
Abstract
Objectives
Health education may improve health in geriatric patients. To evaluate differences between remote and in-person education, the DREAMS (
Research Design
Nonrandomized two-arm interventions occurred remotely or in-person. About 130 diverse, older adults (M age: 70.8 ± 9.2 years; in-person n = 95; remote, n = 35) enrolled. Data from 115 completers (In-person n = 80; Remote n = 35) were analyzed for performance outcomes. Feasibility, adherence, and satisfaction benchmarks were evaluated at baseline, immediately post intervention, and 8 weeks post intervention. Adjusting for baseline performances, outcomes on health literacy and cognitive measures were compared between groups after intervention (at posttest and at 8-week follow-up) using adjusted mean differences (β coefficients).
Results
Eighty in-person and all remote participants completed at least six modules. Both programs had high satisfaction, feasibility, and strong adherence. After adjusting for demographic covariates and baseline values, cognitive and motor cognitive measures between groups were domain specific (e.g., global cognition, executive function, spatial memory, mental tracking capacity, and cognitive integration).
Discussion and Implications
This work explores feasible measures of knowledge acquisition and its link to health literacy and cognitive outcomes. Identifying effective delivery methods may increase involvement in clinical research. Future studies may encourage remote learning for increased accessibility.
Impact Statement
We certify that this work consists of recent novel clinical research. Our study highlights the differences between remote and in-person delivery methods of a health education program for diverse, older adults to better understand how different pedagogical methods may impact feasibility, satisfaction, health literacy, and cognitive performance outcomes. The DREAMS (
Introduction
Patient empowerment in health care demands measurable, reproducible approaches to address health disparities for diverse older adults, as this population is becoming ethnically diverse, identifying as part of historically underrepresented minority groups (Silverstein & Giarrusso, 2010). Unfortunately, many older, low-income minority adults, specifically Black patients, experience disparities related to poverty and low health literacy, creating barriers to engaging with health care (Kaiser et al., 2017; Kuczmarski et al., 2016). Historically underrepresented individuals are more susceptible to diseases at earlier ages than affluent counterparts (National Research Council (US) Panel on Race, Ethnicity, and Health in Later Life, 2004; Steptoe & Zaninotto, 2020). Engaging the clinical research community with diverse older adults is necessary to address health disparities.
Health-education programs include lessons as strategies to improve older adults’ control over their health. Older adults participating in health-education programs may improve their quality of life (Aghamolaei et al., 2005; Badger et al., 2013). By engaging in intellectual tasks, older adults may improve brain function, promote healthier behaviors, and enhance performance of activities of daily living (ADLs) (Smith et al., 2013; Willis et al., 2006). Health-education programs, thus, contribute to information processing, attention, memory, and other cognitive mental processes (Bijwaard et al., 2015; O’Grady et al., 2008).
In-person educational programs may enhance health literacy, cognition, and quality of life. However, lack of mobility and transportation are substantial barriers to in-person education (Lövdén et al., 2020; Syed et al., 2013). Telehealth approaches are increasingly popular, and in 2020, the COVID-19 pandemic highlighted the need for more telehealth options (Patel et al., 2021). While in-person interventions emphasize didactic presentations and group interaction, telemonitoring in conjunction with remote learning prioritizes individual study and one-on-one accountability.
Telehealth models may stimulate research participation. For example, “senior university”-style online seminars are offered nationwide to cognitively nonimpaired adults; however, those with lower socio-economic status may have limited access to technological-resources required for participation (Hansen & Reich, 2015). Using “high-tech” computerized web-based programs (e.g., Zoom, Google Meet, etc.) may enhance cognition but are prone to technical failure (Fatani, 2020; Realdon et al., 2016; Voinea et al., 2020). Common technical failures of web-based programs include poor network connection, rising security threats, and slow remote internet speeds (Boland et al., 2022). Using “high-tech” tools for educational purposes may be disadvantageous to older adults due to limited access to internet servers and low proficiency in “high-tech” language (Jones et al., 1987; Kaye et al., 2008). A “low-tech” health-education model may be a more effective learning method compared to “high-tech” alternatives. Active learning via “low-tech” tools, examples including hard copy reading materials, phone calls, written notebooks, may be as effective as email communication. Advantages of “low-tech” methods are avoiding technical difficulties, low accessibility, and knowledge gaps in technological proficiency (Vaportzis et al., 2017).
In 2014 to 2016, the DREAMS program (
This study compared two “low-tech” programs: In-person and Remote DREAMS. Both programs were “low-tech” because they involved a simple structure. In-person participants experienced interactive lectures and facilitated group discussions; remote participants read lessons independently from take-home binders followed by weekly one-on-one phone calls from the research team. Unlike a “high-tech” educational program, both “low-tech” models did not require internet access, technological proficiency, and controlled for participants’ lack of familiarity with “high-tech” tools. The nonrandomized two-arm interventions were based on the Learning Theory, which is described below.
Purpose of Study
The purpose of this study is to (a) compare feasibility, adherence, and satisfaction of Remote versus In-person DREAMS; (b) compare the efficacy of Remote versus In-person DREAMS for cognitive and health literacy measures; and (c) compare health literacy, cognitive, and motor cognitive performance outcomes between in-person and remote participants after intervention (immediate posttest and 8-week follow-up).
Hypothesis
Our primary hypothesis is we expect to observe similar feasibility and satisfaction levels in both programs with Remote DREAMS having lower attrition due to its increased accessibility. Our secondary hypothesis involved gathering outcome measures to observe if the studies were efficacious. We expect in-person participants to exhibit greater health literacy, cognitive, and motor cognitive outcomes after intervention compared to remote participants due to active learning via lectures and small peer group discussion.
Methods
Study protocol was approved by a review committee on the protection of human participants; all participants provided informed consent. The study was conducted from 2015 to 2017.
Participants
Adults aged 55 years and older, who were cognitively nonimpaired, in the metro-Atlanta area were recruited through presentations at local community partner organizations, flyers in senior living facilities, and word of mouth. Partner organizations included the following: senior living communities at high-, moderate-, and low-income levels; a volunteer organization associated with an Emory community service-learning program (Dillard et al., 2018). Interested participants were contacted to schedule initial assessments. Inclusion criteria included being older than 55 years and being cognitively nonimpaired. Enrolled participants were sequentially assigned by research investigators to an 8-week program of either in-person or remote education. Around 130 diverse, older adults participated (In-person DREAMS n = 95; Remote DREAMS n = 35), with more than 50% identifying as part of an underrepresented minority group and 91% racially identifying as Black or White (Table 2). Remote participants were recruited after in-person participants were recruited for this study, leading to more participants in the in-person group.
DREAMS Program Description
DREAMS incorporated Community Based Participatory Research strategies. Study team members used vital information from PSA feedback and focus groups to build course content. Participatory elements were included throughout the curriculum, including engaging discussion questions for participants (Perkins et al., 2019).
In-Person DREAMS
Part I of DREAMS included in-person sessions co-taught by local investigators and medical students who underwent standardized training for instructing the participants. Participants met once per week over eight consecutive weeks for 90 minutes (60 minutes of interactive lecture via PowerPoint presentations followed by 30 minutes of small group discussion). The first class was an introductory research-focused lesson. Other class topics concerned speakers’ areas of health expertise (Table 1). PowerPoint slides were different for each lecture, as the study team developed lectures of their own for each topic (Dillard et al., 2018). Group discussions were facilitated by DREAMS research staff using the following prompts:
What did you learn today?
Did anything strike you as particularly interesting or new?
What did you know about (topic) before the lesson?
How will this information apply to your life?
What would you tell your peer groups (e.g., circle of friends) about today’s lecture?
Main Weekly Topics Covered in DREAMS Program. a
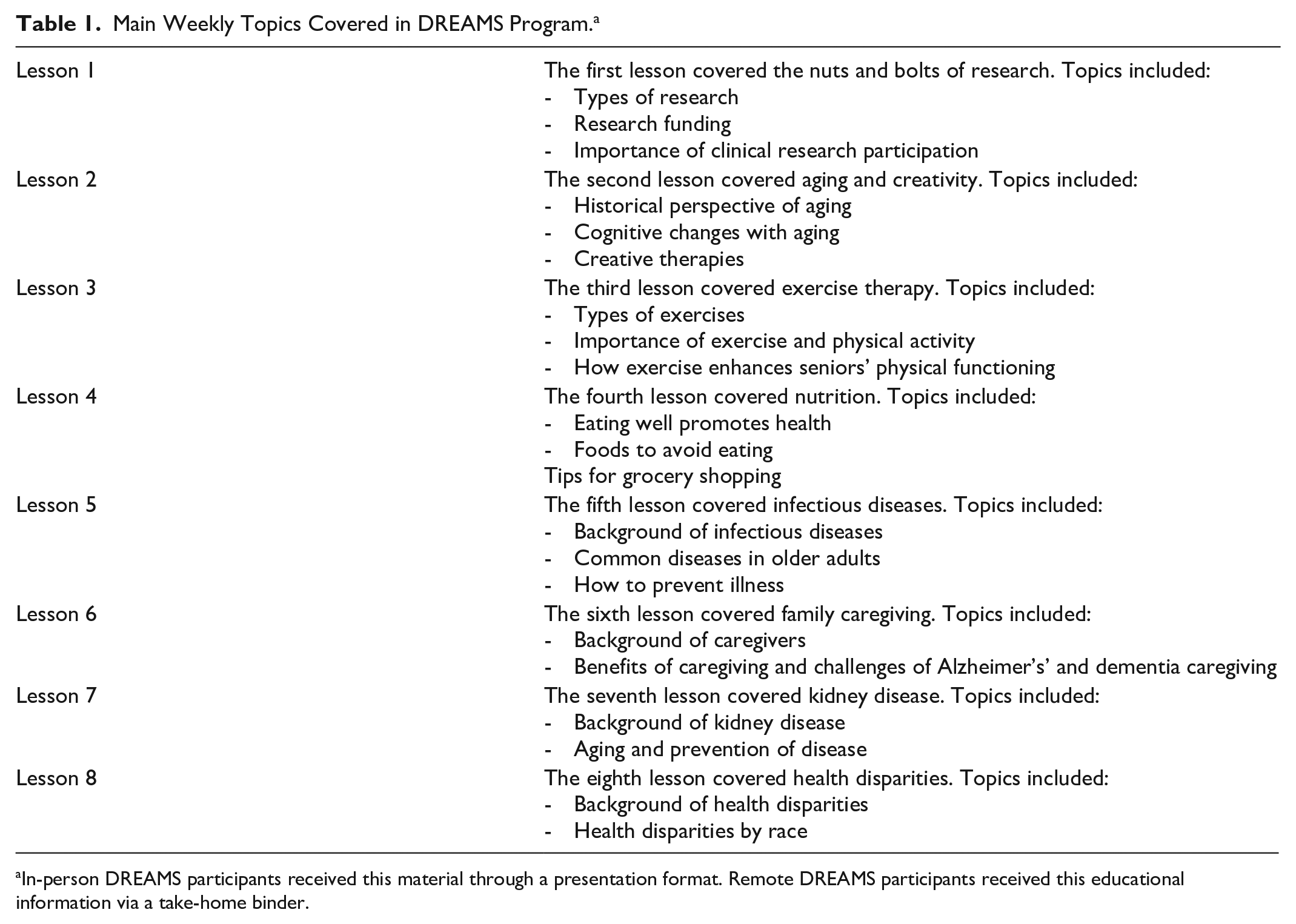
In-person DREAMS participants received this material through a presentation format. Remote DREAMS participants received this educational information via a take-home binder.
In-person participants also received print-out copies of the PowerPoint lectures and were allowed to take home their lecture notes for information retention purposes.
Learning Theory
Learning Theory states that discussing educational concepts with others and drawing connections between new and familiar learned material enhances information retention and mental vitality (Mukhalalati & Taylor, 2019). During the in-person 30-minute small group sessions, participants were asked to (a) summarize information learned with a partner in their own words, which was aided by moderators (Craik & Tulving, 1975); (b) identify what participants found novel and familiar from each topic and relate how new information adds to their prior knowledge. This step was required because learners who utilize prior knowledge in their comprehension are more likely to incorporate new information into their long-term memory store, that is, their “knowledge” (Medin & Ross, 2001); (c) generate three or more questions about educational material; and (d) present questions for the lecturer to the larger group to exchange information and feedback. To guide small group discussions, moderators asked questions exercising Learning Theory concepts to guide participants’ information retention (wee questions for In-person DREAMS listed above).
Remote DREAMS
Peer interaction may strongly impact individuals’ knowledge acquisition of health education. Assuming in-person socialization may improve educational attainment, we controlled for peer interaction with the remote group. Remote DREAMS included take-home binders, designed based on in-person presentations for participant learning. Binders contained eight weekly lesson plans. Participants were directed to complete one lesson (estimated completion time: 1.5 h) per week. Weekly lessons included: research, creativity, exercise, nutrition, infectious disease, family caregiving, kidney disease, and health disparities (Table 1). Each lesson included 20 to 30 pages (14-point font) of accessible, eighth-grade reading-level material. Supplemental websites and videos were provided (Garfin, 2020; Appendix).
Remote participants received weekly phone calls to ascertain progress and discuss each completed lesson with moderators. They were asked the same exact follow-up questions as in-person participants, such as what participants learned, if they found any concepts particularly interesting, if they knew anything about the topic prior to the lesson, if they learned anything they could use later in their life, and what they would share to their peers/friends about the lesson. Remote participants were also asked if they viewed the provided supplemental materials (e.g., informational websites).
Measures
Participants completed demographic surveys before intervention (Table 2). Both participant groups were assessed for outcome measures preintervention, postintervention, and 8-week postintervention follow-up via in-person visits (Tables 3 and 4). Breaks were given ad libitum. Testing lasted approximately 2 to 3 hours. Assessors were blinded to group assignment.
Demographic Characteristics by Group (In-Person vs. Remote).
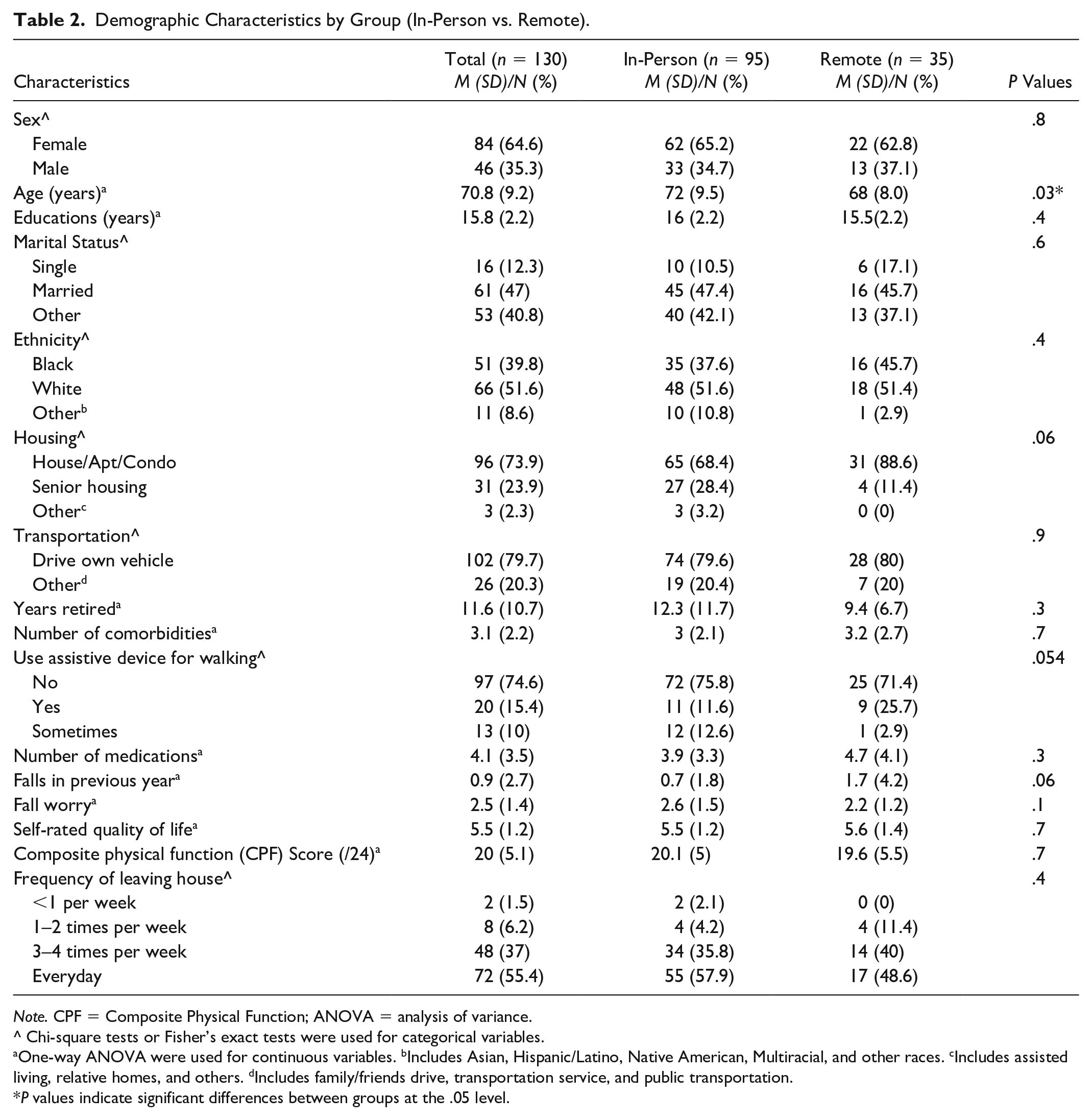
Note. CPF = Composite Physical Function; ANOVA = analysis of variance.
Chi-square tests or Fisher’s exact tests were used for categorical variables.
One-way ANOVA were used for continuous variables. bIncludes Asian, Hispanic/Latino, Native American, Multiracial, and other races. cIncludes assisted living, relative homes, and others. dIncludes family/friends drive, transportation service, and public transportation.
P values indicate significant differences between groups at the .05 level.
Pretest, Posttest, and Follow-Up Values for Health Literacy Outcome Measures in DREAMS In-Person vs. Remote Group.
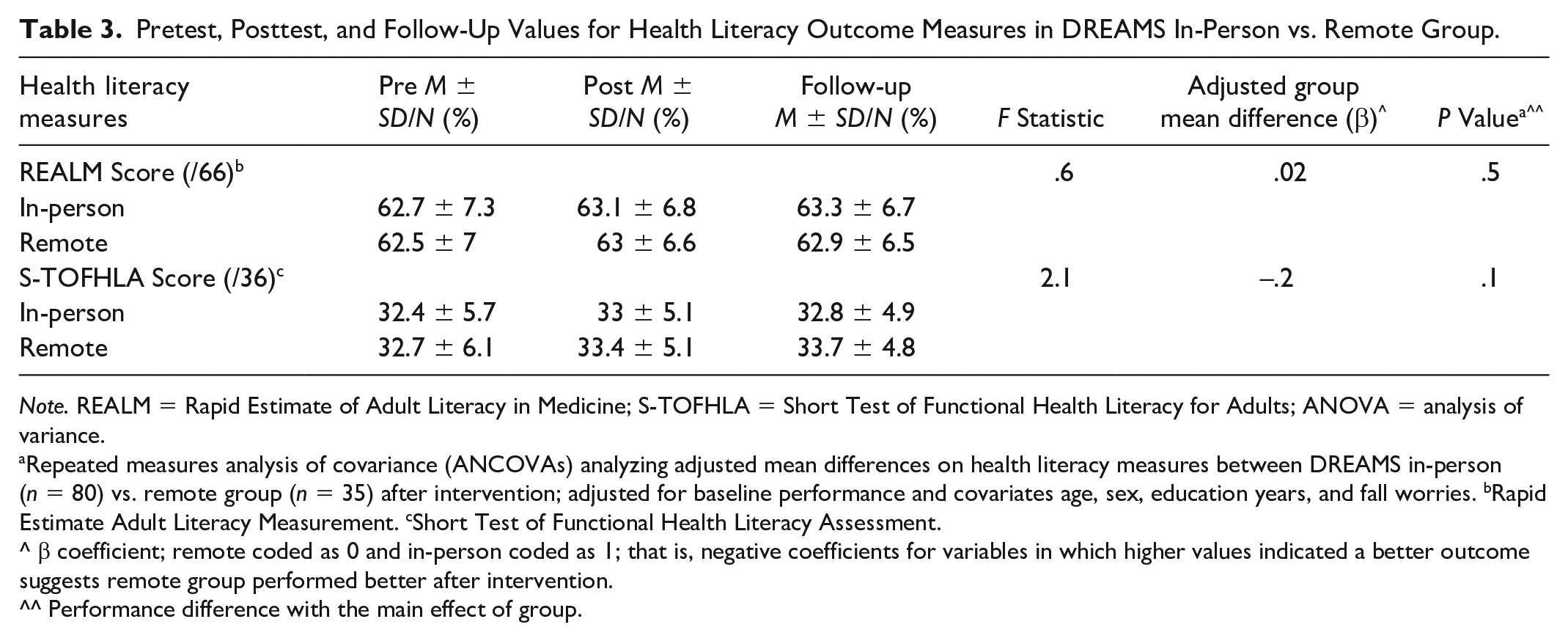
Note. REALM = Rapid Estimate of Adult Literacy in Medicine; S-TOFHLA = Short Test of Functional Health Literacy for Adults; ANOVA = analysis of variance.
Repeated measures analysis of covariance (ANCOVAs) analyzing adjusted mean differences on health literacy measures between DREAMS in-person (n = 80) vs. remote group (n = 35) after intervention; adjusted for baseline performance and covariates age, sex, education years, and fall worries. bRapid Estimate Adult Literacy Measurement. cShort Test of Functional Health Literacy Assessment.
β coefficient; remote coded as 0 and in-person coded as 1; that is, negative coefficients for variables in which higher values indicated a better outcome suggests remote group performed better after intervention.
Performance difference with the main effect of group.
Feasibility
Feasibility was measured by accomplishing experimental set-up and programmatic objectives and methods. Feasibility was the primary measure for our primary hypothesis.
In-person feasibility measures included the ability to recruit speakers; find an intervention location; include participants without their own transportation; coordinate specific lecture times; address hearing and visual impairments that may limit participant engagement with the material; communicate effectively between speakers and moderators prior to each lecture; and ensure that moderators guided group discussions.
Remote feasibility measures involved: creating educational binders; converting In-person DREAMS PowerPoint presentations into prose format; performing approximately 280 instructional calls over 8 weeks to motivate participants (this estimate does not count repeat call attempts that were necessary when contact was not made); and providing supplemental resources to increase participants’ understandings on the topics.
Adherence
Program completion was participation in at least 6 of 8 modules. To maintain program adherence, in-person and remote participants were called immediately if they missed lessons and encouraged to return. Remote participants’ adherence was assessed through phone call; if participants could not discuss the lesson, we assumed they did not read it. Obstacles that prevented participants from physically reaching the program site were troubleshooted by providing transportation services to those who were underserved.
Satisfaction
At immediate posttest, an exit survey was administered to evaluate participants’ views on the programs via a Likert-type scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree). Qualitative feedback was collected via four open-ended questions that asked participants what their favorite topics were, what their least favorite topics were, what additional topics they want to learn about in the future, and what additional suggestions they have about DREAMS (Hackney et al., 2015).
Health Literacy
Health Literacy was evaluated with Rapid Estimate of Adult Literacy in Medicine (REALM) and Short Test of Functional Health Literacy for Adults (S-TOFHLA). REALM is a 66-item word recognition test evaluating risk for poor literacy skills and categorizes participants’ reading levels: third grade and below (0–18), fourth to sixth grade (19–44), seventh to eighth grade (45–60), and high school (61–66) (Bass et al., 2003). S-TOFHLA assesses comprehension of health-related material and is divided into inadequate (0–16), adequate (17–22), and functional (23–36) categories, based on a 36-item reading comprehension subscale (Baker et al., 1999).
Cognition
Cognitive battery included standard, valid, and reliable measures of global cognition, executive function, spatial memory, and mental tracking capacity.
Montreal Cognitive Assessment (MoCA) is a 30-question test that measures global cognition, screening individuals for mild cognitive impairment by assessing attention, executive functions, memory, visuo-constructional skills, and conceptual thinking domains. Out of 30 points, a score ≥26 is considered normal cognitive function (Nasreddine et al., 2005) (Table 4).
Pretest, Posttest, and Follow-Up Values for Cognitive and Motor Cognitive Outcome Measures in DREAMS In-Person vs. Remote Group.
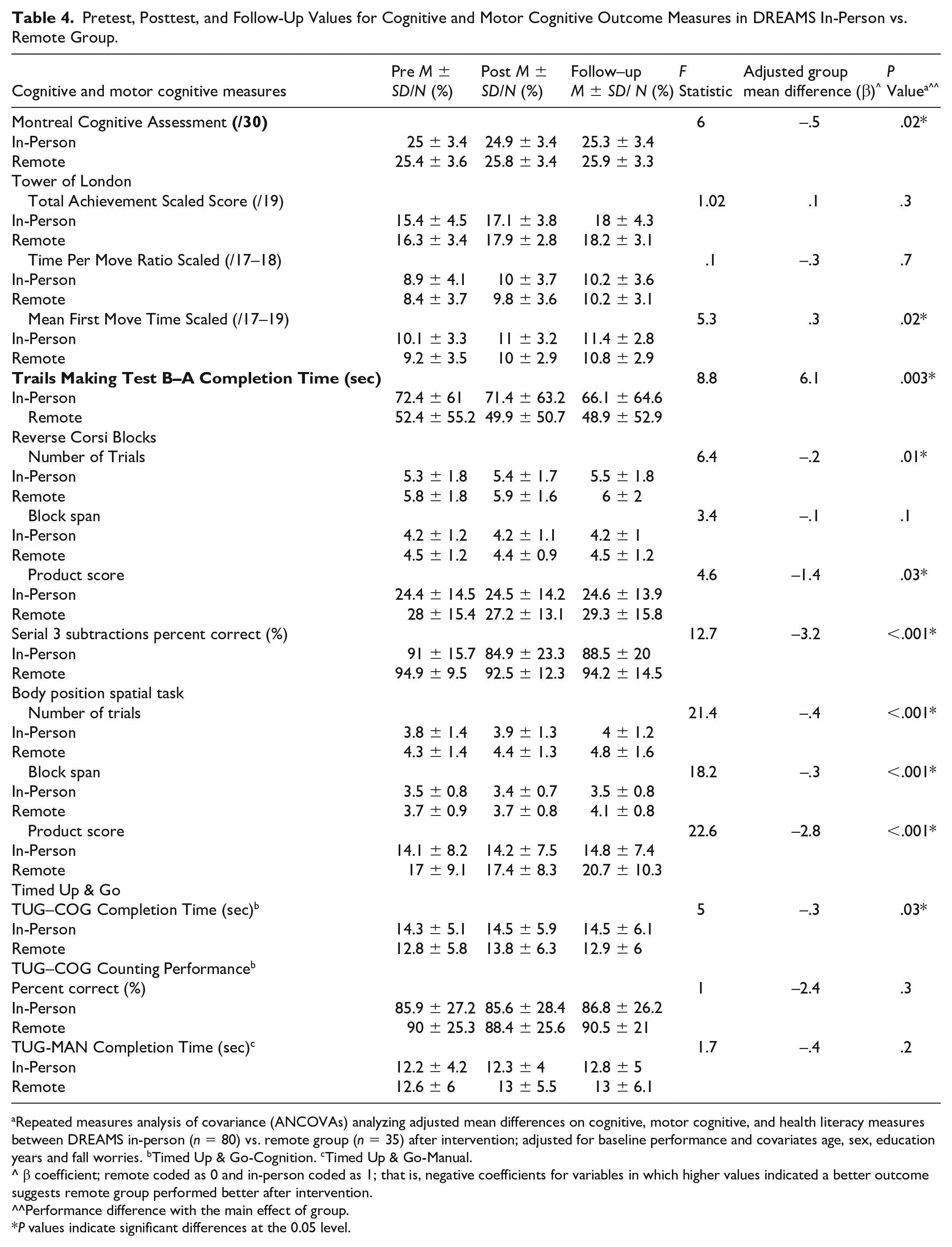
Repeated measures analysis of covariance (ANCOVAs) analyzing adjusted mean differences on cognitive, motor cognitive, and health literacy measures between DREAMS in-person (n = 80) vs. remote group (n = 35) after intervention; adjusted for baseline performance and covariates age, sex, education years and fall worries. bTimed Up & Go-Cognition. cTimed Up & Go-Manual.
β coefficient; remote coded as 0 and in-person coded as 1; that is, negative coefficients for variables in which higher values indicated a better outcome suggests remote group performed better after intervention.
Performance difference with the main effect of group.
P values indicate significant differences at the 0.05 level.
Tower of London (ToL) assesses planning ability as executive function. An administrator presents a card with an arrangement and participants move rings of differing sizes to three pegs to match the arrangement. Scaled total achievement score, time per move ratio, and mean first move time (measuring planning time before task completion) were collected (Rainville et al., 2012) (Table 4).
Trails Making Test (TMT) assesses cognitive processing speed. TMT B-A isolates task-switching, which may be related to performance-based measures of ADLs (Sánchez-Cubillo et al., 2009). TMT B-A was the primary outcome measure for our secondary hypothesis because TMT B-A is widely used for assessing executive function (Table 4).
Reverse Corsi Blocks tests visuospatial function and working memory and requires participants to watch the examiner point to a pattern of a series of blocks and then repeat the pattern backwards. Each level consists of two trials. Participants advance to the next level if they successfully complete at least one trial in a level. Number of trials successfully completed, block span (length of sequence of moves participant successfully performs), and product score were analyzed (Kessels et al., 2008) (Table 4).
Serial 3 Subtractions assesses mental tracking capacity, as administers request for examinees to subtract by 3 from 100. Each subtraction is considered a unit and calculations are made based on 14 possible correct subtractions (Bristow et al., 2016) (Table 4).
Motor Cognition
Motor cognition measures evaluated motor and cognitive integrations (Table 4).
Body Position Spatial Task (BPST) modeled after the Corsi Blocks task measures whole-body spatial cognition. The examiner demonstrates a sequenced pattern of steps to the side, forward, and turning (in place) and the participant attempts to repeat the pattern. The number of trials performed correctly, block span (length of sequence of moves successfully performed), and product score were analyzed (Battisto et al., 2018).
Timed Up & Go Test (TUG) evaluates functional mobility. Participants are timed and rise from a chair, walk 3 m, turn around, and return to the chair. TUG cognitive (TUG-COG) and manual conditions (TUG-MAN) measure dual-task ability. Participants perform serial subtractions by 3 seconds in TUG-COG and carry a full glass of water in TUG-MAN. Correct percentage of subtractions performed during TUG-COG (TUG-COG Counting Performance) and completion times for both tasks were analyzed, with time ≥15 seconds for TUG-COG and time ≥14.5 seconds for TUG-MAN indicating impaired dual-task ability and fall risk (Cardon-Verbecq et al., 2017).
Data Analysis
Descriptive statistics were compared between groups using Chi-square and Fischer’s exact tests for categorical variables and one-way analysis of variance (ANOVA) for continuous variables. For outcome analyses, covariates age, sex, education years, and fall worry were controlled for demographic group differences. Adjusting for baseline values collected at pretest and covariates, analysis of covariance (ANCOVA) was used to compare differences in cognitive, motor cognitive, and health literacy outcomes between groups after intervention. Group × timepoint interaction was first included in the model but then dropped due to nonsignificance found in the change of outcomes from posttest to 8-week follow-up between groups Thus, performance outcomes were analyzed after intervention (at both posttest and at 8-week follow-up) without group × time interaction to obtain adjusted mean differences (β coefficients) between in-person and remote groups with baseline variance removed. Adjusted mean differences were compared with the remote group coded as 0 and in-person group coded as 1; therefore, for example, negative coefficients for variables in which higher values indicated a better outcome suggests remote participants performed better after intervention. P value <.05 was overall the significance level. Satisfaction ratings in the exit survey were evaluated for groups using Fischer’s exact test and Mann-Whitney U-test. Statistical analyses were completed using R software (version 3.4.4).
Results
About 130 participants (age 70.8 ± 9.2; In-person DREAMS, n = 95; Remote DREAMS, n = 35) were included. In-person DREAMS participants were significantly older than the remote group. Other demographic characteristics were similar (Table 1).
Feasibility
Both programs were feasible in accomplishing experimental set-up and programmatic objectives. In-person DREAMS recruited faculty and medical students to lecture participants about aging research in a clinical academic facility. Around 20% of in-person participants (n = 19) were provided transportation. We successfully coordinated lecture times that worked for many participants, medical students, and faculty; participants’ auditory and visual limitations were addressed; and moderators provided participants equal opportunities to discuss the lecture. Remote DREAMS was feasible with successful creation of a cohesive, educational binder. Participants engaged with weekly calls. Times were coordinated to call participants after they read the module and supplemental material was offered.
Adherence
Both programs had strong adherence. Eighty of 95 in-person participants completed six of eight modules. Fifteen enrolled participants withdrew (15%–16% attrition rate) either before attending any classes (n = 6) or before completing at least six of the modules (n = 9) with the most frequent reason being participants were no longer interested in the classes. All remote participants completed 6 of 8 modules (n = 35; Figure 1).
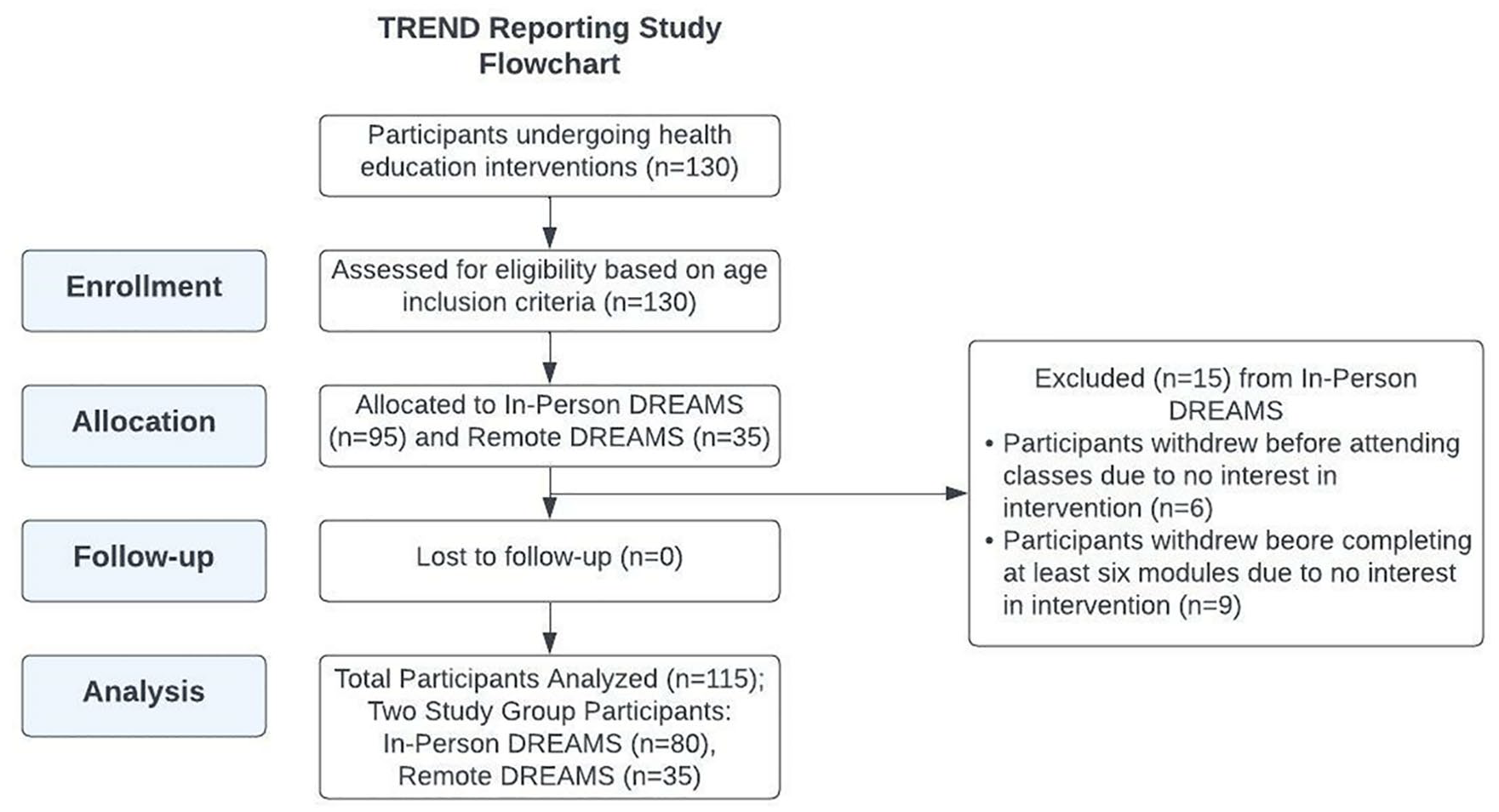
Study flowchart highlighting participants’ adherence to the DREAMS health education intervention.
Satisfaction
Both in-person and remote participants reported they agreed or strongly agreed that the modules enhanced their knowledge about health (Mdn = 5; interquartile range [IQR] = [4,5]), influenced how they take care of themselves (Mdn = 4; IQR = [4,5]), and provided them with useful information (Mdn = 4.5; IQR = [4,5]). Both groups agreed or strongly agreed that quality of classes was high (Mdn = 4; IQR = [4,5]) and that they would attend future programs offered (Mdn = 5; IQR = [4,5]). Participants enjoyed both programs (Mdn = 5; IQR = [4,5]) and agreed they would continue the programs if they could (Mdn = 4; IQR = [4,5]). Both groups were neutral or agreed that they were more physically active after intervention (Mdn = 4; IQR = [3,4]). Participants agreed or strongly agreed that they have been more mentally active (Mdn = 4; IQR = [4,5]; Figure 2).
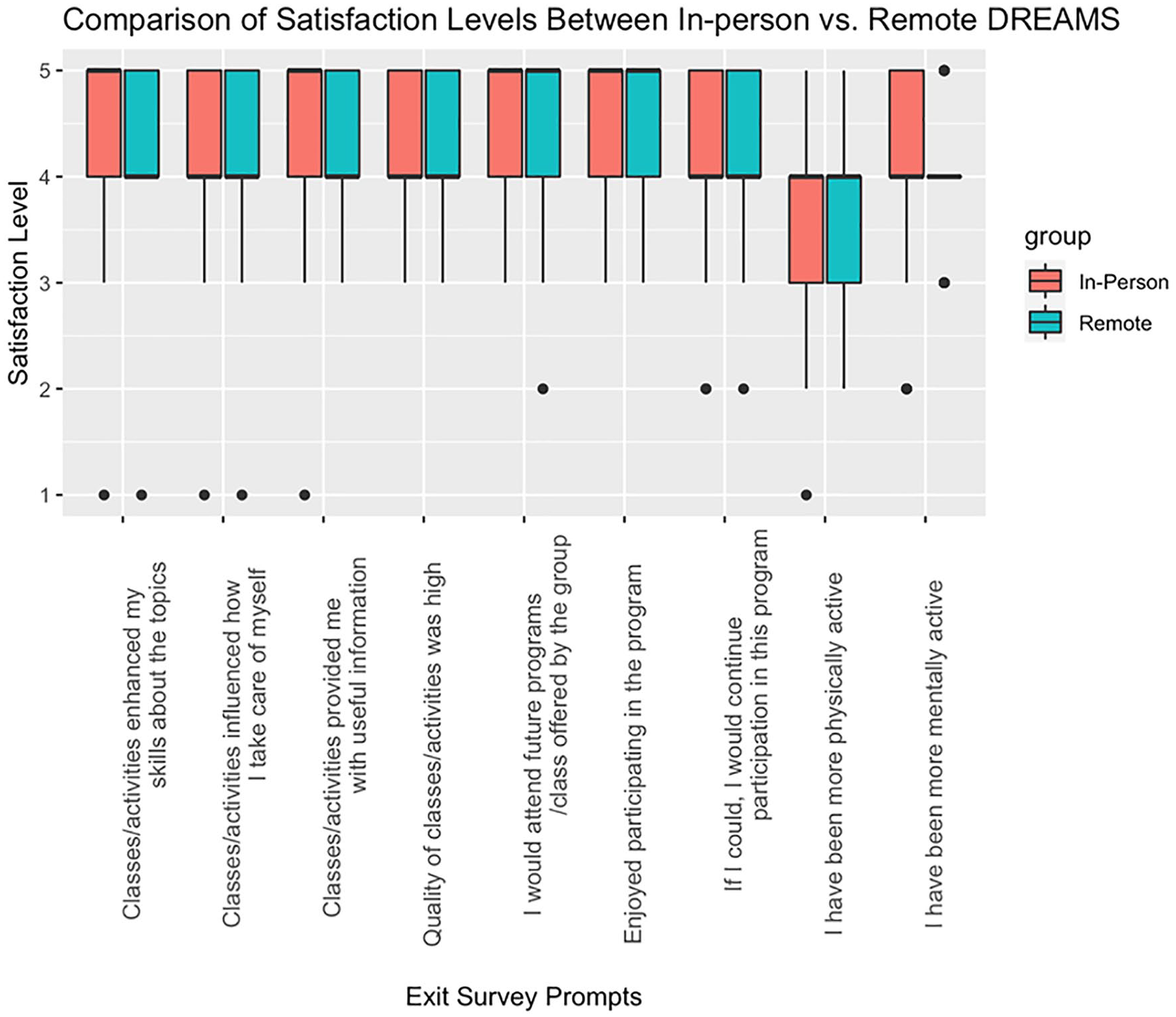
Box and whisker plot comparing satisfaction levels between In-person and Remote DREAMS participants based on exit survey prompts regarding how DREAMS impacted different aspects of participants’ lives and measured via a Likert-type scale (1 = strongly disagree; 2 = strongly agree; 3 = neutral; 4 = agree; 5 = strongly agree).
Responses to open-ended questions reflected positive feedback for future interventions. Many in-person participants stated the nutrition module was their favorite. One participant stated, “I learned some things I can do and food I can eat to maybe keep me from getting dementia or Alzheimer’s—walking, crossword puzzles, and more fruits and vegetables.” Many remote participants stated kidney disease module was their favorite. Suggestions included increasing the length of in-person classes and providing more supplemental materials for remote participants.
Outcome Measures
Significant group effects for performance outcomes adjusted for baseline after intervention were detected.
Health Literacy
Remote participants did not perform significantly differently in comparison to in-person participants on REALM (β = 0.02, p = .5) and S-THOFLA (β = −0.2, p = .1) after intervention.
Cognitive Tasks
Remote participants performed significantly better than in-person participants after intervention on MoCA (β = −0.5, p = .02), TMT B-A (β = 6.1, p = .003), Corsi Blocks number of correct trials (β = −0.2, p = .01) and product score (β = −1.4, p = .03), and Serial 3 Subtractions percentage correct (β = −3.2, p < .001).
In-person participants performed significantly better than remote participants after intervention on ToL mean first move time scaled (β = 0.3, p = .02) (Table 4).
Motor Cognitive Tasks
Remote participants performed significantly better than in-person participants after the intervention on BPST with a greater number of trials completed (β = −0.4, p ≤ .001), greater span (β = −0.3, p ≤ .001), and greater product score (β = −2.8, p < .001); whereas in-person participants performed significantly quicker on TUG-COG (β = −0.3, p = .03) compared to remote participants after intervention (Table 4).
Discussion and Implications
This study compared In-person and Remote DREAMS to examine measures of feasibility, adherence, satisfaction, health literacy, cognition, and motor cognition among older adults. Both models were highly feasible and satisfactory with strong adherence. After adjusting for demographic covariates and baseline values, we cannot conclude that there is a significant difference in health literacy performance for in-person and remote participants postintervention.
We hypothesized in-person participants would exhibit greater overall cognitive and motor cognitive outcomes after intervention compared to remote participants. However, we can conclude that remote participants had an overall greater cognitive performance compared to in-person participants after intervention.
Feasibility
Feasibility of In-person DREAMS suggests this delivery method has potential for successful implementation of group learning. By anticipating programmatic barriers, the group learning protocol was effective with best practices for a successful intervention (Tickle-Degnen, 2013). Remote DREAMS’ feasibility suggests “low-tech” methods with advantages, which telehealth technology programs lack, could be a viable option for future programs (Vaportzis et al., 2017).
Adherence
In-person DREAMS attrition (15%–16%) is relatively low, as other in-person health-education programs have documented 20% to 25% attrition (Amico, 2009; Valentine & McHugh, 2007). Strong adherence may reflect effectiveness of group discussions or development of friendships/camaraderie (Dehi Aroogh & Mohammadi Shahboulaghi, 2020). Age may have played a factor in completion status. Remote DREAMS had 0% attrition, possibly due to this model’s greater accessibility that increased reach to participants with health limitations (e.g., mobile impairments), personalized learning, and reduced social pressure (Hahn & Rahman, 2016). Because of the study design and imbalance in group size, findings should be interpreted with caution.
A post hoc analysis using an independent t-test was performed to compare the age (years) of completers and noncompleters among the whole sample of participants (n = 130). A total of 15 participants were noncompleters, and 115 participants completed either In-Person or Remote DREAMS. Noncompleters were significantly older than completers (M age of noncompleters: 75.53 ± 10.7; M age of completers: 70.29 ± 8.9; p = .04) (Table 5).
Post Hoc Analysis of Adherence Among the Whole Participant Sample (Both In-Person and Remote DREAMS Participants). a
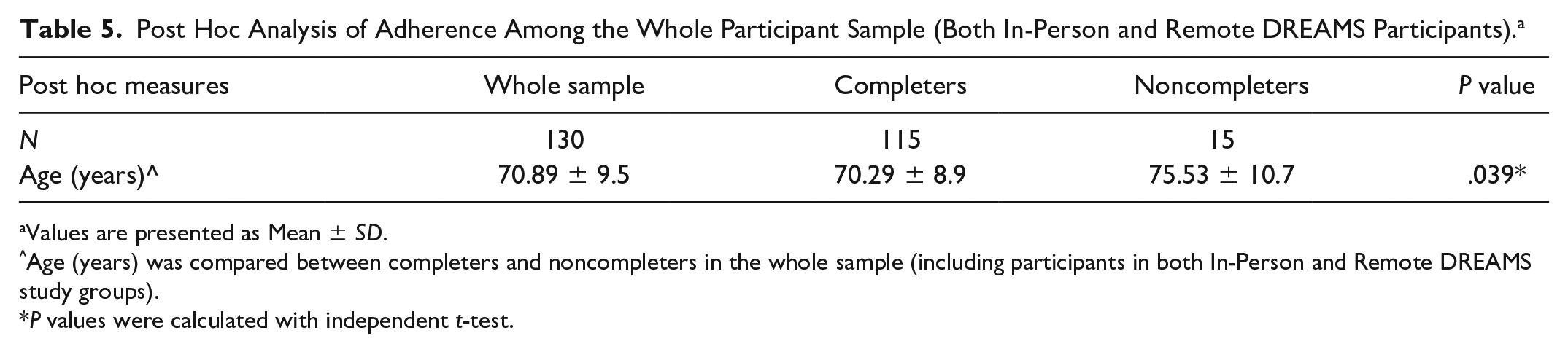
Values are presented as Mean ± SD.
Age (years) was compared between completers and noncompleters in the whole sample (including participants in both In-Person and Remote DREAMS study groups).
P values were calculated with independent t-test.
Satisfaction
Both programs were highly satisfactory. Positive feedback indicated an inclination for continued participation in future research. To further understand the impact of In-person and Remote DREAMS on knowledge acquisition, participants should be assessed in longitudinal evaluations in the future.
Cognitive and Motor Cognitive Performance
Enhanced global cognition among remote participants after intervention suggests solo-coaching methods may prioritize participants’ personalized learning goals. Faster task-switching speed among remote participants may be associated with consistent practice and ample time to understand concepts (Carrier et al., 2015). Collaborative inhibition, the concept that people who remember together while part of a group recall less than if they remembered alone due to memory interference, may explain why in-person participants did not have enhanced working memory after intervention compared to remote participants (Wright & Klumpp, 2004). Better mental tracking was observed in remote participants, perhaps due to less social anxiety and peer distractions during Remote DREAMS. In comparison, interpersonal interactions and perspective taking during In-person DREAMS may lead to enhanced executive function (Perry et al., 2019).
Remote participants learned material at their own pace; therefore, enhanced body spatial cognition may be attributed to the fact that BPST is not a timed test (Battisto et al., 2018). In-person participants had faster motor cognition after intervention. Cognitive and motor function deficits with aging have been elucidated, as geriatric participants may be prone to slower mental processing and motor coordination; however, studies indicate that amplifying social engagement may restore levels of motor activity, contributing to faster motor cognition (Seidler et al., 2010).
Limitations
This study had several limitations. Participants were recruited from metro-Atlanta, so findings may not be generalizable to older populations not living in this region. Unequal sample sizes between study groups were due to remote participants being recruited after in-person participants. Remote DREAMS was developed to reach more underserved and geographically distant individuals, but the model’s resources were limited (e.g., staff to make calls to participants and the take-home binders with lesson plans). Therefore, a convenience sample of 35 individuals was assigned to Remote DREAMS. Participants were not offered a treatment choice. Our study was a nonrandomized two-arm study intervention, thus, unmeasured differences in Remote versus In-person DREAMS may have affected results unknowingly. Unequal sample sizes between groups reduce power to detect effects and increase the chances of making a Type I, that is, “false-positive,” error (Rusticus & Lovato, 2014). Our p values were not corrected for Type I error. This study’s literacy tools may not have detected all effects (Table 3) (Wolf et al., 2009). Other health literacy tools can be considered in the future.
Future Direction
To conclude, aging communities play a vital role in understanding how knowledge acquisition from in-person and remote methods links to health performance. Overall, remote participants had greater cognitive performance (Cyrus et al., 2020). Future measures of clinical significance may indicate how meaningful these performance differences are (Ranganathan et al., 2015). To determine if enhanced cognition among remote participants is a long-lasting effect, a follow-up assessment few years later could be compelling. Specific performance differences between both groups will be utilized to power a larger, controlled trial in the future.
Supplemental Material
sj-docx-1-heb-10.1177_10901981221121258 – Supplemental material for Remote versus In-Person Health Education: Feasibility, Satisfaction, and Health Literacy for Diverse Older Adults
Supplemental material, sj-docx-1-heb-10.1177_10901981221121258 for Remote versus In-Person Health Education: Feasibility, Satisfaction, and Health Literacy for Diverse Older Adults by Anjali R. Shah, Liang Ni, Allison A. Bay, Ariel R. Hart, Molly M. Perkins and Madeleine E. Hackney in Health Education & Behavior
Footnotes
Acknowledgements
All authors contributed to the study conception and design. Material preparation, data collection, and data analysis were performed by L.N., A.A.B., A.H., M.P., and M.E.H. The first draft of this manuscript was written by A.R.S., and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Author’s Note
Anjali R. Shah is also affiliated to Nova Southeastern University College of Osteopathic Medicine, Tampa, FL, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial financial support was received from the Patient-Centered Outcomes Research Institute (PCORI) Award (1099-EU), the National Parkinson Foundation (NPF) Community Grant (A-01), and the Parkinson’s Foundation Grant (PF-PLA-1706).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.