
Abstract
Deaths of despair (DOD) is a new term appearing in public health literature to describe deaths attributable to suicide, liver disease, and drug overdose. In Florida, suicide and liver disease are the 8th and 10th leading causes of death, respectively. Additional mortality data show that the rate of drug overdose deaths in Florida is 12.5% higher than the suicide death rate. Some have hypothesized that economic social determinants of health (SDH) may be responsible for the recent increase in DOD. The current study, using secondary data, sought to identify what county-level SDH were significantly associated with county-level DOD. Using backward regression methodology, the results of the analysis indicate that 44% of the variance in county-level DOD is significantly associated with six county-level SDH: (a) Recent Medical Checkup, (b) Income, (c) Education Level, (d) Age, (e) Mental Health Professionals, and (f) the Income × Age interaction term. Higher than average income, age, and mental health professionals in a Florida county was associated with significantly higher rates of DOD. Higher than average levels of education and recent checkups in a Florida county were associated with a significant decrease in DOD. Possible explanations and implications are discussed.
After economic research led to the discovery of major increases in mortality and morbidity rates from suicide, drug overdose, and liver disease in the United States, Case and Deaton (2015) introduced a new term to encapsulate the phenomenon: Deaths of Despair. The Deaths of Despair (DOD) construct illuminated the element of despair that is associated with the self-induced means by which these deaths occur as well as with the feeling of hopelessness that might precede them (Case & Deaton, 2015).
Suicide is the 10th leading cause of death in the United States, with 44,965 deaths in 2016 (American Foundation for Suicide Prevention, 2016). In the United States, the suicide death rate is 13.9 per 100,000, accounts for 1.6% of deaths in the United States annually, and is increasing across the country with half of the states seeing an increase of at least 30% since 1999 (Centers for Disease Control and Prevention [CDC], 2018; Drapeau & McIntosh, 2017). The death rate associated with drug overdose, particularly prescription opioid overdose, is increasing. Between 1999 and 2002, there was a 129.2% increase in unintentional opioid overdoses in the United States (Meyer, Patel, Rattana, Quock, & Mody, 2014). Similarly, there was a 467.7% increase in reported methadone deaths between 1999 and 2005 (Martins, Sampson, Cerdá, & Galea, 2015). Recently, heroin overdose deaths tripled between 2010 and 2015 (Dasgupta, Beletsky, & Ciccarone, 2018). According to the CDC (2017a), deaths from liver disease rose by 31% from 2000 to 2015 for people ages 45 to 64 years. The toxic influence of alcohol on the liver is the primary cause of liver disease (Penny, 2013).
Stein, Gennuso, Ugboaja, and Remington (2017) noted that the observed increases in DOD were more notable among non-Hispanic Whites. Communities of color continue to evidence high rates of DOD, though they did not experience the same acute increase in DOD. Diez Roux (2017) hypothesized that this disparate impact is the result of White communities encountering economic hardships that are new to their lived experience. Scutchfield and Keck (2017) offered a similar explanation, saying that “Whites have a greater expectation that they will have a job, family, and reasonable economic life” (p. 1565) while communities of color may not have those expectations because of racism, oppression, and discrimination. Results from Meit, Heffernan, Tanenbaum, and Hoffmann (2017) show that counties with higher economic distress had higher DOD rates than counties with lower economic distress. Case and Deaton (2017) found that DOD rates for individuals with a high school degree or less are rising much faster than the rates for individuals with at least a 4-year college degree. These findings have called attention to the critical role of social factors in DOD.
Braveman and Gottlieb (2014) conceptualized such social factors as the “causes of the causes” (p. 19) of ill health. The World Health Organization Commission on Social Determinants of Health (CSDH, 2008) identified several critical social factors associated with health outcomes, calling them social determinants of health and health inequities (SDH). These include, among others, access to adequate housing, access to health care, adequate health insurance, available childcare, adequate education, consistent employment, racial equality, gender equality, and stable income (Braveman, Egerter, & Williams, 2011; CSDH, 2008). The CSDH (2008) noted that, in matters of public health, a fuller conceptualization of SDH can aid in health monitoring endeavors and in translating research to practice. This may be especially true when there are sudden and notable shifts in health status of a community, region, or country and/or when a community, region, or country evidences dramatic and acute health needs.
Florida has the third highest number of alcohol dependence and abuse cases, outranked only by Texas and California (The Kaiser Family Foundation, 2015b), and is in the highest category for illicit drug abuse and dependence (The Kaiser Family Foundation, 2014b). Florida residents with problematic alcohol use have also historically not gotten the treatment that they need (The Kaiser Family Foundation, 2014a). The state evidences the second highest number of prescription opioid overdose deaths in the United States (The Kaiser Family Foundation, 2016b). As with alcohol use, Florida was among the highest category of states with residents that needed but did not receive treatment for drug abuse and dependence (The Kaiser Family Foundation, 2014c). Finally, data show that Florida is among the top five states with respect to mental illness prevalence (The Kaiser Family Foundation, 2015a). Suicide is the 8th leading causes of death in the state (CDC, 2017c). Florida is among the highest in Health Professional Shortage Areas (HPSAs) in the United States, ranking the fourth highest both for primary health professionals (The Kaiser Family Foundation, 2016c) and mental healthcare professionals (The Kaiser Family Foundation, 2016a). In an attempt to address the state’s poor health standings, Florida county health departments are involved in efforts such as partnering with public health accreditation boards and applying tools such as Environmental Public Health Performance Standards self-assessment and the Protocol for Assessing Community Excellence in Environmental Health (Price, Grigg, & Byrne, 2013). Despite this, Florida is ranked 48th in health system performance in the United States, determined by The Commonwealth Fund health care scorecard (Radley, McCarthy, & Hayes, 2018).
Considering all the aforementioned research, the current analysis seeks to answer the research question: Do the SDH create a viable model to explain a significant portion of the variance in DOD within Florida counties? The aim of this is to (a) clarify the relationship between SDH associated with DOD and (b) elucidate the DOD research implications in Florida.
Method
Sample
Data were collected for all 67 Florida counties. These data were at the county level rather than at the individual resident level. As such, the independent variables included in the current analysis represent the aggregate of the county as a whole, rather than any specific or prototypical resident within the county.
Measures
The Florida Department of Health (DOH) website (DOH, 2018) contained all relevant data and was thus the sole data source. The Florida DOH obtained these data from their own records, from other Florida departments, and from the U.S. Census Bureau. A full list of the data sources is available at http://www.flhealthcharts.com/Charts/documents/training/FLHealthCHARTSCalendar.pdf.
The dependent variable, deaths of despair, was conceptualized as the summed rate (per 100,000) of deaths from alcoholic liver disease, unintentional poisoning, and suicide. Unintentional poisoning is the term for drug overdose used within the DOH database, and is the language used by the International Classification of Diseases (see CDC, 2013). The independent variables were SDH hypothesized to be associated with DOD. These included (a) Regular Medical Care, (b) Insurance Coverage, (c) Income, (d) Education, (e) County Health Expenditures, (f) Unemployment, (g) Unstable Housing, (h) Age, (i) Mental Health Care Availability, and (j) Race. These were operationalized as (a) Percentage of Adults with a Medical Checkup in the Last 12 months, (b) Percentage of Adults with any Type of Health Insurance, (c) Median Household Income, (d) Percentage of Adults over 25 with a Bachelor’s Degree or Higher, (e) County Public Health Department Expenditures in Dollars per Resident, (f) Unemployment Rate, (g) Percentage of Population that Had Lived in a Different House 1 year Earlier, (h) Median Age, (i) Number of Licensed Social Workers, Psychologists, Marriage and Family Therapists, and Counselors per 10,000 Residents, and (j) Percentage of Residents who are White.
Means and standard deviations for all variables are included in Table 1. Due to DOH data collection cycles, not all variables were available for the same years. The dependent variable was the 2016 rate, the most recent year available. Table 1 includes the year of the data used for each variable.
Descriptive Statistics.
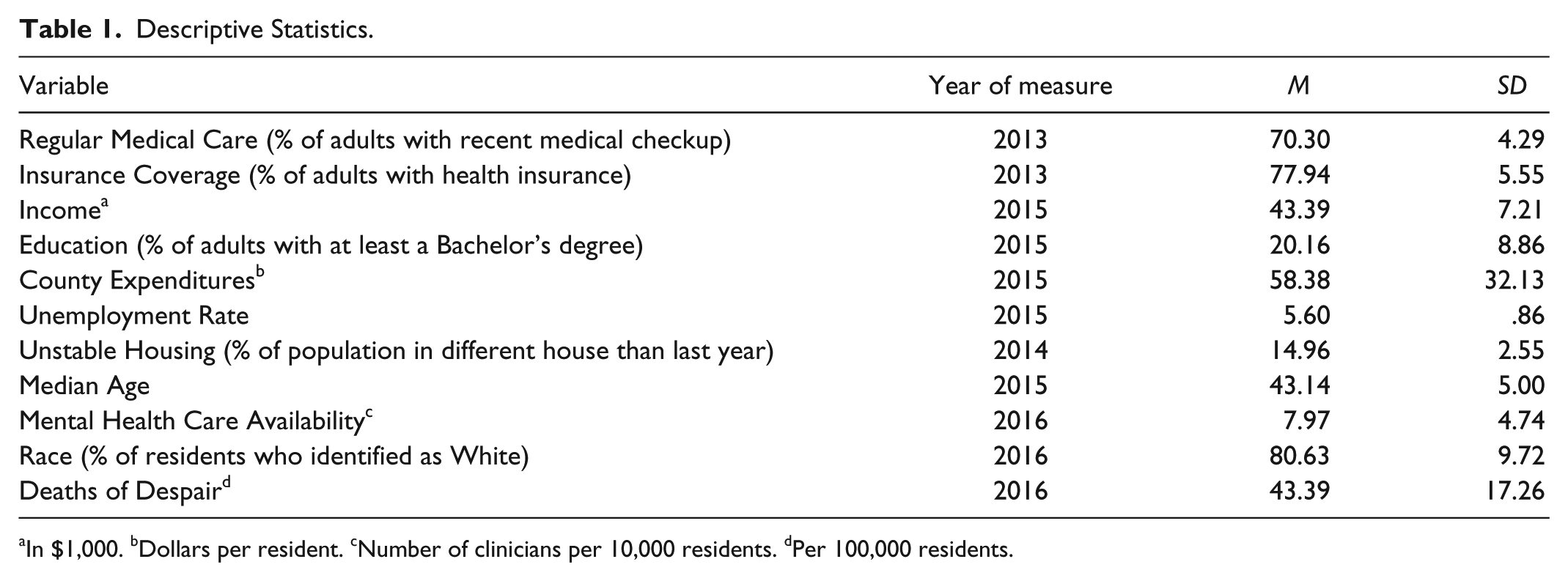
In $1,000. bDollars per resident. cNumber of clinicians per 10,000 residents. dPer 100,000 residents.
Analysis
All analyses were conducted using SPSS version 24.0 for Windows. All independent variables were centered in order to improve interpretability of results. Also, independent variable data points that were more than 2.5 standard deviations from the mean were removed from the analysis. A total of 10 counties were removed because of outlier data, resulting in a final sample size of n = 57. Of those 10 counties, 6 were removed for having one outlier data point. The highest number of outlier data points was three (one county).
Regression assumptions were tested and no deviations from linearity or homoscedasticity were evidenced. One variable, County Expenditures, did evidence a deviation in normality with a positive skew. To correct for this, the square root of all County Expenditure values was used in the regression analysis. Multicollinearity diagnostics showed a mean variable inflation factor of 2.66 (maximum = 6.04) and a mean tolerance level of .58 (minimum = .17). In the aggregate, these multicollinearity checks did not reveal a cause for significant concern.
A backwards multiple regression was conducted to identify the model containing the fewest individual predictors of DOD. Considering the constraints on sample size, a criterion power analysis was conducted to identify the required alpha for use in the modeling. With an anticipated effect size of .25, β = .20, n = 57, and 11 independent variables (the model included an Income × Age interaction term after initial descriptive statistics and regression assumption testing revealed a possible relationship between these two variables), the critical alpha was calculated as α = .14. This was the alpha used as the criterion for removal from the model at each step.
Results
The analysis first sought to identify geographic patterns in the DOD rates (per 100,000) across Florida. The five counties with the highest DOD rates were Manatee (81.50), Citrus (79.80), Monroe (79.50), Marion (71.50), and Nassau (68.3). The five counties with the lowest DOD rates were Madison (3.30), Liberty (9.50), Lafayette (10.50), Gulf (14.40), and Calhoun (15.40). Some counties evidenced notable absolute changes in DOD rates between 2015 and 2016. The counties with the greatest increase in DOD rates were Glades (38.10), Citrus (33.10), and Jefferson (32.70). The counties with the greatest decrease in DOD rates were Jackson (−39.90), Gulf (−24.60), and Lafayette (−23.10). Figures 1 through 5 show choropleth maps of various iterations of DOD.
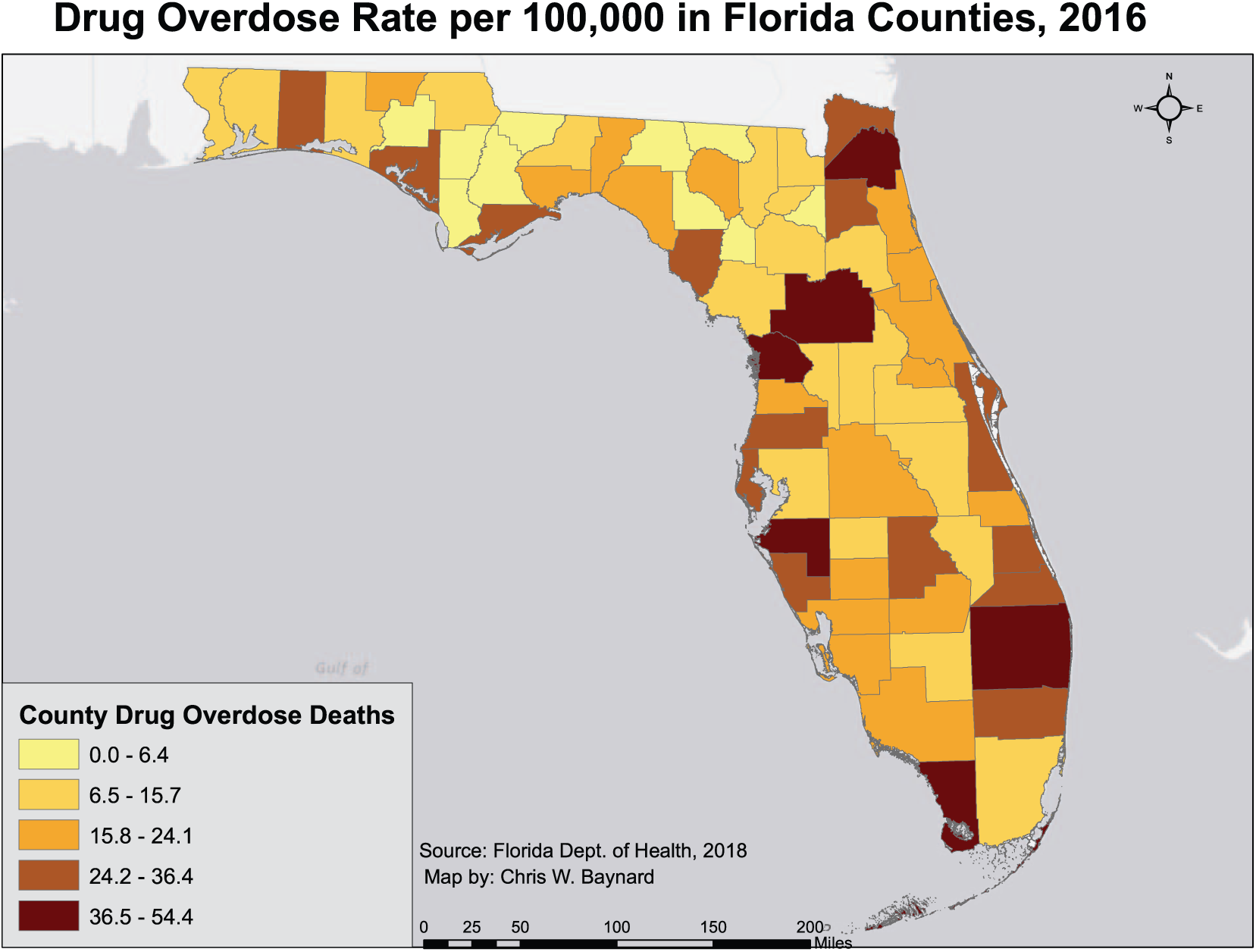
A choropleth map of the drug overdose death rate in Florida counties.
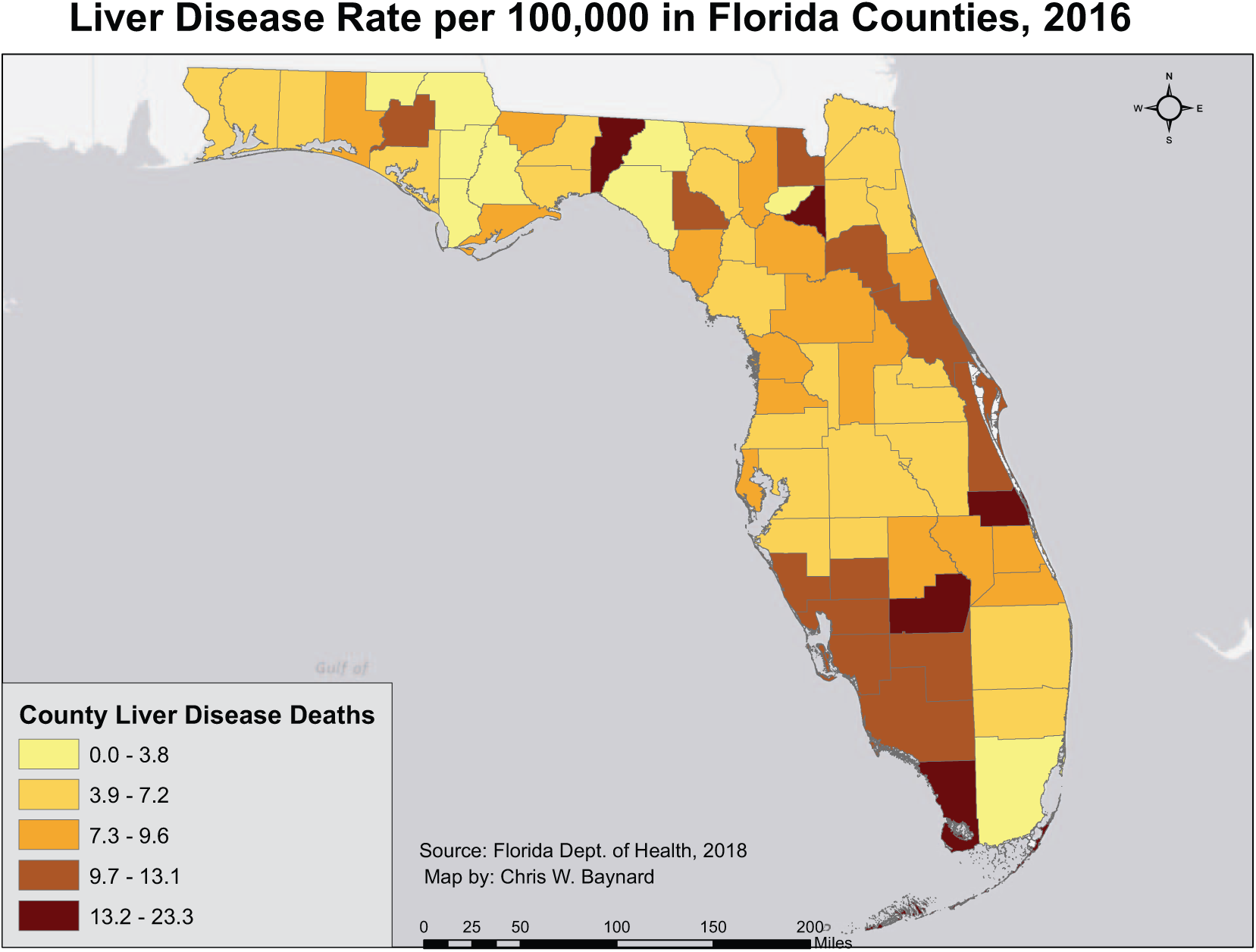
A choropleth map of the alcoholic liver disease death rate in Florida counties.
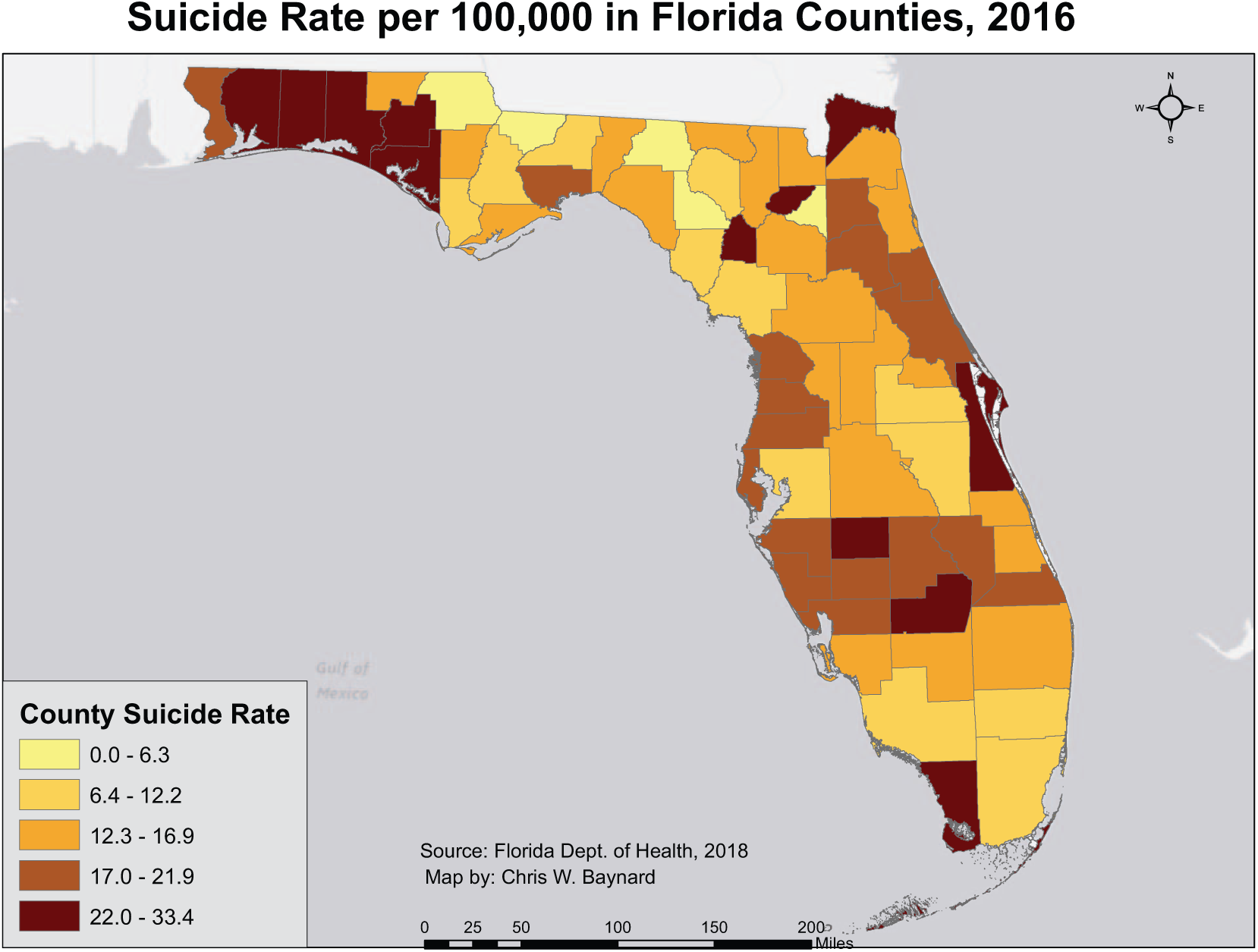
A choropleth map of the suicide death rate in Florida counties.
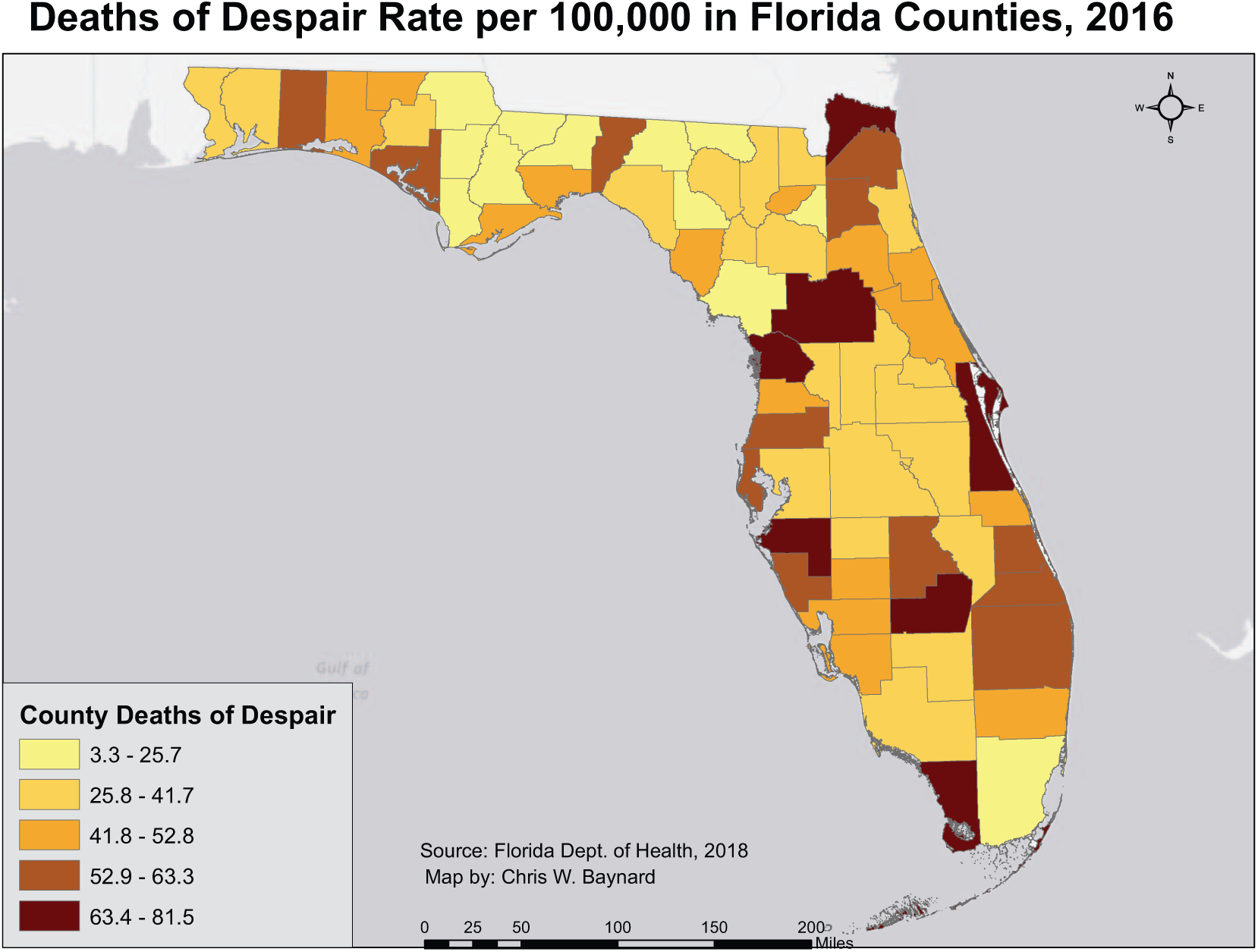
A choropleth map of the death of despair death rate in Florida counties.
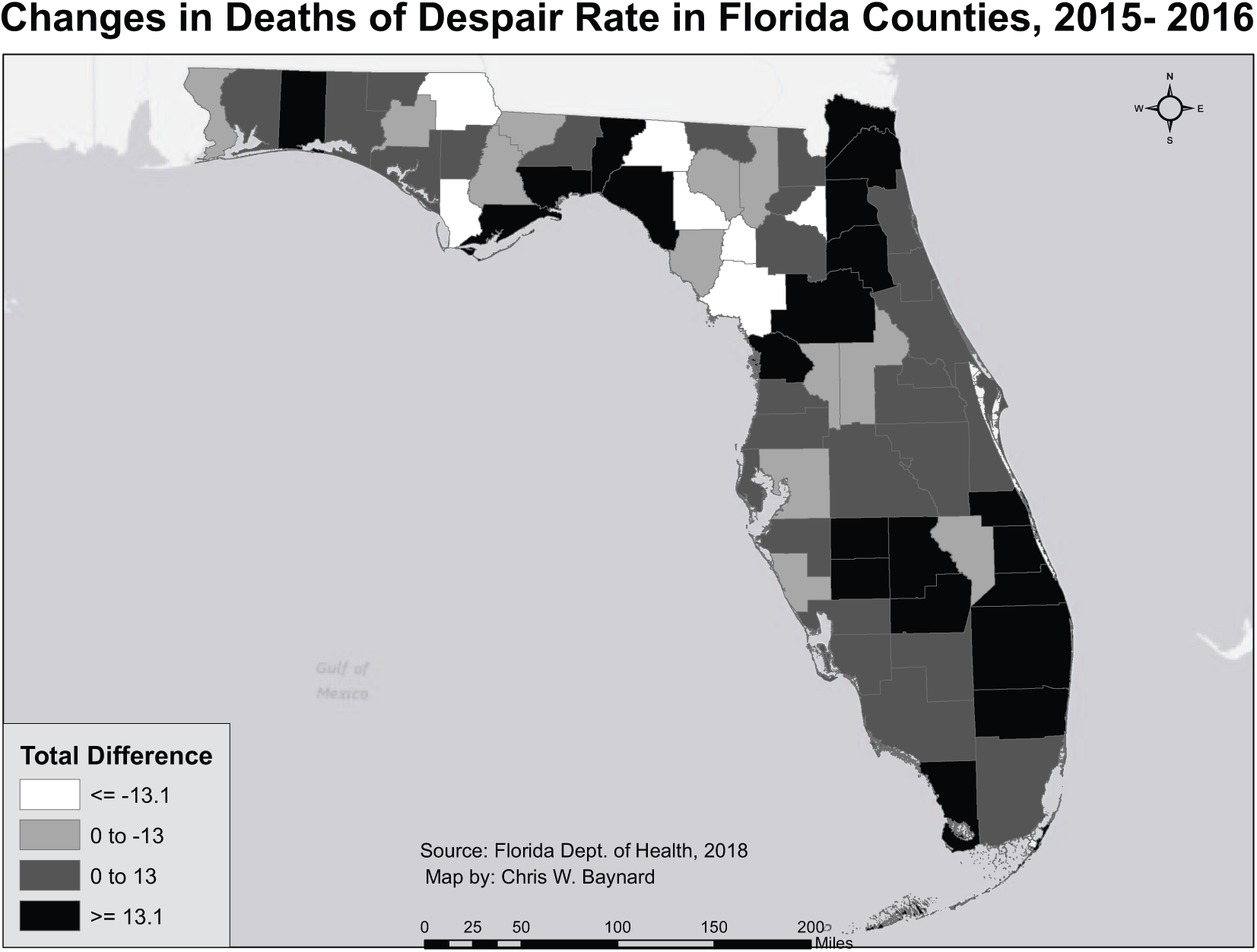
A choropleth map of the absolute change in death of despair rates in Florida counties from 2015 to 2016.Positive numbers (in red) represent an increase while negative numbers (in blue) represent a decrease.
The initial full model, with all 11 independent variables entered into the regression, was statistically significant, F(11, 44) = 4.38, p < .001, R2 = 40. The backwards regression retained 6 of the initial 11 variables in the final model: (a) Regular Medical Care, (b) Income, (c) Education, (d) Age, (e) Mental Health Care Availability, and (f) the Income × Age interaction term. This model was statistically significant, F(6, 49) = 8.21, p < .001, accounted for approximately 44% of the variance in DOD (see Table 2), and produced a mean residual of .532. Though the alpha used as the backward regression criterion was α = .14, the highest p value in the final model was half that (p = .07). All other p values were under the traditional alpha of α = .05.
Results of Linear Regression Predicting Deaths of Despair.
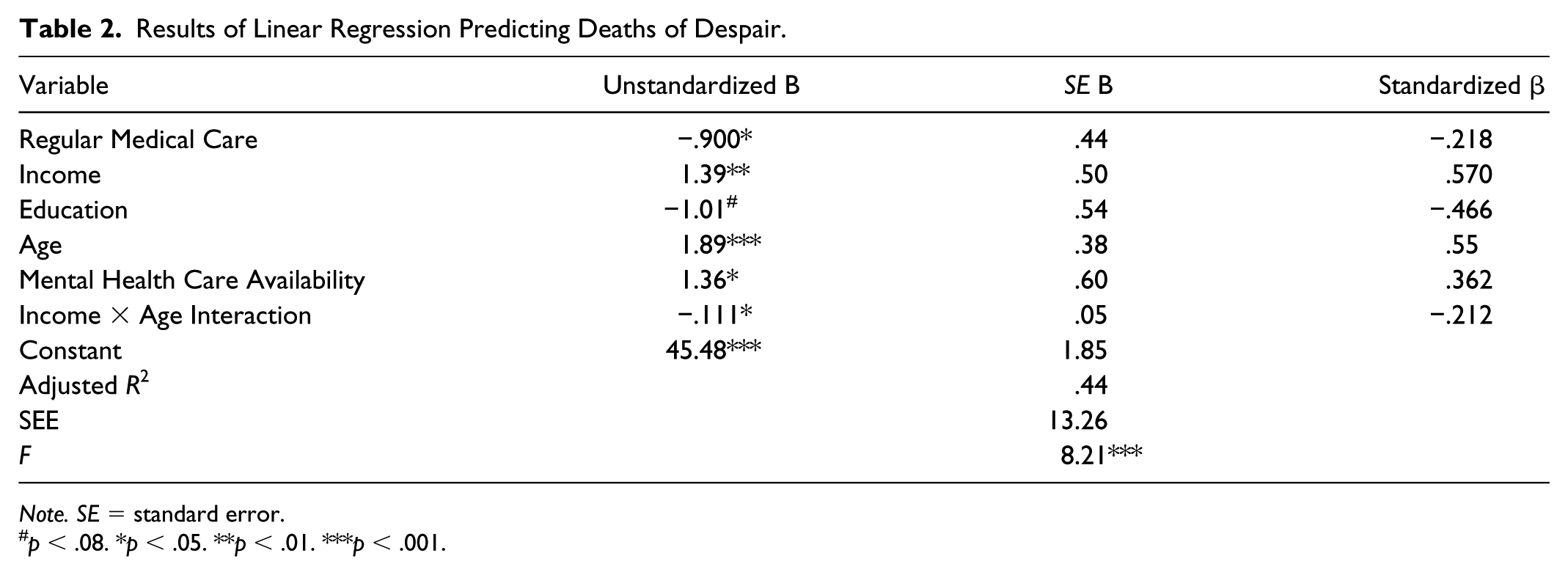
Note. SE = standard error.
p < .08. *p < .05. **p < .01. ***p < .001.
Higher than average income (p = .007), median age (p < .001), and mental health professionals in a Florida county (p = .027) were associated with significantly higher DOD rates in that county. Conversely, higher than average levels of education (p = .066) and recent checkups in a Florida county (p = .046) were associated with a significant decrease in DOD in that county. Also, the interaction between income and age was significant in the negative direction (p = .04; see Figure 6).
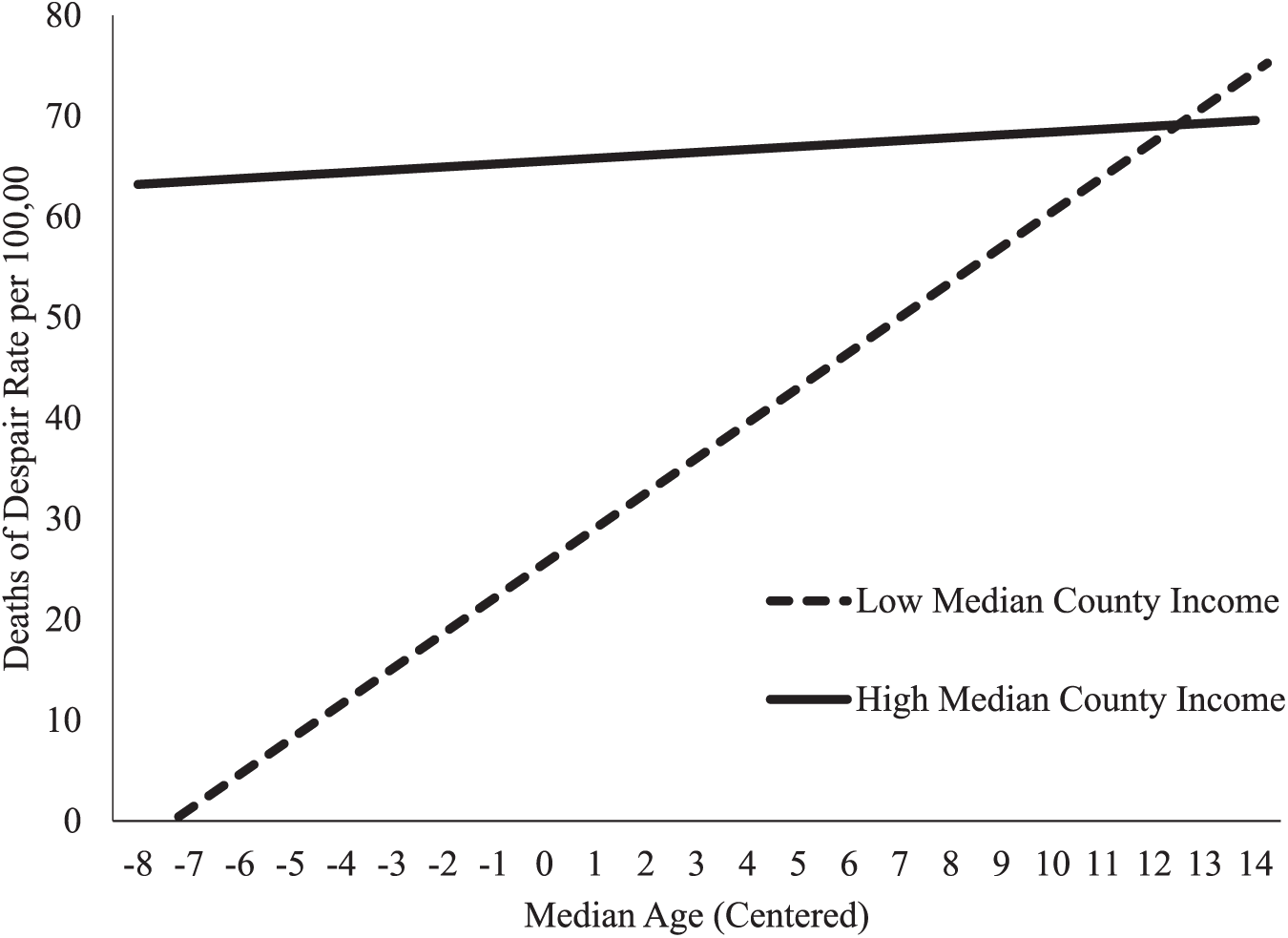
Interaction between county age and county income. Low and high median incomes were calculated as two standard deviations below and above the mean, respectively.
Discussion
Because the analysis was conducted at the county level, the results indicate associations between county-level variables rather than at the individual level. As such, there is a concern that individual-level explanations for the results may suffer from the ecological fallacy, wherein aggregated associations do not necessarily correlate to individual experiences. The below discussion of the results is an attempt to frame the results within the existing literature base as thoroughly as possible. However, the authors recognize the potential for the ecological fallacy. Future research, particularly with a larger sample size and at multiple levels, can better account for this possibility.
Results of the present analysis offered a mix of expected and unexpected results. First, the analysis showed that a model containing regular medical care, income, education, age, and mental health care availability accounts for 44% of variance in DOD. Given the complexity of the DOD epidemic (Case & Deaton, 2017; Scutchfield & Keck, 2017), this is considered substantial. There is still undoubtedly a need to clarify the specific independent predictors and their relationship with DOD as well as to elucidate variables that could account for additional variance. At present and until then, the results of the present analysis do suggest that (a) SDH can provide a viable model through which to measure and monitor DOD and (b) some SDH may have greater explanatory power than others, thus serving as feasible targets of intervention. Because of this, it might first be prudent for DOH to track SDH more regularly.
Expectedly, regular medical care and higher education were associated with lower DOD rates in a county. This result is congruent with the extant literature on SDH and health outcomes, including suicide, drug overdose, and liver disease (Braveman et al., 2011; Case & Deaton, 2017; CSDH, 2008; Meit et al., 2017). Regular medical checkups, a privilege of those that have both access to providers and the means to afford preventative services, may identify behavioral and/or health risks associated with DOD. Individuals, as a result, receive preventative care and/or treatment, slowing illness progression, and delaying mortality (CDC, 2017b; Cherrington, Corbie-Smith, & Pathman, 2007; CSDH, 2008). Similarly, counties with higher levels of college-educated residents evidenced lower DOD rates. This is congruent with existing literature on education’s impact on health outcomes (Brown et al., 2012; CSDH, 2008; Meara, Richards, & Cutler, 2008). Individuals living in these counties may have a greater knowledge of health-related issues and can consequently more efficiently navigate the health care system (Baker et al., 2007; Berkman, Davis, & McCormack, 2010). Another hypothesis is that, for residents in these counties, higher education begets higher income and therefor an ability “to use their considerable resources to maximize their life chances under current conditions” (Brown et al., 2012, p. 835). However, the intriguing income-related results in the current analysis may indicate that simple access to resources does not explain the whole picture. Age was also significantly associated with DOD, with older counties evidencing higher DOD rates. This is not wholly unanticipated, as liver disease and suicide are, respectively, the fourth and fifth leading causes of death among individuals ages 45 to 54 and the sixth and eighth leading causes of death for individuals ages 55 to 64. The suicide rate was highest for males ages 75 and older and for females ages 45 to 64 in the United States (National Institute for Mental Health, 2017).
Unexpectedly, greater levels of income and mental health care availability were associated with higher DOD rates. Higher income, in previous SDH literature, is typically associated with better health outcomes (Clouston, Rubin, Colen, & Link, 2014). This might suggest something unique about Florida’s source and/or distribution of income. Florida is a state known for its tourism and retirees. These features of Florida’s economy represent a nontraditional income flow, marked by both caprice and fragility (Marcouiller & Xia, 2008; Sherman, 2014; Tang & Jang, 2009). As a result, plaiting income with consistent access to resources may not be as straightforward as it appears (Boyce, Brown, & Moore, 2010; Brown et al., 2012). Additionally, Florida was recently ranked fifth in income inequality (Sommeiller, Price, & Wazeter, 2016). This fact, perhaps more than any other, may be precisely where the ecological fallacy is most likely. The average income of a county may be the function of relatively few highly wealthy residents, while the vast majority of the county is significantly less wealthy. This may affect how truly representative any measure of typical income for a Florida county may be. Future models ought to consider including a measure of income inequality, as this has been associated with poor health outcomes (Hiilamo, 2014; Pickett & Wilkinson, 2015). A more direct and parsimonious explanation may be that money truly does not buy happiness (the inverse of despair) in Florida. Boyce et al. (2010) noted that income rank and comparative income utility was a greater predictor of life satisfaction than was raw income. This has intriguing implications when juxtaposed the results of the current analysis. Perhaps, in counties with higher than average income, there is lower comparative income utility, thus leading to greater despair and DOD-related behaviors. Future research may benefit from including a measure of ranked income to clarify this possibility. Also worth consideration is the relationship between income and education level. The present analysis identified a significant negative relationship between education and DOD and a significant positive relationship between income and DOD. Considering that alcohol is relatively affordable and accessible regardless of education level and is the precipitant to alcoholic liver disease, such a deviation may not be wholly unexpected. It does however indicate that these two variables need to be thoughtfully incorporated into future research on this topic in order to more clearly understand how they work together to facilitate or mitigate DOD.
Traditionally within SDH literature, greater access to health care is associated with better health outcomes (CSDH, 2008). It would seem logical then to expect that greater mental health care availability would decrease deaths of despair. However, in the present analysis mental health care availability was significant in the opposite-than-expected direction. Three possible explanations are considered. First, it is possible that this finding reifies the difference between availability and access. Just because the mental health services are available does not mean that residents are able to access those services. Residents in these counties seem to be dying from despair despite the density of mental health professionals nearby. It is possible that the counties with higher mental health care availability, being the same counties with higher income, are less likely to encounter mental health services without specific motivation for such. In lower income counties, there may be a higher proportion of residents receiving public health care benefits, which include free comprehensive mental health services and early intervention programs. Future research is needed to test this hypothesis. Second, it is possible that mental health professionals are recognizing the counties in need and have begun infiltrating those communities. The benefits of this may not be evidenced in the data until future data collection cycles. Third, it is possible that the focus of treatment by the mental health professionals in the counties with higher mental health care availability, again being the same counties with higher income, is not on DOD-related behaviors. There may be an erroneous bias against making DOD-related behaviors the focus of treatment for higher income clients, opting instead to focus on qualitatively different needs (Noltemeyer, Bush, Patton, & Bergen, 2012). Again, data are needed to investigate the veracity of this hypothesis.
Finally, the interaction term between income and age was statistically significant. For counties with high median income, DOD rates are relatively stable across age. However, for low-income counties, DOD rates increase dramatically as age increases. There are three hypothesized explanations for this interaction effect. The first revisits an earlier note about early intervention. Low-income families, particularly those with children, are often the focus of early intervention efforts (Kelly, Jorm, & Wright, 2007; Podorefsky, McDonald-Dowdell, & Beardslee, 2001; Reynolds et al., 2007). The counties captured by the leftmost side of the x-axis in Figure 6 have a median age of approximately 35; this would seem to be precisely the cohort of individuals targeted by the early intervention programs. As families age out of eligibility for these programs, they can become more and more susceptible to DOD-related risks; Figure 6 demonstrates this. The second hypothesis relates most directly to the component of despair within DOD and leverages an earlier note about comparative income utility. Hope is a powerful experience, a “personal rainbow of the mind” (Snyder, 2002, p. 269). For younger low-income individuals, there may be hope for upward mobility (DiPrete, 2007; Serravallo, 2004). As these individuals age, hope for mobility may fade and lead to despair. In contrast, young high-income individuals may not have similar hope (as their mobility is constrained by a ceiling effect) and may actually have comparatively negative views of their financial standing and income utility (Boyce et al., 2010; DiPrete, 2007), leading to despair. Somewhat relatedly, the third hypothesis considers the lived experience of older low-income adults. This cohort of individuals experiences generally high levels of social isolation and stress from financial hardship (Eng, Rimm, Fitzmaurice, & Kawachi, 2002; Kahn & Pearlin, 2006; Seeman, Epel, Gruenewald, Karlamangla, & McEwen, 2010; Smith & Hirdes, 2009). These experiences have been associated with DOD-related behaviors (Hawthorne, 2008; Kahn & Pearlin, 2006). The trend displayed in Figure 6, wherein DOD increases as age increases in low median income counties, may be indicative of a compounding allostatic load. Allostatic load, the health burden of chronic stressors, has been identified with higher rates in older adults and has been associated with psychological dysregulation and distress (Juster et al., 2011; Kahn & Pearlin, 2006; O’Hara, 2006). Each of these hypotheses require further empirical validation. Again, the possibility of the ecological fallacy may be at play here as well. Because of the aforementioned unique density of retirees in the state, the average age of a county, particularly in counties with higher average ages, may not be truly representative of the actual dispersion of ages within that county.
Implications for Future Research and Public Health Practice
As DOD is still a relatively new construct, there is still significant research required to fully understand it. Researchers in various fields (e.g., psychology, public health, sociology, criminology, counseling, social work, medicine, nursing, health administration) may find DOD a compelling variable for inclusion in their work. The present study called attention to several specific areas that would benefit from further inquiry. Future research could further clarify the role of SDH in DOD generally. The present analysis resulted in a model that accounted for 44% of variance in DOD in Florida; future research could explore similar models in other states and at the national level. Ultimately, by better clarifying the relationship between SDH and DOD, more informed health and policy solutions can be created, tested, and implemented.
The results of the present analysis included some unanticipated results. Future research could further elucidate the catalyzing factors related to these results. Most notable were the results related to income and mental health care availability. It is unclear whether these results are specific to Florida or not; this alone is an opportunity for future research. Additionally, further research is needed to discern whether the hypothesized explanations for these results are valid or not. A longitudinal study may be most suitable to show causal relationships between SDH and DOD. Multilevel models, with residents nested within counties, could clarify how individual residents experience the SDH within their communities.
Race was not retained in the final model. This suggests that, at least in Florida, a county’s racial composition was a nonfactor in the county’s DOD rate. As such, though some do argue that DOD is only now getting attention because it has begun to affect White working-class families (Scutchfield & Keck, 2017; Stein et al., 2017), it is important to recognize that concentrating on this cohort may be too narrowly focused; other communities have been dying from despair for years. Lesbian, gay, bisexual, and transgender individuals are five times more likely to attempt suicide (Hatzenbuehler, 2011). Military veterans are at higher risk for suicide than the general population (Kang et al., 2015). Homeless individuals evidence high rates of drug overdose deaths (Baggett et al., 2013). Hispanic individuals experience greater severity of alcoholic liver disease at significantly younger ages than White individuals (Levy, Catana, Durbin-Johnson, Halsted, & Medici, 2015). There is a need for future research to clarify how these and other historically marginalized communities experience the SDH and DOD association.
Limitations
This analysis is subject to several limitations. First is the asynchronicity of the independent variables. Though only one of the variables retained in the model was older than 2015, the possibility that this influenced the results cannot be confidently ruled out. Future research can address this by collecting data in real time or gaining access to synchronous data. A second limitation is the removal of 10 counties (15% of the sample) from analysis due to outliers; these outlying counties may have something to offer with respect to SDH and DOD. Future multilevel research, where individual residents are nested within these counties, may be able to capture this. Third, the small sample size could be, as with any small sample, a liability. Though regression assumptions were tested in the present study and addressed when necessary, a larger sample in future studies can strengthen the confidence in any results. Last, the restricted sample size did not allow the present analysis to assess for regional effects. Such regional differences could be included in future research (e.g., zip code). Despite these limitations and considering the lack of DOD literature to date, the current analysis achieved its goal of assessing whether SDH would produce a viable model with which to monitor DOD in Florida counties.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.