
Abstract
Background. Identifying effective relapse prevention interventions is a vital step to help smokers maintain abstinence for the long term. Aims. The purpose of this study is to determine if providing recently quit smokers with self-directed relapse prevention booklets is effective at maintaining abstinence after intensive group smoking cessation treatment. Method. Two hundred and twenty-five participants were randomized to receive Forever Free (FF) relapse prevention booklets or a control booklet (Surgeon General’s report, SG) at the end of a 6-week group treatment program. Participants were then contacted by phone to assess whether they had read the materials. Smoking status was assessed 6 months after their target quit date. Primary analyses focused on the 115 participants who quit at the end of treatment. Results. There was no difference in the 6-month quit rate between groups (40.7% quit FF vs. 44.6% quit SG, p = .67). The FF group read a significantly smaller proportion of the materials versus the control booklet (20.0% read most or all of FF vs. 72.0% of SG, p < .001). Conclusion. Forever Free self-directed relapse prevention booklets did not reduce relapse or enhance cessation over general tobacco and health information when added to intensive group smoking cessation treatment. However, this study lacked power to detect a small but clinically meaningful positive effect.
Keywords
Cigarette smoking adversely affects almost every organ system in the body, making quitting smoking the single most important thing a smoker can do to improve their health (Fiore, 2008; U.S. Department of Health and Human Services, 2014). Unfortunately, the majority of smokers who make a quit attempt will relapse to smoking within the first year (Hughes, Keely, & Naud, 2004; Hughes, Peters, & Naud, 2008), making identifying effective relapse prevention interventions a vital step in helping smokers maintain abstinence for the long term.
A previous review of the effectiveness of smoking relapse prevention interventions for abstinent smokers (Agboola, McNeill, Coleman, & Leonardi Bee, 2010) concluded that self-directed relapse prevention materials, such as Forever Free (FF) booklets, appear to reduce relapse in smokers who achieved abstinence without treatment or professional assistance (Brandon et al., 2004). In addition, there are a number of trials showing at least partial effectiveness of this intervention for self-quitters and quitline callers (Brandon, Collins, Juliano, & Lazev, 2000; Brandon et al., 2004; Brandon et al., 2012; Sheffer, Stitzer, Brandon, & Bursac, 2010; Unrod et al., 2016) and one showing effectiveness in low-income postpartum women (Brandon et al., 2012).
Providing FF booklets to recently quit smokers aligns well with self-directed learning theory, which suggests that adults “have learning needs closely related to changing social roles” and they are “problem-centered and interested in immediate application of knowledge” (Merriam, 2001, p. 5). Through the lens of this theory, FF materials are a readily available source of information for recently quit smokers to use as they navigate their changing role to that of a former smoker.
However, adult learners must also find the information relevant to their learning needs. A recent study by Maskrey et al. (2015) did not find any significant effect of FF booklets on relapse rates among smokers who received a variety of face-to-face treatments from smoking cessation clinics in England (individual or group treatment and the option of nicotine replacement therapy [NRT], bupropion, or varenicline). The authors suggested that during in-person treatment, participants received similar information to what was provided in the FF booklets which made the booklets redundant.
Another possible explanation is that the face-to-face treatment and medications that participants received during that study were not standardized and this variability was not controlled for in the analysis. To our knowledge, no previous study has evaluated the FF booklets in smokers who received standardized medication and intensive face-to-face treatment. Therefore, the purpose of this study is to determine if FF booklets are effective at preventing relapse when added to treatment consisting of group support plus transdermal nicotine patches. Providing these booklets to recently quit smokers is a relatively simple, low-cost intervention that, if effective, could be easily implemented in clinical practice.
Study Design and Method
Smoking Cessation Treatment Phase: Part 1
This report is Part 2 of a two-part randomized controlled clinical trial designed to help smokers quit smoking (Part 1) and stay quit (Part 2). Details of Part 1 have been reported elsewhere (Foulds et al., 2015). In brief, 225 participants aged 21 years or older who smoked >4 cigarettes per day and were ready to make a quit attempt in the next month participated in a 6-week smoking cessation trial designed to test the motivational effect of lung age feedback (at baseline assessment) on 1 month quit rates in smokers seeking intensive group treatment. Participants attended 6 weekly group sessions with the quit date at the second visit. Quit status was assessed at 1 month post target quit date (TQD).
Relapse Prevention Phase: Part 2
At the assessment visit, prior to the start of the treatment phase (Part 1), all participants were randomized to receive written self-directed relapse prevention booklets (active or control condition) at the end of the treatment phase. The primary analysis of this report is focused on those participants who were abstinent at the 1-month follow-up. A secondary analysis was also conducted using all 225 participants to assess whether the FF materials provided any cessation benefit to participants regardless of quit status at the end of the treatment phase. Materials were given to all participants in person at the last group support session (1 month after the target quit date) in a plain manila envelope and they were encouraged to read and refer to the materials as needed. Those who did not attend the last group session had the booklets mailed to them. One week after receiving the booklets, participants were followed up with a phone call to encourage them to use the booklets and to assess what proportion of the materials they had read. They were then followed-up 6-months post-TQD to assess quit status (5 months after receiving relapse prevention materials). Both parts of the trial are registered at Clinicaltrials.gov (NCT01980485).
Self-Directed Relapse Prevention Materials
The active condition was receipt of all FF booklets (Brandon et al., 2004) in a single packet. The control booklet was the “A Report of the Surgeon General: How Tobacco Smoke Causes Disease” (U.S. Department of Health and Human Services, 2010). The FF booklets are a series of eight evidence-based colorful booklets (8 to 17 pages each and 100 total pages) written at a fifth- to sixth-grade level to provide recent ex-smokers with information relevant to remaining quit. The booklets were developed to be a comprehensive overview of common barriers that smokers encounter after quitting and they offer suggestions for dealing with these barriers. Topics covered in the booklets are descriptions of nicotine dependence, managing high-risk situations, suggestions for lifestyle changes and how to handle initial slips and urges, information on weight gain, life without cigarettes, and managing stress (Brandon et al., 2004). The control booklet was a summary of the 2010 Surgeon General’s (SG) report written specifically for nonscientific consumers. It is a full color, 20-page booklet that is freely available on the Centers for Disease Control and Prevention website and includes topics such as the chemical make-up of cigarettes, their addictive nature, how they cause harm (cancer, circulatory, respiratory, diabetes, children), and why it is important to quit. It does not contain specific advice on quitting or relapse prevention but provides the national quitline phone number for additional help and support.
Follow-Up of Treatment Components
At the phone contact, 1 week after receipt of materials, participants were asked the following questions: “Have you had a look at the materials?” (response: yes/no), “Roughly what proportion of the materials would you say you have read?” (responses: just glanced at it, read less than half, read most but not all, read all of it). At both the phone contact and the 6-month follow-up, participants were asked two open-ended questions to gain qualitative feedback on the helpfulness of the booklets: “What part did you find most helpful?” and “In what ways do you think the booklet could be made more helpful?” Participants could comment on one or both questions at both contact points. At the 6-month follow-up, participants were asked to rate the helpfulness of each treatment component on a scale of 1 (not helpful at all) to 7 (very helpful). Components included receiving “nicotine patches,” “group support meetings,” “having your carbon monoxide and lung function measured,” “tips and advice provided by clinicians,” “reading materials provided at the end of the group sessions,” and “knowing you would be returning for a 6-month follow-up.”
Quit Status and Relapse Assessment
At the end of the treatment phase (Part 1) and at the 6-month follow-up, participants were considered quit if they reported no tobacco use in the past 7 days (“Have you smoked [or used smokeless tobacco] in the past 7 days?” [yes/no]) and had an exhaled carbon monoxide (CO) less than 10 parts per million (ppm). We used intention to treat (ITT) principles for these two visits, and participants who did not provide in-person CO validation of their self-reported quit status were counted as smokers for the analysis (generally nonattenders). Participants were considered to have relapsed if they had a validated (CO < 10 ppm) quit status at the end of the treatment phase and said “yes” to the following question at the 6-month follow- up: “In the past 5 months, since your last group meeting, did you ever smoke or use tobacco for 7 consecutive days.” Days to relapse was calculated for those who responded “yes” using the following question “If yes, around how many days ago did those 7 days of smoking/tobacco use begin?”
Data Analysis
Quantitative data were analyzed using SAS version 9.3 (SAS Institute, Inc., Cary, NC). Chi-square tests were used to determine differences between categorical variables and two-tailed t tests for continuous variables of interest. A multivariate logistic regression model was set up with all covariates in Table 1 to determine predictors of abstinence at 6 months using the SAS stepwise procedure (iterative backwards and forwards stepwise). A second model was then set up to include the intervention and any covariates from the first model that had a p value ≤.05. In addition, although the lung age feedback intervention for Part 1 of the study was not found to have an effect on short-term (1-month) abstinence (Foulds et al., 2015), it was included in this model to control for any possible effect. An identical procedure was followed for the secondary outcome that included all 225 participants, regardless of smoking status at 1 month. The initial power calculations were based on a two-tailed Fisher’s exact test with 5% significance level. The sample size included in this study (115 for the primary analysis) provides 80% power to detect a quit rate of 56% in the intervention group compared with a quit rate of 30% in the control group, an absolute difference of 26%. The original Brandon et al. study reported on a sample size and effect size similar to the present trial though their follow-up period was much longer (12 months vs. our 5 months). In their subsample of 138 smokers who were short-term quitters at intake, they found continuing abstinence rates of 88% in the group who received mailed booklets versus 65% in the group that did not (Brandon et al., 2000), an absolute difference of 23%.
Characteristics of Participants Who Were Abstinent at the End of the Treatment Phase and Were Randomized to Receive Either Forever Free (FF) Relapse Prevention Materials or the A Report of the Surgeon General: How Tobacco Smoke Causes Disease (SG) Control Materials (n = 115).
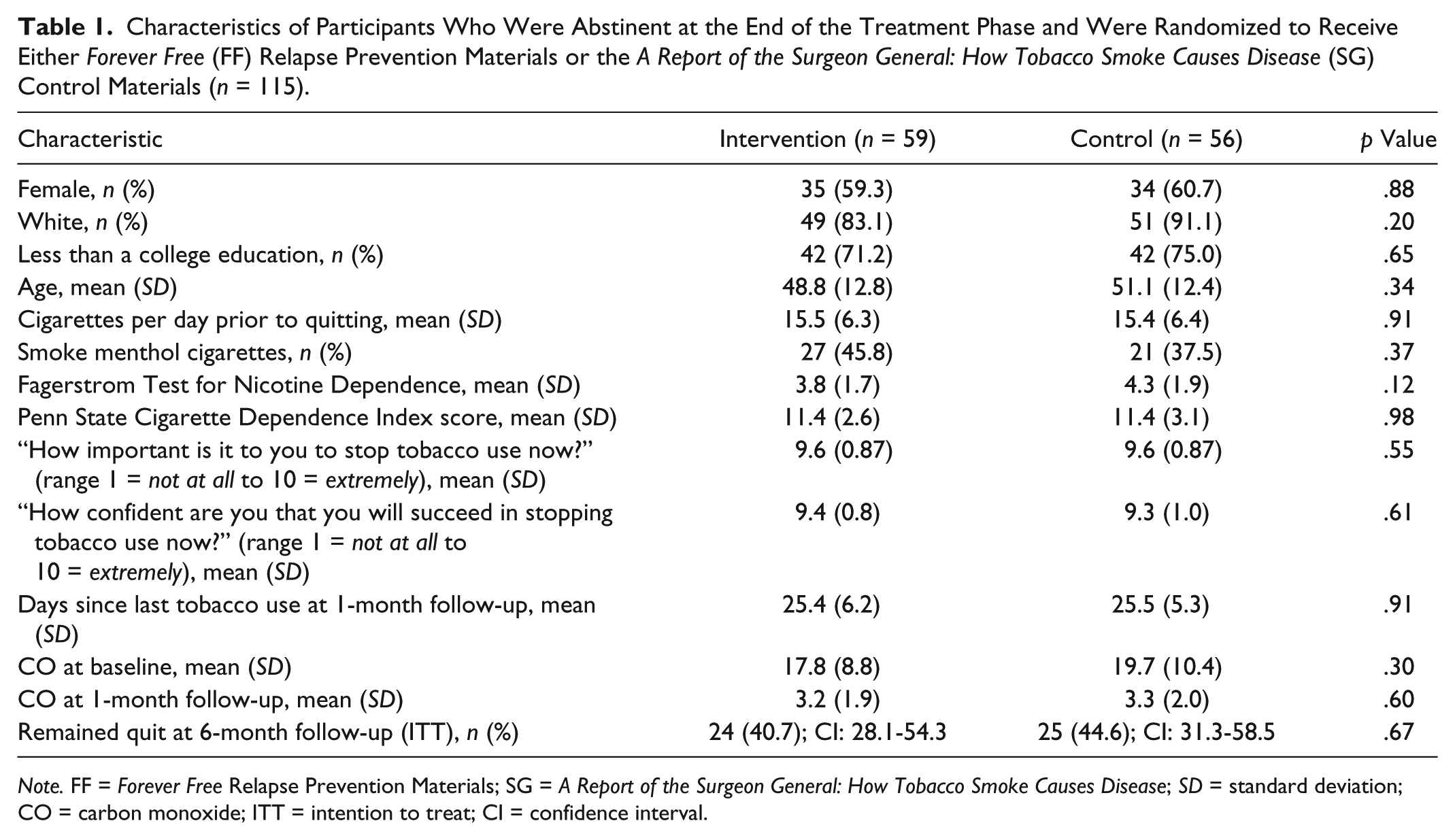
Note. FF = Forever Free Relapse Prevention Materials; SG = A Report of the Surgeon General: How Tobacco Smoke Causes Disease; SD = standard deviation; CO = carbon monoxide; ITT = intention to treat; CI = confidence interval.
A survival analysis was conducted using R (The R Foundation, n.d.) to determine if there was a difference between the groups with respect to time-to-relapse. The R package “survival” (Terry & Gramsbch, 2000) was used to calculate values for the Kaplan–Meier curves and to perform the log-rank test. The R package “ggplot2” (Wickham, 2009) was used to graph the results. Participants who did not complete the 6-month follow-up were assumed to have relapsed 1 day after group sessions ended. Two tailed p values of <.05 were considered significant.
Qualitative data were in the form of brief comments. Comments from both the phone call and the 6-month follow-up were combined and responses were grouped together into general themes by intervention group.
Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at the Penn State Milton S. Hershey Medical Center and College of Medicine. REDCap is a secure, web-based application designed to support data capture for research studies (Harris et al., 2009). This study was approved by the Penn State Hershey Institutional Review Board.
Results
A CONSORT diagram showing the flow of participants from randomization through the 6-month follow-up is presented in Figure 1. A total of 115 or 225 participants were abstinent at the end of the treatment phase (51.1%) and were included in the primary analysis.
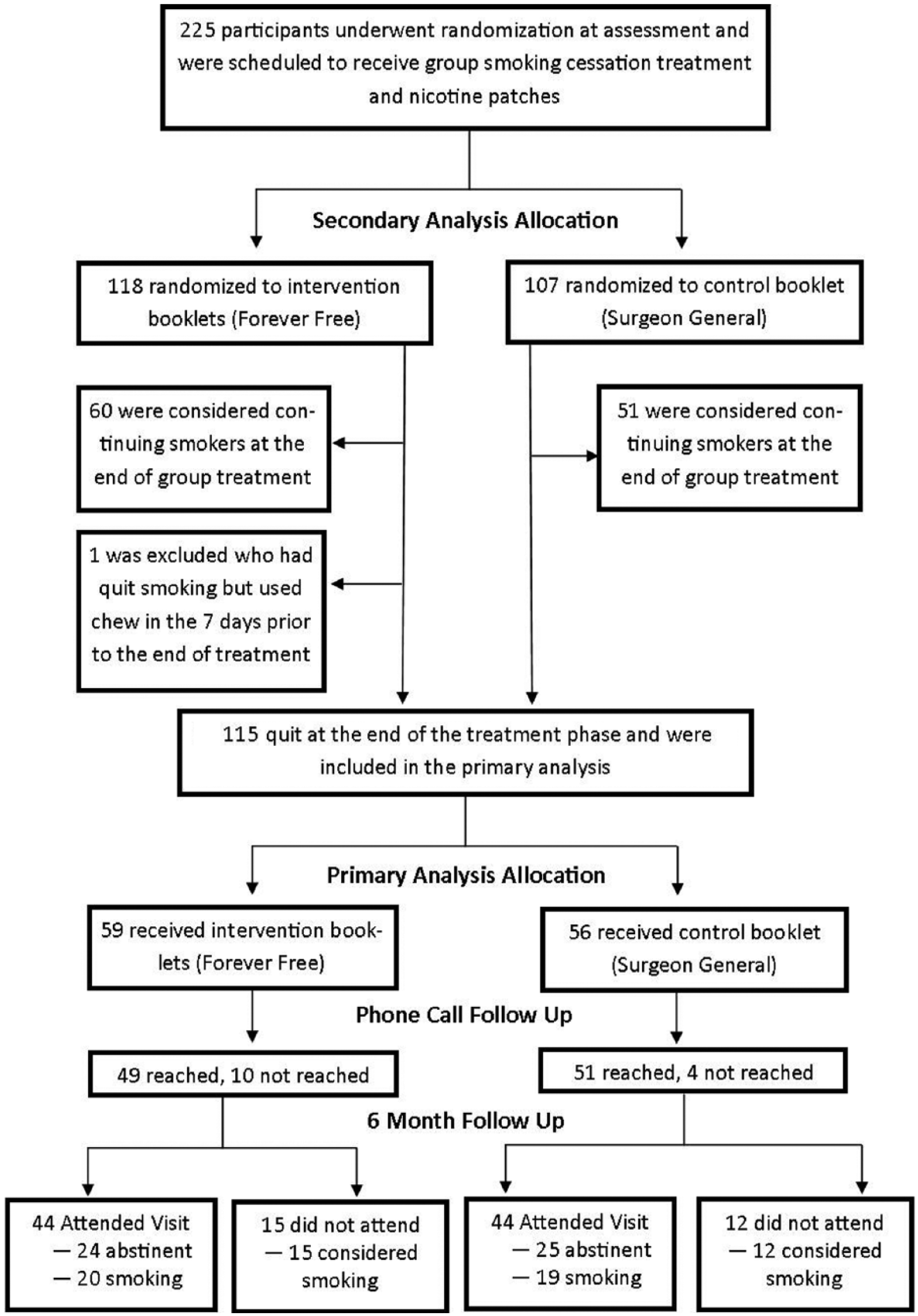
Study flow diagram for the primary analysis (participants who were quit at the end of the treatment phase) and the secondary analysis (all study participants).
Primary Analysis
Basic demographic, tobacco use, and dependence characteristics of the primary analysis sample are described in Table 1. There were no significant differences between the groups for any characteristic. The 6-month ITT biochemically validated quit rate for those who were quit at end of the treatment phase by intervention group was 40.7% FF (n = 24/59, confidence interval [CI] = 28.1-54.3) versus 44.6% (n = 25/56, CI = 31.3-58.5) SG, p = .67 (42.6% overall [n = 49/115, CI = 33.4-52.2]).
When considering predictors of successful quitting at 6 months from the multivariate logistic regression, the intervention was not found significant (p = .65) and the only predictors were male gender (p = .01) and increasing days since last tobacco use at the 1-month follow-up (p = .04). The mean number of days to relapse was 91.5 days for FF and 105.8 days for SG (p = .20). Results of the time-to-relapse survival analysis are presented in Figure 2 (p = .30).
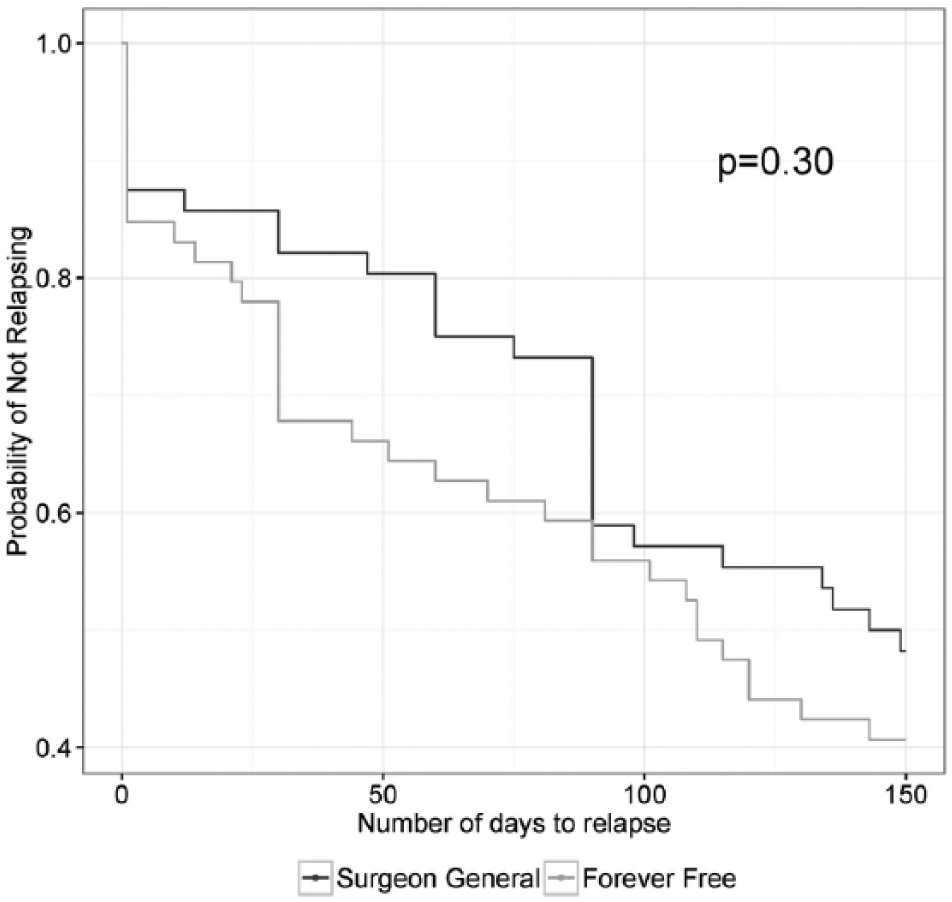
Results of survival analysis for time-to-relapse in days by intervention group (Forever Free and Surgeon General).
One hundred participants were able to be reached for a phone contact 1 week after receiving the materials (n = 49 FF, and n = 51 SG). There was no difference between the groups in the proportion of participants who stated that they looked at the materials (82.4% FF vs. 77.6% SG, p = .55). Participants in the FF group were significantly less likely to report that they read most or all the reading materials compared with those in the SG group (20.4% FF vs. 72.0% SG, p ≤ .001).
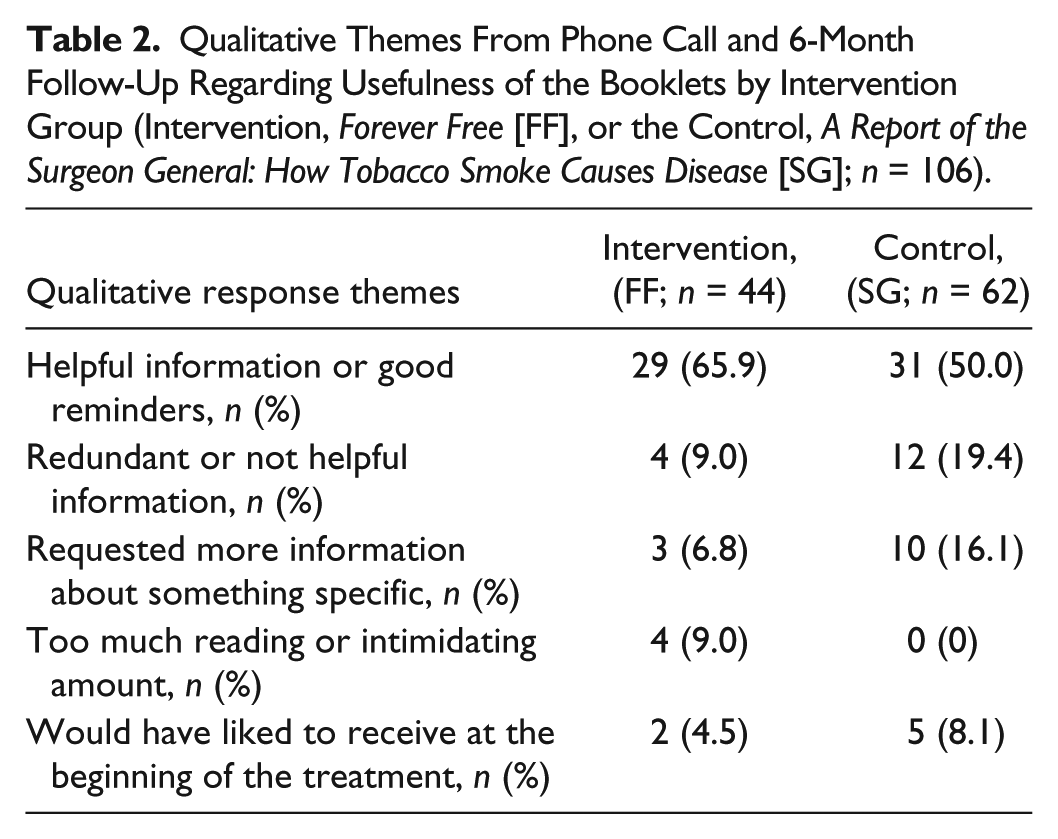
There were 106 qualitative comments received from both the phone call and the 6-month follow-up. Themes derived from the qualitative responses related are presented in Table 2 by intervention group.
Qualitative Themes From Phone Call and 6-Month Follow-Up Regarding Usefulness of the Booklets by Intervention Group (Intervention, Forever Free [FF], or the Control, A Report of the Surgeon General: How Tobacco Smoke Causes Disease [SG]; n = 106).
At the 6-month follow-up, 91 participants (45 FF and 46 SG) provided ratings for the treatment components either over the phone or in person. The highest rated treatment component (range: 1 = not helpful at all to 7 = very helpful) was group support meetings (M = 5.8, SD = 1.7) followed by nicotine patches (M = 5.5, SD = 2.1) and tips and advice provided by the clinicians (M = 5.5, SD = 1.6). The lowest rated treatment component was the booklets (M = 4.3, SD = 1.7). There were no significant differences between the groups for any rating (all p values >.1). When comparing the booklets to each treatment component, the mean rating for each treatment component was significantly higher than the booklets (all p values <.001).
Secondary Analysis
The 6-month ITT biochemically validated 7-day point prevalence abstinence rate for all study participants by intervention group was 22.0% (n = 26/118, CI = 14.9-30.6) for those receiving FF booklets and 28.0% (n = 30/107, CI = 19.8-37.5) for those receiving the SG booklet, p = .30 (24.9% overall [n = 56/225, CI = 19.4-31.1]). The predictors of quitting from the multivariate logistic regression in the secondary analysis with all 225 participants yielded results similar to the primary analysis with the intervention as nonsignificant (p = .31) and significant predictors of abstinence as male gender (p = .02) and increasing days since last tobacco use at the 1-month follow-up (p < .01).
Discussion
This study found no evidence that FF self-directed relapse prevention booklets added additional benefit to participants after intensive group smoking cessation treatment plus nicotine patches, as compared with a control booklet focusing on the harms to health from smoking. This is in contrast to some previous studies that did find these booklets to be effective in certain populations (Brandon et al., 2000; Brandon et al., 2004; Brandon et al., 2012; Sheffer et al., 2010; Unrod et al., 2016).
Our finding is in agreement with Maskrey et al. (2015), who found almost identical prolonged abstinence rates at the 3- and 12-month follow-up among those randomized to receive FF booklets versus those given a single control booklet. The current study adds to their findings that providing the FF booklets after intensive treatment (including medication), whether it is standardized or not, does not seem to add any further benefit for relapse prevention. In addition, since the FF booklets were originally designed as a self-help intervention for smokers who achieved abstinence without professional assistance, these studies taken together suggest that although the materials have been found to be effective with untreated quitters, they may be less effective with those who received intensive treatment to quit.
When considering self-directed adult learning theory, “The emphasis of this orientation is on meeting the needs of the individual” (Tisdell & Taylor, 2001, p. 8), and in this case, it is possible that the FF booklets did not meet their needs. It is also possible that the information provided during intensive treatment in both the Maskrey et al. (2015) study and our study made the reading materials redundant, and this was a comment made by a few of our FF study participants. However, while our qualitative data provide some insight, because fewer participants in the FF group reported reading most of materials, we received a lower number of comments overall from this group. It should be noted that the FF booklets contained many more pages than the SG booklet (100 pages for FF vs. 20 pages for SG) so that it could be argued that although a much lower proportion of the participants read most or all the FF booklets, they may have read a similar total amount of information. However, the point remains that the specific relapse prevention information did not result in less relapse. If the FF booklets were perceived as redundant to the intensive treatment, this could also be an explanation as to why there was such a low proportion of participants who actually read all of the FF materials, and also be an explanation of why they were not effective in our study or the Maskrey et al. (2015) study.
It is worth considering that a large percentage of the participants in our study (73%) had less than a college education, making it of particular interest as to whether written educational materials or whether the amount of material provided at one time is the most appropriate intervention in this population. As noted by some of the participants in the FF group, the volume of materials provided all at one time was “intimidating,” which may have made them less inclined to read all the materials. Brandon et al. (2004) conducted a randomized trial to evaluate whether the number of FF booklets provided to participants at one time (vs. sequentially over time) influenced relapse rates. The authors found that there was no difference in relapse prevention rates between those who were mailed the FF booklets individually over 12 months and those who received all 8 booklets at one time. However, those who received one mailing of all 8 books reported lower levels of satisfaction with the intervention as compared with those who received the booklets individually over time suggesting that although relapse rates did not differ, acceptability of the intervention did. Unrod et al. (2016) also found that among highly nicotine dependent smokers (Fagerstrom Test for Nicotine Dependence score >5), having the booklets mailed out individually over a longer period of time had a significant impact on quit rates compared with a mass mailing or standard quitline care. Our data are in agreement with both these findings suggesting that, at the very least, a large amount of materials may be perceived as less appealing by participants. If it is the case that participants found the FF packet in our study to be too much information received at one time, it is certainly possible that this is an explanation for why there was such a difference between the groups in the proportion of the materials they read. In addition, as suggested by the study participants, giving the materials at the beginning of the treatment phase instead of after it is completed may provide an opportunity to reinforce what was discussed during treatment.
Strengths of this study include a standardized treatment phase with group counseling and nicotine patches and biochemically validated quit rates including a 6-month outcome. Limitations of this study include a small sample size particularly by the 6-month follow-up, which may have limited our ability to detect a difference in participant rated satisfaction levels between the groups. Although our result is very consistent with the larger Maskrey et al. (2015) trial and relapse occurred slightly less rapidly in the control group, this study was powered to detect a large effect (56% vs. 30% remaining abstinent at 6 months), but was underpowered to detect a smaller yet worthwhile effect (e.g., 56% vs. 45% remaining abstinent). Therefore, it remains possible that more adequately powered future studies could detect a small, yet clinically significant positive effect on relapse prevention among smokers who have received intensive smoking cessation treatment.
Our study was not initially designed to assess reasons that the participants did not read the materials, although the data we present here suggest that further investigation into acceptability and delivery methods of self-directed relapse prevention materials would be helpful for the formation of other programs based on this model. In particular, the two conditions in our study differed greatly in the amount of reading required (100 pages FF vs. 20 pages SG), which may have affected the proportion of materials read (or not read) overall.
Conclusion
Forever Free self-directed relapse prevention materials did not reduce relapse or enhance cessation over general health information when added to intensive group smoking cessation treatment with nicotine patches. However, this study lacked power to detect a small but clinically meaningful positive effect. Although self-directed learning theory suggests that adults could use these materials as a source of immediately available information as they navigate into new roles as former smokers, in practice, much of the intervention material was not read by the majority of the participants.
Footnotes
Acknowledgements
The authors would like to acknowledge the Penn State Clinical and Translational Research Institute, Penn State University CTSA, NIH/NCATS Grant Number UL1 TR000127 for providing the REDCap data management tools used in this study.
Authors’ Note
The contents of this article are solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Food and Drug Administration.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JF has done paid consulting for pharmaceutical companies involved in producing smoking cessation medications, including GSK, Pfizer, Novartis, J&J, and Cypress Bioscience. The other authors have no conflicts of interest to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an internal grant from Penn State Cancer Institute to JF. JF, SV, JY, and SH are primarily funded by the National Institute on Drug Abuse of the National Institutes of Health and the Center for Tobacco Products of the U.S. Food and Drug Administration (under Award Numbers P50-DA-036107-01 and P50-DA-036105).