
Abstract
Introduction:
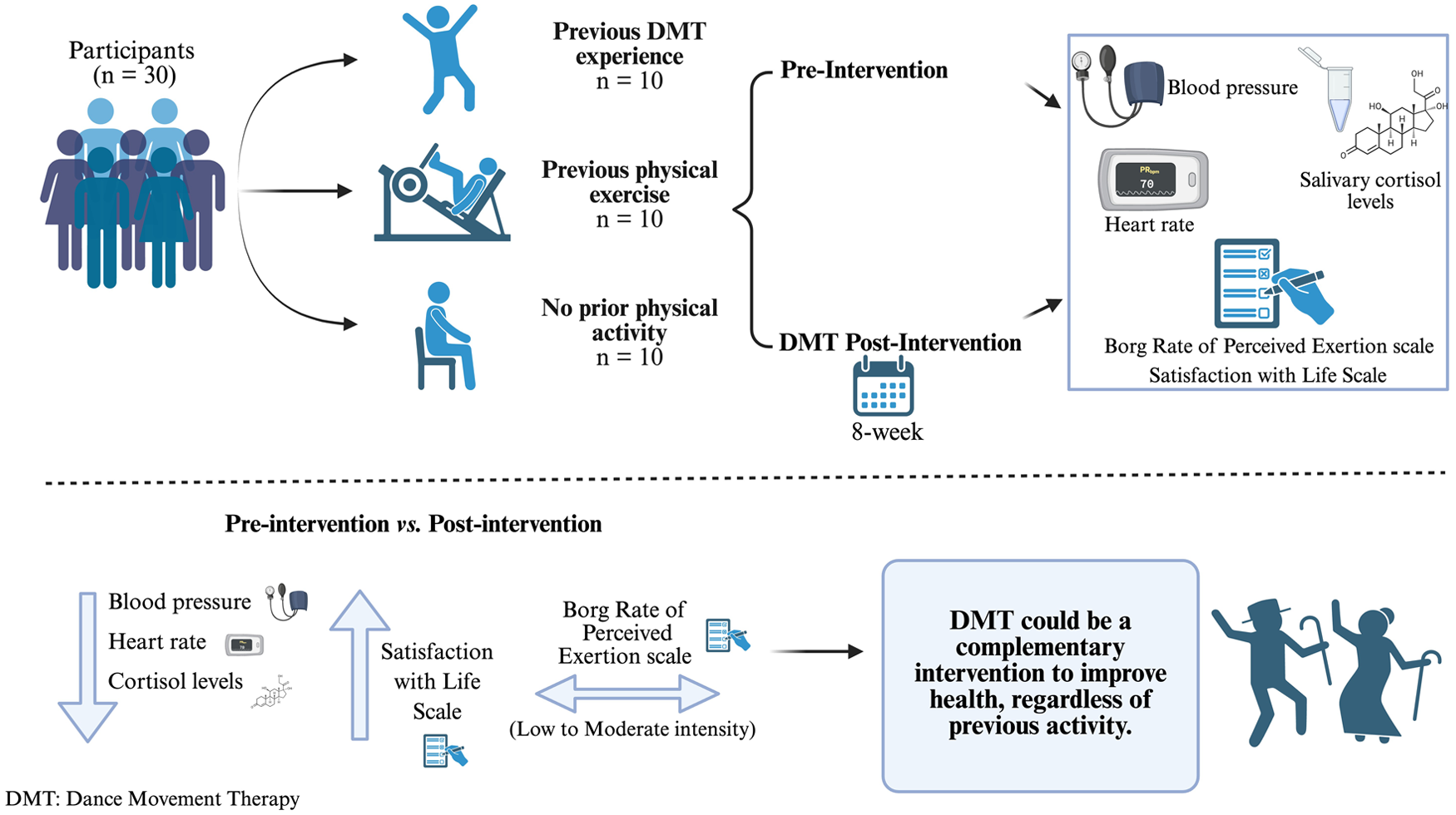
Dance Movement Therapy (DMT) is based on the mind-body interaction, where changes in movement can promote psychological well-being and physical health. This study aimed to assess the effects of DMT on stress-related physiological markers and psychological health outcomes, and to explore whether previous physical activity influenced participants’ responses.
Methods:
A pre-post experimental design was used with three groups classified by prior activity: previous DMT experience, previous physical exercise, and no prior physical activity. Thirty healthy adults (aged 25-55) participated in an 8-week DMT intervention. Salivary cortisol, systolic and diastolic blood pressure, heart rate, Borg of Perceived Exertion (RPE) scores, and the Satisfaction with Life Scale (SWLS) were measured at baseline and post-intervention.
Results:
All participants showed significant reductions in cortisol levels (P < .001), systolic and diastolic blood pressure (P < .05) and heart rate (P < .05) at the end of the session. Participants who had previously exercised had significantly lower heart rate values throughout the session (P < .05). Borg RPE scores fluctuated over time, with week-to-week changes suggesting variable perceived exertion. SWLS scores increased significantly from baseline to post-intervention (P < .001), with similar trends in all groups.
Conclusions:
DMT was associated with improvements in both physiological stress markers and life satisfaction, regardless of participants’ prior physical activity levels, and was perceived as a low-to-moderate intensity intervention. These findings could support the use of DMT as a non-pharmacological approach that can be used to improve emotional well-being and cardiovascular regulation in a wide range of situations.
Key Points
Dance Movement Therapy significantly reduced stress-related physiological markers, including cortisol levels, blood pressure, and heart rate, indicating its calming and regulatory effects on the body.
Participants experienced greater emotional well-being and life satisfaction, regardless of their previous levels of physical activity, highlighting the accessibility and psychosocial benefits of Dance Movement Therapy.
Dance Movement Therapy was perceived as a low-to-moderate intensity activity, making it a feasible, enjoyable, and inclusive intervention for adults, older individuals, and those with neurodegenerative conditions.
Introduction
Dance has been present in all cultures and societies since the dawn of humanity, providing individuals with a means of expression and communication of feelings and emotions. 1 At the beginning of the 20th century, a movement called “modern dance” emerged in dance, emphasizing expressiveness, spontaneity, and creativity. These influences contributed to the emergence of Dance Movement Therapy (DMT) in the 1950s. 2 Some of the DMT’s basic assumptions include that our mind and body are in constant interaction, and that changes in movement patterns lead to psychological changes, promoting personal growth and an overall improvement in health. 1 Additionally, DMT promotes communication, increases self-esteem and motivation, and it relieves tension in practitioners, while activating our physical body and improving our cardiovascular system 3 or reducing stress levels. 4
Cortisol, a steroid hormone, is released in response to stress and low levels of glucocorticoids in our blood. 5 Short-term elevations of cortisol have immediate beneficial effects on our health (survival-acute stress or eustress), but prolonged elevations have harmful effects (chronic stress), causing alterations in the body such as cardiovascular problems, sleep disorders, anxiety/depression, endocrine system disruption, cognitive problems, and even substance abuse.6 -8 The study by Flórez-Villamizar et al 7 has shown that music-based physical practices, such as DMT, can reduce cortisol levels and increase dopamine and endorphins, promoting serenity and mental calmness. Marian Chace work’s was well received by neuropsychiatric professionals, who, after observing the positive effects of dance on psychotic patients, incorporated DMT as a non-pharmacological treatment approach. 1
Therefore, the study aimed to explore the overall effects of DMT on stress-related and psychological outcomes, and to examine whether participants’ prior physical activity influenced their responses to the intervention.
Methods
Study Design
This study employed a quasi-experimental, pre-post intervention design with three non-randomized groups classified according to their previous physical activity: previous experience with DMT, engagement in other types of physical exercise, and no prior regular physical activity.
All participants completed a two-month DMT program, consisting of weekly 45-minute sessions led by a certified dance therapist. The activities combined music-guided movement, improvisation, and mind-body connection exercises, aiming to enhance emotional expression, body awareness, and stress regulation. These goals are supported by research showing that integrating movement and creativity helps channel emotions, improve emotional self-efficacy, and reduce stress markers such as cortisol. Physiological and psychological variables were assessed before and after the intervention.
Study Population
This study included a total of 32 participants, aged between 25 and 55 years. All participants were healthy adults who voluntarily agreed to participate and signed an informed consent form. Exclusion criteria for all groups included the presence of any pre-existing medical condition or the use of pharmacological treatment.
Although the study included three groups the sample size estimation was based on the primary binary comparison of interest: participants with previous DMT experience versus those with no history of physical activity. The sample size was calculated using OpenEpi (v3.01). Assuming a two-sided confidence level of 95%, 80% power, and a 1:1 ratio of controls to cases, it was estimated that 20% of controls (participants with lower post-intervention improvement in life satisfaction) and 80% of cases (participants with greater improvement) had prior DMT experience. 9 Based on these parameters, the minimum sample size required was 18 participants (9 in each group). In the end, 30 participants completed the study, with an equal distribution of 10 participants in each group.
Prior to participation, all individuals were thoroughly informed about the nature of the study and provided written informed consent. All data were anonymized and managed in compliance with current data protection regulations. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki and approved under Agreement 13/CG 1-2-2019 of the Local Governing Council, in accordance Article 12 of Law 14/2007 of July 3 on Biomedical Research, and Royal Decree 53/2013 of February 1.
Dance Movement Therapy Intervention
The DMT sessions comprised a series of structured activities designed to activate the body and mind progressively. Each session began with a ten-minute general warm-up using the ‘Tree of Life’ exercise, followed by a five-minute ‘march’ at varying speeds to enhance body awareness and movement coordination. This was followed by a ten-minute ‘Creation in Pairs’ exercise to promote bodily expression and creative interaction between participants. This was followed by a five-minute ‘ReConnect the March’ activity, which introduced a brief pause before transitioning to the next task. The ten-minute “Expansion Levels” exercise encouraged movement improvisation along the body’s three axes (floor work, standing, and jumping). Finally, each session ended with a five-minute cool-down in a relaxed position on the floor, accompanied by guided relaxation led by the dance therapist.
To sustain participants’ motivation while maintaining a consistent structure encompassing physical and mental activation, activities and music varied between sessions, with the structure consisting of a warm-up, psychomotor engagement and final relaxation, integrating individual, partner and group movement work.
Clinical Evaluation of Participants
Weight and height measurements were obtained following the standard measurement procedure using the Laica® scale Mod. EP1450 and the mechanical platform stadiometer T628, respectively. The body mass index (BMI) was calculated using Quetelet’s formula: weight (kg)/height (m2). Systolic and diastolic blood pressure, as well as heart rate, were measured using a digital blood pressure monitor: OMRON-M2-BASIC-HEM-7121J-E (standard cuff: 12-13 cm wide and 35 cm long; accuracy: pressure ± 3 mmHg; pulse ± 5% of the displayed reading; measurement range: 20 to 280 mmHg for blood pressure and 40 to 180 beats per minute (bpm) for pulse). Participants rested for 5 minutes before the first measurement, and two readings were taken 1 to 2 minutes apart. If the initial readings differed by more than 10 mmHg, additional measurements were performed. The final blood pressure value was calculated as the average of the last two readings. Heart rate was measured using the OMRON-M2-BASIC-HEM-7121J-E device. If the initial and final heart rate measurements differed by ± 10 bpm, additional readings were taken. The final heart rate and blood pressure values were calculated as the average of the last two readings.
Determination of Salivary Cortisol
Salivary cortisol samples were collected to assess stress levels at the beginning and end of the study. Cortisol levels were measured using an enzyme immunoassay. The reference values for salivary cortisol were provided by the laboratory, considered the morning range of 1.19 to 7.21 ng/mL. Salivary cortisol samples were collected before physical activity, minimizing the effect of movement on the measured levels. Participants were instructed on precautions prior to sample collection, such as not smoking or eating for 30 minutes beforehand. An external collaborator was responsible for transporting the samples to the laboratory in less than five minutes, using the coolers provided. To avoid bias, samples were collected within the same time frame depending on the study group (previous DMT experience: 9:00 am; previous physical activity: 10:00 am; no previous physical activity: 11:00 am).
The samples were then stored at 4°C and subsequently analyzed at the reference laboratory (authorization number: 3034, and subject to external quality control – AEFA – 2021).
Measurement Scales
Borg Rate of Perceived Exertion scale
Borg Rate of Perceived Exertion (RPE) scale 10 is a tool used to measure the intensity of physical effort perceived by an individual during physical activity. Data collection took place after each DMT session. The scale is based on a numerical range, typically from 6 to 20, representing: very light effort (scores 6-8); Light effort (scores 9-12); somewhat hard effort (scores 13-14); Hard effort (scores 15-16); very hard effort (scores 17-19); and maximum effort (score 20). The use of Borg’s tool has expanded in recent decades in both sports sciences and DMT research. 10 It allows researchers to gather data on how a person feels during physical activity, providing a subjective assessment that complements more objective analyses, thereby enriching both the research and its evaluation.10,11 Additionally, this tool offers the advantage of being an easily accessible and non-invasive method, reducing administration costs and allowing for application in different contexts. 12
Satisfaction with Life Scale
Satisfaction with Life Scale (SWLS) is a global life satisfaction scale designed to generally assess a person’s subjective well-being, with strong psychometric properties in terms of reliability and validity. 13 Data collection occurred at three points in the study: at the beginning, midway, and at the end of it. The scale consists of five items, each with five response options indicating the degree of agreement (Most aspects of my life are as I want them to be; The circumstances of my life are very good; I am satisfied with my life; So far, I have gotten the important things I want in life; If I could live my life over, I would change almost nothing). Response options for each item: 1 = strongly disagree; 2 = disagree; 3 = neutral; 4 = agree; and 5 = strongly agree.13,14 This scale provides valuable data regarding an individual’s subjective life satisfaction in a simple, cost-free, and risk-free manner, while also being a reliable assessment tool. 15
Statistical analysis
The data were analyzed using SPSS software version 28.0.1.0 (IBM Corp.) and Jamovi (2.6.26). A Shapiro-Wilk test was applied to assess the normality of the distribution of continuous variables. Data were expressed as mean ± standard deviation (SD) for normally distributed variables and as median with interquartile range (IQR) for non-normally distributed variables. Categorical data were presented as percentages. To compare categorical variables between groups, the Chi-square (χ2) test was used. The mean values between groups were compared using the Student’s t-test or Welch’s t-test for continuous and normally distributed variables. Mann-Whitney U test was used to compare variables non-normal distribution. ANOVA or Kruskal-Wallis were used for comparisons of continuous variables with normal or non-normal distribution, respectively, between groups. The significance level of P < .05 (two-tailed) was considered statistically significant.
Results
Clinical Characteristics of the Study Participants
Table 1 presents the clinical and biochemical parameters of three groups based on their history of physical activity and DMT practice. The groups are homogeneous, with no significant differences in sex, age, or clinical parameters and no additional information was collected regarding gender expression or identity.
Clinical Characteristics and Biochemical Parameters of the Different Participant Groups in the Study.
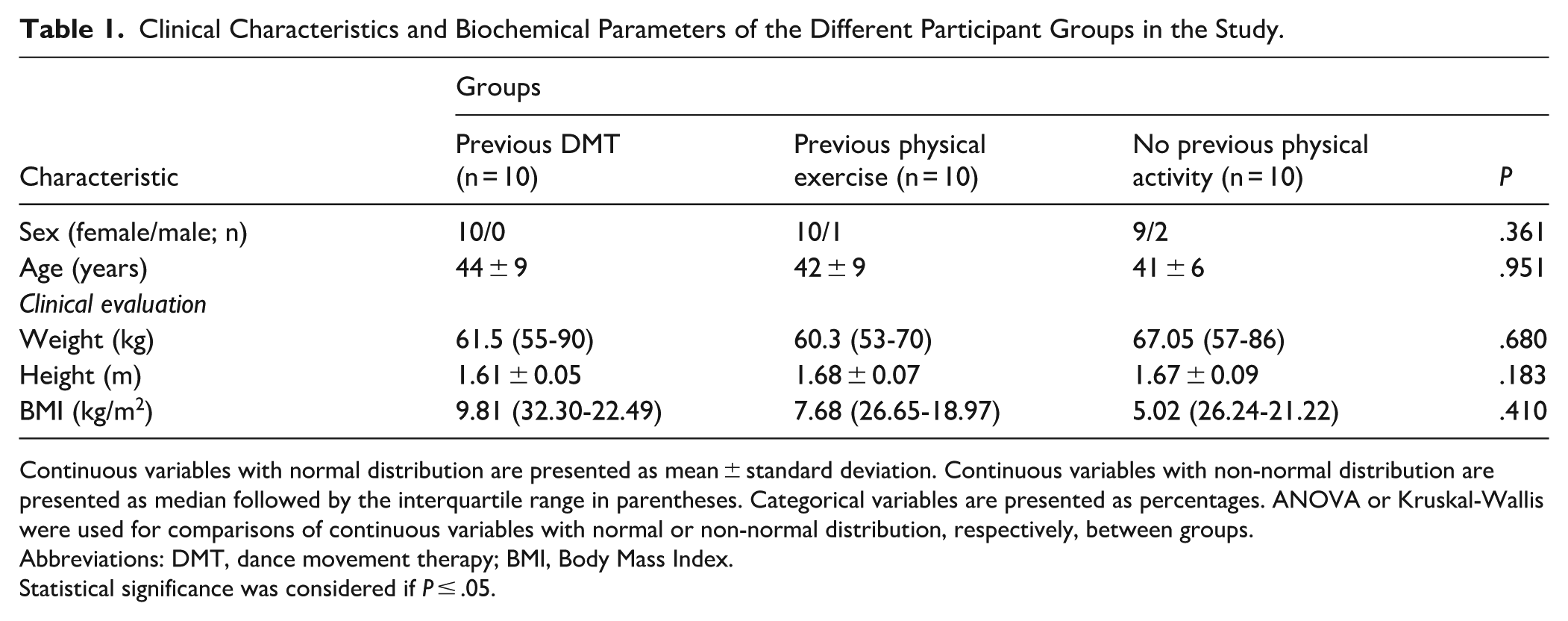
Continuous variables with normal distribution are presented as mean ± standard deviation. Continuous variables with non-normal distribution are presented as median followed by the interquartile range in parentheses. Categorical variables are presented as percentages. ANOVA or Kruskal-Wallis were used for comparisons of continuous variables with normal or non-normal distribution, respectively, between groups.
Abbreviations: DMT, dance movement therapy; BMI, Body Mass Index.
Statistical significance was considered if P ≤ .05.
Blood Pressure Measurement During the Study
The systolic blood pressure of all participants showed an overall decrease at the end of each DMT session in the weekly difference (initial-final) (Table 2). When comparing the initial systolic blood pressure of weeks 1 and 8, no significant differences were found. However, when comparing the final systolic blood pressure between weeks 1 and 8 (107 ± 13 vs 111 ± 15 mmHg; P = .035), a significant decrease in blood pressure was observed. When participants are separated according to groups, significant differences in systolic blood pressure are found between weeks (Table 2).
Relevant Parameters of the Systolic and Diastolic Blood Pressure of All Participants and the Significant Differences by Groups About Systolic Blood Pressure. Initial Versus Final of Each Week.
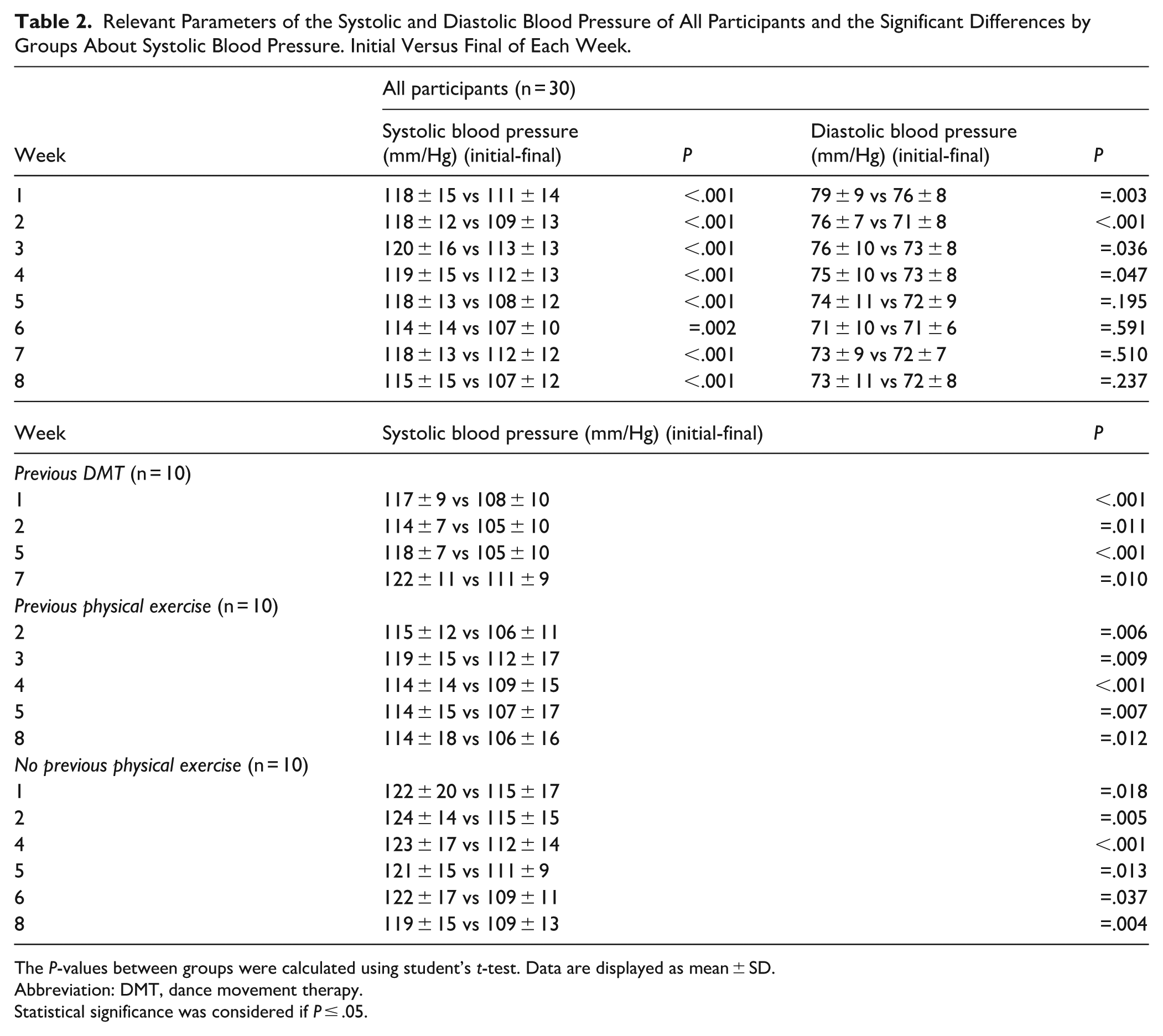
The P-values between groups were calculated using student’s t-test. Data are displayed as mean ± SD.
Abbreviation: DMT, dance movement therapy.
Statistical significance was considered if P ≤ .05.
Regarding diastolic blood pressure there were significant differences in the results of the first four weeks (initial-final) (Table 2). Moreover, significant differences were found when comparing the initial and final values between weeks 1 and 8 (79 ± 9 vs 73 ± 11 mmHg; P = .002) and (76 ± 8 vs 72 ± 8 mmHg; P < .001), respectively. No significant differences were observed between the groups in diastolic blood pressure measurements. No significant differences were observed between the groups in either systolic or diastolic blood pressure measurements, both at the beginning and end of each week of the study (P > .05).
Heart Rate Response
Heart rate measurements across the intervention showed a significant reduction at the end of each DMT session compared to the beginning, in all weeks except week 1. These reductions were consistent across the total sample, indicating an acute physiological response to the activity (Table 3). When participants were grouped by prior physical activity, significant within-group changes in heart rate were also observed across weeks (Table 3).
Relevant Parameters of the Heart Rate of All Participants and the Significant Differences by Groups About Heart Rate. Initial Versus Final of Each Week.
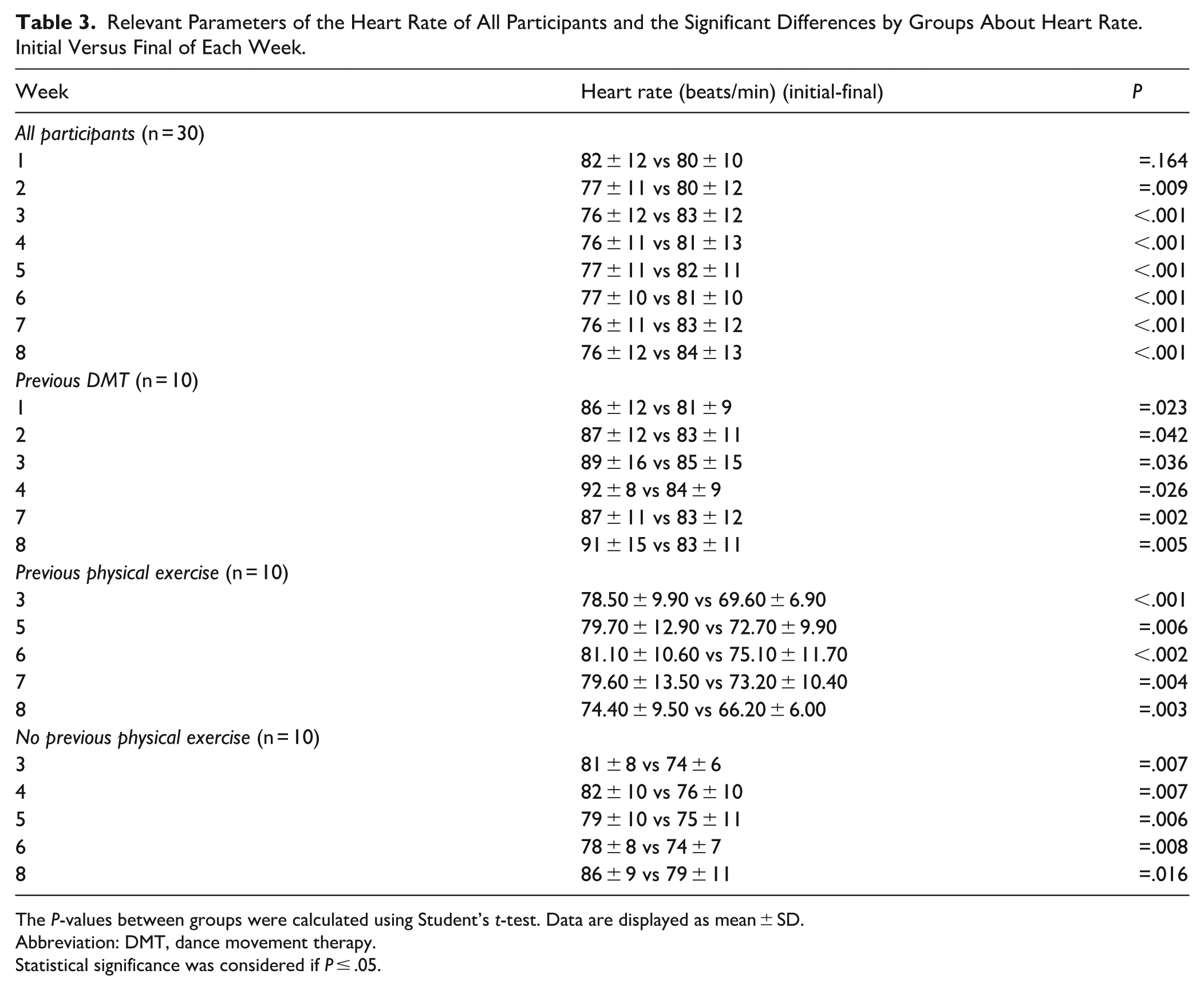
The P-values between groups were calculated using Student’s t-test. Data are displayed as mean ± SD.
Abbreviation: DMT, dance movement therapy.
Statistical significance was considered if P ≤ .05.
Between-group comparisons of initial heart rate revealed significantly lower values in the prior physical exercise group compared to the no prior activity group in week 2 (75 ± 9 vs 88 ± 12 bpm; P = .018), week 4 (70 ± 9 vs 92 ± 8 bpm; P < .001), and week 8 (74 ± 10 vs 91 ± 15 bpm; P = .012). Additionally, the prior exercise group also showed significantly lower initial heart rates than the prior DMT group in week 4 (70 ± 9 vs 82 ± 10 bpm; P = .016). Regarding final heart rate, the prior exercise group displayed significantly lower values than the no prior activity group in week 2 (71 ± 8 vs 83 ± 11 bpm; P = .036), week 3 (70 ± 7 vs 85 ± 15 bpm; P = .005), week 4 (69 ± 11 vs 84 ± 9 bpm; P = .003), week 5 (73 ± 10 vs 84 ± 10 bpm; P = .038), and week 8 (66 ± 6 vs 83 ± 11 bpm; P = .002). Moreover, a significant difference was observed between the prior exercise group and the DMT group in week 8 (66 ± 6 vs 79 ± 11 bpm; P = .024). These results may indicate that individuals with prior physical activity tended to show a more favorable cardiovascular response during the intervention.
Determination of Salivary Cortisol Levels
The salivary cortisol levels of all participants showed a significant decrease at the end of the activity compared to the beginning (3.18 ± 2.05 vs 7.17 ± 2.83 ng/mL; P < .001) (Figure 1). However, the initial cortisol levels of each participant before starting the DMT activity did not show significant differences between the three groups (P = .833). Similarly, the cortisol measured at the end of the intervention also did not show significant differences between groups (P = .218).
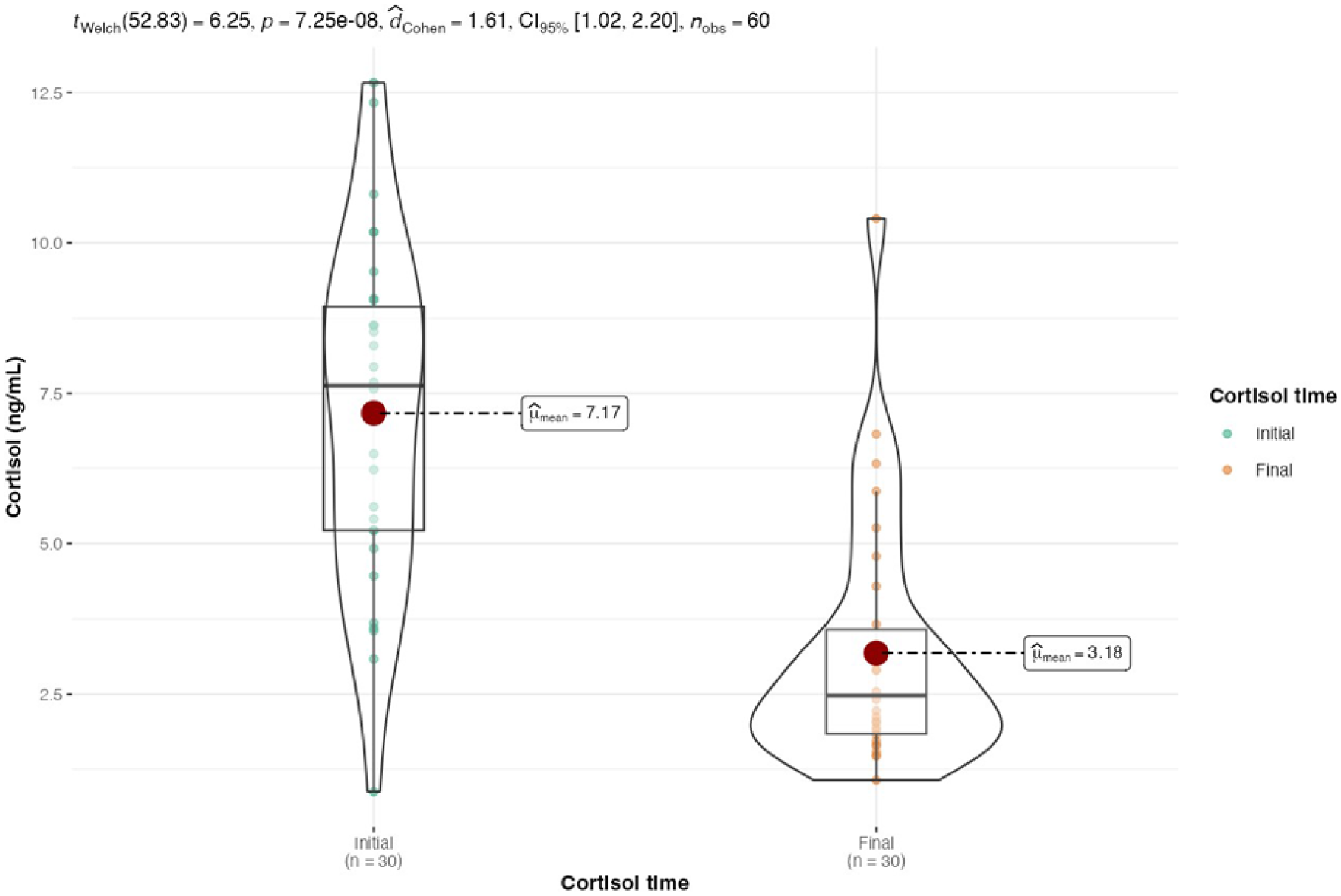
Overall results of initial and final salivary cortisol levels for all participants.
Significant intergroup differences were observed in cortisol levels measured at the beginning of the intervention compared to the end, with the group that did not engage in any previous activity. The group that did not engage in any physical activity previously showed 6.95 ± 2.93 vs 2.39 ± 1.06 ng/mL (P < .001), the group that practiced some physical activity previously showed 6.72 ± 3.37 vs 3.09 ± 1.45 ng/mL (P = .009), and the group that practiced DMT previously showed 7.83 ± 2.31 vs 4.06 ± 2.96 ng/mL (P = .005). Overall, the findings seem to suggest a potential positive modulation of salivary cortisol levels in participants, independent of prior physical activity.
Comprehensive Assessment of the Borg Rate of Perceived Exertion Scale
The Borg RPE scores recorded during the eight DMT sessions revealed several significant changes over time in the overall sample. Notably, significant differences were observed between week 1 and week 2 (11 ± 2 vs 10 ± 2 score; P = .007), as well as between week 2 and subsequent weeks: week 3 (10 ± 2 vs 11 ± 2 score; P = .046), week 4 (10 ± 2 vs 11 ± 2 score; P = .034), week 5 (10 ± 2 vs 11 ± 2; P = .009), week 6 (10 ± 2 vs 11 ± 2 score; P = .002), week 7 (10 ± 2 vs 10 ± 2 score; P = .004), and week 8 (10 ± 2 vs 12 ± 2 score; P < .001). Additionally, week 3 differed significantly from week 8 (11 ± 2 vs 12 ± 2 score; P = .045). These findings suggest dynamic changes in perceived exertion throughout the program.
When participants were stratified by prior physical activity, distinct patterns emerged. In the group with previous DMT experience, significant differences were noted between weeks 1 and 2 (12 ± 1 vs 10 ± 1; P = .004 score), weeks 1 and 5 (12 ± 1 vs 11 ± 2; P = .012 score), weeks 2 and 7 (10 ± 1 vs 12 ± 1 score; P = .007), and weeks 2 and 8 (10 ± 1 vs 12 ± 1 score; P = .007). In the group with prior physical activity, significant increases in perceived exertion were found between weeks 1 and 8 (10 ± 2 vs 11 ± 3 score; P = .039), weeks 2 and 8 (10 ± 2 vs 11 ± 3 score; P = .001), weeks 6 and 8 (10 ± 2 vs 11 ± 3 score; P = .010), and weeks 7 and 8 (10 ± 2 vs 11 ± 3 score; P = .018). In the group without prior physical activity, perceived exertion increased significantly between weeks 2 and 5 (11 ± 1 vs 12 ± 1 score; P = .041), weeks 2 and 6 (11 ± 1 vs 12 ± 1 score; P = .011), and weeks 3 and 6 (11 ± 1 vs 12 ± 1 score; P = .012), followed by decreases from week 6 to week 7 (12 ± 1 vs 11 ± 1 score; P = .032) and from week 6 to week 8 (12 ± 1 vs 11 ± 1 score; P = .010). These group-specific trends suggest that prior activity level may influence adaptation and perception of physical effort throughout the intervention.
Group-specific patterns revealed that participants with previous DMT experience reported a decline in moderate-to-high exertion levels (scores 13-15) over time. Those with prior physical exercise maintained relatively stable exertion levels throughout, predominantly within the moderate range (scores 9-11). In contrast, participants without prior physical activity exhibited a marked increase in perceived exertion between weeks 2 and 6, suggesting lower tolerance or slower adaptation. These patterns, broadly aligned with the overall sample trend, may reflect shifting perceptions of physical effort throughout the intervention and suggest a potential role of prior activity levels in shaping exertion responses (Figure 2).

Weekly distribution of Borg Rating of Perceived Exertion (RPE) scores (range: 6-20) across the eight Dance Movement Therapy (DMT) sessions.
Integral Assessment of the Satisfaction with Life Scale
SWLS scores were evaluated at three time points: baseline (initial), mid-intervention (intermediate), and post-intervention (final). In the total sample, a significant increase in life satisfaction was observed from the initial to the final assessment (3.44 ± 0.90 vs 4.02 ± 0.54 score; P < .001), as well as from the intermediate to the final assessment (3.56 ± 0.61 vs 4.02 ± 0.54 score; P < .001). No significant change was detected between the initial and intermediate scores (P = .260), suggesting a gradual improvement that became statistically meaningful toward the end of the program (Figure 3).
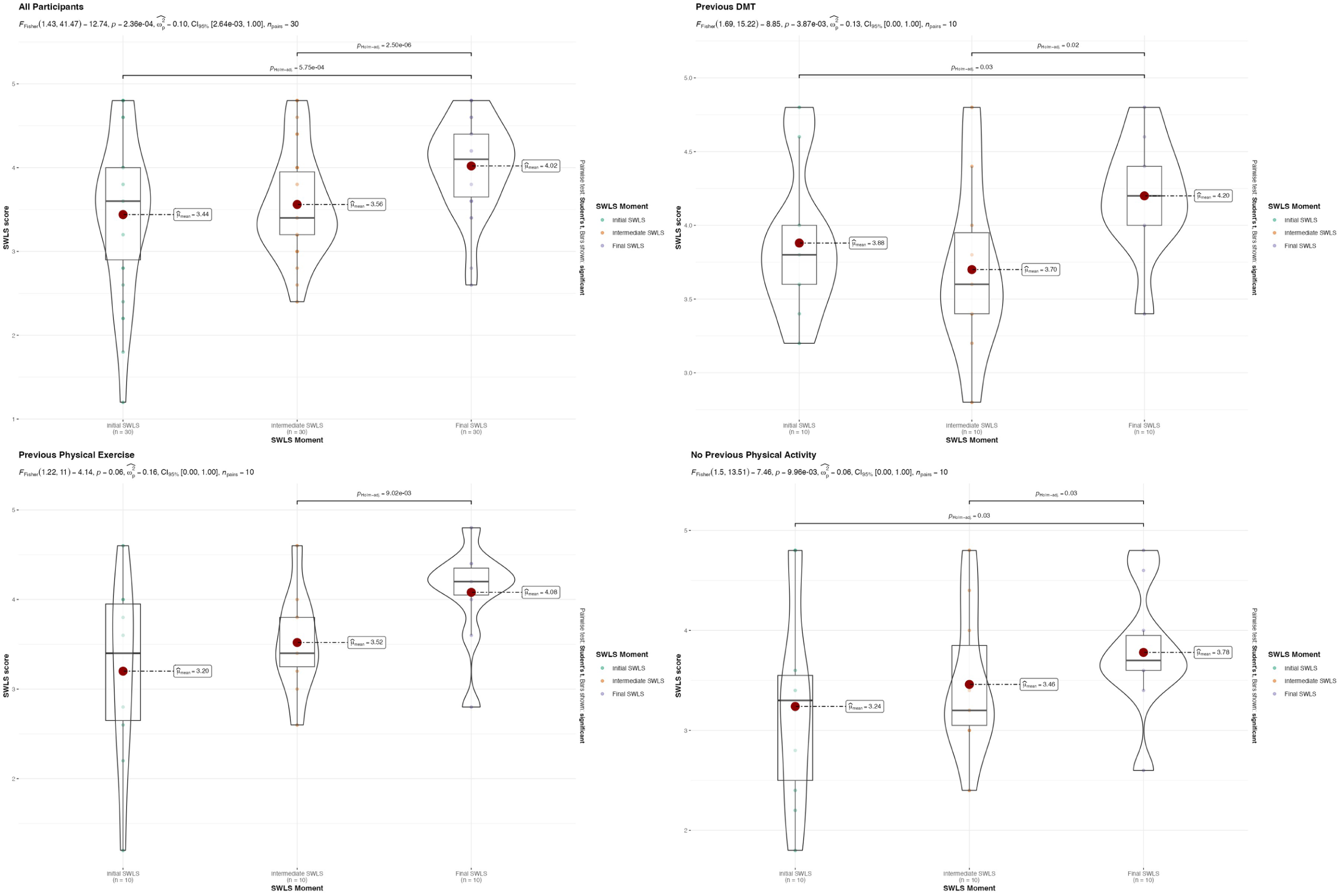
Violin plots illustrating the distribution of Satisfaction with Life Scale (SWLS) scores at three time points (initial, intermediate, and final) across the total sample and by participant group.
When analyzed by group, all three groups exhibited a similar upward trend in life satisfaction across the intervention. The group with previous DMT experience showed significant improvements from the initial to the final measurement (3.88 ± 0.50 vs 4.20 ± 0.39 score; P = .03) and from the intermediate to the final score (3.70 ± 0.58 vs 4.20 ± 0.39 score; P = .02). The group with prior physical activity also demonstrated a significant increase from the intermediate to the final assessment (3.52 ± 1.02 vs 4.08 ± 0.54 score; P < .001). Likewise, the group without prior physical activity showed a significant improvement both from the initial to the final time point (3.24 ± 1.01 vs 3.78 ± 0.61 score; P = .03) and from intermediate to final (3.46 ± 0.72 vs 3.78 ± 0.61 score; P = .03). These results may suggest a tendency toward improved life satisfaction over the course of the intervention. However, in all groups, the difference between initial and intermediate scores was not statistically significant (P > .05) (Figure 3). Additionally, no significant differences in SWLS scores were observed between groups at any of the three time points (P > .05).
Discussion
This study represents a preliminary exploration of the potential health benefits of DMT. The findings demonstrate a significant reduction in blood pressure among participants following the intervention. Additionally, heart rate measurements showed a consistent decrease at the end of each session, particularly in individuals with a prior history of physical activity. Salivary cortisol levels also significantly decreased post-intervention, with no significant differences between participant groups, indicating a general stress-reducing effect of DMT. In terms of psychological outcomes, no significant changes were observed on the Borg RPE scale between the first and final sessions. However, SWLS scores increased significantly from baseline to post-intervention in all groups, suggesting an improvement in subjective well-being. Overall, these results suggest that DMT may contribute positively to both physiological regulation and psychological well-being, regardless of participants’ prior physical activity levels.
Some of the studies have been developed at the intersection of DMT and 20th-century Psychology. 16 DMT is an inclusive discipline that promotes participation regardless of race, culture, age, or sexual identity, and is characterized by its capacity to integrate diverse groups. 17 Additionally, the literature has indicated that activities that generate enjoyment, such as DMT, may promote adherence to physical exercise and support its long-term maintenance. 18
It is important to highlight the relationship with the body through the practice of DMT, which intervenes in basic elements observed in movement, where movement factors such as flow, weight, time, space, or spatial aspects like direction and trajectory of movement, or the vertical, horizontal, and sagittal dimensions, provide the ontological development of the individual symbolically. 19 DMT does not require prior physical preparation like some sports or more specific physical exercises; it is independent of age and physical or mental condition to engage in this practice.7,17
In line with the findings reported by Hogan (2019), which indicate a marked female overrepresentation in movement-based therapeutic practices (87% women), our study similarly reflected this trend, with 94% of participants being female. 20 This aspect suggests the need for strategies to encourage male participation in DMT and other activities with similar benefits.
Effects of the intervention on blood pressure: a significant reduction in systolic blood pressure was observed at the end of each DMT session compared to the initial values, suggesting a relaxing and vasodilatory effect. This may be related to the nature of DMT, which combines guided movement, music, and mind-body awareness to promote relaxation and moderate aerobic activity. These results are consistent with previous studies that associate DMT and other forms of aerobic activity with improvements in blood pressure and blood flow.7,21 The literature highlights that aerobic capacity is a key component of cardiovascular health, supporting the hypothesis that DMT could contribute to the prevention of cardiovascular diseases. 22 Valero et al 23 emphasizes that aerobic capacity is the physical condition component most related to health, as it constitutes a direct measure of a person’s overall health, specifically the condition of the cardiovascular, metabolic, and respiratory systems. Therefore, the practice of DMT could be beneficial at the cardiovascular, metabolic, and respiratory levels, according to related studies, 24 reinforcing the World Health Organization’s recommendation for engaging in regular aerobic physical activity at appropriate levels to help improve cardiorespiratory, functional, and musculoskeletal health. 7
Heart rate to the intervention: a significant reduction was observed at the end of each session, with a more pronounced effect in participants who engaged in prior physical exercise. This finding is consistent with previous research showing that moderate aerobic activity can improve cardiovascular system efficiency and reduce resting heart load. 24 It is worth noting that physical practices with a high playful and enjoyable component, such as fitness, allow heart rate to reach frequent intervals of maximum heart rate, where participants describe their perceived effort as moderate or low during some intervals. 7 Thus, musicalized practices such as DMT could be considered more enjoyable physical activities, akin to moderate/low-intensity aerobic exercise.7,25
Salivary cortisol response to DMT: It has been shown that cortisol levels can vary in relation to abnormal levels of adrenocorticotropic hormone associated with conditions such as clinical depression, psychological stress, and physiological stress. In this study, cortisol levels decreased significantly after the practice of DMT, indicating a reduction in physiological stress. This finding aligns with previous research showing that creative and expressive therapies, such as music therapy, laughter therapy, and DMT, can promote relaxation and improve stress regulation.8,26 In contrast, intense physical exercise can stimulate the release of cortisol and prolong its presence in the bloodstream.8,9 Furthermore, a reduction in cortisol has been linked to an improvement in subjective well-being.9,27 In line with this, it has been observed that reducing stress and muscle tension through music-based physical activities such as DMT may lead to a decrease in systolic blood pressure, as reported by Flórez Villamizar et al. 7 The group with no prior physical activity experienced the greatest reduction in average cortisol levels, which could indicate that DMT might have a more marked effect on individuals who are less accustomed to physical exercise, suggesting a potential avenue for future research.
On the other hand, there is extensive evidence supporting the use of salivary cortisol as a reliable diagnostic tool, due to its predictable correlation with total blood cortisol levels. Most of the published studies on this biomarker have explored its application in psycho-neuroendocrinology research and the diagnosis of Cushing’s syndrome.28,29
In the field of mental health, DMT facilitates emotional expression and the release of repressed bodily tensions, helping to unlock the so-called “defensive armors” created by stress and anxiety. 1 In this study, cortisol levels decreased significantly after the practice of DMT, indicating a reduction in physiological stress. This finding is supported by research suggesting that creative and expressive interventions, such as DMT, can promote relaxation and improve stress regulation.7,17
Additionally, the effects of DMT on Alzheimer’s patients have been explored, observing improvements in quality of life, communication, and social interaction for those who participated in these interventions. 30 These findings align with the results of our study, where a significant increase in SWLS scores was observed at the end of the intervention, indicating an improvement in the perception of well-being and life satisfaction. Previous studies have linked higher life satisfaction levels with lower depression rates and greater life expectancy.31,32 Furthermore, in older adult populations, the practice of music-based aerobic activities has been shown to increase confidence, autonomy, and emotional well-being. 33
Physical strain assessment: the results obtained from the Borg RPE scale indicate that the perceived effort during DMT was mostly rated as “fairly light” or “very light,” suggesting that this practice can be considered moderate or low-intensity aerobic exercise, as per previous studies.24,34 This characteristic makes DMT easily tolerable for participants and enhances their adherence to continued practice. 24
Effect of DMT on SWLS: Another relevant aspect derived from the use of the SWLS scale is the relationship between moderate-intensity aerobic exercise and life satisfaction in older adults. Sepúlveda Mancilla et al 33 emphasize that aerobic activity programs not only improve physical and mental well-being but also reinforce confidence and autonomy in daily life. Additionally, music-based activities facilitate adherence to exercise, promoting greater commitment to regular practice.
These findings suggest that DMT may hold potential as a non-pharmacological therapeutic approach for vulnerable populations, such as older adults or individuals with neurodegenerative conditions, by potentially offering both physiological and emotional benefits that support quality of life.
Despite the review and analysis of previous studies on DMT and its benefits, the available literature remains limited. Most existing research focuses on music-based practices 25 and their effects on cardiovascular health as aerobic exercise.8,24 In this study, DMT was applied to various groups with different mental capabilities, using qualitative evaluation methods through validated scales and direct observation to analyze changes in stress levels and emotional expression.1,17 Among the main limitations of this study, the small sample size stands out, which may affect the generalizability of the results. Larger studies with more participants are needed to obtain more robust conclusions that can be extrapolated to different populations. Additionally, there is a lack of standardized criteria for the training of DMT professionals. Accreditation as a dance therapist is obtained through various pathways, including psychology, dance, or general university education, without specific requirements regarding multidisciplinary competencies. Therefore, it is important to highlight the need for adequate training for dance therapists, even though it is not mandatory to have a background in the artistic sciences of dance, health sciences, psychology, and/or group psychotherapy and movement, as recommended by international associations. Bräuninger et al 35 reported that 11 therapists completed intervention checklists during the sessions; however, their level of certification or professional training was not specified, which should be addressed in future research.
One of the main strengths of this study is its contribution to the existing evidence base on DMT, suggesting possible effects on cardiovascular function, stress regulation, and perceived well-being. Additionally, the analysis of biochemical parameters and the use of validated scales for a comprehensive evaluation of its effects are emphasized. To date, no studies have been identified with such a comprehensive approach, which can serve as a foundation for future research and promote the development of more specialized and multidisciplinary training in the field of DMT.
Conclusion
Overall, the findings of this study suggest that DMT has the potential to support physiological regulation and psychological well-being. The reductions observed in blood pressure, heart rate and cortisol levels, together with an improvement in life satisfaction, indicate the potential value of DMT as a non-pharmacological approach to complementing health and well-being promotion. However, further research using larger samples and more rigorous designs is needed to confirm these preliminary results and elucidate the underlying mechanisms.
Footnotes
Acknowledgements
The authors thank the director Alejandro Liendo y co-supervisor Tanusú Liendo of the Integral center of physical exercise, health and training – DxD, for providing the place to carry out the activity for the participants. Graphical Abstract created in BioRender. García-Fontana, B. (2025) (![]() ). This article is part of the doctoral thesis entitled: Beneficios de la Danza Movimiento Terapia en Relación con el Ejercicio Físico Convencional, which is part of PhD program in Ciencias Médicas y Farmacéuticas, Desarrollo y Calidad de Vida – Department of Basic Medical Sciences at the University of La Laguna (Spain).
). This article is part of the doctoral thesis entitled: Beneficios de la Danza Movimiento Terapia en Relación con el Ejercicio Físico Convencional, which is part of PhD program in Ciencias Médicas y Farmacéuticas, Desarrollo y Calidad de Vida – Department of Basic Medical Sciences at the University of La Laguna (Spain).
Ethical Considerations
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and approved under Agreement 13/CG 1-2-2019 of the Governing Council of the University of La Laguna, in accordance with Article 12 of Law 14/2007 of July 3 on Biomedical Research, and Royal Decree 53/2013 of February 1. Informed consent was obtained from all subjects involved in the study.
Author Contributions
OM. B-R, VC.M-R and N. M-G conceived and designed research; OM. B-R and VC.M-R conducted the intervention; OM. B-R, JF. R-P and S. G-S analyzed data; OM. B-R, N. M-G and S. G-S interpreted results; OM. B-R and S. G-S prepared figures; OM. B-R, MM. S-C, JF.R-P, N. M-G, and S. S-G drafted manuscript; OM. B-R, MM. S-C, N. M-G, and S. S-G edited and revised manuscript; OM. B-R and S. G-S approved final version of manuscript. All listed authors commented on multiple versions of the manuscript and supported the decision to submit the final draft.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Basic Medical Sciences, PhD Program in Medical and Pharmaceutical Sciences, Development and Quality of Life, Tenerife, University of La Laguna. Funding for the open access charge: Biblioteca Virtual del Sistema Sanitario Público de Andalucía (BV-SSPA), through the institutional agreement with SAGE Publishing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.