
Abstract
Introduction:
Dance-based exercise has been increasingly explored as a complementary intervention in oncology, with potential benefits for physical, psychological, and social health. However, evidence remains inconsistent, and the overall strength of evidence has not been clearly established. The purpose of this systematic review and meta-analysis was to evaluate the effects of dance-based exercise on health indicators in individuals with cancer.
Methods:
A systematic search of the literature was conducted in April 2025. Randomized controlled trials investigating dance-based interventions in adults with cancer were included. Outcomes of interest were quality of life, depression, and stress. Methodological quality was assessed using the PEDro scale, and certainty of evidence was evaluated using the GRADE approach. Where outcome measures were comparable, random-effects meta-analyses were performed using standardized mean differences (SMD) with 95% confidence intervals.
Results:
Meta-analytic results indicated that dance-based exercise significantly improved physical aspects of quality of life (standardized mean difference [SMD] = 0.61, 95% CI [0.07, 1.15], P = .03). A positive but non-significant trend was observed for the social/family component of quality of life (SMD = 0.87, 95% CI [−0.21, 1.95], P = .11). Heterogeneity across studies was high for both analyses. For depression and stress, pooled results did not reach statistical significance, although several individual trials reported improvements, particularly among participants with higher baseline stress levels. Evidence was very low to low quality.
Conclusions:
Overall, findings suggest that dance-based exercise represents a feasible and beneficial complementary intervention that can enhance selected dimensions of quality of life among cancer patients. Further research employing standardized intervention protocols and consistent outcome measures is needed to better characterize the magnitude and specificity of effects across psychological and physical health domains.
Key Points
Dance-based exercise may improve the physical component of quality of life in individuals with cancer, although overall certainty of evidence is very low.
Current evidence does not support a clear effect of dance interventions on depression or stress in cancer patients.
Substantial heterogeneity and low methodological quality limit clinical recommendations and highlight the need for more rigorous trials.
Introduction
Cancer is a group of 100+ diseases affecting all human tissues and a leading cause of death globally. In 2022, approximately 10 million people died from cancer with 20 million new cases reported. 1 In Slovenia, approximately 16 413 new cases and 6367 deaths annually (2017-2021). Most common types globally: lung, breast, colorectal, prostate, and stomach.1,2 Risk factors are intrinsic (random DNA errors) and extrinsic (modifiable). Major factors: tobacco, alcohol, inactivity, poor diet, excess weight, risky sexual behavior, radiation.3,4 Tobacco is the greatest preventable risk factor, linked to many types, especially lung cancer. 5 Alcohol is associated with oral, liver, and breast cancer. 6 Treatment includes surgery, radiotherapy, and systemic therapy, often in combination. 7 Side effects: spinal cord damage, lung fibrosis, hair loss, mucositis, hot flashes, sexual dysfunction. 6 Cancer severely impacts mental health. Following diagnosis, anxiety, depression, and PTSD are common. 8 One-third of hospitalized cancer patients suffer from mental disorders. 9 Mental disorders are linked to 53% higher mortality risk. 10
Physical exercise is an important supplementary support in cancer treatment 11 and provides numerous physiological and psychological benefits. 12 Increased activity improves cognitive and physical abilities, 13 mental health, 14 and quality of life, 15 while protecting against Alzheimer’s 16 and Parkinson’s disease 17 and post-traumatic stress disorder. 18 In cancer, exercise improves quality of life, treatment tolerance, reduces side effects, and inhibits tumor growth, 19 particularly for colorectal and breast cancer. 3 Best results come from supervised aerobic exercise, strength training, and combined programs.20,21 The American Cancer Society recommends 150 to 300 minutes of moderate-intensity or 75 to 100 minutes of vigorous-intensity exercise weekly22,23 confirmed that regular moderate-intensity aerobic exercise (3 times weekly for 12+ weeks) or combined programs (2-3 times weekly for 6-12 weeks) significantly reduce anxiety, depression, and fatigue while improving quality of life. Exercise must be individualized considering cancer type, treatment stage, and comorbidities, 24 which is critical for safety and effectiveness.
Dance in various forms represents an alternative exercise that can reduce negative consequences experienced by cancer patients. 25 It combines movement, rhythm, emotion, and symbolism and is one of humanity’s oldest and most universal forms of expression. 26 Dance is organized or spontaneous physical movement, performed individually or in groups, often accompanied by music, which transcends the aesthetic aspect, representing physical activity, self-expression, relaxation, and social interaction. Art and movement intertwine, giving it a unique position among activities, making it ideal for physical and mental health. In addition to these effects, dance interventions have been shown to enhance social connections, body self-awareness, emotional expression, and long-term preference for physical activity, representing important yet often overlooked dimensions of health in cancer populations. Increasingly, studies investigate the impact of dance interventions in cancer patients. Dance/movement therapy (DMT) is frequently studied, defined as psychotherapeutic use of movement for emotional, social, cognitive, and physical integration to improve health and well-being. 27 Fatkulina et al 28 recommend DMT as a supplement to standard cancer treatment as it improves quality of life and mental health in women with breast cancer. Abu-Odah et al 29 present positive effects of DMT on depression, fatigue, stress, and pain but note inconsistency and weakness in study results. Bradt et al 30 found no evidence of DMT effects on depression, stress, anxiety, fatigue, or self-perception, with low-quality evidence due to high bias risk. Rudolph et al 31 highlights the positive effect of social dance, which this group prefers in safe, adapted environments. Nelson et al 32 found that community dance programs positively impact cancer patients, with improvements in functionality, fatigue, and health-related quality of life. Research shows dance interventions have potential for cancer patients, but results are often inconsistent and low-quality, indicating need for higher-quality research.
Due to the inconsistency and low quality of existing research on the effects of dance interventions in cancer patients, the purpose of this paper is to conduct a systematic review of quality studies to better understand the impact of dance on the physical and mental health of this population and provide clearer guidelines for clinical practice.
Methods
This systematic review and meta-analysis was conducted in accordance with the PRISMA. A review protocol was not prospectively registered, which should be considered when interpreting the findings.
Search Strategy and Inclusion Criteria
A systematic literature search was conducted in April 2025. The search included two electronic databases: PubMed (National Library of Medicine) and DOAJ (Directory of Open Access Journals). The following search string was applied: “cancer” AND “dance”. Because these filters are not fully reliable, systematic reviews were also included in order to identify additional relevant primary studies that might have been missed by automated filtering. Duplicate records were removed before screening. The selection of studies proceeded in three steps: screening by title, screening by abstract, and full-text assessment. Two reviewers (SG and SJ) independently screened all records, with disagreements resolved through discussion and consultation of the third reviewer (ZK).
The eligibility of each study was determined using predefined inclusion criteria structured according to the PICOS framework 33 :
P (Population): Patients with cancer or cancer survivors, regardless of cancer type, disease stage, treatment modality, sex, age, race, or any other demographic or clinical variable.
I (Intervention): Dance-based exercise (all dance styles and modalities), including dance classes, structured dance exercise, or movement-based dance therapy.
C (Comparison): A control group receiving no intervention.
(Outcome): The most commonly reported variables in included studies, with an emphasis on quality of life, depression, and stress.
S (Study design): Randomized controlled trials (RCTs) with a control group.
Only studies that met all PICOS components were included in the final synthesis.
Data Extraction
All studies meeting the inclusion criteria were reviewed in detail, and relevant data were extracted into Microsoft Excel 365 (version 2503). Extracted information included:
Baseline participant characteristics: sex, age, education level, marital status, and health-related information (cancer type, cancer stage, treatment modality).
Intervention characteristics: duration of the intervention, duration and frequency of individual sessions, exercise intensity, dance style and music tempo, format of delivery, group size, progression, and supervision.
Outcome data: means and standard deviations for all measured variables reported across studies.
Two reviewers (SG and ZK) independently performed the data extraction, with disagreements resolved through discussion and consultation of the third reviewer (SJ).
Quality Assessment of Included Studies and Quality of Evidence
The methodological quality of all included studies was assessed using the PEDro scale, a valid and widely used tool for evaluating the quality of clinical trials. 34 The scale consists of 10 scored items (0-1), yielding a total possible score between 0 and 10. Based on their PEDro scores, studies were categorized into four quality levels: high quality: ≥9 points, moderate quality: 6 to 8 points, low quality: 4 to 5 points, and very low quality: ≤3 points
The certainty of evidence was assessed according to the GRADE Working Group guidelines. 35 The GRADE approach considers five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. For each comparison, the certainty of evidence was categorized as high, moderate, low, or very low. All comparisons initially started as high certainty and were downgraded if one or more of the following criteria were met: (a) substantial heterogeneity among studies (I2 > 50% or a statistically significant heterogeneity test), indicating inconsistency; (b) more than 25% of included studies were rated as fair or poor quality, indicating risk of bias; (c) indirect assessment of intervention effects (e.g., non-representative population, intervention, or outcomes), indicating indirectness; (d) imprecision, defined by wide CIs or a total sample size <200 participants; and (e) suspected publication bias, indicated by discrepancies between reported outcomes and the original study protocols or objectives.
Assessment of study quality and certainty of evidence was performed by two reviewers (SJ and ZK) independently performed the data extraction, with disagreements resolved through discussion and consultation of the third reviewer (MP).
Meta-Analysis
Meta-analyses were performed using Review Manager Software (Version 5.3; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, London, UK). A For each eligible outcome, effect sizes were calculated as standardized mean differences (SMD) with corresponding 95% confidence intervals, based on post-intervention means and standard deviations. Specifically, random-effects model with the inverse variance method was applied to determine the pooled effects of dance-based interventions on the selected outcome variables reported across studies. Statistical heterogeneity was assessed using the I2 statistic, interpreted as follows: 0% to 30%: low heterogeneity, 30% to 60%: moderate heterogeneity, 60% to 90%: high heterogeneity, 90% to 100%: very high heterogeneity.
Results
General Overview of the Search Results
PubMed search with filters for randomized controlled trials, meta-analyses, and systematic reviews yielded 65 results. After title screening (excluding 37 irrelevant and 1 non-English article, removing 1 duplicate), abstract review (excluding 12 articles), and full-text evaluation (excluding 5 articles), 9 eligible studies remained. Three additional relevant articles identified within reviewed studies were included, totaling 12 studies from PubMed. DOAJ search yielded 87 results. After removing 11 duplicates and 4 non-English articles, title screening excluded 47 irrelevant articles, abstract screening excluded 18, and full-text review excluded 7 articles, resulting in 0 eligible studies from DOAJ. The study selection process is illustrated using a PRISMA flow diagram Figure 1.
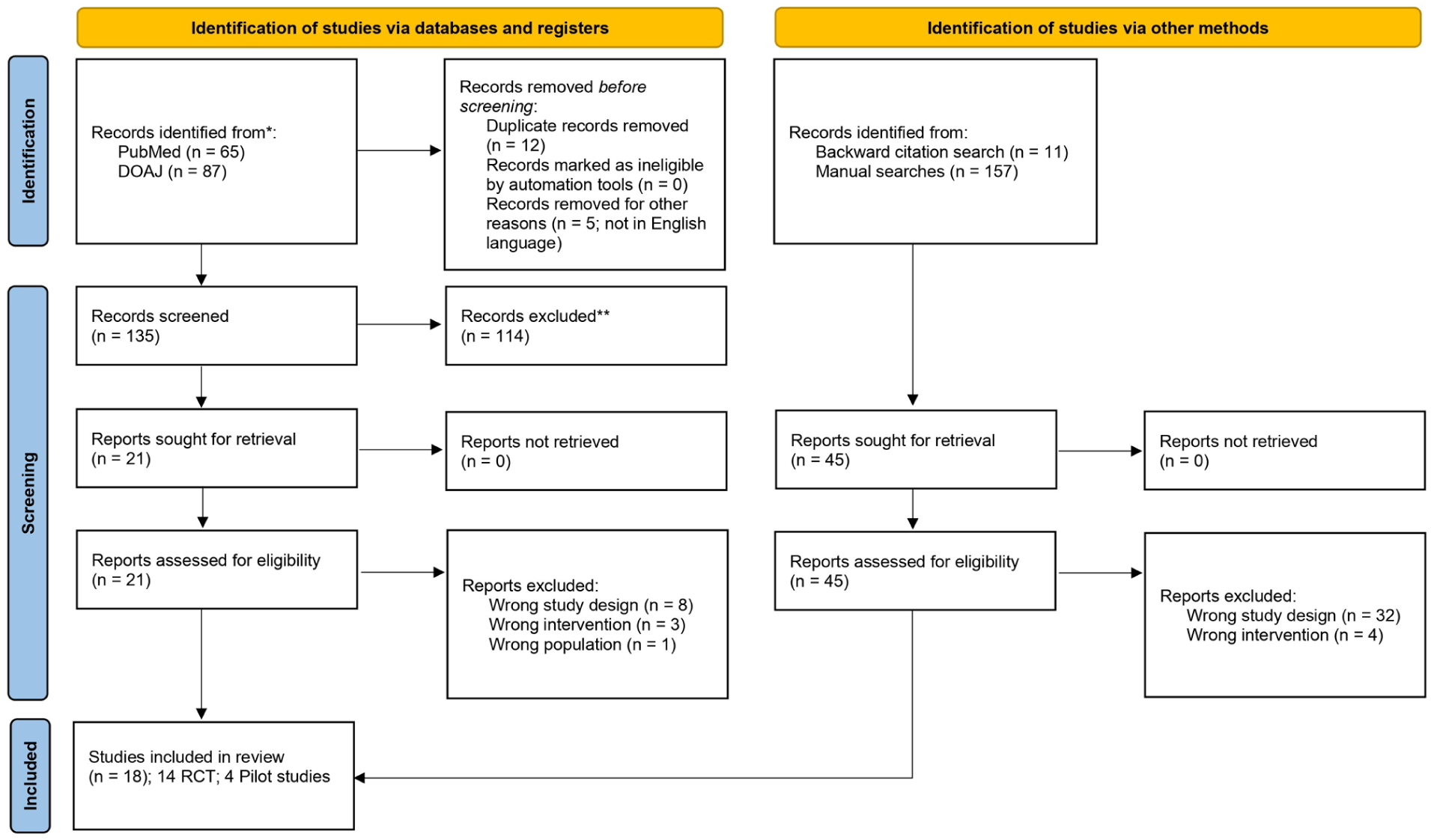
PRISMA flowchart.
Patient demographics
Eighteen RCT studies (4 pilot studies) were included in the review, of which 10 were selected for meta-analysis based on outcome comparability. A total of 1205 participants were included across the studies analyzed. Based on the available data, most participants were women (>90%), reflecting the dominance of breast cancer populations (three studies included any cancer type36-38). Regarding cancer status, about half of the studies involved participants receiving active treatment (such as chemotherapy, radiotherapy, or hormone therapy), while the other half was focused on cancer survivors in the post-treatment phase. Exact proportions vary due to inconsistent reporting across studies. Regarding disease stage, most studies included participants with early to moderate stages of cancer (stage 0-3), with only a few including individuals with advanced disease (stage 4). In many studies, staging information was not explicitly reported, which limits accurate quantification.
Interventions
The included studies used various dance styles, which can be grouped into several categories. Commonly used were structured cultural dance forms, such as traditional Greek dance, Latin dances, and culturally specific group dances like Guang Chang Wu, usually performed in groups with moderate intensity and increasing complexity. Partner dances, including adapted tango and ballroom styles (e.g., waltz, foxtrot, cha-cha), were also included, often emphasizing coordination, balance, and social interaction. Other methods included creative, improvised dances, combining dance with elements of exercise like Pilates, or focusing on rhythm, flexibility, and coordination through music-driven movements. The majority of studies implemented DMT (Dance Movement Therapy) as an intervention,39-42 followed closely by belly dance.3,43-45 Interventions lasted an average of 13 weeks (range: 3-24 weeks), were conducted an average of 2 times per week (range: 1-5 times weekly), and individual sessions lasted an average of 64 minutes (range: 30-180 minutes). Studies measured diverse outcomes across three health domains: physical (grip strength, blood pressure, 6-minute walk, pain, fatigue), mental (depression, stress, anxiety, anger, cognition), and social (support, relationships, life satisfaction, sexual function). Most studies assessed multiple domains, reflecting a holistic approach. Control group varied widely across the included studies. In some trials, participants in the control group continued their usual daily activities or received standard care without any structured physical intervention. Other studies included control conditions that involved educational or counseling programs covering topics such as cancer management, nutrition, physical activity, and self-care. Some studies used active control groups that included different forms of exercise, such as home-based rehabilitation programs, balance and strength training, Pilates, or mind-body interventions such as Qigong or Tai Chi. Additionally, several trials employed delayed-intervention (wait-list) control designs, where participants received no intervention during the study but were offered participation afterward.
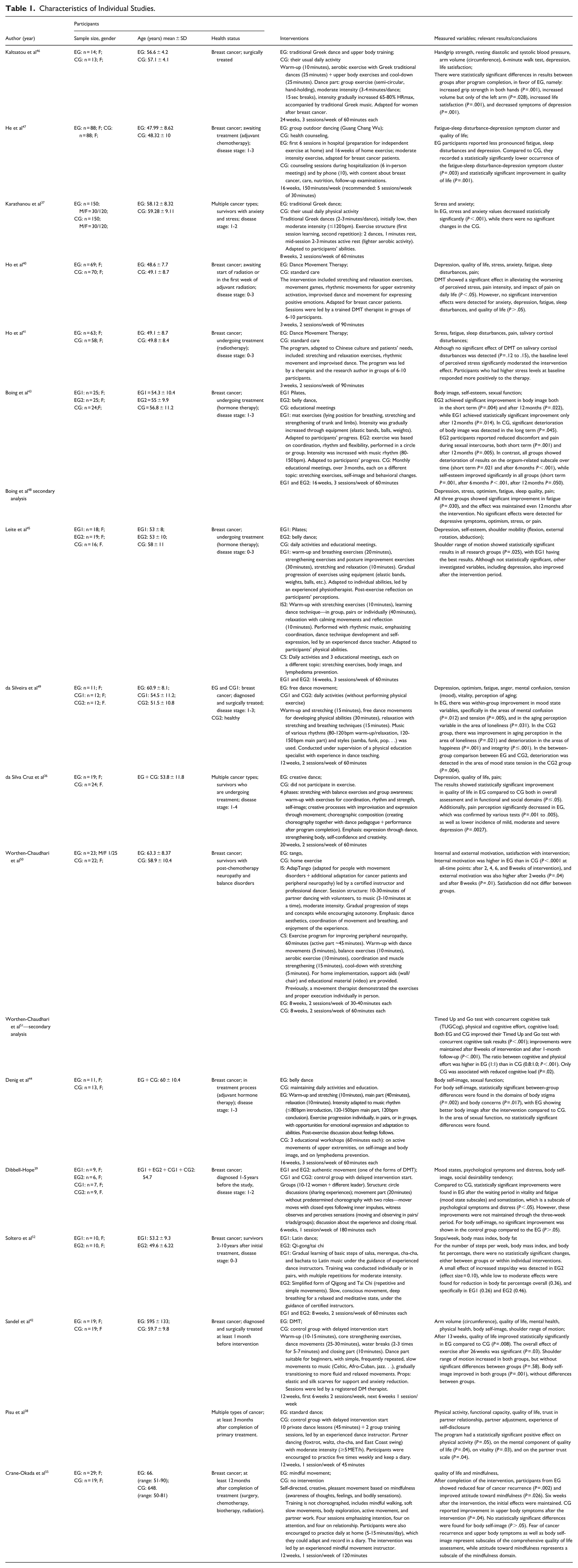
Details are in Table 1.
Characteristics of Individual Studies.
Assessment of Study Quality
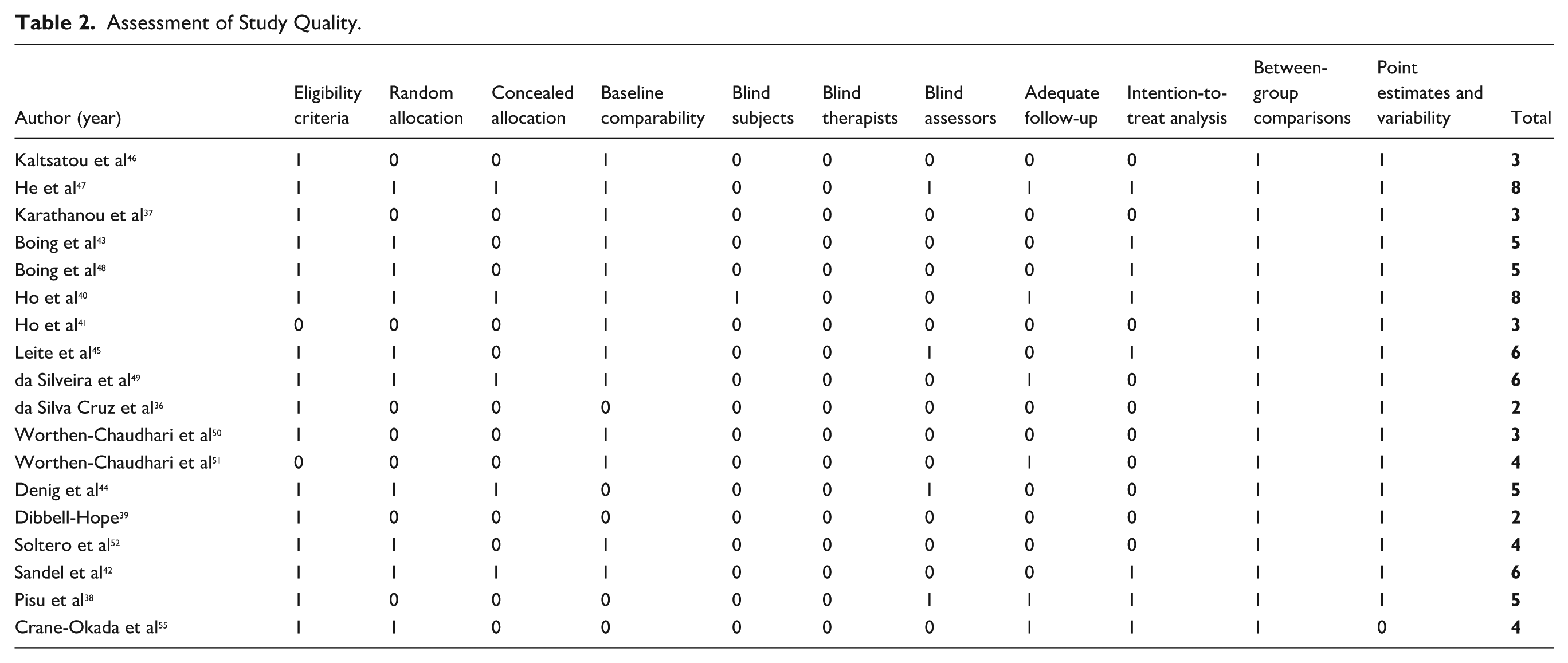
Using the PEDro scale, we assessed study quality and found no studies met criteria for high quality rating. Five studies were classified as moderate quality, seven as low quality, and six as very low quality, with an average score of 4.6, indicating low overall quality. Studies scored highest on “between-group comparisons” and “difference and variability estimates,” but most lacked blinding. Blinding of assessors was commonly reported, which is expected given the nature of dance interventions, as participant and therapist blinding is often unfeasible. Major limitations included inadequate allocation concealment and high participant attrition. Detailed data are presented in Table 2.
Assessment of Study Quality.
Meta-Analysis
Meta-analyses on quality of life variables are shown in Figure 2. Four studies examining the effect of dance therapy on general quality of life in cancer patients were included in the meta-analysis, with higher values indicating better quality of life. Results showed a statistically significant positive effect of dance therapy compared to control conditions (standardized mean difference = 0.97; 95% CI: [0.30, 1.63]; P = .005). Although effects across studies were predominantly in favor of the experimental group, heterogeneity was high (I2 = 88%), indicating substantial differences between studies. The largest effects were observed in studies by da Silva Cruz et al 36 and Sandel et al. 42 The quality of evidence was rated as very low.
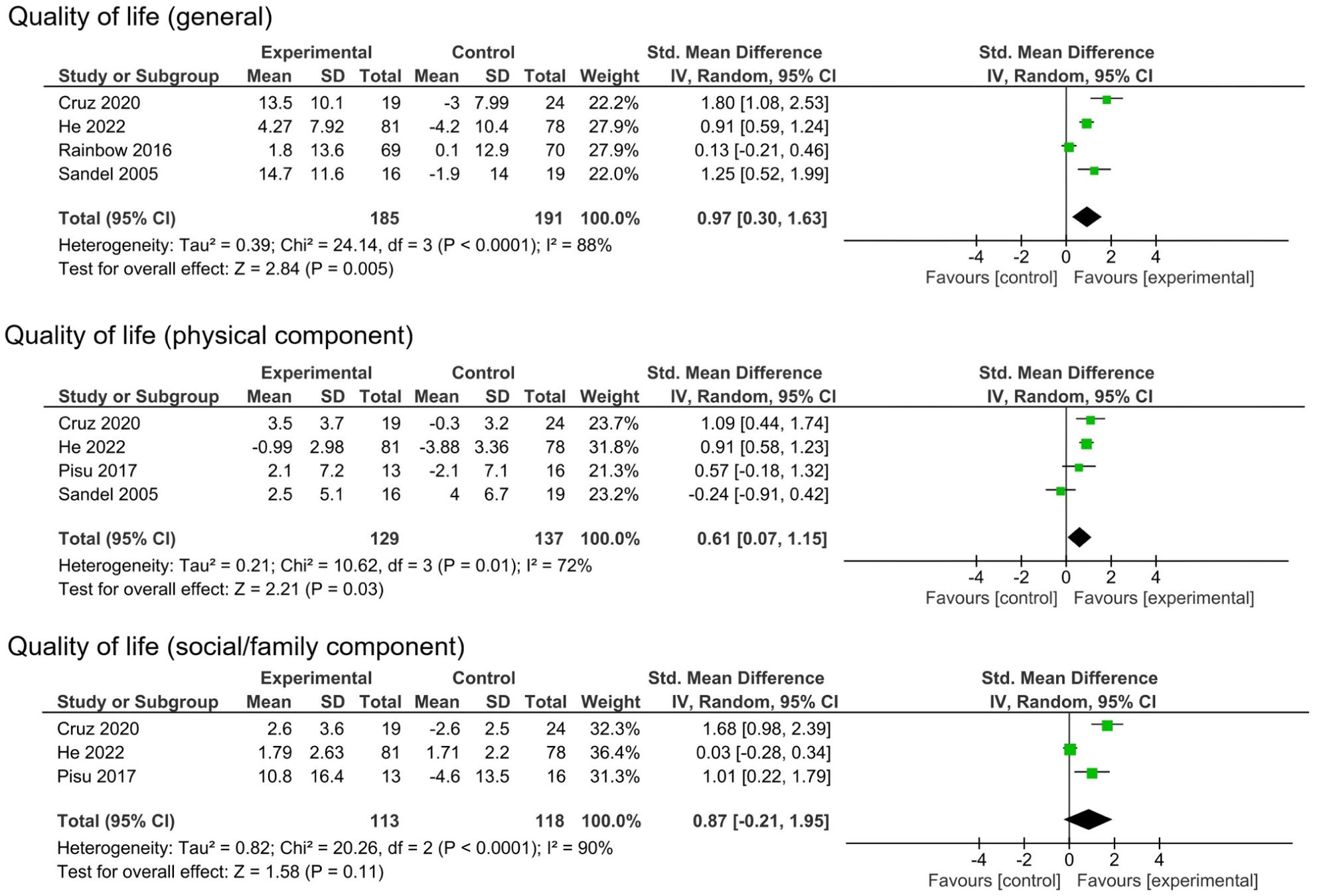
Meta-analyses (forest plots) for quality of life outcomes.
An additional meta-analysis included four studies evaluating the impact of dance therapy on the physical component of quality of life in cancer patients. Results showed a statistically significant positive effect favoring the experimental group (standardized mean difference = 0.61; 95% CI: [0.07, 1.15]; P = .03), indicating that the physical component of quality of life was higher after dance therapy compared to the control group. Heterogeneity between studies was high (I2 = 72%), suggesting substantial variability among individual study results. All but one study 42 reported effects favoring the experimental group, with the largest effects observed in studies by da Silva Cruz et al 36 and He et al. 47 The quality of evidence was rated as very low.
The final meta-analysis regarding quality of life included three studies evaluating the impact of dance therapy on the social/family component of quality of life in cancer patients. Overall analysis showed a positive trend favoring the experimental group; however, the effect did not reach statistical significance (standardized mean difference = 0.87; 95% CI: [−0.21, 1.95]; P = .11). Heterogeneity was high (I2 = 90%), indicating substantial differences in results among individual studies. The largest effect was observed in the study by da Silva Cruz et al, 36 while He et al 47 and Pisu et al 38 showed smaller or moderate effects, with He et al 47 results not reaching statistical significance. The quality of evidence was rated as very low.
Depression and stress
Meta-analyses on depression and stress are shown in Figure 3. Meta-analysis on stress showed that the intervention had no statistically significant impact (standardized mean difference = −0.17; 95% CI: [−0.51, 0.17]; P = .34). Analysis revealed low heterogeneity between studies (I2 = 27%), indicating consistency among included studies. Based on these results, no reliable conclusion can be drawn about the intervention’s effect on reducing depression, although all but one study 40 suggested modest improvement. The quality of evidence was rated as low.
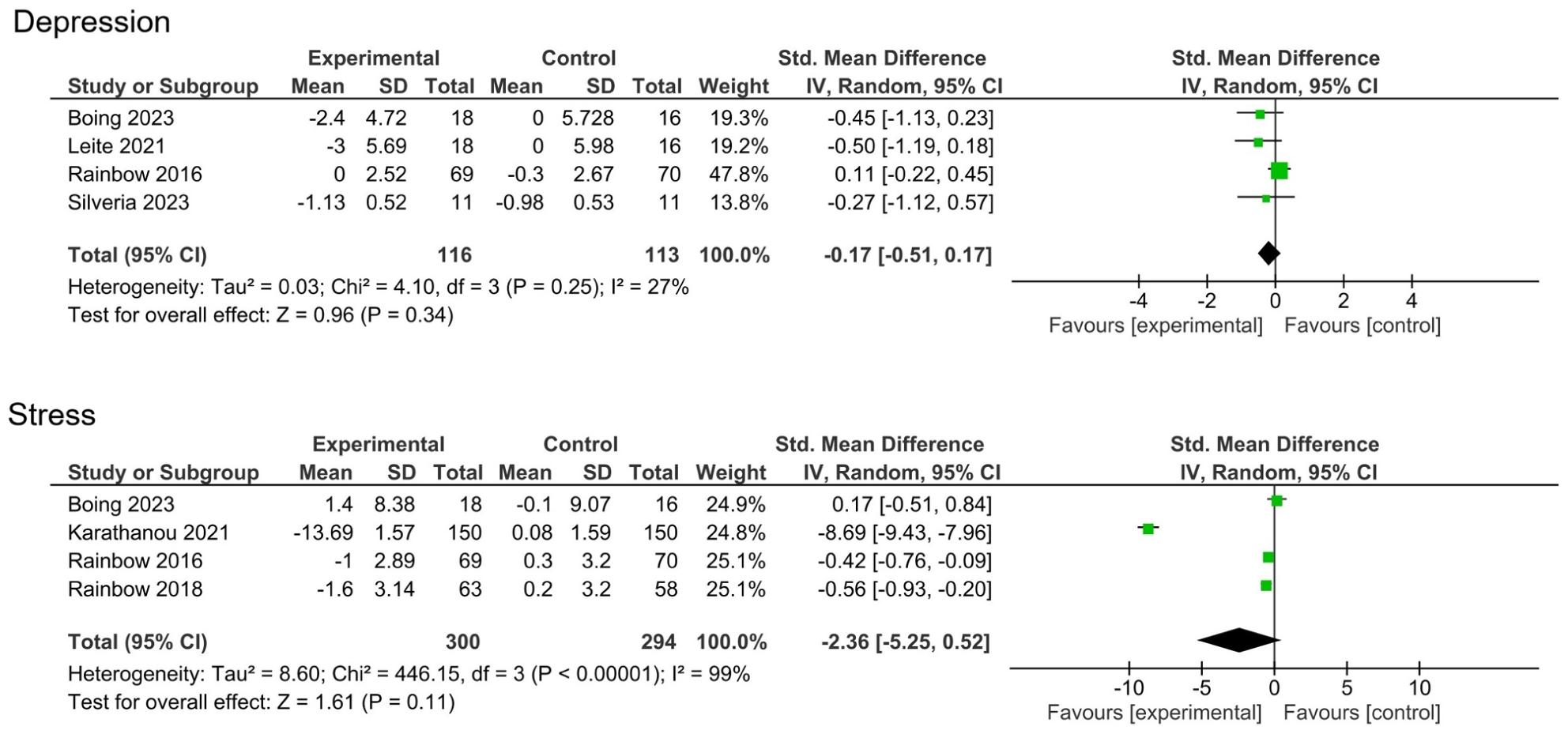
Meta-analyses (forest plots) for depression and stress outcomes.
Four studies examining the effect of dance therapy on stress in cancer patients were included in the final meta-analysis. Overall analysis showed no statistically significant effect (standardized mean difference = −2.36; 95% CI: [−5.25, 0.52]; P = .11), meaning that based on these data, no reliable conclusion can be drawn about the effectiveness of the intervention. Extremely high heterogeneity was detected among included studies (I2 = 99%), indicating substantial differences in results and/or methodology of individual studies. One study 37 reported a very large effect favoring the experimental group (SMD = −8.69), while other studies showed either small negative effects (favoring control) or detected no effect. The quality of evidence was rated as very low.
Discussion
The purpose of this systematic review and meta-analysis was to synthesize current evidence on the effects of dance-based exercise on key health outcomes in individuals with cancer or a history of cancer. Across the included randomized controlled trials, dance interventions were applied in diverse clinical contexts, using a wide spectrum of modalities ranging from highly structured cultural dance forms to expressive dance/movement therapy. This variability reflects the broad conceptualization of dance within supportive oncology but also introduces substantial methodological heterogeneity that must be considered when interpreting the findings. Overall, the results indicate that dance exercise can improve selected dimensions of quality of life, particularly its physical component, while evidence for effects on psychological outcomes such as depression and stress remain inconclusive. These findings align with a growing body of literature suggesting that dance may serve as a feasible complementary intervention in cancer care; however, effect estimates in the present analysis were influenced by low methodological quality, inconsistent intervention protocols, and substantial between-study variability.
Meta-analysis results show that included studies demonstrated statistically significant positive effects on quality of life in cancer patients following dance intervention compared to control groups. Similarly, other systematic reviews28,32,53 found positive effects of dance interventions on patient quality of life. Nelson et al 32 and Koch et al 53 report statistically significant improvements, while Fatkulina et al 28 note quality of life improvements without meta-analysis. Conversely, Abu-Odah et al 29 found no statistically significant differences, though their meta-analysis included only two DMT intervention studies. An important methodological limitation of our analysis is the inclusion of highly diverse dance interventions—from oriental dance3,43,45 to DMT40,42 and traditional Greek dance. 37 Koch et al 54 emphasize that different dance intervention types may have different mechanisms of action and efficacy. Largest effects were shown in studies by da Silva Cruz et al 36 and Sandel et al, 42 while the smallest effect was recorded in Ho et al, 40 which lasted only 3 weeks. Clinical significance concerns arise from high heterogeneity (I2 = 88%) despite statistical significance (P = .005), complicating result generalization. 30 Critical quality assessment shows an average score of 4.6/10 on the PEDro scale, indicating low evidence quality. Bradt et al 30 similarly warn that low study quality limits conclusion reliability. Additional analyses demonstrate statistically significant effects on the physical component of quality of life, while the social/family component did not reach statistical significance. Studies not included in meta-analysis also show improvements in specific quality of life aspects.38,55 Based on the above, hypothesis 1 is confirmed, though with limitations of low evidence quality and high heterogeneity among studies. Most results indicate a positive association between dance exercise and improved quality of life in cancer patients.
Meta-analysis results did not show a statistically significant effect of dance interventions on reducing depression in cancer patients, although individual studies suggested modest improvements. Analysis revealed low heterogeneity among studies, indicating consistency of results. Bradt et al 30 report similar findings, determining that DMT had no effect on depression in breast cancer women. Our results differ from Nelson et al, 32 who found that dance intervention significantly contributes to reducing depression in cancer patients; however, they excluded DMT intervention studies, which may explain the differences. Koch et al 53 found that DMT and other dance interventions positively affect depression, though their study did not examine only cancer patients. Koch et al 54 further analyzed intervention type effects and concluded that DMT is more effective at reducing depression than other forms of dance exercise. Abu-Odah et al 29 demonstrate that dance-movement interventions showed statistically significant positive effects on depression in cancer patients. It is important to note that low heterogeneity (I2 = 27%) in our meta-analysis indicates consistency of results among studies, differing from Koch et al 54 findings. A possible explanation is that our analysis predominantly included structured dance exercises, while DMT was represented by only one study. 40 Studies not included in meta-analysis showed improvements. Kaltsatou et al, 46 da Silva Cruz et al, 36 and Björneklett et al 56 report statistically significant reductions in depression symptoms, while He et al 47 note less pronounced depression. Fatkulina et al 28 in reviewing dance intervention effects on breast cancer patients also found positive effects on depression. Results among studies are inconsistent, and intervention effects are likely dependent on numerous factors such as dance intervention type, duration, exercise frequency, and study quality and design. Based on the above, hypothesis 2: “Dance contributes to reducing depression” cannot be confirmed.
The results of this meta-analysis did not show a statistically significant effect of dance interventions on stress in individuals with cancer, meaning that we cannot reliably confirm their effectiveness. Similarly, Bradt et al, 30 in their study focusing on dance/movement therapy (DMT), also found no evidence of stress reduction. A major concern is the extremely high heterogeneity among the included studies (I2 = 99%), which calls into question the validity of synthesizing their results. Christopher et al 57 reported similar issues in their meta-analysis on the effects of DMT on stress. Such high heterogeneity may suggest that different dance interventions operate through distinct mechanisms, making it difficult to draw unified conclusions. Our findings further show that one study 37 demonstrated a considerably stronger effect on stress reduction compared to the others, which showed small40,41 or no effects. 48 A likely reason is the specific sample selection in that study, which included only patients with elevated anxiety and stress at baseline. Ho et al 41 likewise report that higher initial stress levels predict a better response to the intervention. Based on the overall evidence, the hypothesis that dance exercise reduces stress must be rejected. Nevertheless, some individual studies indicate potentially beneficial effects,37,40,41 as supported by narrative literature reviews.28,29 It is possible that dance does not directly reduce stress levels but rather supports more effective coping, as suggested by the exploratory study by Quiroga Murcia et al. 58
Analysis of included studies reveals fundamental differences in dance intervention components that may explain high heterogeneity. The review demonstrates diversity of dance styles, from psychotherapy-oriented DMT40,42 through structured cultural dances37,52 to free creative movement.36,49 Koch et al 54 emphasize that different styles operate through different mechanisms—DMT through emotional expression, while structured dances operate through physical activity and social interaction. Studies used tempos ranging from 80 to 150 beats per minute. Fong Yan et al 59 emphasize that music tempo directly affects physiological response. Studies also differed in exercise structure—duration from 30 47 to 180 minutes, 39 frequency from once weekly 50 to five times weekly, 38 total duration from 3 40 to 24 weeks. 46 Different types of instructors represent an additional heterogeneity dimension—certified DMT therapists,40,42 professional dance instructors,37,45 or group exercises without dance partners. 43 Worthen-Chaudhari et al 51 used healthy volunteers as dance partners. Such heterogeneity makes existing meta-analyses methodologically problematic. Nelson et al 32 recognized this issue and excluded DMT studies, resulting in more consistent findings.
Practical and Clinical Applications and Implications
Dance-based exercise may be considered a feasible and acceptable complementary activity for individuals with cancer across different disease stages and treatment phases. From a clinical perspective, dance may serve as an alternative or adjunct to conventional exercise programs for patients who experience low motivation, limited adherence, or psychological barriers to traditional training modalities. Clinicians and rehabilitation professionals should note that the evidence most consistently supports improvements in the physical component of quality of life, while effects on depression and stress remain uncertain. Therefore, dance interventions should not be prescribed as a primary treatment for psychological distress but may support broader rehabilitation goals when integrated into multidisciplinary cancer care. Selection of dance modality, session intensity, and program duration should be individualized based on patient health status, treatment burden, and prior physical activity experience. For dance medicine practitioners and instructors, structured dance programs emphasizing moderate intensity, gradual progression, and adaptive movement appear most suitable for oncology populations. Interventions led by trained professionals familiar with cancer-related limitations may enhance safety and adherence. Group-based formats may offer additional social engagement, although current evidence does not allow firm conclusions regarding social or emotional outcomes. Given the low certainty of evidence and substantial heterogeneity among studies, current findings support cautious implementation rather than standardized prescription. Dance-based exercise may be recommended as an enjoyable and potentially beneficial complementary intervention, with clear communication to patients regarding the limited strength of evidence and the need for ongoing evaluation of individual responses.
Limitations
Several limitations should be considered when interpreting the findings of this review. First, the overall methodological quality of the included studies was low, as reflected by the PEDro scores, with no studies classified as high quality and frequent issues related to allocation concealment, blinding, and attrition. These limitations increase the risk of bias and reduce confidence in the estimated effects. Second, substantial heterogeneity was observed across studies in terms of participant characteristics (e.g., cancer type, stage, and treatment status), intervention design (e.g., type of dance, intensity, frequency, and duration), and outcome measures. This variability complicates direct comparisons between studies and limits the interpretability and generalizability of pooled estimates.
Third, the number of studies included in individual meta-analyses was relatively small, often based on only three to four trials per outcome. This reduces statistical power, increases the influence of individual studies, and contributes to imprecision in effect estimates, as reflected by wide confidence intervals. Fourth, outcome assessment was inconsistent across studies, particularly for psychological variables such as depression and stress, where different instruments with varying sensitivity and conceptual focus were used. This may have contributed to the lack of statistically significant findings despite positive trends observed in individual studies. Finally, the review was limited to randomized controlled trials, which strengthens internal validity but may have excluded relevant evidence from non-randomized or mixed-methods studies that could provide additional insight into the broader effects of dance interventions. In addition, variability and limited reporting of intervention details restricted the ability to identify specific components responsible for observed effects.
Conclusion
The aim of this paper was to determine through literature review and meta-analysis how dance affects cancer patients. Results show that dance exercise may positively affect quality of life in cancer patients; however, evidence is limited by low study quality and high heterogeneity. Although statistically significant improvements were observed in overall QoL, especially in its physical components, these changes might not directly lead to measurable reductions in specific psychological outcomes like depression and stress. Improvements in physical function, fatigue, and social engagement could indirectly support psychological well-being. However, such effects may require longer intervention periods or more targeted psychosocial elements to become apparent. Additionally, variability in measurement tools and the limited sensitivity of psychological assessments may have contributed to the lack of statistically significant results in these areas. Future studies must be larger, methodologically well-designed, and focused on specific types of dance interventions with adequate blinding and long-term follow-up. Until such research is conducted, dance exercise can be considered a potentially beneficial supplementary activity for cancer patients, though it cannot be recommended as proven therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study is a systematic review and meta-analysis of previously published studies. Ethical approval and review by an institutional review board were not required.
Data Availability Statement
Data supporting the findings of this study are derived from published articles included in the systematic review. Extracted data used for the meta-analyses are available from the corresponding author upon reasonable request.