
Abstract
Introduction:
Classical ballet is a high-performance artistic discipline that entails high physical and mental demands that increase the risk of health conditions linked to dance. Medication is of interest to athletes due to its therapeutic role in the management of pain, injuries and medical conditions and their ergogenic effects in elite sports. However, their use in dance-related pathologies, injuries, or their performance effects is currently unknown.
Objective:
To compile the medications used by ballet dancers, study their perceived effects on performance and health conditions, and to find out if they are used by self-medicating or under the supervision of a health professional.
Methods:
125 ballet dancers aged between 18 and 35 years within the Spanish scope completed an online survey about their workload, health issues and medication use, whether self-medicated or under medical supervision, and dancers’ perception on the effects of medication on their health and performance. The collected data were analysed to obtain prevalence measurements and their 95% confidence intervals.
Results:
84.69% (95% CI: 77.57-91.82) of participants reported the intake of at least one medication. The most prevalent therapeutic medications used are NSAID 67.59% (95% CI: 58.06-76.63) and paracetamol 48.98% (95% CI: 39.08-58.88), while caffeine is the most used for ergogenic purposes 17.35% (95% CI: 9.85-24.84).
Conclusions:
It was found that there is a high prevalence of medication use for therapeutic purposes in ballet dance, especially analgesics and anti-inflammatories. On many occasions, dancers begin using medications on their own initiative or based on recommendations from fellow dancers or dance masters rather than medical professionals.
Key Points
Medicine use prevalence reported that almost 85% of surveyed dancers use at least one medication and nearly half of them use two or more.
The most taken medications are over-the-counter analgesic and anti-inflammatory drugs, NSAID and paracetamol.
While medication plays a significant role in a dancer’s day-to-day life, research on the use of pharmacotherapy among dancers is an understudied topic.
Introduction
Classical ballet is a performing art where movement expresses emotions or interpret a narrative from the established bases of classical ballet technique which fundamental features are body alignment and codified movements that describe how to move according to ballet’s aesthetics. 1 Ballet is classified as a high-intensity intermittent physical exercise, 2 that requires complex movements, a wide range of joint mobility, coordination and balance associated with efficient strength and flexibility. 3
To understand the most frequent pathologies and injuries in dance, it is important to examine the demands of pre-professional and professional ballet dancers. A distinction can be made between periods of training and rehearsals and periods of stage performances, usually more demanding with a greater load of active hours. A dancer’s day usually begins with an average of 90 minutes of dance class to prepare the body to spend the rest of the day in rehearsal. 4
Despite long periods of rehearsals, over 90% of professional dancers report less than 60 consecutive minutes of rest, with one third of dancers reporting having less than 20 minutes. 4 Lower resting time, compared to their workload, can be an indicator of a higher risk of fatigue pathologies and injuries, and the additional concern about the intake of enough nutrients, in less than an hour, to meet both the energy demands and macro- and micronutrient requirements of the dancers. 4
Historically, ballet dancers were perceived solely as artists but due to the comparable physical demands to high performance sports they are currently also considered as elite athletes. 5 However, dancers still don’t have the support from specialised organizations, such us the International Olympic Committee (IOC) or the National Collegiate Athletic Association (NCAA).
Given this background it is hypothesised that the most prevalent pathologies expected in ballet dancers are musculoskeletal injuries due to high physical demands and mental health disorders (eg) anxiety, depression, and eating disorders.
Ballet has been categorized as a high-risk activity due to the discipline demands. High rates of injury have been observed in epidemiological studies comparable to other athletic populations but higher overall risk was noted in ballet dancers due to a more intense training load exposure.6 -8
– A 70.3% prevalence of time-loss injuries has been observed in female professional dancers, 61.4% in male professionals and 32.1% in pre-professional dancers.9,10
– The prevalence of medical attention injuries, those that resulted in a dancer seeking care from a medical practitioner, reported in professionals is 91.5% for women, 88.4% for men and 67.4% in pre-professionals.9,10
– A 67.4% prevalence has been observed in pre-professional dancers for all-complaint injuries.10,11
Overuse injuries are predominant among professional dancers, accounting for 60% to 68% of all injuries, being statistically grater in incidence and severity than traumatic injuries.6,9,12
Similar to aesthetic sports, dancers are often judged based on their performance, but also on their appearance. Therefore, they feel pressured to adhere to an ideal body image. 13 Along with other stressors (normalization of injuries, professional uncertainty, training load) can negatively impact their mental health. 13 High-performance disciplines in which body shape plays a significant role (such as gymnastics, dance, skating, swimming), require higher levels of perfectionism, self-discipline and supervision of nutrition that can contribute to dysfunctional eating behaviors. 14 It was found that, one in five dancers (20.8%) experience symptoms of depression, generalized anxiety or eating disorders related to musculoskeletal pain and chronic symptoms of low mood, which is significantly more prevalent than in the general population. 13
Eating disorders are common in athletes who consume performance and image-enhancing substances, including anabolic-androgenic steroids, amphetamine derivatives and other central stimulants such as caffeine and ephedrine. 15
The Role of Medication in Dance
The physical and mental demands of classical ballet, especially at pre-professional and professional levels, are associated with a higher incidence of health problems.7,16 Dance culture – similar to high-performance sports – continuously demands dancers to be at the top of capabilities, 15 training by overcoming signs of fatigue or overload and normalizing pain in daily practice.16,17 This environment can lead dancers to use medication in their daily practice to alleviate symptoms, enhance performance and meet expectations.
Pharmacotherapeutic treatment of pain
Dancers, like elite athletes, are likely to experience and treat pain differently than the general population, being more likely to use and receive analgesics. 18 Different types of medications are used by athletes to prevent or treat pain, in different forms of administration, including over-the counter analgesics, such as paracetamol and some non-steroidal anti-inflammatory drugs (NSAID), and prescription-only medications such as glucocorticoids, opioids, muscle relaxants, anti-depressants, and anxiolytics.18,19
NSAID and paracetamol are a broad class of drugs with analgesic, anti-inflammatory and antipyretic effects, while paracetamol has excellent analgesic activity with minimal anti-inflammatory effects. 20 NSAID are effective against mild to moderate pain, particularly associated with inflammation or tissue damage. 20 They are the most commonly used drugs among elite athletes, some studies reporting a prevalence higher than 50%.18,19,21 Reasons athletes provide for using analgesics include treatment of sports-related pain and injury, managing associated symptoms, treating illness, enhancing performance and preventing or blocking pain to enable participation in sports. 21
Concerns arise due to the simultaneous use of multiple NSAID by different routes, higher doses, use for pain prophylaxis and chronic use, often unsupervised by medical professionals.18,21 In addition to their adverse effects and the limited evidence in relation to the effects on injury treatment. 18 Although NSAID reduce the signs and symptoms of inflammation, they may have little impact on the actual course of the disease, masking underlying conditions and increasing diagnosis and recovery times.20,21
Glucocorticoids are potent anti-inflammatory drugs which also have inhibitory effects on the immune response. 20 Corticosteroid use among athletes remains unclear, but they tend to be much lower than NSAID. 18 Injectable corticosteroids are administered to help injured athletes speed up return to activity, especially on competition days. 22 Potential side effects in soft tissue changes may occur in the long term, including tendon or ligament weakening and rupture and cartilage and bone degeneration, with numerous reports of tendon rupture after corticosteroid injections.23,24 Although their safety and efficacy in athletes remains limited as glucocorticoid use is generally restricted or prohibited in sports subject to drug testing. 25
Opioids are potent analgesics that reduce the transmission of nociceptive impulses by diminishing neuronal excitability and neurotransmitter release. 26 Opioids reported use rates below 1% to 13% of athletes from different disciplines.18,19 They may be considered and reserved for the management of severe acute pain when other strategies are insufficient (eg, post-operative pain, initial fracture pain). 27 They are associated with risk of addiction and cognitive disturbances even on a short term and later in life in former athletes, highlighting the importance of cautiously monitoring prescribing and monitoring.19,27
Muscle relaxants are medications not classified as analgesics or anti-inflammatories but relevant in the relief of musculoskeletal disorders. These include central acting muscle relaxants such as cyclobenzaprine and methocarbamol. They reduce pain associated with muscle contractures and spasms and improve mobility associated with acute painful musculoskeletal conditions.28,29 The most frequent adverse effects that could impair sports performance are drowsiness and dizziness.28,29 Certain benzodiazepines have also approved muscle-relaxant indications, which will be discussed in the next section.
Pharmacotherapy for mental health disorders
Although psychotherapy is the first-line treatment for mild to moderate mental health disorders, pharmacological support may be necessary in certain cases. 15 In dancers and athletes, it is essential to consider prior to prescription possible effects on performance (negative or enhancing), performance enhancement by alleviating the condition that the drug is intended to treat and the general side effects. 15
The main options for the pharmacological treatment of mental disorders in athletes are selective serotonin reuptake inhibitors (SSRIs), in particular, fluoxetine which has no demonstrated negative impact on performance, as well as escitalopram and sertraline; 15 and other antidepressants like bupropion for depressive disorders. Other medications such as lisdexamfetamine may be useful for binge eating disorders. Benzodiazepines are not usually recommended because they may decrease performance. 15
Selective serotonin reuptake inhibitors (SSRIs) are drugs used for both depression and anxiety. In eating disorders, pharmacological treatment is indicated in patients who are already receiving nutritional counselling and psychotherapy, in addition to antidepressants, orexigenic drugs such as pizotifen are also used in this pathology, with an appetite-stimulating effect. 28
Benzodiazepines treat symptoms of anxiety disorders faster acting than antidepressants, mediating the inhibitory synaptic transmission in the CNS 30 leading to a fast anxiety effect, induction of sleep, reduction of muscle tone, anticonvulsant effects and anterograde amnesia. 30 Their main side effects that can decrease physical performance are drowsiness, confusion, amnesia, and impaired coordination.15,30 An important inconvenience of benzodiazepines is their risk of dependence, with sometimes compulsive use, and withdrawal syndrome in the absence of a gradual tapering protocol. 30
Drugs used for ergogenic purposes
Drugs used for non-therapeutic purposes, but rather aesthetic, body composition, social purposes or to improve athletic capabilities, are taken voluntarily to achieve an aspiration unrelated to the treatment for a disease. 31 Commonly-consumed substances among athletes include alcohol, caffeine, nicotine, cannabis, stimulants and anabolic-androgenic steroids.15,32 This paper focuses on non-recreational drugs with approved therapeutic indications, but potentially used for other purposes: stimulants and anabolic-androgenic steroids. Some substances, including stimulants, anabolic agents and glucocorticoids, are included on the World Anti-Doping Agency (WADA) Prohibited List for competitive sport contexts; 25 however, these regulatory frameworks do not extend to dance. This may contribute to maladaptive use aimed at achieving functional or aesthetic effects in the absence of regulatory oversight. 33
Some of the most commonly used stimulant drugs in sports are amphetamines, caffeine, ephedrine, pseudoephedrine and phenylephrine. 34
Amphetamines and related compounds (lisdexamfetamine and methylphenidate) are psychomotor stimulants clinically used to treat attention deficit/hyperactivity disorder. 35 They increase the extracellular concentration of dopamine and norepinephrine in nerve terminals. 35 They are consumed in elite sports for their main central effects: locomotor stimulation, euphoria and excitement, greater resistance to fatigue and increased ability to mentally prepare for events.15,31,35
Ephedrine is a sympathomimetic amine with an indirect action; it has central effects similar to amphetamines but with weaker action. 36 Some trials have shown that ephedrine can improve performance in activities, such as sprint races, and in experimental conditions increase muscle power and significantly reduce muscle fatigue. 31 There have been cases of athlete deaths who had consumed amphetamines and ephedrine-like drugs in endurance competitions because of their serious adverse reactions: coronary insufficiency associated with hypertension, hyperthermia associated with cutaneous vasoconstriction, and dehydration. 31
Caffeine is a widely used stimulant for ergogenic purposes, for its mild excitatory effects, enhancing neural activity across multiple brain regions.28,35 In addition, it stimulates heart rate and increases cardiac output. 28 Caffeine appears to be more effective in improving muscle performance than other potent stimulants. 31 Although high doses may increase the likelihood of adverse effects such as anxiety, insomnia, gastric irritation, tachycardia and tremors. 15
Anabolic-androgenic steroids (AAS) include testosterone and synthetic derivatives analogues (mesterolone, methenolone, prasterone). 34 When administered in combination with training and a protein-rich diet, they reduce body fat, increase muscle mass and strength, as well as having anti-catabolic effects.15,31 AAS can induce feelings of well-being, increase competitiveness and aggressiveness, which sometimes can evolve into psychosis. 31 They can have potential performance-diminishing effects such as cognitive impairment, negative mood symptoms and injuries such as tendon tears or ruptures. 15 A meta-analysis reported a lifetime use of 6.4% for males and 1.6% for females, being highest among recreational and competitive athletes, the odds of use increasing by 91% with participation in at least one sport.34,37 Additionally, some athletes who use anabolic-androgenic steroids develop body dysmorphia, a disorder that involves high concern that their body is not lean and muscular enough, often with significant body image distortion. 15 Although systematic data in dancers is limited, use of AAS is most commonly reported in strength, power and physique-oriented sports. 37 Added to the pressures related to body composition and appearance described in other aesthetic sports, suggests a potential area of concern in performance disciplines that prioritize specific body ideals. 15
As described above, there is a clear need to expand research in dance medicine, both in daily practice and during pathologies and injuries, to develop preventive strategies adapted to dancers’ demands. Given the uniqueness of the practice compared to other elite sports and the limited evidence available, dancers may feel insufficiently supported by healthcare professionals and resort to self-medicate to manage their pathologies or enhance performance, often using advice that is passed between fellow dancers.17,32 Establishing a line of research in the use of medication in dance could be a significant step towards improving dancer’s health and developing health interventions on its safe and effective use.
Objectives
– To perform a pharmacological compilation of the medications used by ballet dancers;
– To study the perceived effects of these medications on dancers’ performance and treatment and symptom relief of health conditions; and
– To find out whether dancers self-medicate or use these medications under the supervision of a health professional.
Material and Methods
To obtain information aligned with the objectives, an observational, descriptive, cross-sectional study was carried out. Data were collected through an anonymous and self-completed online survey of closed-ended questions and an optional open field, the survey was addressed to dancers within the Spanish national scope in dance companies, professional schools, dance conservatories and through physiotherapists specialized in dance informing about the confidentiality of the data. The questionnaire consisted of two sections (Supplementary Material):
Dance level, workload in ballet dance and other physical activities, presence or absence of injuries or pathologies.
Medications used, dancers’ perceptions on their injuries, pathologies and performance, and reason to start using them.
The inclusion criteria were dancers 15 to 35 years old. 15 years old as the minimum age to study the last cycle of the professional dance conservatory; 1-year experience on ballet at least; and practice at least 4 hours of ballet and/or neoclassical dance per week, regardless of the practice of other disciplines within dance.
Exclusion criteria being the practice of another type of dance or physical activity and ballet occupying less than 60% of the hours practiced.
Statistical Analysis
Data obtained were extracted to perform descriptive statistics to calculate the prevalence as the proportion of dancers reporting any injury, health condition, or medication use out of the total sample or, when relevant, stratified by subgroup: dance level (professional, pre-professional, amateur) or presence of pathology or injury. It is expressed as a percentage accompanied by its 95% confidence interval.
In addition, dancer’s responses regarding each medication were also analysed as the number and percentage of dancers who indicated how these influenced performance and treatment of injuries and pathologies (essential, timely support, no effect or worsen), form of administration they were administered (oral, topical or parenteral) and the reason for started taking each medication (prescribed by a physician, indicated by a pharmacist, recommended by a physiotherapist or by a non-medical professional)
Results
Demographic Characteristics
A total of 125 responses were collected, of which 27 were excluded for not meeting the inclusion criteria (aged over 35 years old or engaging in less than 4 hours of ballet per week and more than 15 hours of other dance styles or physical activity). Final sample size consists of n = 98 participants, with a mean age of 23 years old (SD = 4.61), among them, 70.41% have over 10 years of dance experience (Table 1).
Demographic Statistics (Dance Level, Age, Years Dedicated to Dance and Weekly Dancing Hours).
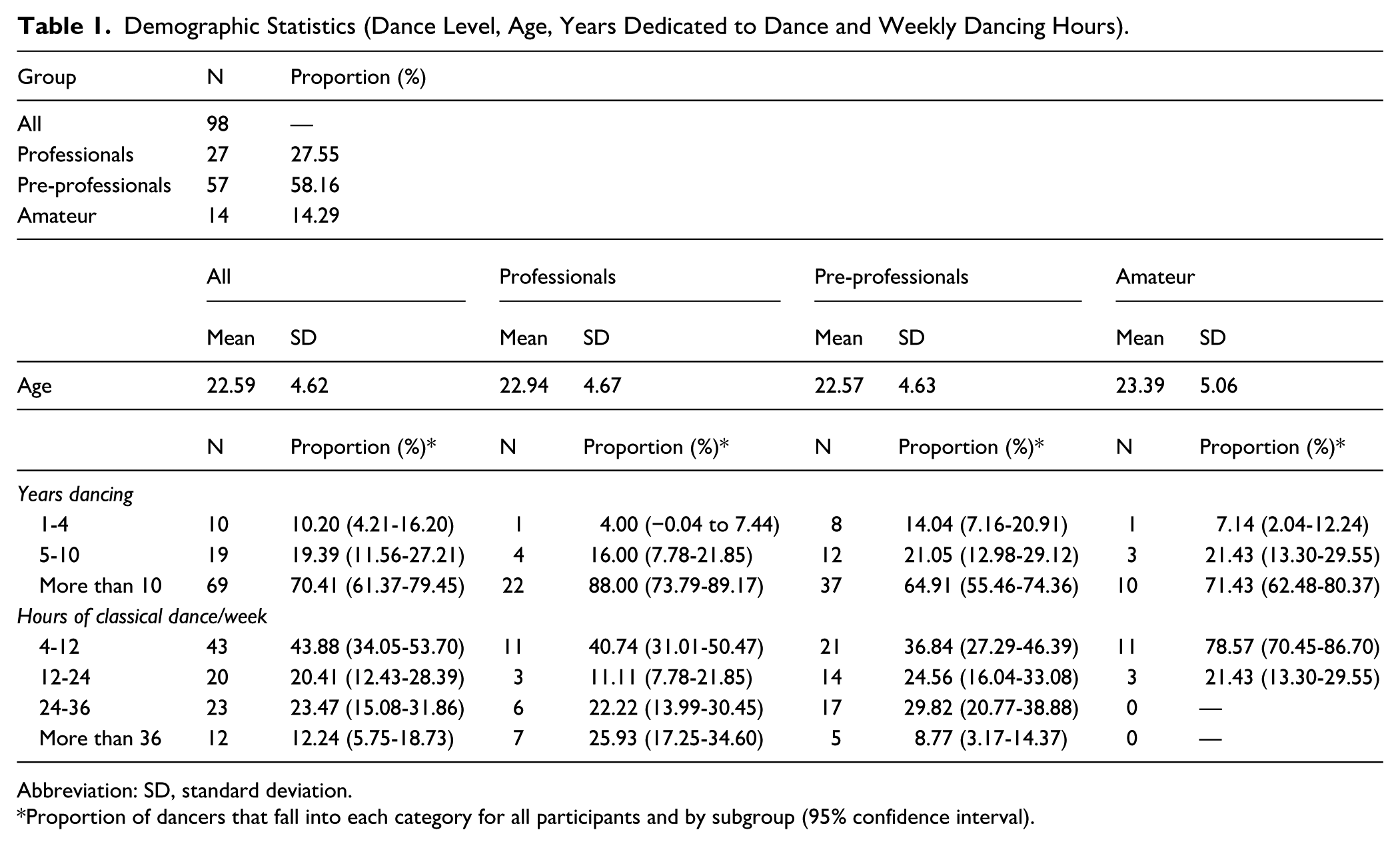
Abbreviation: SD, standard deviation.
Proportion of dancers that fall into each category for all participants and by subgroup (95% confidence interval).
Participants were categorized into the following subgroups according to their level of dedication to ballet:
– Professionals (n = 25; 27.55%): dancers with a contract at a dance company.
– Pre-professionals (n = 57; 58.16%): dancers enrolled in conservatories, professional training programs or preparing to audition.
– Amateurs (n = 14; 14.28%): dancers not pursuing a professional career.
– 2 dance teachers: due to their similarity to how long they have dedicated to dance and workload, their data was analysed within the category of professionals.
Prevalence of Health Conditions
In total, 64.29% (95% CI: 54.80-73.77) suffered some acute, chronic injury or both, with chronic injuries being the most frequent across all groups (52.04%). Regarding mental health conditions: anxiety disorders, depression and eating disorders, 59.18% (95% CI: 49.45-68.91) of respondents answered having at least one. The individual prevalences were 45.92% for anxiety disorders, 13.27% for depression and 21.43% for eating disorders (Table 2).
Prevalence of Injuries and Mental Health Conditions (95% Confidence Interval).
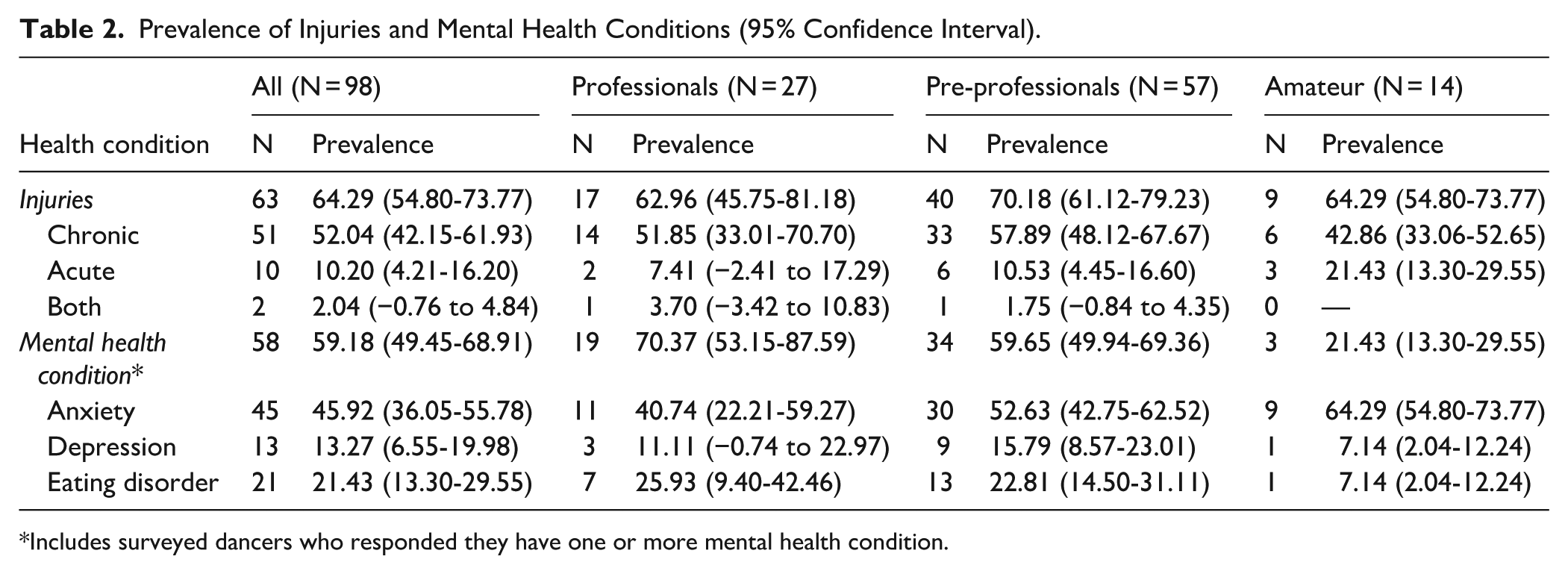
Includes surveyed dancers who responded they have one or more mental health condition.
Prevalence of Medication Use
84.69% (95% CI: 77.57-91.82) of dancers reported using at least one medication while 48.98% (95% CI: 39.08-58.88) used two or more medications. Medication use by therapeutic group is detailed in the Supplemental Table 1 and presented in Figure 1. It is also detailed their influence on performance and effects on treatment of injuries and mental health disorders (Figure 2) and the reason to start using each medication (Figure 3).
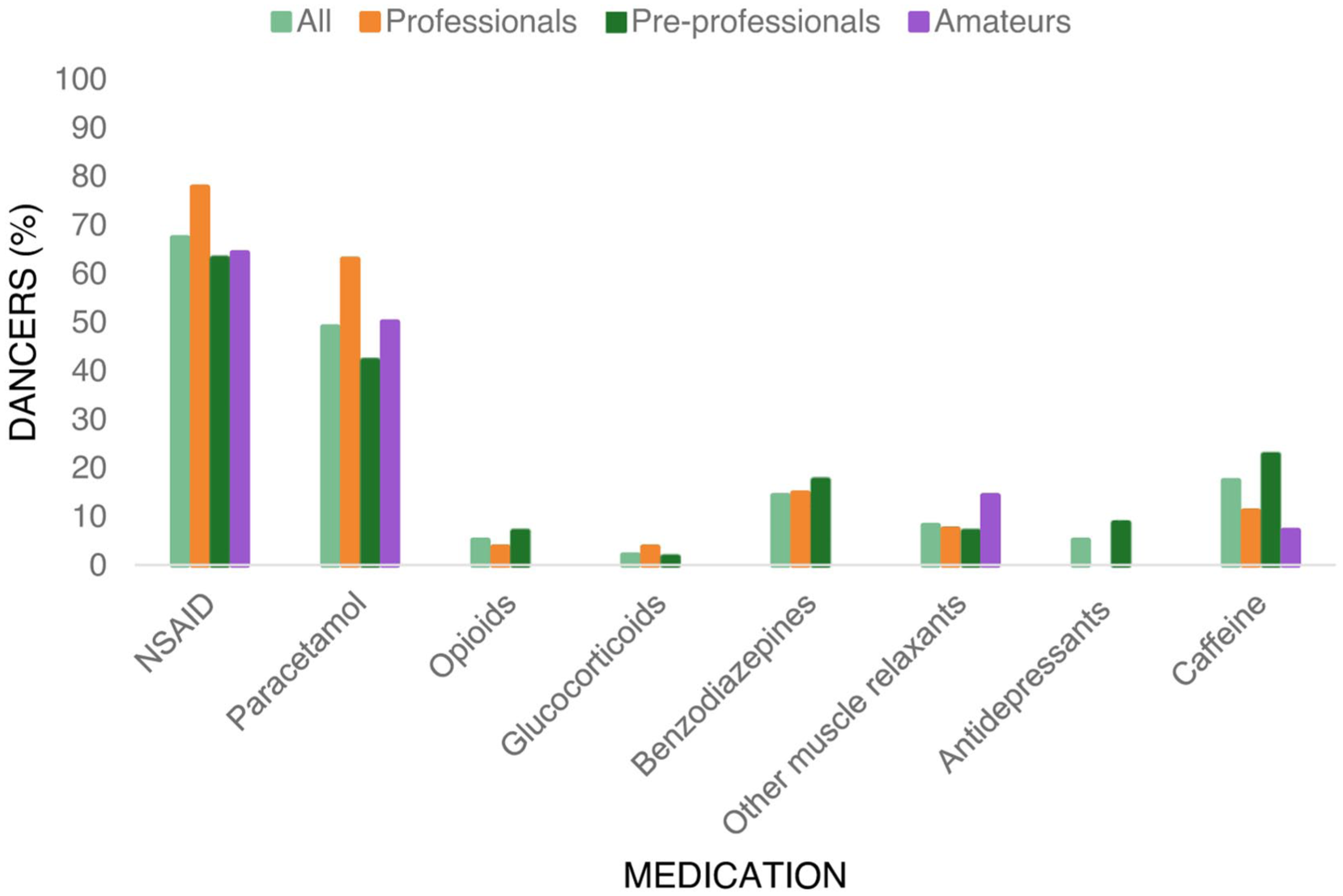
Prevalence of medication use by therapeutic group and dance level.
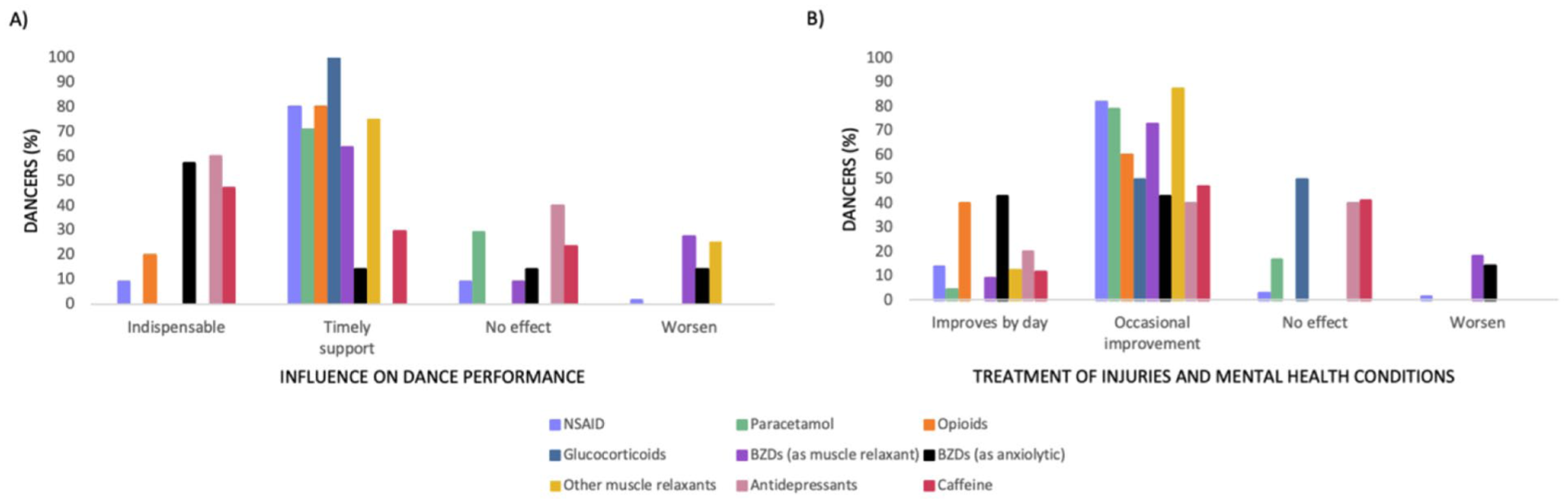
Medication effects on performance and treatment of injuries and mental health conditions by therapeutic group. Percentage of dancers, taking each medication, who feel whether the medication is indispensable, a timely support, does not influence or worsen their (a) dance performance or (b) treatment or symptom relief of injuries and mental health conditions.
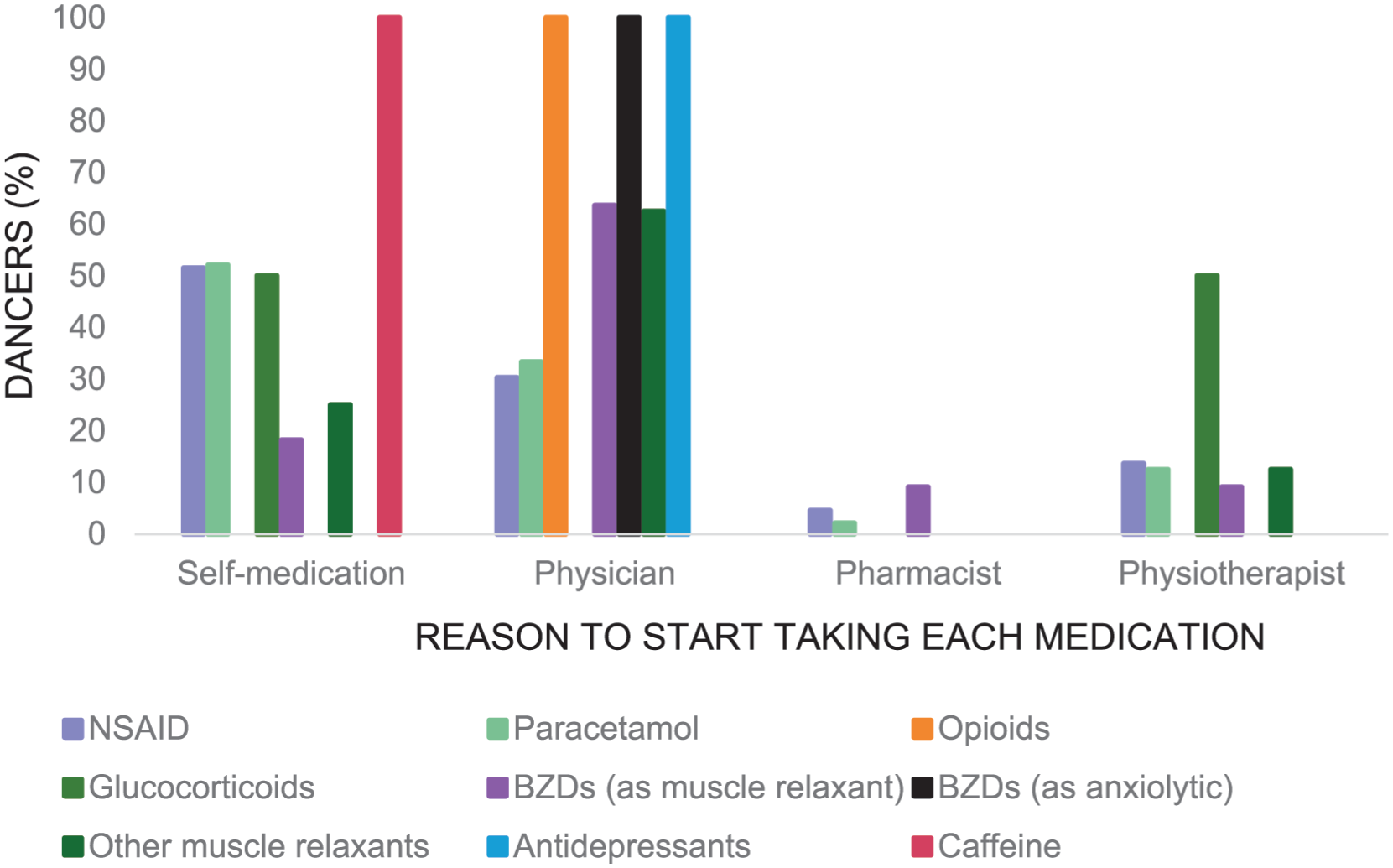
Reasons why dancers started using medication by therapeutic group. Percentage of dancers who started using each medication by personal experience or recommendation of a peer/teacher, prescribed by a physician, indicated by a pharmacist or recommended by a physiotherapist.
NSAID
In total, 67.59% of respondents reported they used some type of NSAID, with the highest prevalence among professional dancers (77.78%), followed by amateurs (64.29%) and pre-professionals (63.16%). Notably, 65.15% of NSAID users reported having some type of injury, indicating that NSAID consumption largely aligns with injury status and perceived necessity for performance.
The most common route of administration was oral (50.0%), followed by the combination of oral and topical NSAID (46.97%), and the minority (3.03%) applied NSAID topically. This distribution is consistent across professional and amateur subgroups, but it is reversed in the pre-professionals subgroup, where the combination of oral and topical NSAID was more frequent (58.33%). The concurrent use of multiple routes of administration (oral and topical) in near half of the respondents, raises additional concerns regarding potential risk of exceeding recommended dose limits. 18
Of the 66 dancers who used NSAID, 9.09% stated that they were essential in their day-to-day for performance – most of them being pre-professional dancers. However, 80.30% viewed NSAID as occasional support, 9.09% reported no influence, and 1.52% reported they worsened their performance. While most dancers described NSAID as occasional support, reliance on NSAID for routine performance may reflect inadequate recovery, pressure to train or perform while injured, or normalization of pain suppression. 18
Perceived improvement of injuries, pathologies and symptom relief followed the same pattern as performance; this makes sense since injuries or pathologies are often a limiting factor. The most frequent answer at all levels was that these medications represent an occasional improvement in 81.82% of dancers, followed by daily improvement in 13.64%, 3.03% feel that it did not influence their pathologies or injuries and 1.52% feel they worsened.
The main reason to start NSAID administration in all groups was their own experience or recommendation from peers or teachers (51.52%), followed by medical prescription (30.30%), physiotherapist recommendations (13.64%) and lastly, pharmaceutical indication (4.55%).
Paracetamol
48.98% of surveyed took oral paracetamol as an analgesic; 64.58% of them suffer from an injury. It was used in the highest percentage among professional dancers (62.96%), followed by amateurs (50.0%) and pre-professionals (42.11%).
No participants reported a worsening of performance or their pathologies and injuries due to paracetamol. Similar to NSAID, in all the subgroups it resulted in occasional support in performance (70.83%) and in the treatment and symptoms relief associated to injuries or pathologies (79.17%). To a lesser extent, it was reported that it did not influence performance (29.17%) or the treatment and symptom relief (16.67%) and, finally, 4.17% of the dancers, all pre-professionals, considered paracetamol essential for the treatment and symptom relief of their injuries and pathologies.
The main reason for starting to use paracetamol was self-medication based on one’s experience or peer/teacher recommendation (52.08%), followed by a medical prescription (33.33%), physiotherapist recommendation (12.50%), and pharmacist indication (2.08%).
Opioids
Five of the respondents (5.10%) used oral opioids by medical prescription and all associated with the presence of a chronic or acute injury, one of them was a professional dancer and four were pre-professionals. Opioids were perceived as an occasional help in performance in 80.0% of cases and essential in 20.0% of them, and resulted in occasional improvement of symptoms in 60.0% of cases and a daily improvement in 40.0%.
Glucocorticoids
Two dancers (2.04%) reported the use of glucocorticoids. A professional dancer received injectable glucocorticoids on the recommendation of a physiotherapist, despite not reporting currently any injuries. Another pre-professional dancer with a chronic injury took glucocorticoids orally based on personal experience or peer/teacher recommendation. As these medications require a medical prescription, these findings may suggest access outside formal medical channels and raise concerns regarding the risks associated with unsupervised glucocorticoid use (eg, musculoskeletal tissue damage, hypothalamic-pituitary-adrenal axis suppression).24,26
Benzodiazepines and other centrally acting muscle relaxants
Benzodiazepines were used by 14.29% of the respondents, 14.81% of professionals and 17.54% of pre-professionals by subgroups. Among users, 50.0% took them as muscle relaxants, 21.43% as anxiolytics and 28.57% for both purposes. Among dancers who used benzodiazepines, all suffered from some chronic or acute injury and/or anxiety.
For anxiolytic purposes, 57.14% considered them essential for performance while dancing, while 14.29% felt they were a timely support in performance and same prevalence applied to dancers who said they had no effect (14.29%) or worsen performance (14.29%). Regarding improvement of their pathologies and symptoms, 42.86% reported benzodiazepines as essential, 42.86% an occasional improvement was experienced and, finally, 14.29% noticed benzodiazepines worsen their condition. In this group, all began treatment by medical prescription.
Most dancers who used benzodiazepines as muscle relaxants found them an occasional help in performance (63.64%) and for the improvement of their pathologies and injuries (72.73%). In addition, 63.64% started taking them by medical prescription, 18.18% by their own experience or peer/teacher recommendation, 9.09% by pharmacist indication, and 9.09% by physiotherapist recommendation.
Other centrally acting muscle relaxants (eg, cyclobenzaprine, methocarbamol) were used by 8.16% of all respondents, half of whom had acute or chronic injuries. Most reported muscle relaxants as an occasional help in performance (75.0%) and for the relief of injuries (87.50%) and 25.0% noted a negative impact on performance. In addition, 62.50% began using them by medical prescription, 25.0% on their own experience or recommendation, and 12.50% by physiotherapist recommendation.
Antidepressants
Five respondents (5.10%) used antidepressants by medical prescription, and all suffered from some mental health disorder. All pre-professionals aged 16 to 21 years and four reported they suffered from eating disorders, anxiety and depression concomitantly.
For 60.0% of them, antidepressants were essential for their daily performance while 40% reported no effect on performance. 40.0% felt antidepressants occasionally improve their condition, 40.0% felt no effect, and another 20% experienced day-to-day improvement.
Stimulants
In total, 17.37% of respondents took caffeine in the medication form (oral tablets) as a stimulant, either from personal experience or peer/teacher recommendation. Prevalence was highest between pre-professional (22.81%) compared to 11.11% in professionals and 7.14% in amateurs.
For 47.06%, caffeine was considered essential in their daily performance, 29.41% a timely support, and 23.53% reported no influence in performance. Regarding symptom relief of their pathologies or injuries, 11.76% considered that caffeine contributed to daily improvement but for most it was an occasional improvement (47.06%) or did not influence (41.18%).
No respondents reported the use of ephedrine or amphetamine derivatives.
Anabolic-androgenic steroids
None of the dancers participating in the survey reported using AAS.
Discussion
To the best of our knowledge, this is the first study that addressed prevalence of pharmacological drug use among ballet dancers. Medication use is widespread among dancers, with pain relief medications, particularly NSAID and paracetamol, being the most prevalent, followed by caffeine tablets or capsules and benzodiazepines. Caffeine use was assessed only when consumed as a medication, and intake though other common sources such as coffee, energy drinks or dietary supplements was not captured. Consequently, the prevalence of caffeine use among dancers is likely considerably higher.
Professional dancers (n = 27) primarily use analgesic and anti-inflammatories, while medications for mental health disorders, benzodiazepines and antidepressants, are more prevalent among pre-professionals (n = 57).
Overall prevalence for injuries and mental health conditions align with the current evidence in professional dancers, except being higher in pre-professional dancers in our findings.6,9,10 Regarding mental health conditions (anxiety, depression and eating disorders), prevalence of having at least one condition is greater with 59.18%,13,38 often observed concomitantly in a young population aged 16 to 25. In most cases, medication use is linked to the existence of injuries or health conditions, indicating a primarily therapeutic purpose. Caffeine being the only medication predominantly used for ergogenic purposes.
The prevalence of NSAID and paracetamol use in this cohort is consistent with the reported in athletic populations, with systematic reviews indicating prevalences over 50%.18,19 The use of analgesics and anti-inflammatories seems to be highly linked to musculoskeletal injury, as around 65% of dancers who used these medications reported having at least one injury. Other reasons for use could be pain management in the absence of injury, such as muscle soreness or cramps or other discomfort as well as blocking or preventing pain during physical performance, a non-recommended practice, seen in other athlete populations. 19
Given the high prevalence of mental health disorders, benzodiazepine use was more common than antidepressants (14% vs. 5%), all dancers on these medications reported experiencing from anxiety, depression or an eating disorder. International guidelines for the management of mental health disorders in athletes, such as those from the International Olympic Committee (IOC), recommend antidepressants, specifically SSRIs, as first-line treatments for anxiety, depression and certain eating disorders, while benzodiazepines are generally discouraged for their negative cognitive and performance effects. 15 This discrepancy could suggest a suboptimal pharmacological management of mental health conditions in this population.
Notably, more than half of the dancers started using prescription or over-the-counter medications based on personal experience or peer/teacher recommendation, without consulting a healthcare professional such as a physician or a pharmacology expert such as a pharmacist.
Limitations
Subgroup comparisons should be interpreted cautiously, as stratification by discipline and medication-related variables resulted in small samples and sample size differences, reducing statistical power. Although the overall sample size is acceptable for an exploratory study in a specialized population, it may not fully represent the heterogeneity of ballet dancers. In addition, as the study was conducted within a Spanish context, the results may not be directly generalizable across broader or international populations. Gender was not included as a variable since the study focused on general pharmacological practices within ballet, aiming a population-level epidemiological perspective rather than individual analysis. However, a potential bias is acknowledged due to a predominance of female participants, reflecting typical gender distribution in ballet.
Future Recommendations
Future studies should further explore the therapeutic categories of medications and the specific pathologies they are intended to treat within dance. Assessing the therapeutic efficacy of these medications, performance-based testing and monitor adverse effects. This would support the development of evidence-based, dancer-specific pharmacological protocols that effectively manage health conditions while promoting performance and safety.
Practical and Clinical Applications and Implications
The high prevalence of injuries and health conditions in dancers highlights the need for a multidisciplinary approach involving specialized healthcare professionals to establish ongoing care, building trust and encouraging dancers to seek help when health concerns arise without hesitation. Education on managing pain, injuries and health conditions including safe pharmacotherapy practices – should be incorporated into dancers’ training, teachers, coaches and masters.
Conclusions
This study reveals that medication use is widespread among classical ballet dancers, with non-steroidal anti-inflammatory drugs (NSAID) and paracetamol being the most reported, reported by over half of participants, followed by caffeine and benzodiazepines. The primary motivation for medication use appears to be therapeutic, to manage and alleviate symptoms related to the high incidence of injuries and mental health conditions. An exception is caffeine, which is predominantly used for its ergogenic effects. Notably, the initiation of medication use is often based on personal experience or recommendations from individuals outside the healthcare profession, particularly in over-the-counter medications. With the potential risks self-medication carries – masking underlying conditions, pharmacological interactions, and delayed diagnosis and appropriate treatment – not only affecting health but may also hinder physical performance and progression within the discipline. Addressing these issues through education and access to specialized healthcare support is essential for promoting safer pharmacological practices in dance.
Supplemental Material
sj-docx-1-dmj-10.1177_1089313X261448063 – Supplemental material for Medication Use for Therapeutic and Ergogenic Purposes in Ballet Dancers: Prevalence, Self-Medication, and Perceived Effects
Supplemental material, sj-docx-1-dmj-10.1177_1089313X261448063 for Medication Use for Therapeutic and Ergogenic Purposes in Ballet Dancers: Prevalence, Self-Medication, and Perceived Effects by Marian Vela-Andreu, Lucinda Villaescusa Castillo and Cristina Zaragozá Arnáez in Journal of Dance Medicine & Science
Supplemental Material
sj-docx-2-dmj-10.1177_1089313X261448063 – Supplemental material for Medication Use for Therapeutic and Ergogenic Purposes in Ballet Dancers: Prevalence, Self-Medication, and Perceived Effects
Supplemental material, sj-docx-2-dmj-10.1177_1089313X261448063 for Medication Use for Therapeutic and Ergogenic Purposes in Ballet Dancers: Prevalence, Self-Medication, and Perceived Effects by Marian Vela-Andreu, Lucinda Villaescusa Castillo and Cristina Zaragozá Arnáez in Journal of Dance Medicine & Science
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.