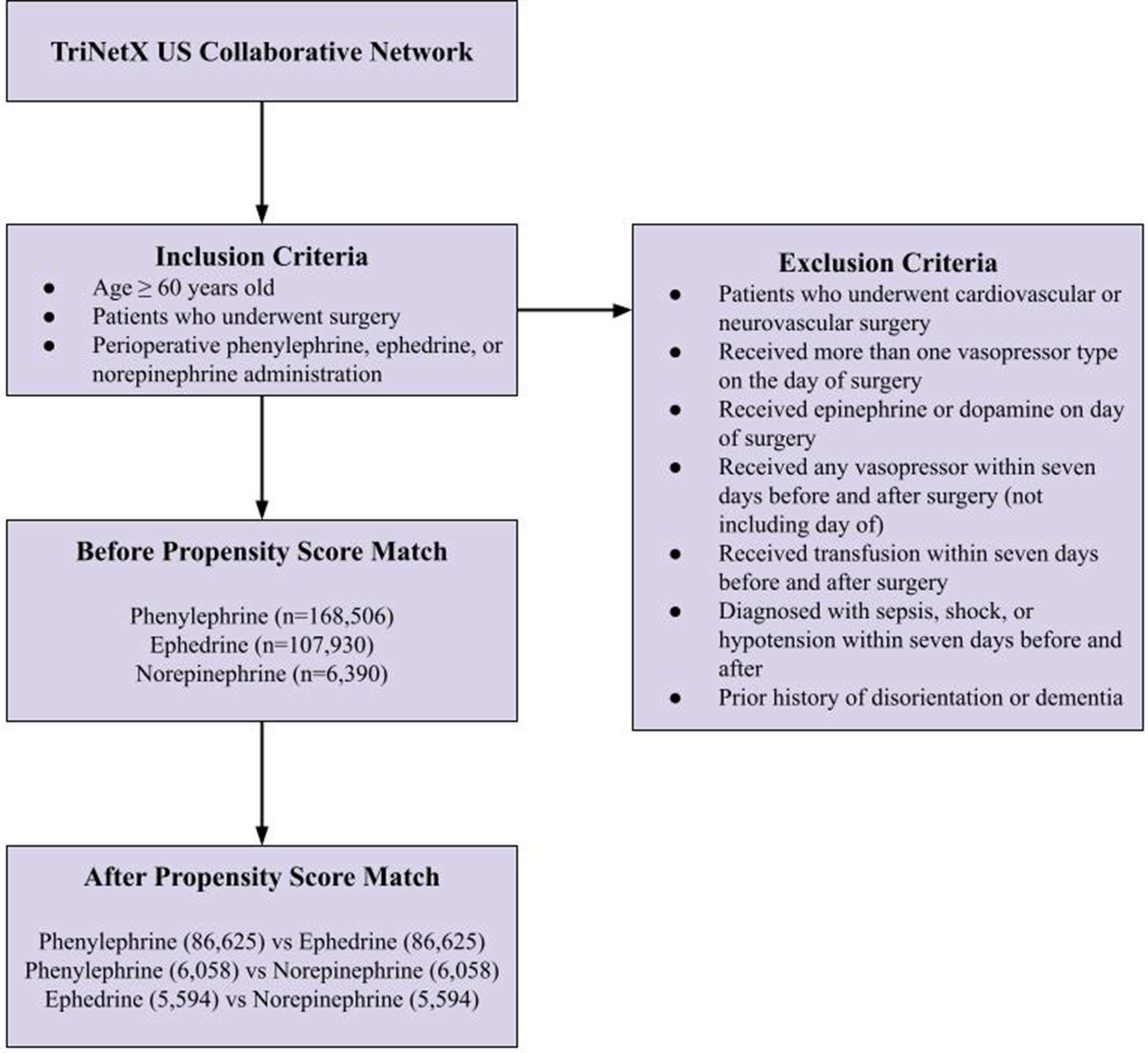
Propensity Score Matching
Propensity score matching (1:1) using greedy-nearest-neighbor without replacement (caliper = 0.1) through TriNetX was performed to adjust for potential confounders, including demographic factors such as age, sex, race, and ethnicity; comorbidities including essential hypertension, hypertensive heart disease with and without heart failure, hypertensive heart and chronic kidney disease, other chronic obstructive pulmonary disease, asthma, emphysema, bronchiectasis, unspecified chronic bronchitis, depression, type 2 diabetes mellitus, occlusion and stenosis of precerebral arteries or cerebral arteries (not resulting in cerebral infarction), cerebral infarction, hyperlipidemia, overweight and obesity, BMI, neoplasms, chronic kidney disease, heart failure, hypothyroidism, chronic ischemic heart disease, hypotension, other diseases of the respiratory system, chronic lower respiratory diseases, influenza and pneumonia, aplastic and other anemias and other bone marrow failure syndromes, other disorders of blood and blood-forming organs, coagulation defects, purpura and other hemorrhagic conditions, nutritional anemias, certain disorders involving the immune mechanism, and hemolytic anemias; behavioral and medication-related factors such as alcohol abuse and dependence, nicotine dependence, use of antipsychotics, and use of benzodiazepines/sedatives; infectious diseases; clinical context variables including critical care management; and prior surgical history and index surgical procedure type.
For each surgical system, matching was performed at one hierarchical level below the parent CPT category as categorized within the TriNetX platform (e.g., “Surgical Procedures on the Urinary System”), corresponding to its immediate subcategories (e.g., “Surgical Procedures on the Kidney,” “Surgical Procedures on the Ureter,” “Surgical Procedures on the Bladder,” and “Surgical Procedures on the Urethra”). Deeper hierarchical CPT levels were not included in the matching process to avoid exceeding the variable limit for propensity score modeling and to maintain adequate statistical power within each stratum. Standard mean differences (SMD) were calculated and are presented in Supplemental Table S1, with acceptable SMD <0.1.
Outcome and Statistical Analysis
To evaluate the relationship between vasopressor choice and postoperative delirium, separate propensity score-matched analyses were performed comparing phenylephrine, ephedrine, and norepinephrine cohorts. The outcome of postoperative delirium was measured using the ICD-10 codes F05 (delirium due to known physiological condition), R40 (somnolence), and R41 (disorientation). The ICD-10 codes for somnolence and disorientation had a modifier of delirium and were therefore included to define the outcome of delirium. The occurrence of postoperative delirium was tracked from the day of surgery to one week postoperative. Risk differences and odds ratios (OR) with 95% confidence intervals were computed for each pairwise comparison (phenylephrine vs ephedrine, ephedrine vs norepinephrine, phenylephrine vs norepinephrine) to assess differences in postoperative delirium incidence. The TriNetX platform (TriNetX, LLC; Cambridge, MA, USA) was used for all analyses, which utilizes logistic regression for binary outcomes. To account for multiple pairwise comparisons among vasopressor groups, P-values were adjusted using the Holm–Bonferroni method, with two-sided adjusted P < 0.05 representing statistical significance. This manuscript was completed in alignment with the STROBE guidelines.
Results
Patients who met inclusion criteria for phenylephrine (n = 168,506), ephedrine (n = 107,930), and norepinephrine (n = 6390) were identified and propensity score matched individually. After matching, the analysis consisted of three separately matched cohorts: phenylephrine vs ephedrine (173,250 total patients), phenylephrine vs norepinephrine (12,116 total patients), and ephedrine vs norepinephrine (11,188 total patients). All covariates were adequately balanced after matching (SMD <0.1) except for BMI which remained moderately imbalanced between the phenylephrine vs norepinephrine (SMD = 0.1671) and ephedrine vs norepinephrine (SMD = 0.1276) comparisons.
Phenylephrine Versus Ephedrine
After matching, both cohorts were adjusted to 86,625 patients each, with mean ages of 67.5 ± 9.0 and 67.5 ± 8.8, respectively. The odds of postoperative delirium was approximately 30% higher in patients receiving phenylephrine (n = 198 [0.23%]) vs ephedrine (n = 153 [0.18%]) (RD 0.05% [0.01%–0.09%]; OR 1.30 [1.05-1.60]; P = 0.0162; Figure 2). Seven-day incidence of postoperative delirium following intraoperative phenylephrine vs ephedrine administration (P = .0162)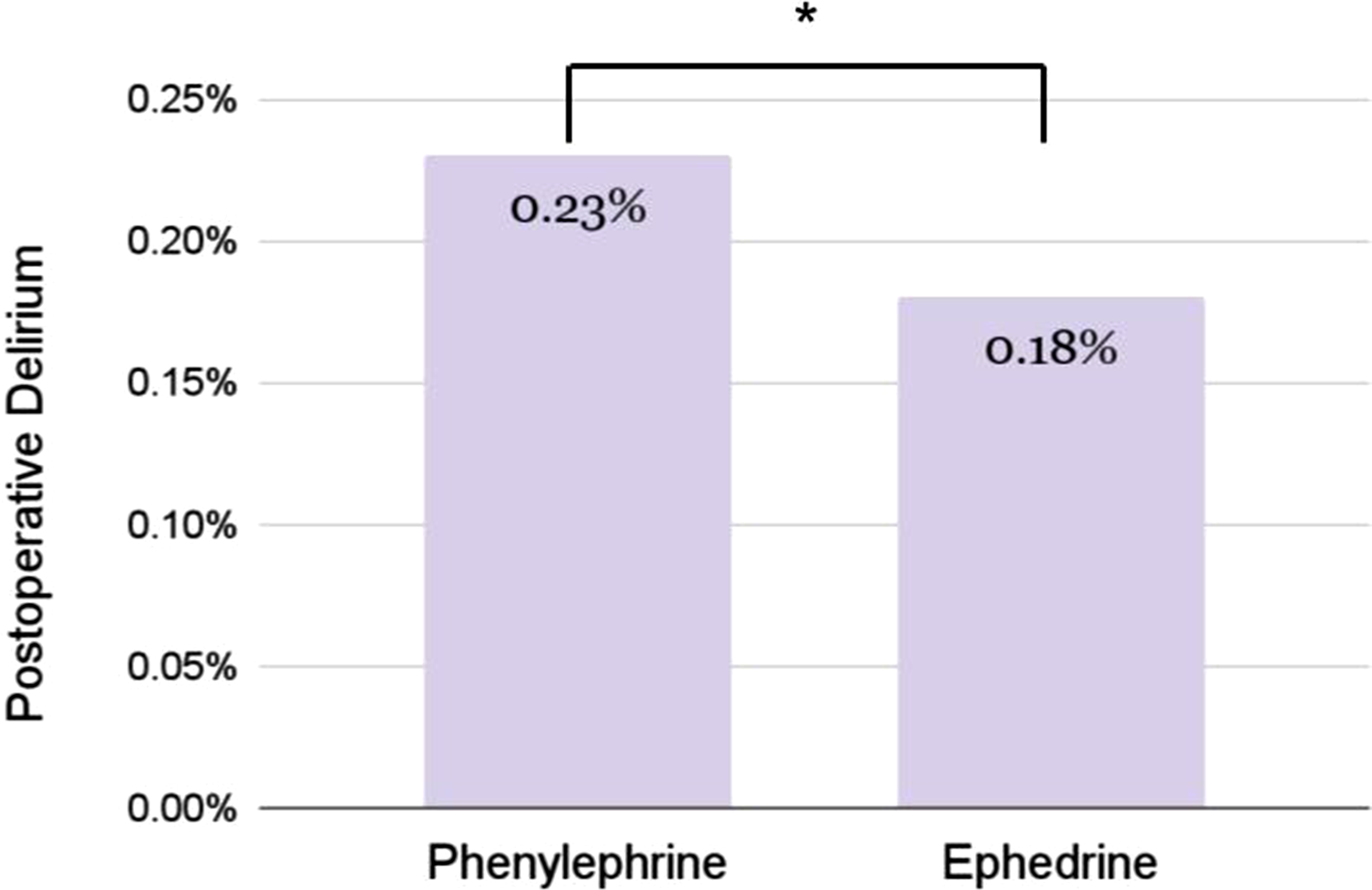
Phenylephrine Versus Norepinephrine
After matching, both cohorts were adjusted to 6058 patients each, with mean ages of 69.5 ± 9.2 and 69.5 ± 9.1, respectively. There was no significant difference in postoperative delirium between the phenylephrine (n = 36 [0.59%]) and norepinephrine (n = 37 [0.61%]) cohorts (RD -0.02% [-0.29%–0.26%]; OR 0.97 [0.61-1.54]; P = 0.9065; Figure 3). Seven-day incidence of postoperative delirium following intraoperative phenylephrine vs norepinephrine administration (P = .906)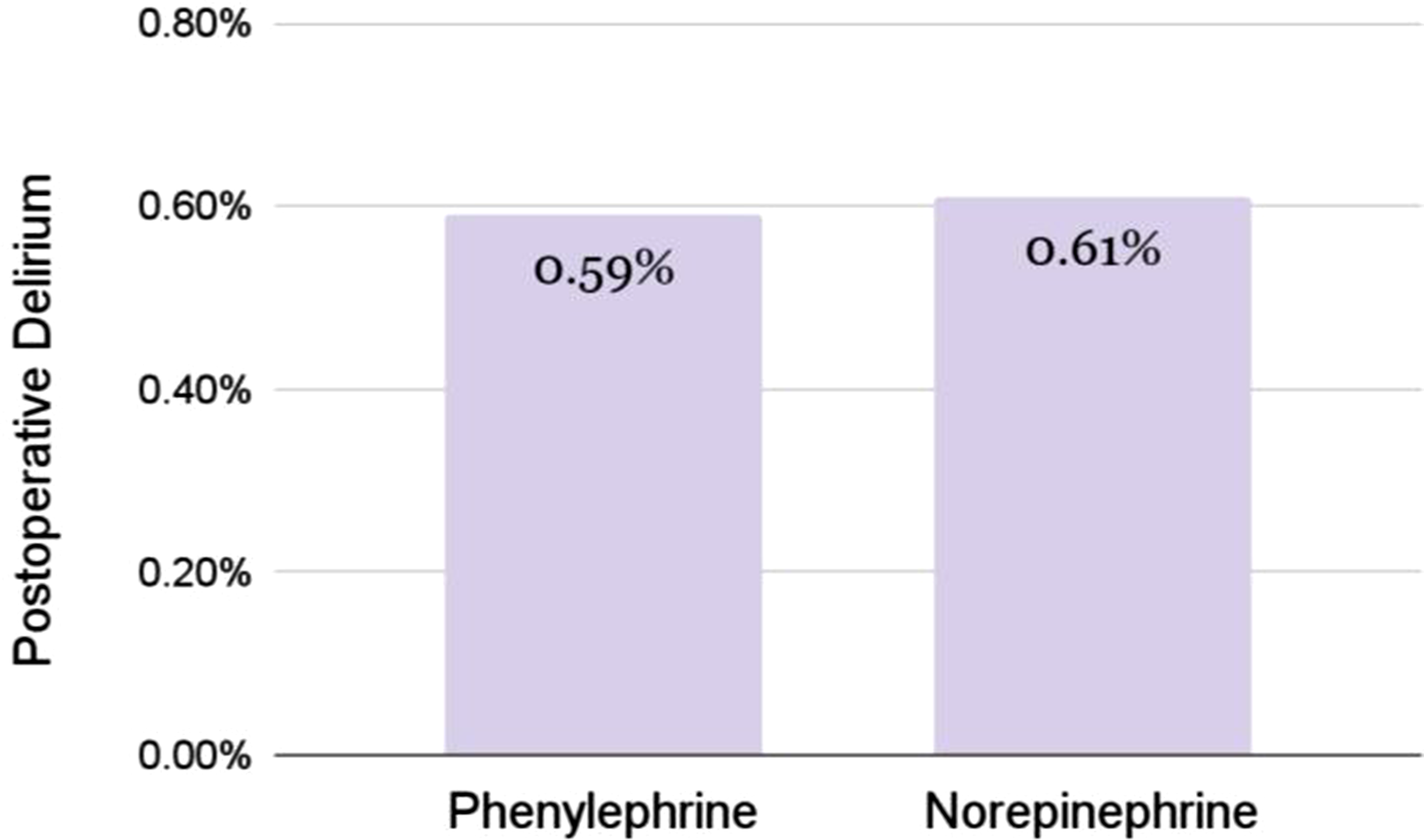
Ephedrine Versus Norepinephrine
After matching, both cohorts were adjusted to 5594 patients each, with mean ages of 69.6 ± 8.8 and 69.5 ± 9.1, respectively. There was no significant difference in postoperative delirium between the ephedrine (n = 20 [0.36%]) and norepinephrine (n = 27 [0.48%]) cohorts (RD -0.13% [-0.37%–0.12%]; OR 0.74 [0.41–1.32]; P = 0.3062; Figure 4). Seven-day incidence of postoperative delirium following intraoperative ephedrine vs norepinephrine administration (P = .3062)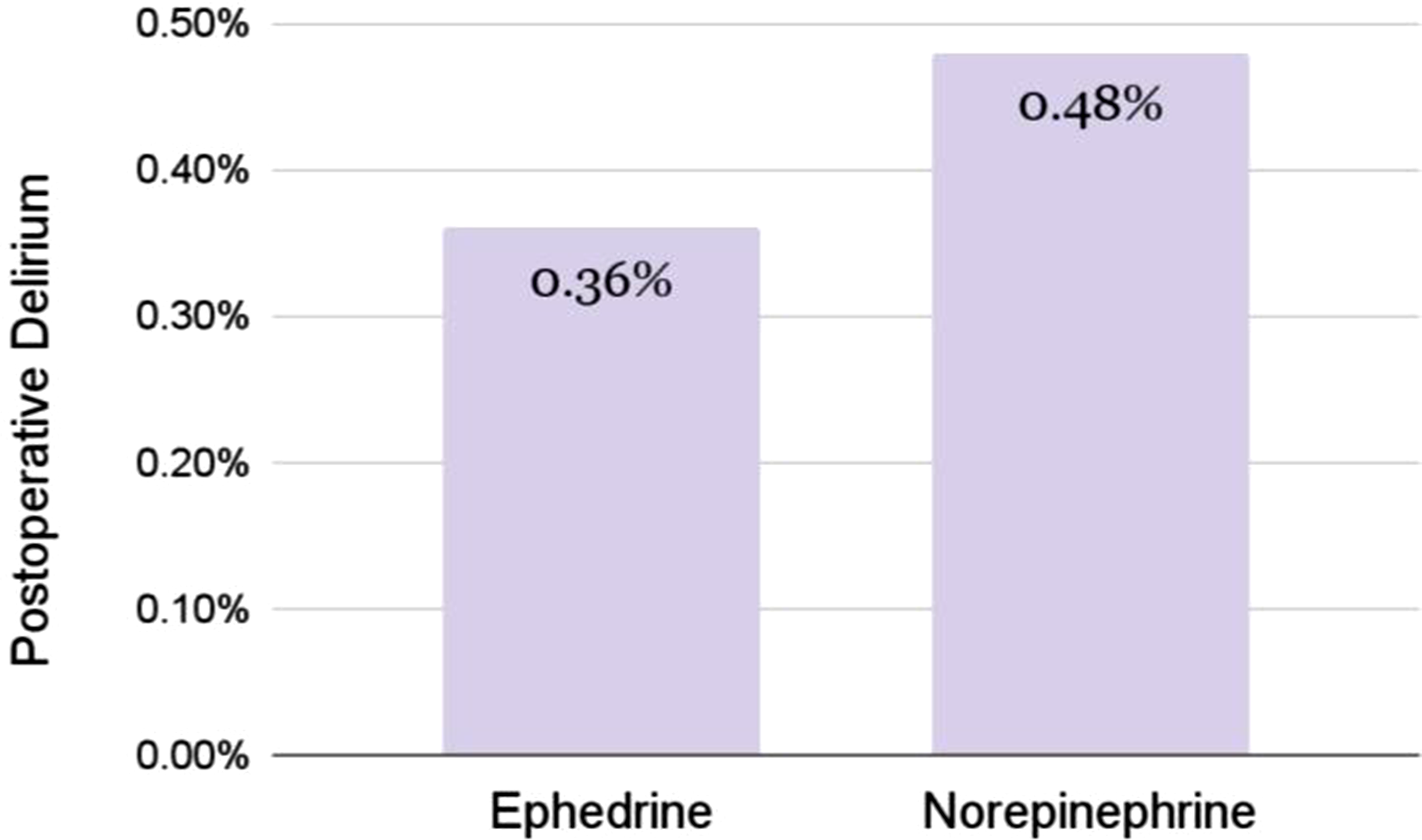
After Holm correction for three pairwise comparisons, the phenylephrine vs ephedrine association remained statistically significant (P = 0.0486), and the other comparisons remained non-significant.
Discussion
This multicenter retrospective database analysis provides an association between postoperative delirium and vasopressor selection (phenylephrine vs ephedrine vs norepinephrine) in a population of patients undergoing non-cardiac and non-neurosurgical procedures and receiving single vasopressor therapy. Key strengths include the large sample size and multi-center study design. When combined with propensity score matching and large sample size, the observed association is less likely to be influenced by confounding factors.
Our findings demonstrated significantly higher odds of developing postoperative delirium after phenylephrine administration compared with ephedrine. While the results are statistically significant, the incidence of postoperative delirium may not be clinically significant between these two cohorts, given the low absolute risk difference. This study estimates approximately 5 additional cases of postoperative delirium per 10,000 patients and an estimated number needed to harm of 2000. Therefore, the clinical relevance of this association may be insufficient to alter vasopressor selection in isolation. However, these findings support prior research, including a large multi-center retrospective cohort study by Ma et al which reported an odds ratio of 1.35 (95% CI: 1.06 to 1.71; P = 0.02) for phenylephrine compared to ephedrine with a postoperative delirium incidence of 0.9% (685 of 78,900) for patients receiving intraoperative phenylephrine as compared to 0.4% (85 of 24,112) for patients receiving intraoperative ephedrine. 6 A randomized controlled trial in 120 patients with total knee arthroplasty found a postoperative delirium incidence of 33% (20 of 60) on the first postoperative day in a group receiving continuous phenylephrine infusion vs 7% (4 of 60) in a group with continuous ephedrine infusion (P < 0.001). This study revealed a decreased rSO2 in the phenylephrine group (−8.4% ± 0.6%) with a milder decrease in rSO2 in the ephedrine group (−1.3% ± 0.6%) and a difference between the two cohorts of 7.2% (95% CI: 6.0 to 8.3; P < 0.001). 5
A potential explanation includes different mechanisms of action between these drugs. However, these mechanisms were not explicitly tested in this study and should therefore be interpreted as hypothesis-generating rather than definitive. Ephedrine exerts strong β1 and β2 effects, leading to increased cardiac output and therefore improved blood flow to the brain. Additionally, ephedrine causes a smaller increase in systemic vascular resistance due to its β2-mediated vasodilation, which may enhance cerebral perfusion and oxygenation. 9 Another potential mechanism involves ephedrine’s central action on VMAT2 reuptake receptors, which induces amphetamine-like central stimulation of dopamine and serotonin. 10 For example, ephedrine exposure within monkey models was shown to alter neurotransmitter levels in the hippocampus. 11 Administration of ephedrine thus indirectly releases stimulatory neurotransmitters and may improve cognition or awareness, thereby reducing the incidence of delirium. Despite the association between ephedrine and tachyphylaxis, ephedrine has recently been investigated as a slow infusion for delirium treatment, demonstrating a 26% absolute reduction in postoperative delirium rates on the first postoperative day, though no significant changes were observed over seven days. 5
When compared to ephedrine, phenylephrine is a pure α1-adrenergic receptor agonist. 12 The primary effects of phenylephrine are limited to peripheral vasoconstriction with minor increases in cardiac output or cerebral autoregulation. This potent vasoconstriction may reduce cerebral perfusion pressure and regional oxygen delivery, especially in vulnerable postoperative patients. Unlike ephedrine, phenylephrine lacks β2 receptor activity, causing greater increases in systemic vascular resistance and further contributing to decreased cerebral perfusion. Additionally, phenylephrine does not cross the blood-brain barrier and therefore lacks the central neuromodulatory effects seen with ephedrine, which may help stabilize neurotransmitter balance and counteract neuroinflammation. 12 As a result, phenylephrine is unlikely to stimulate dopamine and serotonin the way ephedrine does, potentially leading to reduced alertness.
Interestingly, norepinephrine did not exhibit any differences in postoperative delirium odds compared with phenylephrine or ephedrine. Since norepinephrine exhibits potent α1-adrenergic receptor activity with modest β1 and minimal β2 receptor activity, 13 it is likely to affect cerebral perfusion and postoperative delirium similarly to phenylephrine. However, its cardiostimulatory properties may help maintain cerebral perfusion more effectively than phenylephrine, though still to a lesser extent than ephedrine. Given that norepinephrine is typically administered to more hemodynamically unstable or critically ill patients,14-16 residual confounding by indication likely remains. Vasopressor selection is not random and often reflects the patient’s underlying physiology, severity of hemodynamic instability, and anesthetic management. Furthermore, norepinephrine is usually reserved for non-transient, continuous vasopressor support, and longer durations of intraoperative hypotension have been associated with increased delirium. 3 Consequently, the observed neutral association may underestimate a potentially protective effect of norepinephrine relative to phenylephrine with respect to postoperative delirium.
Given the association of postoperative delirium with increased mortality and complications rates in older patients, an understanding regarding the impact of vasopressor selection on postoperative cognitive function is essential. 17 Future studies are warranted to further assess the underlying mechanism by which vasopressors influence postoperative delirium. Prospective studies are also warranted to better assess the relationship between norepinephrine and postoperative delirium as retrospective analyses are likely confounded by underlying selection bias.
As with all retrospective studies, causality cannot be established. Electronic medical record data are subject to variations in billing codes and gaps in documentation which may affect the accuracy of the findings. Vasopressin, angiotensin II, and metaraminol were not considered in this analysis. Secondary outcomes, including downstream clinical consequences such as length of stay, discharge disposition, readmission, postoperative complications, and mortality, were not evaluated. Furthermore, due to the nature of TriNetX, vasopressor exposure was defined by medication administration codes and could not reliably account for dose, duration, timing, or mode of administration, such as bolus vs infusion. The authors also lacked access to the specific intraoperative clinical context surrounding vasopressor use, including hemodynamic instability, ASA physical status, and surgery duration. Vasopressor selection is often driven by intraoperative hemodynamic conditions or clinician preference, which may result in confounding by indication despite matching. For example, patients receiving norepinephrine may have had greater hemodynamic instability, contributing to reduced cerebral perfusion. Despite including somnolence and disorientation in our definition, the true incidence of postoperative delirium may have been underestimated due to under-documentation or transient episodes that resolve before being recorded. In contrast, inclusion of ICD-10 codes for somnolence and disorientation may have reduced the specificity of delirium ascertainment and introduced potential outcome misclassification. Additionally, the broad inclusion of surgical procedures likely captured many operations with a low baseline risk of postoperative delirium, which may have further contributed to the low observed incidence and should be considered when interpreting study power and generalizability. Although extensive cohort matching aimed to decrease confounders, propensity score matching was also limited to the variables available within the database.
Conclusion
In this large cohort of older adults undergoing non-cardiac, non-neurosurgical procedures, rates of postoperative delirium within seven days of surgery were found to be significantly lower with use of ephedrine compared to use of phenylephrine on day of surgery. Norepinephrine was not associated with increased risk of postoperative delirium when compared to either phenylephrine or ephedrine. These findings warrant further pharmacologic studies to individualize anesthetic choice, especially in the high-risk geriatric population.
Supplemental Material
Supplemental Material—Vasopressor Selection and Postoperative Delirium in Older Adults: A Propensity-Matched Database Analysis
Supplemental Material for Vasopressor Selection and Postoperative Delirium in Older Adults: A Propensity-Matched Database Analysis by Tiffany Dong, William Mao, Christopher Baker, Blake Han, Leonard J. Soloniuk, Gary Stier, Daniel A Novak, Ioana Pasca, Jiapeng Huang, in Seminars in Cardiothoracic and Vascular Anesthesia
Footnotes
Ethical Considerations
This study received a Determination of Non-Human Subjects Research (Protocol #30442) and was registered in ClinicalTrials.gov (NCT06844201).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.