
Abstract
Given the long induction time of many cancers and the fact that modifiable risk factors (e.g., cigarette smoking) including preventive factors (e.g., human papillomavirus [HPV] vaccination, healthy dietary and physical activity patterns) are influenced in adolescence, educating adolescents about cancer causation and risk reduction may have a large impact on reducing the cancer burden. We conducted a systematic review of literature evaluating the impact of cancer education interventions on adolescent knowledge of cancer risk reduction. We searched for articles published from 2000 to 2019 and identified 33 studies meeting our criteria. Given the methodological heterogeneity across studies, we briefly assessed effectiveness but focused on examining the design of the intervention and study. The majority of studies took place outside of the United States (67%). Most studies solely addressed skin or cervical cancer (67%) with only 18% (n = 6) discussing multiple cancers. The majority of interventions were a single-session (55%), did not involve a control or comparison group (67%), and were evaluated using a pre-test and a single post-test (61%); some studies administered multiple post-tests. Few studies (12%) investigated adolescents’ knowledge of lifestyle and environmental risk factors at both the individual and community level. Most studies (94%) reported improvement in knowledge following an intervention. Our review revealed wide methodological variation and a deficit in research evaluating interventions that address multiple cancer types and risk factors. Future research should robustly test whether comprehensive cancer education for adolescents can reduce the cancer burden, particularly in communities with major cancer health disparities.
Adolescence is a life stage of unique susceptibility to cancer risk–related exposures and behaviors and thus a critical time for educational intervention. Education about reducing the cancer burden is commonly delivered through public service announcements, public health departments according to national and state cancer control plans, clinicians, and community forums. Several public education programs have focused on adolescents. Given the long induction time of many cancers and the fact that several risk factors are influenced during the adolescent period (e.g., tobacco use, excessive sun exposure) including important preventive factors (e.g., human papillomavirus [HPV] vaccination, exercise habits), educating adolescents about cancer causation and risk reduction may have a profound impact on reducing the cancer burden. For example, successful smoking cessation has been associated with later age at initiation (Breslau & Peterson, 1996). In the United States, an increase in cancer diagnosed in young adults below the age of 40 further supports the need for earlier cancer prevention education (Kehm et al., 2019). Even for cancers in adults above the age of 40, educating adolescents may prove to have a large impact because many common cancers have roots in adolescence.
School-based and community-based cancer prevention education is central to cancer prevention efforts. Most U.S. adolescents receive general health education in middle and high school during health or science class. Teachers and school personnel are often trusted sources of information about nutrition and diet (Satia et al., 2010). In addition, students may be a source of information for their parents, especially in financially disadvantaged communities and communities with a large percentage of foreign-born individuals (Katz, 2014). Thus, cancer education for adolescents may reduce the cancer burden across two generations, directly by influencing adolescent risk and indirectly by providing adolescents with cancer screening information to share with parents and relatives.
There is a need to develop more comprehensive cancer education efforts specific to adolescents. The U.S. Centers for Disease Control and Prevention (CDC) has targeted adolescents in cancer prevention efforts regarding tobacco use, ultraviolet (UV) radiation, and HPV vaccination (Holman et al., 2013). Lifestyle (e.g., diet, alcohol use) and environmental factors (e.g., exposure to endocrine disrupting chemicals) may affect cancer risk; however, it is unclear whether existing education programs address these factors. Given the limited time allotted to school-based health education, risk factors besides smoking often go unaddressed (Holman et al., 2013). In fact, the CDC has called to “change how we approach cancer prevention” by taking a transdisciplinary, disparity-focused approach to address the interaction of multiple risk factors—genetic, behavioral, demographic, carcinogenic, social, and political—by working with and educating communities, schools, and families (Holman et al., 2013).
To inform our own efforts at revising and enhancing high school curricula that we have developed (Zeinomar et al., 2021), we conducted a systematic review of literature to summarize the types and findings of cancer education interventions in adolescents who have already been fielded. We aimed to characterize the scope and content of educational interventions as well as to understand if specific interventions improve students’ knowledge and beliefs about cancer and its risk factors. We focused on studies that implemented an educational intervention—a lesson or series of lessons—and evaluated knowledge before and after the intervention. Although the ultimate goal is to convert adolescent knowledge to behavior change, most educational interventions are not proceeded by a follow-up period long enough to assess behavior change. If studies evaluated knowledge and behavior, they remained under consideration for inclusion in our review. We were primarily interested in how educators conveyed (a) the interrelated nature of lifestyle, environmental, and genetic risk factors; (b) the associations of these risk factors with multiple cancer types; and (c) larger structural issues of equity. Secondarily, we were interested in the intervention and evaluation methods, for example, the content and pedagogy of the lesson(s) as well as the content and timing of pre-tests and post-tests.
Method
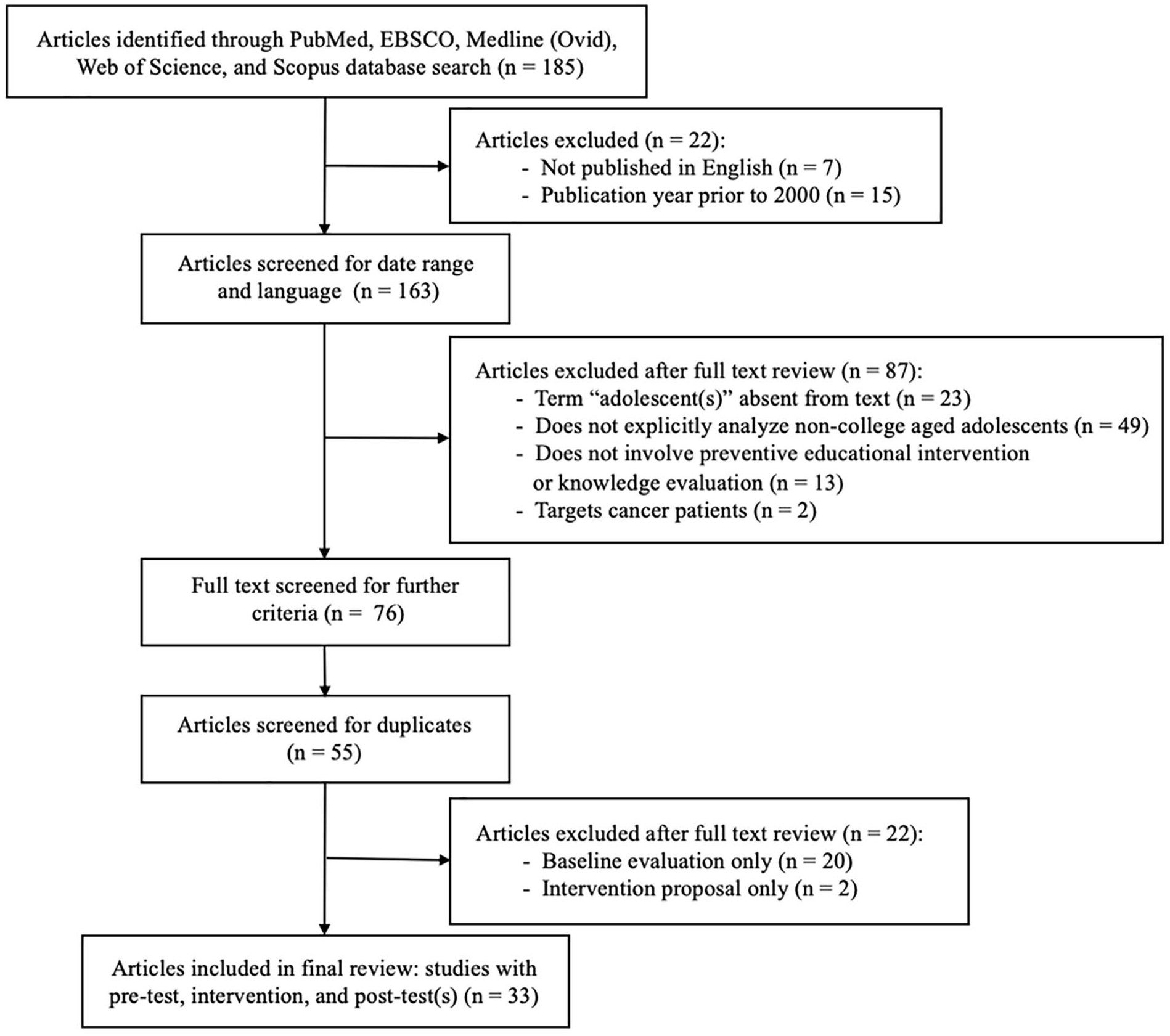
We conducted a systematic review using PubMed, EBSCO, Medline (Ovid), Web of Science, and Scopus databases (Figure 1). We searched literature published from 2000 to 2019. We selected the start date of 2000 given changes in technology and pedagogy. We focused on studies that implemented and evaluated programs whose eligible participants included secondary school students or people 10 to 19 years of age. We excluded studies that solely targeted university students. Our procedure was as follows: (a) identify articles based on search terms, (b) screen for date range and language, (c) screen the full text for additional exclusion and inclusion criteria, (d) screen for duplicates. Two reviewers independently screened articles and then worked together to create a final list which was then validated by one of the reviewers, who repeated the entire search process.
Systematic review of peer-reviewed literature published 2000–2019 on studies evaluating cancer education interventions in adolescents.
As Figure 1 illustrates, we searched PubMed and EBSCO for academic, peer-reviewed journal articles containing the following terms in the abstract (EBSCO) or in the title or abstract (PubMed): [education or educational or educate or educating] and [intervention or lesson or program or evaluation or evaluate] and cancer and [prevention or risk or awareness] and [adolescent or adolescents or “secondary school” or “high school” or “middle school”] and [knowledge or belief] not [survivor or survivors] not [patient or patients]. In addition, we searched Medline (Ovid), Web of Science, and Scopus for articles of the content type “journal article” or “scholarly publications” tagged with the subject terms “cancer,” “adolescent,” “adolescents,” and “health knowledge/attitudes/ practice” and containing the keywords: [education or educational or educate or educating] and [intervention or lesson or program or programme or evaluation or evaluate] and cancer and [prevention or risk or awareness] and [adolescent or adolescents or “secondary school” or “high school” or “middle school”] and [knowledge or belief] not [survivor or survivors] not [patient or patients]. We excluded articles that that were not published in English or published prior to 2000. We proceeded to screen full texts for additional exclusion criteria: missing the term “adolescent(s)” from the text, targeted cancer patients, solely focused on university students or did not specify the 10 to 19 age group, or neither administered a cancer prevention education program nor evaluated student knowledge. In addition, we eliminated duplicates. During a final review of the full text, we excluded articles that proposed but did not implement an intervention or only evaluated students’ baseline knowledge without implementing an intervention.
We classified cancer risk factors as a lifestyle, environmental, and/or genetic factor. We defined lifestyle as behaviors and associated exposures including viral (i.e., alcohol consumption, smoking, HPV, diet, parity). We recognize that viral transmission involves both community and individual-level dynamics. We defined environmental as physical or chemical exposures or relating to the built environment (i.e., UV radiation, water pollution, secondhand smoke).
Results
Figure 1 details the literature search. Our initial search from the various databases yielded 185 articles, of which 22 were excluded because they were not in English (n = 7) or were outside the date range (n = 15). After screening the full text, we excluded articles that lacked the term “adolescent(s)” (n = 23), targeted cancer patients (n = 2), solely focused on university students or did not specifically analyze the 10 to 19 age group (n = 49), or neither administered a cancer prevention program nor evaluated knowledge (n = 13). Of the 76 articles remaining, 55 duplicates were excluded. Twenty-two of the 55 articles were omitted for not incorporating the implementation and evaluation of the intervention using pre- and post-tests. Two of the 22 articles (Kyle, Macmillan, et al., 2013b; Satia et al., 2010) proposed and/or piloted lessons but did not formally implement or evaluate them; although excluded from the formal review, they addressed multiple cancer types and provided important insights. This left 33 studies meeting our inclusion criteria (see Table 1). Most (n = 19; 58%) of the 33 studies jointly evaluated knowledge, attitude, and/or behavior (see Table 2).
Studies Evaluating the Impact of a Cancer Prevention Intervention on Adolescent Knowledge (2000–2019).
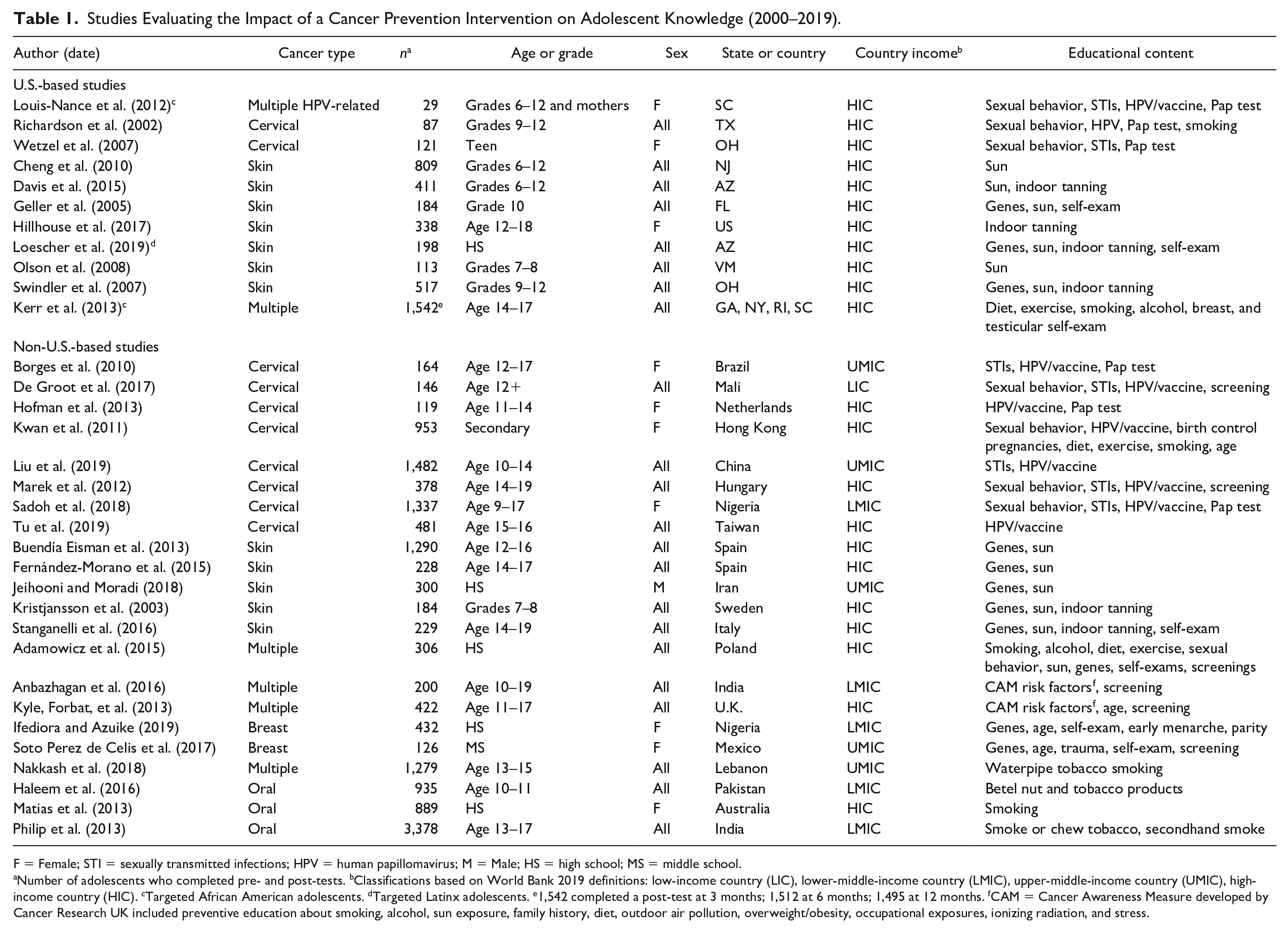
F = Female; STI = sexually transmitted infections; HPV = human papillomavirus; M = Male; HS = high school; MS = middle school.
Number of adolescents who completed pre- and post-tests. bClassifications based on World Bank 2019 definitions: low-income country (LIC), lower-middle-income country (LMIC), upper-middle-income country (UMIC), high-income country (HIC). cTargeted African American adolescents. dTargeted Latinx adolescents. e1,542 completed a post-test at 3 months; 1,512 at 6 months; 1,495 at 12 months. fCAM = Cancer Awareness Measure developed by Cancer Research UK included preventive education about smoking, alcohol, sun exposure, family history, diet, outdoor air pollution, overweight/obesity, occupational exposures, ionizing radiation, and stress.
Characteristics of Studies Evaluating Cancer Prevention Programs for Adolescents.
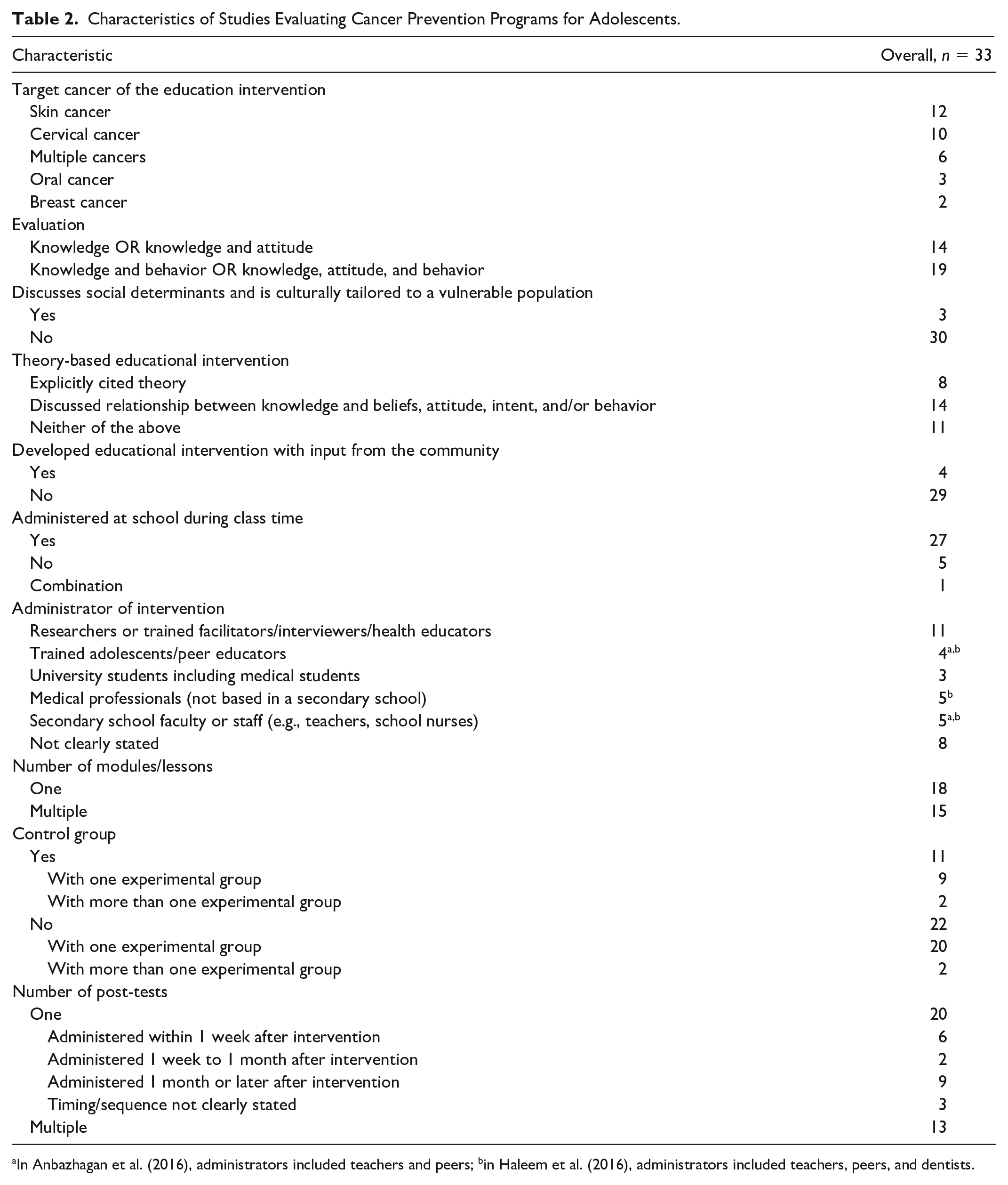
In Anbazhagan et al. (2016), administrators included teachers and peers; bin Haleem et al. (2016), administrators included teachers, peers, and dentists.
Sample size ranged widely across studies, from 29 to 3,378 adolescents. Of the 33 studies, most included male and female adolescents (n = 22), whereas others targeted females (n = 10) or males only (n = 1). Studies varied in their identification of adolescents, some specifying age (n = 17) or academic grade levels (n = 8) and others classifying the associated institution as high school (n = 5), middle school (n = 1), secondary school (n = 1), or a teen center (n = 1).
Intervention Content: Cancer Types and Risk Factors
Of the 33 studies reviewed, 27 (82%) addressed a single cancer type or risk factor, with most focused on HPV education (i.e., vaccination, safe sex) to prevent cervical cancer (n = 10) or sun protection education (i.e., wearing sunscreen and clothes, avoiding indoor tanning) to prevent skin cancer (n = 12; Table 2). Few addressed breast, oral, or other cancers (n = 11). Twenty-two of the 33 studies were conducted outside of the United States, and of those, roughly equal numbers took place in high-income countries as in lower- and middle-income countries. Studies were conducted in the United States (n = 11), Europe (n = 8), Asia (n = 8), Africa (n = 3), Central and South American (n = 2), and Australia (n = 1) (Table 2). Of the 11 U.S. studies, most (n = 7) exclusively tackled skin cancer and sun exposure (Cheng et al., 2010; Davis et al., 2015; Geller et al., 2005; Hillhouse et al., 2017; Loescher et al., 2019; Olson et al., 2008; Swindler et al., 2007).
Three of the 33 studies addressed environmental, lifestyle, and genetic risk factors (Adamowicz et al., 2015; Anbazhagan et al., 2016; Kyle, Forbat, et al., 2013), all of which considered multiple cancer types including leukemia, colorectal, breast, cervical, skin, oral, testicular, and lung cancer and highlighted the importance of screening as secondary prevention. Adamowicz et al. (2015), Kyle, Forbat, et al. (2013), and Anbazhagan et al. (2016) evaluated knowledge of the following risk factors: smoking, alcohol, diet, exercise, sexual behavior, sun exposure, and family history. Kyle, Forbat, et al. (2013) and Anbazhagan et al. (2016) used the U.K. Cancer Awareness Measures questionnaire which additionally dealt with outdoor air pollution, obesity, occupational exposures, ionizing radiation, and stress.
Eight of the 33 studies discussed a combination of genetic and environmental risk factors (n = 8), all focusing on sun exposure and/or tanning salons (Buendía Eisman et al., 2013; Fernández-Morano et al., 2015; Geller et al., 2005; Jeihooni & Moradi, 2018; Kristjansson et al., 2003; Loescher et al., 2019; Stanganelli et al., 2016; Swindler et al., 2007). One study discussed lifestyle, more specifically parity, in addition to genetic risk factors for breast cancer (Ifediora & Azuike, 2019). One study educated about first and secondhand smoke, simultaneously tackling lifestyle and environmental factors (Philip et al., 2013). Most studies (n = 15) focused solely on lifestyle factors, namely smoking or HPV. Four studies targeted sun exposure as their risk factor of concern (Cheng et al., 2010; Davis et al., 2015; Hillhouse et al., 2017; Olson et al., 2008). One study only addressed genetic factors (Soto Perez de Celis et al., 2017). In addition to teaching adolescents about risk factors, many studies equipped them with knowledge of preventive actions such as self-examination, HPV vaccination, Pap tests, and screening more broadly.
Three of the 33 studies designed culturally appropriate interventions tailored to a vulnerable or understudied population (Kerr et al., 2013; Loescher et al., 2019; Louis-Nance et al., 2012). Kerr et al. (2013) created an intervention tailored to African American adolescents in four U.S. cities that “invok[ed] positive cultural characteristics that reflect the African American experience.” Louis-Nance et al. (2012) prioritized African American adolescents in response to HPV racial disparities. Loescher et al. (2019) worked with community partners to adapt a sun safety program to Latinx adolescents in response to the increasing rate of skin cancer and lack of education research in Latinx populations. All three studies connected the risk of developing cancer with social determinants of health. Four of the 33 studies developed an educational intervention with input from the community in which the program was deployed (De Groot et al., 2017; Loescher et al., 2019; Louis-Nance et al., 2012; Wetzel et al., 2007). In addition to the community-based work by Loescher et al. (2019) and Louis-Nance et al. (2012), one study performed community needs assessments (De Groot et al., 2017) and another obtained curricular feedback from local teenagers (Wetzel et al., 2007).
Administration of Intervention and Evaluation
Approximately half of the interventions consisted of a single 30- to 60-minute session, whereas others entailed two or more lessons over several days. Most studies (n = 20; 61%) had one experimental arm and no control arm (i.e., another classroom using the standard curriculum). Two of the 33 studies had multiple experimental arms and no control arms (Anbazhagan et al., 2016; Haleem et al., 2016). For example, one study compared a lecture method in one school with a peer-performed skit in another school (Anbazhagan et al., 2016). Of the remaining 13 studies, 11 had one control arm and two had multiple experimental arms (Adamowicz et al., 2015; Tu et al., 2019). In Tu et al. (2019), experimental arms received different message framing—on the benefits of HPV vaccination or the consequences of not vaccinating.
Most interventions were conducted at school during class time (82%). Interventions were administered by various people, most commonly a researcher, trained facilitator, interviewer, or health educator (33%). Many studies did not specify an administrator (24%). Only two of the 33 studies integrated an online component (Buendía Eisman et al., 2013; Hillhouse et al., 2017) that was self-guided, allowing adolescents to learn without instruction from administrators.
Most studies discussed the importance of knowledge in affecting change in beliefs, attitudes, intent, self-efficacy, and/or behavior (n = 22). Of these studies, some went further to explicitly cite theory as the foundation for their intervention (n = 8). Theories included social cognitive theory (Haleem et al., 2016; Kerr et al., 2013; Nakkash et al., 2018), the health belief model (Davis et al., 2015), theory of reasoned action (Olson et al., 2008), theory of planned behavior (Tu et al., 2019), the transtheoretical model of behavior change (Kristjansson et al., 2003), and behavioral alternative and behavioral willingness models (Hillhouse et al., 2017). Social cognitive theory, for example, posits that the environment shapes behavior and knowledge acquisition affects self-efficacy (in this case, belief in one’s ability to enact behavior change like healthy eating) and perceived susceptibility (in this case, to developing cancer; Bandura, 1986).
Four of the 33 studies discussed the transfer of knowledge about cancer prevention from an adolescent to their parent or relative (Adamowicz et al., 2015; Louis-Nance et al., 2012; Philip et al., 2013; Soto Perez de Celis et al., 2017). Interested in how to increase knowledge of secondhand smoke and reduce indoor smoking, Philip et al. (2013) found that 34% of adolescents reported influencing their parental figures to quit tobacco. Educating adolescents about cancer prevention and lifestyle risk factors could in turn inform their parents, who are “at an age where breast cancer morbidity peaks and colorectal and cervical cancer are diagnosed” (Adamowicz et al., 2015). Louis-Nance et al. (2012) investigated HPV knowledge among mother–daughter pairs but did not explicitly inquire about a transfer of knowledge. Soto Perez de Celis et al. (2017) conducted student and parent questionnaires to explicitly investigate and promote the transfer of knowledge. Some studies did not address a transfer of knowledge yet discussed educating family members to serve as support systems for adolescents to make positive behavior change (Hillhouse et al., 2017; Jeihooni & Moradi, 2018; Kwan et al., 2011). Other studies explored the dynamics of communication and permission, for example, to receive the HPV vaccine (De Groot et al., 2017; Tu et al., 2019).
Overall, most studies (n = 31) observed an increase in student knowledge from the pre-test to the first post-test, regardless of the number and timing of post-tests. Two studies did not explicitly report a numerical change in knowledge (Buendía Eisman et al., 2013; Louis-Nance et al., 2012), and one study found a positive association that was not statistically significant (Matias et al., 2013). Methodological heterogeneity across studies (i.e., sample size, age) made it difficult to assess the relative statistical significance of results; therefore, we emphasized any reported improvement in knowledge.
Twenty of the 33 studies evaluated knowledge using one post-test, six of which were administered within 1 week of the intervention. The studies that administered a post-test at least 1-month post-intervention were interested in longer-term knowledge retention. In the 13 with a second post-test, researchers observed a decrease in knowledge retained from the first to second post-test. Of note are those that administered post-tests 6 months (Geller et al., 2005; Haleem et al., 2016; Kerr et al., 2013; Kyle, Forbat, et al., 2013) and 1 year (Adamowicz et al., 2015; Haleem et al., 2016; Kerr et al., 2013; Liu et al., 2019; Philip et al., 2013) following the intervention and still found improvements relative to pre-test levels. In addition to administering pre-tests and post-tests, two of the 33 studies used additional assessments to inform the selection of intervention content (Adamowicz et al., 2015; Buendía Eisman et al., 2013). Most notably, a two-part study administered a questionnaire between Stages 1 and 2 to inform the ratio of content delivered in Stage 2 (Adamowicz et al., 2015). Using pre-test results to inform content development allows educators to tailor material to students’ current levels of understanding. However, doing so may require more time and possibly delay a more rapid, widespread, or standardized implementation of the intervention to multiple groups and/or at multiple locations.
Discussion
Our review summarizes the types and findings of educational interventions that assess adolescent knowledge of cancer and cancer prevention. Given dramatic increase in cancers, it is essential to educate about cancer risk reduction earlier in life. The limited number of studies conducted in the United States highlights the need for more research into the impact of high school educational programs specific to cancer risk reduction. Although much can be learned from studies conducted abroad, differences in culture, resources, and educational systems may restrict the translation of their methods to U.S. classrooms.
Cancer Types and Risk Factors
Most interventions focused on a single cancer type or risk factor. They failed to comprehensively address joint effects of risk factors such as alcohol, environmental exposures, poor diet, and smoking, which, in combination, can increase the risk for various cancers. Of the six studies that discussed multiple cancer types, three taught about environmental, lifestyle, and genetic risk factors shared by common cancers (Adamowicz et al., 2015; Anbazhagan et al., 2016; Kyle, Forbat, et al., 2013). Drawing upon studies not included in this review, additional risk factors to consider teaching include exposure to pesticides (Pérez-Contreras et al., 2004), occupational carcinogens, and x-rays (Lana et al., 2013).
More research is needed on the relative efficacy of a holistic intervention given its alignment with cancer literature. Discoveries in cancer biology and treatment have demonstrated the efficacy of treating common etiological pathways such as immune pathways, which are involved in the development of numerous cancer types, rather than targeting a single cancer type. The epidemiological literature indicates the complex and intersecting nature of risk factors on various cancers. For example, although exposure to a single factor like smoking may increase the chances of developing many types of cancer, people are never exposed to a single risk factor in isolation. Furthermore, smoking is one of many factors that could increase risk of lung cancer.
Health education programs commonly take a risk factor approach rather than a health outcome approach. One exception is sexually transmitted infections (STIs); most adolescent STI prevention programs collectively address shared STI risk factors to increase knowledge and risk-reducing behaviors (Bowring et al., 2018; Lee et al., 2013; Lopez et al., 2016). This same approach could be applied to cancers. Skin cancer and HPV-related cancers are unique cases, each with one well-established risk factor, which may explain why educational interventions to reduce these cancers have been limited to a single risk factor. Yet, even HPV education, which often focuses on cervical cancer and targets females, could be more inclusive and move beyond gender-specific education. Louis-Nance et al. (2012) addressed HPV-related cancers beyond cervical cancer but was limited to female adolescents. Among HPV-attributable cancers (cervical, vagina, vulva, penis, anus, and oropharynx), the number of oropharynx cancers now exceeds estimates of cervical cancers attributable to HPV (Saraiya et al., 2015). Teaching about a single risk factor and/or a cancer may inadvertently lead some to believe that the material is irrelevant to them when in fact many cancers share risk factors.
One way to implement a more holistic approach is to adapt an existing chronic disease prevention intervention, expanding it to address more cancer types and risk factors (Zeinomar et al., 2021). For instance, a cervical cancer program focused on HPV vaccination could be expanded to include other HPV-related cancers including oropharynx cancer, an obesity intervention to include cancer, a smoking cessation program to include cancers besides lung cancer, a breast cancer family history workshop to include environmental risk factors. Building upon this lattermost example, interventions should empower students with knowledge that cancer is not fully determined by inherited mutations but also by acquired mutations through endogenous and exogenous exposures throughout life. Acquired mutations should be taught in a way that positions health in the larger context and history of environmental and social justice to demonstrate that change is possible at the individual and societal level. For example, Kerr et al. (2013) evaluated knowledge of diet, exercise, alcohol, and smoking while addressing structural challenges, like inaccessible healthy food, that hinder adolescents’ control over their diets.
Culturally Tailored Approaches: Equity and Inclusion
Empowering adolescents requires an understanding of their specific needs and cultural setting. Three of the 33 studies created culturally tailored interventions (Kerr et al., 2013; Loescher et al., 2019; Louis-Nance et al., 2012). Loescher et al. (2019) conducted community-based participatory research that involved community members in designing the educational program. Louis-Nance et al. (2012) formed community relationships that guided focus group selection. Kerr et al. (2013) was tailored to African American teenagers but the program was not developed in partnership with local community members in each state of deployment. Building a relationship with and receiving feedback from community members may lead to the creation of more impactful educational interventions (Kerr et al., 2013; De Groot et al., 2017; Loescher et al., 2019; Louis-Nance et al., 2012; Wetzel et al., 2007). Additional studies, which were excluded from our review for only conducting baseline evaluations, demonstrated additional culturally responsive methods that engaged American Indians, African and Caribbean Americans, inner city students, and mothers, among others (Dell et al., 2000; Jara-Palacios et al., 2015; Read et al., 2010; Schmidt-Grimminger et al., 2013; Shetty & Brown, 2009).
Many adolescents face barriers to access nutritious food, clean water, safe housing, and services and to avoid environmental exposures. Partnering with community organizations or local health departments could strengthen programs by connecting adolescents with resources to tackle structural barriers to health. Culturally responsive education programs, especially those that integrate social justice frameworks, succeed in part because they validate adolescents’ experiences in a manner that empowers them with knowledge upon which to act and share with friends and family. Particularly, in low-income and immigrant populations, adolescents can serve as messengers of risk reduction strategies to relatives. Some studies have modeled how to assess this transfer of knowledge from adolescent to relatives (Adamowicz et al., 2015; Louis-Nance et al., 2012; Philip et al., 2013; Soto Perez de Celis et al., 2017). The CDC identified that collaborating with families and schools is vital to “address structural barriers and the special needs of vulnerable populations” (Holman et al., 2013).
Structure and Administration of Interventions and Evaluations
Aiming to deepen knowledge about cancer risk reduction, studies should administer more than one post-test to assess longer knowledge retention. Another more accurate way to measure intervention impact is using a control arm, which must be carefully designed to ensure that adolescents are not denied beneficial information. Studies should define experimental and control arms by school to avoid contamination between arms within a school. If restricted to one school, the control arm should receive the intervention after the experimental group, only after both arms have been evaluated. In this way, all adolescents benefit.
Additional methods to improve knowledge may be the incorporation of peer education and digital content. Four of the 33 studies trained adolescents as peer educators (Anbazhagan et al., 2016; Haleem et al., 2016; Loescher et al., 2019; Sadoh et al., 2018). One study found a peer-to-peer program to be more effective than a teacher-to-student program (Anbazhagan et al., 2016). In another study, which did not meet inclusion criteria, Lana et al. (2013) created a website with games, videos, links, and a discussion forum about multiple cancer risk factors. Internet- or app-based education, especially game-based methods, has the potential to empower adolescents to reduce cancer risk (Abraham et al., 2021). Adolescents spend an increasing amount of time online; in 2018, 95% of U.S. adolescents had access to smartphones and 88% to a home computer (Anderson & Jiang, 2018). In 2018, more than 83% of U.S. adolescents played video games (Anderson & Jiang, 2018). Most recently, the COVID-19 pandemic has ushered in an era of remote or e-learning that may have a lasting impact on pedagogy, curricula, and classroom dynamics. Moving forward, it is vital that educators embrace internet and app-based tools.
Given the catalytic role of knowledge on the path toward behavior change, researchers may also consider incorporating theory (i.e., behavior change models) into intervention design. The diversity of theoretical approaches and the absence of theory from many studies prevented us from analyzing whether explicit integration of theory improved knowledge post-intervention.
As “cancer” was a required key word for eligibility, it is possible we missed educational interventions that did not explicitly discuss cancer. We observed that many studies about smoking or lung cancer education do not explicitly mention cancer, possibly due to existing public awareness of the link between lung cancer and smoking. For example, our search produced only a couple of smoking-related cancer studies, suggesting that studies may focus on preventing tobacco use but do not explain how lifestyle or environmental risk factors connect to cancer development.
Conclusion
Our review highlighted various methods of teaching and evaluating adolescent knowledge of cancer and primary cancer prevention. Overall, more research is needed on the relative efficacy of interventions that address multiple cancer types and risk factors. More holistic interventions would align with the state of the science of cancer biology, cancer risk factors, and cancer treatment and may be more practical considering the time constraints faced by classroom educators. Introducing concepts of cancer biology, public health, and equity may equip adolescents to become more engaged community members and to establish healthier habits during a formative period of their lives. Researchers should consider that particularly in low-income and immigrant populations, adolescents may play critical roles relaying knowledge to their relatives. Cancer educators in the United States can learn from both national and global efforts in crafting more technologically innovative and rigorously assessed interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the National Cancer Institute (NCI) and the National Institute for Environmental Health Sciences (NIEHS): U01ES026122-03, NCI P30CA013696-47.