
Abstract
This article reports on a 3-year longitudinal study focused on the impact of cross-sector, collective impact approaches to creating cultures of campus health. The study sought to understand the integration of health and well-being concepts into university operations, including business practices and policies, as well as the contribution of public health initiatives focused on health-promoting universities to creating cultures of campus health for students, staff, and faculty. Research was carried out from spring 2018 to spring 2020 via focus group data collection and rapid qualitative analysis involving template and matrix analysis. A total of 18 focus groups were conducted across the 3-year study, six with students, eight with staff, and four with faculty. The initial cohort included 70 participants: 26 students, 31 staff, and 13 faculty. Qualitative analysis findings indicate a general pattern of change over time from a primary focus on well-being characterized by programs and services (e.g., fitness classes) to policy and structural-level interventions (e.g., stairwell beautification and hydration stations) promoting well-being for all. Grass-top and grassroots leadership and action were instrumental to changes in working and learning environments, policies, and campus environment/infrastructure. This work contributes to the growing literature on health-promoting universities and colleges and demonstrates the critical role of both top-down and ground-up approaches and leadership efforts to create more equitable and sustainable cultures of campus health and well-being.
Keywords
Introduction
Institutions of higher education are an ideal place for public health education and promotion. Akin to small communities or even cities, they serve diverse groups (e.g., students, service workers, senior level faculty, and administrators) and have established governing structures to institute policies and communication channels to disseminate information. Members of these communities spend significant time within the confines of the institution: students often live, work, and study within its borders and employees (administrators, faculty, staff) spend significant time within classrooms, departments, and offices (American Time Use Survey, n.d.; Goetzel & Ozminkowski, 2008; Hill-Mey et al., 2015). Many institutions of higher education have fitness centers, health and medical facilities, and faculty, staff, and student well-being departments and programs (Linnan et al., 2010). Despite being environments germane to public health and well-being initiatives, there has been limited attention to health promotion for all (Travia et al., 2020). Historically, efforts have focused on student health with some, but limited, attention to employee health.
Scholars have only recently implemented whole systems and collective impact approaches, a model that brings together diverse stakeholders across multiple sectors to collaborate and enact large-scale social change (Kania & Kramer, 2011), to promote healthy working, learning, and physical campus environments for all (Black, 2019; Cheney et al., 2020; Slusser et al., 2018; Suarez-Reyes & Van den Broucke, 2016). Leaders within such movements use collective impact approaches to develop and implement environmental interventions intended to foster cultures of health across the entire institution. These healthy campus movements focus on embedding and integrating health and well-being practices and policies into business operations, academia, and overall campus life, creating healthy norms, values, and ultimately cultures. Healthy beverage initiatives aimed to reduce the consumption of sweetened beverages have utilized such approaches to change policy and implement structural-level changes to promote behavior change and reduce consumption of sugar-sweetened beverages, resulting in a positive impact on both health and the environment (Di Sebastiano et al., 2021; Patel & Schmidt, 2021; Rickrode-Fernandez et al., 2021).
To date, much of what we know about campus health is based on students’ perceptions and experiences as well as research on workplace health (Goetzel et al., 2014; Travia et al., 2020). While there is understanding and recognition of institutions of higher education as building and promoting cultures of health, there is a continued need to understand how these institutions can serve as catalysts of change by fostering and maintaining cultures of health within college and university settings (Seifer, 2018).
Given the need for additional research on this topic, we conducted a longitudinal qualitative research study assessing the perceived impact of collective approaches promoting well-being for all and creating healthy campus cultures. Our concept of “cultures of campus health” is informed by definitions and conceptualizations of a culture of health put forth by the Robert Wood Johnson Foundation (RWJF) Culture of Health Framework and the Health Enhancement Research Organization (HERO) which includes 24 key elements (e.g., norms, values, communication, and leadership behavior) that foster employee health and well-being (HERO, 2016; Seifer, 2018). Cultures of campus health refers to learning and working environments within institutions of higher education that are intentionally designed to foster health and well-being among faculty, staff, and students. This article summarizes the key findings of our study involving cohorts of students, staff, and faculty who participated in focus group discussions over three years. The following questions guided this research:
Methods
Setting
The research presented in this article is based on a 3-year longitudinal study carried out at the University of California Riverside (UCR), a 4-year public research institute located in the inland region of southern California with ~24,000 students (20,500 undergraduate and 3,350 graduate and professional students), 8,800 staff, and 1,950 faculty. UCR is part of the Healthy Campus Network (HCN), a UC system-wide initiative promoting innovative reforms in all dimensions of health and well-being with the goal to “make the UC system the healthiest place to work, learn, and live.” The HCN is a robust network of diverse coalitions across all 10 campuses working together to promote both individual campus and system-wide changes that advance a culture of health and well-being. In response to a request for improved collaboration across the campuses, in 2017 former President of the UC system endorsed and provided funding to support healthy campuses across the education system. The original request, put forth by faculty, staff, and students sought to improve communication around food insecurity and incorporate health and well-being in campus activities, programs, business practices, and policies. The initiative set out to build an inter-campus foundation and coordinating structure that provided support, resources, and lessons learned to each campus within the system as they developed their locally specific healthy campus initiatives (Slusser et al., 2018).
The HCN organizes its campus-level population and public health promotion efforts into four RWJF Culture of Health Framework action areas: (a) making health a shared value; (b) fostering cross-sector collaboration; (c) creating healthier, more equitable communities; and (d) strengthening integration of health services and systems (Seifer, 2018); and engages stakeholders both on-campus (administrators, faculty, staff, and students) and off-campus (e.g., public health departments and community-based organizations) in developing and implementing strategies to infuse health into everyday operations, business practices, and academic life. Elsewhere, we report on the UCR Healthy Campus infrastructure, our approach to fostering cross-sector collaborations and initiatives to make health a shared value and build healthier and more equitable campus communities (Cheney et al., 2020).
Longitudinal Study
This 3-year longitudinal study involved the impact of healthy campus efforts on the (a) integration of health and well-being elements into daily operations, (b) promotion of health and well-being for all, and (c) creation of a campus culture of health and well-being. The University of California Riverside Institutional Review Board approved all procedures, measurement tools, and consent forms prior to the start of research.
From spring 2018 to spring 2020, we conducted a total of 18 focus groups, including six with students, eight with staff, and four with faculty. Focus group sizes varied from 2 to 13 participants (most included 6–8 participants). Participants had to be 18 years or older, an active member of the UCR community (e.g., current student or employee, retirees, and alumni), and speak English. Following the guidelines set forth by Guest et al. (2017), we sought to conduct two to three focus groups with each stakeholder group (students, staff, and faculty) per year of the study to accurately identify patterns/themes and reach data saturation. A facilitator and a note-taker attended each focus group: the facilitator read over a consent form, responded to participant concerns and questions, and obtained verbal consent prior to beginning the focus group discussion, while the note-taker took notes on what was shared. In Years 1 and 2 of the study, interviews were conducted in person in a private group space, but Year 3 interviews were conducted via Zoom video conference due to COVID-19 pandemic restrictions. Interviews were audio-recorded and transcribed by professional services and in-house dictation software. Student participants received a US$10 gift card and faculty and staff participants a US$20 gift card to thank them for their time and participation.
Trained team members used a semi-structured interview guide with open-ended questions to elicit information on current health and wellness resources, perceptions of current health and wellness efforts, visions for creating a campus culture of health, and perceptions about the role of leadership, as well as students, staff, and faculty in creating healthy campus cultures. In Years 2 and 3 of the study, an additional question about perceived changes in campus health and well-being was added. In Year 3, a question about COVID-19 was added.
Data Analysis
Template and matrix analysis, a rapid analytic approach used in public health and health services research, was used to conduct cross-case analyses within and across each year of the study (Averill, 2002; Hamilton, 2013). Per year of the study, trained team members read transcripts line by line and inserted data into templates organized by the semi-structured interview questions. The templates summarized the key findings and exemplar quotes per focus group. Then, a matrix (Focus Group × Domain/Interview Question) was created. Template summary data were transferred to the matrix and analyzed to identify themes in responses to each question as well as across the focus group discussions. Data from the matrices created per year of the study were then transferred to a final matrix that enabled an analysis of thematic change over time.
Results
Our initial sample included 70 participants, including 26 students, 31 staff, and 13 faculty, of whom six students, 14 staff, and five faculty participated in the final year of the study. The majority of participants across all 3 years of the study were female staff. Table 1 provides an overview of the total number of focus groups and participants per year of the study.
Focus Groups and Participant Characteristics Per Year of Data Collection.
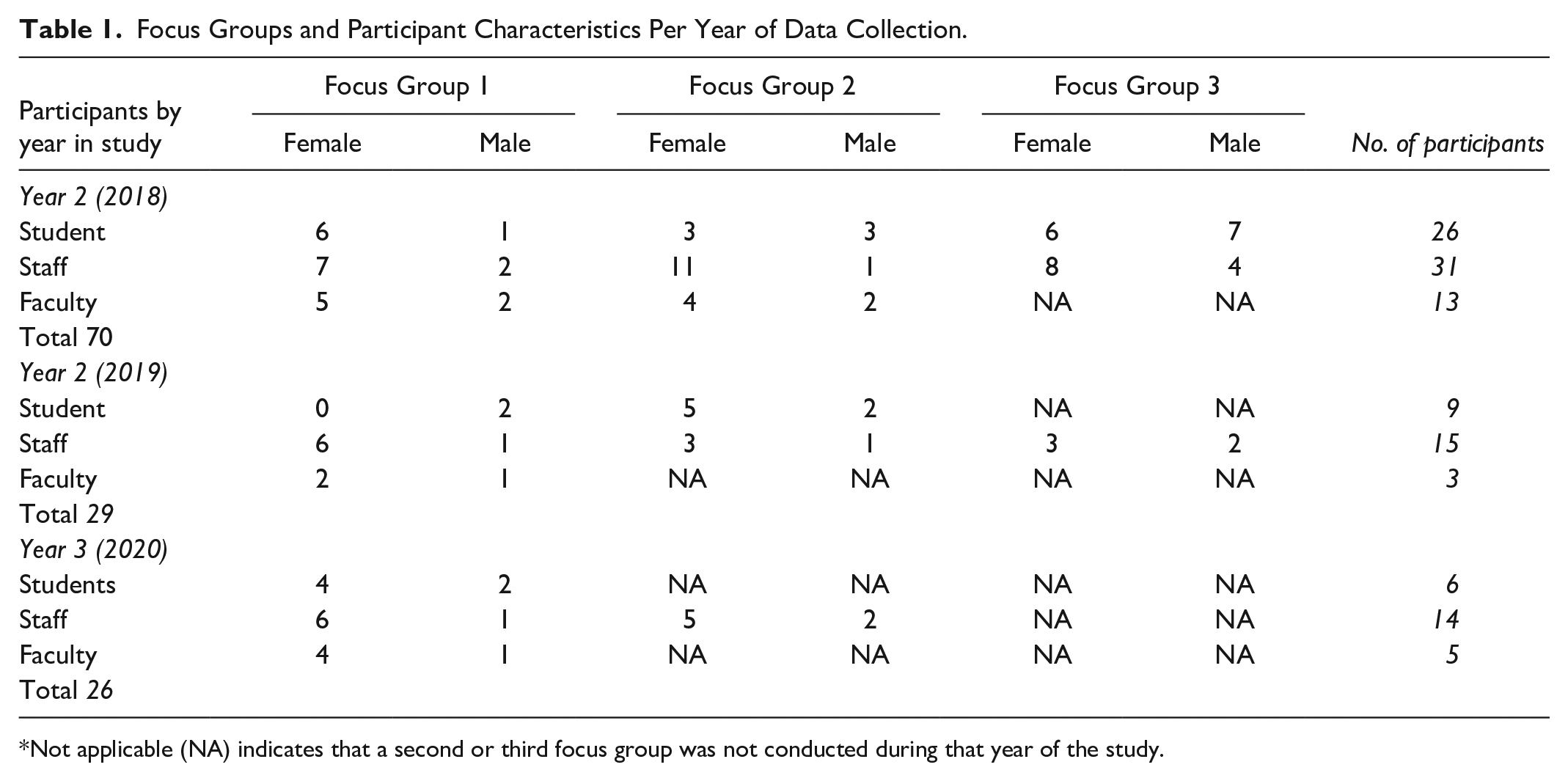
Not applicable (NA) indicates that a second or third focus group was not conducted during that year of the study.
Overview
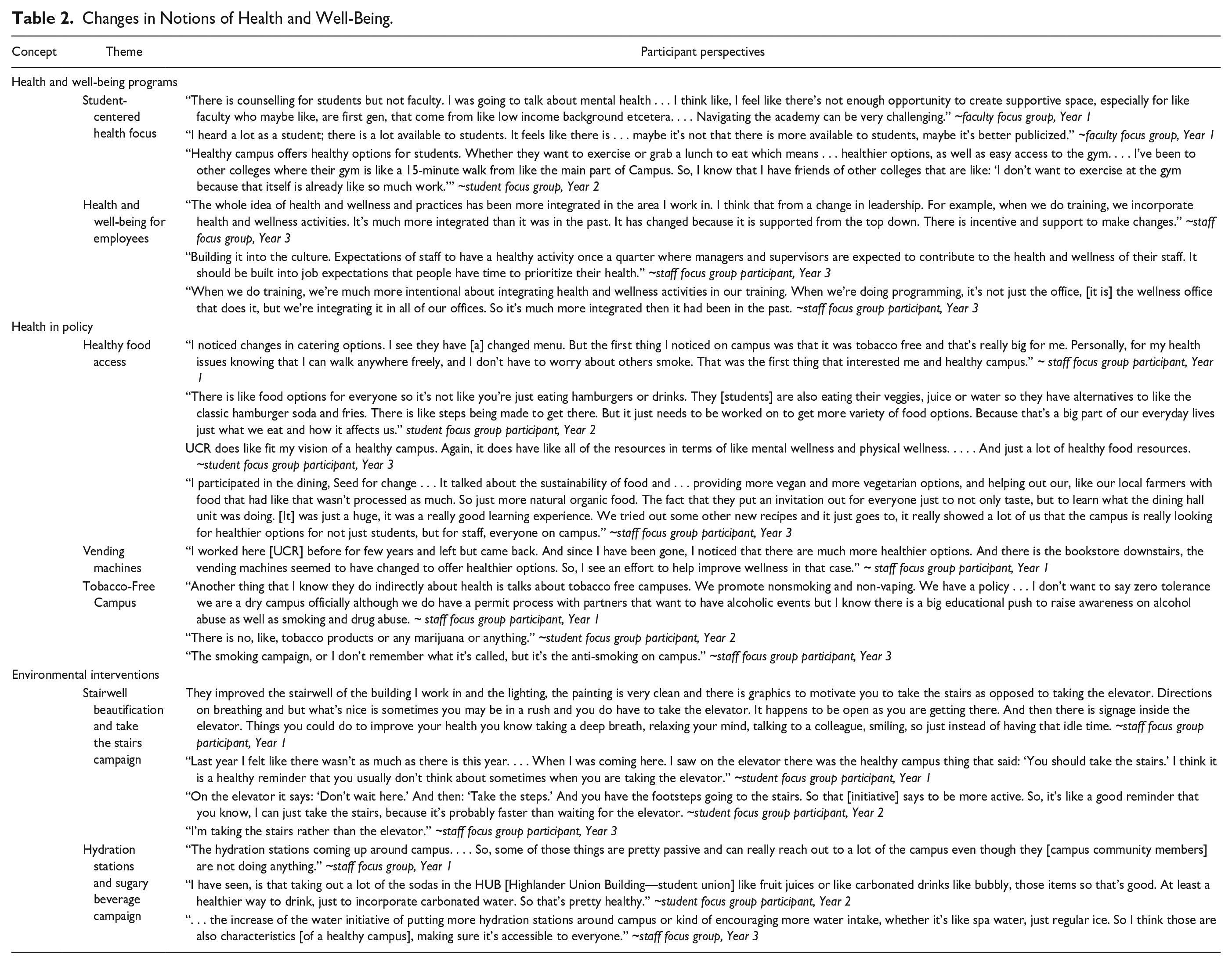
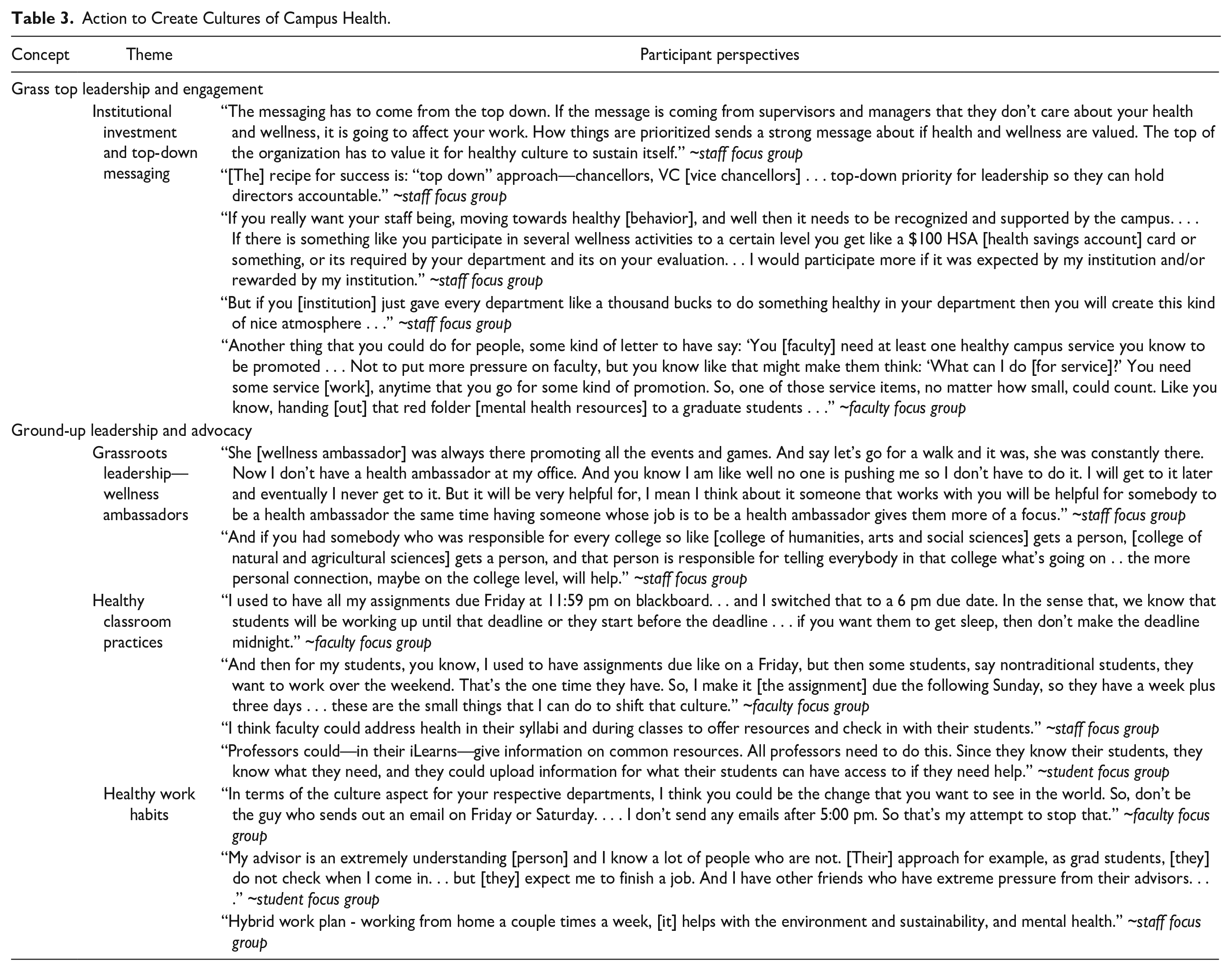
A general pattern of change exists across the 3 years of the study. The shift was from a primarily focus on health and well-being programs and services (e.g., fitness classes and health care services primarily for students) to policy (e.g., smoke and tobacco free) and structural-level interventions involving changes to the built environment (e.g., stairwell beautification, hydration stations, and access to healthy food options) that benefits all—faculty, staff, and students. Over time, participants noted an increase in programs for faculty and staff, campus leadership support for large-scale health events as well as participation in competitions (e.g., healthy departments), and department chairs, faculty, and staff modeling health promotion (e.g., leadership walk and talks, walking meetings). As we describe below, findings indicate that both grass-top action involving leadership enforcement of policy and commitment to campus infrastructure change, and grassroots leadership and advocacy from faculty, staff, and students are necessary to create cultures of campus health. Tables 2 and 3 provide illustrative quotes of how concepts of health and well-being changed over time through public health initiatives (e.g., stairwell beautification and hydration stations), as well as the integration of health and well-being into university operations (e.g., business practices and policies)?
Changes in Notions of Health and Well-Being.
Action to Create Cultures of Campus Health.
Health and Well-Being Programs and Services
In the first year of the study, participants often discussed programs (i.e., individual level services/resources), whereas in Years 2 and 3 participants tended to discuss more so collective campus practices and the integration of health into classroom and business practices. For instance, across all years of the study, there was a strong awareness of student-centered programs, including physical health (student recreation center), mental health (counseling and psychological services), and basic needs (e.g., food pantry)—all services that focused on individual level behavior or services/resources. Similarly for staff and faculty the focus was on the limited services (wellness programs, preventive services) and resources offered to employees. In Years 2 and 3, participants, especially faculty and staff, discussed changes in wellness such as the integration of health into classroom (e.g., healthy deadlines), office (sending emails during business hours), and campus (leaders promoting health) practices.
The focus on programs such as student recreative services, student wellness and mental health care services, and campus-wide health initiatives was linked to campus investment in the services/resources and physical on-campus visibility. Participants were aware of the resources offered by the student wellness department (e.g., running groups) and large-scale staff/faculty wellness activities such as system-wide walks involving campus leadership. They were much less aware of department and campus-level programs for faculty/staff. For instance, a staff member commented: “As far as, faculty and staff goes, I don’t hear very much.” Faculty and staff commented on the lack of access to fitness and recreation services, on-campus preventive care (e.g., flu shots only available for students), and mental health resources.
However, discussion of health and well-being and their existence on campus, as well as awareness and access changed over time. Comments such as “People I talk to take health seriously . . . Healthy Campus is making an impact on staff, faculty, and students” were more present in Year 3 of the study. This change was likely spurred by shifts to campus and system-wide changes in policy, development of a cross-departmental and campus collaborative structure as party of health initiatives, and changes to the built environment (e.g., stairwell beautiful in buildings across campus, implementation of hydration stations).
Policy
Over the 3 years of the study, several policies were either made more visible or implemented by the HCN and UCR Healthy Campus. For instance, since 2014 UC campus policy dictates that all campuses are smoke and tobacco free: “Another thing they [Healthy Campus] do indirectly about health, is, talks about tobacco free campuses. We promote nonsmoking and non-vaping.” UCR Healthy Campus efforts made this policy more visible through signage in strategic locations where smokers were known to gather, as well as annual events held in collaboration with the county public health department to pick up discarded cigarette butts. Participants also discussed healthier options in vending machines and from catering. Such changes were seen as improving individual and campus health. Others discussed the importance of the zero-alcohol tolerance policy and the educational push to raise awareness of alcohol, tobacco, and drug abuse on campus.
Structural Level Interventions
Over the 3 years of the study, the HCN provided funds to change aspects of the built environment of all UC campuses, in particular stairwell beautification and implementation of hydration stations. UCR Healthy Campus also led initiatives to delineate walking, running, and biking paths as well as increase visibility of healthy food options in highly frequented stores. Participants commented on the improvements to the built environment, emphasizing the value of such changes to individual and community health: “They [Healthy Campus] improved the stairwell of the building I work in and the lighting, the painting is very clean and there is graphics to motivate you to take the stairs as opposed to taking the elevator.”
Others mentioned the increase in hydration stations on campus as part of HCN efforts to reduce the consumption of sugary beverages. This illustrates that changes to the built environment collectively benefit the campus community—they extend beyond individual behavior and action to integration of health and well-being as part of daily life and practice. Participants viewed changes to the built environment as evidence of health as a campus value helping move toward a healthy campus community as they “encourage [UCR] communities to be more healthy.” They recommended continued efforts to change the built environment to include more campus spaces for rest, relaxation, and mindfulness activities (e.g., quiet spaces surrounded by natural beauty), shaded walking/running trails for physical activity and stress management, as well as more visible health care services for whole campus preventive health. In addition, staff members advocated for better and more flexible staff mental health services.
Creating Healthy Campus Communities
The findings highlight the importance of grass-top and grassroots leadership and engaged action in creating healthy campus communities, as well as the value of both top-down and ground-up approaches to advance change.
Grass-Top Leadership and Engagement
Participants stressed the importance of campus leadership, those in decision-making positions such as Presidents/Chancellors, Vice Presidents, Provosts, Deans, as well as system-wide leadership in communicating the value of campus health. Participants discussed the importance of openly discussing and modeling health values. For instance, participants discussed campus leadership publicly advocating for increased access for those with disabilities, commenting on senior leaderships participation in walks to recognize “undulating hills to understand what access was like for people.” Such top-level leadership support and commitment formalizes action and sends messages that the campus prioritizes health and well-being across all levels of the organization, recognizing health as a strategic priority across the institution. Staff and faculty participants frequently referred to the importance of UC walks, an annual event across the UC system to promote physical activity: “with the whole campus walks, they’re encouraging staff and students to come out, walk with the chancellor and the provost, and being able to meet people.” High-level leadership engagement in campus activity elevates the profile of health-related events and sends the message that health is valued.
Staff and faculty participants also talked about the importance of department chairs and supervisors in communicating the value of health through ongoing health-related messages and the promotion of resources and services. For instance, staff participants consistently discussed healthier work environments characterized by supervisor accountability, flexible work schedules, work from home options, and mental health breaks.
Creating healthy campus cultures requires top-level leadership support, investment in health resources and infrastructure, and the promotion and encouragement of utilization of programs and services focused on health and well-being.
Ground-Up Leadership and Advocacy
Across the 3 years of the study, participants discussed the role of instructors/professors, wellness ambassadors, and student leaders in creating healthier campus environments. Participants, specifically students and faculty, discussed ways to create healthier classroom environments (e.g., by instating deadlines that promote well-being and selfcare), such as ones that do not encourage late nights and rather promote time management and sleep as well as ones that accommodate diverse student needs (e.g., nontraditional students). Being mindful of diverse student needs and their role in modeling health and well-being in the classroom was also discussed. Comments about health and well-being, as students mentioned, have a lasting impression as they can model healthy behavior: “They [instructors] can just say . . . ‘Take care of yourself’. Something so that students can be like, ‘Okay you know my professor is doing this, let me try eating healthy’.” Instructors/professors can play an instrumental role in changing classroom learning environments by incorporating elements of health into grading, teaching, and scheduling.
Participants also discussed work practices to promote work-life boundaries and respect for others. This included not sending emails outside of business hours (Monday to Friday, 8–5 p.m.), being mindful of others’ competing demands and the expectations on diverse roles in the academy. For instance, graduate students are expected to study and work and must simultaneously prioritize both coursework and research.
Finally, participants discussed grassroots leadership and advocacy for healthy cultures through wellness ambassadors. Faculty and staff participants were aware of existing networks of wellness ambassadors embedded in campus departments/units whose mission is to improve the sense of belonging, community, and well-being.
Discussion
Both ground up and top-down approaches are needed to create a cultural shift toward health as a shared value and movement toward healthier and more equitable campus communities. The findings from this research illustrate the importance of integrating health and well-being practices into educational and work settings, daily operations, and business practices. Our findings reinforce the transformative vision for health-promoting universities and colleges put forth by the Okanagan Charter in that concepts of health and well-being need to be holistic and capture mental and physical well-being, as well as equitable and sustainable for the health of communities, places, and the environment (International Conference on Health Promoting Universities & Colleges, 2015).
Student, staff, and faculty recommendations align with the objectives of Health Promoting University that by definition “promotes healthy and sustainable policies and planning throughout the university” (Suarez-Reyes & Van den Broucke, 2016). This framework also emphasizes personal and social development of campus community members, a broad interest in health promotion, and healthy working and physical environments. Participants in our study similarly discussed more holistic concepts of health and well-being and embedding them into existing learning and working practices and policies (e.g., student orientation, staff recognition, and faculty advancement) in an effort to build cultures of health and healthier and more equitable communities.
Changes to policy is one example of a top-down approach that can be used to initiative culture change. For instance, participants consistently discussed access to healthy food as a key aspect of a healthy campus. Administrators and university leadership can lead efforts to increase access to healthy food options for students, staff, and faculty by setting policy around healthier options in residential halls, retail stores, catering services, and vending options (Rickrode-Fernandez et al., 2021). UC Berkeley was one of the first universities in the nation to enact a campus-wide nutrition policy. The Food and Beverage Choice policy established nutrition standards for retail foodservice and markets, vending machines, athletic concessions, dining halls, and university-sponsored meetings. The policy ensured that in addition to promoting healthier choices through marketing and advertising standards, there were accessible whole, fresh foods and healthier alternatives to sugar-sweetened beverages present in all university food environments.
Another approach is to subsidize healthier options by taxing high sugar drinks (e.g., soda). Researchers at the University of Illinois-Chicago studied the implementation of sugar-sweetened beverage taxes in the city of Seattle, Washington, where the tax was implemented in 2018. They found that the Sweetened Beverage Tax had a sustained impact 2-years post-tax implementation suggesting that sugar-sweetened beverage taxes may yield permanent reductions in demand for sugary beverages and associated health harms (Powell & Leider, 2021; Powell et al., 2021).
As participants indicated, top-down approaches are necessary to better understand the systemic and institutional norms that contribute to stress and poor mental and psychological health such as burnout. Inefficient managers and processes, as well as lack of attention to diversity and inclusion, contribute to high workloads, microaggressions, and burnout. University leadership and administrators can work toward creating healthier campus communities by providing management trainings focused on creating healthy workplace environments that integrate and align with diversity, equity, and inclusion standards to ensure accessibility, inclusivity, and equity to build an organizational culture that improves the employee experience and advances positive health outcomes.
From a ground-up perspective, students, staff, and faculty can begin to take “mental health days” in an effort to prioritize mental health and reduce burnout. Furthermore, ground-up approaches can contribute to creating healthier and more equitable classroom and office cultures. Faculty play an especially critical role in the health and well-being of students and staff as they shape both classroom and office culture through their daily practices. Participants in our study offered ways to create healthy classroom cultures by being mindful of deadlines and considering how some deadlines (e.g., Fridays at midnight) negatively affect sleep patterns, where nonflexible deadlines may have negative impacts on nontraditional students, a student population underrepresented in higher education who may experience competing societal, family, and work demands as well as structural inequities to academic success (Hughes, 1983).
Similarly, faculty discussed setting communication parameters specifically around email to maintain boundaries between work and home life. Deciding not to send emails after 5 p.m. sets a precedent and shapes others’ responses. Sorensen et al. (2018) identified such practices as representative of “best practices” to foster workplace safety, health, and well-being because they promote positive working conditions. They recommend that those in leadership positions (e.g., managers) set policies/practices with parameters around email communication. For instance, managers should not send emails over weekends or expect responses from employees on leave or vacation. This speaks to participants’ recommendations that middle management (e.g., principal investigators and supervisors) need to develop their leadership skills and identify ways to create more flexible and family friendly learning and working environments. Such approaches are critical to accommodate the needs of students, staff, and faculty in higher education in the current COVID-19 pandemic (Vazquez et al., 2022).
Implications of Our Work
This research advances understanding of the ways higher education can integrate health and well-being into institutional practices, accomplished through top-down and ground-up approaches. There has been a strong international and state-wide movement for health-promoting universities and colleges guided by the Okanagan Charter. Its purpose is to guide colleges and universities to be leaders in developing and modeling health-promoting strategies; moving beyond traditional approaches of influencing individual behavior; and moving upstream to systems level and environmental strategies that influence the health and well-being of person, place, and planet (http://ushpcn.org/about/). As our work illustrates, cross-sector collaborations and buy-in from both grass tops (administrators) and grassroots (faculty, staff, and students) is critical to changing politics and everyday practices that incorporate health, which ultimately spur culture change.
Limitations
There are several limitations of study findings. First, there was significant participant attrition especially among students and faculty across the 3 years of the study. For students, this is likely due to graduation; for faculty and staff it may be departure from the university setting. Despite attrition, there was sufficient participation from each stakeholder group (faculty, staff, students) to obtain data saturation across the study period. Second, the overrepresentation of female-identified participants compared to male-identified participants may result in gender response bias and more so reflect the positions they hold within the institutions (e.g., administrative assistants, financial analysts). Third, culture change takes time. A period of 3 years is not sufficient to see a substantial cultural change, which can be undermined when leadership/turnover results in losing trustful grass-tops and grassroots leaders and champions, which was the case at our university. Finally, Year 3 of our study occurred in the context of COVID-19, which shaped conversations of hybrid models of remote and in-person work and learning cultures. We noticed a stronger emphasis on holistic health and emotional well-being, including mental, social, and physical health, and the need for campus leadership to prioritize campus health in the pandemic and postpandemic period.
Conclusion
Health-promoting institutions can infuse health into everyday operations, business practices, and academic mandates (Suarez-Reyes & Van den Broucke, 2016). University administrators and leadership need to communicate the value of health via ongoing health messages as well as promote health-related resources, policies, and practices. By doing so, institutions can create campus cultures of care, compassion, well-being, equity and social justice, enhancing the potential success of all members of its community while also strengthening the social and economic sustainability of our surrounding communities and society more generally (International Conference on Health Promoting Universities & Colleges, 2015). The COVID-19 pandemic has necessitated new models of learning and working (e.g., hybrid teaching and tele-commuting), creating classroom and workplace flexibility (Vázquez et al., 2022). In this context, higher education must consider how remote learning/working and social distancing impacts social connection, psychological well-being, and healthy habits. Institutions of higher education, especially public research universities, generate and disseminate new knowledge through scholarship and scientific discovery, making them ideal settings to promote health, well-being, and shared values of health among learners and workers, which can influence the health of families, communities, and society more generally (WHO: https://www.who.int/).
Footnotes
Acknowledgements
The authors thank Jo Gerrard at the University of California, Riverside School of Medicine, for her editorial support, as well as all Healthy Campus team members, advisory board members, subcommittee co-leads and student assistants, and healthy campus champions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was, in part, funded by the University of California Office of the President system-wide funding for the development and implementation of healthy campus infrastructures.