
Abstract
Introduction:
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterised by motor impairments compromising daily functioning and quality of life. While pharmacological treatments primarily address motor symptoms, non-pharmacological therapies such as exercise, gained recognition for their potential in improving motor function and mobility. Among various forms of physical activities, dance positively influences motor functions in PD, according to study results. Assessing the feasibility and investigating whether an adapted slow waltz-based program could improve gait and balance in patients with PD have been the main aims of this study.
Methods:
Twelve subjects (age 72 ± 9 years; MMSE score ≥24; H&Y stages 1-4; ability to stand unaided) were involved in the project. Participants attended eight sessions of slow waltz combined with basic technical exercises performed at home for 8 weeks. Assessments were conducted at the beginning (T0) and after the end of the program (T1) using Body Sway Test, Gait Analysis, Stepping in Place and Timed Up and Go (TUG) Tests.
Results:
Data have been compared using Wilcoxon test on 9 out of 12 participants. It appears, from collected data, that Mean distance A/P, Mean distance M/L and Area in Body Sway Test with opened feet had improved during the 8 weeks. The same trend was observed with Closed feet. An enhancement in Stride time, Cadence and Velocity, has been highlighted through the Parameters of Gait Analysis, while Stride length appears significantly decreased. The Stepping in Place Test demonstrated significant improvements in A/P Displacement, along with improvements in R/L displacement and Area. The reduced task completion time and the increased score in the assessment of biomechanical strategies tool in the TUG, pointed out a significant positive shift in performance.
Conclusions:
First data analysis shows a highly encouraging potential, indicating that a slow waltz-based program can improve gait and balance in patients with PD.
Key Points
Slow waltz and its distinctive rhythm, rich in vertical movements, may offer unique motor benefits for people with PD; largely unexplored in previous research, slow waltz provided an original focus for this study.
Waltz intervention led to significant improvements in postural control, functional mobility and biomechanical strategies.
Strong motivation standards brought forward a high attendance and permanent adherence to home exercises and dance lessons, demonstrating feasibility and acceptability of a structured slow waltz intervention in individuals with PD.
Introduction
Parkinson’s disease (PD) is described as a complex and common neurodegenerative disorder characterised by significant degeneration of dopaminergic neurons in the substantia nigra, leading to impaired initiation and regulation of voluntary movements. The exact cause of this disorder, akin to many others, remains unclear. However, it is generally considered to be multifactorial, involving a complex interplay of genetic, biological, environmental and age-related factors. 1
Clinically, PD is classified as a movement disorder and it is primarily characterised by resting tremor, rigidity, bradykinesia and postural and gait impairments, which significantly compromise functional capacity and reduce the individual’s level of autonomy. Furthermore, with the progressive development of the disease, a wide range of non-motor symptoms frequently co-occur, contributing to the overall disease burden. 2 Being a chronic disease, PD influences every aspect of life in any individual affected by the disorder, weighting on general well-being and satisfaction of the patients. Treatment currently focuses on alleviating symptoms, delaying motor complications and extending the patient’s autonomy as long as possible, as no definite cure has yet been provided. 1
Physical exercise has been widely proposed as an effective intervention to be taken into consideration in treating various chronic conditions, demonstrating significant benefits across multiple health parameters. Advantages in physical fitness, cognitive functioning and mind-body connection have been proved, as well as positive enhancements in neurogenesis and in neuroprotection. 3 Exercise protocols incorporating gait training, balance exercises and muscle strengthening have shown significant improvements in patient’s physical capacity and are considered both safe and effective. 3
A certain amount of systematic reviews have highlighted the positive effects of physical exercise in PD, reporting improvements in balance, gait, motor skills, mobility, cardiorespiratory endurance and overall quality of life. 3 Among the various modalities, dance-based interventions have shown particularly strong efficacy in improving motor symptoms.4 -6 Compared to other forms of exercise, dance uniquely integrates rhythmic movement, cognitive engagement and social interaction, 7 all of which support motor coordination, movement fluidity and neuroplasticity. 4 Several studies have also confirmed significant improvements in balance, functional mobility and motor symptom severity, with particularly promising results coming from practice of Argentine tango and other styles, characterised by upright and continuous movements. 8 Beyond general gait enhancements, dance was also found to positively influence specific aspects such as gait symmetry and cognitive motor integration. 9 Additional studies reported clinically meaningful reductions in motor symptom severity and gains in balance and functional mobility.10,11 The benefits of dance extend beyond short-term improvements. Longitudinal data indicated a slower progression of both motor and non-motor symptoms in dancers with an history of regular dance practice over a 3-year period, compared to non-dancers; 12 moreover, dancers consistently outperformed non-dancers in terms of balance and motor severity. 13 Multimodal approaches have yielded further improvements in postural control, functional mobility and gait parameters.14,15 Interventions modelled on Dance for PD framework have demonstrated motor related benefits, particularly in functional mobility. 16 Less commonly studied approaches, such as Garba and Biodanza®, have also shown therapeutic potential, suggesting that benefits may not be limited to specific genres, but emerge from a combination of rhythmic movement, structured repetitions and sensory engagement.17,18 These features appear to stimulate adaptive responses that promote postural control, gait fluidity and balance regulation.
Collectively, this body of evidence reinforces the role of dance as a multimodal and adaptable intervention, capable of managing the different motor challenges associated with PD. For this reason, the present study aims to further investigate its potential. Slow waltz has been chosen as a dance style not sufficiently examined in previous literature.
Therefore, the primary aim of this study was to evaluate the feasibility of a slow waltz-based intervention in people with PD, while the secondary aim was to explore whether its specific characteristics could lead to improvements in gait and balance.
Methods
Experimental Design
A single-arm within-individual pilot study was conducted from October to December 2024. Recruitment took place from July to September, following specific inclusion criteria. All participants were asked to express their informed consent in written form before the beginning of data collection. No important changes to the study methods, eligibility criteria, or pilot trial assessments and measurements were made after trial commencement. This was conducted using four laboratory-based tests in October followed by the actual intervention, performed from October to December. Participants attended 1-hour waltz sessions every Friday morning for 8 weeks. Additionally, they were asked to perform basic technical exercises at home, at least twice a week, keeping an activity diary to verify the completion of the different activities. Final data were collected in December by repeating the same laboratory tests previously administered. Data analysis was subsequently performed to evaluate the effects of the waltz intervention on gait and balance in the participants. The pilot trial was completed according to the study protocol following the planned 8-week intervention period.
The timeline illustrating the steps of the experimental procedures is presented in Figure 1.
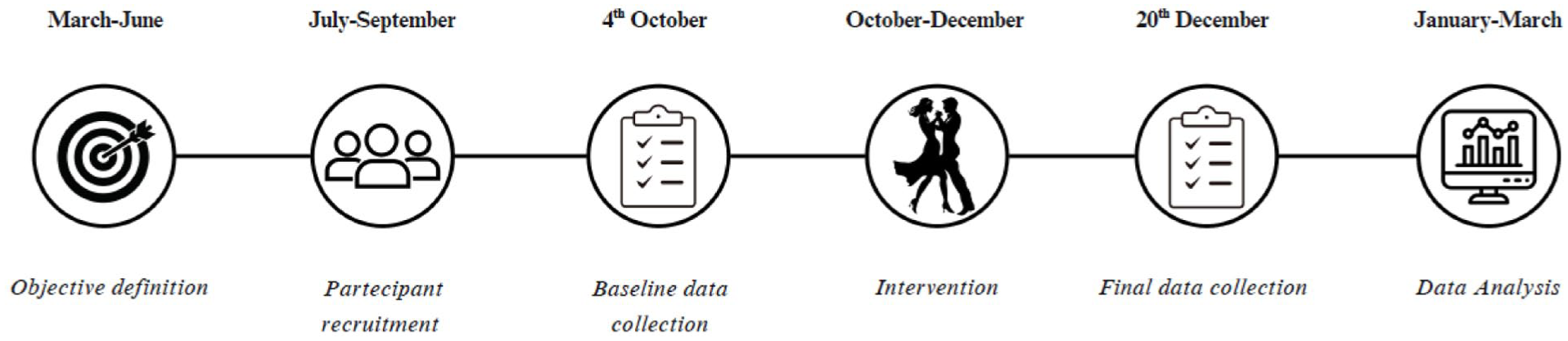
Timeline of the experimental design.
Participants
Inclusion criteria included a clinical diagnosis of PD with a disease severity rating from stage 1 to 4 on the Hoehn and Yahr (H&Y); an age of 50 to 85 years; a Mini Mental State Examination (MMSE) score ≥24. Individuals unable to stand independently and those with serious medical conditions which precluded dancing or could be worsened by exercise were excluded.
Initial recruitment provided a group of twenty participants with balanced sex distribution (10 males, 10 females), recruited by the non-profit organization Moov-it through their contact network. Eight participants were excluded (5 males, 3 females) after applying inclusion criteria, while three additional participants dropped out during the intervention (2 males, 1 female). The final sample, therefore, consisted of nine participants (3 males, 6 females). As an association, Moov-it organizes physical adapted activities for individuals experiencing physical impairments related to chronic degenerative diseases, especially those of neurological origin, with special attention to PD. People included in the final sample are all residents in Lombardy, and became aware of the project through promotional flyers explaining the nature of the intervention and all the details regarding location and schedule. All participants were requested to give written informed consent for the assessment and intervention. The present pilot trial was conducted and reported according to the CONSORT 2010 extension for randomized pilot and feasibility trials (Supplemental Material). The study flow diagram is presented in Figure 2.
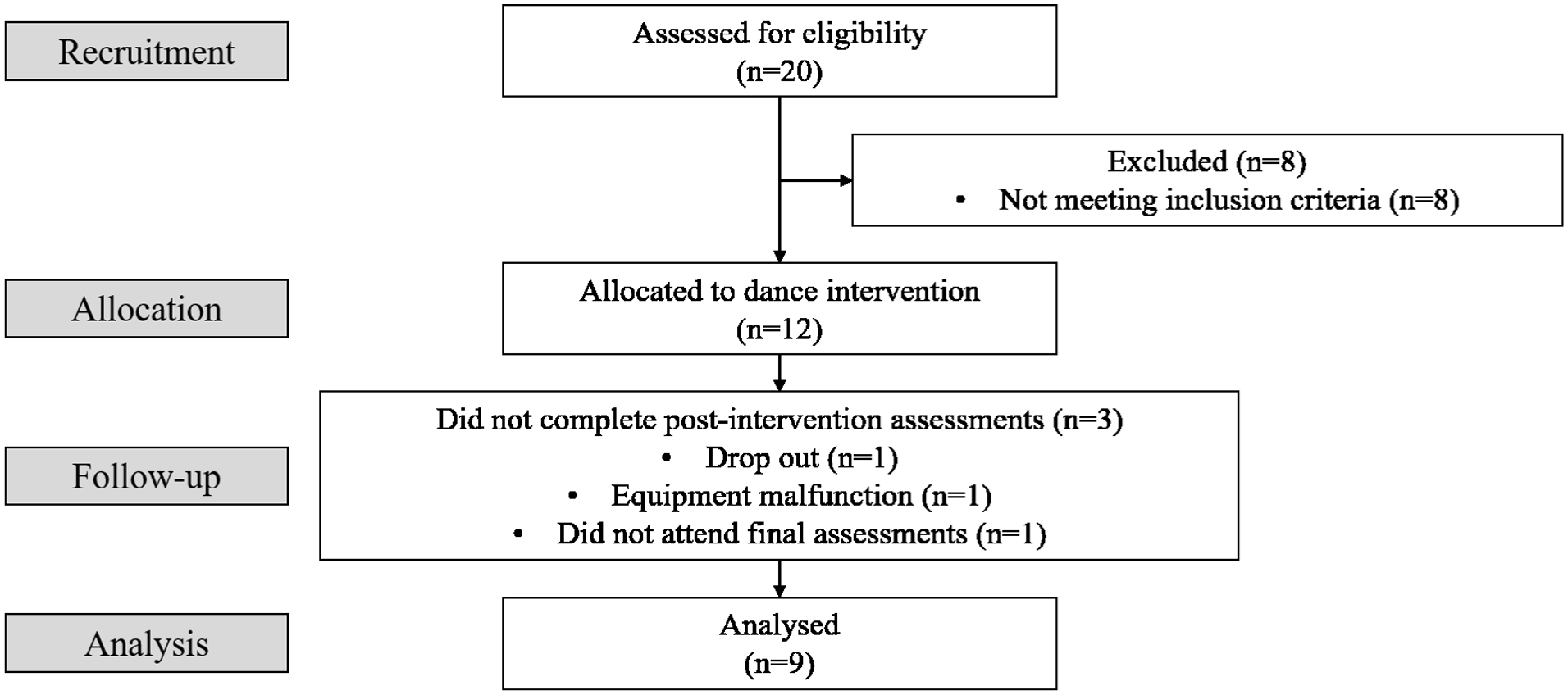
CONSORT (Consolidated Standards of Reporting Trials), flow diagram.
Experimental Procedures
All chosen tests for the evaluation of patients were performed with the support of laboratory instruments: Gyko (Microgate, Italy), a 3D inertial sensor measuring linear acceleration, angular velocity and magnetic field; and Optogait (Microgate, Italy), an optical system that detects movement-related events (eg, contact and flight times) by monitoring interruptions in infrared signals between LED bars.
Testing protocol
Two kinesiologists with strong expertise in adapted physical activity conducted the assessment of participants in the week before starting the intervention and at the end of it in a dedicated room at a dance school in Milan. The testing protocol consisted of the following outlined tests.
Body sway test
This is a static test designed to assess the subject’s stability and balance. The participant is requested to stand upright, barefoot and still with arms at the sides for 30 seconds. Two trials were performed: the first one with feet at hip-width and the second one with feet close together, 19 both were conducted using a Gyko, with an elastic belt placed at the level of the pelvis, which allowed real-time monitoring of the vertical projection of the body’s centre of mass on the ground, providing information on postural control.
Stepping in place test
This is a dynamic test that required the participant to step in place for 1 minute (without standardising knee height) within the area defined by the operator, while wearing a Gyko placed in the subscapular region which provided accurate information on stability and coordination of the upper body. Otte administered the test for 40 seconds to prevent exhaustion, 20 but we considered an extended duration up to 1 minute, in order to ensure a more stable and representative dataset, while maintaining an appropriate level of effort for the participants.
Gait analysis overground
This is a dynamic test designed to assess gait parameters on the ground, using the Optogait system. The established protocol involves a 4-meter Optogait corridor, preceded by 1-meter acceleration zone and followed by 1-meter deceleration zone. This setup aligns with previous research, utilising a 10-meter corridor but analysing only the central 4 meters across three trials. 19 The two Optogait bars are set in a parallel configuration, 6 meters apart. Participants were asked to walk along the corridor three times, so that a total of 12 meters would be taken into consideration by the Optogait system. The representation of the setting prepared for this test is shown in Figure 3.
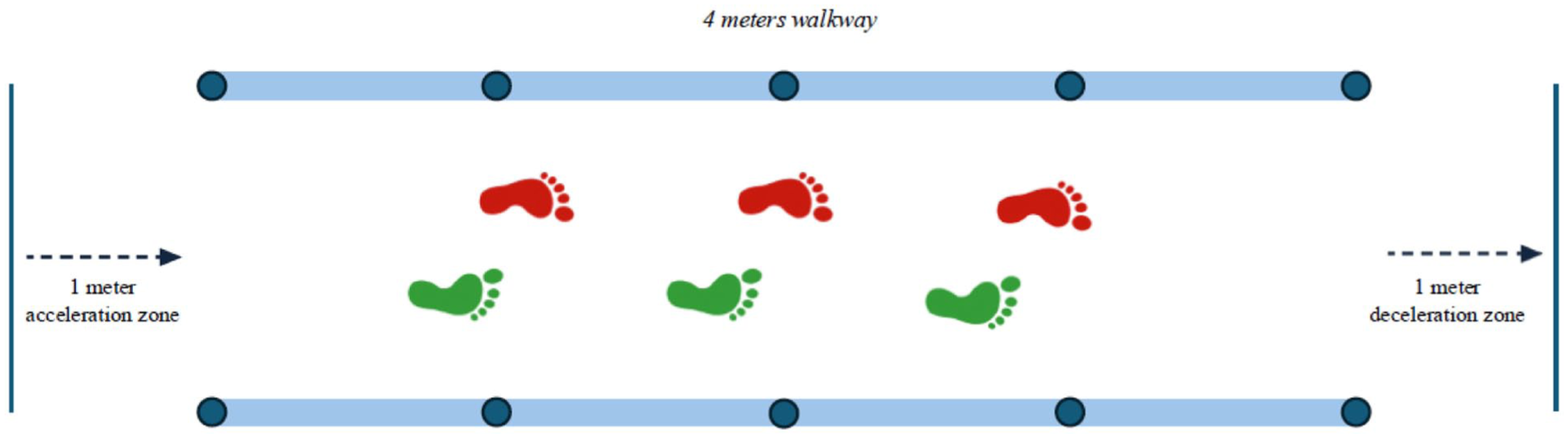
Schematic representation of the setting planned for the overground gait assessment.
Timed up and go test
This test was carried out following the protocol recommended by Podsiadlo and Richardson 21 and measures, in seconds, the time taken by an individual to stand up from a standard chair (approximately 46 cm in height), walk for 3 meters, turn around a cone, return to the chair and sit down again. The participant was asked to wear normal footwear, and no physical assistance was provided. Participants began with their back against the chair and arms resting on the armrests. Following a ‘go,’ the patient had to stand up and perform the described track. The test included a familiarisation trial before the evaluation. The test performances were video-recorded so that the operator could fill the observational grid Timed Up and Go – Assessment of Biomechanical Strategies (TUG-ABS). 22
Intervention
The participants attended a total of 8 slow waltz lessons held in a dedicated room at a dance school in Milan. The space had a rectangular parquet floor, with mirrors along one side, and chairs arranged around the perimeter, so that participants could sit during breaks. The classes were all delivered by a professional dancer with around 10 years of experience both as a competitive performer and as a teacher, and specific expertise in PD. The teaching techniques were the same used with non-PD waltz beginners. Each lesson lasted 1 hour, including 10 minutes of warm-up with basic technique and standard footwork exercises, followed by the execution of a routine consisting of 18 basic slow waltz steps. Slow waltz involves a complex motor task, characterised by many direction changes, combined with maintenance of the correct posture while listening to the music, and the ability to manage one’s body in relation to that of the partner. The participants first learned the steps individually, then reproduced them in pairs. If an even number of participants was not available, caregivers were invited to join as partners, ensuring that all participants could engage fully. The final aim of the project was to make participants dance in pairs with other couples on the dance floor, managing space and not clashing into each other.
In addition to the classes, participants were provided with weekly videos containing basic technical exercises to be performed at home during their free time, at least twice a week for 15 minutes without interruption. The focus was set on improving foot technique, balance and ankle mobility. The execution was monitored through the completion of an activity diary, which was distributed during the initial assessments and collected after the final assessments.
All assessments and intervention sessions were performed in the ON medication state. No changes in dopaminergic therapy occurred during the intervention period.
Data Analysis
Direct aim of this study was to collect quantitative and qualitative data from each test, and use the relevant data reports to create a database. In the Body Sway Test, the use of Gyko allowed the setup of the ‘Sway’ protocol for postural stability assessment, thus analysing a subject’s control capabilities and strategies. The parameters extracted were Area (mm2), Mean Distance Anterior/Posterior (A/P) (mm) and Mean Distance Medio/Lateral (M/L) (mm). Regarding the Stepping in Place Test, a Gyko was placed in the subscapular region of the patient with a vest, to collect data about dynamic posture. Gyko provides accurate information about the stability and coordination of the upper body, giving data about the kinematics of the torso in a synchronised way (step by step). The data selected were Area (cm2), A/P (cm) and Right/Left (R/L) (cm) displacements. Gait Analysis was carried out thanks to a modular system with a configuration including a 4-meter Optogait corridor. The data considered were Stride Time (s), Stride Length (cm), Velocity (m/s) and Cadence (steps/s). Timed Up and Go Test was the last assessment performed. This didn’t require any laboratory instrument other than a chair, a stopwatch and an observational grid.22,23 Data analysed in this test were Time (sec) and TUG-ABS score (. . ./45).
To perform statistical analysis StatView (version 5.0.1) was used. Data were expressed as median and interquartile range (IQR) and compared using Wilcoxon test to find their significance (P < .05). Effect sizes (η2) were calculated for the non-parametric analyses using the formula η2 = Z2/N derived from the standardised Wilcoxon test statistic and they were interpreted according to Cohen’s benchmarks, with 0.1 indicating a small effect, 0.3 a medium effect, and 0.5 a large effect. 24 95% confidence intervals (CI) were also reported.
Results
Nine subjects (3 men, 6 women, mean age 74 (10), H&Y 1.5 (1.1)) completed the study and all outcome measures were available for all participants.
Participant adherence was assessed considering the parameter of non-attendance/attendance to the eight live sessions, and evaluating the percentage of prescribed home exercises actually completed. All participants attended between six and eight dance sessions. According to their diaries, 78% of participants completed the home exercises at least twice weekly for 10/15 minutes per session, whereas 22% performed them once a week. None of them engaged in other forms of structured activity or independently performed home exercises, outside of those prescribed, for the entire duration of the study. Ancillary analyses therefore indicated good overall adherence to the intervention, with high compliance to both supervised and home-based components.
Baseline characteristics of the sample are presented in Table 1.
Baseline Characteristics. a
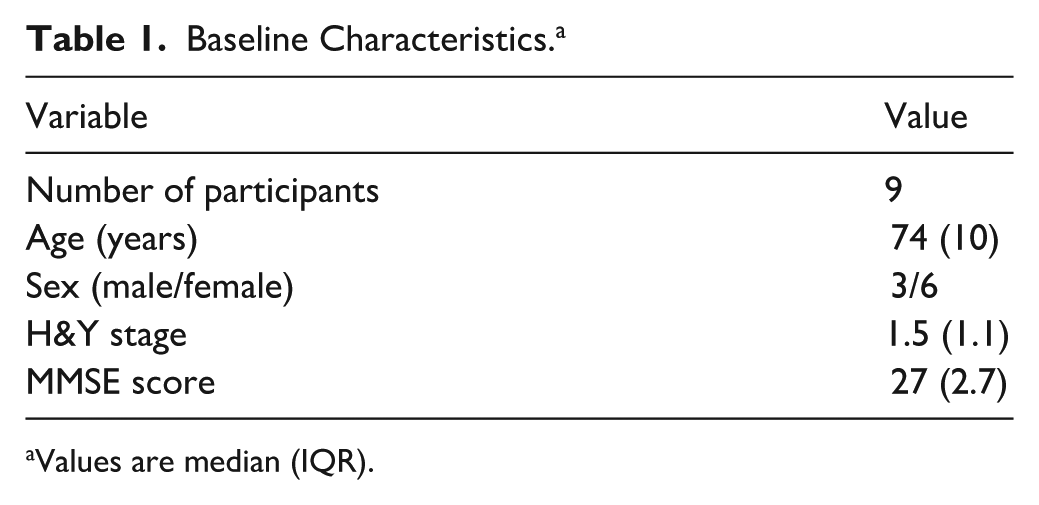
Values are median (IQR).
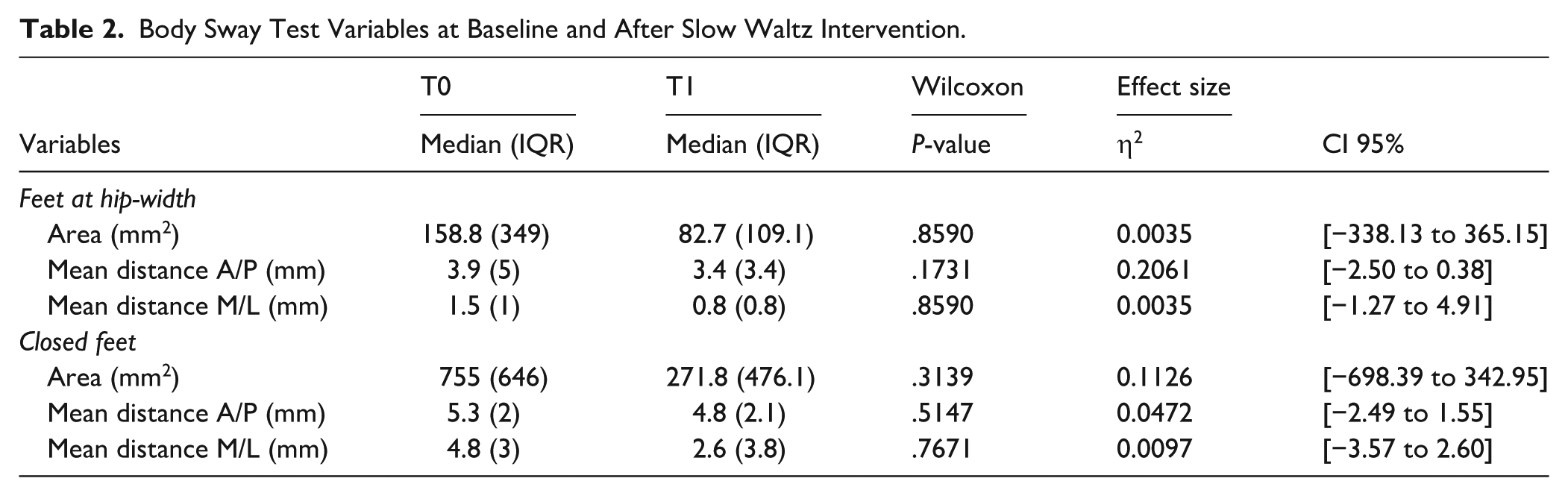
Following the slow waltz intervention, participants exhibited no significant improvements in postural control across all conditions of the Body Sway Test. With feet at hip-width, there was a reduction in Sway Area as well as in mean A/P and M/L distances. Similarly, when standing with closed feet, Sway Area decreased, while A/P and M/L distances also showed reductions. Table 2 presents the data of postural sway parameters before and after the slow waltz intervention.
Body Sway Test Variables at Baseline and After Slow Waltz Intervention.
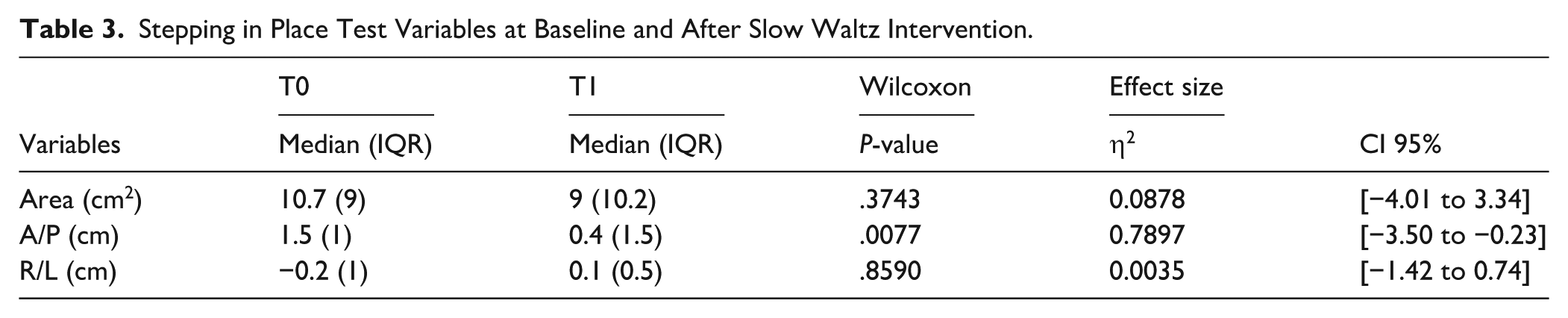
As shown in Table 3, all measured parameters in the Stepping in Place Test improved following the slow waltz intervention. A reduction in Sway Area was observed, accompanied by a statistically significant decrease in A/P displacement, showing a large effect size (P = .0077, η2 = 0.7897). Moreover, the R/L displacement had improved, shifting from a slight leftward tendency to a near symmetrical position.
Stepping in Place Test Variables at Baseline and After Slow Waltz Intervention.
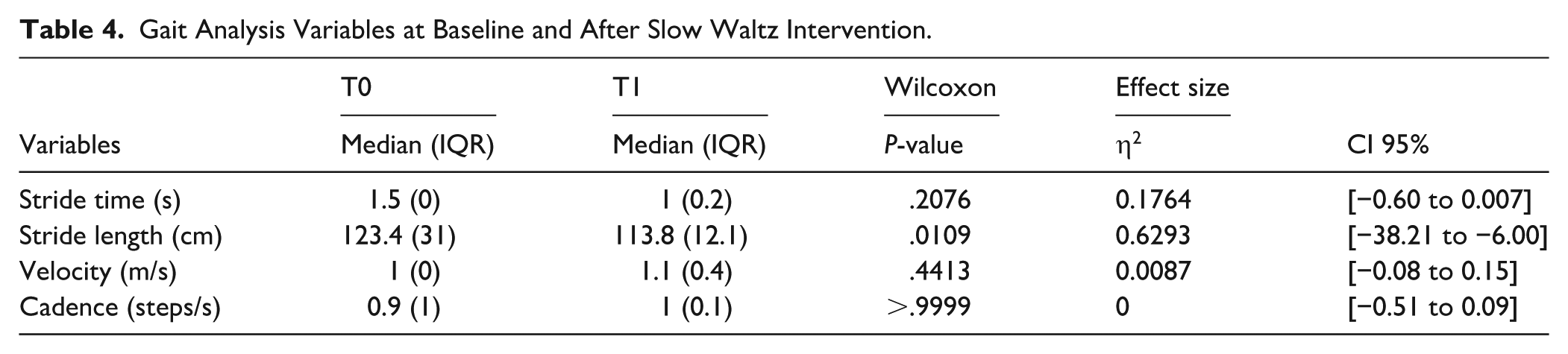
Regarding Gait Analysis, Stride Time decreased following the intervention, indicating a faster gait cycle. Conversely, the analysis revealed a statistically significant reduction in Stride Length accompanied by a large effect size (P = .0109, η2 = 0.6293), reflecting shorter steps. Gait Velocity showed a modest increase and Cadence improved as well; however, in the absence of reported P-values, these changes cannot be considered statistically relevant. These data are reported in Table 4.
Gait Analysis Variables at Baseline and After Slow Waltz Intervention.
As shown in Table 5, Time Up and Go Test highlighted significant improvements of large magnitude (P = .0051, η2 = 0.7897) in execution time, with participants completing the task more quickly compared to the baseline. Additionally, significant increases (P = .018, η2 = 0.5382) were found in the scores of the observational grid, indicating enhanced movement quality across all four sections (sit-to-stand, gait, turn, and stand-to-sit).
TUG Variables at Baseline and After Slow Waltz Intervention.

No adverse events occurred during the intervention period.
Discussion
The aim of the present study had been to assess the feasibility and to examine whether an adapted slow waltz-based program could help improve gait and balance in patients with PD. The study proved to be feasible both in terms of intervention and proposed assessments for people with PD. The major findings showed that dance-based intervention resulted in statistically significant changes across multiple gait and functional parameters. Notably, three out of four variables (A/P sway, task completion time and TUG-ABS score) underlined improvements from baseline (T0) to post-intervention (T1) while stride length statistically decreased.
Our sample consisted of nine participants. Although smaller than most samples reported in literature,9,14,15 this specific sample was highly homogeneous in terms of disease severity and cognitive integrity. Gender distribution was not perfectly balanced, as we encountered a higher proportion of women in the final sample, emerging after eligibility screening and participant dropout, despite an initially balanced recruitment. Being a pilot study, the primary aim was to assess the feasibility, safety, and preliminary efficacy of slow waltz training on gait parameters. In small pilot samples, even minimal differences in exclusion or attrition rates may substantially influence the final sex distribution, resulting in an uneven representation between men and women. Nevertheless, despite these gender differences and the small sample size, the population completing the study appears representative and methodologically consistent with the criteria used in the main reference studies.12,16
Clinical assessment in most studies was based exclusively on validated rating scales, with little to no adoption of technological instrumentation.11,13 When technology was implemented, it was invariably used alongside traditional clinical tools. 8 However, only a limited number of studies employed objective instrumental assessments, such as inertial sensors 9 or computerised posturography systems 15 to quantify motor features in patients with PD. The present study belongs to this minority, integrating wearable sensor technology and optical detention system to provide quantitative and reproducible measures of postural stability and gait performance. This approach offers enhanced sensitivity in detecting subtle motor impairments, complementing traditional clinical evaluation methods and contributing to a more comprehensive assessment framework.
Previous studies explored the effects of various dance genres and movement approaches on individuals with PD including contemporary dance, 15 Feldenkrais method, 14 Biodanza®, 18 Garba dance 17 and structured dance programs specifically designed for people with PD.9,12,16 In addition to these, some systematic reviews focused on the therapeutic potential of partner dances, particularly in improving balance, mobility and quality of life.8,11,13 Our study is to be considered within this context. While most of the previous research works examined the effects of Argentine tango, classic tango, or, less frequently, styles such as smooth waltz and foxtrot,8,11,13 our study specifically investigated the effects of slow waltz, a discipline belonging to the standard ballroom dance category. This choice aimed to further expand the understanding of how different partner-based dance modalities may influence motor and functional outcomes in PD. Slow waltz was selected as a standalone intervention, based on its feasibility and potential benefits: its structured rhythm and the nature of the motor tasks make it accessible, while at the same time it offers a level of challenge due to its unique motor demands. Unlike tango, where dancers typically maintain flat-footed contact with the floor and flexed knees, slow waltz incorporates a prominent elevation component, requiring dynamic foot and leg lifting movements. This vertical displacement may have a positive impact on balance control, particularly in individuals at higher risk of falls.
Compared to existing studies,8,12,14,16,18 our intervention was shorter in duration and involved fewer weekly sessions. This decision to adopt a relatively low frequency and dose of intervention was based on two main reasons. First of all, participants were asked not to engage in any additional physical activity outside the one prescribed by the experimental protocol. Secondly, given the pilot nature of the study, the aim was to investigate whether it would still be possible to observe significant improvements with a lower frequency and dose of intervention in comparison with those commonly reported in the dedicated literature. Another difference compared to other studies is the absence of a control group8,9 or comparison with groups engaged in other activities such as physiotherapy,10,15 which is still justified by the pilot nature of our study.
The observed reductions in A/P sway during the Stepping in Place Test and the decreased time to complete the TUG suggest enhanced dynamic balance and efficiency in motor execution, while the increase in TUG-ABS scores indicates improved biomechanical strategies and overall functional performance. These findings support the hypothesis that structured dance training can positively impact postural control and mobility, potentially by promoting multisensory integration, rhythmical coordination and movement precision. Significantly, the mean improvement in the TUG test (4.8 s) exceeded the lower bound of minimal detectable change (MDC) values reported in PD (3.5-11 s), 25 highlighting the clinical relevance of the observed functional gains. The reduction in stride length, observed in the present study, may reflect a potential adaptive gait strategy. Previous evidence has shown that backward margins of stability (MoS) can be increased by decreasing stride length, suggesting that shorter steps may contribute to enhanced dynamic stability. 26 Although MoS was not directly assessed in our study, the observed change in stride length could be interpreted as a stabilising adjustment.
The present study confirms recent findings on dance as an effective intervention for PD. In line with previous data,8,14,15 the intervention improved postural control, with reduced sway area and both A/P and M/L excursions. Improvements in the TUG test further support enhanced functional mobility and execution speed after rhythm-based movement interventions.8,11 Overall movement quality, assessed through an observational grid, also increased, consistent with evidence on the effects of rhythm and visually guided dance on upper motor symptoms. 10 Motor symmetry improved as well, with more balanced right-left distribution, reinforcing the hypothesis that dance promotes coordinated motor integration. 9
In addition to confirming existing evidence, this study represents one of the first systematic investigations into the effectiveness of slow waltz as a rehabilitative intervention in PD, a genre thus far underexplored compared to others such as tango or folk dance. 8 The distinctive features of the slow waltz, continuous and controlled movements, predictable rhythm and progressive changes in direction, appear to facilitate not only balance, but also a smoother and safer gait execution.
Strengths and Limits
This study explored the effects of a rarely investigated partner-based dance style. The chosen modality introduced novelty from a scientific perspective while offering participants an engaging and emotionally rewarding experience. The involvement of caregivers as partners when participant numbers were low, preserved the format and may have further enhanced the intervention by fostering shared moments between patients and caregivers. Another strength lies in the use of validated testing protocols combined with advanced technological tools to objectively assess motor performance.
Nonetheless, limitations must be acknowledged. The small sample size reduces generalisability and statistical power. Additionally, the low frequency of weekly sessions and the short duration may have constrained functional improvements. The intervention was complemented by home exercises, but since the participants were asked to self-report autonomous practice, their frequency, accuracy, and adherence could not be controlled, only estimated through self-reported diaries. This limited the ability to determine their precise contribution. Finally, the absence of a follow-up and control group reduces the solidity of the findings, preventing assessment of long-term sustainability or conclusive attribution of effects to the intervention.
Practical and clinical applications and implications
All participants attended most of the dance sessions and adhered well to the prescribed home exercises, indicating that the intervention is feasible and acceptable for people with PD. These findings suggest that structured dance programs can achieve high engagement and adherence in this population. While social, emotional, and relational outcomes were not formally assessed, the partnered nature of the activity may provide opportunities for interaction and enjoyment, which could be explored in future research. The results also support further investigation into integrating dance interventions to support rehabilitation pathways for people with PD, with potential benefits such as improved motor function and reduced fall risk. Overall, these findings should be interpreted as preliminary evidence to inform the design and applicability of future definitive trials in similar populations and settings.
Conclusion
The findings of this study are encouraging and suggest that even a relatively short and low-frequency slow waltz intervention may be associated with improvements in motor function, postural control and overall motor performance in people with PD. These results should be interpreted with caution, given the pilot nature of the study, but they provide preliminary evidence suggesting the potential of dance-based interventions as a complementary, non-pharmacological strategy in PD management. Future research should replicate these findings with larger, more diverse samples, examine long-term effects through follow-up assessments and compare different partner dance styles.
Supplemental Material
sj-doc-1-dmj-10.1177_1089313X261461437 – Supplemental material for Efficacy of a Slow Waltz-Based Program on Gait and Balance Problems in Parkinson’s Disease: A Pilot Study
Supplemental material, sj-doc-1-dmj-10.1177_1089313X261461437 for Efficacy of a Slow Waltz-Based Program on Gait and Balance Problems in Parkinson’s Disease: A Pilot Study by Martina Spiantini, Viviana Daniela Ghizzardi and Christel Galvani in Journal of Dance Medicine & Science
Supplemental Material
sj-docx-1-dmj-10.1177_1089313X261461437 – Supplemental material for Efficacy of a Slow Waltz-Based Program on Gait and Balance Problems in Parkinson’s Disease: A Pilot Study
Supplemental material, sj-docx-1-dmj-10.1177_1089313X261461437 for Efficacy of a Slow Waltz-Based Program on Gait and Balance Problems in Parkinson’s Disease: A Pilot Study by Martina Spiantini, Viviana Daniela Ghizzardi and Christel Galvani in Journal of Dance Medicine & Science
Footnotes
Acknowledgements
The authors are grateful to the participants for their kind cooperation. The authors would like to acknowledge Matteo Pellicanò for his help in data collection.
Ethical Considerations
All procedures were carried out in line with the Declaration of Helsinki. The Institutional Scientific Committee approved this study.
Consent to Participate
Participants gave their written informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the corresponding author on request.*
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.