
Abstract
Background
To examine the relationship between incarceration history and an individual’s compliance toward COVID-19 mitigation strategies and vaccination status/intentions.
Method
Data are from the Crime, Health, and Politics Survey (N = 1,735), a national probability sample of community-dwelling adults aged 18 and above living in the United States. Data were collected from May 10, 2021 to June 1, 2021. Multinomial logistic regression models were used to assess the relationship between incarceration history and COVID-19 mitigation strategies and vaccination status/intentions.
Results
Individuals with a history of incarceration reported approximately twice the relative risk of rarely/never using hand sanitizer and rarely/never wearing a mask compared with always/very often. Incarceration history was associated with more than 3 times greater relative risk of reporting not being vaccinated and not planning to get vaccinated compared with currently being vaccinated.
Conclusion
Formerly incarcerated individuals are less likely to abide by key COVID-19 mitigation protocols and exhibit higher levels of vaccine hesitancy. These findings suggest that formerly incarcerated individuals, as well as their families and communities, may therefore be at greater risk of accelerated spread of COVID-19 because of these factors.
The COVID-19 pandemic exposed widespread disparities in public health and has brought these issues to the forefront of dialogue in the United States (Abedi et al., 2021; Lopez et al., 2021). As of early November 2021, more than 46 million Americans have been infected and almost 750,000 people have died due to complications from SARS-CoV-2 (Centers for Disease Control and Prevention [CDC], 2021b). Although community mitigation strategies, such as social distancing, avoiding large social gatherings, and using hand sanitizer, are protective (Okano & Blower, 2020), they do little to fully eradicate the virus. Likewise, by November 2021, only approximately 58% of the U.S. adult population was fully vaccinated (CDC, 2021a), with stark differences in vaccination rates occurring across segments of the population (Ndugga et al., 2021). Such mitigation and vaccination efforts are particularly challenging in certain contexts, such as correctional facilities (Novisky et al., 2021), where some of the worst COVID-19 outbreaks have occurred (Barnert et al., 2020).
As correctional facilities continue to operate as usual, incarcerated people—many unvaccinated—are churning through prisons and jails and into the community. On an annual basis, approximately 600,000 individuals leave prisons (Carson, 2020), and millions cycle in and out of local jails (Zeng & Minton, 2021). In turn, this high rate of transition from correctional facilities to the community fuels the spread of COVID-19, especially in communities marked by high rates of incarceration and socioeconomic disadvantage (Lofgren et al., 2020; Reinhart & Chen, 2020, 2021). Indeed, estimates suggest that the churning of individuals through Cook County Jail in Chicago in March 2020 alone accounted for roughly 17% of total cases in majority-Black and/or majority-Hispanic ZIP codes, as well as approximately 21% of all COVID-19 racial disparities in Chicago by August 2020 (Reinhart & Chen, 2021). In addition, other elements of correctional facilities play an important role in the spread of COVID-19. For instance, recent studies have demonstrated that a significant association between COVID-19 prevalence among prison staff, the larger community, and among incarcerated persons, suggests that correctional staff are vital to infection control in prisons and the broader community (Nowotny et al., 2021; Wallace et al., 2021).
To limit the spread of the novel coronavirus, the CDC, alongside state and local health agencies have recommended preventive measures such as physical distancing, avoiding large social gatherings, consistent hand washing/sanitizing, and mask wearing, and encouraged Americans to get vaccinated. However, currently and formerly incarcerated persons tend to distrust the health care system and medical health providers (Brayne, 2014; Howerton et al., 2007; Porter, 2019; Vandergrift & Christopher, 2021), potentially making them less amenable to comply with such efforts. Subgroups of the population, who are already burdened by higher rates of contact with the criminal justice system, also generally tend to be skeptical of broad medical guidance. For example, a review of 13 studies on COVID-19 vaccination hesitancy found that across the board, Hispanics and African Americans were more reluctant to receive the vaccine (30.2% and 41.6%, respectively) compared with the overall pooled prevalence rate (26.3%; Khubchandani & Macias, 2021). Moreover, recent research has validated distrust of formerly incarcerated Black and Latino men using the Group-Based Medical Mistrust Scale linked to prior discrimination in health care settings and perceived suspicion of the medical field and health care providers (Valera et al., 2018). Similarly, correctional facilities may inadvertently induce trauma within their health care systems, creating a fear of health care providers during and after incarceration (Elumn et al., 2021). In this case, that fear of medical institutions may inculcate formerly incarcerated people to not only comply less with COVID-19 mitigation strategies but also create apprehension around getting vaccinated. To be sure, previous research among the general public has demonstrated that when individuals begin to lose faith in the medical system, they reduce their utilization of preventive medicine in general (Alsan & Wanamaker, 2018; Armstrong et al., 2006; Bogart et al., 2010; LaVeist et al., 2009), and are less likely to engage in COVID-19 protective behaviors more specifically (Allington et al., 2021; Cairney & Wellstead, 2021; Plohl & Musil, 2021). Thus, an elevated lack of medical trust among carceral populations can contribute to an especially challenging set of circumstances considering that the spread of COVID-19 occurs at higher rates in both correctional facilities (Barnert et al., 2020) and communities marked by high rates of incarceration and prisoner reentry (Lofgren et al., 2020; Reinhart & Chen, 2020, 2021).
Research shows that the overall correctional response to the pandemic was fragmented across jurisdictions, and that although many systems engaged in certain preventive measures, there were also many deficiencies including lack of testing, personal protective equipment, and sanitizing products (Novisky et al., 2020). Thus, to some extent, because correctional facilities did not do enough when the pandemic began, this may have further eroded trust and worsened COVID-19 mitigation compliance among formerly incarcerated populations. Moreover, persons with a history of incarceration are already vulnerable to poor health and experience several comorbidities that make them especially susceptible to the health consequences of COVID-19 infection (Massoglia & Remster, 2019; Novisky et al., 2021). Taken together, these factors suggest that individuals with a history of incarceration may be an especially high-risk population during the COVID-19 pandemic, for whom infectious disease mitigation efforts and vaccination uptake should be of heightened importance.
Even so, no known research has examined the relationship between incarceration history and an individual’s compliance toward COVID-19 mitigation strategies and vaccination plans. In an effort to examine how, if at all, formerly incarcerated people are adhering to the recommended guidelines, we use data from a nationally representative sample collected during the COVID-19 pandemic to assess adherence to mitigation strategies including minimizing large social gatherings, using hand sanitizer, wearing masks, as well as vaccination status among persons with a history of incarceration.
Data
This study uses data from the 2021 Crime, Health, and Politics Survey (CHAPS). The CHAPS is a multistage probability sample of 1,771 community-dwelling adults aged 18 and above living in the United States. Respondents were sampled from the National Opinion Research Center’s (NORC) AmeriSpeak panel, which is representative of households from all 50 states and the District of Columbia. Further information on the AmeriSpeak panel is available at https://amerispeak.norc.org/Documents/Research/AmeriSpeak%20Technical%20Overview%202019%2002%2018.pdf. Sampled respondents were invited to complete the online survey in English between May 10, 2021, and June 1, 2021. The data collection process yielded a survey completion rate of 30.7% and a weighted cumulative response rate of 4.4%. Importantly, the average response rate for national web-based surveys ranges between 20% and 25% (Fan & Yan, 2010; Millar & Dillman, 2011) and the weighted cumulative response rate accounts for survey outcomes in all response stages. The multistage probability sample resulted in a margin of error of ±3.23% and an average design effect of 1.92. A design effect of 1.92 means that the variance is only about twice as large as to be expected with a simple random sample. The median self-administered web-based survey lasted approximately 25 minutes. All respondents were offered the cash equivalent of US$8.00 for completing the survey.
The survey received human participants research ethics approval by the Institutional Review Board (IRB) at NORC and The University of Texas at San Antonio IRB. Informed consent was obtained from all participants. The current study uses data on 1,735 respondents with valid responses on the variables used in the current study.
Dependent Variables
The dependent variables measure a respondent’s self-reported compliance with COVID-19 mitigation protocols and their vaccination status/intentions at the time of the survey. Questions were developed by the research team on the basis of the CDC’s COVID-19 mitigation recommendations at the time of survey construction. COVID-19 mitigation measures include the following: attended social gatherings (“During the coronavirus (COVID-19) pandemic, how often have you attended indoor gatherings with more than 10 people?”), used hand sanitizer (“During the coronavirus (COVID-19) pandemic, how often have you used hand sanitizer to kill germs after being in public places?”), and wore a mask (“During the coronavirus (COVID-19) pandemic, how often have you worn a mask or other face covering in public places?”). Response options included 1 = always, 2 = very often, 3 = sometimes, 4 = rarely, and 5 = never. Because of relatively few responses in the always and never categories, we collapsed responses into the following categories: 1 = always/very often, 2 = sometimes, 3 = rarely/never. Vaccination status/intentions is measured using a question asking respondents “Have you been vaccinated for the coronavirus (COVID-19)?” Responses included 1 = yes, 2 = no, but I am planning to be vaccinated, 3 = no, and I do not plan to be vaccinated, and 4 = no, and I am undecided about getting a vaccine.
Independent Variables
Incarceration history is a binary variable based on a question asking respondents, “Have you ever spent any time in a correctional facility such as a jail or prison because you were convicted of a crime?” (1 = yes, 0 = no).
Control Variables
Control variables include a range of measures related to a respondent’s demographics, socioeconomic status, political affiliation, and COVID-19 history. Demographic measures include age in years, biological sex (1 = female, 0 = male), race/ethnicity (White, Black, Hispanic, Other race/ethnicity), born in U.S. (1 = yes, 0 = no), and marital status ([a] married, [b] widowed, divorced or separated, [c] never married, or [d] cohabitating). Socioeconomic variables include educational attainment (less than high school, high school graduate/general educational development [GED], some college, bachelor’s degree, or postgraduate study), annual household income (less than US$30,000, US$30,000 to less than US$60,000, US$60,000 to less than US$100,000, or US$100,000 or more). We also include a variable for the number of people living in a household, including children, household size. Political identification is a measure of whether a respondent identifies as a Democrat, Independent, or Republican. A binary measure is included to capture whether a respondent resides in a metropolitan area (1 = yes, 0 = no). Finally, we control for a binary variable of whether a respondent tested positive for COVID-19 (1 = yes, 0 = no).
Analytic Approach
We begin by displaying the summary statistics. Next, we examine the relationship between incarceration history and the outcome variables using multinomial logistic regression. All models include poststratification weights via iterative proportional fitting or raking to general population parameters derived from the Current Population Survey. Poststratification weights were used to reduce sampling error and nonresponse bias, and accounts for survey outcomes in all response stages, including panel recruitment rate, panel retention rate, and survey completion rate.
Results
Table 1 presents the summary statistics of the analytic sample. Overall, 5.2% of the sample reported having a history of incarceration. Across the COVID-19 mitigation measures, a few notable patterns emerge. Most respondents reported never/rarely attending social gatherings of 10 or more people, whereas 21.6% reported sometimes, and less than 10% of the sample reported always/very often attending such social gatherings. Likewise, most respondents reported always/very often using hand sanitizer (71.0%), compared with 18.6% reporting sometimes and 10.4% reporting never/rarely. Finally, the majority of the sample reported always/very often wearing face masks (85.8%), compared with just 8.0% reporting sometimes and 6.2% reporting never/rarely. Regarding COVID-19 vaccination status, most reported having received a vaccination (64.6%), yet about one third of the sample reported not planning to get vaccinated (18.1%) or being unsure about getting vaccinated (11.6%).
Weighted Descriptive Statistics of Analytic Sample (N = 1,735).
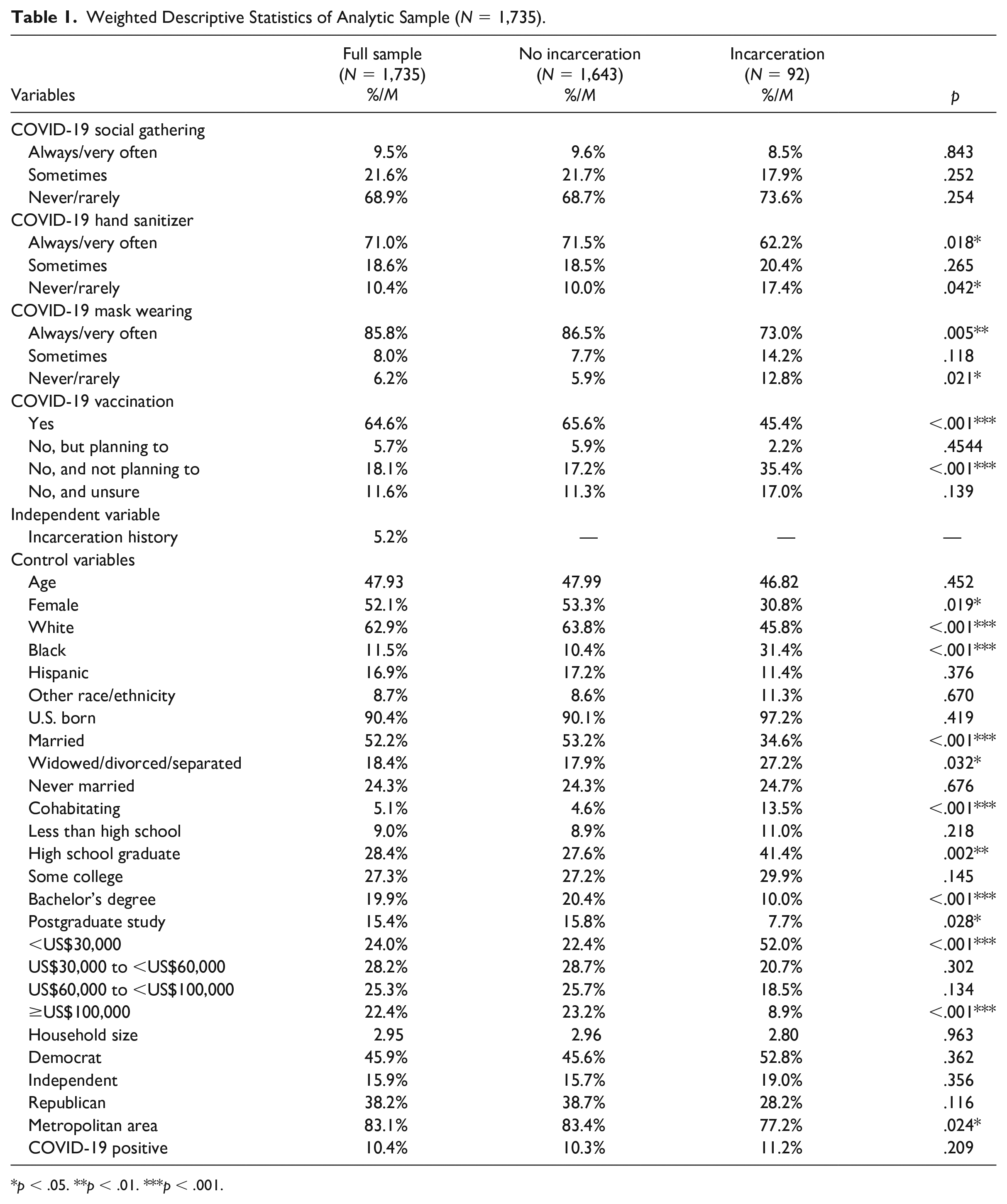
p < .05. **p < .01. ***p < .001.
Table 2 displays the multinomial logistic regression assessing the association between incarceration history and a respondent’s compliance with COVID-19 mitigation measures. Across all models, responses of always/very often are set as the reference category. Model 1 shows no association between incarceration history and attending social gatherings during COVID-19. Findings in Model 2 indicate that those with a history of incarceration reported approximately twice the relative risk of rarely/never using hand sanitizer compared with always/very often (relative risk ratio [RRR] = 2.265, 95% confidence interval [CI] = [1.077, 4.765]). Model 3 displays that incarceration history is associated with more than 3 times greater relative risk of rarely/never wearing a mask compared with always/very often (RRR = 3.345, 95% CI = [1.327, 8.435]).
Multinomial Logistic Regression of COVID Mitigation Measures on Incarceration (N = 1,735).
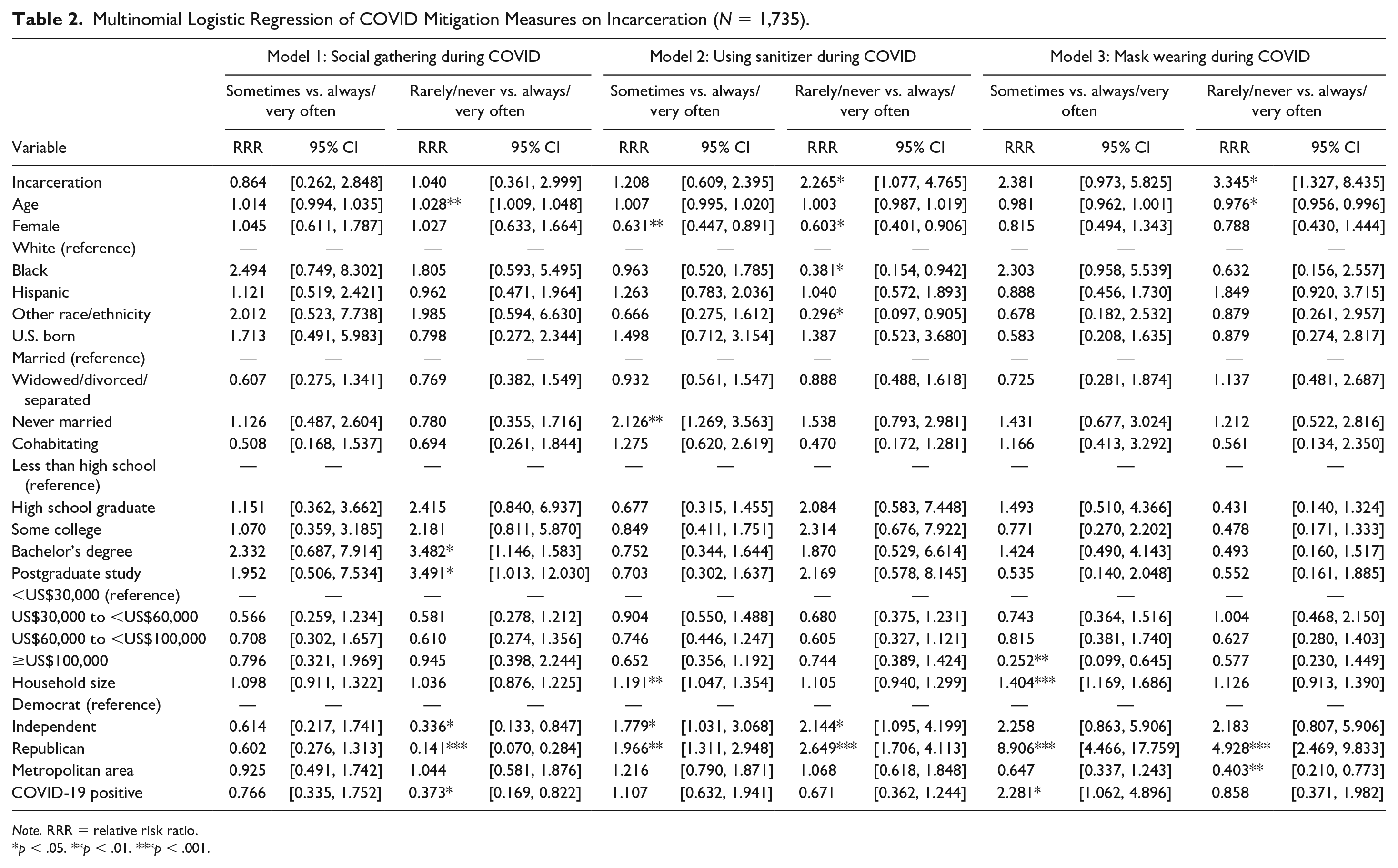
Note. RRR = relative risk ratio.
p < .05. **p < .01. ***p < .001.
Table 3 provides the results of the multinomial logistic regression assessing vaccination status/intentions with currently being vaccinated set as the reference category. The findings show that incarceration history is associated with more than 3 times relative risk of reporting not being vaccinated and not planning to get vaccinated compared with currently being vaccinated (RRR = 3.480, 95% CI = [1.575, 7.689]).
Multinomial Logistic Regression of COVID Vaccination Status on Incarceration (N = 1,735).
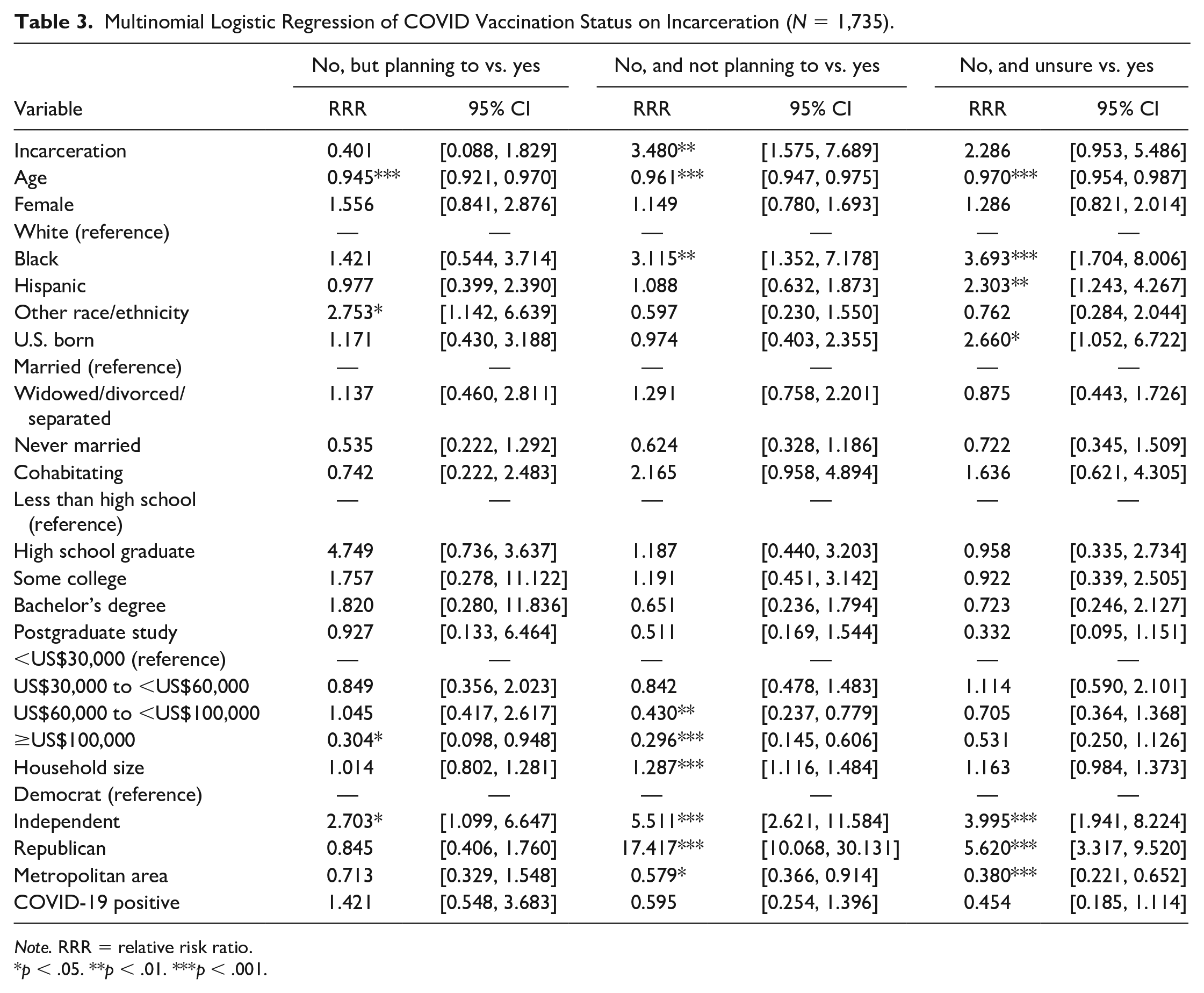
Note. RRR = relative risk ratio.
p < .05. **p < .01. ***p < .001.
Discussion
The COVID-19 pandemic highlighted substantial public health challenges and vulnerabilities in the United States. A key challenge in stopping the spread of COVID-19 is getting the public to get vaccinated and abide by COVID-19 mitigation protocols. One group that remained particularly vulnerable during the COVID-19 pandemic were those who have been incarcerated (Novisky et al., 2021; Reinhart & Chen, 2020, 2021). Although some research has assessed defiance during the COVID-19 pandemic (Burruss et al., 2021; Graham et al., 2020), no prior studies have assessed differential behavior related to COVID-19 mitigation and attitudes toward COVID-19 vaccines among those with a history of incarceration. Using nationally representative data, the current study filled this gap, showing that formerly incarcerated persons were less likely to use hand sanitizer and wear masks, as well as were more likely to report not planning to become vaccinated. Taken together, these findings highlight important disparities in vulnerability to COVID-19 among the formerly incarcerated and may, in part, explain the differential spread of COVID-19 among communities with high rates of incarceration (Reinhart & Chen, 2020, 2021).
These findings hold several implications for public health practice. Existing evidence suggests that incarcerated populations have greater degrees of distrust of the medical system (Alang et al., 2020, 2021; Brayne, 2014; Howerton et al., 2007; Porter, 2019; Vandergrift & Christopher, 2021). Thus, it may be that those who have been incarcerated are less trusting of medical guidance surrounding steps to mitigate COVID-19, as well as the safety and efficacy of vaccinations. Indeed, recent research has surmised that the lack of medical trust is a key factor that may create challenges in mitigating COVID-19 spread among currently and formerly incarcerated populations. On this point, Elumn and colleagues (2021) suggest that even though the COVID-19 pandemic has disproportionately affected incarcerated populations, “existing mistrust of the health care system during incarceration and fears around lack of treatment, segregation, punitive responses, may complicate incarcerated people’s responses to COVID-19 treatment and vaccine acceptance” (p. 2). To some extent, our findings provide support for this assertion by detailing that key mitigation efforts and vaccination uptake were less commonly endorsed by individuals with a history of incarceration. Although building greater trust is a formidable task, there may be a few steps that can be taken. For instance, one approach is a greater expansion of information both within correctional facilities and during the reentry process that provides information on the efficacy of infectious disease mitigation protocols. Novisky and colleagues (2021) note that although the vast majority of adults in the general population use internet access to gain primary health information, incarcerated persons “often have little to no access to the internet and other digital technologies, resulting in reduced abilities to independently learn about COVID-19, its impacts and what is being done to address it” (p. 8). Therefore, efforts to expand information and medical literacy to currently and formerly incarcerated persons may be an important step in improving infectious disease mitigation compliance. Relatedly, criminal justice and medical practitioners can work to build greater trust with currently and formerly incarcerated persons during their interactions. Porter (2019) finds that the high degree of medical distrust among formerly incarcerated persons stems from feelings of interactions with medical providers acting in a degrading manner and a sense that medical staff do not trust them. Therefore, this suggests that medical providers—through their interactions with patients—have a strong opportunity to build greater trust. Indeed, Khorasani and Wurcel (2021) have recently suggested that it is pivotal for the medical and public health community to “prioritize and engage people experiencing incarceration to build trust in vaccination efforts with the ultimate goal of improving health outcomes and health equity” (para. 11). Finally, the results suggest that public health outreach campaigns that seek to spread knowledge about infectious disease transmission and the safety and efficacy of vaccines, as well as provide easy access to vaccinations in communities with high rates of incarceration, may be an important and beneficial public health measure.
Limitations
There are a few limitations with the current study that can be expanded upon in future research. First, the survey was conducted between May 10, 2021 and June 1, 2021. Although this provides a novel snapshot of behavior during the COVID-19 pandemic, we are unable to assess behavior of formerly incarcerated individuals during other periods of the pandemic. Second, the measure of incarceration is a binary indicator of lifetime incarceration. Therefore, we cannot assess heterogeneity in the findings based on the type of facility an individual was incarcerated in (i.e., jail or prison), the length of incarceration, number of times incarcerated, or how recent the incarceration was. Future research that assesses the role of these features of incarceration on behavior during COVID-19 would be valuable. Third, there are some potentially relevant variables that were not included in the CHAPS survey. For instance, important intermediary mechanisms to be tested in future research may involve trust in the medical system (Brayne, 2014; Porter, 2019; Valera et al., 2018) as well as personality traits, such as self-control, which could be related to both incarceration (Gottfredson & Hirschi, 1990) and COVID-19 mitigation compliance (Xu & Cheng, 2021). Finally, although we use a nationally representative sample, because of sample size limitations, we could not reliably assess variation in the impact of incarceration on our outcome variables by key features such as respondent sex, race, or political affiliation.
Conclusion
Both COVID-19 and incarceration are serious public health concerns (Testa & Fahmy, 2021), and existing evidence shows disproportionate rates of COVID-19 infection among incarceration-exposed populations (Saloner et al., 2020). The results from the current study detailed that formerly incarcerated individuals were less likely to abide by key COVID-19 mitigation protocols and exposed higher levels of vaccine hesitancy. These findings suggest that formerly incarcerated individuals, as well as their families and communities, may therefore be at greater risk of accelerated spread of COVID-19 because of these factors. Given the profound health risks that COVID-19 presents to formerly incarcerated individuals—who in general are in poorer health and express greater numbers of comorbidities than the general population—these findings suggest that public health and criminal justice practitioners should develop targeted outreach and intervention efforts to increase knowledge related to infectious disease transmission and health risk, as well as actively work to improve medical trust among currently and formerly incarcerated persons in the United States.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.