
Abstract
Licensure of an HIV vaccine could reduce or eliminate HIV among vulnerable populations. However, vaccine effectiveness could be undermined by risk compensation (RC), defined by an increase in risky behavior due to a belief that the vaccine will confer protection. Interest in an HIV vaccine for reasons indicative of RC may serve as an indicator of actual RC in a postlicensure era. This study assessed factors associated with interest in an HIV vaccine for reasons indicative of RC among African American women aged 18 to 55 years, recruited from a hospital-based family planning clinic in Atlanta, Georgia (N = 321). Data were collected using audio-computer–assisted surveys. Survey items were guided by risk homeostasis theory and social cognitive theory. Multivariable logistic regression was used to assess determinants of interest in an HIV vaccine for reasons indicative of RC. Thirty-eight percent of the sample expressed interest in an HIV vaccine for at least one reason indicative of RC. In the final model, interest in an HIV vaccine for reasons indicative of RC was positively associated with higher impulsivity, perceived benefits of sexual risk behaviors, and perceived benefits of HIV vaccination; it was negatively associated with having at least some college education, positive future orientation, and self-efficacy for sex refusal. Results suggest that demographic, personality, and theory-based psychosocial factors are salient to wanting an HIV vaccine for reasons indicative of RC, and underscore the need for risk-reduction counseling alongside vaccination during the eventual rollout of an HIV vaccine.
Keywords
The U.S. HIV epidemic disproportionately affects African American women. In 2014, among all women diagnosed with HIV in the United States, an estimated 62% (5,128) were African American (Centers for Disease Control and Prevention, 2015b). Although behavioral and biomedical interventions have shown efficacy in reducing rates of HIV infection (Centers for Disease Control and Prevention, 2012; Crepaz et al., 2009), disparities still persist. Thus, HIV prevention is especially important for African American women, including many who are likely to experience social and financial barriers to care if diagnosed (Centers for Disease Control and Prevention, 2015a; Denning & DiNenno, 2015).
A safe and effective HIV vaccine has great potential to reduce or eliminate HIV among priority subpopulations (Fauci, 2008). A licensed HIV vaccine would present an opportunity for African American women to exhibit control over their risk for HIV, beyond existing interventions, despite intersecting factors that might place them at increased risk for HIV—including higher rates of poverty, limited health care access, and intimate partner violence (Bauer et al., 2002; Cavanaugh, Hansen, & Sullivan, 2010; Centers for Disease Control and Prevention, 2015b; Coker, 2007; Crosby et al., 2008; Denning & DiNenno, 2015; Mosack et al., 2010).
With at least one clinical trial supporting the safety and efficacy of a potential vaccine (Rerks-Ngarm et al., 2009) and many candidate vaccines in ongoing trials (HIV Vaccine Trials Network, 2015), the reality of a licensed HIV vaccine is closer than ever. However, the potential benefits an HIV vaccine might be reduced by risk compensation (RC), conceptualized as an increase in risky behavior due to a decrease in perceived risk of HIV (Cassell, Halperin, Shelton, & Stanton, 2006). Mathematical models suggest that RC, combined with an imperfect vaccine, could lead to increases in HIV risk and potentially apply selective pressure toward more virulent HIV strains (Massad, Coutinho, Burattini, Lopez, & Struchiner, 2006). RC could also lead to other adverse outcomes, such as increases in sexually transmitted infections or unintended pregnancies.
Guided by risk homeostasis theory (RHT; Eaton & Kalichman, 2007; Wilde, 1982) and social cognitive theory (SCT; Bandura, 1977), we sought to examine factors associated with interest in an HIV vaccine for reasons indicative of RC. Although an HIV vaccine is not yet available, investigating why women might want an HIV vaccine could provide important insights into how behavior may change if vaccinated. Interest in an HIV vaccine for reasons indicative of RC (e.g., reducing condom use or and having sex with more partners) may foreshadow actual RC in a postlicensure era. Understanding risk factors associated with such interest is essential for developing relevant, theory-based interventions to reduce risk compensatory behavior.
In the context of HIV risk, RHT posits that people have an acceptable level of HIV risk, and that they will adapt their behavior to maintain perceived risk at their accepted level (i.e., maintain risk homeostasis). Thus, if vaccinated against HIV, a person may increase sexual risk behaviors to compensate for the perceived level of protection conferred by the vaccine. In this model, perceived costs and benefits of sexual risk behaviors influence a person’s target level of HIV transmission risk, and perceived costs and benefits of HIV prevention technologies influence a person’s perceived level of HIV transmission risk. The target level of HIV transmission risk and perceived level of HIV transmission risk are balanced in risk calibration, which may lead to behavior adjustment to maintain risk at the accepted homeostatic level 1 (Eaton & Kalichman, 2007).
While RHT provides a logical framework to explain RC in the context of HIV vaccination, this theory alone may not sufficiently explain risk compensatory behaviors. SCT is a well-established health behavior theory; an abundance of research has demonstrated its applicability to a wide range of health behaviors (Bandura, 1977; Painter, Borba, Hynes, Mays, & Glanz, 2008). SCT posits that both personal factors (e.g., self-efficacy, outcome expectations) and environmental factors (e.g., social norms) influence human behavior. Studies support that key SCT constructs, such as self-efficacy to refuse sex or engage in a conversation about safer sex and peer norms supportive of unsafe sex, can influence HIV risk for African American women (Crepaz et al., 2009; DiClemente et al., 2009; DiClemente et al., 2014; O’Leary, 2001).
This study assessed demographic, behavioral, and theory-based psychosocial factors associated with interest in an HIV vaccine for reasons indicative of RC among African American women presenting for health services at a hospital-based family planning clinic in Atlanta, Georgia. We hypothesized that constructs from both RHT and SCT would be significantly associated with interest in an HIV vaccine for reasons indicative of RC.
Method
Sample, Recruitment, and Data Collection
Study participants comprised HIV-negative African American women aged 18 to 55 years presenting for clinical services at a hospital-based family planning clinic in Atlanta, Georgia. After providing verbal informed consent for study participation, eligible women completed a 1-hour audio computer-assisted self-interview (ACASI) survey. Based on previous research and theoretical application, psychosocial survey items were guided by RHT and SCT (Bandura, 1977; Eaton & Kalichman, 2007; Jackson & Blackman, 1994). The survey was developed based on (1) theoretical concepts, (2) a thorough literature review, and (3) discussions with content experts. Details regarding eligibility criteria, recruitment strategies, and data collection methods have been published elsewhere (Painter et al., 2013). This study was approved by the institutional review boards at the researchers’ institutions.
Measures
Main Outcome
The concept of an HIV vaccine was introduced to participants as follows: Right now, there is no HIV vaccine (HIV shot), but scientists are working on making one. An HIV vaccine (shot) would NOT be a cure for people who already have HIV. The vaccine would PREVENT people from getting HIV. For the next questions, please imagine that there is an HIV vaccine that is proven safe and effective, and is approved for women.
Participants were presented a list of reasons why they would or would not want an HIV vaccine. For each reason, answer choices ranged from 1 (strongly disagree) to 5 (strongly agree). Interest in an HIV vaccine for reasons indicative of RC was measured by a dichotomous variable, calculated as responding “agree” or “strongly agree” to at least one of the following reasons for wanting an HIV vaccine: “It would reduce the hassle of using condoms,” “It would allow me to take more sexual risks,” “It would allow me to have sex with a partner who is HIV positive,” or “It would allow me to have sex with more sexual partners.” All other participants, including those who were interested in the vaccine for other reasons and those who were not interested in the vaccine at all were included in the “not interested in an HIV vaccine for reasons indicative of RC” group.
Background Variables
Demographic variables included age, education level, and receipt of public assistance (Welfare, WIC, SNAP, or Section 8 housing) in the past 12 months. Sexual health history and behavior variables included previous sexually transmitted disease (STD) diagnosis, previous HIV test, condom use at last sex, multiple vaginal sex partners in the past 3 months, and at least one casual partner for any sex (vaginal, anal, or oral) in the past 3 months.
Personality variables included the following: (1) sensation seeking (8 items, α = .91, sample item: “I like doing things just for the thrill of it”; Zuckerman, Kuhlman, & Joireman, 1993), (2) impulsivity (5 items, α = .80, sample item: “I often do things on impulse”; Zuckerman et al., 1993), (3) sexual adventurism (10 items, α = .81, sample item: “Having sex with a new partner is exciting to me”; Spitalnick et al., 2007), and (4) positive future orientation (4 items, α = .90, sample item: “What happens to me in the future mostly depends on me”; Crockett, Weinman, Hankins, & Marteau, 2009). All personality items were assessed using 5-point Likert-type scales, ranging from 1 (strongly disagree) to 5 (strongly agree). Sensation seeking, impulsivity, sexual adventurism, and positive future orientation were included in analyses, because ample evidence supports the association between these personality variables and sexual risk behaviors (Burns & Dillon, 2005; McCord, 2014; Raiford et al., 2014; Robbins & Bryan, 2004; Sales et al., 2013; Spitalnick et al., 2007; Swartzendruber et al., 2013; Voisin, Hotton, Tan, & Diclemente, 2013).
Theory-Based Variables
Risk homeostasis theory
Variables included the following: (1) perceived benefits of unprotected sex (6 items, α = .90, sample item: “Having unprotected sex feels better than using a condom”); (2) perceived costs of unprotected sex (5 items, α = .89, sample item: “Having unprotected sex could cause me to get HIV”); (3) perceived benefits of HIV vaccination comprised reasons for wanting an HIV vaccine, excluding reasons indicative of RC (7 items, α = .84, sample item: “I would want an HIV vaccine because it would reduce my worry about getting HIV”); (4) perceived costs of HIV vaccination comprised reasons for not wanting an HIV vaccine (13 items, α = .90, sample item: “I would not want an HIV vaccine because I believe the vaccine might give me HIV”); and (5) perceived level of HIV transmission risk (2 items, α = .87, sample item: “What do you think is the chance you will get HIV in the future?”). RHT variables were assessed using 5-point Likert scales, ranging from 1 (strongly disagree) to 5 (strongly agree), except for perceived level of HIV transmission risk items, which were measured by 6-point Likert-type scales ranging from 1 (no chance = 0%), to 6 (very strong chance = 81%-100%).
Social cognitive theory
Variables included the following: (1) self-efficacy for sex refusal (7 items, α = .89, sample item: “How sure are you that you would be able to say NO to someone who refuses to wear a condom?”): Items were assessed using 4-point Likert-type scales, ranging from 1 (very hard to say no) to 4 (very easy to say no); (2) self-efficacy for sex communication (6 items, α = .89, sample item: “How hard is it for you to ask how many sex partners he has had?”): Items were assessed using 4-point Likert scales, ranging from 1 (very hard) to 4 (very easy); (3) negative outcome expectations for condom negotiation (4 items, α = .89, sample item: “If I asked my partner to use a condom, he would think that I don’t trust him”; Wingood & DiClemente, 1998): Items were assessed using 5-point Likert-type scales, ranging from 1 (strongly disagree) to 5 (strongly agree); (4) peer norms supportive of unsafe sex (5 items, α = .85, sample item: “How many of your friends think that it’s okay to have sex without a condom?”; DiClemente et al., 2004): Items were assessed using 5-point Likert-type scales, ranging from 1 (none) to 4 (all).
Analysis
Items comprising personality and theory-based variables were combined into scales, and Cronbach’s alphas were calculated to assess internal consistency. Bivariate (unadjusted) logistic regression analyses were conducted to assess the association between background and theory-based variables with interest in an HIV vaccine for reasons indicative of RC. Only variables associated with the outcome at the p ≤ .10 level in bivariate analyses were included in multivariable analyses. Pearson correlations were used to check for multicollinearity among predictor variables; no evidence of multicollinearity was present. Multivariable logistic regression was used to identify variables associated with interest in an HIV vaccine for reasons indicative of RC. Three multivariable models were created, where independent variables included background factors alone (Model 1), background factors plus RHT variables (Model 2), and background factors plus RHT and SCT variables (Model 3).
Results
A total of 321 women participated in the study. The mean age was 27.4, and 35.3% of participants had at least some college education. Most participants (78.5%) received some type of public assistance in the past 12 months. Almost all participants (95.3%) had previously been tested for HIV, and 65.4% had previously been diagnosed with an STD.
Almost all participants reported at least one reason for wanting an HIV vaccine (95.3%). The most common reasons for wanting an HIV vaccine were “The vaccine could prevent me from getting HIV” (84.7%) and “It would reduce my worry about getting HIV” (84.4%) (Table 1). Reasons indicative of RC comprised the least common reasons for wanting an HIV vaccine. Overall, 122 participants (38.0%) reported interest in an HIV vaccine for at least one reason indicative of RC. Comparatively, over half of women (59.5%) reported at least one reason for not wanting an HIV vaccine. The most common reason for not wanting an HIV vaccine was “I would worry about vaccine safety or side effects” (40.2%).
Reasons for Wanting or Not Wanting an HIV Vaccine Among African American Adult Women Aged 18 to 55 Years Seeking Health Services at a Family Planning Clinic in Atlanta, GA (N = 321).
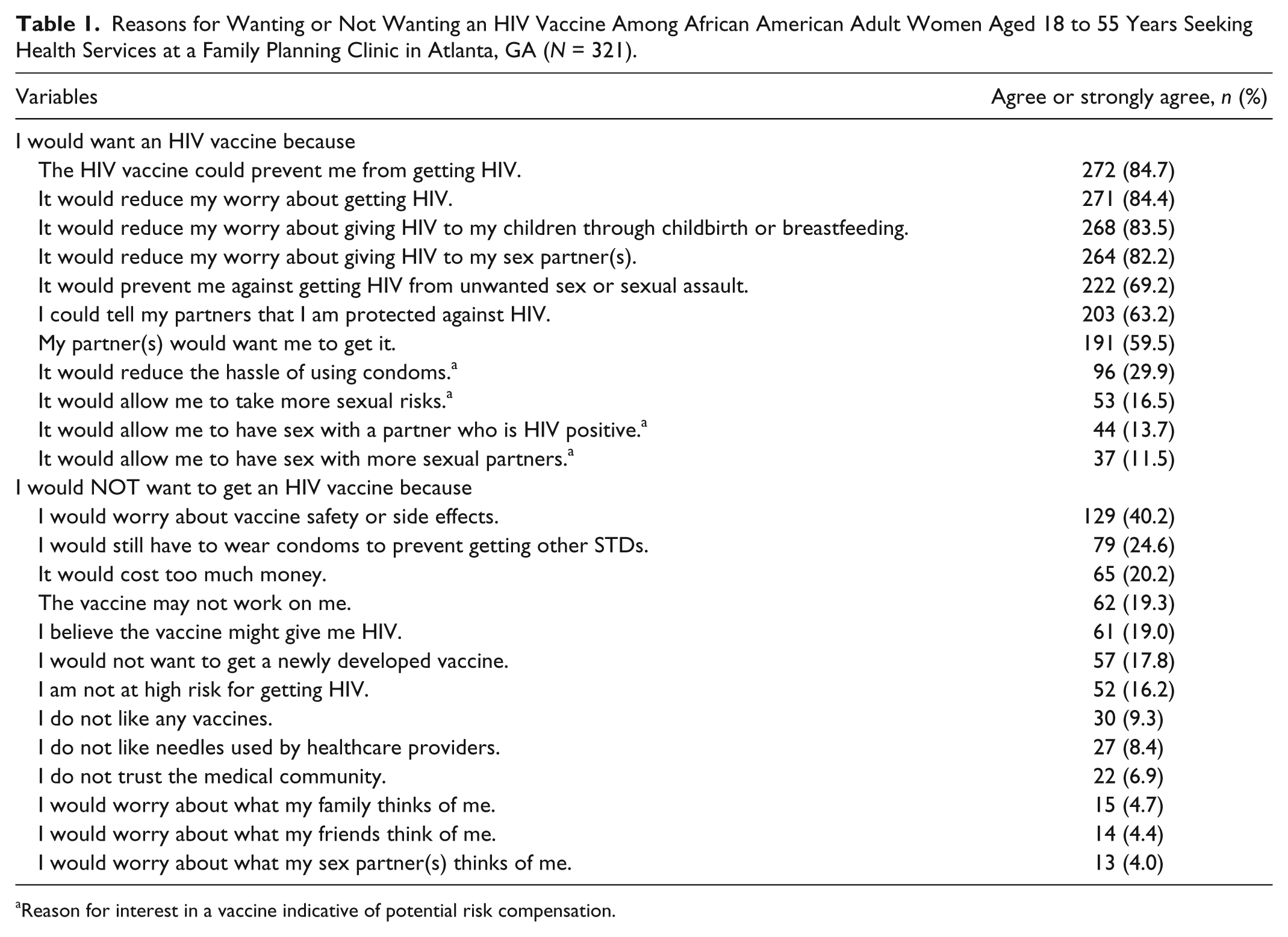
Reason for interest in a vaccine indicative of potential risk compensation.
In bivariate analyses, participants with higher scores on scales measuring sensation seeking, impulsivity, sexual adventurism, perceived benefits of sexual risk behaviors, perceived benefits of HIV vaccination, and negative outcome expectations for condom negotiation were significantly more likely to express interest in an HIV vaccine for reasons indicative of RC (Table 2). Participants with at least some college education and higher scores on scales measuring positive future orientation and self-efficacy for sex refusal were significantly less likely to express interest in an HIV vaccine for reasons indicative of RC.
Participant Characteristics by Interest in an HIV Vaccine for Reasons Indicative of Risk Compensation Among African American Adult Women Aged 18 to 55 Years Seeking Health Services at a Family Planning Clinic in Atlanta, GA (N = 321).
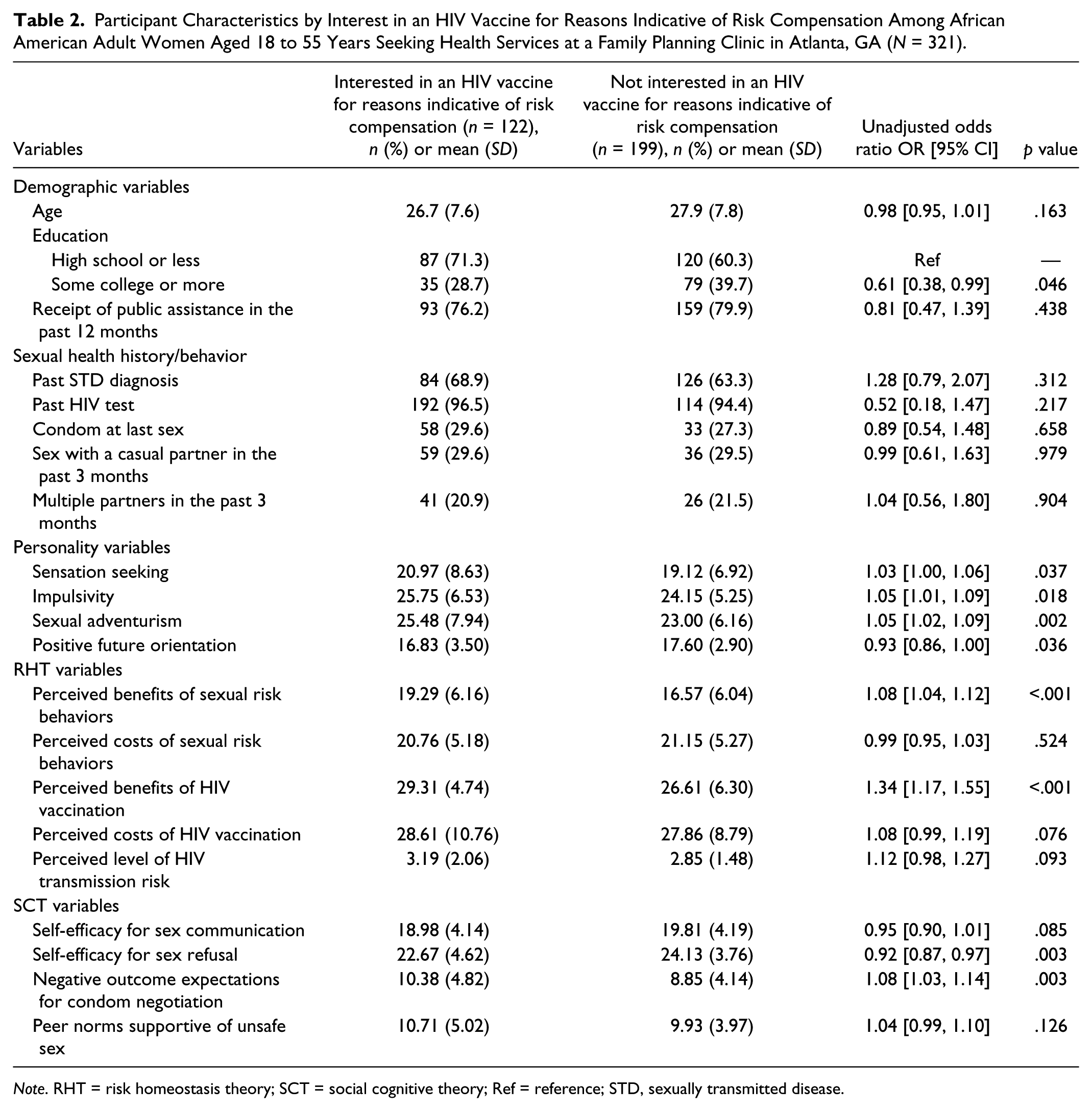
Note. RHT = risk homeostasis theory; SCT = social cognitive theory; Ref = reference; STD, sexually transmitted disease.
In Model 1 (background variables only), participants with higher scores on scales measuring impulsivity (aOR = 1.07, CI [1.01, 1.13]) and sexual adventurism (aOR = 1.07, CI [1.02, 1.12]) were significantly more likely to express interest in an HIV vaccine for reasons indicative of RC (Table 3). Participants with at least some college education (aOR = 0.55, CI [0.33, 0.93]) and higher scores on the scale measuring positive future orientation (aOR = 0.91, CI [0.84, 0.99]) were significantly less likely to express interest in an HIV vaccine for reasons indicative of RC.
Factors Associated With Interest in an HIV Vaccine for Reasons Indicative of Risk Compensation Among African American Adult Women Aged 18 to 55 Years Seeking Health Services at a Family Planning Clinic in Atlanta, GA (N = 321). a
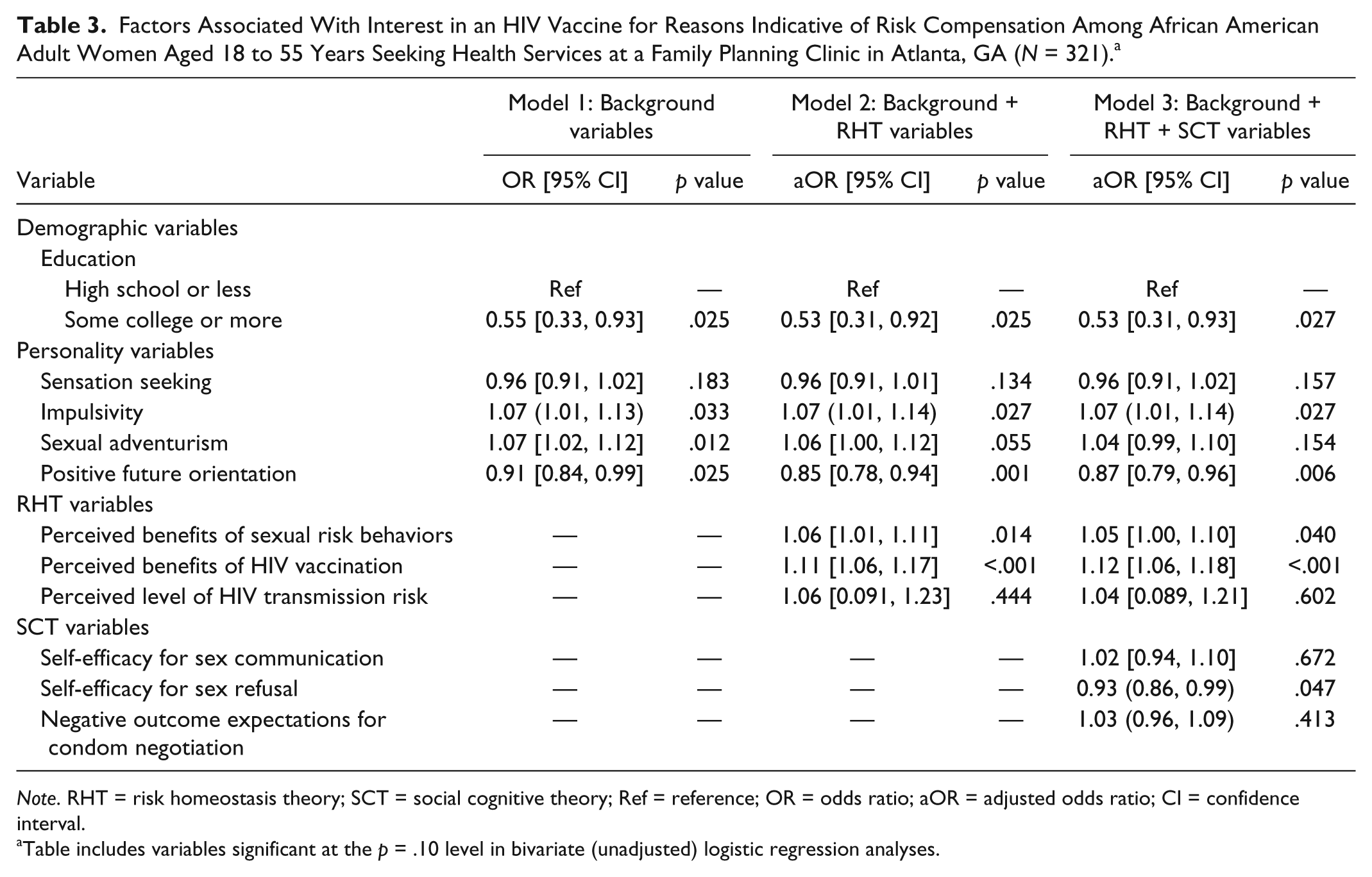
Note. RHT = risk homeostasis theory; SCT = social cognitive theory; Ref = reference; OR = odds ratio; aOR = adjusted odds ratio; CI = confidence interval.
Table includes variables significant at the p = .10 level in bivariate (unadjusted) logistic regression analyses.
In Model 2 (background plus RHT variables), participants with higher scores on scales measuring impulsivity (aOR = 1.07, CI [1.01, 1.14]), perceived benefits of sexual risk behaviors (aOR = 1.06, CI [1.01, 1.11]), and perceived benefits of HIV vaccination (aOR = 1.11, 95% CI [1.06, 1.17]) were significantly more likely to express interest in an HIV vaccine for reasons indicative of RC. Participants with at least some college education (aOR = 0.53, CI [0.31, 0.92]) and higher scores on the scale measuring positive future orientation (OR = 0.85, CI [0.78, 0.94]) were significantly less likely to express interest in an HIV vaccine for reasons indicative of RC.
In Model 3 (background plus RHT and SCT variables), participants with higher scores on scales measuring impulsivity (aOR = 1.07, CI [1.01, 1.14]) and perceived benefits of HIV vaccination (aOR = 1.12, CI [1.06, 1.18]) were significantly more likely to express interest in an HIV vaccine for reasons indicative of RC. Perceived benefits of sexual risk behaviors (aOR = 1.05, 95% CI [1.00, 1.10]) approached statistical significance. Participants with at least some college education (OR = 0.53, CI [0.31, 0.93]) and higher scores on scales measuring positive future orientation (OR = 0.87, CI [0.79, 0.96]) and self-efficacy for sex refusal (OR = 0.93, CI [0.86, 0.99]) were significantly less likely to express interest in an HIV vaccine for reasons indicative of RC.
Discussion
This study is novel in its assessment of demographic, behavioral, and theory-based psychosocial factors associated with interest in an HIV vaccine for reasons indicative of RC among African American women. Almost all participants reported at least one reason for wanting an HIV vaccine. Consistent with previous research, this finding indicates that, once licensed, interest in an HIV vaccine may be high (Newman & Logie, 2010; Painter et al., 2013; Rudy et al., 2005). The most common reasons for wanting an HIV vaccine were not related to RC; however, a substantial proportion (38%) wanted an HIV vaccine for at least one reason indicative of RC. This finding supports general concerns about RC associated with HIV vaccination. Studies of other priority subpopulations, including at-risk adults in Los Angeles (Newman et al., 2009), volunteers undergoing screening for participation in phase I/II HIV vaccine trials in South Africa (Andersson et al., 2012), and participants of HIV vaccine trials in the United States, Caribbean, South America (Novak et al., 2013), and South Africa (Gray et al., 2013) have similarly demonstrated potential for increased risk behavior following HIV vaccination (Eaton & Kalichman, 2007).
It should be noted that there has been no evidence of RCs associated with vaccination against human papillomavirus (HPV), another sexually transmitted disease (Bednarczyk, Davis, Ault, Orenstein, & Omer, 2012; Liddon, Leichliter, & Markowitz, 2012; Zimet, Rosenberger, Fisher, Perez, & Stupiansky, 2013). However, key differences between HPV and HIV which could affect risk appraisal must be acknowledged. First, HIV is a more widely known and feared disease compared to HPV (Samkange-Zeeb, Pöttgen, & Zeeb, 2013; Samkange-Zeeb, Spallek, & Zeeb, 2011). Second, while HIV and HPV can both be spread through sexual contact, HIV can also be spread through sharing needles, receiving blood transfusions, and from mother to child via pregnancy, birth, or breastfeeding (Centers for Disease Control and Prevention, 2016). Each of these factors might affect reasons for wanting an HIV vaccine, including reasons related to RC.
Another novel aspect to this study was its assessment of constructs from multiple theories, including RHT and SCT, in explaining interest in an HIV vaccine for reasons indicative of RC. Our hypothesis that constructs from both theories would be significant was supported, albeit with small effects. From RHT, perceived benefits of unprotected sex and perceived benefits of an HIV vaccination for reasons other than RC were associated with increased interest in a vaccine for reasons indicative of RC. In the context of RHT, people with a higher valuation of the benefits of unprotected sex or the benefits of the HIV vaccine might have a higher target level of HIV transmission risk, and therefore be more prone to increasing their risk behavior after receiving an HIV vaccine to achieve risk homeostasis (Eaton & Kalichman, 2007). This finding highlights that, once an HIV vaccine is licensed for use, risk reduction counseling should highlight the actual risks and benefits of the vaccine.
From SCT, participants with increased self-efficacy for sex refusal were less likely to express interest in a vaccine for RC, although the effect size was small. A person more empowered to refuse sex or to insist a partner use a condom might also feel more empowered to reduce engagement in sexual risk behavior after HIV vaccination. Furthermore, participants who are more empowered to refuse sex may find condom use less of a burden, lessening their interest in compensatory risky behavior following vaccination. Self-efficacy for sex refusal has been identified as a key mediator of risk behavior among African American women in previous research (Salazar et al., 2004) and may similarly affect RC following HIV vaccination. Further studies will be needed to explore this area.
Of note, participants with increased educational attainment were less likely to express interest in an HIV vaccine for reasons indicative of RC. In all analyses, participants who completed at least some college were less likely to want an HIV vaccine for reasons indicative of RC compared with participants who were less educated. This was the most robust association found in our study, and it highlights the important link between educational attainment and HIV risk among African American women (Klein, Sterk, & Elifson, 2016; Painter, Wingood, DiClemente, Depadilla, & Simpson-Robinson, 2012). There are several possible explanations for this association. It is possible that women with higher levels of education are better able to understand, without explicit counseling, that an HIV vaccine would not provide protection against STIs or pregnancy, and therefore be less interested in getting an HIV vaccine for reasons indicative of RC. It is also possible that educational attainment, a structural determinant of HIV risk (Wingood & DiClemente, 2002), might affect more proximal determinants, such as self-efficacy for sex refusal. Finally, there could be underlying personality factors, such as positive future orientation, simultaneously affecting both educational attainment and interest in an HIV vaccine for reasons indicative of RC (Painter et al., 2012; Robbins & Bryan, 2004; Sales et al., 2009).
Among personality variables, participants with increased positive future orientation were less likely to express interest in an HIV vaccine for reasons indicative of RC, while impulsivity was predictive of interest in an HIV vaccine for reasons indicative of RC. These associations remained significant across all analyses, although the effect sizes were small. Impulsivity has been identified as a risk factor for sexual risk behaviors among African American women (McCord, 2014; Swartzendruber et al., 2013), and it may similarly operate as a risk factor for RC associated with HIV vaccination. Positive future orientation has been identified as a predictor of condom use among African American college students (Burns & Dillon, 2005), while low future prospects have been associated with increased sexual risk behavior among African American women (Raiford et al., 2014). Women who are more optimistic about their futures might be more likely to protect their long-term health and welfare (Robbins & Bryan, 2004), and therefore less likely to express interest in an HIV vaccine for reasons indicative of RC. Further research is needed to determine if these associations hold true in the context of HIV vaccination.
Limitations
This study is subject to limitations. First, since no licensed HIV vaccine exists, it may be difficult for participants to accurately anticipate pros and cons of vaccination. Once a vaccine is licensed, vaccine characteristics (e.g., efficacy and cost) may affect interest. Second, this study examined behavioral intent, as opposed to actual behaviors. Thus, persons who expressed interest in an HIV vaccine to reduce the hassle of using condoms might not actually stop using condoms if vaccinated. Third, constructs from both RHT and SCT were significant in this study, but with only small effects. Although small effect sizes are common in behavioral science research, they are nonetheless difficult to interpret. In this case, small effect sizes may be related to the limited sample size, single recruitment setting, or recruitment of only individuals accessing health care. Further research will help determine if these constructs are important for actual RC. Fourth, the causal effects of predictor variables could not be determined due to cross-sectional study design. Fifth, even with ACASI, social desirability may have limited participant’s answers about sexual risk-taking, possibly leading to underestimated effects. Sixth, elicitation interviews were not conducted prior to survey development; thus, additional reasons for wanting or not wanting an HIV vaccine may not have been captured. Finally, the study population comprised sexually active African American women aged 18 to 55 years in a low-income clinic setting in Atlanta, Georgia. Thus, the results of this study may not be generalizable to broader populations.
Implications for Theory and Practice
Within the context of RHT and SCT, interventions that attempt to influence RC can act on either an individual’s target level of risk or perceived risks and benefits of an intervention. Principles of RHT and SCT can guide public health interventions to mitigate the impacts of RC related to HIV vaccination, once a vaccine becomes available. Findings from this study stress the need for health educators, clinicians, and researchers to emphasize the importance of continued condom use in conjunction with HIV vaccination, particularly if the vaccine is less than 100% effective.
The need to combine vaccination with other HIV prevention methods, such as condom use, must be stressed continually over time. This may prove to be a challenge, particularly if the vaccine entails only a single dose or a several dose series (Hammer et al., 2013; Rerks-Ngarm et al., 2009). After receipt of the vaccine, people may discontinue seeking medical care. This represents a sharp contrast from preexposure prophylaxis, which requires routine health care visits to obtain medication, presenting multiple opportunities for risk reduction counseling. Medical and public health professionals will need to develop creative strategies for sustaining risk reduction counseling over time, particularly with hard-to-reach populations.
Our findings further suggest that the ability to refuse sex may be an important contributor to reducing RC among African American women. Interventions to increase self-efficacy for sex refusal and address partner-level factors, such as intimate partner violence and sexual assault prevention (Crepaz et al., 2009; Stockman, Lucea, & Campbell, 2013), may be beneficial in conjunction with HIV vaccination. Findings also indicate that efforts to understand and address the influence of educational attainment and positive future orientation, especially as it pertains to acceptable levels of risk related to HIV infection, are warranted.
Conclusion
Findings of this study support concerns about potential RC associated with HIV vaccination. Findings also demonstrate that educational level, as well as constructs from at least two behavioral change theories, RHT and SCT, might be useful in explaining RC associated with HIV vaccination among African American women. These findings highlight the continued need for research to explore the potential for RC associated with HIV vaccination and underscore the need for risk-reduction counseling alongside vaccination during the eventual rollout of an HIV vaccine.
Footnotes
Acknowledgements
The authors wish to thank the Grady Family Planning Clinic staff for their support of the HVARC study. We would also like to thank the HVARC research assistants who assisted with data collection, and Dianne Miller for providing administrative support. Finally, we would like to thank the study participants.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Allergy and Infectious Diseases, the National Institutes of Health, or Emory’s Center for AIDS Research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Award Number T32AI074492 from the National Institute of Allergy and Infectious Diseases and Award Number P30 AI050409 from Emory’s Center for AIDS Research.