
Abstract
Objectives. Although pregnant women are a high-priority group for seasonal influenza vaccination, vaccination rates in this population remain below target levels. Previous studies have identified sociodemographic predictors of vaccine choice, but relationships between preconception heath behaviors and seasonal influenza vaccination are poorly understood. This prospective cohort study followed pregnant women during the 2010-2011 influenza season to determine if certain health behaviors were associated with vaccination status. Method. Participants were pregnant women receiving prenatal care from Kaiser Permanente Northwest and Kaiser Permanente Northern California. Women were surveyed about preconception smoking, alcohol consumption, and vitamin/supplement use. Vaccination data were obtained from health plan databases and state immunization records. Results. Data from 1,204 women were included in this analysis. Most participants (1,204; 66.4%) received a seasonal influenza vaccine during the study period. Women vaccinated prior to pregnancy were more likely to use a supplement containing folic acid (80%) or vitamin D (30%) compared with women who were vaccinated during pregnancy (72% and 15%, respectively) or unvaccinated women (62% and 12%, respectively, p < .001). Women vaccinated prior to or during pregnancy were more likely (75%) to have never smoked compared with women who were not vaccinated (70%, p = .005). There were no significant differences in alcohol use or household cigarette smoke exposure by vaccination group. Conclusions. Women who engaged in specific preconception health behaviors were more likely to receive seasonal influenza vaccination. Failure to participate in these health behaviors could alert health care practitioners to patients’ increased risk of remaining unvaccinated during pregnancy.
Keywords
Pregnant women are at increased risk for influenza-related complications and hospitalizations (Centers for Disease Control and Prevention [CDC], 2010; Creanga et al., 2010; Ellington et al., 2011; Jamieson et al., 2009; Louie, Acosta, Jamieson, & Honein, 2010; Rasmussen et al., 2011; Siston et al., 2010). The CDC and the American College of Obstetricians and Gynecologists (ACOG) recommend that all pregnant women receive influenza vaccination regardless of trimester (ACOG, 2010; Fiore et al., 2010). Despite these recommendations, influenza vaccination rates among pregnant women have remained below 50%, well below the Healthy People 2020 goal of 80% and the ACOG target of 100% (Ding et al., 2011; Ding, Euler, & Singleton, 2013; Healthy People, 2013; Henninger, Crane, & Naleway, 2012).
Several recent studies have identified demographic and personal factors associated with receipt of influenza vaccination during pregnancy, including older maternal age, higher education and higher occupational status, perceived susceptibility to influenza, perceived risk of getting seriously ill from the flu, receipt of recommendations and offers from a health care provider, and perceived effectiveness of influenza vaccination (CDC, 2012; Ding et al., 2011; Fabry, Gagneur, & Pasquier, 2011; Freund et al., 2011; Henninger, Naleway, Crane, Donahue, & Irving, 2013; Steelfisher et al., 2011). Factors associated with lower vaccination rates during pregnancy include Black or Hispanic race/ethnicity, concerns about vaccine effects on maternal or infant health, and lack of knowledge about increased influenza risk during pregnancy, about the benefits of vaccination, or about where to get vaccinated (Fisher et al., 2011; Henninger et al., 2013; Steelfisher et al., 2011; White, Petersen, & Quinlivan, 2010).
To date, research on influenza vaccination among pregnant women has not examined associations with other health behaviors widely accepted as having an impact on maternal and fetal health outcomes, including behaviors associated with tobacco use, alcohol use, and vitamin/supplement use. The objective of this study was to determine whether engagement in specific health-promoting preconception behaviors is associated with receipt of seasonal influenza vaccination among pregnant women.
Method
The Pregnancy and Influenza Project (PIP) was a prospective cohort study of pregnant women enrolled in Kaiser Permanente Northwest (KPNW) and Kaiser Permanente Northern California (KPNC) during the 2010-2011 influenza season. These two integrated health care delivery systems serve a combined 3.8 million members in Oregon, Washington, and Northern California. Details of the study were published previously (Thompson et al., 2011). In brief, participants in the study included English- and Spanish-speaking pregnant women who had at least one prenatal visit at a Kaiser Permanente clinic, an expected delivery date after November 15, 2010, and were at least 16 years of age in the KPNW region or 18 years of age in the KPNC region. The difference in the minimum age requirement was due to institutional review board policy differences in the two regions regarding recruitment of minors (allowed at KPNW, not at KPNC). Potential participants were identified through electronic medical records (EMR) and recruited between December 2010 and May 2011. The women were contacted by telephone, screened for eligibility, and asked to provide written consent for study participation. Inclusion criteria included enrollment in the health plan for the entire 2010-2011 influenza season and completion of the enrollment interview. Women vaccinated postpartum were excluded from analyses. All study procedures, recruitment materials, and forms were reviewed and approved by the institutional review boards at both sites and CDC to ensure that the research was conducted in accord with prevailing ethical principles.
Data Collection
Enrolled participants completed a 20- to 30-minute baseline enrollment interview via telephone that included questions about demographics, obstetric history, health behaviors (smoking, alcohol use, vitamin/supplement use), and seasonal influenza vaccination, among other topics.
Participants were asked about their current and previous use of cigarettes and were categorized as never-smoked, quit prior to pregnancy, or smoked during pregnancy. Additionally, all participants reported if anyone in their household currently smoked in their presence.
Participants reported on alcohol use in the 3 months prior to becoming pregnant. Participants were asked to indicate how many days during a typical week they had consumed a beverage containing alcohol, as well as how many beverages containing alcohol, on average, they consumed on the days they did drink. Alcohol use was conceptualized in several ways. First, we assessed mean number of drinks per week. Second, we developed risk categories for drinking based on guidelines from the National Institute on Alcohol Abuse and Alcoholism (National Institute of Alcohol and Alcoholism, 2013): Low-risk prepregnancy drinkers were defined as those who consumed no more than three drinks per day and no more than seven drinks per week, while at-risk drinkers were defined as those who consumed more than the low-risk single-day or weekly amounts. Finally, we defined prepregnancy binge-drinking as consumption of four or more alcoholic beverages on a single day, regardless of risk category (National Institute of Alcohol and Alcoholism, 2004).
Participants answered questions about their use of vitamins and supplements (multivitamin, prenatal vitamin, vitamin D, and folic acid) during the 3 months prior to becoming pregnant. While vitamin D supplementation is not a standard recommendation for women prior to pregnancy, it is increasingly recommended for adults, including pregnant and lactating females (Institute of Medicine, 2011). The U.S. Public Health Service and CDC recommend that all women of child-bearing age consume 400 µg of folic acid daily to prevent common and serious birth defects (CDC, 1992). Because multivitamins, prenatal vitamins, and folic acid supplements all contain folic acid, we collapsed the individual vitamin categories into one “folic acid” category. We created two variables for both vitamin D and folic acid: any use and daily use.
The presence of a high-risk medical condition associated with increased risk of influenza complications, for example, asthma, diabetes, immune disease (Fiore et al., 2010), was ascertained from ICD-9CM coded medical records (detailed code list available from the authors). This information was collected because we believed the presence of a high-risk medical condition could affect the likelihood of a patient receiving vaccination during the study period.
Vaccination status was confirmed at the end of influenza season by EMR and state immunization data, and participants were categorized into three vaccination groups: vaccinated prior to pregnancy, vaccinated during pregnancy, and unvaccinated. It is important to note that influenza vaccination is strongly recommended at prenatal visits. Additionally, Kaiser Permanente has implemented a number of strategies to increase influenza vaccination during pregnancy. Examples of strategies include clinician checklists, standard order sets for prenatal visits that include influenza vaccination, and “flags” in the EMR for pregnant women who have not yet been vaccinated. Additionally, walk-in vaccination clinics are typically offered in the fall of each year.
Statistical Analyses
We performed descriptive univariate analyses to examine the association between prespecified health behaviors and vaccination status as well as between sociodemographic characteristics and vaccination status, with outcomes in three categories (vaccinated prior to pregnancy, vaccinated during pregnancy, and unvaccinated). Comparisons were made using chi-square or Fisher’s exact tests for categorical variables and Wilcoxon tests (nonparametric one-way ANOVA) for continuous variables. No adjustments were made for multiple comparison testing. Multinomial logistic regression models were performed independently for each health behavior found to be significant in univariate analyses, using unvaccinated women as the reference group. Each model adjusted for maternal age, pregnancy start date, study site, ethnicity, race, education, gravidity, and parity; p values <.05 were considered statistically significant. All analyses were conducted using SAS 9.2 (SAS Institute, Cary, NC).
Results
A total of 1,616 women were enrolled in the PIP study. We excluded from analysis women who were not enrolled at Kaiser Permanente for the entire 2010-2011 season (n = 139), those who did not complete the enrollment interview (n = 125), those who did not complete the interview prior to delivery (n = 138), and those who received influenza vaccination postpartum (n = 10). After exclusions, the study population was 1,204 pregnant women. In comparing our final study population with women who were excluded, we found that excluded women were slightly younger (mean 31.9 vs. 32.5; p = .04), less educated (some college or less 35% vs. 26%; p = .01), and more likely to be from KPNC (66% vs. 59%; p = .02). There were no other significant differences between these two groups on the sociodemographic characteristics listed in Table 1.
Maternal Characteristics by Vaccination Status.
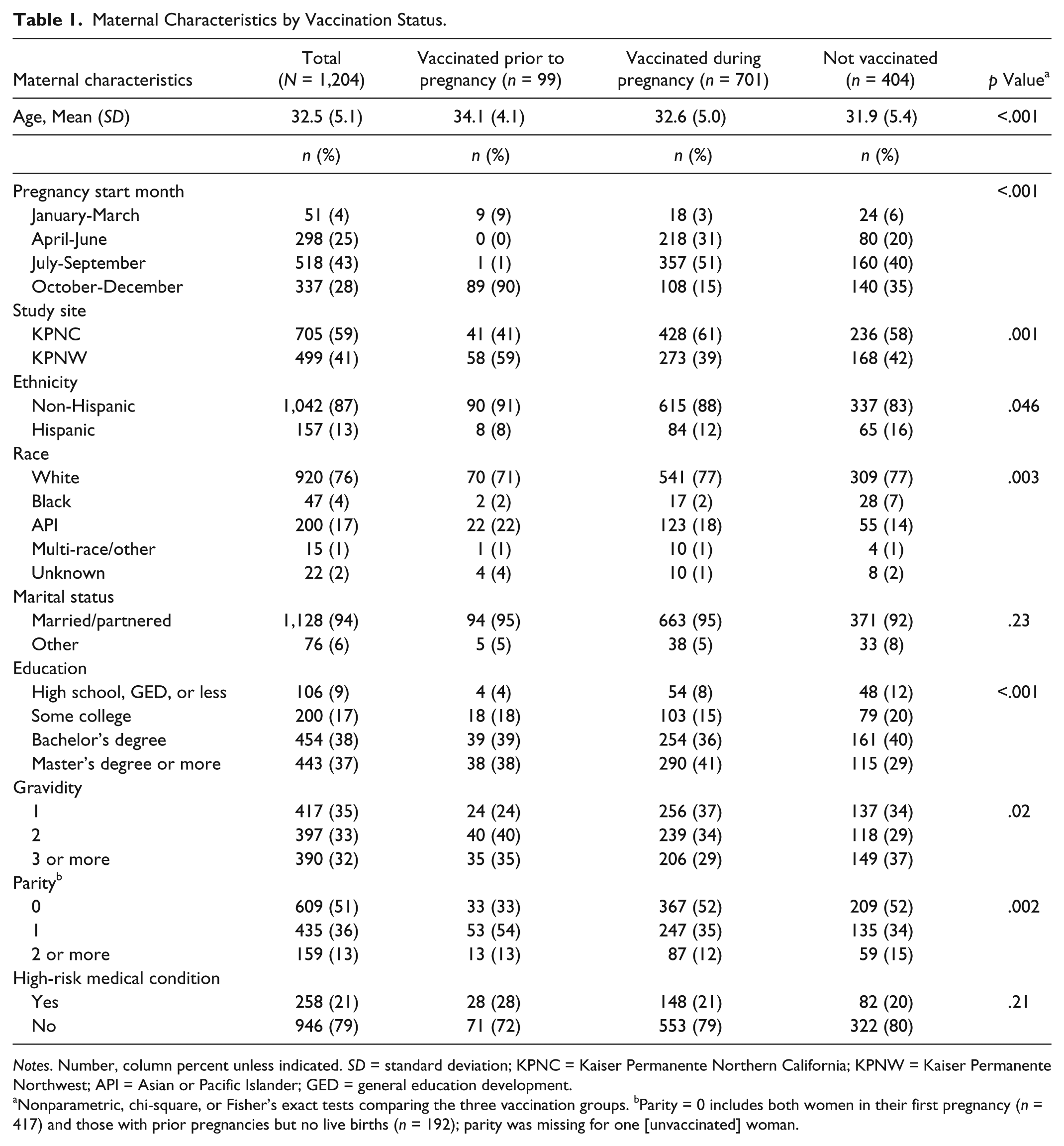
Notes. Number, column percent unless indicated. SD = standard deviation; KPNC = Kaiser Permanente Northern California; KPNW = Kaiser Permanente Northwest; API = Asian or Pacific Islander; GED = general education development.
Nonparametric, chi-square, or Fisher’s exact tests comparing the three vaccination groups. bParity = 0 includes both women in their first pregnancy (n = 417) and those with prior pregnancies but no live births (n = 192); parity was missing for one [unvaccinated] woman.
Vaccination rates and basic sociodemographic characteristics are shown in Table 1. Two thirds of participants (800/1,204; 66%) received a 2010-2011 seasonal influenza vaccine during the study period. Of those vaccinated, 701 (88%) received the vaccine during pregnancy and 99 (12%) were vaccinated prior to pregnancy onset. Women who were vaccinated during pregnancy had pregnancy start dates in the spring or summer, whereas women who were vaccinated prior to pregnancy were more likely to have pregnancy start dates in the fall. Overall, the majority of women were vaccinated in October or November (49% and 28%, respectively, data not shown).
The majority of women in the study were White (76%), non-Hispanic (87%), married/partnered (94%), and had completed at least a bachelor’s degree (75%); mean age at pregnancy end was 32.5 years. Twenty-one percent of women had a high-risk medical condition other than pregnancy placing them at risk for influenza complications.
Vaccination status varied by enrollment site; vaccinated women at KPNW were more likely to have been vaccinated prior to pregnancy whereas vaccinated women at KPNC were more likely to have been vaccinated during pregnancy. KPNW began recruitment 2 months prior to KPNC, and recruited more women in their first trimester, which may explain some of the difference in the timing of vaccination by site. Rates of vaccination were similar at both sites (66.5% for KPNC and 66.3% for KPNW). Women vaccinated either before or during pregnancy were more likely to be older, non-Hispanic, married, and to have a graduate degree, compared with unvaccinated women. Vaccination status was also associated with number of pregnancies (gravidity) and number of live births (parity) (Table 1). In general, women with fewer prior pregnancies or live births were more likely to get vaccinated.
Differences in vaccination status by self-reported health behavior are shown in Table 2. Overall, 73% of respondents reported they had never smoked, while 22% reported quitting smoking prior to pregnancy. Only 5% of women reported they smoked during pregnancy. Women who were vaccinated prior to or during pregnancy were more likely to report that they had never smoked compared with women who were not vaccinated (75% vs. 70%, p = .005). Likewise, women who were not vaccinated were more likely to report that they had smoked during pregnancy in comparison to women who were vaccinated during pregnancy or prepregnancy (8% vs. 4% vs. 2%, p = .005).
Vaccination Status by Self-Reported Health Behavior.
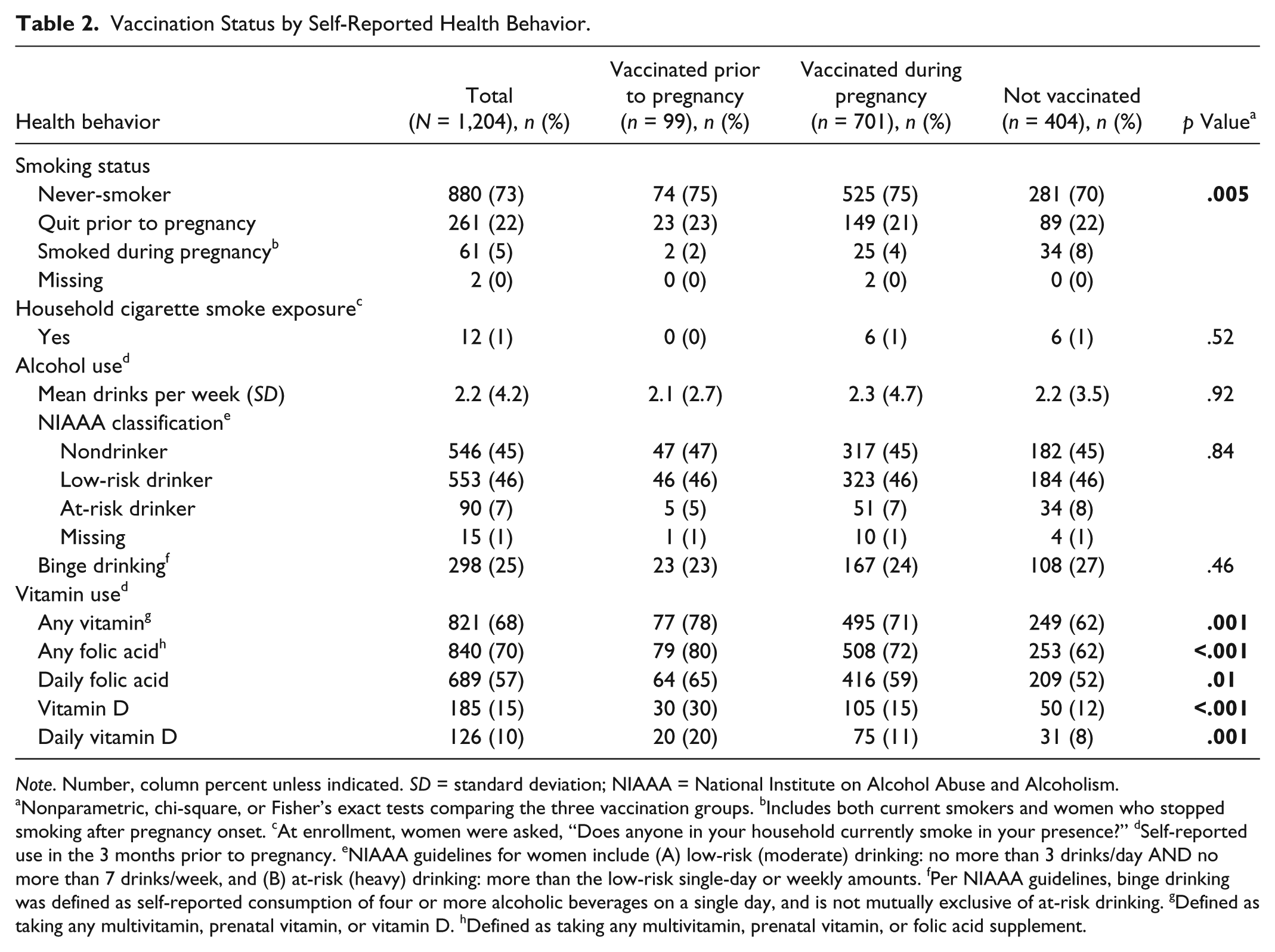
Note. Number, column percent unless indicated. SD = standard deviation; NIAAA = National Institute on Alcohol Abuse and Alcoholism.
Nonparametric, chi-square, or Fisher’s exact tests comparing the three vaccination groups. bIncludes both current smokers and women who stopped smoking after pregnancy onset. cAt enrollment, women were asked, “Does anyone in your household currently smoke in your presence?” dSelf-reported use in the 3 months prior to pregnancy. eNIAAA guidelines for women include (A) low-risk (moderate) drinking: no more than 3 drinks/day AND no more than 7 drinks/week, and (B) at-risk (heavy) drinking: more than the low-risk single-day or weekly amounts. fPer NIAAA guidelines, binge drinking was defined as self-reported consumption of four or more alcoholic beverages on a single day, and is not mutually exclusive of at-risk drinking. gDefined as taking any multivitamin, prenatal vitamin, or vitamin D. hDefined as taking any multivitamin, prenatal vitamin, or folic acid supplement.
Among the 1,189 women who answered alcohol-related questions, in the 3 months prior to pregnancy the mean number of drinks per week reported was 2.2. Forty-five percent of respondents reported that they had been nondrinkers in that time period (Table 2). The majority of women who reported a history of drinking were classified as low-risk drinkers, and incidence of binge drinking prior to pregnancy was 25%. We found no significant differences in vaccination status by reported alcohol use.
Sixty-eight percent of women reported vitamin use in the 3 months prior to pregnancy (Table 2). The proportion of women reporting any vitamin use was highest among women vaccinated prior to pregnancy (78%, p = .001). Women vaccinated prior to pregnancy were more likely to report folic acid use (80% vs. 72% vs. 62%, p < .001) and vitamin D use (30% vs. 15% vs. 12%, p < .001), compared with women vaccinated during pregnancy or those not vaccinated.
In multinomial models adjusting for maternal age, pregnancy start date, site, ethnicity, race, education, gravidity, and parity, women who reported vitamin D use in the 3 months prior to pregnancy were significantly more likely to be vaccinated prior to pregnancy than to go unvaccinated (Table 3, p = .003). After adjustment for the covariates listed above, women who reported never smoking or quitting smoking prior to pregnancy were more likely to be vaccinated during pregnancy than to go unvaccinated (p = .009). Women who reported folic acid use were also more likely to be vaccinated during pregnancy than to go unvaccinated (p = .019).
Association Between Health Behaviors and Vaccination: Multinomial Modeling Results a .
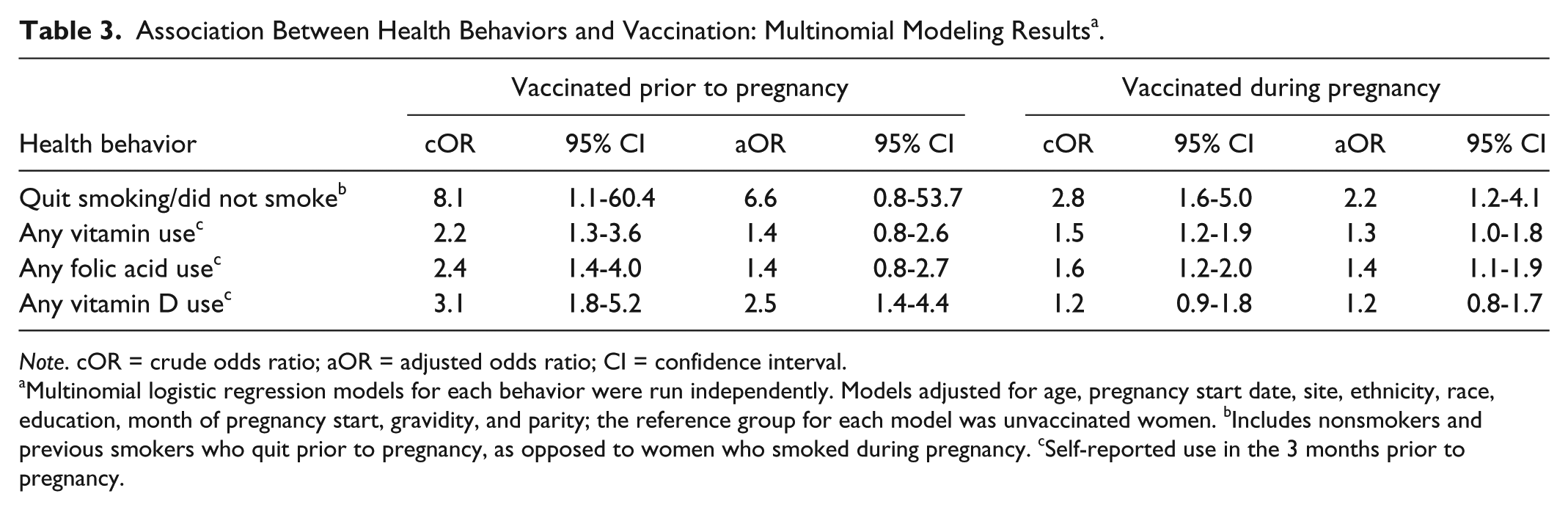
Note. cOR = crude odds ratio; aOR = adjusted odds ratio; CI = confidence interval.
Multinomial logistic regression models for each behavior were run independently. Models adjusted for age, pregnancy start date, site, ethnicity, race, education, month of pregnancy start, gravidity, and parity; the reference group for each model was unvaccinated women. bIncludes nonsmokers and previous smokers who quit prior to pregnancy, as opposed to women who smoked during pregnancy. cSelf-reported use in the 3 months prior to pregnancy.
Discussion
Our findings indicate that women who do not take vitamins/supplements prior to pregnancy and those who smoked during pregnancy may be less likely to receive seasonal influenza vaccination before delivery. This finding persists even after controlling for other maternal and demographic factors that previously have been associated with vaccination status, such as maternal age and ethnicity. Our results are consistent with previous studies that demonstrated an association between lack of participation in some periconceptional health-promoting behaviors and lower likelihood of following other recommended health behaviors during pregnancy (Haslam & Lawrence, 2004; Haslam, Lawrence, & Haefeli, 2003). While the health behaviors analyzed (vitamin/supplement use, alcohol use, smoking) differ in some key ways from vaccination (i.e., the former are repetitive, while the latter is a one-time behavior), the association between these behaviors may provide important information to the clinician regarding overall likelihood of engaging in a variety of preventative health behaviors during pregnancy.
Interestingly, we found that women with fewer pregnancies (lower gravidity) and fewer live births (lower parity) were more likely to be vaccinated. This trend has been demonstrated in previous studies as well (Henninger et al., 2012) and could be an important area of focus for clinicians working to increase vaccination rates.
Limitations of the study include the fact that we did not collect data on pregnancy intention, which may account for some of the associations identified between health behaviors and vaccination. Previous studies have shown that women with unintended pregnancies are more likely to smoke before and during pregnancy (Khajehpour, Simbar, Jannesari, Ramezani-Tehrani, & Majd, 2013; Than et al., 2005) and less likely to use prenatal vitamins before becoming pregnant (Morin et al., 2002; Rosenberg, Gelow, & Sandoval, 2003). Similarly, we did not collect information about prenatal care utilization, which could be correlated with vaccination as well as the other health behaviors analyzed. However, we did not expect much variation in prenatal care utilization due to the study setting. For example, 95% of pregnant women in our population receive a prenatal visit within the first trimester (of within 42 days of health plan enrollment, if they join after their first trimester) and are scheduled for regular follow-up visits subsequent to the first visit. Finally, our study population may not be representative of the general population of pregnant women in the United States, as our participants are predominantly White, older (≥30 years), highly educated, and less likely to engage in unhealthy behaviors. As mentioned above, our population also may be more likely to receive earlier and more regular prenatal care than is the general population, thus increasing the opportunity for vaccination during pregnancy.
The results of the current study highlight that influenza vaccination prior to or during pregnancy is correlated with other pregnancy health behaviors, and that future studies assessing adverse pregnancy outcomes should control for these potentially confounding influences. Additionally, a lack of patient engagement in these health-promoting behaviors during early pregnancy or the preconception period could serve as a flag to clinicians to intensify interventions encouraging influenza vaccination. Prior research has demonstrated that provider recommendations to vaccinate, and health education about the benefits of vaccination, are effective tools in increasing influenza vaccination rates among pregnant women (McCarthy, Pollock, Nolan, Hay, & McDonald, 2012; Mouzoon et al., 2010; Yudin, Salripour, & Sgro, 2010). Targeting these recommendations and education efforts to pregnant smokers and those who do not take vitamins/supplements prior to pregnancy may be helpful in increasing the rate of influenza vaccination among this population. Hence, the associations found in the current study could have meaningful clinical implications for providers, in addition to an impact on future research regarding vaccination during pregnancy.
Footnotes
Authors’ Note
The findings and conclusions reported in this article are those of the authors and do not necessarily represent the views of the Centers of Disease Control and Prevention, Abt Associates, or Kaiser Foundation Research Institute.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention (Contract 200-2010-F-33132 to Abt Associates, Inc.).