
Abstract
Background. Researchers willing to publish their interventional studies’ results must register their studies before starting enrollment. This study aimed to describe all “open” (i.e., recruiting or not yet recruiting) behavioral studies in 16 of 20 top worldwide leading causes of death. Method. Search on Clinicaltrials.gov database (March 2010). Results. Of 204 studies, 66% accounted for the following diseases: diabetes (26%), colon and rectum cancers (16%), cerebrovascular diseases (14%), and HIV/AIDS (11%). Less than 3% were on tuberculosis, stomach cancer, cirrhosis of the liver, and lower respiratory infections combined; no study was open on malaria, nephrosis and nephritis, and diarrheal diseases. A total of 81% of the studies were interventional, and 19% were observational. Fifty-nine percent were conducted in the United States. A total of 79%, 35%, and 5% were sponsored by universities, U.S. federal agencies, and industry, respectively. Twenty-one percent of studies were cofunded. A typical interventional study had a two-arm prospective parallel design, lasting approximately 3 years and involving 100 to 400 subjects. Conclusions. Increasing the number of trials and participating countries (including developing ones) is necessary to make available behavioral interventions in different settings in the future.
Keywords
Since 2005, all clinical researchers aiming to have their trials’ results published have to comply with the International Committee of Medical Journal Editors and World Health Organization policy: The clinical trial should be registered before the first subject is enrolled (De Angelis et al., 2004; Sim, Chan, Gulmezoglu, Evans, & Pang, 2006). To comply with this policy, the study must be registered on a registry that should fulfill a number of requirements (World Health Organization, 2010). Clinical trial is defined as
any research study that prospectively assigns human participants or groups of humans to one or more health-related interventions to evaluate the effects on health outcomes. Clinical trials may also be referred to as interventional trials. Interventions include but are not restricted to drugs, cells and other biological products, surgical procedures, radiologic procedures, devices, behavioral treatments, process-of-care changes, preventive care, etc. (World Health Organization, 2010)
What has happened during the past years is that scientists have been registering their studies—not only interventional but also observational—on well-recognized registries, such as the U.S. NIH Clinicaltrials.gov or ISRCTN ([International Standard Randomised Controlled Trial Number], Current Controlled Trials, 2010). Thus, Clinicaltrials.gov, the largest registry had, on March 2010, close to 88,000 registered studies: some 73,000 and 15,000 interventional and observational studies, respectively. ISRCTN, the second largest registry, had 8,300 studies, the vast majority (>97%) being interventional trials. Three years ago, the World Health Organization (2008) published “The Global Burden of Disease, 2004 Update,” a comprehensive report in which, among other data, the leading causes of death—globally and by income group (low-, middle-, and high-income countries)—are provided.
This study aimed to describe the main characteristics of currently open behavioral (both interventional and observational) studies on the major causes of mortality.
Method
This analysis was conducted using Clinicaltrials.gov registered studies as of March 24, 2010. A careful assessment on the impact of the search fields to provide the optimal inclusion of the data for review was carried out. To fulfill the study objective, it was preferred to use the “open” (i.e., “recruiting,” “not yet recruiting”) rather than the “closed” (i.e., “active, but not recruiting”) descriptor, and although studies that were “active, but not recruiting” anymore may be lost, it would avoid the inclusion of studies that have been “terminated” or “completed” some years back (see the appendix). So, the fields chosen were “study type: interventional, observational and all,” “recruitment: open”; “study results: all”; “conditions”; “interventions: behavioral”; “gender”; “age group”; “funded: university/organization (UNO), industry (INY) and National Institutes of Health and other U.S. Federal Agency (FED)” merged together. To limit the search to those studies involving only behavioral interventions, those with other nonbehavioral interventions (i.e., biologicals, devices, dietary, drugs, procedures, and others) were not included. Although Clinicaltrials.gov has a validation system in place (Zarin et al., 2007), it relies ultimately on the accuracy of the data introduced by thousands of scientists, this being a source of inconsistencies and errors when filling in the database fields. A review of inconsistencies was conducted when reviewing the data provided on Clinicaltrials.gov.
For both interventional and observational studies, the estimated enrollment, number of arms, date of registration, and projected duration were recorded. The estimated study completion date or, if provided, the final data collection date for primary outcome measure, was considered to calculate the projected duration of the study. Interventional trials were classified by type of the study principal intervention. Types considered were “education and training,” “lifestyle (including physical training),” “special support or care,” “distant support,” and “other.” Although “dietary” was not included in the search as a descriptor, diet modifications were part of several programs or support activities that have been included in “lifestyle (and physical training).” Because of the wide variety of methods used among the observational studies, it was impossible to classify them in a reasonable limited number; their design (cohort, case-only, case–control, cross-sectional, and other) was, however, recorded.
Sixteen of the 20 leading causes of death in 2004, accounting for 58% of all worldwide mortality, were included in the analysis (World Health Organization, 2008). Since the World Health Organization and Clinicaltrials.gov may name diseases or conditions differently, among Clinicaltrials.gov’s “conditions,” the one that could best match each of the World Health Organization’s causes of death was chosen, using ICD10 as guidance (World Health Organization, 2007). However, with ischemic heart disease, hypertensive heart disease, and cerebrovascular disease, more than one “condition” was chosen to capture the majority of studies (Table 1). On the other hand, World Health Organization’s diarrheal diseases is more restrictive that Clinicaltrials.gov’s diarrhea; hence, the search was done excluding traveller diarrhoea, antibiotic-associated, chemotherapy-induced, radiation, irritable bowel disease, IBS (irritable bowel syndrome), and cancer.
Sixteen of the 20 World Health Organization’s “Leading Causes of Death” (World Health Organization, 2008) and Corresponding “Conditions” as per Clinicaltrials.gov Terminologies, Respectively
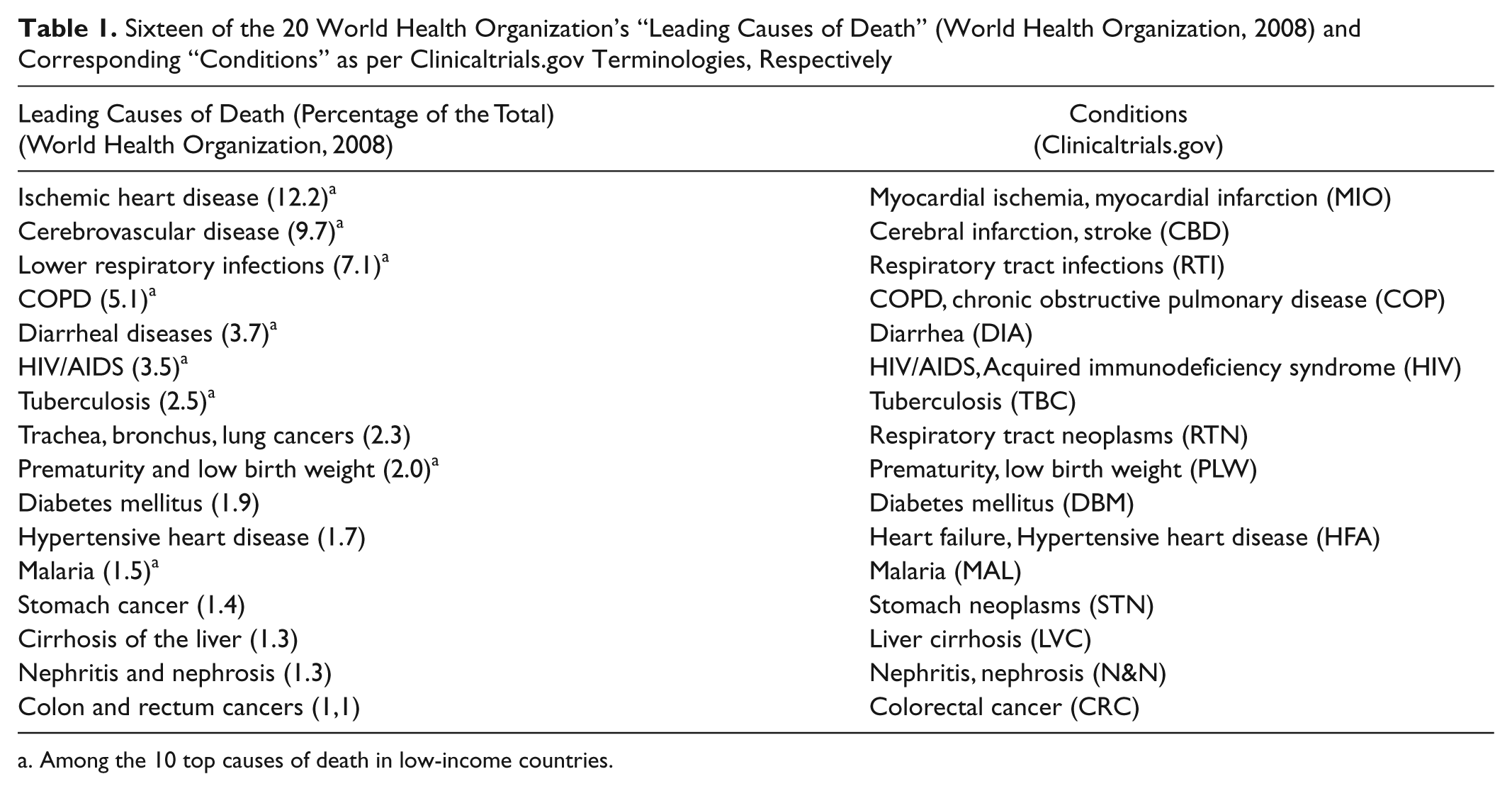
Among the 10 top causes of death in low-income countries.
Among the 20 top leading causes of death, 4 conditions were not included in this analysis: three are not suitable for experimental clinical research (“road traffic accidents,” “self-inflicted injuries,” and “birth asphyxia and birth trauma”), whereas the fourth one (“neonatal infections”) had a complex definition—a category that following the World Health Organization description also includes “other noninfectious causes arising in the perinatal period, that are responsible for 20% of deaths in this category,” that makes it impossible to match it with Clinicaltrials.gov conditions.
Results
The total numbers of “open” and “open” “behavioral” studies registered on Clinicaltrials.gov were 30,918 and 2,970, respectively; of the latter, 983 were exclusively behavioral, 785 (80%) being interventional whereas 198 (20%) were observational studies. U.S. sites were involved in 65% (642/983) of all “open” behavioral studies.
There were 204 “open” “behavioral” studies on 13 of the 16 considered conditions—no studies were “open” for malaria, nephrosis and nephitis, and diarrheal diseases. A total of 165 (81%) were interventional whereas 39 (19%) were observational studies (Table 2).
Number of Behavioral Studies Distributed by Clinicaltrials.gov’s “Condition” Corresponding to World Health Organization’s (2008) “Leading Causes of Death” and by Type (Interventional, Observational), Age Group, and Gender
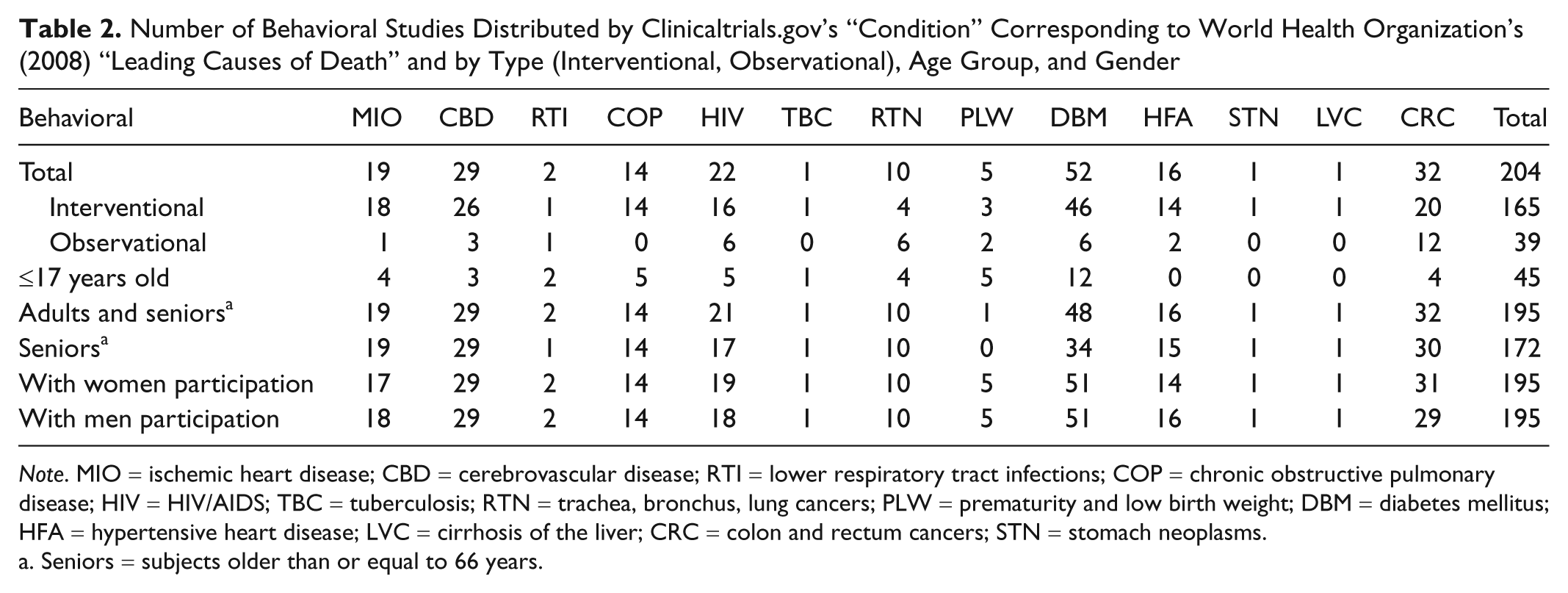
Note. MIO = ischemic heart disease; CBD = cerebrovascular disease; RTI = lower respiratory tract infections; COP = chronic obstructive pulmonary disease; HIV = HIV/AIDS; TBC = tuberculosis; RTN = trachea, bronchus, lung cancers; PLW = prematurity and low birth weight; DBM = diabetes mellitus; HFA = hypertensive heart disease; LVC = cirrhosis of the liver; CRC = colon and rectum cancers; STN = stomach neoplasms.
Seniors = subjects older than or equal to 66 years.
Four conditions accounted for 66% of all studies (Table 2): diabetes (26%, 52/204), colon and rectum cancers (16%, 32/204), cerebrovascular diseases (14%, 29/204), and HIV/AIDS (11%, 22/204). On the contrary, less than 3% (5/204) were on other four conditions: tuberculosis, stomach cancer, cirrhosis of the liver, and lower respiratory infections. Subjects ≤17 years old were accepted to participate in 45 studies, 27% (12/45) of them on diabetes. Seniors (≥ 66 years old) were a suitable age group in 84% (172/204) of studies. Almost all studies were open for inclusion to both women and men.
UNO were the main source of funding (79%, 162/204); FED and INY sponsored 35% (72/204) and 5% (11/204) of all studies, respectively (Table 3). Overall, 21% of studies were cofunded. U.S. sites were involved in 59% (120/204) of all studies; 75% (90/120) of these were devoted to diabetes mellitus, colon and rectum cancers, cerebrovascular diseases, and HIV/AIDS.
Number of Studies Distributed by Clinicaltrials.Gov’s “Condition” Corresponding to World Health Organization’s (2008) “Leading Causes of Death” and by Clinicaltrials.Gov’s by Funding Source and U.S. Involvement
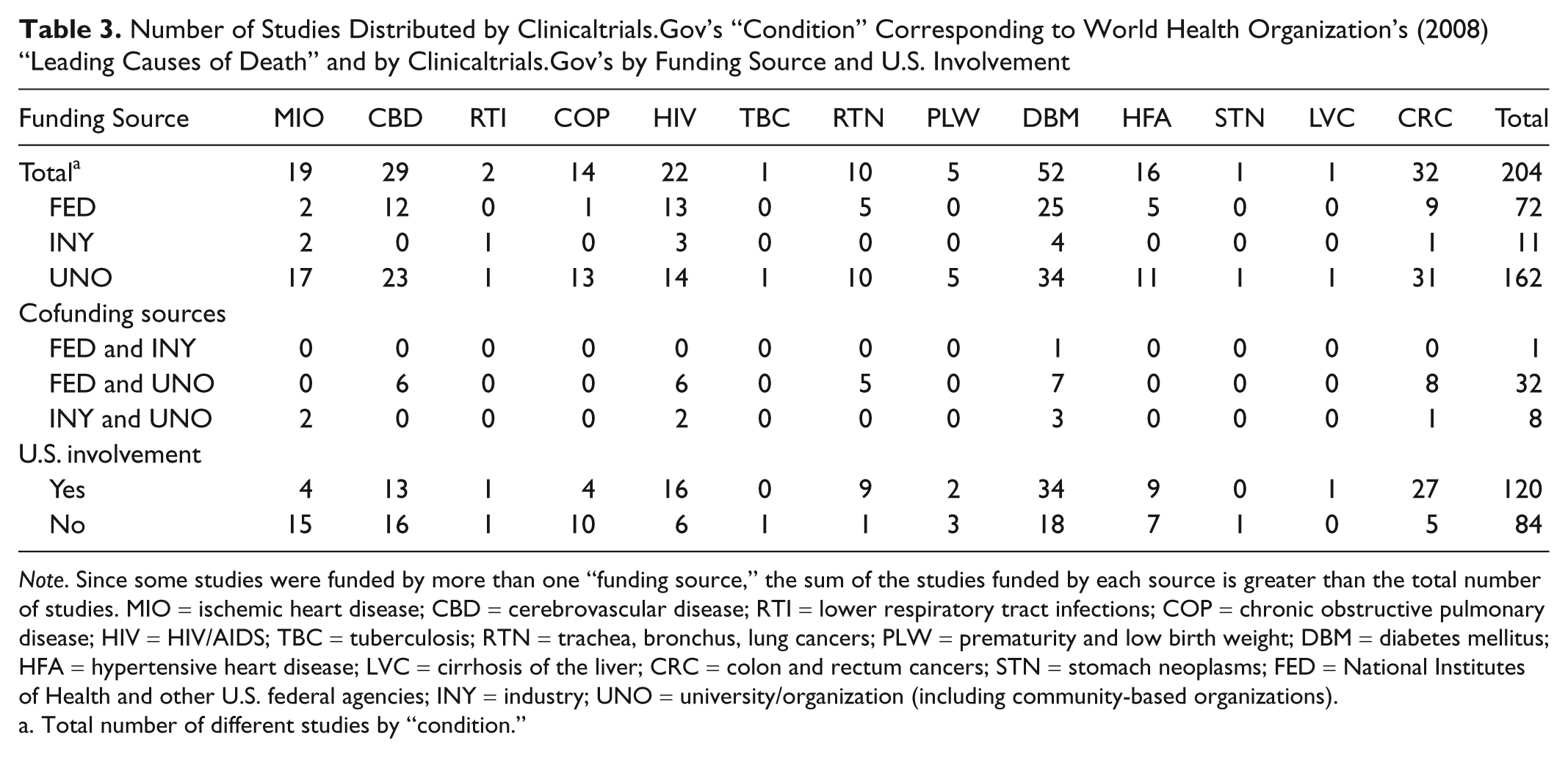
Note. Since some studies were funded by more than one “funding source,” the sum of the studies funded by each source is greater than the total number of studies. MIO = ischemic heart disease; CBD = cerebrovascular disease; RTI = lower respiratory tract infections; COP = chronic obstructive pulmonary disease; HIV = HIV/AIDS; TBC = tuberculosis; RTN = trachea, bronchus, lung cancers; PLW = prematurity and low birth weight; DBM = diabetes mellitus; HFA = hypertensive heart disease; LVC = cirrhosis of the liver; CRC = colon and rectum cancers; STN = stomach neoplasms; FED = National Institutes of Health and other U.S. federal agencies; INY = industry; UNO = university/organization (including community-based organizations).
Total number of different studies by “condition.”
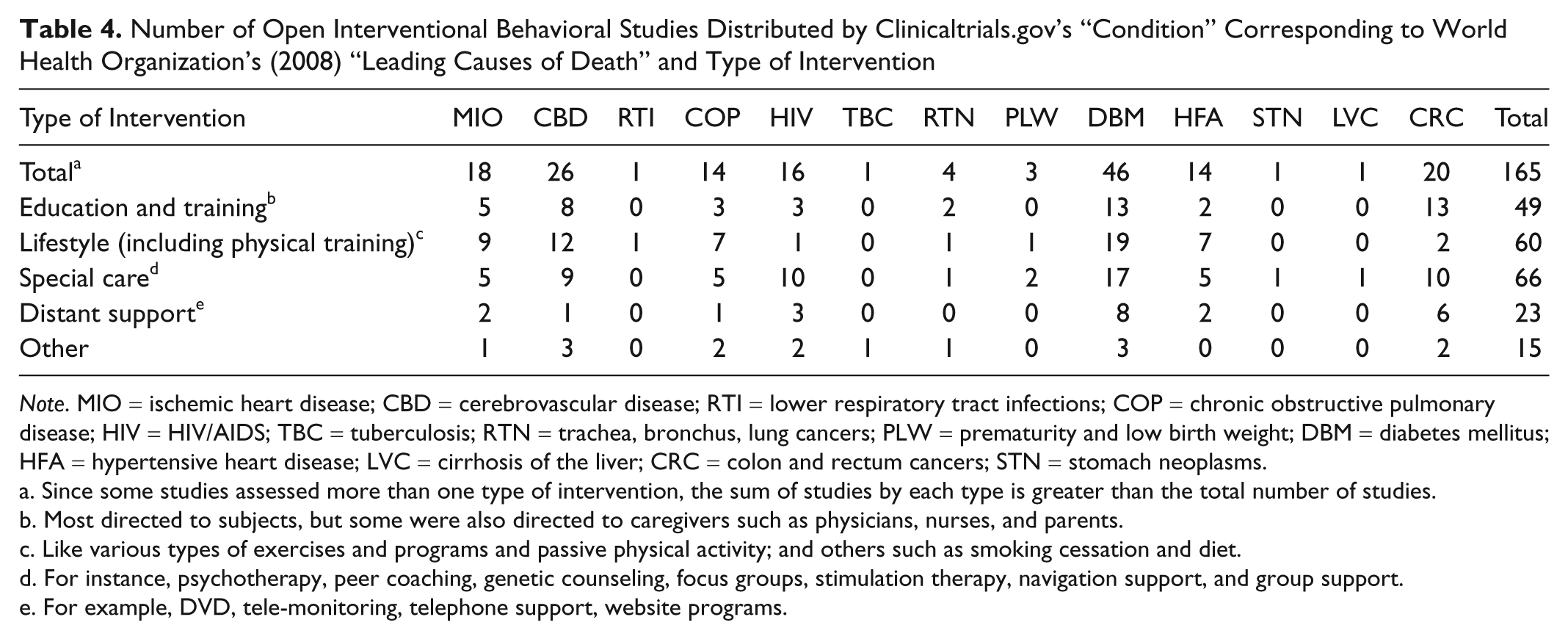
The variety of behavioral interventions assessed in the 165 studies, have been grouped in five different types as shown in Table 4. Modification of lifestyle (including physical training) was the most common intervention assessed on five diseases: diabetes mellitus, chronic obstructive pulmonary disease, cerebrovascular disease, ischemic heart disease, and hypertensive heart disease, whereas special care management was the most common one on HIV/AIDS.
Number of Open Interventional Behavioral Studies Distributed by Clinicaltrials.gov’s “Condition” Corresponding to World Health Organization’s (2008) “Leading Causes of Death” and Type of Intervention
Note. MIO = ischemic heart disease; CBD = cerebrovascular disease; RTI = lower respiratory tract infections; COP = chronic obstructive pulmonary disease; HIV = HIV/AIDS; TBC = tuberculosis; RTN = trachea, bronchus, lung cancers; PLW = prematurity and low birth weight; DBM = diabetes mellitus; HFA = hypertensive heart disease; LVC = cirrhosis of the liver; CRC = colon and rectum cancers; STN = stomach neoplasms.
Since some studies assessed more than one type of intervention, the sum of studies by each type is greater than the total number of studies.
Most directed to subjects, but some were also directed to caregivers such as physicians, nurses, and parents.
Like various types of exercises and programs and passive physical activity; and others such as smoking cessation and diet.
For instance, psychotherapy, peer coaching, genetic counseling, focus groups, stimulation therapy, navigation support, and group support.
For example, DVD, tele-monitoring, telephone support, website programs.
Table 5 shows several characteristics of the interventional studies, such as median number (and range) of arms and cases per study and condition, their projected duration, and the year in which they were registered in Clinicaltrials.gov. The typical study was a two-arm, prospective, parallel design trial, lasting around 3 years, involving between 100 and 400 subjects and registered in 2007 or 2008. In fact, the majority (67%, 111/165) of trials had two arms, whereas 4% (7/165) and 9% (14/165) had one or four arms, respectively. In eight cases (5%), neither the number of arms was specified nor was it possible to deduce it from the information provided. In all, 24% (40/165) of trials were to last 4 or more years, whereas in 10% (17/165), the intention was to conclude them in less than 1 year. In 13 (8%) trials, the end projected date was not provided; hence it was impossible to know the projected duration of the study. It was not common to inform about the final data collection date for primary outcome measure. The recruitment objective was ≤ 50 and ≥ 500 cases in 16% (26/165) and 21% (35/165) of studies, respectively. A total of 29% (48/165) were trials registered in 2009 or 2010, whereas 20% (33/164) were registered in 2003, 2004, or 2005. Finally, it is worth mentioning that many of these studies (mainly on cerebrovascular disease, ischemic heart disease, HIV/AIDS, and hypertensive heart disease) informed about the development phase (one to four).
Number of Open Interventional Behavioral Studies Distributed by Clinicaltrials.gov’s “Condition” Corresponding to World Health Organization’s (2008) “Leading Causes of Death” and by Number of Study Arms, Duration, Number of Cases to be Enrolled, and Year of Registration
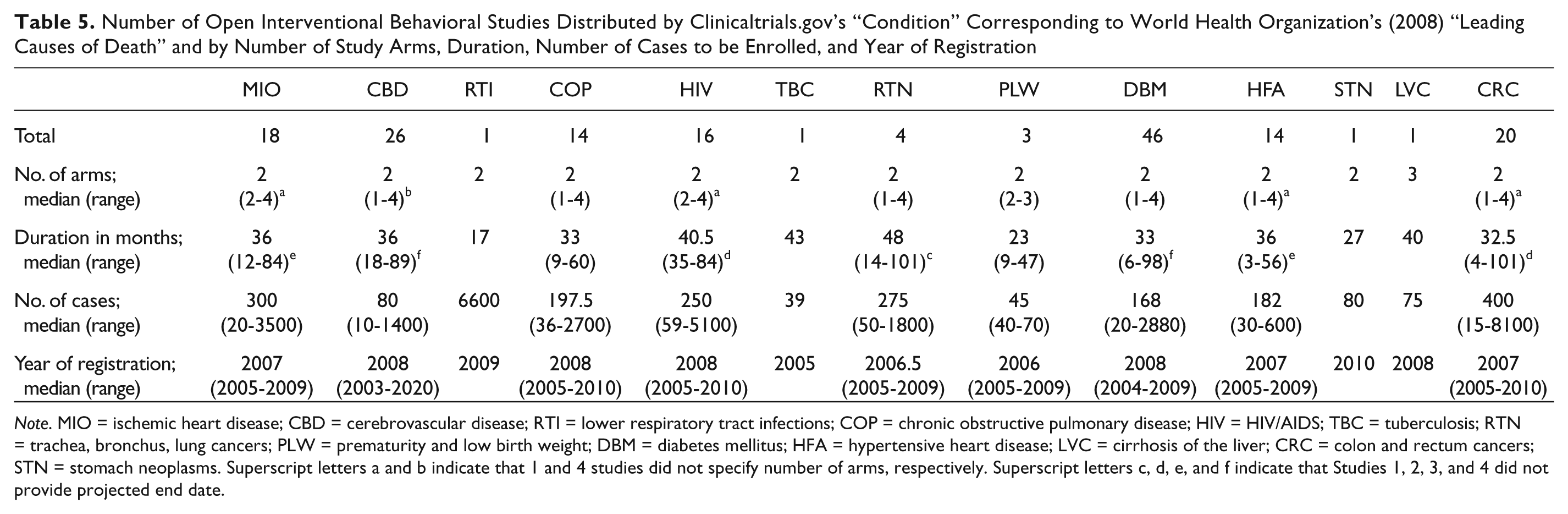
Note. MIO = ischemic heart disease; CBD = cerebrovascular disease; RTI = lower respiratory tract infections; COP = chronic obstructive pulmonary disease; HIV = HIV/AIDS; TBC = tuberculosis; RTN = trachea, bronchus, lung cancers; PLW = prematurity and low birth weight; DBM = diabetes mellitus; HFA = hypertensive heart disease; LVC = cirrhosis of the liver; CRC = colon and rectum cancers; STN = stomach neoplasms. Superscript letters a and b indicate that 1 and 4 studies did not specify number of arms, respectively. Superscript letters c, d, e, and f indicate that Studies 1, 2, 3, and 4 did not provide projected end date.
There were 39 open observational behavioral studies retrieved, albeit 2 were conducted on patients with 2 (NCT00381992) or 3 (NCT00368095) of the 13 conditions considered; hence, the actual number of different studies was 36. The majority 72% (26/36) were conducted in the United States. The designs were as follows: case-only prospective 53% (19/36), cohort prospective 19% (7/36), cross-sectional 14% (5/36), case–control 11% (4/36), and other (3%, 1/36). After carefully reading the information provided, 8 cohort studies have been reclassified as case-only studies; similarly, 1 cohort study was reclassified as case-only design. The observational studies had to enroll between 10 and 3,500 subjects, lasting 8 to 360 months. They had different objectives and methods although, for example, in studies on cancers, the majority was based on interviews and/or questionnaires to be filled in by patients or, exceptionally, their relatives. They were registered on Clinicaltrials.gov between 2005 and 2010, although the majority were in 2007 (33%, 12/36) or 2008 (28%, 10/36).
The data provided in this analysis were cleaned of inconsistencies such as, for instance, a prematurity and low birth weight study (NCT00179933), including seniors, or a study in veterans with heart failure (NCT00555360) that accepted children. More important is a long-term oxygen therapy study on chronic obstructive pulmonary disease patients (NCT00692198) that was considered as a behavioral study when seems more appropriate to consider it as a therapeutic (drug) trial. Another study aimed to evaluate the prevalence of type 2 diabetes or impaired glucose tolerance in children (NCT00042042), was observational rather than interventional, or, on the contrary, a study (NCT00461513) in which heart failure patients were to be randomized to patient-centered disease management versus usual care, described as a “multisite randomized study,” hence being experimental rather than observational.
There are other facts that should be taken into consideration when assessing the information provided by Clinicaltrials.gov. Thus, sometimes it could be observed that scientists forget to update the information after registering the trial. This happened, for instance, when the study was registered as “Not yet recruiting”; if no update was provided since then, the study will still be in the not recruiting phase many years after. This is the case, for example, with a diabetes trial (NCT00257218) and a cerebrovascular disease study (NCT00173992), both also registered in 2005, in which the information provided did not allow to know 5 years later if the trials have started yet.
Discussion
Although behavioral studies are an essential part of the current clinical research, it is still to be developed much further in many diseases and settings. To have behavioral interventions routinely used in community and individual management of conditions, many more successful studies, that is, yielding positive results, should be conducted. There are a number of factors limiting the full development of this type of studies, two of them being that they require resources (human, technical, and economical) for long periods of time, and that they are more suitable for chronic conditions. These could explain why behavioral interventions are only assessed, as previously mentioned, in less than 10% of all “open” studies registered in Clinicaltrials.gov. A further evaluation showed two remarkable data: (a) very few (3%) of all “open” studies were exclusively behavioral in nature, with no other (e.g., drugs, dietary, devices) assessed intervention; and (b) almost 2/3 of all studies were conducted in the United States. An additional factor that also contributes to the relatively few behavioral studies with regards to other type of interventional or observational studies is the funding source. Thus, clinical trials assessing drugs, devices, and biologicals are strongly supported by INY—a founding source that only marginally sponsored behavioral studies. Finally, the scarce percentage of cofunding studies also affected negatively in the number of “open” behavioral studies conducted.
This study provides a picture of ongoing behavioral research conducted in 16 of the 20 major causes of death in 2004, worldwide. Only 204 exclusively behavioral studies were “open” (i.e., recruiting or not yet recruiting). In fact, 7 of the 16 conditions considered had no or minimal number of studies; thus, malaria, nephrosis and nephritis, and diarrheal diseases had not even 1 “open” study, whereas tuberculosis, stomach cancer, cirrhosis of the liver, and lower respiratory infections had only 1 or 2 studies. All these conditions, except nephrosis and nephritis, have had several studies of this type conducted in the past or are currently in the “active, not recruiting” phase.
Behavioral studies are clustered in four diseases accounting for two thirds of all studies: diabetes, colon and rectum cancers, cerebrovascular diseases, and HIV/AIDS. A total of 81% were interventional trials, hence comparing one or more behavioral interventions with a control one—this percentage being almost identical to that of the total number of Clinicaltrials.gov behavioral registered studies (80%).
This analysis shows that only 165 were experimental trials exclusively evaluating behavioral interventions. This figure is heavily influenced by the fact that four of the diseases considered (diabetes, cerebrovascular disease, colon and rectum cancers, and ischemic heart disease) accounted for 67% of all “open” trials. Most interventional trials had a two-arm parallel, prospective design, were registered 2 or 3 years ago, had a projected duration of some 3 years, and were aiming to recruit 100 to 400 subjects. Acknowledging that each of the 13 conditions has its own special characteristics requiring specific approaches and considerations, generally speaking, both the number of subjects (only 21% with ≥500 cases) and the duration (only 24% with ≥4 years) of the trials seem insufficient to really end up with positive behavioral interventions that could be useful in the long-term clinical practice in different settings.
Several of the diseases causing worldwide highest mortality rates are chronic conditions and, hence, suitable for educational (with or without special support or care) and lifestyle changes management aiming for long lasting effects; that’s why experimental trials assessing these type of behavioral interventions are common as shown in this analysis. This probably may be due to, among other factors, the fact that self-management educational programs have only resulted in low or moderate short-term effects, and only in some chronic diseases (Foster, Taylor, Eldridge, Ramsay, & Griffiths, 2007; Warsi, Wang, LaValley, Avorn, & Solomon, 2004).
What is really important, however, is that although many interventional behavioral studies were on conditions that deeply afflict developing countries—45% were conducted in the projected four top causes of mortality in low-income countries in 2030 (i.e., ischemic heart disease, HIV/AIDS, cerebrovascular disease, and chronic obstructive pulmonary disease; Mathers & Loncar, 2006)—68 were run in the United States, Canada, and western European countries, whereas only 4 in Taiwan and 2 in China. Since the social, cultural, economical, and psychological conditions are critically different between developed and developing countries, conducting experimental behavioral trials in communities of these latter countries is a must to have useful interventions in these settings.
Strengths and Limitations
The main limitation is that the data used in the analysis refers to a single database, Clinicaltrials.gov. However, Clinicaltrials.gov is, by far, the largest registry. As commented, Clinicaltrials.gov data accuracy relies on the information registered by thousands of scientists. Several examples have been described to show the type of observed inconsistencies. Some depend on errors when filling-in the database fields, others depend on the lack of updated information and, last, others on how to describe the study design—observational or interventional, cohort or case-only. In fact, almost all these inconsistencies or errors—that were corrected, if appropriate—had no impact at all regarding the objective of this analysis. It is interesting to observe that the trial classification by phase (1 to 4), aimed for clinical development of medicines, is widely used by behavioral experimental researchers, suggesting some lack of training to this respect among scientists filling in Clinicaltrials.gov fields.
Clinicaltrials.gov is an American registry that is increasingly becoming very popular among international sponsors and investigators; in fact, 47% of all “open” studies have no involvement of U.S. sites. Behavioral studies registered on Clinicaltrials.gov were mainly (65%) conducted in the United States; it is not possible to know if this reflects reality or, on the contrary, there are many non-U.S. studies that were not registered on this database. However, since the policy of registering interventional trials applies also to behavioral ones, it seems reasonable to accept that the number of (U.S. and non-U.S.) studies registered on Clinicaltrials.gov is correct enough to draw general valid conclusions. This, however, cannot be applied to observational studies—although, Clinicaltrials.gov hosted about 7,000 open observational studies, 983 of these being exclusively behavioral in nature. It should be highlighted, however, that among the leading causes of death considered in this analysis, studies with non-U.S. involvement was 17% greater than on all conditions (41% vs. 35%), hence reinforcing the idea that the figures provided by Clinicaltrials.gov were accurate enough.
It is difficult to assess how the “conditions” in Clinicaltrials .gov correspond exactly to the World Health Organization’s “leading causes of death.” In most instances, there was no problem in making this match. However, in diseases such as ischemic heart disease and cerebrovascular disease, some trials could have been lost in the search performed on Clinicaltrials .gov. This, again, should not have affected the overall results obtained, since to fulfill the aim of the analysis it was not necessary to include all the studies, but the majority.
This analysis was on major causes of death, which will continue to be an important source of mortality and morbidity in the next future. Thus, 11 of the diseases considered are among the 15 leading causes of mortality projected in 2030, whereas 5 of them are among the top 10 of the projected major causes of disability-adjusted life years (Mathers & Loncar, 2006). Hence, the conditions chosen seem appropriate, not only from the perspective of the 2004 data but also from the projected causes of death and disability in 2030.
Conclusions
The number of “open” exclusively behavioral studies on 16 of the 20 top causes of death in 2004 seems rather limited (n = 204). This analysis showed that most (two thirds) of all behavioral studies were clustered in four conditions: diabetes, cerebrovascular diseases, HIV/AIDS, and colon and rectum cancers; the first three are projected to be among the 10 leading causes of mortality in 2030, not only at a worldwide level but also in low-income countries (Mathers & Loncar, 2006). U.S. researchers were involved in 59% of all interventional studies. Since the prevention and management of these 16 conditions cannot rely solely on the use of other interventions such as drugs or biologicals, a significant increase in the number of trials and countries (including developing ones) participating in behavioral studies is deemed necessary for the future availability of efficient and long-term sustainable interventions in different settings.
Footnotes
Appendix
The author declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author received no financial support for the research and/or authorship of this article.